Embed Size (px)
Citation preview

Get Homework Done Homeworkping.comHomework Help https://www.homeworkping.com/
Research Paper helphttps://www.homeworkping.com/
Online Tutoringhttps://www.homeworkping.com/
click here for freelancing tutoring sitesA CASE STUDY OF A 62 YEARS OLD, FEMALE
DIAGNOSED WITH BRONCHOGENIC CARCINOMA
This Study is Presented to theFaculty of San Lorenzo Ruiz School of Health Sciences
Mapúa Institute of TechnologyMakati City
In Partial Fulfillment of the Requirements onCurative and Rehabilitative Nursing Management 2
Part A (RLE)
Submitted to:
Prof. Ana Liza ManzanasProf. Mary Ann NeryProf. Leah Santillan
Prof. Delia Tan

Submitted by:
Adriano, Karen B.Alejandro, Valery Benedict O.
Cabrera, Christianne S.Cauntay, Immanuel Carlo L.
Galang, Jean Abegail B.Indita, Ericxandria Ivi D.U.
Misa, Samuel Adrian A.Racpan, Joana Lyn M.
Realco, Robert Daryl A.Reyes, John Michael
AN01
September 18, 2009
1. CLIENT PROFILE
I. General Information
a. Name: Client REb. Hospital: Lung Center of the Philippines
i. Ward: 3C Wardii. Bed: Room 3305
c. Date of admission: July 28, 2009d. Age: 62 years olde. Birth date: July 23, 1947f. Address: Kamuning, Quezon Cityg. Occupation: Retired MMDA Officerh. Educational Attainment: College Graduatei. Spouse: n/a (Single)j. Names of children, Ages, and educational attainment
n/a
II.Chief Complaint
Upon admission, Patient complains of occasional Difficulty of Breathing.
III.Brief History of Present Hospitalization

Five (5) months prior to admission, patient had non-productive cough and was negative for fever. Patient consultation was done and revealed to have pulmonary mass (L) in CT-Scan. However, result was negative for the presence of malignant cells.
Four (4) months prior to admission, patient still suffering for non-productive cough and now associated with difficulty in breathing. Patient was admitted and diagnosed with Pleural Effusion (L). Thoracentesis was done and accumulated 355 mL of fluid. Days passed and she was discharged from the institution.
Five (5) days prior to admission, patient was positive for anorexia, experiences persistent nausea and vomiting, has intermittent non-productive cough and occasional difficulty of breathing. Persistence of symptoms accompanied by general body weakness led to consultation, hence admission.
IV. Medical Diagnosis
Bronchogenic Carcinoma, Left Pleural Effusion with Bronchial Asthma.
2. NURSING HISTORY
Last August 11, 2009, client RE was interviewed for her nursing history. This was based on Gordon’s Functional Health Pattern which comprises of 12 different categories used to provide more comprehensive nursing assessment for the client.
Starting with Health Perception and Health Management pattern, before the hospitalization, client is working as an MMDA officer and her general health seems fine. Accordingly, she was a blue baby (cyanotic), when she was born, the reason behind was not noted by the client. Only now that she is old, she starts to have asthma. Her family has a history of Blood Cancer and illness in the Pancreas. Right now that she is in the hospital; she feels to have a big change and hope for her health. For the past 6 months, she has been curing for the same illness. They don’t have any allergies to food. Same as before, she eats nutritious foods to keep her body healthy. She neither engaged to cigarettes, alcohol drinks nor illegal drugs. For the past 9 months, she is very cooperative with Dr. Raymond, her physician. Before, she follows certain traditions like; a woman who has monthly period should not eat sour foods and should take a bath using warm water.
On Nutritional and Metabolic pattern, like before, she loves eating any foods except Shrimp because her appetite doesn’t like it. For her 24-hour recall food consumption, she had bread and milk for breakfast, she ate steamed ham sandwich for her lunch and a rice and viand for her dinner. Her diet is as tolerated. She takes supplements like Vitamin B

Complex and Calcium Nitrate and even herbal tea. Before, she drinks 6 glasses of water every day but currently, she only drinks 3 glasses of water every day, because lately, she don’t get thirst easily. She used to have a good appetite before, but now, she losses her appetite when she eats and experiences nausea. She does not have any eating discomforts before, but recently she dislikes eating foul smelling foods especially seafoods, which not her type of food. She does not have any diet restrictions and allergies to food as mentioned above. Before, she weighs 60 kgs (132 lbs.) and stands 5 feet (150 cms.)tall. Currently, she weighs 53 kgs (117 lbs) and still 5 feet tall. Her BMI is 22.8 kg/m 2, which makes her height and weight appropriate for his age.
For her Elimination pattern, before she defecates twice (2) a day, the stool is yellow brown in color, soft in consistency with no accompanying foul odor present and she does not experience any discomfort. During hospitalization, she defecates once (1) a day, stool is brown in color, soft to hard in consistency, with no foul odor present and she does not experience any discomfort. For her urinary elimination, before she was hospitalized, she urinates seven (7) times a day, approximately 250 milliliters per urination, with clear color, no foul odor and no associated discomforts. During hospitalization, she urinates four (4) times a day, still 250 milliliters per urination, yellowish in color and it smells like medicine specifically the Antibiotics prescribed to her. She does not experience any discomforts. Like before, she does not experience any excess perspiration and odor problems.
On her Activity and Exercise pattern, she used to work and walk along the road as MMDA officer every day, but now; she can only walk in her room, watch television and read books. Before, she does not have sufficient energy in completing desired daily activities, she experiences shortness of breath, and likewise in the hospital her energy is not yet sufficient because she feels weak very easy. Since then, she does not have any exercise pattern. Like what she used to do before, she watches television and takes nap during spare time.
With regards on her Sleep-Rest pattern, before, she sleeps late at night (12:00 a.m.) because she still watches television and wakes up 4:30 a.m. for her work on the next day. She only sleeps 4 and a half hours with nightmares like “Bangungot”, being drowned and in a fight. She takes quick naps during the day but it depends on her scheduled time of duty that is why she doesn’t get enough rest. Right now, she sleeps 10 in the evening and wakes up 6 in the morning. That makes her sleeping time 8 hours with no nightmares. She takes naps during day and she does have enough rest in the hospital.
On Cognitive-Perceptual pattern, before she was hospitalized, she does not experience any change in memory. The easiest way for her to learn things is through reading and watching television. She does not have any hearing difficulty. She do experience difficulty in reading small letters in books other than that she does not have any visual disturbances. Her last eye checked up examination was done before at her work. During hospitalization, she do experience change in memory and she believes it is due to the anesthesia effect, she had on her previous operations. It is easy for her to learn still through reading books and newspaper and watching television. She still doesn’t have

any hearing difficulty. She still experience difficulty in reading small letters in books other than that she still does not have any visual disturbances.
For Self –Perception and Self-Concept pattern, before the hospitalization, client describes herself, healthy with accurately balanced weight but now that she is hospitalized she stated that her weight decreased and she looks much thinner than before. There has been so much change in her body including her weight and strength. Before, she used to work every day but now, all she can do is to lie in the bed and keep her body healthy. Before, she gets annoyed easily when she relaxes and her niece/nephews will jump into the bed and disturb her. Right now, she feels annoyed when she smells foul smelling odor foods like left over foods on her room, but to her condition, she feels saddened about it.
On Role-Relationship pattern, she lives with her parents’ house with her brother and niece/nephews. They have an extended family structure. According to her before hospitalization, she has no difficulty in handling problems, their family usually handle their problems by talking about it. For her social life, she has few friends and she doesn't belong to any social groups. During her hospitalization, she is trying to accept and deal with her problem especially her sickness. Her family deals the problem by just accepting the fact about her illness. She has close friends who visits her in the hospital and she does not belong to any social groups.
For Home and Environment pattern, client describes their home as a small house with 1 floor and 2 rooms both made in cement and wood. The toilet can be seen near their rooms. Their garbage trash is near their house. She describes her neighborhood as a clean city and free from any harm, easily accessible to the hospital and church but far from malls, any markets, factories. She describe her neighbors as all rich but still manage to chat with each other at their free time.
On Sexuality and Reproductive pattern, her menstruation started when she was 12 years old and her last menstrual period was in her early 50's. Before her menopausal period, she menstruates regularly, for about 3 days with an amount of 150 milliliter per month consuming 2-3 pads per day and she does experience dysmenorrhea. She doesn’t have any menstrual problems and her Obstetric score is GTPAL 0(0000).
For Coping-Stress Tolerance pattern, the illness she had was the big change in her life. She lost her dreams of travelling to places after she learned about her disease. Before her hospitalization and during hospitalization, she manages her stress by drinking water and taking enough rest. She handles her problems by praying to God and all conflicts happened to her life went successful.
Lastly, on Value-Belief pattern, the most important thing in her life is her parents. She is a Catholic and what she believes is so important to her. Before hospitalization, she regularly attends mass every Sunday but now that she is in the hospital, she sends offertory prayers for her fast recovery in every mass. These things do really help for her condition because she strongly believes in it.

3. PHYSICAL EXAMINATION
Client RE was given a head-to-toe physical assessment last August 11, 2009. The assessment provided baseline data that were indicative of the client’s functional abilities. The data obtained will help establish appropriate nursing diagnoses and plan of care for the client.
Starting from her baseline data, we recorded her height at 5 feet (150 cm), her weight at 53 kg (117 lbs), her temperature at 36°C taken from her left axillary, her pulse rate at 87 beats per minute from her left radial pulse with a regular rhythm, her respiratory rate at 27 breaths per minute, and her blood pressure at 110/80 on her left arm while she was seated.
For her general appearance, client RE was dressed in pajamas and well groomed during the interview. She has a medium frame body build. She did not have any apparent odor or physical deformity. She spoke comfortably while sitting up in bed. The client chose to sit up in bed rather than to transfer to a chair because she stated that she easily feels tired.
For her mental status, client RE was conscious and oriented to time, place and person. Moreover, she was cooperative and had a pleasant mood. She used simple words and communicated well.
Integumentary system was assessed. Her skin color was normal (brown, warm, dry and smooth). Her skin turgor was elastic and mobile. Her hair was evenly distributed and her nails were convex and ridged. Her capillary refill was 3 seconds. There was no edema present.
For the client’s head and face, her skull is proportionate to her body size (normocephalic), her scalp is clean and her face is symmetrical. Upon asking the client, to puff her cheeks, raise her eyebrows, frown, and smile, it was revealed that her facial movement was symmetrical.
Her eyes are straight and normal, eyebrows are thin, eyelids and eyelashes have effective closure. The eyelashes are thin with a length of 1 cm. She has a negative discoloration on her periorbital region. Her blink response is bilateral and positive. Her eyeballs were symmetrical. Her sclera was white and her pupils were equal with a size of 3 mm. Her bulbar conjunctiva are clear and her palpebral conjunctiva are pinkish. Both her left and right eye had a brisk reaction to light and accommodation. She has good peripheral vision and six ocular movements. Her visual acuity is abnormal for she was unable to recognize the words 12 to 14 inches away. Her lacrimal gland was non-tender upon palpation. Her lacrimal apparatus was moist.

Her ears have normal (brown) racial tone, normoset, symmetric and elastic. The pinna recoils when folded, has no signs of lesions and no signs of inflammation. The external canal has some cerumen present. Her hearing acuity is normal for she responds to normal voice. Her ears are symmetrical for gross hearing and whisper test. There are no signs of AD, AS or AU difficulty.
Her nose, externally, has a normal (brown) racial tone. Her nasolabial fold is symmetrical. The septum is in midline. Mucosa of the nose is pale. The client still has a nasal cannula with a flow rate of 7-10 LPM. The nasal cavity is dry and the sinuses are non - tender. Both right and left nostrils are patent and able to distinguish two scents.
For her mouth, client’s lips are pale and symmetrical, the mucosa is pink; the tongue is in midline, rough and pink. The client has dentures because her teeth are incomplete. Her gums are pale. The speech is intact.
For her pharynx, her uvula is in midline position. Tonsils are not inflamed. Posterior pharynx is not inflamed. Hard and soft palates are pinkish and non-tender. Her gag reflex was present.
For her neck, neck muscle is equal in size, muscle strength is 5/5, which is strong against resistance, and lymph nodes on the neck area are not palpable. The trachea is midline. Thyroid gland is non-palpable.
For the client’s breast and axillae, her breasts are asymmetrical; the left breast is slightly bigger than the right, round in shape. Skin is normal in color, with no redness, edema or prominent veins. Breast is non-tender. Nipple and areola are not inverted, no edema, retraction, deviation and discharges. Lymph nodes are not palpable.
For her chest and lungs, breathing pattern is tachypnic, shallow and use of accessory muscles during inspiration was present. She has 27 breathes per minute (since normal breathing pattern is 16-20 breathes per minute). She has a nasal cannula attached to her nostrils with flow rate of 7-10 LPM. AP lateral ratio is 1:2. Inspiration to expiration is 1:3. There were no bulges or tenderness upon palpation. Tactile fremitus was revealed to be asymmetrical; the tactile fremitus of the right lung is stronger than the tactile fremitus of the left lung which is decreased. Further assessment was done on the left lung field in addition to the tactile fremitus examination, bronchophony revealed clear sound; egophony revealed “aaa” sound; and whispered pectoriloquy revealed clear sounds in which all findings were abnormal. Upon percussion, her right lung had a resonant sound while percussion of the left lung revealed a dull and flat sound. Normal breath sounds (bronchial, bronchovesicular and vesicular) were present on the right lung field but were consolidated on the left lung field (crackles and wheezes breath sounds), the bronchial sound could be heard in the peripheral areas of the lung. Lung expansion is asymmetrical in both anterior and posterior areas with both lag.

For her heart, her precordial area is flat and normodynamic. The point of maximal impulse is best heard at the 5th intercostal space, midclavicular line. The heart sounds were distinct with 86 beats per minute.
For her abdomen, her skin is normal in racial tone. There were no lesions noted on her skin. Her umbilicus is sunken. Moreover, the configuration is flat in shape and has symmetrical movement. The abdomen is non – tender and the liver is palpable upon bimanual palpation. There is no fluid wave, the client is normotensive and the sound upon palpation is tympanitic. Bowel movements were normal with 11 bowel sounds per minute, discharge of fecal matter occurred earlier. Food intake was allowed. Bladder was empty & relaxed.
Client RE’s genital area was not assessed due to personal reasons; the choice of the client was respected by the nurses.
Lastly, for her back and extremities, her nine peripheral pulses were symmetrical, strong, and regular. Her joints were not inflamed and she was able to perform active range of motion exercises on both extremities but with slowed movement. Her upper extremities were mobile and normal tone however she had weakness with muscle strength of 3/5. There were no tenderness, no lesions found and no other deformities present. Client had a heplock attached to his left hand; site is intact and negative for signs of inflammation. Lymph nodes were not palpable in the upper extremities. For her lower extremities, it was also mobile with a normal tone however with muscle weakness grade of 3/5, lymph nodes were not palpable. There were neither lesions nor any other deformities found in the lower extremities. Her spine was the midline and was negative for the costovertebral angle punch and pain in dorsiflexion. Lesion from the clients’ thoracentesis was present on the posterior 6th intercostals space.
4. ANATOMY AND PHYSIOLOGY
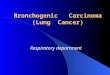
Anatomy of the Lungs
The trachea (windpipe) branches into two smaller airways: the left and right bronchi, which lead to the two lungs. The left lung is longer, narrower, and has a smaller volume than the right lung it shares space in the left side of the chest with the heart. The right lung is divided into three lobes and each lobe is supplied by one of the secondary bronchi. It has an indentation, called the cardiac notch, on its medial surface for the apex of the heart. The left lung has two lobes.
The bronchi themselves divide many times before branching into smaller airways called bronchioles. These are the narrowest airways – as small as one half of a millimeter across. The larger airways resemble an upside-down tree, which is why this part of the respiratory system is often called the bronchial tree. The airways are held open by

flexible, fibrous connective tissue called cartilage. Circular airway muscles can dilate or constrict the airways, thus changing the size of the airway.
At the end of each bronchiole are thousands of small air sacs called alveoli. Together, the millions of alveoli of the lungs form a surface of more than 100 square meters. Within the alveolar walls is a dense network of tiny blood vessels called capillaries. The extremely thin barrier between air and capillaries allows oxygen to move from the alveoli into the blood and allows carbon dioxide to move from the blood in the capillaries into the alveoli.
Each lung is enclosed by a double-layered serous membrane, called the pleura. The visceral pleura is firmly attached to the surface of the lung. At the hilum, the visceral pleura is continuous with the parietal pleura that lines the wall of the thorax. The small space between the visceral and parietal pleurae is the pleural cavity. It contains a thin film of serous fluid that is produced by the pleura. The fluid acts as a lubricant to reduce friction as the two layers slide against each other, and it helps to hold the two layers together as the lungs inflate and deflate.
The lungs are soft and spongy because they are mostly air spaces surrounded by the alveolar cells and elastic connective tissue. They are separated from each other by the mediastinum, which contains the heart. The only point of attachment for each lung is at the hilum, or root, on the medial side. This is where the bronchi, blood vessels, lymphatics, and nerves enter the lungs.
Figure 1. Anatomy of the Lungs

5. PATHOPHYSIOLOGY
Theoretical – Based PathophysiologyFigure 2. Lung Oxygenation
Smoking
Polymorphisms in genes coding for
interleukin-1
Primary Tumor Arises
Periphery of Lung
Invasion of Pulmonary Membranes and
Vasculature
Terminal Airway
Obstruction
Compression
Dyspnea
Pleural Effusion
Atelectasis
Precipitating Factors Predisposing Factors
Occupational Exposure
Asbestos
Radon
Mutations in the K-ras proto-
oncogene

Patient – Based Pathophysiology
Precipitating factor
Occupational Exposure (MMDA
Officer)
Exposure to Second-Hand
Smoke
Primary tumor arises in the periphery of the lungs
Hypermetabolic state from cell proliferation is induced by the tumor’s
growth needs
Weakness
Terminal airway obstruction
Dyspnea, occasionally
nonproductive cough
Invasion of pulmonary
membranes and vasculature.
Increased Permeability of the
pleural space
355 cc of serous fluid leaks into the pleural space
Hydrothorax
Restricted Lung Expansion.
Shallow Respirations
Imbalanced oxygen supply and demand
Pleural fluid accumulates
Secondary infection of Pneumonia
Weight loss


6. DRUG STUDIES
Drug Order
Drug Classification
and Mechanism of
Action
IndicationsContra-
indications Adverse EffectsDesired Actions
Nursing Responsibilities
Generic Name:Piperacillin + Tazobactam
Brand Name:Piptaz
Dosage:4.5 grams
Frequency:Q8
Route:TIV
Classification:Extended spectrum Penicillin, Beta-lactamase inhibitor
Mechanism of Action:Inhibits cell wall synthesis during bacterial multiplication.
Moderate to severe secondary infection of pneumonia.
Hypersensitivity to drug and other penicillins.
No adverse effect noted on client, however, the following should be monitored and reported:
Headache Insomnia Fever Agitation Dizziness Hypertension Tachycardia Chest pain Edema Rhinitis Diarrhea Nausea Constipation Vomiting Dyspepsia Stool changes Abdominal
pain
To free the client from infection.
Before giving drug, ask the patient about allergic reactions to penicillins.
Watch out for any super infections when large doses are given and if therapy is prolonged, especially in elderly and immunosupressed patients. Tell patient to alert a health care professionals about discomfort at the IV site.

Drug OrderDrug
Classification and
Mechanism of Action
Indications Contra-indications
Adverse Effects Desired Actions Nursing Responsibilities
Generic Name:Cephalexin
Brand Name:Keflex
Dosage:500 mg/cap
Frequency:TID
Route:PO
Classification:First generation Cephalosporins
Mechanism of Action:It inhibits cell wall synthesis, promoting osmotic instability, usually bactericidal
Respiratory tract infections
Hypersensitivity to cephalosporins.
No adverse effect noted on client, however, the following should be monitored and reported:
Headache Dizziness Fatigue Confusion Hallucinations Anorexia Diarrhea Nausea Vomiting Anemia Maculopapular
Rash
To treat the respiratory tract infections.
Use cautiously in patients hypersensitive to penicillin because of possible cross-sensitivity with other beta-lactam antibiotics.
Tell to take drug exactly as prescribed, even if she feels better.
Instruct to take drug with food to lessen GI discomfort.
Tell to notify physician if rash or any signs and symptoms of superinfections develop.

Drug OrderDrug
Classification and Mechanism
of Action
Indications Contra-indications
Adverse EffectsDesired Actions
Nursing Responsibilities and Precaution
Generic Name:Hyoscine N- Butylbromide
Brand Name:Buscopan Plus
Dosage:500 mg/1 tab
Frequency:TID
Route:PO
Classification:Antispasmodic
Mechanism of Actions:Inhibits muscarinic actions of acetylcholine on autonomic effectors innervated by postganglionic cholinergic neurons.
Paroxysmal pain in chest.
Hypersensitive to belladonna or barbiturates
Angle-closure glaucoma
Obstructive Uropathy
Obstructive disease of GIT
Myasthenia gravis Paralytic ileus Intestinal atony Unstable CV
status in acute hemorrhage
Tachycardia from cardiac insufficiency
No adverse effect noted on client, however, the following should be monitored and reported:
Disorientation Restlessness Irritability Drowsiness Headache Confusion Hallucination Delirium Impaired
memory Palpitations Tachycardia Flushing Blurred vision Difficulty
swallowing Constipation Dry mouth Nausea Vomiting
To relief paroxysmal or spastic pain.
Advise to take the drug after meals
Raise side rails as a precaution because some patients become temporarily excited or disoriented and some develop amnesia or become drowsy. Reorient patient, as needed.
Warn patient to avoid activities that requires alertness until CNS effects of drug are known.
Monitor I & O for urinary retention.

Drug OrderDrug
Classification and Mechanism
of ActionIndications
Contra-indications Adverse Effects
Desired Actions
Nursing Responsibilities and Precaution
Generic Name:Esomeprazole
Brand Name:Nexium
Dosage:40mg/tab
Frequency:OD
Route:PO
Classification:Proton pump inhibitor
Mechanism of Actions:Suppress gastric secretion by inhibiting Hydrogen Potassium ATPase enzyme system in the gastric parietal cell characterized as a gastric acid pump inhibitor since it blocks the final step of acid production.
Prevention of duodenal and gastric ulcers
Hypersensitive to drug long term administration of bicarbonate with calcium or milk will cause milk alkali syndrome
No adverse effect noted on client, however, the following should be monitored and reported:
Weight loss Recurrent
vomiting Dysphagia Angina Tachycardia Bradycardia Headache Dizziness Rash Diarrhea Abdominal
pain Nausea Acid
regurgitation
To prevent gastric upset since client is taking antibiotics which may aggravate gastric discomforts.
Assess GI system. Bowel sound 8 hours, pain abdomen & smelling, appetite loss.
Should be taken before breakfast.
Patient may experience anorexia, small frequent meals may help to maintain adequate nutrition.
Report severe headache diarrhea,changes in respiratory status.

Drug Order Drug Classification and Mechanism of
Action
Indications Contra-indications
Adverse Effects Desired Actions
Nursing Responsibilities
Generic Name:Tramadol + Paracetamol
Brand Name:Dolcet
Dosage:325 mg/1 cap
Frequency:Q6
Route:PO
Classification:Non Opoid Analgesic
Mechanism of Actions:It inhibits the reuptake of norepinephrine and serotonin.
Paracetamol has analgesic activity.
Used together, tramadol and paracetamol has faster onset of action compared to tramadol alone and longer duration of action compared to paracetamol alone
Moderate to severe pain
Hypersensitivity to drug or other opiods
Acute Intoxication
Alcohol hypnotics
Centrally acting analgesics, opiods
Psychotropic drugs.
Patients with of anaphylactic reaction to codeine and other opiods maybe at increase risk
No adverse effect noted on client, however, the following should be monitored and reported:
Dizziness Headache Vertigo Anxiety Confusion Malaise Nervousness Sleep
disorder Constipation Abdominal
pain Anorexia Diarrhea Dry mouth Flatulence Urine
retention Repiratory
depression
To relief moderate to severe pain.
The nurse should know that serious hypersensitivity reactions can occur, usually after the first dose.
Reassess patient’s level of pain at least 30 minutes after administration.
Monitor respiratory status. Withhold dose and notify Prescriber if respirations decrease or rate is below 12 breaths/min.
Monitor bowel and bladder function. Anticipate need for laxatives.
For better analgesic effect, give drug before onset of intense pain.

Drug OrderDrug Classification and Mechanism of
Action
Indications Contra-indications
Adverse Effects Desired Actions
Nursing Responsibilities and
Precaution
Generic Name:Levodropropizine
Brand Name:Levopront
Dosage:10 cc/syrup
Frequency:TID
Route:PO
Classification:Mucolytics
Mechanism of Action:Levodropropizine is a cough suppressant that exerts peripheral action in nonproductive cough
Non-productive cough
Contraindicated in patients with excessive mucus discharge and limited mucociliary function
Severe Liver Impairment
No adverse effect noted on client, however, the following should be monitored and reported:
Nausea Vomiting Heartburn Diarrhea Weakness Drowsiness Dizziness Headache Palpitations
To clear the airway. The drug should be
kept in below 30oC.
Tell the patient to take the drug between meals.
Teach client deep breathing exercises.
Maintain adequate hydration status.
Tell patient to report immediately to health care provider if allergic reactions develop such as nausea, vomiting, drowsiness, weakness.

7. Diagnostic Studies
Name of Procedure
Date Done
Indication for the Test or Procedure
Normal Values, Results or Findings
Actual Results or Findings
Interpretation and Significance of the Results
or findings
Pleural Fluid analysis(Cytology Report)
08/03/09 This is often done when a mesothelioma or metastatic cancer is suspected. The presence of certain abnormal cells, such as tumor cells or immature blood cells, can indicate what type of cancer is involved.
Normal structure of cells. No detectable presence of abnormal cells like cells or immature blood cells.
Received approximatley 500ml of brownish yellow, turbid fluid with coagulum and labeled as “pleural Fluid”.smears and cell blocks were prepared.
Smears shows collections of varisized lymphocytes and scanty atypical cells dispersed on a pale proteinaceous background while the cell block yielded polygonal cells with round, hyperchromatic nuclei, occassionally prominent nucleoli, and ample cyto plasm, disposed in acini and fluorettes.
Cytomorphologic features consistent with adenocarcinoma.
Pleural biopsy(Surgical Pathology Report)
07/09 To check for the condition of the lungs, heart related lung problems, the size and outline of the heart and to check blood vessels
All organs in the chest are normal in appearance
The specimen consists of a tan white, soft, irregularly shaped tissue fragments measuring .5x.4x.1 cm and labeled as “left pleura.” block all.
Microscopic examination
Non Small Cell Carcinoma

shows fibromascular tissue and a fragment of fibrocollagneous tissue infiltrated by a malignant neoplasm composed of polygonal cells with hyperchromatic, round nuclei, and ample cytoplasm disposed in small nests and associated with inflammatory cells.
Tumor markers(Blood Specimen)
Carcinoemb-ryonic antigen (CEA)
CA 125(OM-MA)
02/12/09
A CEA test may be ordered when symptoms suggest the possibility of cancer. In patients who have been diagnosed with certain types of cancer, a CEA level is also measured before and after therapy, to evaluate the success of treatment.
CA-125 is primarily used to monitor therapy during treatment for ovarian cancer. CA-125 is also used to detect whether cancer has come back after treatment is
<5.5ng/ml
36.0 U/ml
5.25ng/ml
32.2 U/ml
Tumor markers normal
CA 125 is normal

complete. Series of CA-125 tests that show rising or falling concentrations are often more useful than a single result. This test is sometimes used to test and monitor high-risk women who have a family history of ovarian cancer but who do not yet have the disease.
This test is not used to screen for ovarian cancer because it is non-specific. Levels in the blood can be elevated in other conditions such as normal menstruation, pregnancy, endometriosis, and pelvic inflammatory disease.
CA 19-9 is not sensitive or specific enough to be considered useful as a tool for cancer screening. Its main use is as a tumor marker:
* to help differentiate between cancer of the pancreas and bile ducts and other non-cancerous

CA 19-9(GI-MA)
conditions, such as pancreatitis; * to monitor a patient's response to pancreatic cancer treatment; and * to watch for pancreatic cancer recurrence.
CA 19-9 can only be used as a marker if the cancer is producing elevated amounts of it; if CA 19-9 is not initially elevated, then it usually cannot be used later as a marker.
AFP is used to detect tumors that mark cancers of the liver, testes, and ovaries. Patients with chronic liver diseases such as cirrhosis or chronic hepatitis B must be monitored at regular intervals because they have a lifetime risk of developing liver cancer. A doctor may order an AFP test, along with imaging studies, to try to detect liver cancer when it is in its earliest, and most treatable, stages. An AFP-L3% test may be ordered by some doctors to help further
≤27 U/ml 24.67 U/ml CA 19-9 is Normal

Alpha Feto-protein(AFP)
evaluate the risk of patients with chronic liver disease developing hepatocellular carcinoma in the near future.
If a patient has been diagnosed with hepatocellular carcinoma or another form of cancer, an AFP test may be ordered periodically to help monitor a patient’s response to therapy.
<7 IU/ml 2.59 IU/ml AFP is Normal
Gram’s Stain Report(pleural fluid specimen)
07/29/09 A Gram stain and culture of the material from an infected site are the most commonly performed microbiology tests used to identify the cause of an infection. Often, determining whether an infection is caused by an organism that is Gram positive or Gram negative will be sufficient to allow a doctor to prescribe treatment with an appropriate antibiotic while waiting for more specific tests to be completed. Absence or presence of
No microorganisms seen
Pus cells – FEW
Gram (+) Cocci in pairs
Gram (+) Cocci in chains
Gram (+) Cocci singly
Gram (+) Cocci in clusters
Gram (+) Cocci in tetracis
Gram (-) diplococci
Gram (-) coccobacilli
Gram (-) bacilli
Infection is present at the given specimen, mostly caused by Gram (+) and Gram (-) bacteria. That is why client is taking (1) Piperacillin + Tazobactam; and (2) Cephalexin.

white blood cells in the Gram stain can determine the adequacy of the specimen.
CBC
Hemoglobin
Hematocrit
Leukocytes
07/28/09 This indicates the oxgen-carrying protein found in the red blood cells
Measures the percentage of red blood cells in a given volume of whole blood.
Used to determine the presence of an infection It is also used to help monitor the body’s response to various treatments.
125-160 g/L
.38-.50%
4.5 -11 g/L
119 g/L
.35%
14.1 g/L
Low blood and low blood oxygenation of the body. Client’s state of decreased hemoglobin value was primarily supported by her general manifestations in the physical assessment section.
Possible anemia
Above normal value. An increased production of white blood cells to fight an infection

Lymphocyte
Eosinophils
Neutrophil
Basophil
Monocytes
Thrombocytes
Indictates a viral infection
Indicates a inflammatory response, parasitic infection or allergic reaction
Indicates an inflammatory response bacterial infection or allergic reaction
Indicates a parasitic infection or allergic reaction
Indicates a inflammatory response, parasitic infection or allergic reaction
May indicate bleeding or indicates clients who are
0.20-0.40
0.02 - 0.04
0.40-0.60.
0-0.001
0.02-0.06
150-400
0.20
0.02
0.75
0.01
0.02
442
Normal
Normal
Suggest bacterial infection, as indicated above (Gram Stain Report), presence of bacterial infection was monitored.
Normal
Normal
An unexpectedly high platelet count may have an

Hematology 2 (hemostasis)
Bleeding time
Clotting time
Prothrombin time
Patient
% of activity
07/28/09at risk for thrombosis
Bleeding time is a blood test that looks at how fast small blood vessels close to stop you from bleeding.
The time required for a sample of blood to coagulate in vitro under standard conditions is called "clotting time".
4-9 minutes
7-15 minutes
10-23.5 secs.
80-116%
4 minutes
9 minutes
12.5 secs.
91%
advanced or metastatic malignancy.
Normal
Normal clotting time
Normal prothrombin time
Normal % of activity

Activated partial prothrombin time
patient28-44 secs. 36.9 secs Normal

8. PRIORITIZATION OF NURSING DIAGNOSIS
Rank Problem Rationale
1
Ineffective Airway Clearance related to terminal airway obstruction
Maintaining a patent airway is vital to life. Loss of respiratory function would be life – threatening.
2
Ineffective Breathing Pattern related to terminal airway obstruction secondary to pleural effusion
According to the ABC rule of emergency care, problems with breathing should be checked after ensuring a patent airway since this is a life- threatening problem.
3 Activity Intolerance related to imbalance of oxygen supply and demand
Treatment of her high priority problem (Ineffective Airway Clearance) will relieve one of the etiologies of this problem.
4Anxiety related to difficulty in breathing and concerns over work
Treatment of her high priority problem (Ineffective Airway Clearance) will relieve one of the etiologies of this problem.
5
Sleep pattern disturbance related to difficulty in breathing
Treatment of the problems in breathing and airway clearance would solve this problem. Therefore, this problem would have to be attended after the nurse has improved the client’s airway clearance and oxygenation.

9. NURSING CARE PLANS
PRIORITY #1
CUES NURSING DIAGNOSIS
SCIENTIFIC EXPLANATION
ANDBACKGROUND
PLANNING INTERVENTIONS RATIONALE EVALUATION
Subjective:“Hirap ako huminga,” as verbalized by the client.
Objectives:
With nasal cannula with a flow rate of 7-10 LPM.
Dyspnea Occasional
non productive cough
Difficulty of breathing
Ct scan result:
Ineffective Airway
Clearance Related to Terminal Airway
Obstruction
Presence of tumor
Partial obstruction of bronchus
Ineffective airway clearance
Goal: After 2 weeks of nursing intervention the patient will maintain airway patency.
Objectives:After 8 hours of nursing intervention the patient will:
Verbalize understanding of cause and therapeutic management regimen
Position head midline with flexion appropriate for age/ condition.
Elevate head of the bed/ change in position every 2 hours and prn.
Assist in administering oxygen via nasal cannula.
Encourage deep breathing and coughing exercise
To open or maintain airway.
To take advantage of gravity decreasing pressure on the diaphragm .
To improve ventilation.
To maximize effort in breathing/
After intervention was done the patient:
The goal was met the patient demonstrated behaviors to improve airway patency
Verbalized understanding of cause and therapeutic management regimen
RR: 16-20 breathes/min.

presence of pulmonary mass
Shortness of breath
Shallow respirations
Decreased tactile fremitus on left lung field
RR: 27 breathes/ minute
Demonstrate behaviors to improve airway patency
Administer analgesics as ordered
Auscultate breath sounds
Monitor vital signs especially respiratory rate
Observe signs of respiratory distress
Provide opportunities for rest, limit activities to level of respiratory rate
To improve cough when pain is inhibiting effort/
To ascertain status and note progress/
To assess changes/ complications.
To assess complications.
To prevent fatigue.

PRIORITY #2
CUESNURSING
DIAGNOSIS
SCIENTIFIC EXPLANATIO
NAND
BACKGROUND
PLANNING INTERVENTIONS
RATIONALE
EVALUATION
Subjective:
“Nahihirapan akong huminga” as verbalized by the client
Objective:
(+) use of accessory muscles for breathing
With nasal cannula
(+) dyspnea
(+) shortness of breath
Ineffective Breathing Pattern related to terminal airway obstruction secondary to pleural effusion
Presence of tumor in left lung
Increased in level of pleural fluid
amylase
Increased capillary
permeability or vascular
disruption
Reduction of pressure in
pleural space; lung is unable to
Goal: After1 week of nursing intervention, the client’s respiratory status, ventilation, and respiratory rate will be within normal ranges as manifested by improved respiratory status and ventilation and respitatory rate of 16 to 20 breaths per minute.
Objectives:After 3 days of Nursing Intervention, the
Monitor respiratory rate, depth, and ease of respiration
Note abdominal breathing, use of accessory muscles for breathing, nasal flaring, retractions, irritability, confusion, or lethargy
Observe color of tongue, oral mucosa and skin
To determine the pattern of respiration of the client
These symptoms signal increasing respiratory difficulty and increasing hypoxia
Cyanosis of the tongue and oral mucosa is central
After 1 week of nursing interventions, the client:
Respiratory status, ventilation, and respiratory rate are in normal ranges as manifested by improved respiratory status and ventilation and respiratory rate of 16 to 24 breaths per minute

anddifficulty of breathing
RR: 27 breathes/ minute
expand
Pleural effusion
Obstruction of terminal airway
obstruction
Ineffective breathing pattern
client will be able to: Demonstrate
pursed lip breathing
Report ability to breathe comfortably
Identify and avoid specific factors that exacerbate episodes of ineffective breathing pattern
Auscultate breath sounds noting decreased or absent breath sounds, crackles, or wheezes
Position the client in an upright or semi-fowlers position
Administer ordered oxygen via nasal cannula.
Encourage
cyanosis and generally represents an medical emergency
The abnormal lung sounds can indicate respiratory pathology associated with an altered breathing pattern
An upright position facilitates an lung expansion
Oxygen therapy helps decrease dyspnea
To help relax the client
Demonstrated pursed lip breathing
Reported ability to breathe comfortably
Identified and avoided specific factors that exacerbate episodes of ineffective breathing pattern

client to take deep breaths at prescribed intervals and do controlled coughing
Teach pursed lip and controlled breathing exercises
Teach the client to identify and avoid specific factors that exacerbate ineffective breathing patterns
Pursed lip breathing increases use of intercostals muscles, decreased respiratory rate and improve oxygen saturation
So the client will know the factors that might affect the breathing pattern

PRIORITY #3
Cues Nursing Diagnosis
Scientific Explanation
Planning Interventions Rationale Evaluation Parameters
Subjective: “Madali
akong mapagod kaya lagi lang akong nakahiga at nakaupo, kaya minsan la na ko kagana ganang maglakad” as verbalized by the client.
Objective: weakness
on upper and lower extremities (3/5 muscle strength)
Inability to
Activity IntoleranceRelated to imbalanced oxygen supply and demand
Presence of tumor in the
left lung
Invasion of pulmonary membranes
and vasculature
Restricted lung
expansion
Imbalanced oxygen supply and demand
Weakness, fatigue, dyspnea,
tachypnea
Goal:After 1 week of intervention, the client will demonstrate decrease in physiological signs of intolerance.
Objectives:After 8 hours of intervention, the client will:
a. maintains activity level within capabilities
b. verbalize and use energy-conservation techniques
c. participate to
Determine patient's perception of causes of fatigue or activity intolerance
Assess nutritional status
Establish guidelines and goals of activity with the patient and caregiver
Provide bedside commode as indicated
These may be temporary or permanent, physical or psychologicalAssessment guides treatment.
Adequate energy reserves are required for activity.
Motivation is enhanced if the patient participates in goal setting.
This reduces energy expenditure. NOTE: A
After the intervention, the client demonstrated decrease in physiological signs of intolerance and was able to conserve energy and client participated to treatment regimen.

begin or to perform activity
Dyspnea RR= 27
breaths per minute (tachypnea)
Shallow respirations
Lack of interest in activity
Activity intolerance
treatment regimen within level of situation.
Administer medications as indicated
Health teaching about ROM and strengthening exercisesand importance of it.
bedpan requires more energy than a commode.
To treat underlying condition.
To strengthen body, assess capabilities and also for client’s understanding of his treatment regimen.

10. DISCHARGE PLAN
M – edications
Medications taken at home should include and be centered on antibiotics, pain killers, mucolytics, bronchodilators, anti-emetics and especially dietary supplements such as:
Tramadol + Paracetamol - for Moderate to Severe Pain.325 mg/1 cap, Q6, PO
Levodropropizine - for cough suppressant.10 cc/syrup, TID, PO
C ephalexin - to treat infections500 mg/cap, TID, PO
Hyoscine N- Butylbromide for Spastic Pain500 mg/tab, TID, PO
Esomeprazole for treatment of possible gastric and duodenal ulcer since client takes antibiotics.
40 mg/tab, OD, PO
Exercise
Activity is as tolerated and actually according to physicians advised. While there are many reasons for being physically active during cancer treatment, client’s exercise program should be based on what is safe, effective, and enjoyable for the client. Exercises should take into account any exercise program that the client already follows, what she can do now, and any physical problems or limits she may have. She and her doctor should tailor an exercise program to meet her interests and needs. While some people can safely begin their own exercise program, many will have better results with the help of an exercise specialist, physical therapist, or exercise physiologist. Be sure to get an approval from client’s doctor first. The goal is to have an exercise program that will help client maintain endurance, muscular strength, flexibility, and level of functioning and most especially prevention of fatigue.
To make client’s exercise most effective, it is important to emphasize that she should work her heart. They should pay attention to her heart rate, breathing, and how tired muscles get. Start slowly at first, and over the next few weeks, increase the length of time of exercise. The best level of exercise for someone with cancer has not been established. However, the more exercise, the more ability to exercise can improve the ability to function effectively.
Start slowly with an exercise program. Even if client can only do an activity for a few minutes a day it will help her. How often and how long she will do a simple activity like walking can be slowly increased.

Try short periods of exercise with frequent rest breaks. For example, walk briskly for a few minutes, slow down, and walk briskly again, until she have done 30 minutes of brisk activity. She can divide the activity into three 10-minute sessions, if this is the way to prevent fatigue.
Try to include physical activity that uses large muscle groups. Strength, flexibility, and aerobic fitness are all important parts of an exercise program that works.
Always start with warm-up exercises for about 2 to 3 minutes. Examples of warm-up exercises are shoulder shrugs, lifting arms overhead, toe tapping, marching, and knee lifts. End session with stretching or flexibility exercises. Hold the stretch for about 15 to 30 seconds and relax. Remember to breathe when stretching to relax all the muscle groups.
Exercise moderately.
Treatment
Chemotherapy was planned for the client since she was recently admitted. Chemotherapy treatments may be given in the hospital, doctor’s office or clinic. They are usually given in cycles (such as monthly or weekly) so that the body can rest and repair between cycles. Treatment schedules vary for each patient. A doctor called a medical oncologist will decide what type of chemotherapy will the client receive and how often it should be given. For this reason it is very important to follow the treatment plan exactly and keep all appointments.
Aside from chemotherapy, the medications ordered should be emphasized because it is considered as a treatment as well.
Health Teaching
Health teaching should comprise of effective medications and treatment, diet, exercises, possible side effects monitoring and most especially, ways to prevent development of fatigue. Most cancer patients notice a loss of energy therefore increase susceptibility to develop fatigue.
Tips to reduce fatigue:
Tell the client to set up a daily routine that allows activity when she is feeling at her best.
Exercise regularly at light to moderate intensity (see suggestions above at exercise section)
Get fresh air. Unless it is advised by the physician, emphasize to client to eat a balanced diet
that includes protein (meat, milk, eggs, and legumes such as peas or beans) and drink about 8 to 10 glasses of water a day.
Keep symptoms such as pain, nausea, or depression controlled.

To save energy, keep things that are use often within easy reach. Enjoy hobbies and other activities that gives pleasure. Use relaxation and visualization techniques to reduce stress. Balance activity with rest that does not interfere with nighttime sleep. Most especially, ask for help when needed.
OPD Follow-Up
OPD follow-up is always after 1-2 weeks after discharge. If the client was discharged on September 5, 2009, the client should have a follow-up examination on September 12, 2009, 8AM at OPD department of lung center under Dr. Raymond.
The succeeding follow-up should be based on her chemotherapy schedules.
Diet
Clients with cancer were usually advised to have diet as tolerated, no food restrictions recommended. Good nutrition is important for all of us, but during treatment it is especially important. Maintaining a high intake of calories and protein can prevent body tissue from breaking down and can help rebuild healthy tissue after treatment. The treatments target fast-growing cells found in the lining of the mouth and the digestive system. Damage to these healthy, fast-growing cells may cause some side effects that lead to eating problems.
With good nutrition client can: Prevent or reverse weight loss Tolerate therapy with fewer side effects Keep body in the best physical condition to fight infection Give body a chance to repair normal tissues damaged by chemotherapy and
radiation Have more energy for a quicker recovery Feel better
Accentuate to client the following: Eating small, frequent meals throughout the day. Keeping snacks on hand and eating them whenever she feels like it. Remember to
take a snack with her if she is going to be away from home for an extended length of time.
If she don’t feel like eating solid foods or food seems to grow the more she chew it, try liquids such as juice, soup or milkshakes with a straw. Liquid and powdered nutritional supplements may also benefit her such as Instant Breakfast®, or a 360 calorie supplement (Ensure Plus®)
Eating a bedtime snack each day. Limiting most of her liquids to between meals so that she don’t get too full to eat
solid food.

Making mealtimes relaxing and pleasant. Stress at mealtime will limit the appetite.
Ideas to control weight loss: Choose foods high in calories. Eat largest meal when most hungry during the day. Add additional butter or margarine to soups, gravies or sauces. It
can also be added to meats, rice, pasta, potatoes or other vegetables.
Use whole milk or cream on cereals and in soups (instead of adding water to cream soups, add same amount of milk).
Cheese can be added to casseroles, potatoes, vegetables, eggs or sandwiches to add calories and protein.
Cream cheese and sour cream can be used as dips, spreads or as a topping to add calories.
Think of favorite foods and eat them often.
Source: http://www.nmhs.net/cancer_center
Signs and Symptoms (Side Effects)
Most side effects of chemotherapy can be predicted and can be prevented with medications. Side effects occur because chemotherapy slows the growth of normal cells as well as cancer cells. Examples of normal cells affected by chemotherapy include those found in hair, the lining of the mouth and digestive system and the bloodstream. Side effects that may occur as a result of the effect of chemotherapy on normal cells include:
Hair loss Mouth sores Nausea and/or vomiting Diarrhea Fever Infections Fatigue Bleeding problems Low blood counts Skin/nail problems Constipation
Eating a light meal before your chemotherapy is sometimes helpful. Client’s doctor will watch very closely for the occurrence of possible side effects. Emphasize to the client that she should let her doctor and nurse know if any of these side effects occur. Prescription medication, frequent exams and blood sampling will be used to prevent and/or treat side effects.






![Transbronchial Needle Aspiration Staging of Bronchogenic ...downloads.hindawi.com/journals/dte/1996/237680.pdfChest, 80,48-50. [18] Transbronchialneedle bronchogenic carcinoma, In:](https://img.pdfslide.net/doc/110x75/5fef28f6c0cad34ae7313439/transbronchial-needle-aspiration-staging-of-bronchogenic-chest-8048-50-18.jpg)