Embed Size (px)
Citation preview
6 Solitary Pulmonary Nodule
CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
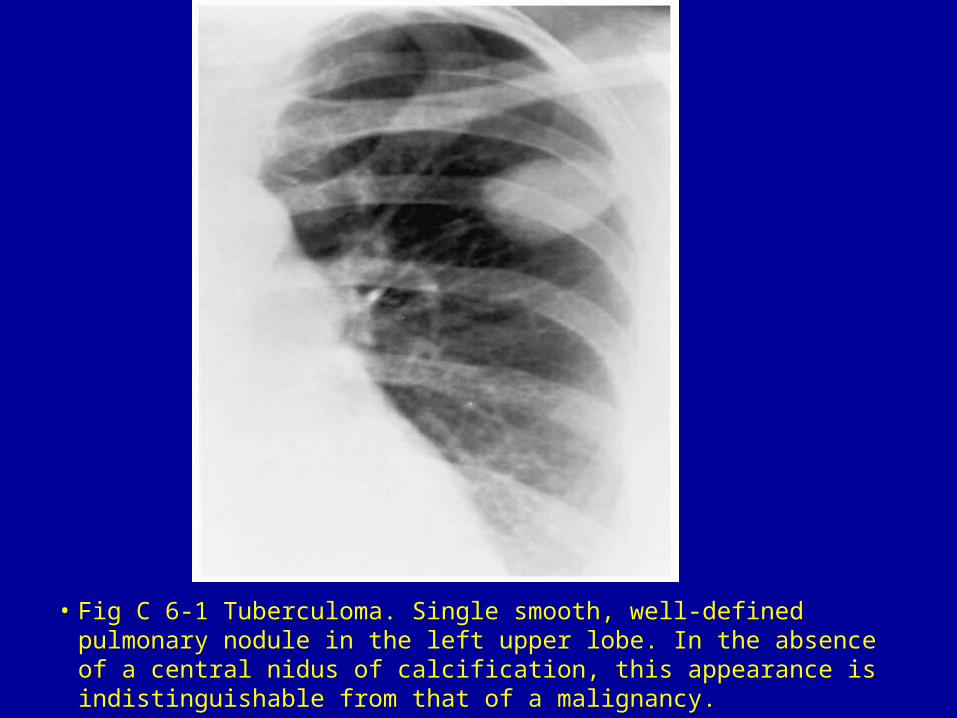
• Fig C 6-1 Tuberculoma. Single smooth, well-defined pulmonary nodule in the left upper lobe. In the absence of a central nidus of calcification, this appearance is indistinguishable from that of a malignancy.
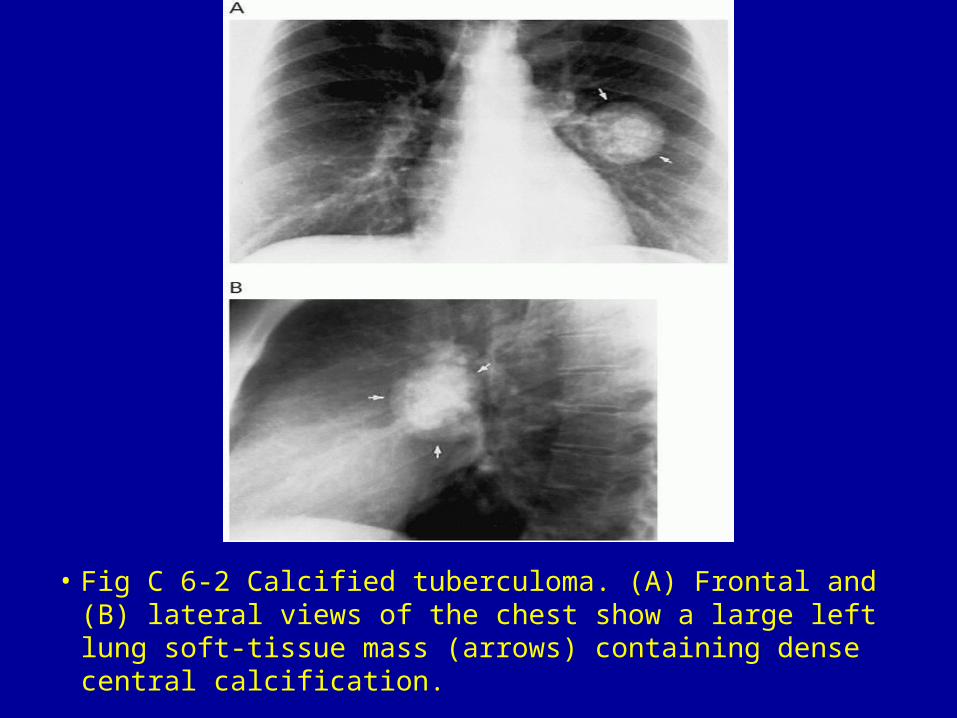
• Fig C 6-2 Calcified tuberculoma. (A) Frontal and (B) lateral views of the chest show a large left lung soft-tissue mass (arrows) containing dense central calcification.
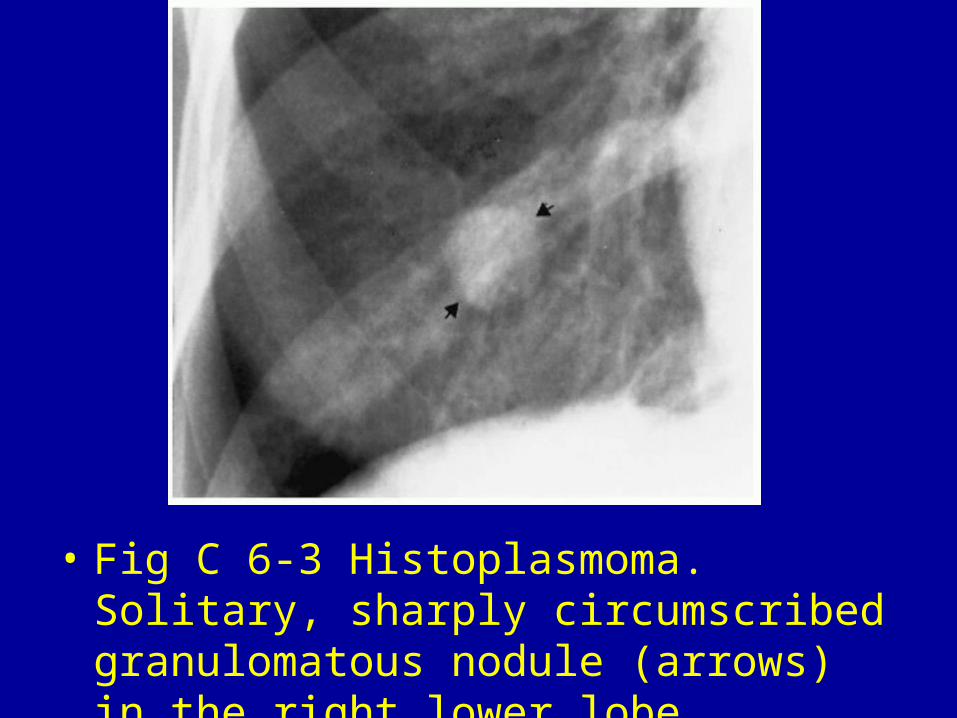
• Fig C 6-3 Histoplasmoma. Solitary, sharply circumscribed granulomatous nodule (arrows) in the right lower lobe.
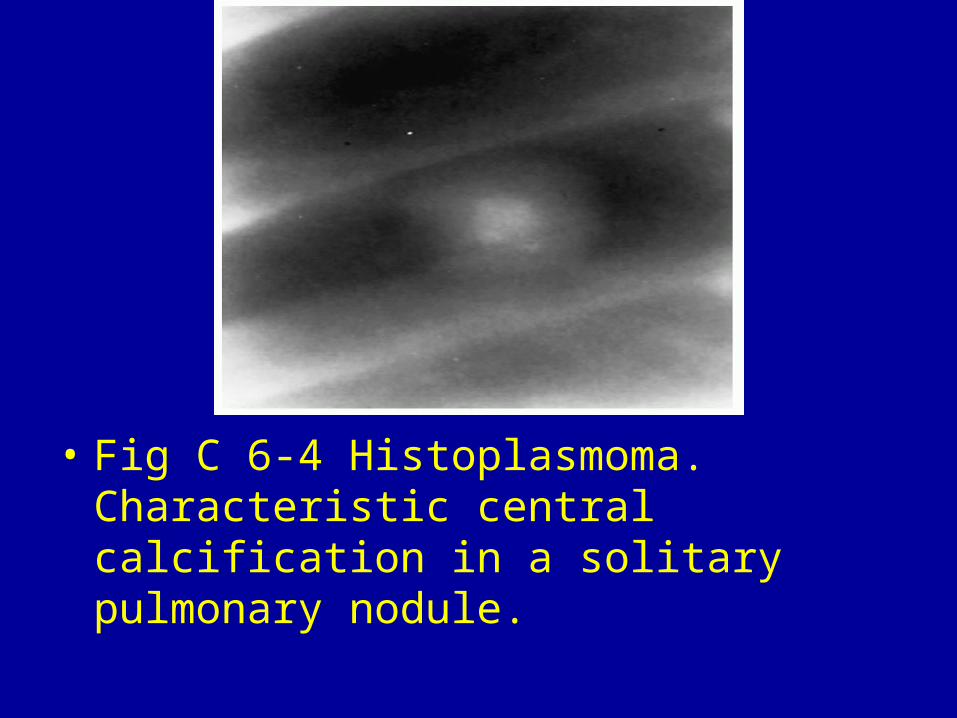
• Fig C 6-4 Histoplasmoma. Characteristic central calcification in a solitary pulmonary nodule.
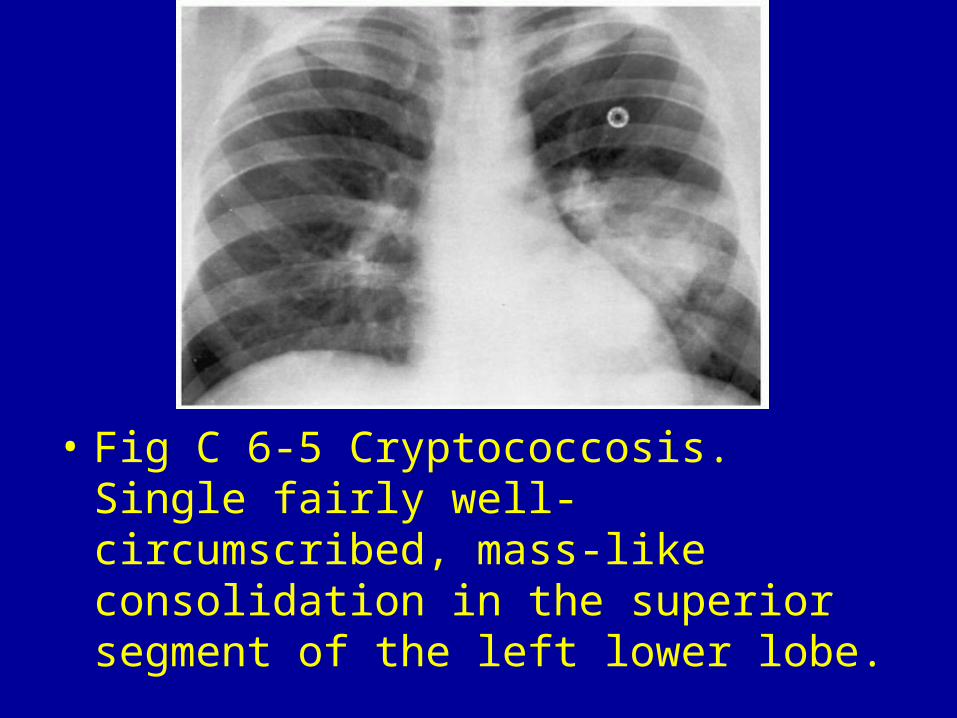
• Fig C 6-5 Cryptococcosis. Single fairly well-circumscribed, mass-like consolidation in the superior segment of the left lower lobe.
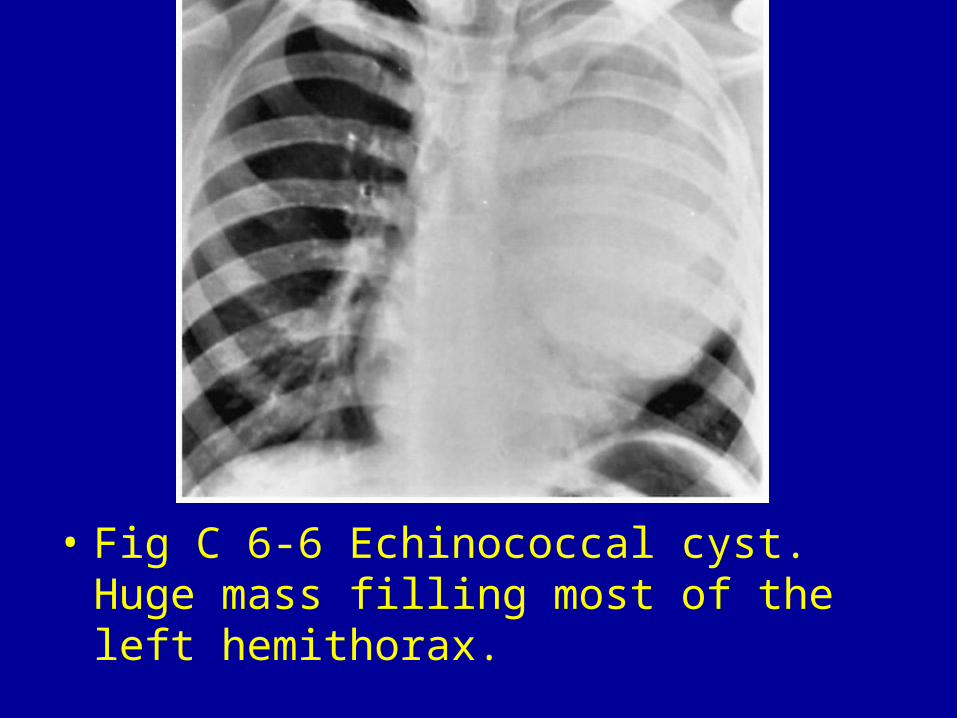
• Fig C 6-6 Echinococcal cyst. Huge mass filling most of the left hemithorax.
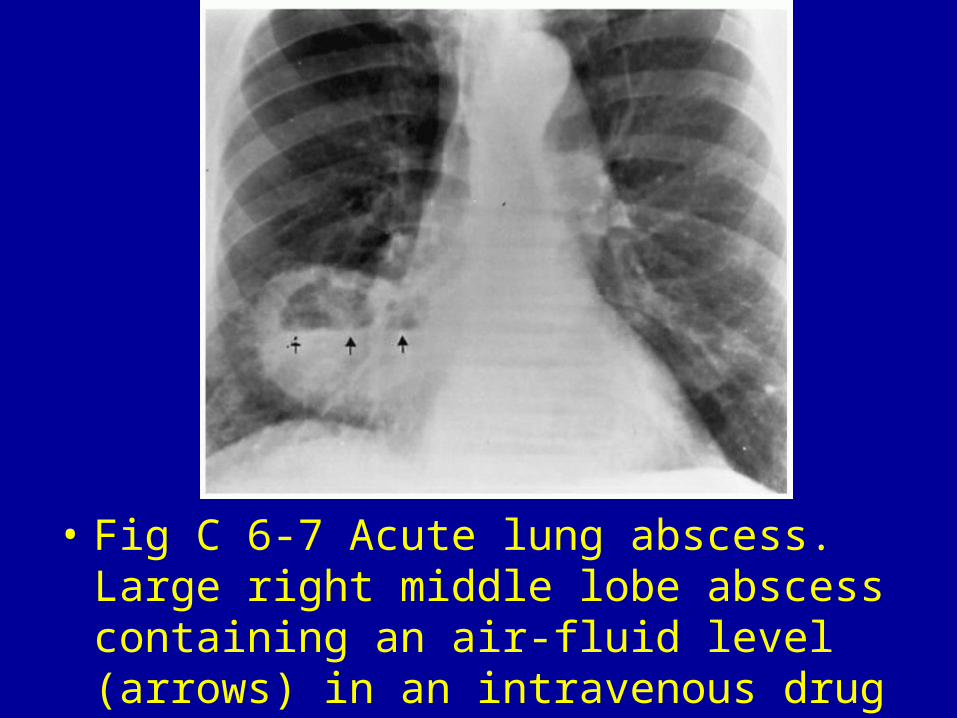
• Fig C 6-7 Acute lung abscess. Large right middle lobe abscess containing an air-fluid level (arrows) in an intravenous drug abuser.
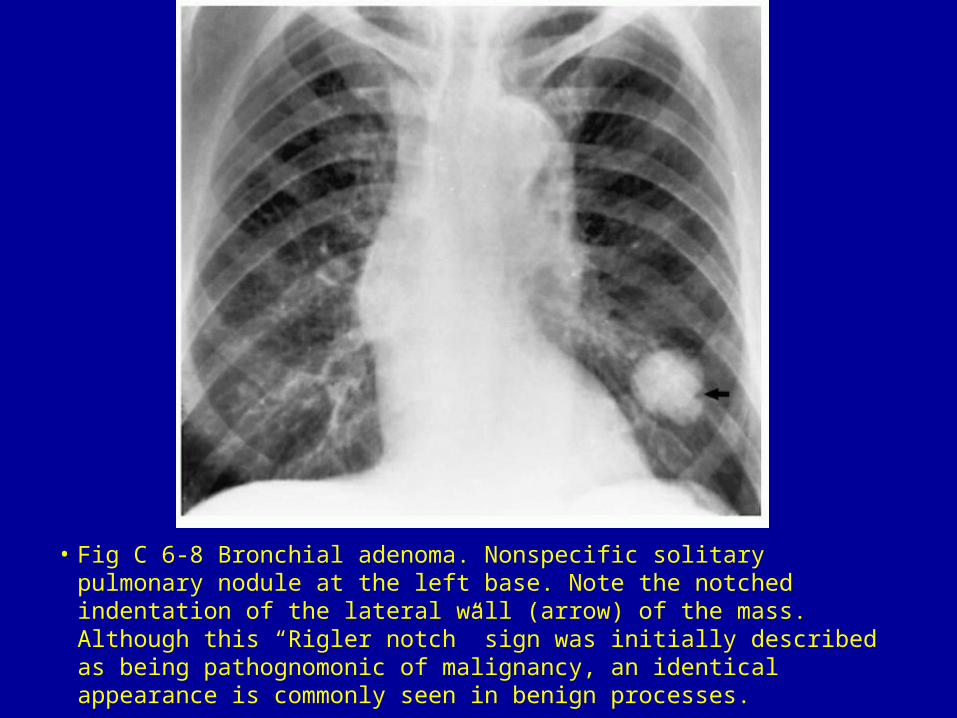
• Fig C 6-8 Bronchial adenoma. Nonspecific solitary pulmonary nodule at the left base. Note the notched indentation of the lateral wall (arrow) of the mass. Although this “Rigler notch” sign was initially described as being pathognomonic of malignancy, an identical appearance is commonly seen in benign processes.
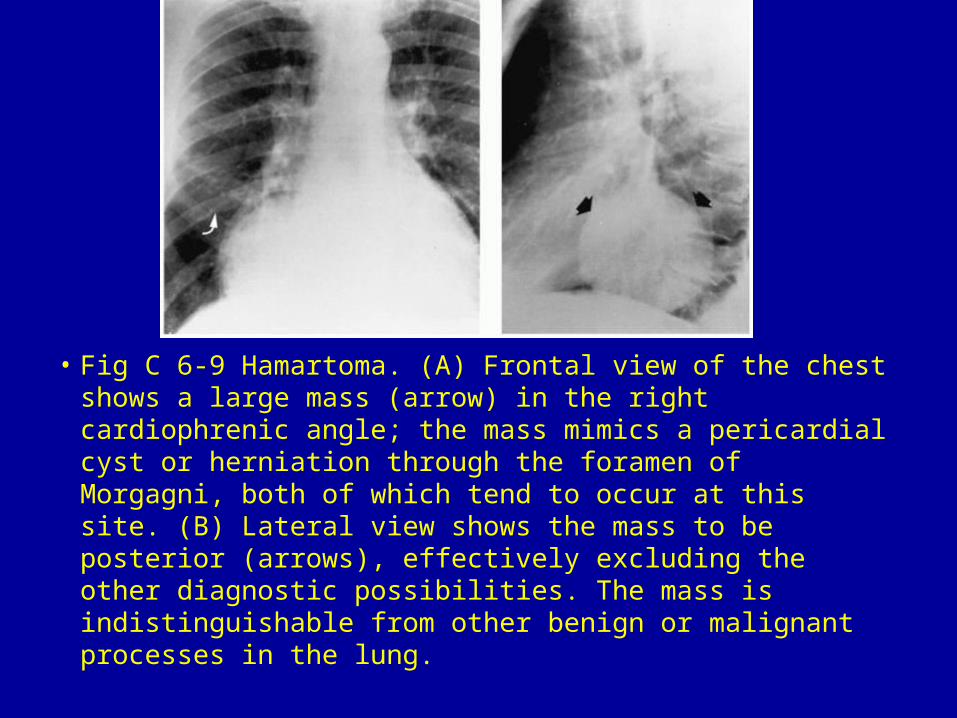
• Fig C 6-9 Hamartoma. (A) Frontal view of the chest shows a large mass (arrow) in the right cardiophrenic angle; the mass mimics a pericardial cyst or herniation through the foramen of Morgagni, both of which tend to occur at this site. (B) Lateral view shows the mass to be posterior (arrows), effectively excluding the other diagnostic possibilities. The mass is indistinguishable from other benign or malignant processes in the lung.
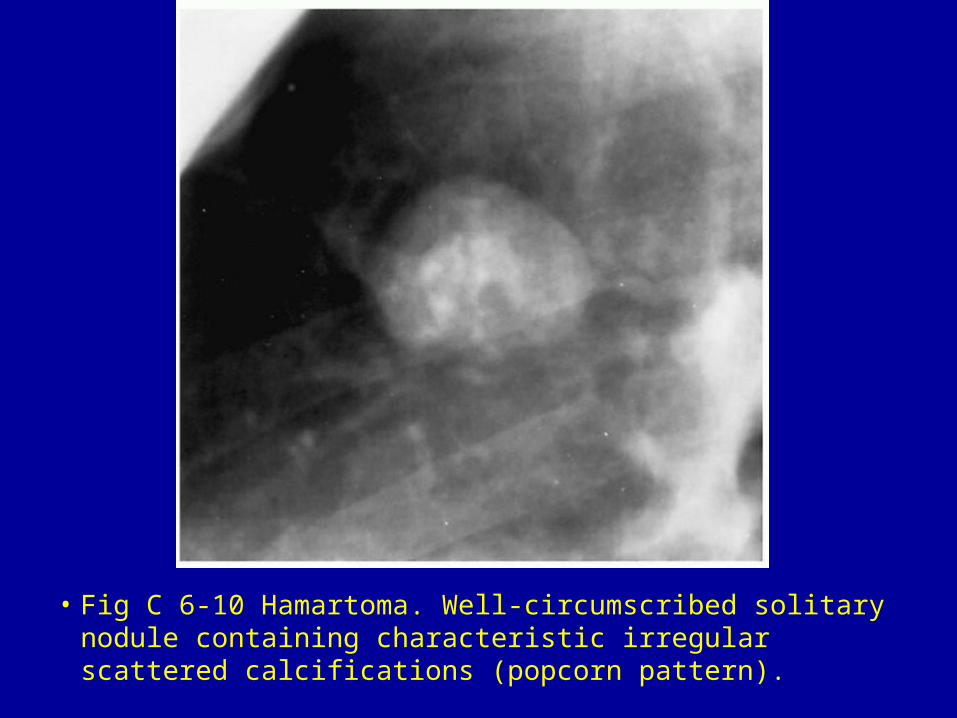
• Fig C 6-10 Hamartoma. Well-circumscribed solitary nodule containing characteristic irregular scattered calcifications (popcorn pattern).
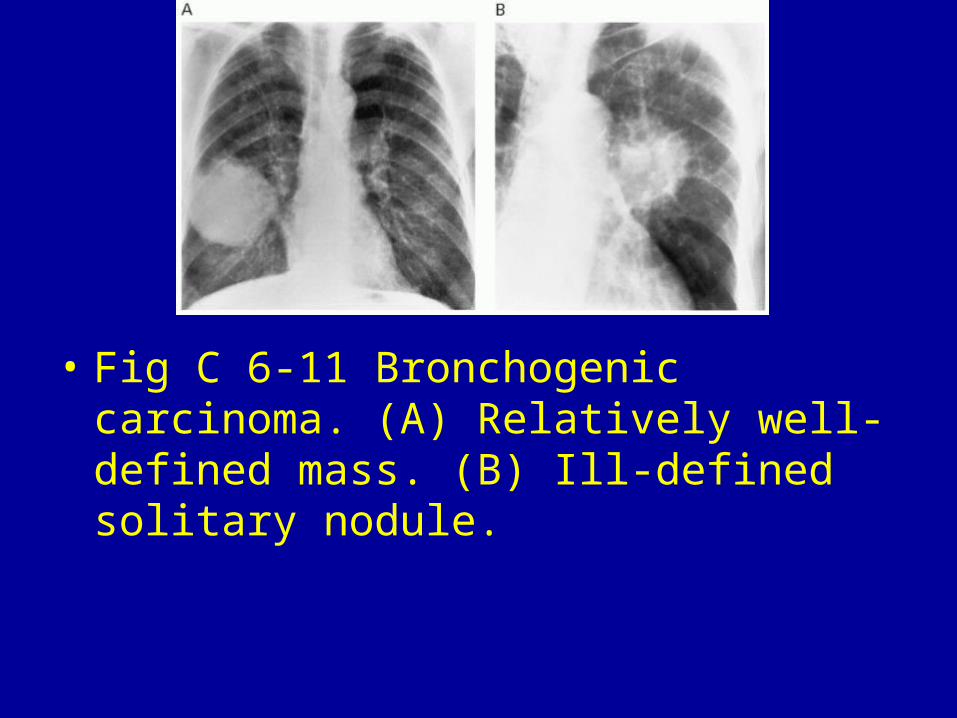
• Fig C 6-11 Bronchogenic carcinoma. (A) Relatively well-defined mass. (B) Ill-defined solitary nodule.
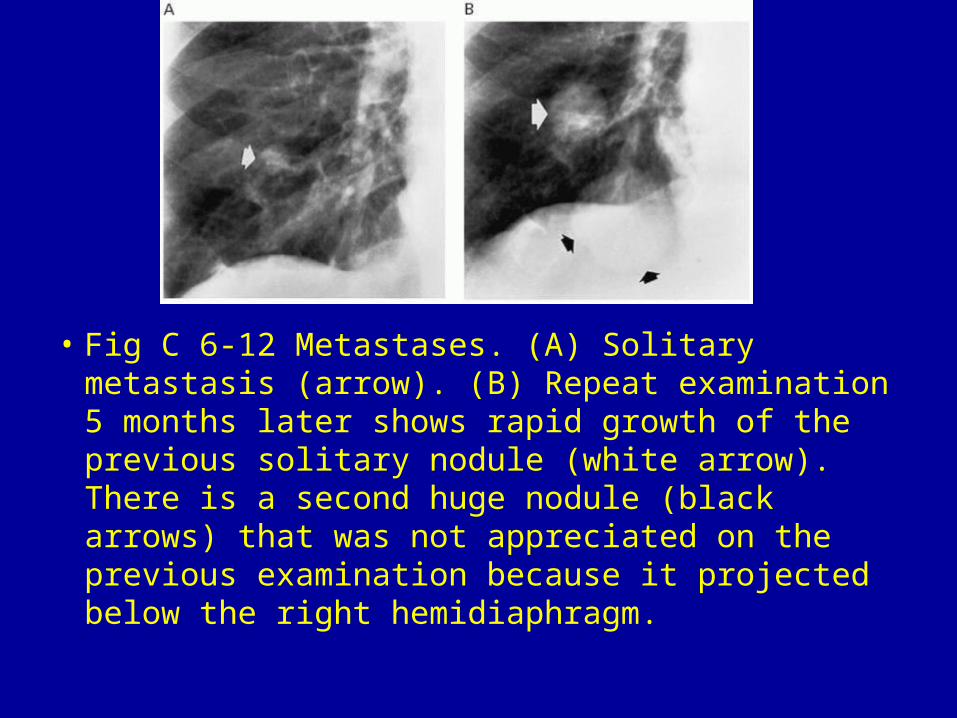
• Fig C 6-12 Metastases. (A) Solitary metastasis (arrow). (B) Repeat examination 5 months later shows rapid growth of the previous solitary nodule (white arrow). There is a second huge nodule (black arrows) that was not appreciated on the previous examination because it projected below the right hemidiaphragm.
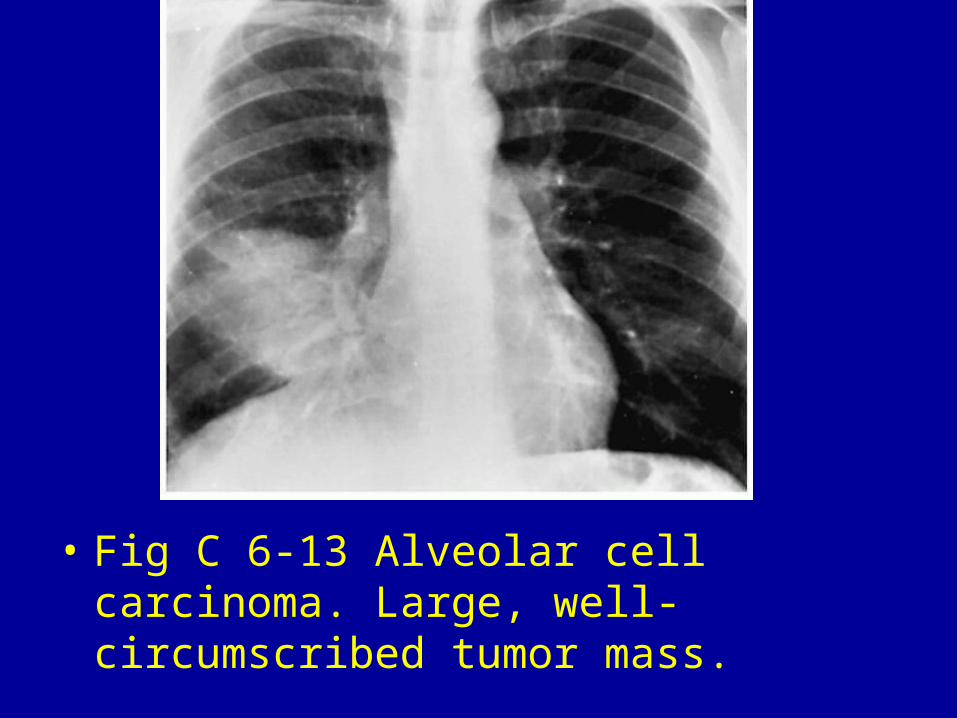
• Fig C 6-13 Alveolar cell carcinoma. Large, well-circumscribed tumor mass.
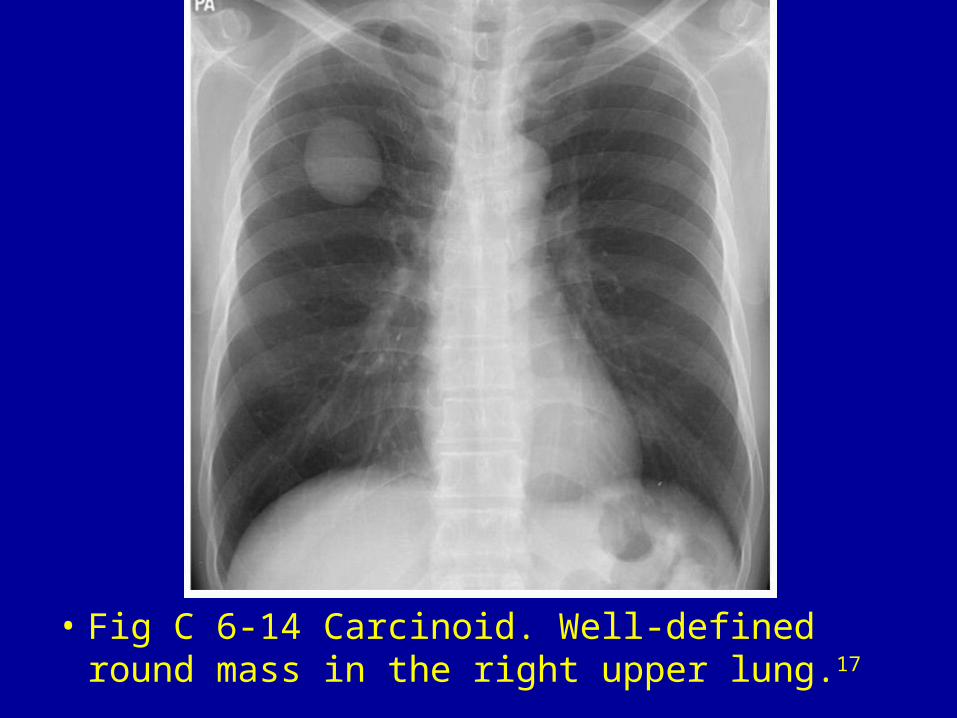
• Fig C 6-14 Carcinoid. Well-defined round mass in the right upper lung.17
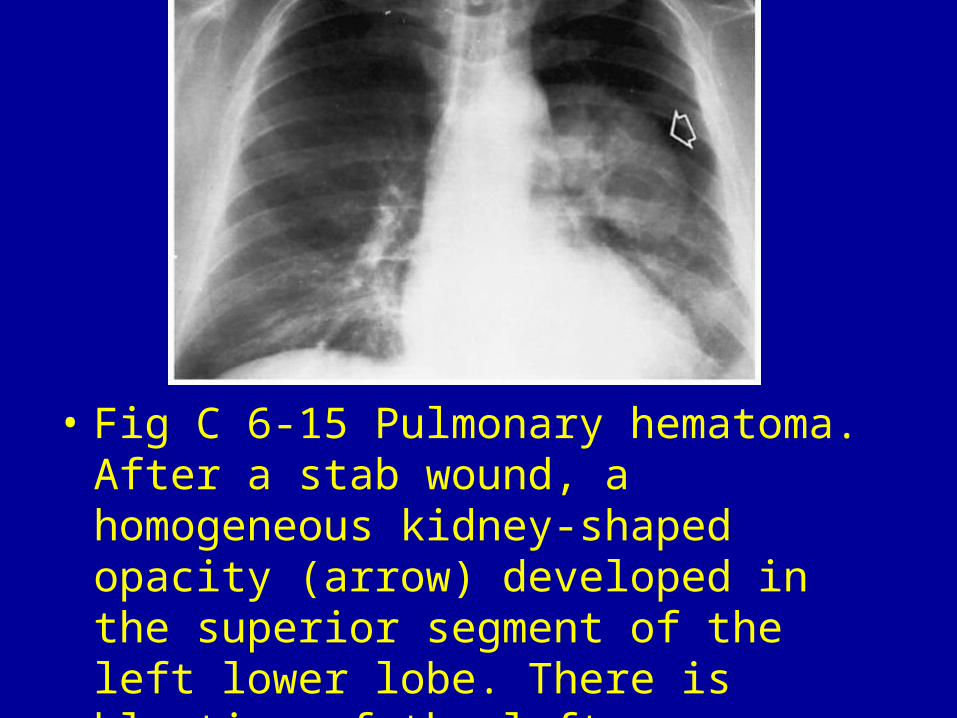
• Fig C 6-15 Pulmonary hematoma. After a stab wound, a homogeneous kidney-shaped opacity (arrow) developed in the superior segment of the left lower lobe. There is blunting of the left costophrenic angle.
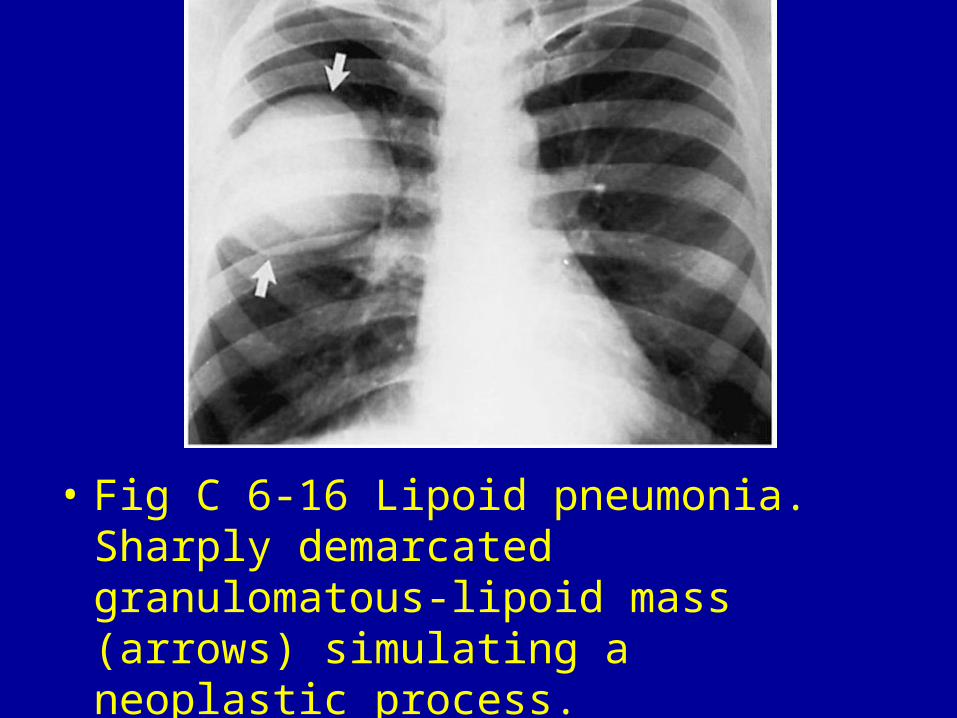
• Fig C 6-16 Lipoid pneumonia. Sharply demarcated granulomatous-lipoid mass (arrows) simulating a neoplastic process.
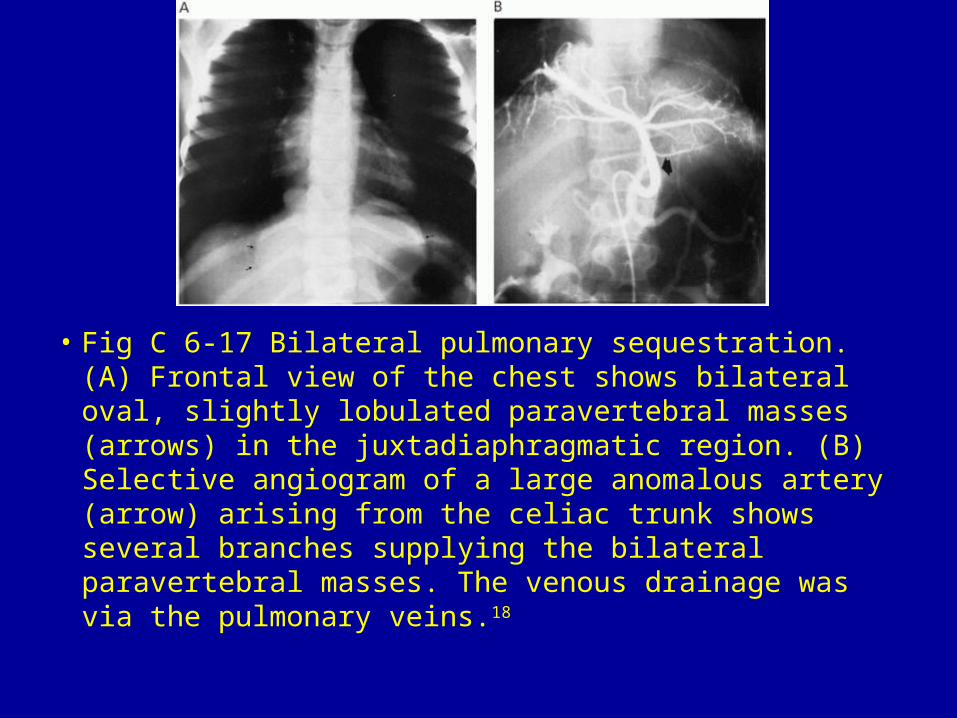
• Fig C 6-17 Bilateral pulmonary sequestration. (A) Frontal view of the chest shows bilateral oval, slightly lobulated paravertebral masses (arrows) in the juxtadiaphragmatic region. (B) Selective angiogram of a large anomalous artery (arrow) arising from the celiac trunk shows several branches supplying the bilateral paravertebral masses. The venous drainage was via the pulmonary veins.18
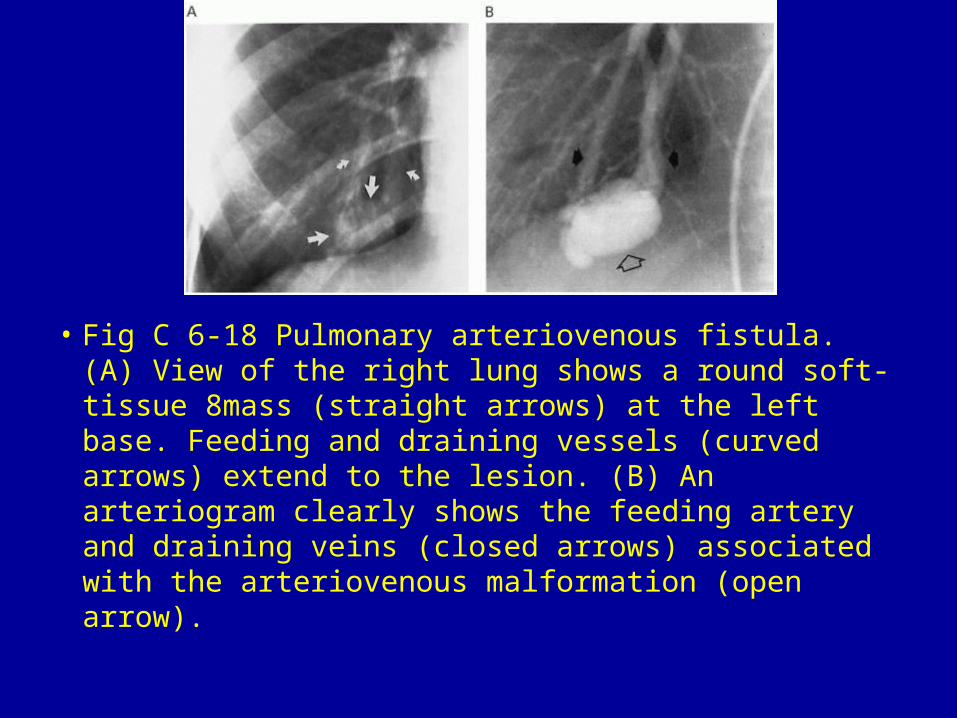
• Fig C 6-18 Pulmonary arteriovenous fistula. (A) View of the right lung shows a round soft-tissue 8mass (straight arrows) at the left base. Feeding and draining vessels (curved arrows) extend to the lesion. (B) An arteriogram clearly shows the feeding artery and draining veins (closed arrows) associated with the arteriovenous malformation (open arrow).
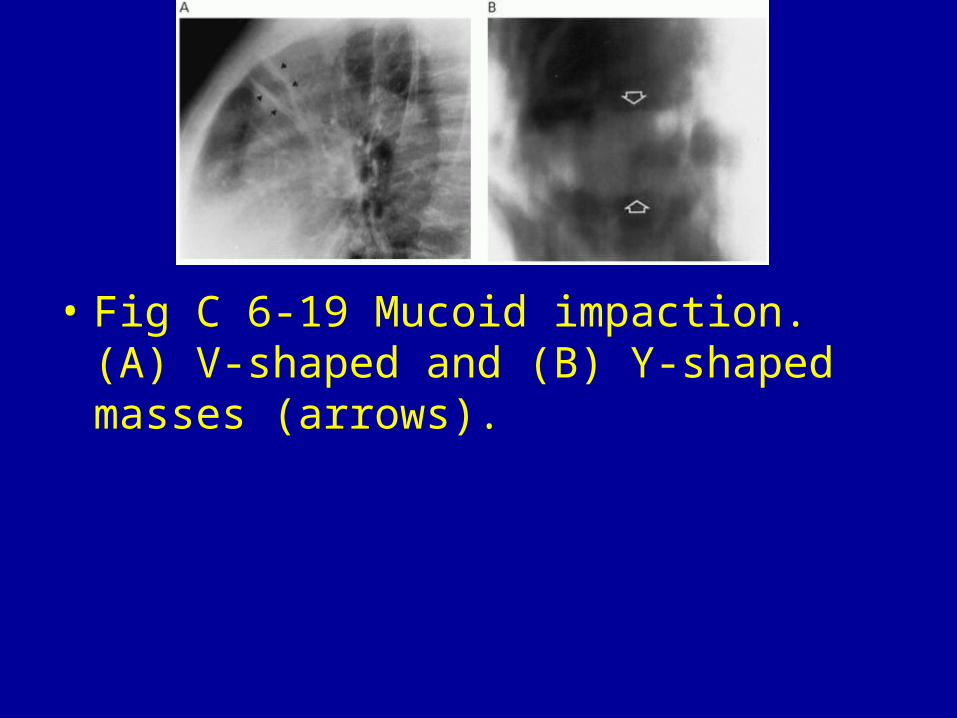
• Fig C 6-19 Mucoid impaction. (A) V-shaped and (B) Y-shaped masses (arrows).
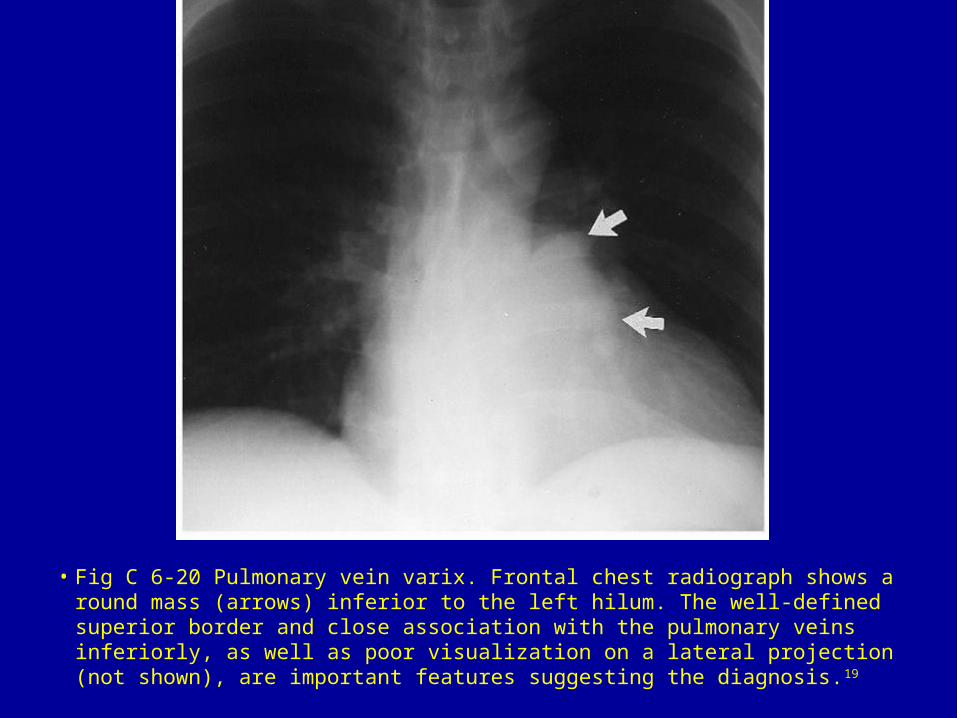
• Fig C 6-20 Pulmonary vein varix. Frontal chest radiograph shows a round mass (arrows) inferior to the left hilum. The well-defined superior border and close association with the pulmonary veins inferiorly, as well as poor visualization on a lateral projection (not shown), are important features suggesting the diagnosis.19
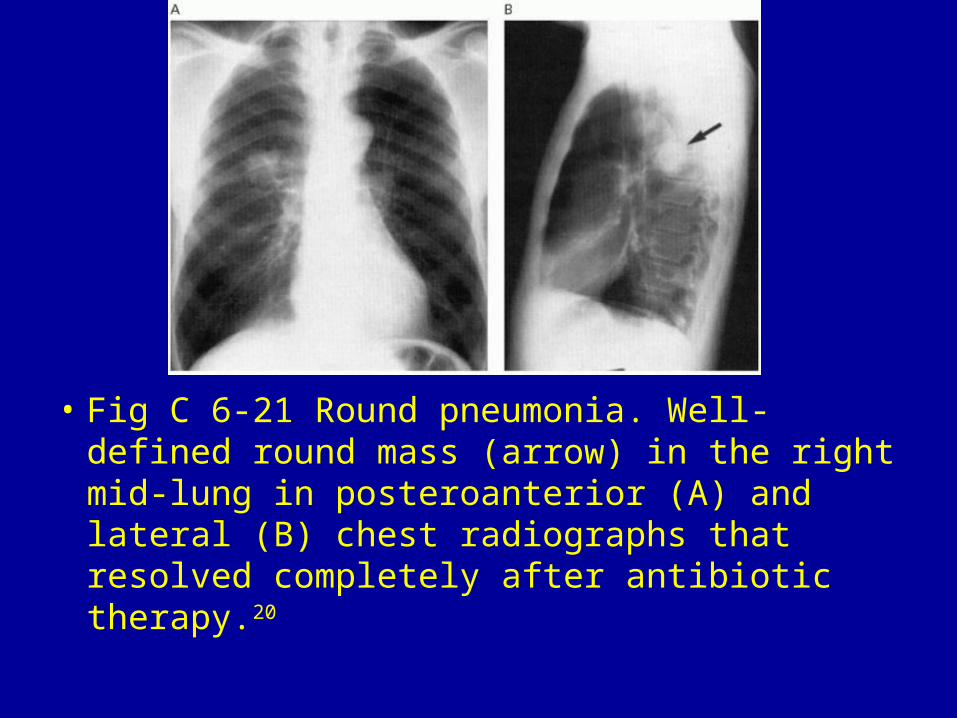
• Fig C 6-21 Round pneumonia. Well-defined round mass (arrow) in the right mid-lung in posteroanterior (A) and lateral (B) chest radiographs that resolved completely after antibiotic therapy.20