Embed Size (px)
Citation preview

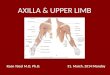
AXILLA & Brachial plexus

The Axilla• A pyramidal
shaped space between the upper part of the arm and the side of the chest through which major neurovascular neurovascular structures pass between neck & thorax and upper limb.
• Axilla has an apex, a base and four walls.

Boundaries of the Axilla
Apex: Is directed upwards
into the root of the neck
is bounded, by 3 bones:• Clavicle anteriorly.• Upper border of the
scapula posteriorly.
• Outer border of the first rib medially.
• It is called cervico-axillary canal.

Anterior wall: Is formed by
• Pectoralis major• Pectoralis minor• Subclavius• Clavipectoral fascia:
Pectoralis major
Pectoralis minor
Clavipectoral fascia

• Posterior wall:• Is formed by:
• Subscapularis• Latissimus dorsi• Teres major
muscles

The medial wall: Is formed by:
• Serratus anterior• Upper 4 or 5 ribs
& Intercostal muscles .
The lateral wall: Is formed by:
• Coracobrachialis• Biceps brachii • Intertubercular
groove of the humerus.

Base: Formed by skin stretching
between the anterior and posterior walls.
It is bounded:• In front by the anterior
axillary fold (formed by the lower border of the Pectoralis major muscle).
• behind by the posterior axillary fold (formed by the tendons of latissimus dorsi and teres major muscles).
• medially by upper 4 to 5 ribs & the chest wall.

Contents of The Axilla
• Cords and braches of brachial plexus.
• Axillary artery and its branches.
• Axillary vein and its tributaries.
• Axillary lymph nodes.
• Axillary fat.• Loose connective
tissue.
The neurovascular bundle is enclosed in connective tissue sheath, called ‘axillary sheath’
Axillary a. & v.
Brachial plexus

Location & Formation
Brachial Plexus is present in the posterior triangle of the neck & axilla.
It is formed by the union of the anterior Rami of the C 5th, 6th, 7th & 8th and the 1st thoracic spinal nerve.
What is a Brachial Plexus ?Brachial Plexus is a network of nerves that present at the root of the neck to enter the upper limb.
The roots of C5 & C6 unite to form---- Upper trunkThe root of C7 continues as the-------- Middle trunkThe roots of C8 & T1 unite to form---- Lower trunk
9

The Plexus can be divided into 5 stages: Roots: in the posterior∆ of the neck.Trunks: in the posterior∆ of the neck. Divisions: behind the clavicle (apex of the axilla).Cords: in the axilla.Branches: in the axilla.NB. The First 2 stages lie in the posterior triangle, while last 2 sages lie in axilla.

The anterior divisions of the upper and middle trunks unite to form the Lateral cord.
The anterior division of the lower trunk continues as the Medial cord. All the posterior divisions of three trunks join to form the Posterior
cord. Cords are named according to there relation to the 2nd part of the
axillary artery 11

BRNCHE S
Lateral cord- 3 Medial cord- 5 Posterior cord- 5Lateral pectoral nerve. Medial pectoral nerve. Axillary nerve.Musculocutaneous nerve. Ulnar nerve. Radial nerve.
Median nerve (lateral root). Median nerve (medial root). Upper & lower subscapular nerves.
Medial cutaneous nerve of arm & forearm.
Thoracodorsal or N. to latissimus dorsi.

Brachial plexus injuries• May involve the roots, trunks,
divisions, cords & branches • Supraclavicular injuries involve
the roots and the trunks, infraclavicular injuries will affect the divisions and cords
• Result due to:– Compression– Traction– Stab wounds
• Symptoms depend on the site of injury & involvement of nerve fibers

Brachial plexus injuries
• Are of two types:– Upper lesions usually involving C5 & C6– Lower lesions usually involving (C8), T1

Upper Lesions of the Brachial Plexus(Erb-Duchenne Palsy)
• These are usually the result of traction & tearing of the 5th and 6th root of the brachial plexus
• This may occur:• In infants during a difficult
delivery • In adults following a fall on or
a blow to the shoulder.• It involves the:
• Nerve to sublavius• Suprascapular nerve• Axillary nerve• Musculocutaneous nerve

• The muscles affected are:– Abductors (supraspinatus &
deltoid) and lateral rotators (Infraspinatus &teres minor) of the shoulder
– Subclavius, biceps, brachialis & coracobrachialis
• Thus:– The limb hangs limply by the
side, and is medially rotated– The forearm is pronated and
extended– There is loss of sensation down
the lateral side of the arm & the forearm
• Another name for this lesion is 'porters tip'

Lower Lesions of the Brachial Plexus (Klumpke Palsy)
• These are usually caused by excessive abduction of the arm as a result of:– Someone clutching for an
object when falling from a height
– Difficult delivery in which baby’s upper limb is pulled excessively.
– Result of malignant metastases from the lungs in the lower deep cervical lymph nodes
– A cervical rib

Person grasping something to prevent a fall

Baby’s upper limb is pulled excessively during delivery

• The hand has a clawed appearance due to:– Hyperextension of the
metacarpophalangeal joints (the extensor digitorum is unopposed by the lumbricals and interossei and extends the metacarpophalangeal joints).
– Flexion of the interphalangeal joints (the flexor digitorum superficialis and profundus are unopposed by the lumbricals and interossei, the middle and terminal phalanges are flexed).
Lower Lesions of the Brachial Plexus (Klumpke Palsy)

Thoracic Outlet syndrome (TOS)

22
Thoracic Outlet SyndromeCauses
1. Many factors can induce thoracic outlet syndrome, including congenital, trauma
and atherosclerotic factors.2. Bony abnormalities are present in 30%
of patients, such as cervical rib, bifid first rib, fusion of first and second ribs or previous thoracoplasty.

Thoracic Outlet Syndrome• Thoracic outlet syndrome results from
compression of the subclavian vessels and brachial plexus.
• Patients may complain of neck and shoulder pain with numbness and tingling in the upper extremity.
• The ulnar side is typically involved.• Using the extremity in an overhead or
elevated position is difficult.

Cervical Rib
Involves Inferior part of Plexus
Thoracic Outlet Syndrome

25
Thoracic Outlet SyndromeANATOMIC CONSIDERATIONS
1. The subclavian vessels and brachial plexus transverse the cervico-axillary canal into the arm.
2. The outer border of the first rib divides the canal into a proximal and a distal division.
3. The proximal division is composed of the scalene triangle and the space bounded by the clavicle and the first rib( costoclavicular space ).

26
Thoracic Outlet SyndromeANATOMIC CONSIDERATIONS
4. The proximal division is the most critical for neurovascular compression. It is bounded superiorly by the clavicle and the subclavius muscle; inferiorly by the first rib; anteromedially by the sternum, clavipectal fascia and the costocoracoid ligament; and posterolaterally the scalenus media muscle and the long thoracic nerve.

Thoracic Outlet SyndromeClinical Signs and Symptoms
• Upper extremity pain.• Upper extremity paresthesias.• Grip weakness• Upper extremity edema.• Upper extremity coldness.• Excessive dryness of the arm or hand.• Excessive sweating of the arm or hand.

28
Thoracic Outlet Syndrome DIAGNOSIS
1. Physical Exam, history, radiographs of chest and cervical spine, neuroloical consultation, NCV (nerve conduction studies).
2. Pulmonary, esophageal and chest wall causes must be ruled out.

29
Thoracic Outlet SyndromeTHERAPY
1. Physiotherapy is performed before surgery.2. Physiotherapy includes heat massage,
active neck exercise, scalenus anterior muscle stretching, strengthening of the upper trapezius muscle.
3. Resection of the first rib, and a cervical rib when present, is best performed through the trans-axillary approach, with decompression of 7th and 8th cervical and 1st thoracic root.

GOOD LUCK