Embed Size (px)
Citation preview
8-1
Anatomy and Physiology, Seventh Edition
Rod R. SeeleyIdaho State UniversityTrent D. StephensIdaho State UniversityPhilip TatePhoenix College
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
*See PowerPoint Image Slides for all figures and tables pre-inserted into PowerPoint without notes.
Chapter 08Chapter 08
Lecture OutlineLecture Outline**
8-2
Articulations or Joints
• Articulation or Joint– Place where two bones (or bone and cartilage)
come together• Arthrology = study of the joints• Kinesiology = study of musculoskeletal• Functions of joints
– Give the skeleton mobility– Hold the skeleton together
• Structure correlated with movement
8-3
Classification of Joints• Structural classes: based on type of
connective tissue type that binds bones and whether or not a joint cavity is present– Fibrous– Cartilaginous– Synovial
• Functional classes: based on degree of motion – Synarthrosis: non-movable– Amphiarthrosis: slightly movable– Diarthrosis: freely movable
8-4
Fibrous Joints
• Characteristics– United by fibrous connective tissue– Have no joint cavity– Move little or none
• Types: – Sutures– Syndesmoses– Gomphoses

8-5
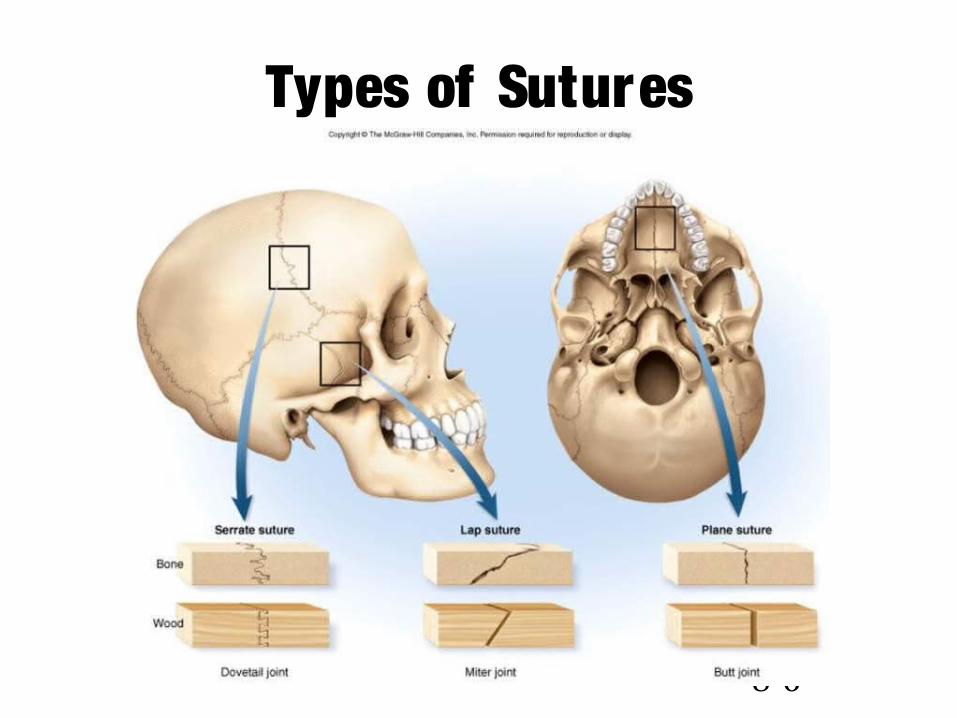
Fibrous Joints: Sutures • Types of sutures
– Serrated: Opposing bones interdigitate (Sagittal suture)– Lap: Over lapping beveled edges (Squamosal suture)– Plane: Straight, non-over lapping edges (Intermaxillary suture)
• Periosteum of one bone is continuous with the per iosteum of the other .
• In adults may ossify completely: synostosis. • Fontanels: membranous areas in the suture between
bones. A llow change in shape of head during bir th and rapid growth of the brain after bir th.
8-6
Types of Sutures
8-7
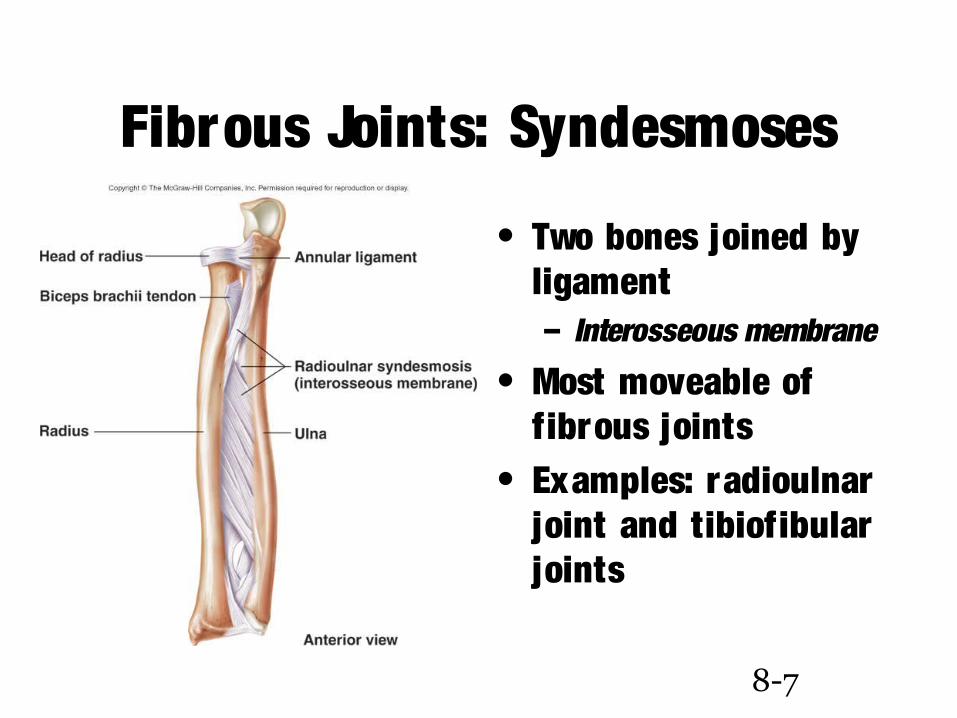
Fibrous Joints: Syndesmoses
• Two bones joined by ligament– Interosseous membrane
• Most moveable of fibrous joints
• Examples: radioulnar joint and tibiofibular joints
8-8
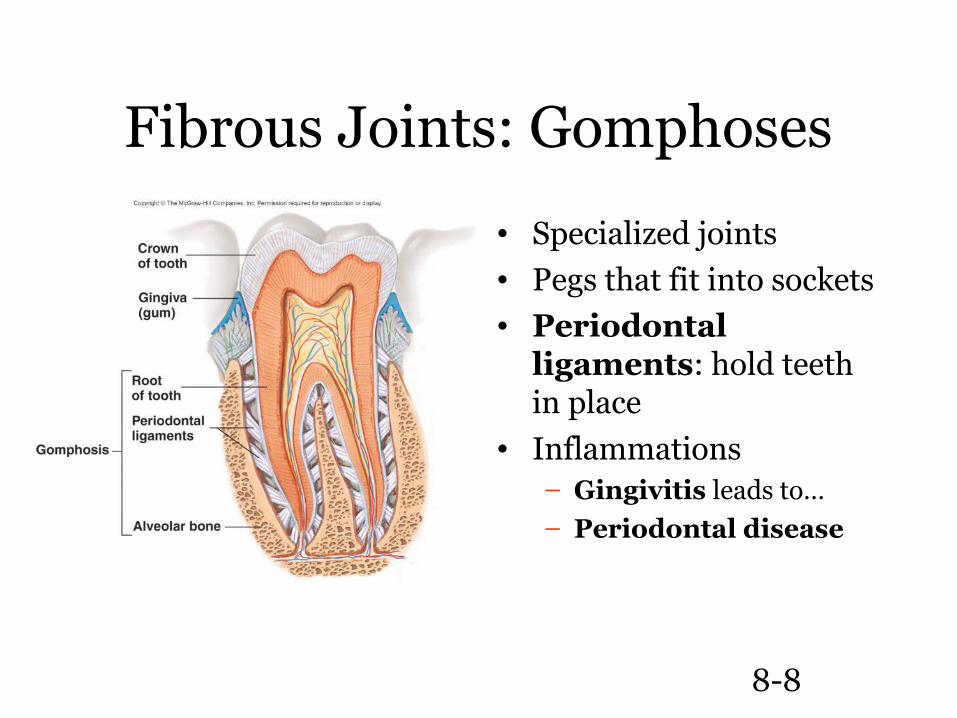
Fibrous Joints: Gomphoses
• Specialized joints• Pegs that fit into sockets• Periodontal
ligaments: hold teeth in place
• Inflammations– Gingivitis leads to…– Periodontal disease
8-9
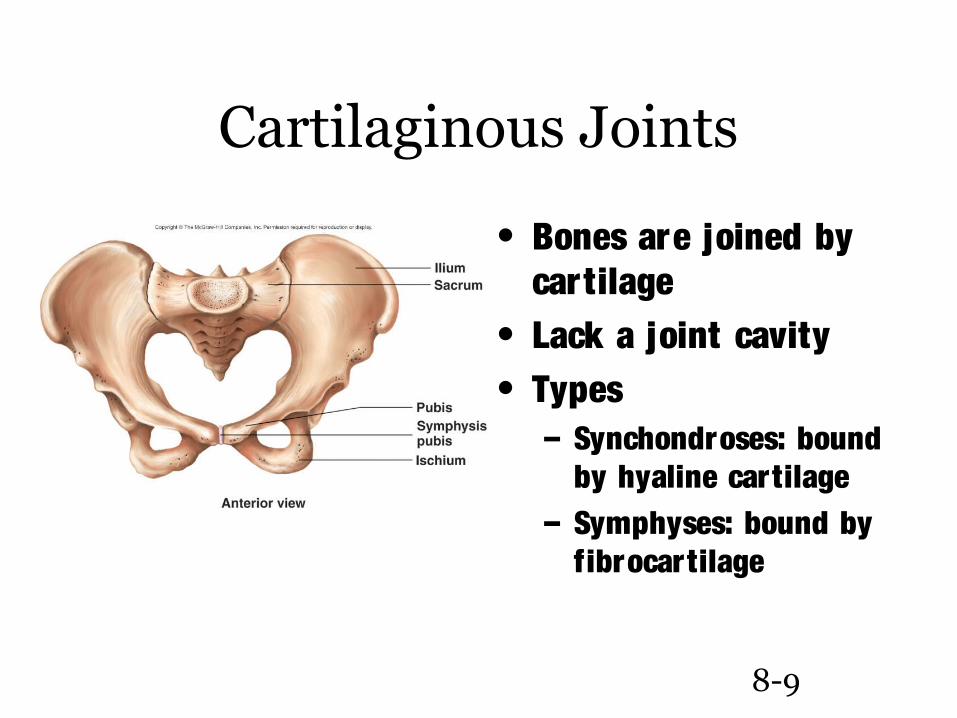
Cartilaginous Joints
• Bones are joined by cartilage
• Lack a joint cavity• Types
– Synchondroses: bound by hyaline cartilage
– Symphyses: bound by fibrocartilage
8-10
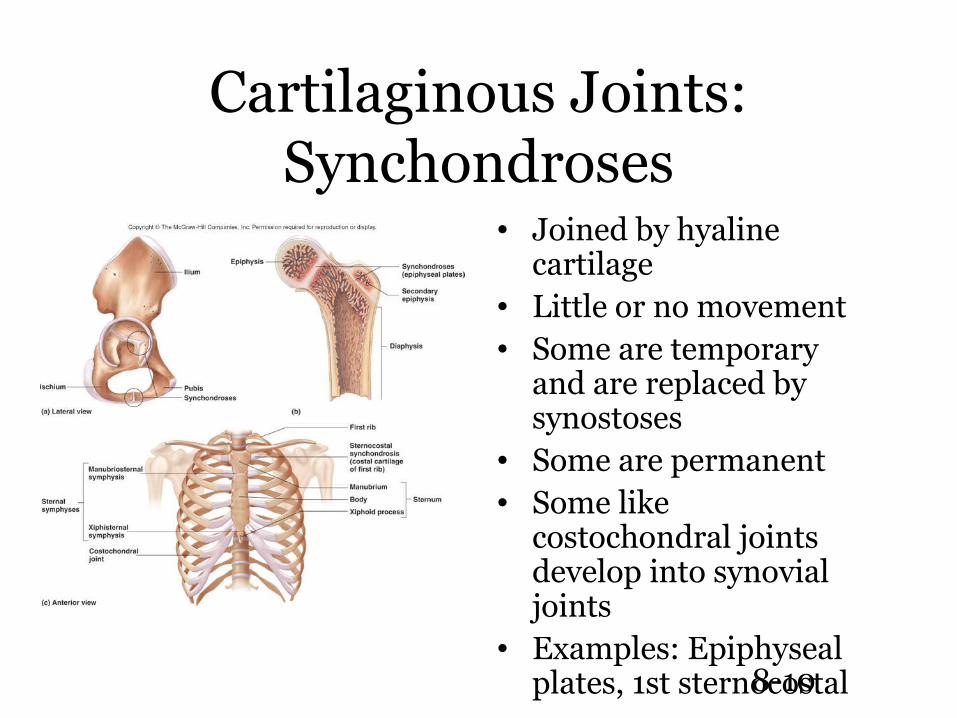
Cartilaginous Joints: Synchondroses
• Joined by hyaline cartilage
• Little or no movement• Some are temporary
and are replaced by synostoses
• Some are permanent• Some like
costochondral joints develop into synovial joints
• Examples: Epiphyseal plates, 1st sternocostal
8-11
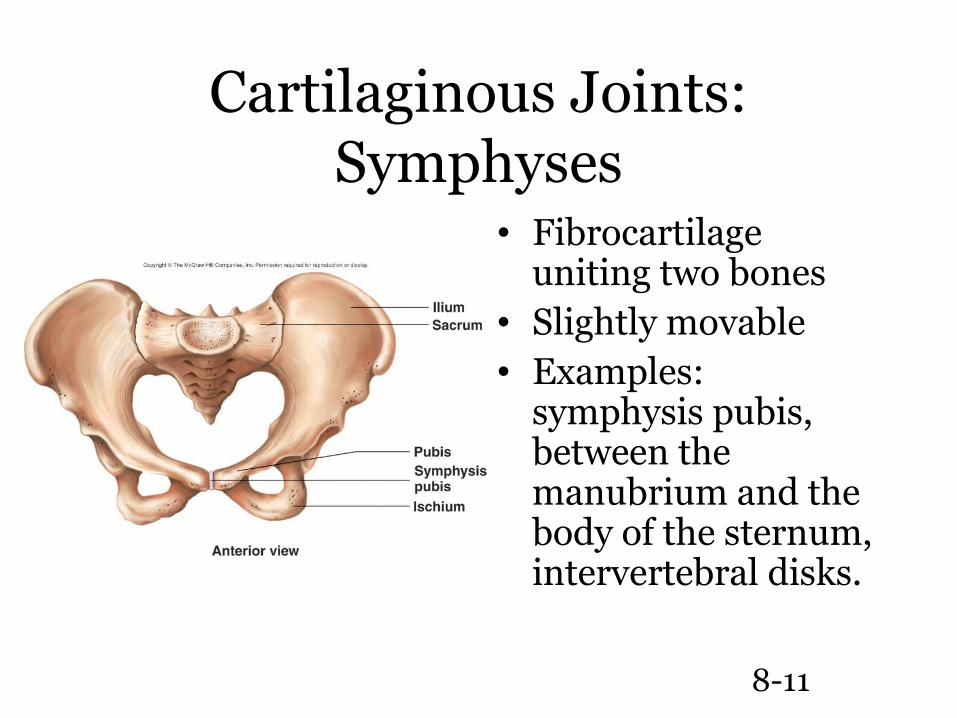
Cartilaginous Joints: Symphyses
• Fibrocartilage uniting two bones
• Slightly movable• Examples:
symphysis pubis, between the manubrium and the body of the sternum, intervertebral disks.
8-12
Synovial Joints
• Contain synovial fluid in a joint cavity called the synovial cavity
• Allow considerable movement (diarthroses)
• Most joints that unite bones of appendicular skeleton reflecting greater mobility of appendicular skeleton compared to axial
8-13
Structure of Synovial
Joints
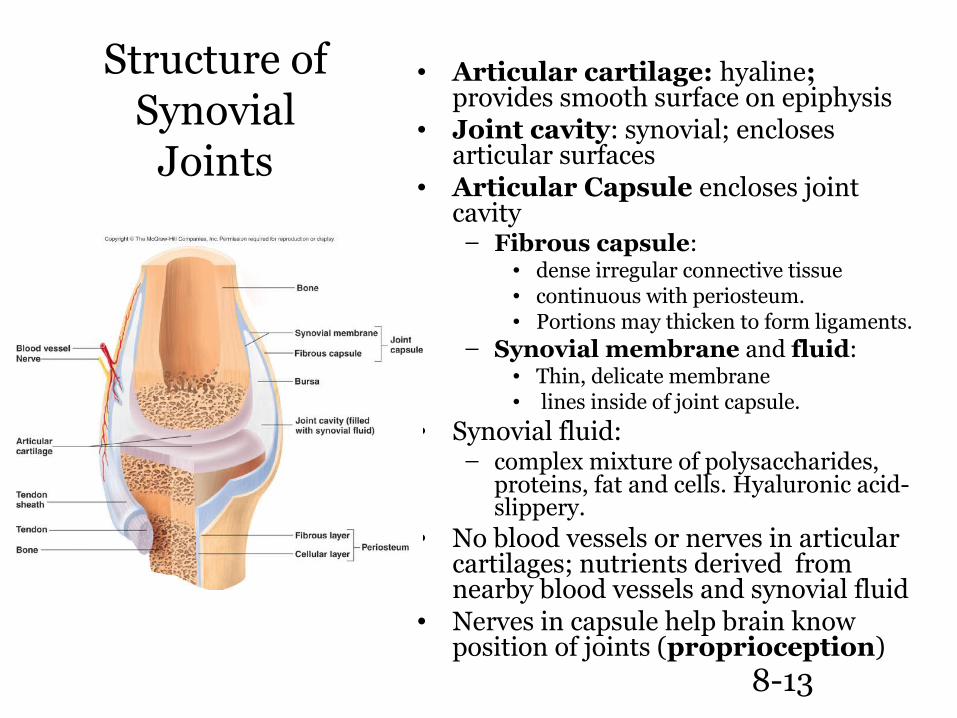
• Articular cartilage: hyaline; provides smooth surface on epiphysis
• Joint cavity: synovial; encloses articular surfaces
• Articular Capsule encloses joint cavity
– Fibrous capsule: • dense irregular connective tissue• continuous with periosteum. • Portions may thicken to form ligaments.
– Synovial membrane and fluid:• Thin, delicate membrane• lines inside of joint capsule.
• Synovial fluid: – complex mixture of polysaccharides,
proteins, fat and cells. Hyaluronic acid- slippery.
• No blood vessels or nerves in articular cartilages; nutrients derived from nearby blood vessels and synovial fluid
• Nerves in capsule help brain know position of joints (proprioception)
8-14
Accessory Structures
• Bursae– Pockets of synovial membrane and fluid that extend from the
joint. Found in areas of friction– Bursitis
• Ligaments and tendons: stabilization• Articular discs: temperomandibular,
sternoclavicular, acromioclavicular• Menisci: fibrocartilaginous pads in the knee.• Tendon sheaths: synovial sacs that surround
tendons as they pass near or over bone
8-15
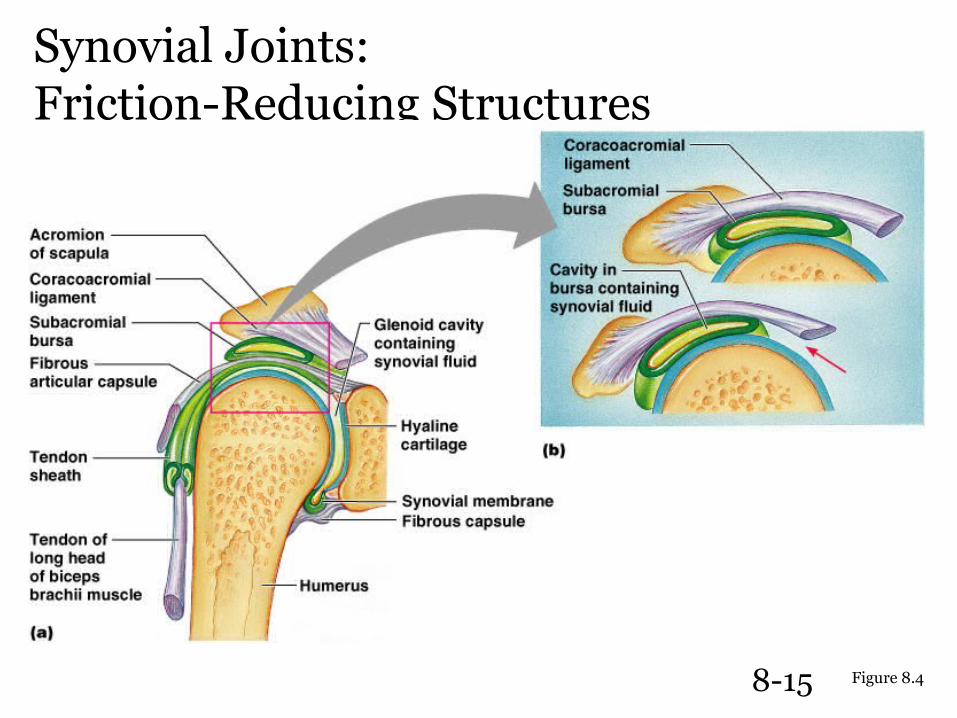
Synovial Joints: Friction-Reducing Structures
Figure 8.4
8-16
Types of Movement
• Gliding: in plane joints; slight movement• Angular
– Flexion and Extension• Hyperextension• Plantar and Dorsiflexion
– Abduction and Adduction
• Circular– Rotation– Pronation and Supination– Circumduction
8-17
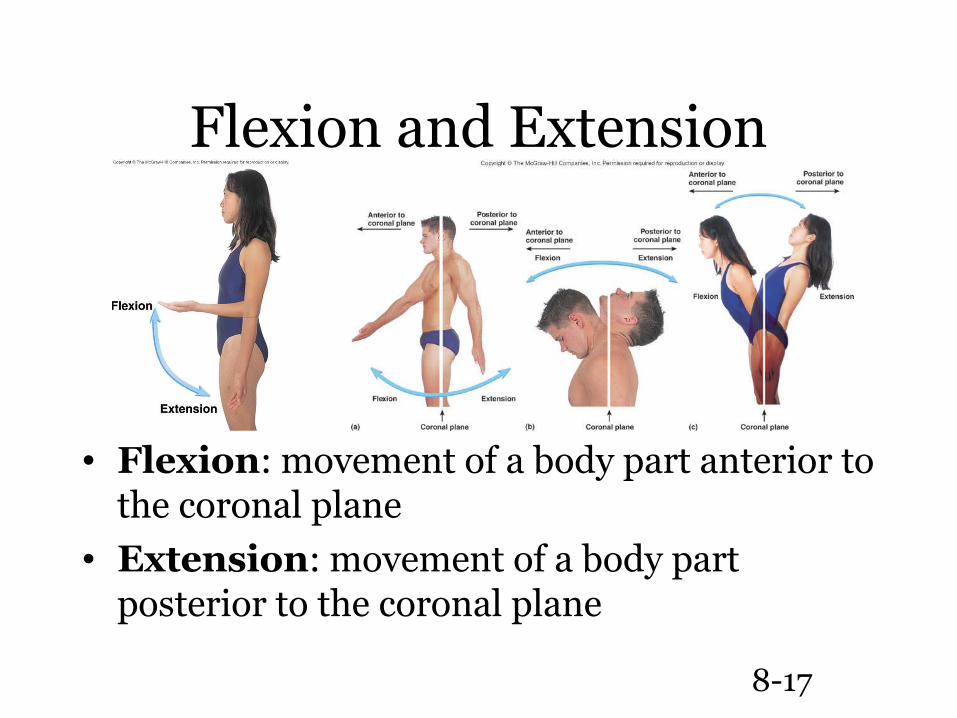
Flexion and Extension
• Flexion: movement of a body part anterior to the coronal plane
• Extension: movement of a body part posterior to the coronal plane
8-18
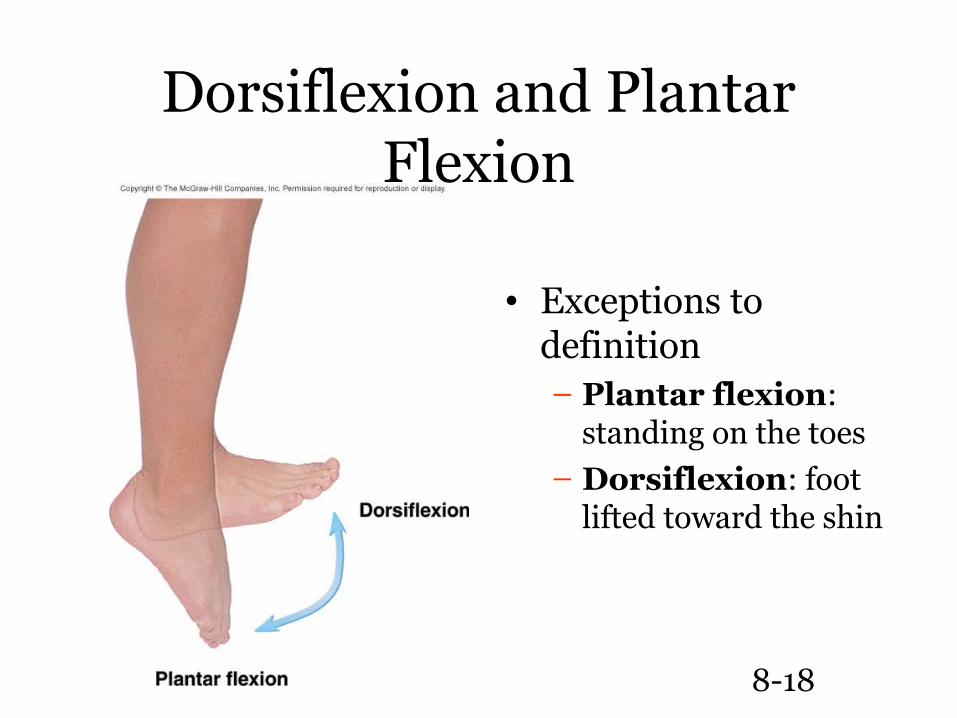
Dorsiflexion and Plantar Flexion
• Exceptions to definition– Plantar flexion:
standing on the toes– Dorsiflexion: foot
lifted toward the shin
8-19
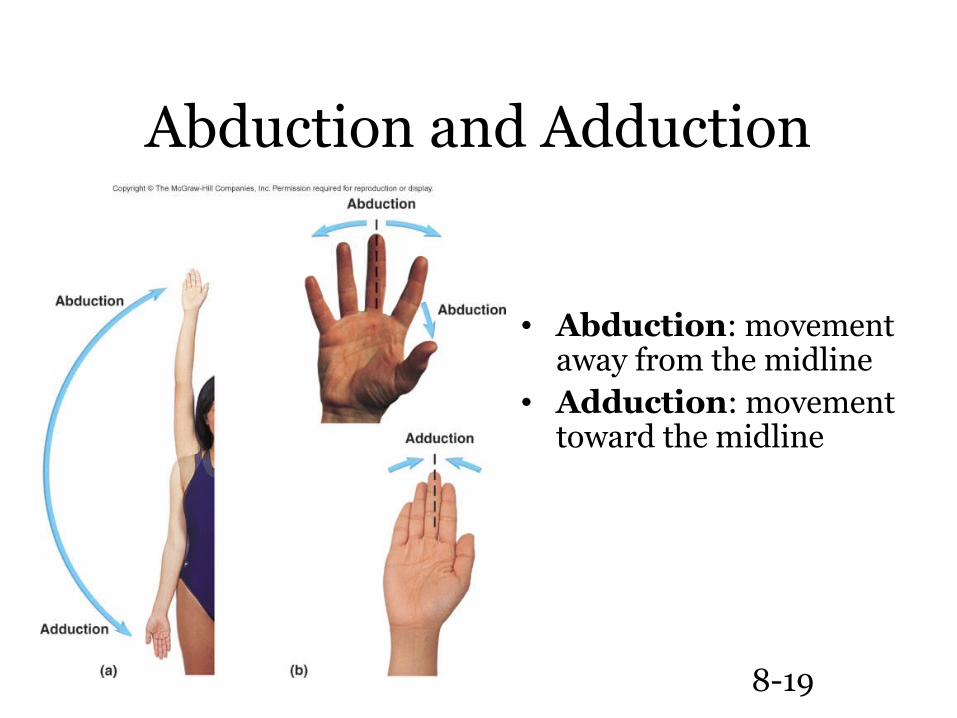
Abduction and Adduction
• Abduction: movement away from the midline
• Adduction: movement toward the midline
8-20
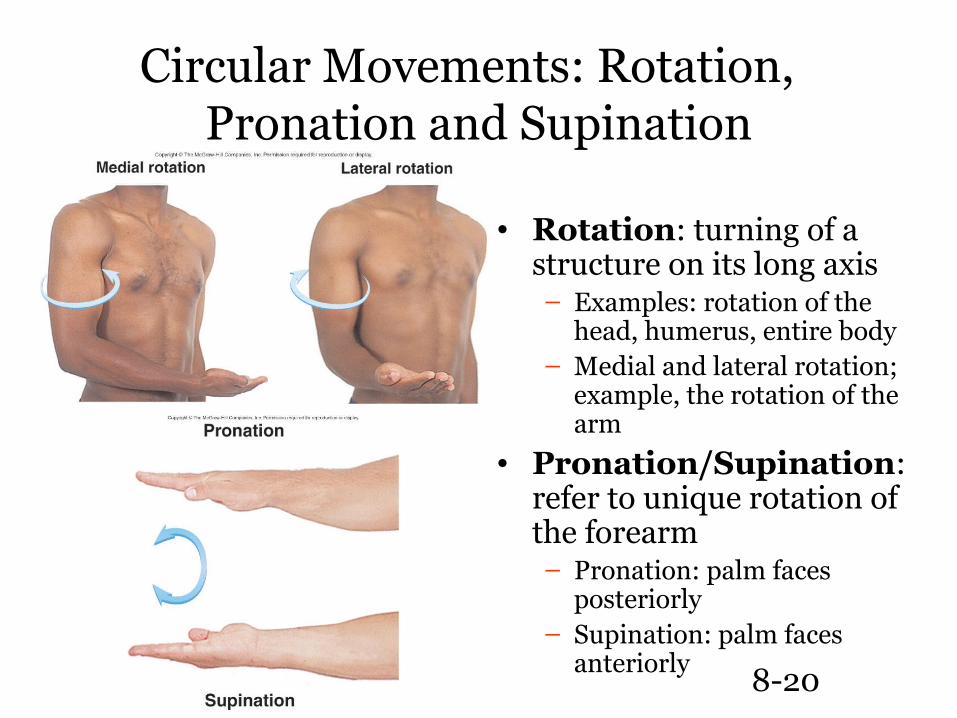
Circular Movements: Rotation, Pronation and Supination
• Rotation: turning of a structure on its long axis– Examples: rotation of the
head, humerus, entire body– Medial and lateral rotation;
example, the rotation of the arm
• Pronation/Supination: refer to unique rotation of the forearm– Pronation: palm faces
posteriorly– Supination: palm faces
anteriorly
8-21
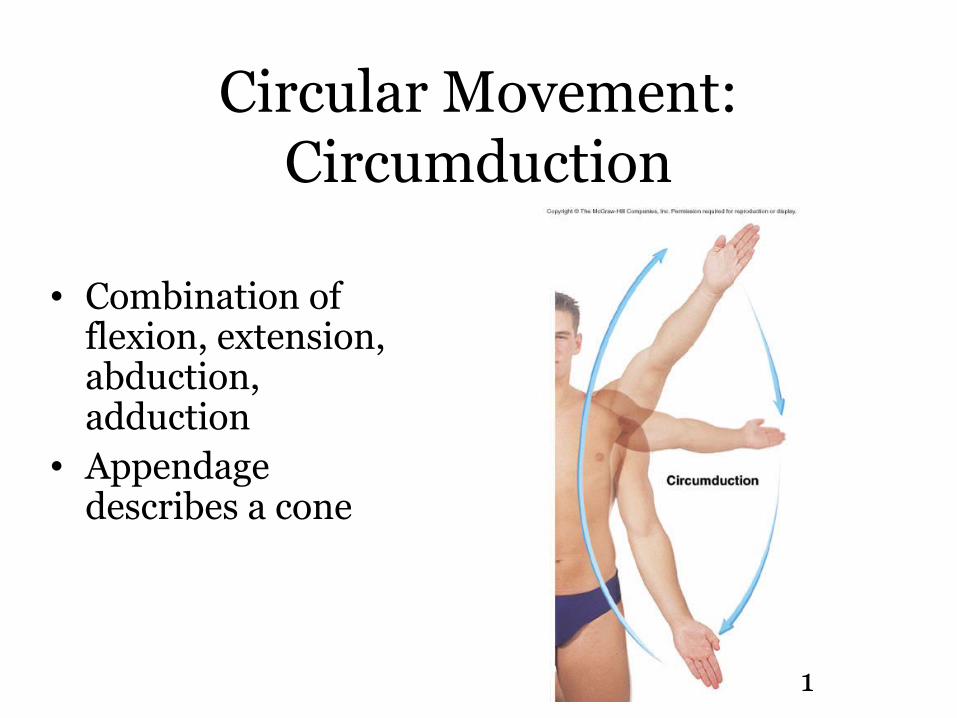
Circular Movement: Circumduction
• Combination of flexion, extension, abduction, adduction
• Appendage describes a cone
8-22
Special Movements
• Unique to only one or two joints• Types
– Elevation and Depression– Protraction and Retraction– Excursion– Opposition and Reposition– Inversion and Eversion
8-23
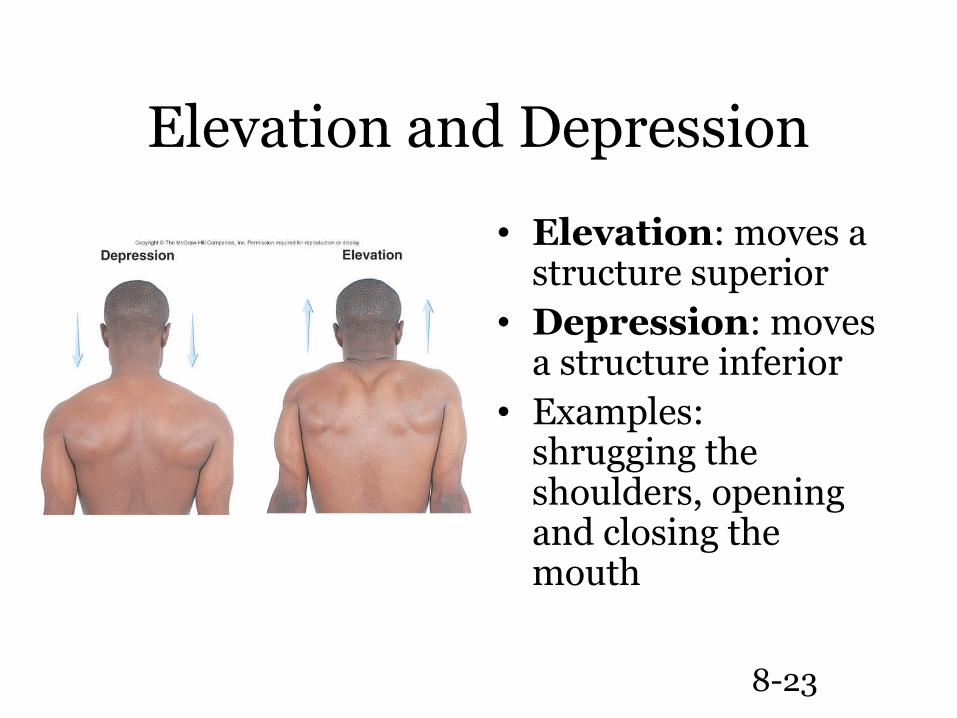
Elevation and Depression
• Elevation: moves a structure superior
• Depression: moves a structure inferior
• Examples: shrugging the shoulders, opening and closing the mouth
8-24
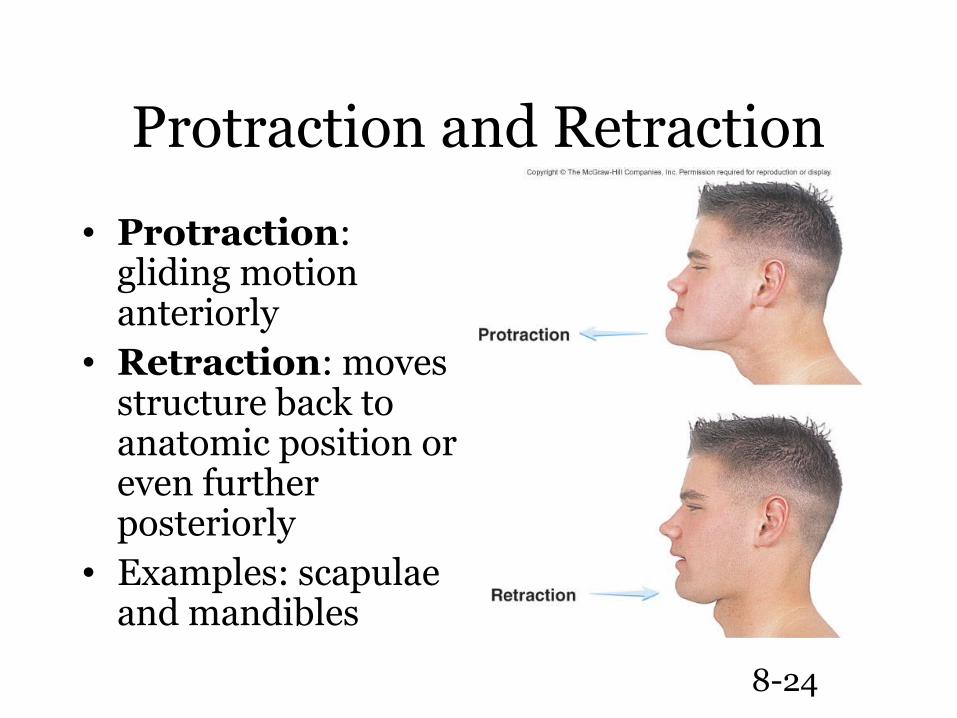
Protraction and Retraction
• Protraction: gliding motion anteriorly
• Retraction: moves structure back to anatomic position or even further posteriorly
• Examples: scapulae and mandibles
8-25
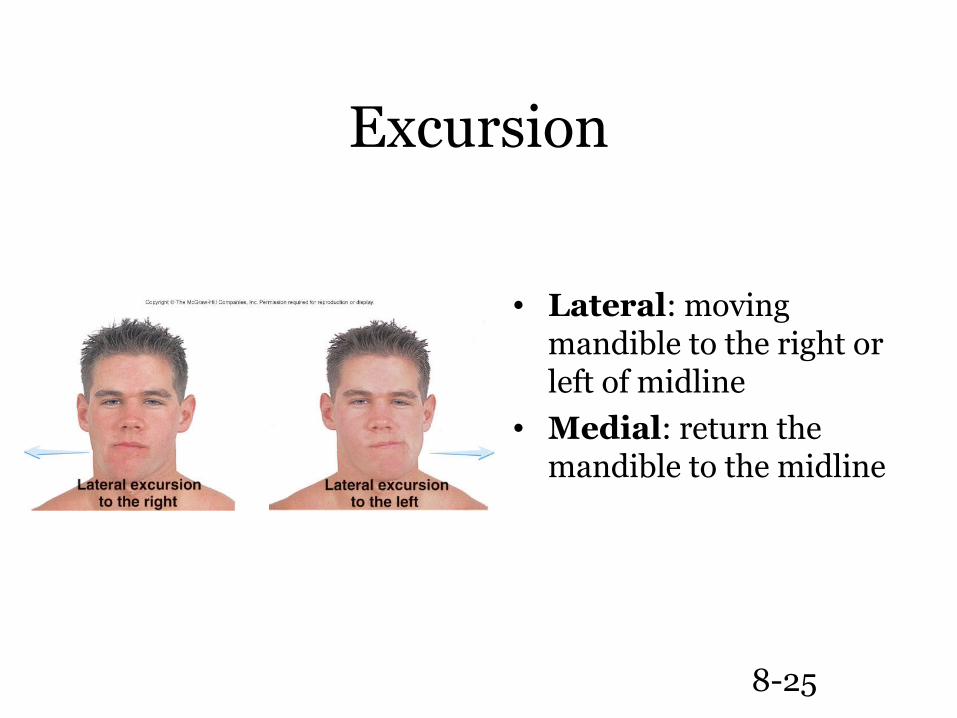
Excursion
• Lateral: moving mandible to the right or left of midline
• Medial: return the mandible to the midline
8-26
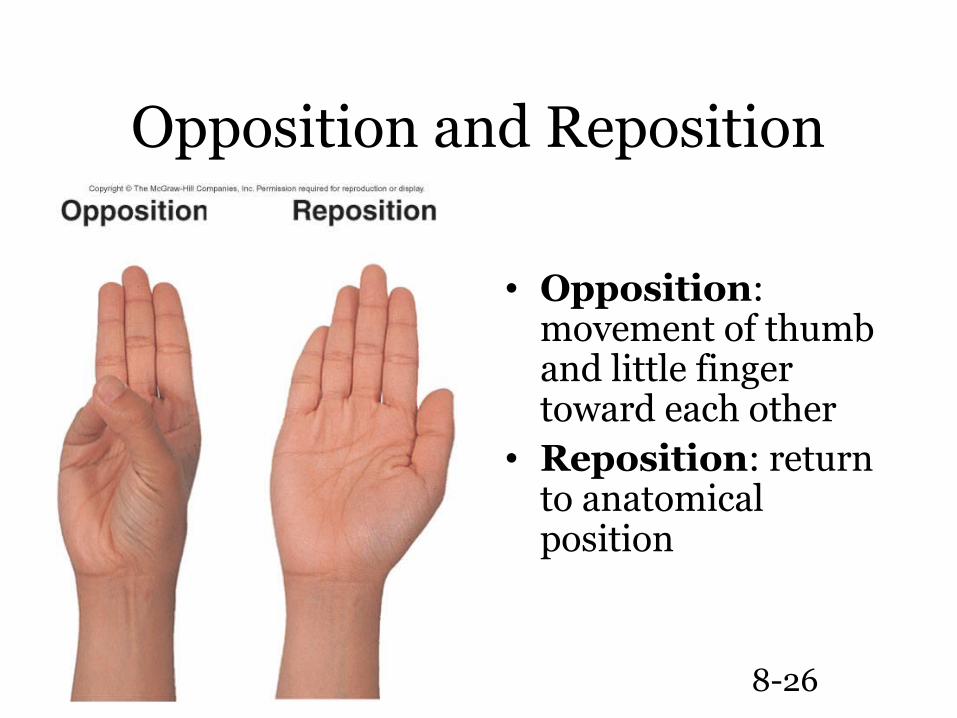
Opposition and Reposition
• Opposition: movement of thumb and little finger toward each other
• Reposition: return to anatomical position
8-27
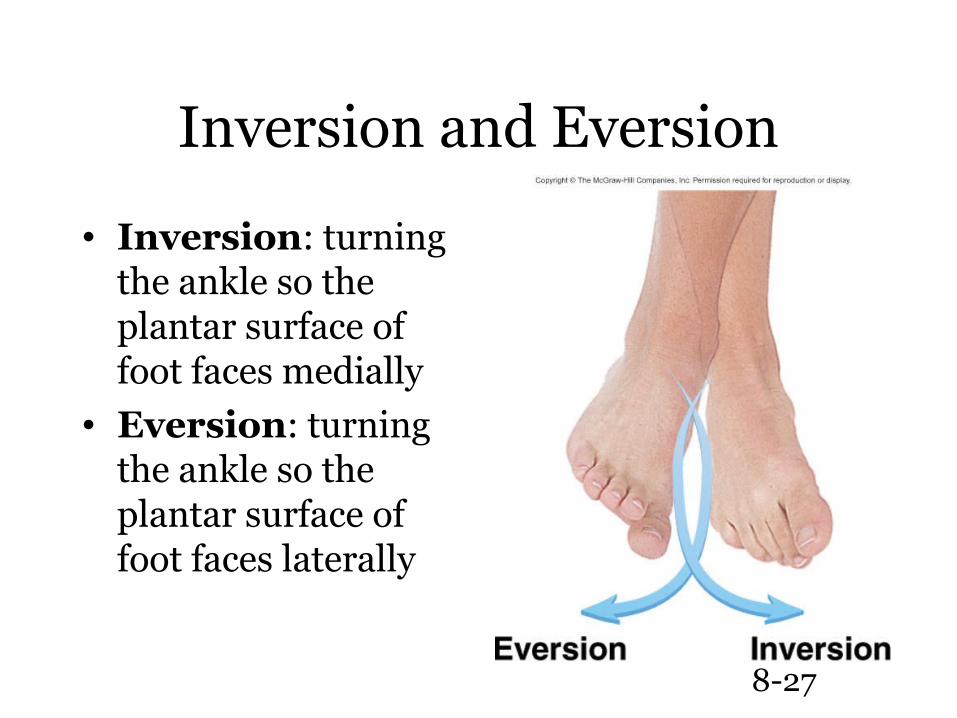
Inversion and Eversion
• Inversion: turning the ankle so the plantar surface of foot faces medially
• Eversion: turning the ankle so the plantar surface of foot faces laterally
8-28
Movements at Synovial joints
• Monoaxial: occurring around one axis• Biaxial: occurring around two axes at
right angles to each other• Multiaxial: occurring around several
axes• See Table 8.2 in text
8-29
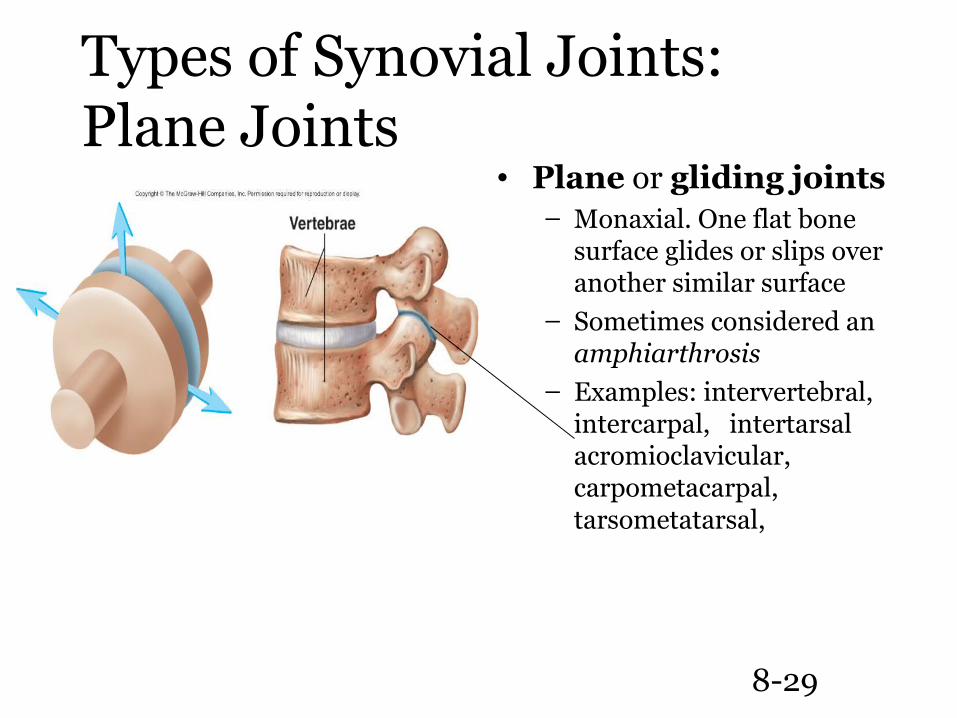
Types of Synovial Joints:Plane Joints
• Plane or gliding joints– Monaxial. One flat bone
surface glides or slips over another similar surface
– Sometimes considered an amphiarthrosis
– Examples: intervertebral, intercarpal, intertarsal acromioclavicular, carpometacarpal, tarsometatarsal,
8-30
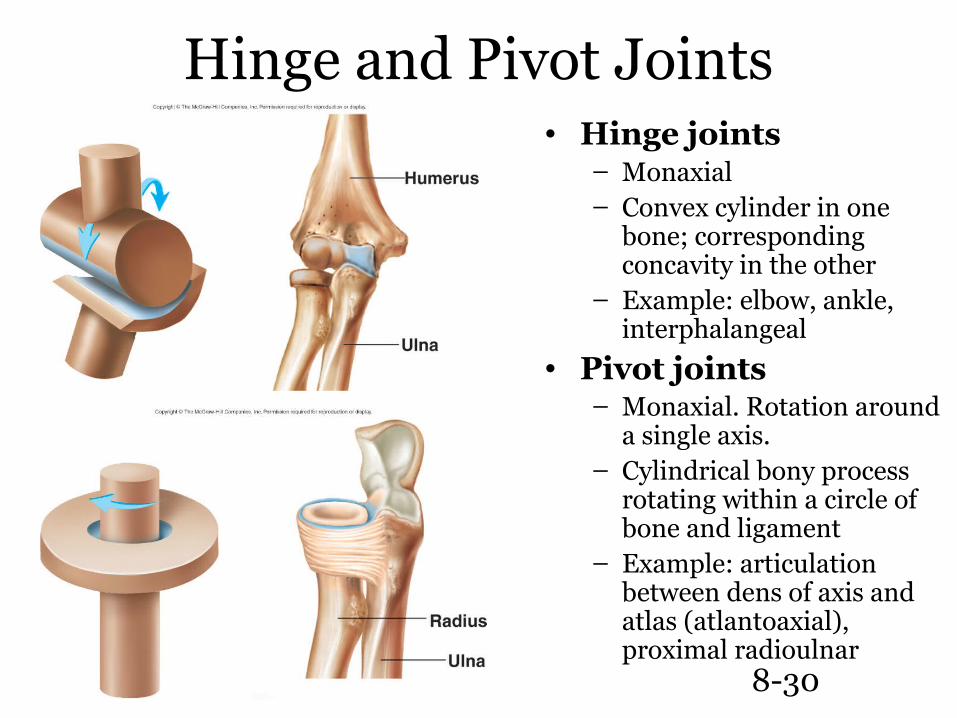
Hinge and Pivot Joints• Hinge joints
– Monaxial– Convex cylinder in one
bone; corresponding concavity in the other
– Example: elbow, ankle, interphalangeal
• Pivot joints– Monaxial. Rotation around
a single axis.– Cylindrical bony process
rotating within a circle of bone and ligament
– Example: articulation between dens of axis and atlas (atlantoaxial), proximal radioulnar
8-31
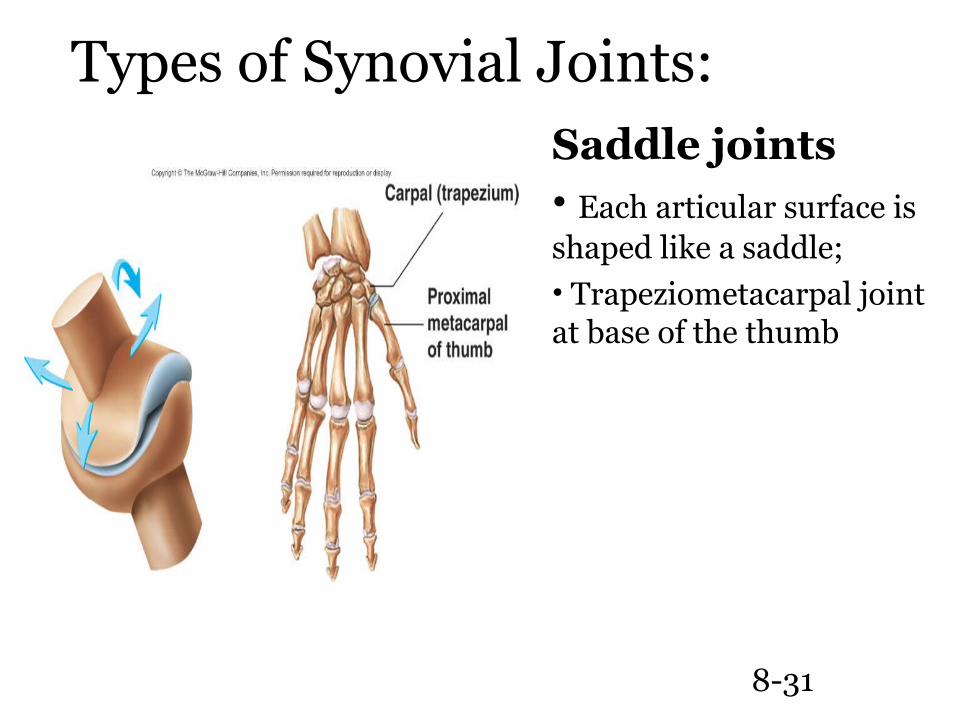
Saddle joints• Each articular surface is shaped like a saddle; • Trapeziometacarpal joint at base of the thumb
Types of Synovial Joints:
8-32
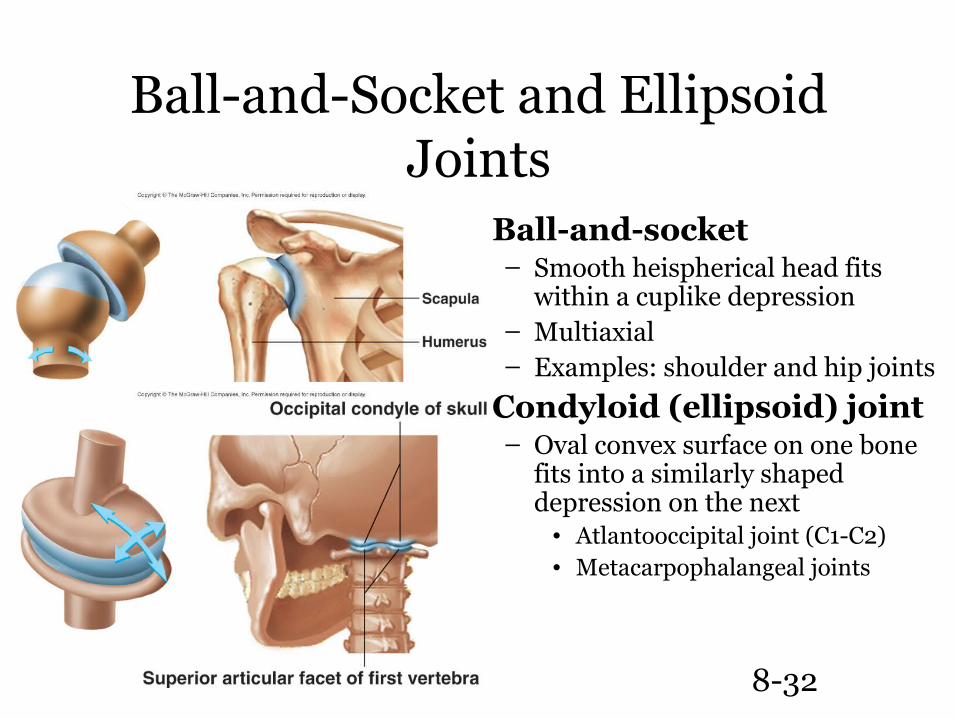
Ball-and-Socket and Ellipsoid Joints
• Ball-and-socket– Smooth heispherical head fits
within a cuplike depression– Multiaxial– Examples: shoulder and hip joints
• Condyloid (ellipsoid) joint– Oval convex surface on one bone
fits into a similarly shaped depression on the next
• Atlantooccipital joint (C1-C2)• Metacarpophalangeal joints
8-33
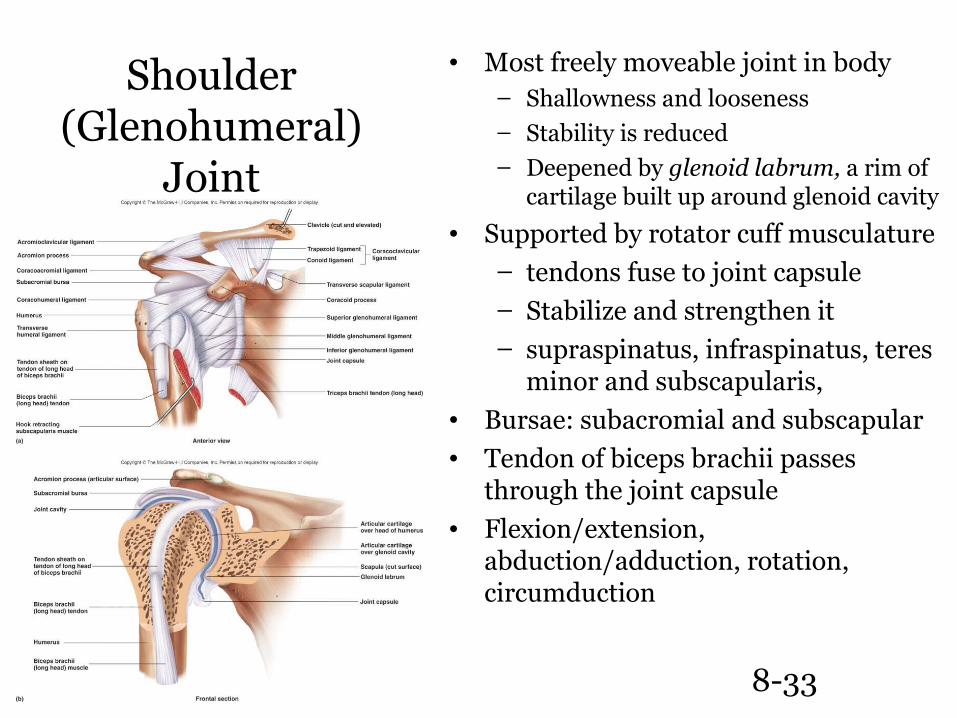
Shoulder (Glenohumeral)
Joint
• Most freely moveable joint in body– Shallowness and looseness– Stability is reduced– Deepened by glenoid labrum, a rim of
cartilage built up around glenoid cavity
• Supported by rotator cuff musculature– tendons fuse to joint capsule – Stabilize and strengthen it– supraspinatus, infraspinatus, teres
minor and subscapularis,• Bursae: subacromial and subscapular• Tendon of biceps brachii passes
through the joint capsule• Flexion/extension,
abduction/adduction, rotation, circumduction
8-34
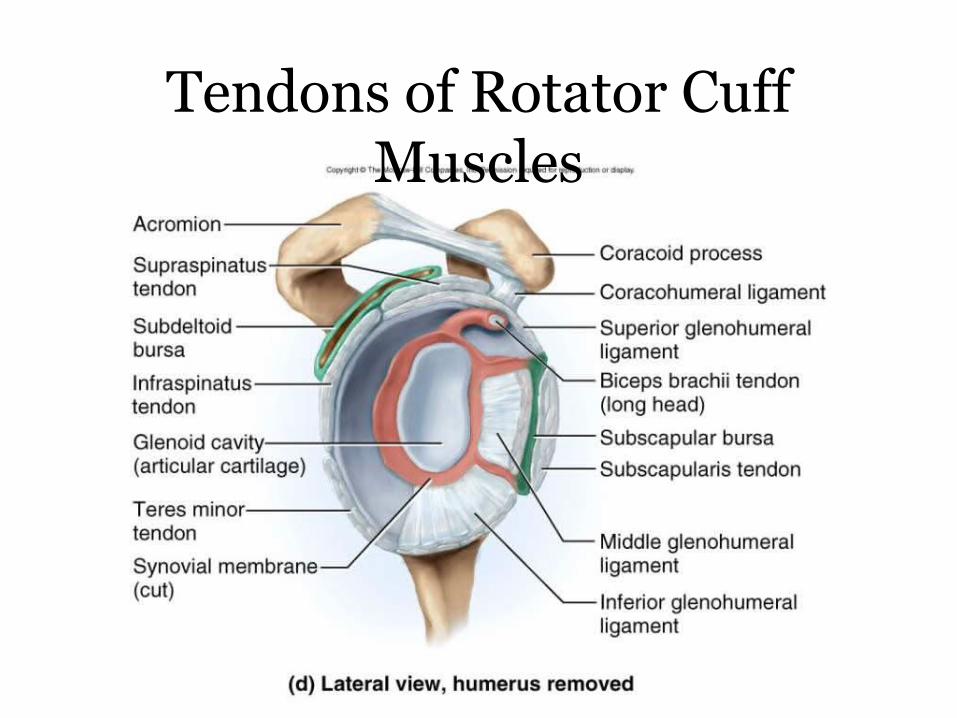
Tendons of Rotator Cuff Muscles
8-35
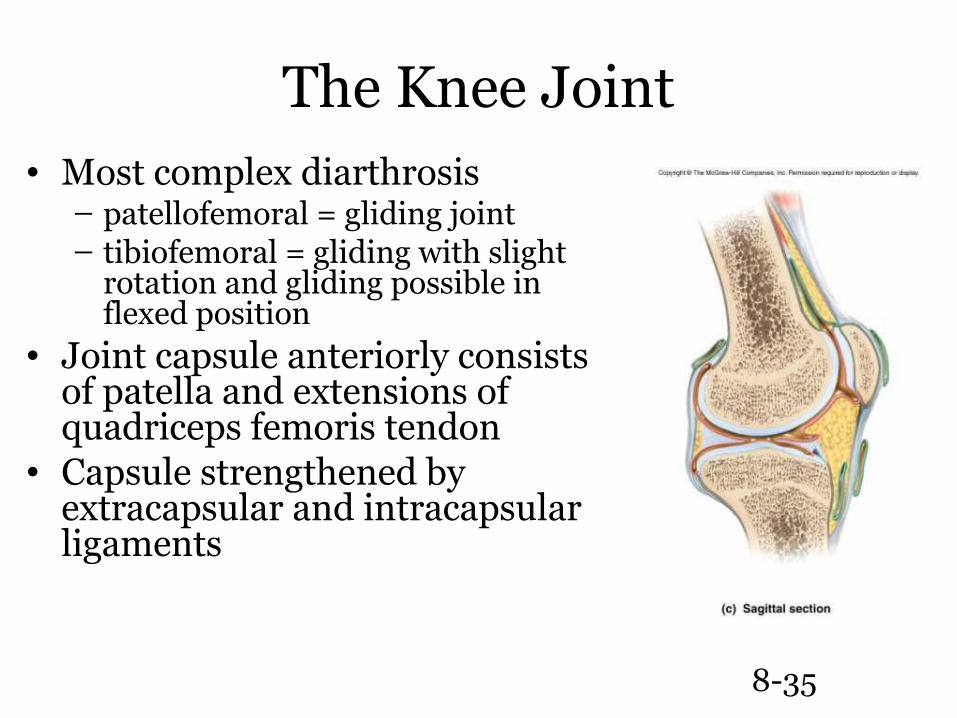
The Knee Joint• Most complex diarthrosis
– patellofemoral = gliding joint– tibiofemoral = gliding with slight
rotation and gliding possible in flexed position
• Joint capsule anteriorly consists of patella and extensions of quadriceps femoris tendon
• Capsule strengthened by extracapsular and intracapsular ligaments
8-36
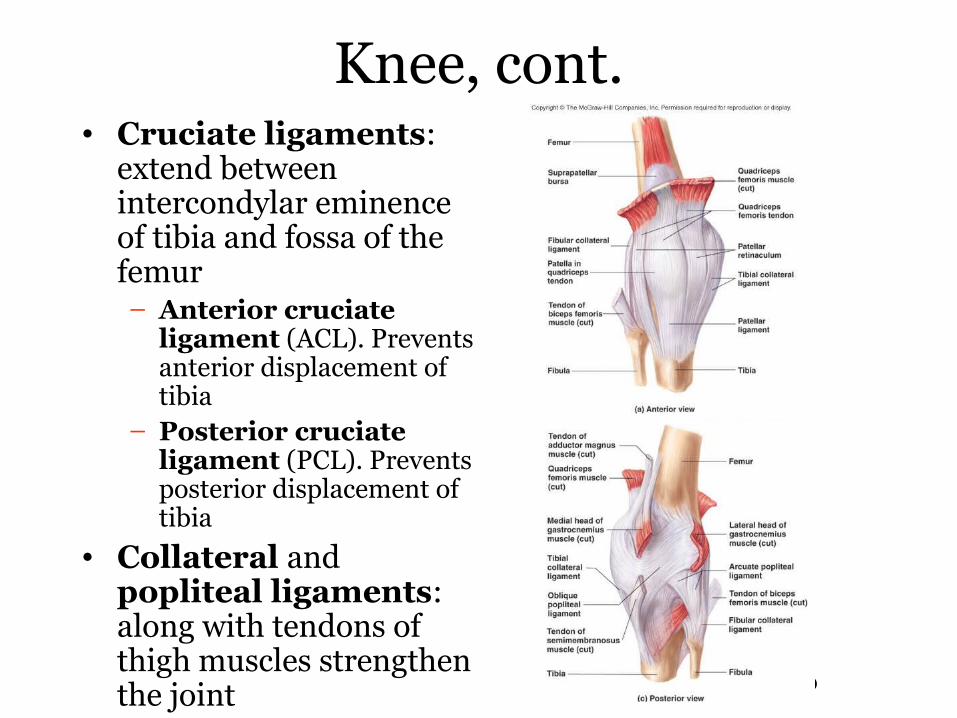
Knee, cont.• Cruciate ligaments:
extend between intercondylar eminence of tibia and fossa of the femur– Anterior cruciate
ligament (ACL). Prevents anterior displacement of tibia
– Posterior cruciate ligament (PCL). Prevents posterior displacement of tibia
• Collateral and popliteal ligaments: along with tendons of thigh muscles strengthen the joint
• Bursae: may result in slow accumulation of fluid in the joint (water on the knee)
8-37
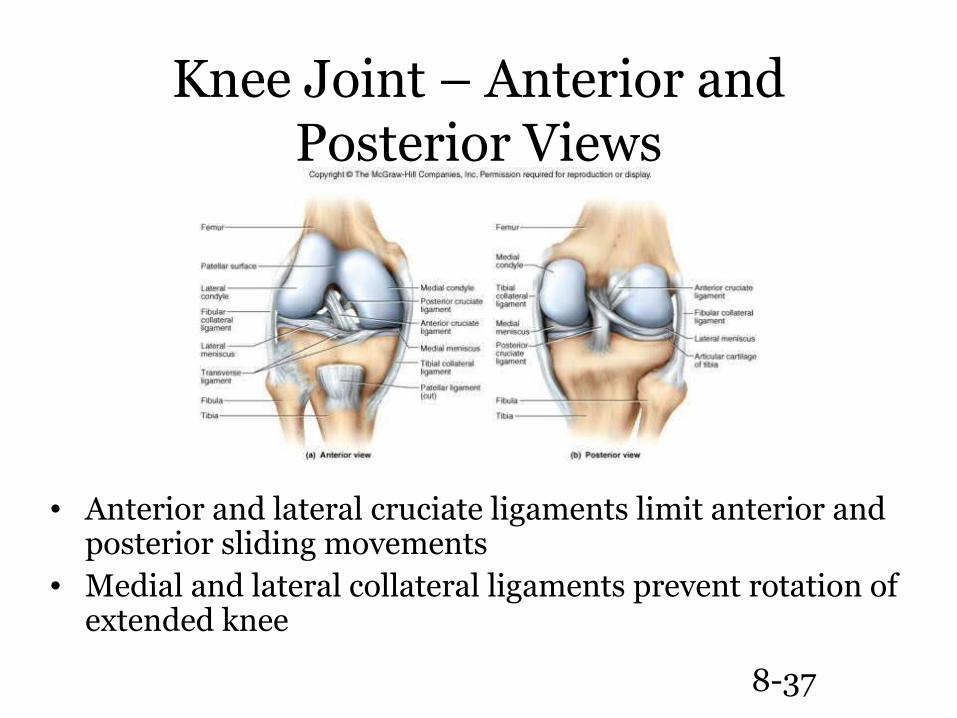
Knee Joint – Anterior and Posterior Views
• Anterior and lateral cruciate ligaments limit anterior and posterior sliding movements
• Medial and lateral collateral ligaments prevent rotation of extended knee
8-38
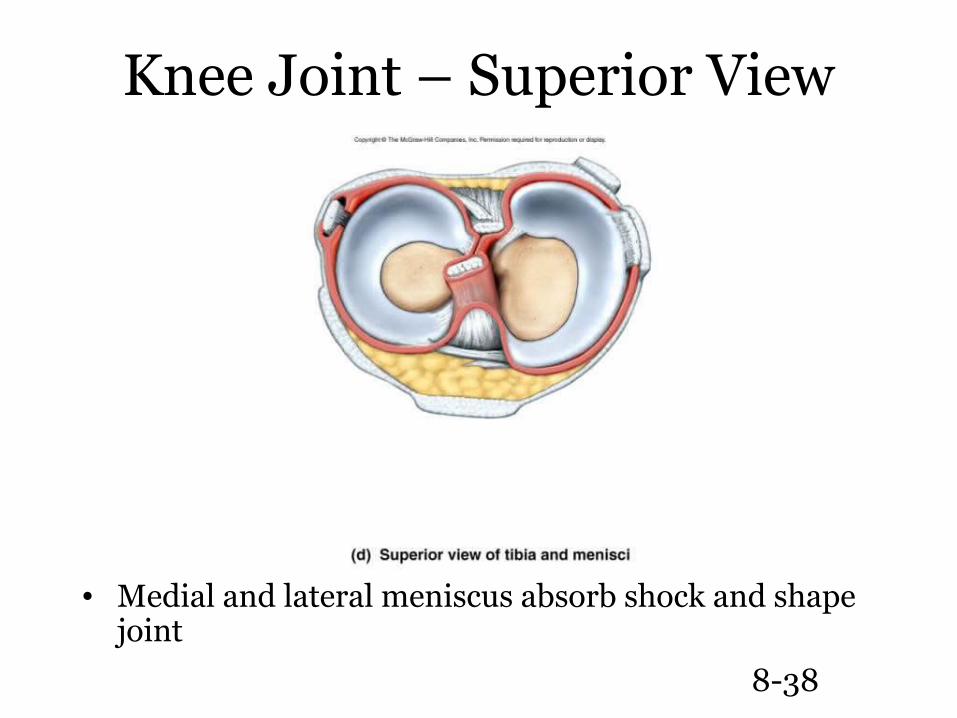
Knee Joint – Superior View
• Medial and lateral meniscus absorb shock and shape joint
8-39
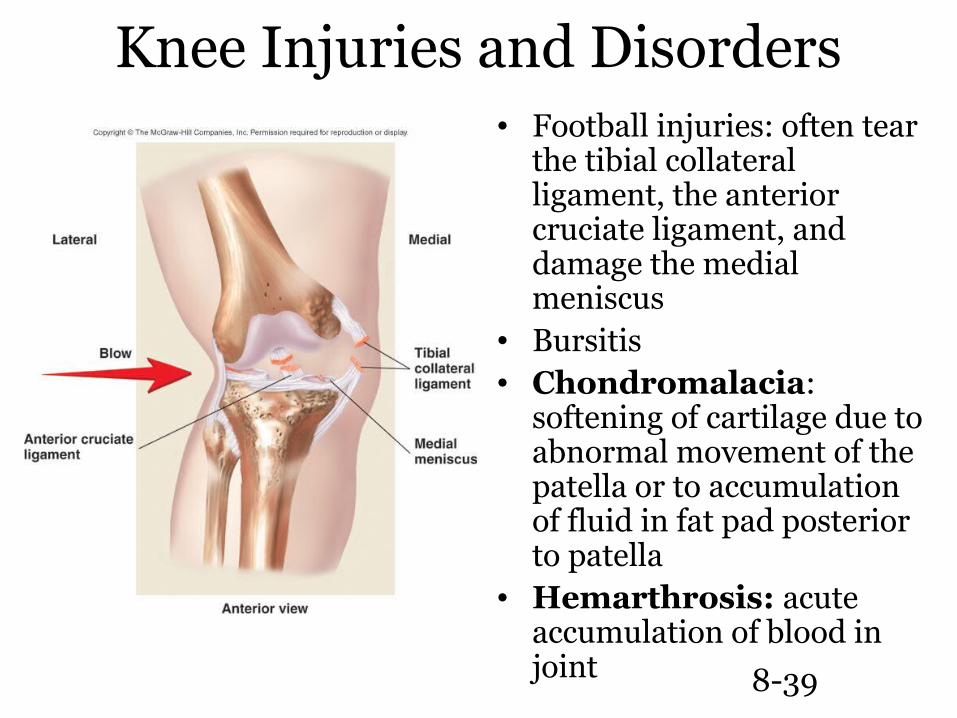
Knee Injuries and Disorders• Football injuries: often tear
the tibial collateral ligament, the anterior cruciate ligament, and damage the medial meniscus
• Bursitis• Chondromalacia:
softening of cartilage due to abnormal movement of the patella or to accumulation of fluid in fat pad posterior to patella
• Hemarthrosis: acute accumulation of blood in joint
8-40
Effects of Aging on Joints
• Tissue repair slows; rate of new blood vessel development decreases
• Articular cartilages wear down and matrix becomes more rigid
• Production of synovial fluid declines• Ligaments and tendons become shorter and
less flexible: decrease in range of motion (ROM)
• Muscles around joints weaken• A decrease in activity causes less flexibility
and decreased ROM
8-41
Sprains
• The ligaments reinforcing a joint are stretched or torn
• Partially torn ligaments slowly repair themselves
• Completely torn ligaments require prompt surgical repair
8-42
Cartilage Injuries
• The snap and pop of overstressed cartilage
• Common aerobics injury• Repaired with arthroscopic surgery
8-43
Dislocations
• Occur when bones are forced out of alignment
• Usually accompanied by sprains, inflammation, and joint immobilization
• Caused by serious falls and are common sports injuries
• Subluxation – partial dislocation of a joint
8-44
Inflammatory and Degenerative Conditions
• Bursitis– An inflammation of a bursa, usually caused by a
blow or friction– Symptoms are pain and swelling– Treated with anti-inflammatory drugs; excessive
fluid may be aspirated
• Tendonitis– Inflammation of tendon sheaths typically caused
by overuse– Symptoms and treatment are similar to bursitis
8-45
Arthritis
• More than 100 different types of inflammatory or degenerative diseases that damage the joints
• Most widespread crippling disease in the U.S.• Symptoms – pain, stiffness, and swelling of a
joint• Acute forms are caused by bacteria and are
treated with antibiotics• Chronic forms include osteoarthritis,
rheumatoid arthritis, and gouty arthritis
8-46
Osteoarthritis (OA)
• Most common chronic arthritis; often called “wear-and-tear” arthritis
• Affects women more than men• 85% of all Americans develop OA• More prevalent in the aged, and is
probably related to the normal aging process
8-47
Osteoarthritis: Course
• OA reflects the years of abrasion and compression causing increased production of metalloproteinase enzymes that break down cartilage
• As one ages, cartilage is destroyed more quickly than it is replaced
• The exposed bone ends thicken, enlarge, form bone spurs, and restrict movement
• Joints most affected are the cervical and lumbar spine, fingers, knuckles, knees, and hips
8-48
Rheumatoid Arthritis (RA)
• Chronic, inflammatory, autoimmune disease of unknown cause, with an insidious onset
• Usually arises between the ages of 40 to 50, but may occur at any age
• Signs and symptoms include joint tenderness, anemia, osteoporosis, muscle atrophy, and cardiovascular problems– The course of RA is marked with exacerbations
and remissions
8-49
Rheumatoid Arthritis: Course
• RA begins with synovitis of the affected joint• Inflammatory chemicals are inappropriately released• Inflammatory blood cells migrate to the joint, causing
swelling• Inflamed synovial membrane thickens into a pannus• Pannus erodes cartilage, scar tissue forms,
articulating bone ends connect• The end result, ankylosis, produces bent, deformed
fingers

8-50
Rheumatoid Arthritis
8-51
Rheumatoid Arthritis: Treatment
• Conservative therapy – aspirin, long-term use of antibiotics, and physical therapy
• Progressive treatment – anti-inflammatory drugs or immunosuppressants
8-52
Gouty Arthritis
• Deposition of uric acid crystals in joints and soft tissues, followed by an inflammation response
• Typically, gouty arthritis affects the joint at the base of the great toe
• In untreated gouty arthritis, the bone ends fuse and immobilize the joint
• Treatment – colchicine, nonsteroidal anti-inflammatory drugs, and glucocorticoids