Embed Size (px)
Citation preview

Chapter 15: Treatment ofPsychological Disorders

Types of Treatment
• Psychotherapy– Insight therapies
• “talk therapy”– Behavior therapies
• Changing overt behavior– Biomedical therapies
• Biological functioning interventions

Bell Work
• Why might a person suffering from a mental disorder not seek treatment?

Who Seeks Treatment?
• 15% of U.S. population in a given year• Most common presenting problems
– Anxiety and Depression• Women more likely to seek help than men• Medical insurance• Education level• Stigma surrounding the receipt of mental
health treatment

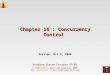
Figure 15.2 Therapy utilization rates

Figure 15.3 Psychological disorders and professional treatment

Who Provides Treatment?• Clinical psychologists• Counseling psychologists
– Doctoral degree (PhD, PsyD, EdD); competitive—comparable to med school
• Psychiatrists: prescribe meds; MD• Clinical social workers: master’s• Psychiatric nurses
– bachelor’s or master’s; hospital inpatient treatment• Counselors
– Schools, colleges, human services– Master’s– Specialize (school, vocational, marital)

Insight Therapies: Psychoanalysis
• Sigmund Freud and followers– Goal: discover unresolved unconscious
conflicts• Free association• Dream analysis• Interpretation: explain the inner
significance of the client’s thoughts, feelings, memories, and behaviors
–Resistance and transference

Figure 15.4 Freud’s view of the roots of disorders

Insight Therapies: Client-Centered Therapy
• Carl Rogers– 40s and 50s– Goal: restructure self-concept to better
correspond to reality– Therapeutic Climate
• Genuineness• Unconditional positive regard• Empathy

Figure 15.5 Rogers’s view of the roots of disorders

Behavior Therapies
• B.F. Skinner and colleagues– Goal: unlearning maladaptive behavior and
learning adaptive ones– Systematic Desensitization – Joseph
Wolpe (1958)• Reduce phobic clients’ anxiety through
counterconditioning• 1. anxiety hierarchy• 2. deep muscle relaxation training• 3. work through hierarchy
– Aversion therapy• Alcoholism, sexual deviance, smoking,
etc.

Figure 15.7 The logic underlying systematic desensitization

Behavior Therapy
• B.F. Skinner and colleagues– Social skills training
• Modeling • Behavioral rehearsal

Cognitive-Behavioral Therapy
• Aaron Beck– Cognitive therapy
• Goal: to change the way clients think– Detect and recognize negative thoughts– Reality testing– Kinship with behavior therapy

Figure 15.10 Beck’s view of the roots of disorders

Biomedical Therapies
• Psychopharmacotherapy– Antianxiety - Valium, Xanax, Buspar– Antipsychotic - Thorazine, Mellaril, Haldol
• Tardive dyskinesia• Clozapine
– Antidepressant:• Tricyclics – Elavil, Tofranil• Mao inhibitors (MAOIs) - Nardil• Selective serotonin reuptake inhibitors
(SSRIs) – Prozac, Paxil, Zoloft

Biomedical Therapies
• Psychopharmacotherapy– Mood stabilizers
• Lithium• Valproic acid
• Electroconvulsive therapy (ECT)

Figure 15.12 Antidepressant drugs’ mechanisms of action

Current Trends and Issues in Treatment
• Managed care• Empirically validated treatments• Blending Approaches to treatment• Multicultural sensitivity• Deinstitutionalization
– Revolving door problem– Homelessness

Figure 15.15 Declining inpatient population at state and county mental hospitals

Figure 15.16 Percentage of psychiatric inpatient admissions that are re-admissions