Embed Size (px)
Citation preview

Aortic stenosis

OVERVIEW• General Considerations• Approach to the patient• Diagnostic Studies• Prognosis • Treatment• Case Study

General consideration

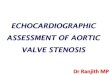
Normal Aortic Valve
Three cusps crescent shaped 3 Commissures 3 sinuses supported by fibrous annulus
3.0 to 4.0 cm2
Node of Arantius

..NORMAL aortic valve surface area is 03 – 04 cm2
..narrowing of aortic orifice is called aortic stenosis

ETIOLOGY
.Congenitally abnormal Bicuspid Aortic Valve
.Senile Degenerated or Calcified Aortic Valve
.Rheumatic heart disease

Bicuspid aortic Valve.congenital abnormality.
.commonly emerge at the age of 50 to 65yrs.
Associated with Coarctation of Aorta and Dilated ascending Aorta


Degenerated or Calcified Aortic valve
25% of patients over age 65yrs have echocardiographic evidence of AS
10 to 20% of them will develop haemodynamically significant Aortic stenosis.
Related with atherosclerotic vascular disease.

Degenerated or Calcified Aortic Valve

Rheumatic Heart Disease
Aortic stenosis is accompanied by Aortic insufficiency and/or mitral valve disease

Aortic Stenosis Mimickers
..Subvalvular Stenosis +Hypertrophic Cardiomyopathy +Subvalvular Membrane
..Supravalvular Stenosis +William syndrome (hypercalcemia ,growth failure and mental retardation)

Risk Factors
..Hyperlipidaemia
..Hypertension
..SmokingFamily history for bicuspid aortic valve

PathphysiologyAortic StenosisProgressive decrease in the area of
the aortic valve
Decreased antegrade velocity when aortic area decrease at least by half
Adaptation by hypertrophy
Early changes
Late changes
Diastolic dysfunction
Systolic dysfunction
Decreased complianceLV Diastolic pressure
Myocardial ischemia myocardial fibrosis abnormal wall motion
Unchanged contractilityNormal stroke volume
Decreased contractilityDecreased stroke volume
Atrial fibrillation
Mitral Regurgitation
Heart Failure

APPROACH

..Patients are initial Asymptomatic
..Patient become symptomatic if: AVA <1.0 Cm2 concomitant CAD
..Systolic Hypertension may coexist but >200mm hg is uncommon
..Hypertrophic Obstructive Cardiomyopathy may also coexist

History
Exertional Angina
Exertional Syncope
Heart Failure
Arrhythmia

Angina Syncope.
..It may occur due to exertion and relieve by rest .. It occurs due to peripheral vasodilatation but unchanged cardiac output.
Sometimes Coronary artery disease may coexist ..It occurs due to exertion

Left sided heart failure
Symptoms Signs.Exertional dyspnea
.Fatigue
.Orthopnea
.Paroxymal Nocturnal Dyspnea
.Wheeze(Cardiac Asthma).Non productive chronic cough
.Tachypnea & Tachycardia
.Pulsus Alternans
.Cardiomegaly
.Ventricular Gallop S3
.Basal Crepitations
Pleural Effusion

Physical Examination..Pulse:Plateau Pulse
..Narrow pulse pressure
..Apex beat may shift to left
..Well- sustained heave
..A2 component of S2 might be absent/soft/normal.
..Prominent S4

Murmur
..Site---Aortic area (Right sec ICS)
..Radiation---To neck through carotid arteries
..Ejection---Systolic murmur
..Character—Harsh
..Position---Leaning forward held in expiration

Severe stenosis is indicated by
..Slow rising pulse
..Narrow pulse pressure
..Longer duration of murmur
..LV heave and S4(LVH)

Diagnostic Studies

1) Electrocardiogram


Chest X ray
..In Early Stage CXR may be normal or Ascending aorta dilatation w/normal heart size
..In Late Stage , Cardiac enlargement Pulmonary Congestion

The ascending aorta (yellow dotted line)leading into the arch is dilated , whereas the distal arch and descending aorta (red dotted line )are normal in size .The left heart border (blue dotted line)

The ascending aorta (yellow dotted line)leading into the arch is dilated, whereas the distal arch and descending aorta red dotted line are normal in size .

Calcified aortic valve (Green arrows)noted on CT

3) Two Dimensional Echocardiography w/Doppler
Diagnostic of AS
Perform the following purposes
..Evaluate Aortic Valve morphology..Calculate Aortic Valve area..Evaluate Left ventricular walls thickness..Calculate Ejection Fraction..Estimate Aortic Valve gradient

Recommendations for Echocardiography in Aortic Stenosis
Classification of Aortic Stenosis
Severity Mean Gradient(mmhg) Aortic Valve area
..Mild
..Moderate
..Severe
..Critical
..<25
..25-40
..>40
..>80
..>1.5
..1-1.5
..<1
..0.5

Anatomic evaluation
Combination of short and long axis images to identify Number of leaflets
Describe leaf mobility, thickness,calcification
Combination of imaging doppler allows the determination of the level of Obstruction;Subvalvular,Valvular,Or Supravalvular.TransEsophageal Echocardiography may be helpful when image quality is suboptimal

Calcific Aortic Stenosis
Nodular calcific masses on aortic side of cusps.
No commissural fusion Free edges of cusps or not involvedStellate –shaped systolic oriface

Calcific Aortic Stenosis
LONG AXIS VIEW SHORT AXIS VIEW

Bicuspid Aortic Valve
Fusion of the Right and Left coronary cusps (80%)Fusion of the Right AND Left Non Coronary cusps (20%)

Bicuspid Aortic ValveTwo cusps are seen in Systole with only two commissures framing an elliptical Systolic oriface(the fish mouth appearance
Diastolic images may mimic a tricuspid valve when a raphe is present

Bicuspid Aortic Valve Parasternal long axis echocardiography may show
An Asymmetric closure line
Systolic doming
Diastolic prolapse of the cusps
In children valve may be stenotic without extensive calcification.
In adult stenosis typically is due to calcific changes ,which often obscures the number of cusps ,making determination of bicuspid VS tricuspid valve difficult.

Calcific Aortic StenosisCalcification of bicuspid valve,the severity can be graded semi quantitavely as
The degree of valve calcification is predictor of clinical outcome.

Aortic SclerosisThickened calcified cusps with preserved mobility.
Typically associated with peak doppler velocity of less than 2.5m/sec.
Rheumatic Aortic StenosisCharacterized by ..Commissural fusion ..Triangular systolic orifice ..thickening &calcificationAccompanied by rheumatic mitral valve changes

Rheumatic Aortic Stenosis Parasternal short axis view showing commissural fusion ,leaflet thickening and calcification ,small triangular systolic orifice.
Subvalvular Aortic Stenosis
1) The discrete membrane consisting of endocardial fold and fibrous tissue.2) A fibromuscular ridge.3) Diffuse tunnel-like narrowing of the LVOT.4) Accessory of anomalous mitral valve tissue.

Supravalvular Aortic Stenosis
Type 1- Thick fibrous ring above the aortic valve with less mobility and has the easily identifiable ‘hourglass’ appearance of the aorta.
Type 2- thin discrete fibrous membrane located above the aortic valve. The membrane usually mobile and may demonstrate doming during systole.
Type 3- diffuse narrowing

Asymptomatic patient murmur of AS heard in physical exam
To dimensional echocardiography with doppler study
Mild to moderate aortic stenosis
Severe aortic stenosis
Follow up the patient
Exercise-testing
Normal Abnormal
Consider cardiac catheterization and Aortic Valve replacement
Algo
rithm
for
man
agem
ent o
f
aorti
c ste
nosis

Symptomatic patient
Two dimensional echocardiography w/doppler study
Mild to moderate aortic stenosis
Severe aortic stenosis
Cardiac catheterization and plan for aortic valve replacement
Work up for other diseases w/h can explain symptoms
Algor
ithm
for
man
agem
ent
of ao
rtic
sten
osis

4) Cardiac catheterization
..Recommended for assessing concomitant CAD
..Recommended prior to aortic valve replacement
..If indications for Dobutamine test have been met

5) Emerging Role of BNP
..Recognized as a marker of EARLY LV failure
..Levels of >550pg/ml are associated with poor outcomes

Prognosis

..Following the onset of symptoms ,prognosis without surgery is poor . 50% 03 years mortality rate
..Mean survival based on Symptoms :1..Angina ->05 years.2..Syncope ->03 years.3..Heart failure ->02 years
..Sudden Cardiac death may occur in asymptomatic individuals ~04%

Treatment

Initial Treatment
..Depend upon the presenting complaints. ..If LV failure,
Symptom-improving drugs Prognosis-improving drugs
..Treating hypertension normalizing lipid profile and smoking cessation have the role .

Definitive treatment
Mechanical solution for mechanical problem
AORTIC VALVE REPLACEMENT
..There are two options for valve replacement ...Surgical valve replacement...Transcatheter Aortic Valve Replacement (TAVR)

Surgical Valve Replacement
.Mechanical Valve Replacement .Bioprosthetic Valve Replacement

TAVR
..It comes second to the surgical valve replacement .
..Performed either as a means of temporary stabilization or patient with surgical risk

Thank you
DR.RAVI KUMAR CTVSKG HOSPITALCOIMBATORETAMIL NADU