Embed Size (px)
Citation preview
Dr Clare Guildinge.mail: [email protected]
Drugs used in haematology; anticoagulants, antiplatelet agents and thrombolytic agents
Learning Outcomes
This session should assist you in acquiring the knowledge & understanding to:
― Describe the basic pharmacology of anticoagulant, antiplatelet and fibrinolytic drugs
Lesson outline
1. Disorders of inappropriate blood clotting (thrombosis)
2. Drugs developed to prevent and/or reverse thrombus formation:
- Anticoagulants
- Antiplatelet agents
- Thrombolytic agents
Drugs used in haematology
Drugs and blood clotting
Before you learn the pharmacology of anticoagulant drugs you should ensure you understand the following physiological processes:
• Normal haemostatic processes1. Vasoconstriction – reduces blood flow therefore reduces
blood loss2. Platelet plug formation – involving platelet adhesion,
platelet release reaction and platelet aggregation3. Stable clot formation (coagulation cascade) – end result is
activation of thrombin which :
a) converts soluble fibrinogen to insoluble fibrinb) induces more platelet recruitment and activation
• Normal fibrinolytic mechanisms
Thrombosis
• Thrombosis – pathogenic state in which the normal haemostatic processes are activated inappropriately
Atrial FibrillationDeep Vein Thrombosis
Pulmonary EmbolusMyocardial infarction
Atrial FibrillationDeep Vein Thrombosis
Pulmonary EmbolusMyocardial infarction
AnticoagulantsAntiplatelet agentsFibrinolytic agents
Thrombosis
• Thrombosis – pathogenic state in which the normal haemostatic processes are activated inappropriately
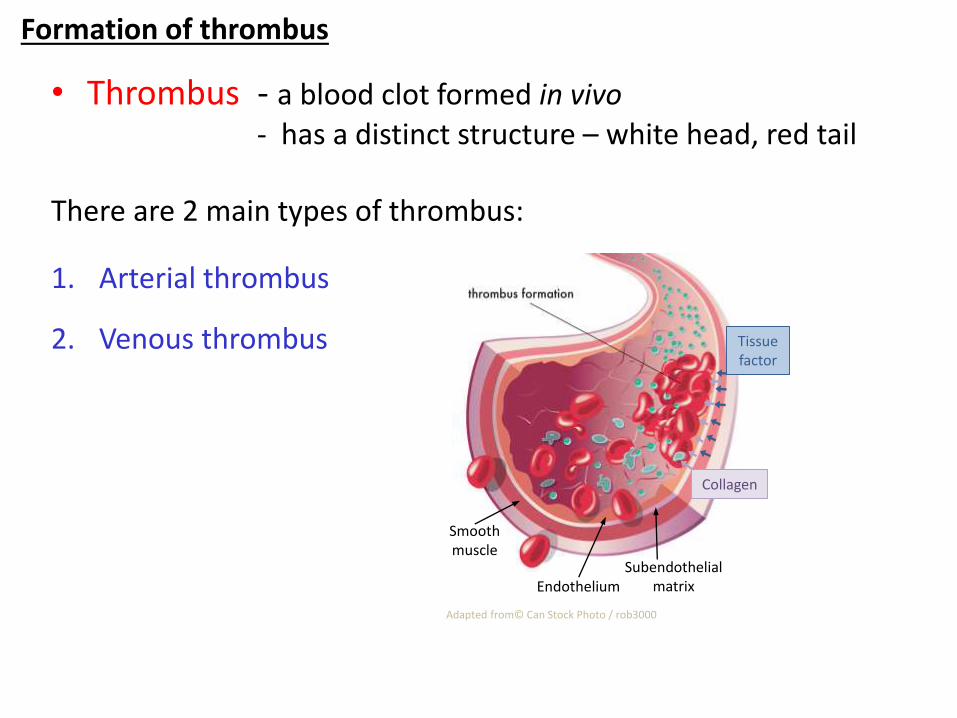
Formation of thrombus
• Thrombus - a blood clot formed in vivo- has a distinct structure – white head, red tail
There are 2 main types of thrombus:
1. Arterial thrombus
2. Venous thrombus
Adapted from© Can Stock Photo / rob3000
Tissue factor
Collagen
EndotheliumSubendothelial
matrix
Smooth muscle
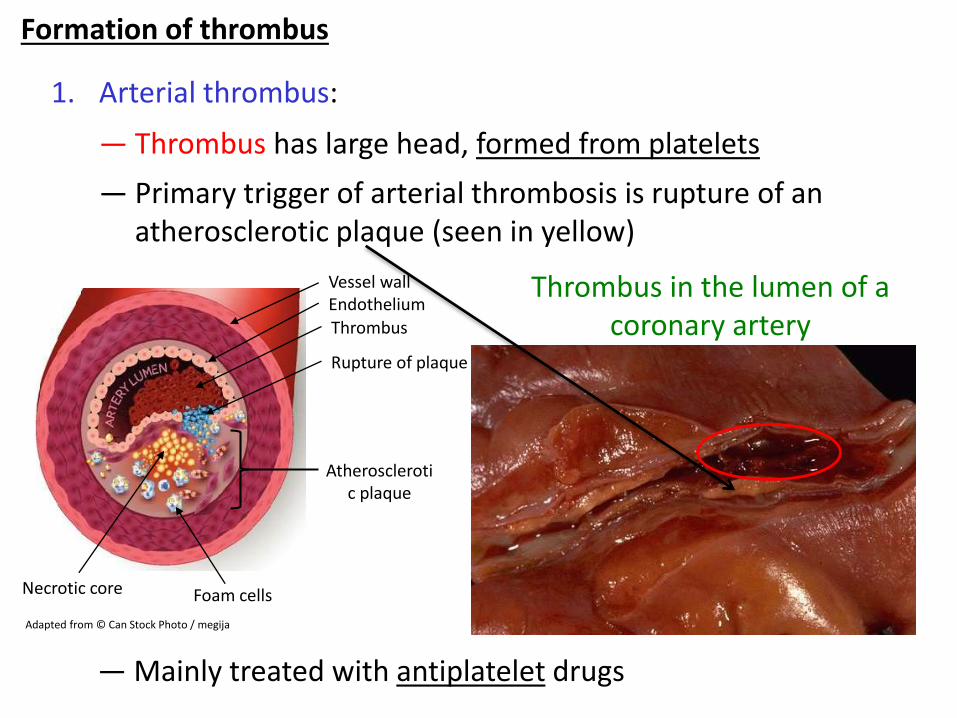
Formation of thrombus
1. Arterial thrombus:
— Thrombus has large head, formed from platelets
— Primary trigger of arterial thrombosis is rupture of an atherosclerotic plaque (seen in yellow)
Thrombus in the lumen of a coronary artery
— Mainly treated with antiplatelet drugs
Adapted from © Can Stock Photo / megija
Foam cells
Rupture of plaque
Thrombus
Atherosclerotic plaque
Necrotic core
EndotheliumVessel wall
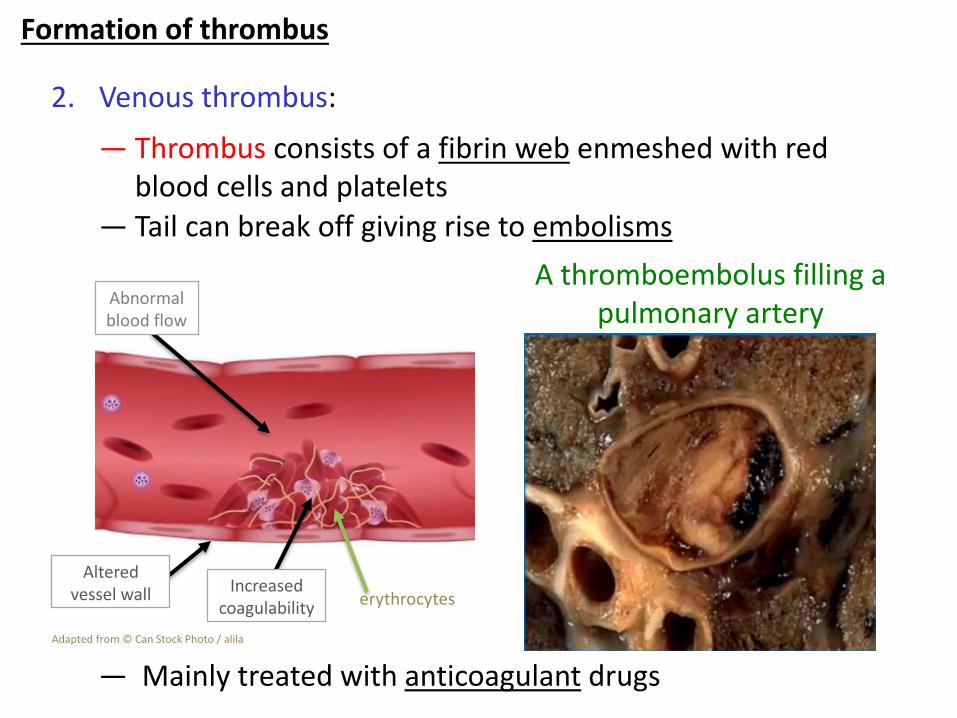
Formation of thrombus
2. Venous thrombus:
— Thrombus consists of a fibrin web enmeshed with red blood cells and platelets
— Tail can break off giving rise to embolisms
A thromboembolus filling a pulmonary artery
— Mainly treated with anticoagulant drugs
Abnormal blood flow
Increased coagulability erythrocytes
Altered vessel wall
Adapted from © Can Stock Photo / alila
Drugs and blood clotting
• Drugs have been developed to prevent and/or reverse thrombus formation. These drugs fall into 3 classes:
1. Anticoagulantse.g Heparin and oral anticoagulants- modify blood clotting mechanisms
2. Antiplatelet agentse.g Aspirin include clopidrogel next year- inhibit COX-1 activity to inhibit platelet aggregation
3. Fibrinolytic agentse.g Alteplase- break down fibrin
Anticoagulants
• There are 4 main classes of anticoagulant
1. Heparin and low molecular weight heparins2. Warfarin3. Selective factor Xa inhibitors4. Direct thrombin (factor IIa) inhibitors
• Anticoagulants target various factors in the coagulation cascade, thereby preventing formation of a stable fibrin meshwork.
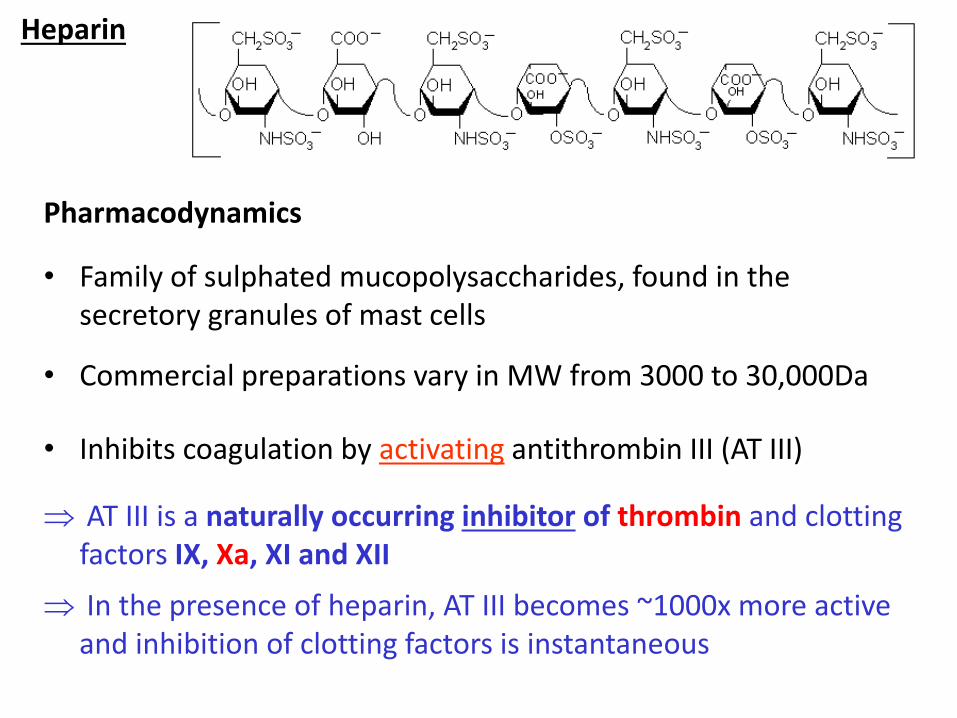
Heparin
Pharmacodynamics
• Family of sulphated mucopolysaccharides, found in the secretory granules of mast cells
• Commercial preparations vary in MW from 3000 to 30,000Da
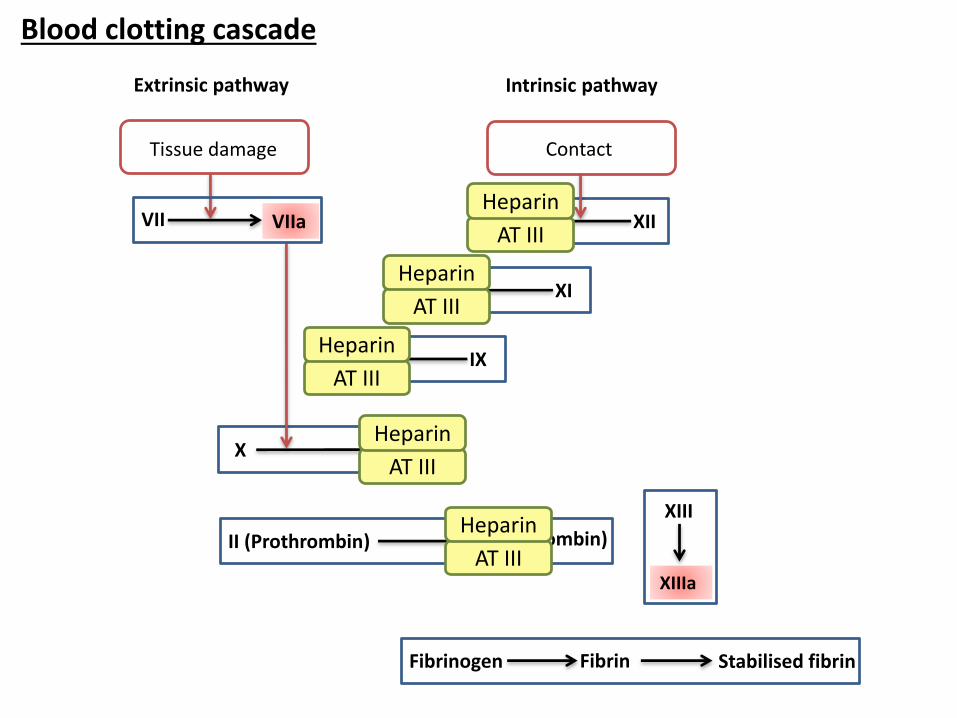
• Inhibits coagulation by activating antithrombin III (AT III)
AT III is a naturally occurring inhibitor of thrombin and clotting factors IX, Xa, XI and XII
In the presence of heparin, AT III becomes ~1000x more active and inhibition of clotting factors is instantaneous
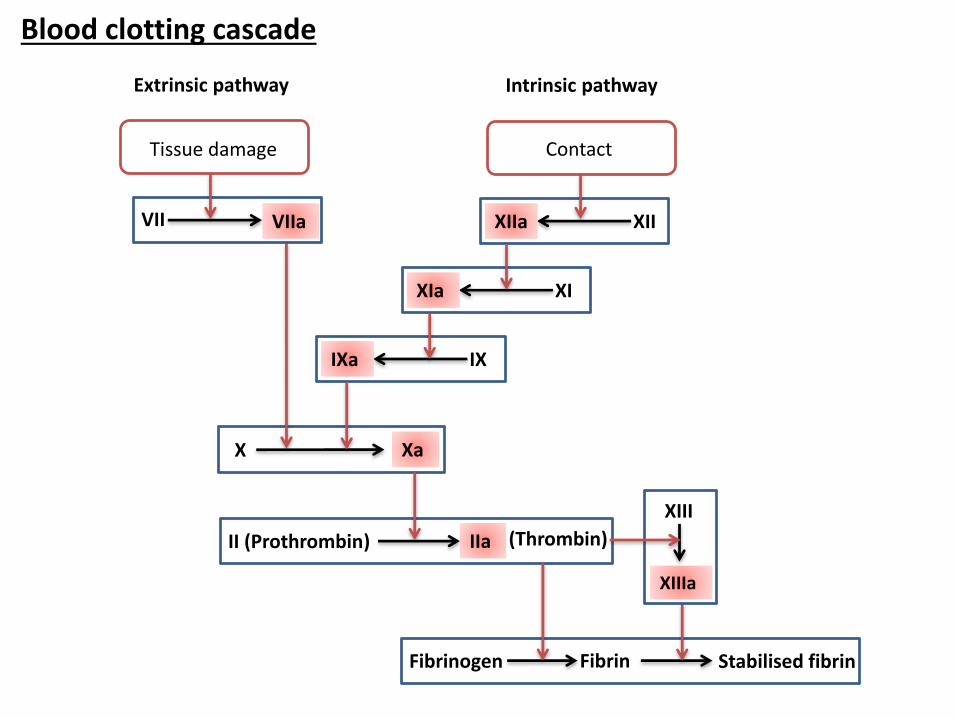
XIIXIIa
XIXIa
X Xa
IXIXa
II (Prothrombin) IIa (Thrombin)
Fibrinogen Fibrin Stabilised fibrin
XIIIa
XIII
ContactTissue damage
Extrinsic pathway Intrinsic pathway
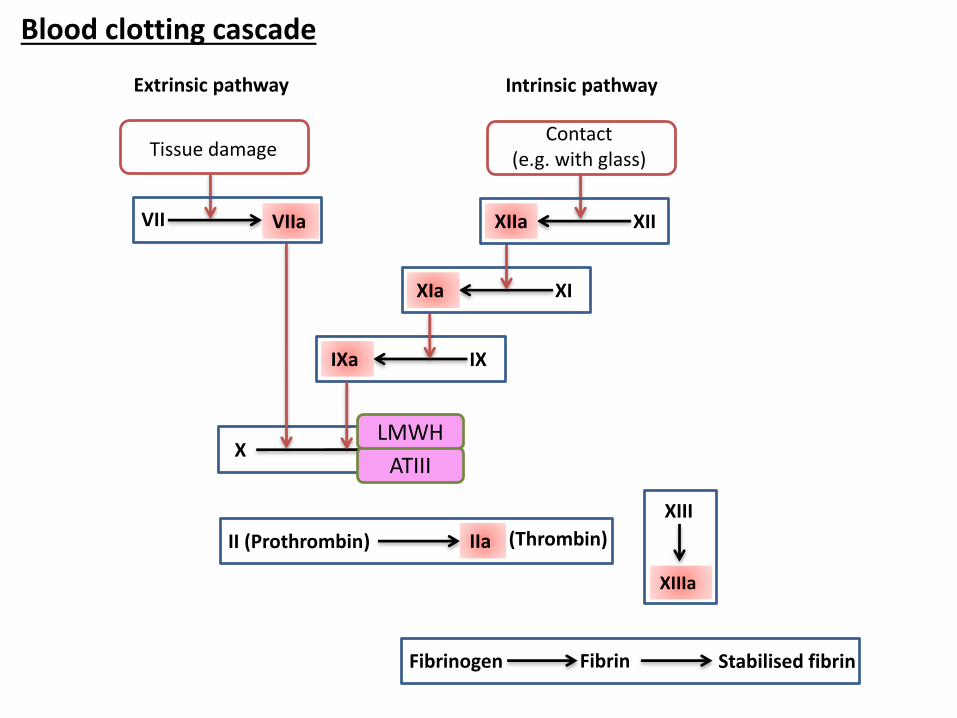
Blood clotting cascade
VII VIIa
XIIXIIa
XIXIa
X Xa
IXIXa
II (Prothrombin) IIa (Thrombin)
Fibrinogen Fibrin Stabilised fibrin
XIIIa
XIII
Intrinsic pathway
AT III
Heparin
AT III
Heparin
AT III
Heparin
AT III
Heparin
AT III
Heparin
Blood clotting cascade
Tissue damage
Extrinsic pathway
VII VIIa
Contact
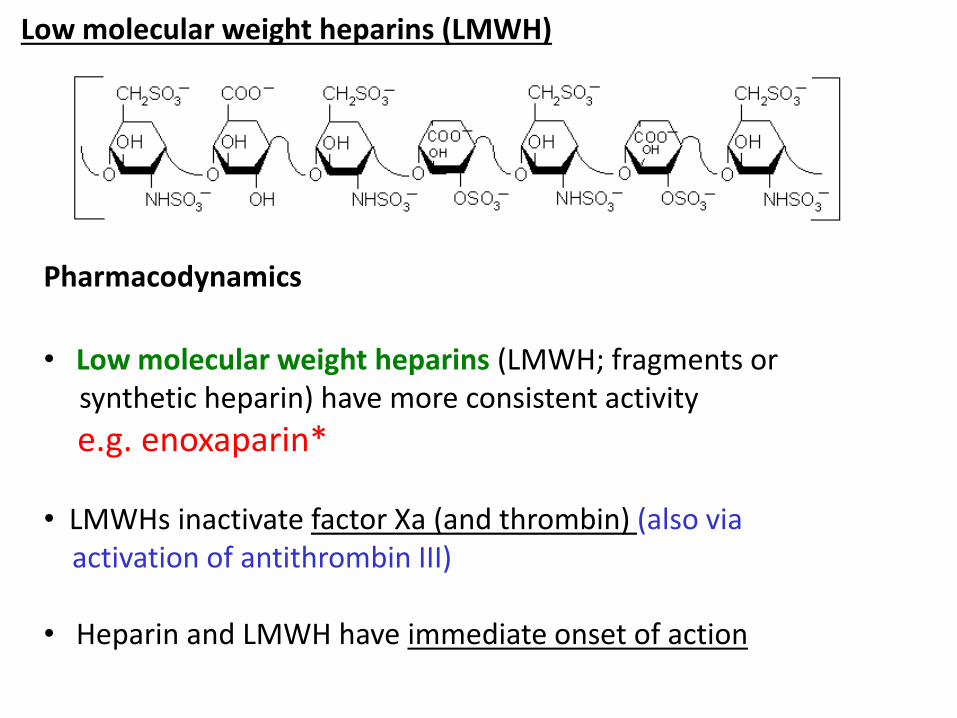
Pharmacodynamics
• Low molecular weight heparins (LMWH; fragments or synthetic heparin) have more consistent activity
e.g. enoxaparin*
• LMWHs inactivate factor Xa (and thrombin) (also via activation of antithrombin III)
• Heparin and LMWH have immediate onset of action
Low molecular weight heparins (LMWH)
XIXIa
X Xa
IXIXa
II (Prothrombin) IIa (Thrombin)
Fibrinogen Fibrin Stabilised fibrin
XIIIa
XIII
Contact(e.g. with glass)
Intrinsic pathway
Blood clotting cascade
ATIII
LMWH
Tissue damage
Extrinsic pathway
VII VIIa XIIXIIa
Heparin and LMWH: Pharmacokinetics
• Inactive given orally (not absorbed from GI tract)
• Administered IV or SC (SC for LMWHs)
• Heparin has a short half life (t ½ <1h low doses, 2h large doses) ― Heparin must be given frequently or as a continuous
infusion
• LMWH have longer duration of action (t ½ ~4-5h)― Allows once daily dosing
• Eliminated mainly by renal excretion― Care needed in patients with renal disease
• Side effects include bleeding and hypersensitivity
• Overdose treated by IV protamine (strongly basic protein)
Heparin: Clinical use
• Treatment of established venous thromboembolism
• Prevention of venous thromboembolism – LMWHs used to prevent post-operative venous thrombosis
• Cardiac disease – reduces risk of venous thromboembolism in patients with angina and following acute MI
Because of the need for frequent dosing, if long-term anticoagulation is required, heparin is often used only to commence
anticoagulation therapy until an oral anticoagulant takes effect
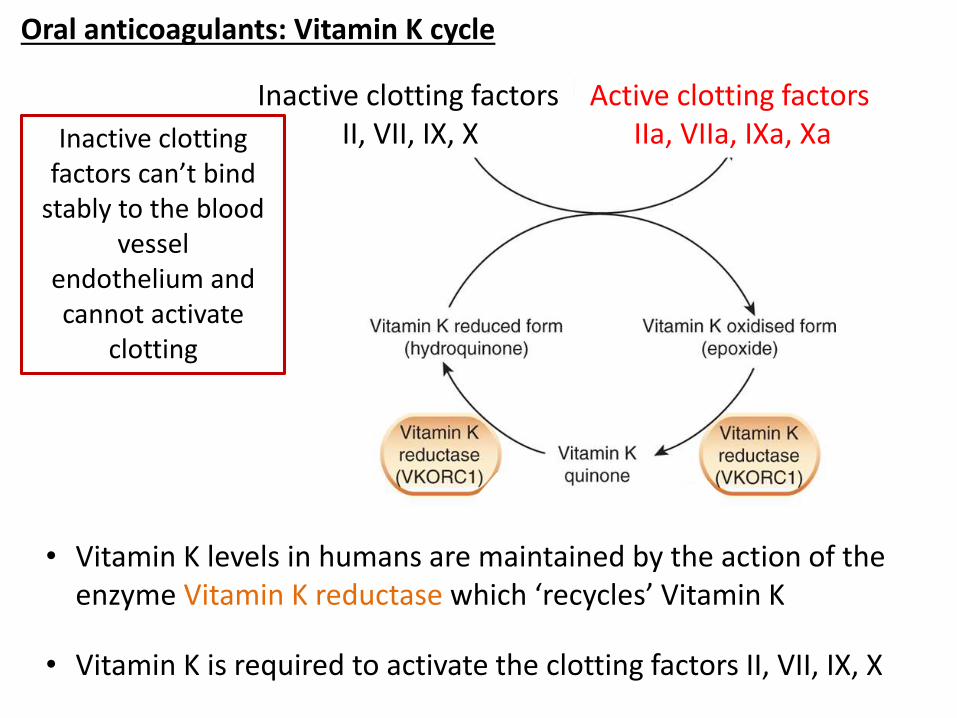
Oral anticoagulants: Vitamin K cycle
Inactive clotting factorsII, VII, IX, X
Active clotting factorsIIa, VIIa, IXa, Xa
• Vitamin K levels in humans are maintained by the action of the enzyme Vitamin K reductase which ‘recycles’ Vitamin K
• Vitamin K is required to activate the clotting factors II, VII, IX, X
Inactive clotting factors can’t bind
stably to the blood vessel
endothelium and cannot activate
clotting
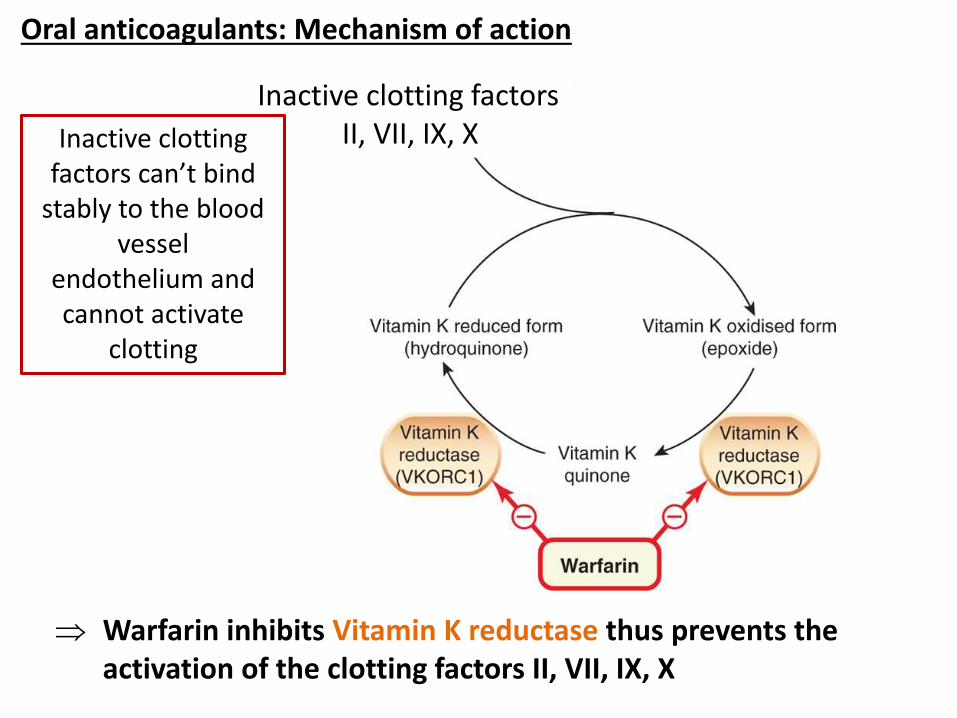
Oral anticoagulants: Mechanism of action
Warfarin inhibits Vitamin K reductase thus prevents the activation of the clotting factors II, VII, IX, X
Inactive clotting factorsII, VII, IX, XInactive clotting
factors can’t bind stably to the blood
vessel endothelium and cannot activate
clotting
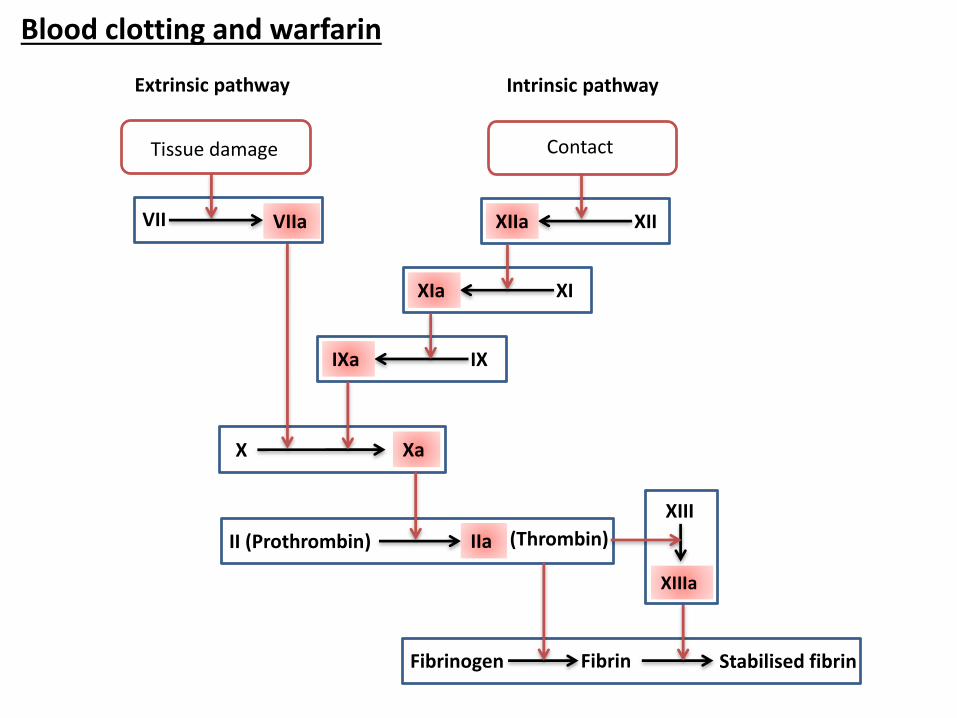
XIIXIIa
XIXIa
X Xa
IXIXa
II (Prothrombin) IIa (Thrombin)
Fibrinogen Fibrin Stabilised fibrin
XIIIa
XIII
Tissue damage
Extrinsic pathway Intrinsic pathway
VII VIIa
Blood clotting and warfarin
Contact
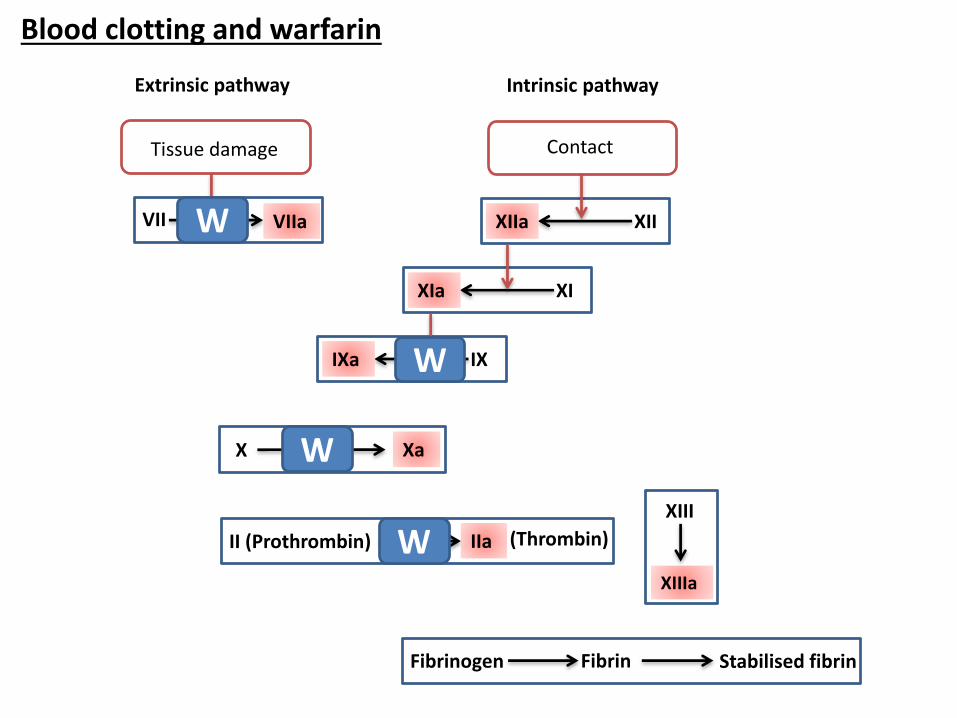
XIIXIIa
XIXIa
X Xa
IXIXa
II (Prothrombin) IIa (Thrombin)
Fibrinogen Fibrin Stabilised fibrin
XIIIa
XIII
ContactTissue damage
Extrinsic pathway Intrinsic pathway
VII VIIa
W
W
W
W
Blood clotting and warfarin
• Inhibits the activation of Vitamin K1 dependent clotting factors II, VII, IX and X
• The shift in haemostatic balance in favour of anticoagulation doesn’t take place until all active vitamin K dependant proteins, made before the drug was administered have been cleared from the circulation.
• The process occurs at different rates for different clotting factors e.g. half life VII ~6h, half life IX and X 9 ~ 8-24h, half life prothrombin (II) ~72hHence there is a 1-2 day lag period before warfarin is
pharmacologically effective
• A small population of patients is genetically resistant to warfarin, due to reduced binding to Vitamin K reductases
Warfarin: Pharmacodynamics and pharmacokinetics
• Absorption - rapidly and almost totally absorbed from the GI tract
- levels peak in blood ~0.5-4h after administration
• Distribution – low volume of distribution as ~ 99% plasma protein bound (mainly to albumin)
• Metabolism – action is terminated by metabolism in the liver by CYP450 enzymes (e.g. CYP2C9, 2C19, 3A4)
• Excretion – metabolites are conjugated to glucuronide and excreted in urine and faeces
• Half life – variable ~ 15-80 hours
• Dose is highly variable - (2-112 mg/week)
Warfarin: Pharmacokinetics
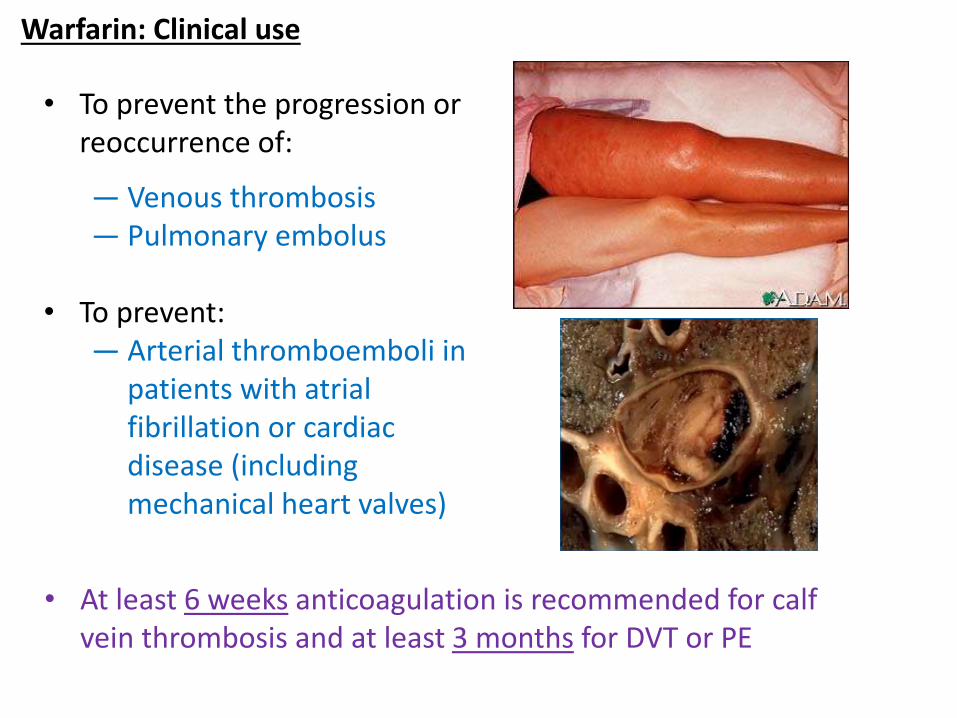
Warfarin: Clinical use
• To prevent the progression or reoccurrence of:
— Venous thrombosis— Pulmonary embolus
• To prevent:— Arterial thromboemboli in
patients with atrial fibrillation or cardiac disease (including mechanical heart valves)
• At least 6 weeks anticoagulation is recommended for calf vein thrombosis and at least 3 months for DVT or PE
• Acute anticoagulation usually starts with heparin and an oral anticoagulant e.g. warfarin
• Heparin is rapidly effective – Effect of heparin is monitored by activated partial
thromboplastin time (APTT)– LMMH – usually no monitoring needed, has less side
effects and fewer bleeding complications
• Warfarin takes several days to achieve full anticoagulation– Effect of anticoagulant monitored using the prothrombin
time (converted to INR: International normalised ratio)
• Heparin therefore covers the lag period and can then be withdrawn
Clinical practice
Your patient is prescribed warfarin. Would the addition of the following drugs to the dosing regimen increase or decrease anticoagulation within the body?
1. Drugs which have a high affinity for the plasma binding protein albumin e.g. sulfonamides
2. Drugs which reduce absorption e.g. sucralfate
3. Drugs which decrease platelet aggregation e.g. aspirin
4. Drugs which inhibit CYP 2C9 e.g. St John’s Wort
Warfarin prescribing questions
Your patient is prescribed warfarin. Would the addition of the following drugs to the dosing regimen increase or decrease anticoagulation within the body?
1. Drugs which have a high affinity for the plasma binding protein albumin e.g. sulfonamides
Increase. Warfarin is highly plasma protein bound. Sulfonamidescomptete with warfarin for binging to albumin, so more warfarin is free/unbound (=more pharmacologically available)
2. Drugs which reduce absorption e.g. sucralfate
3. Drugs which decrease platelet aggregation e.g. aspirin
4. Drugs which inhibit CYP 2C9 e.g. St John’s Wort
Warfarin prescribing questions
Your patient is prescribed warfarin. Would the addition of the following drugs to the dosing regimen increase or decrease anticoagulation within the body?
1. Drugs which have a high affinity for the plasma binding protein albumin e.g. sulfonamides
2. Drugs which reduce absorption e.g. sucralfateDecrease. Less warfarin would be absorbed from the GI tract
3. Drugs which decrease platelet aggregation e.g. aspirin
4. Drugs which inhibit CYP 2C9 e.g. St John’s Wort
Warfarin prescribing questions
Your patient is prescribed warfarin. Would the addition of the following drugs to the dosing regimen increase or decrease anticoagulation within the body?
1. Drugs which have a high affinity for the plasma binding protein albumin e.g. sulfonamides
2. Drugs which reduce absorption e.g. sucralfate
3. Drugs which decrease platelet aggregation e.g. aspirinIncrease. Both drugs ultimately lead to a reduction in blood clot formation, so addition of aspirin would potentiate warfarin’s actions
4. Drugs which inhibit CYP 2C9 e.g. St John’s Wort
Warfarin prescribing questions
Your patient is prescribed warfarin. Would the addition of the following drugs to the dosing regimen increase or decrease anticoagulation within the body?
1. Drugs which have a high affinity for the plasma binding protein albumin e.g. sulfonamides
2. Drugs which reduce absorption e.g. sucralfate
3. Drugs which decrease platelet aggregation e.g. aspirin
4. Drugs which inhibit CYP 2C9 e.g. St John’s WortIncrease. CYP2C9 metabolises (inactivates) warfarin. Less CYP2C9 = less inactivation = more pharmacologically active warfarin remains
Warfarin prescribing questions
3. Selective factor Xa inhibitors4. Direct thrombin (factor IIa) inhibitors e.g. dabigatran
Newer oral anticoagulants
Dabigatran• Competitive reversible inhibitor of thrombin
• Used for:— Prevention of stroke and embolism in patients with
atrial fibrillation— Prophylaxis of venous thromboembolism after hip or
knee replacement surgery
• Has a rapid onset of action
• Does NOT require routine oral anticoagulant monitoring
• No way to reverse anticoagulation in the event of a significant bleed
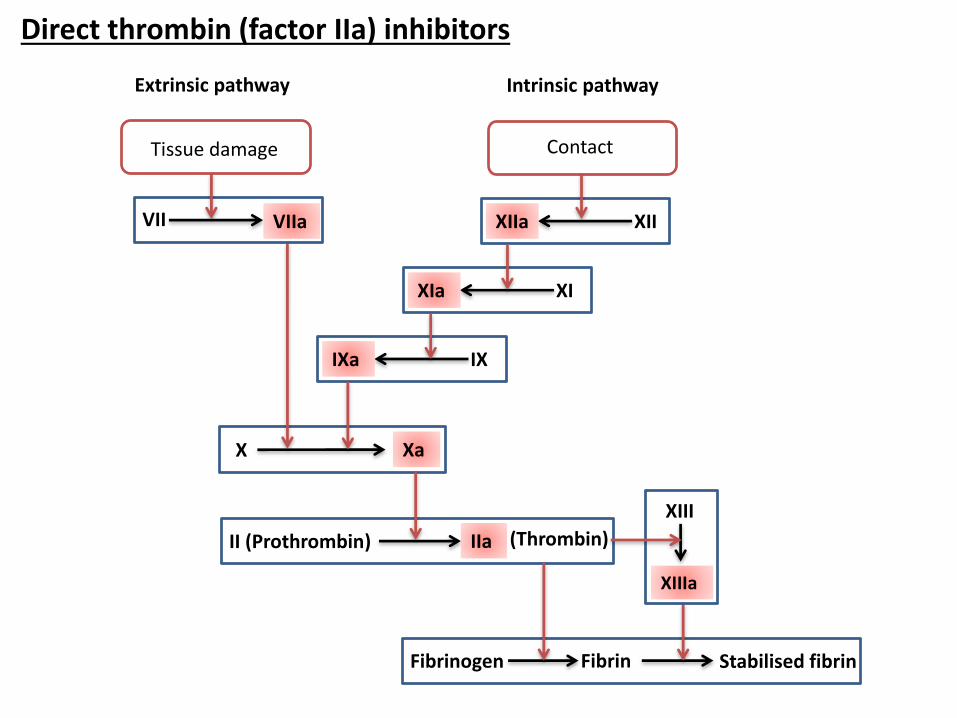
XIIXIIa
XIXIa
X Xa
IXIXa
II (Prothrombin) IIa (Thrombin)
Fibrinogen Fibrin Stabilised fibrin
XIIIa
XIII
Tissue damage
Extrinsic pathway Intrinsic pathway
VII VIIa
Direct thrombin (factor IIa) inhibitors
Contact
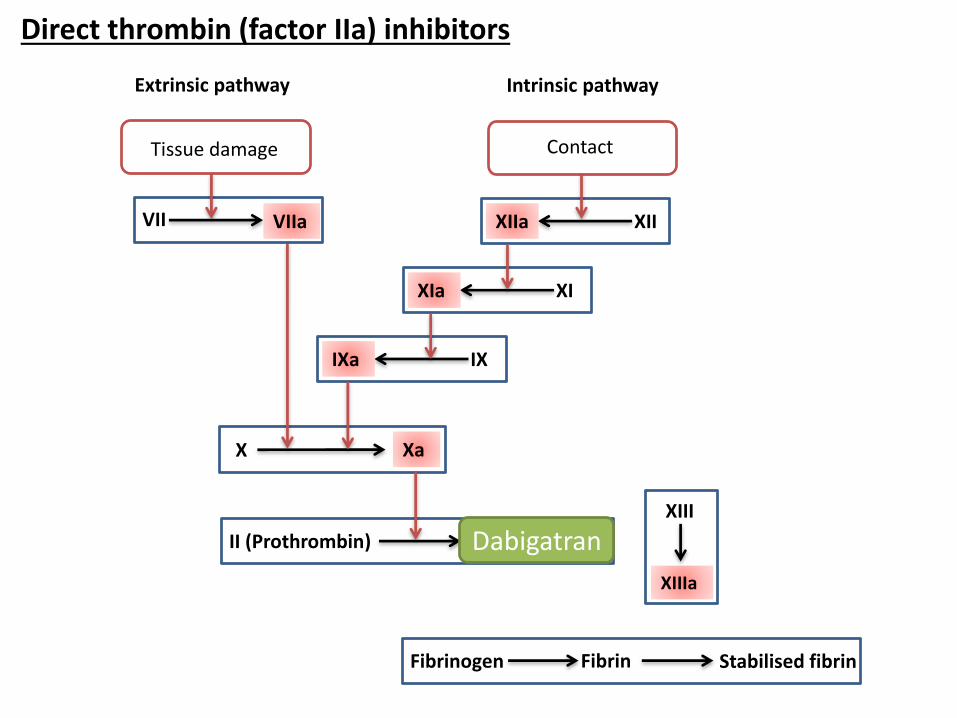
XIIXIIa
XIXIa
X Xa
IXIXa
II (Prothrombin) IIa (Thrombin)
Fibrinogen Fibrin Stabilised fibrin
XIIIa
XIII
Tissue damage
Extrinsic pathway Intrinsic pathway
VII VIIa
Contact
Dabigatran
Direct thrombin (factor IIa) inhibitors
Drugs and blood clotting
Lesson outline
1. Disorders of inappropriate blood clotting (thrombosis)
2. Drugs developed to prevent and/or reverse thrombus formation:
- Anticoagulants
- Antiplatelet agents
- Thrombolytic agents
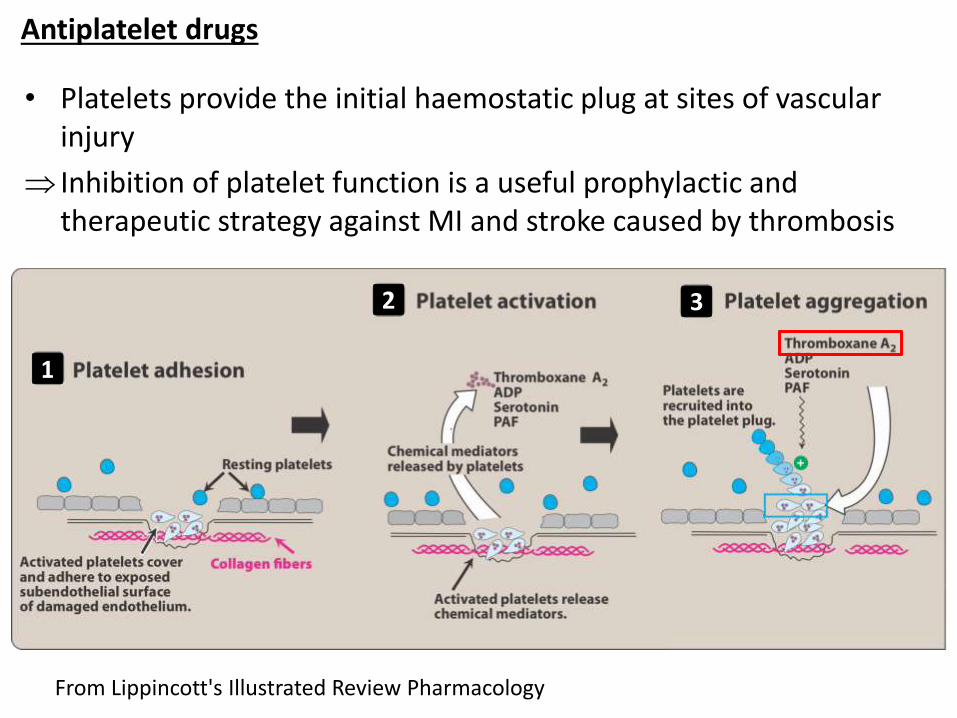
Antiplatelet drugs
• Platelets provide the initial haemostatic plug at sites of vascular injury
Inhibition of platelet function is a useful prophylactic and therapeutic strategy against MI and stroke caused by thrombosis
1
2 3
From Lippincott's Illustrated Review Pharmacology
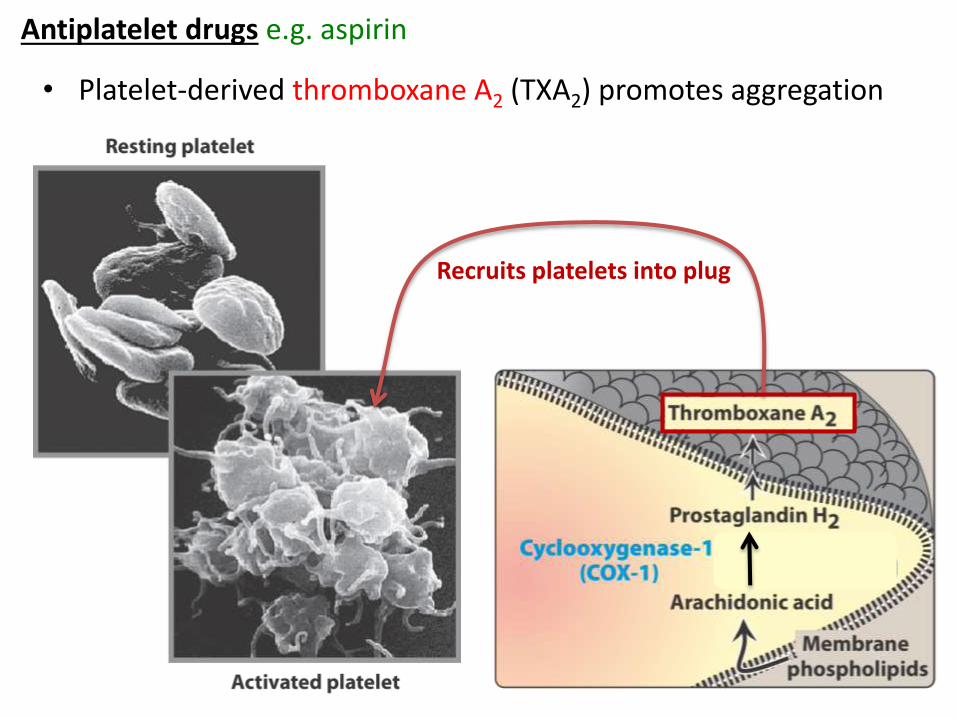
Recruits platelets into plug
Antiplatelet drugs e.g. aspirin
• Platelet-derived thromboxane A2 (TXA2) promotes aggregation
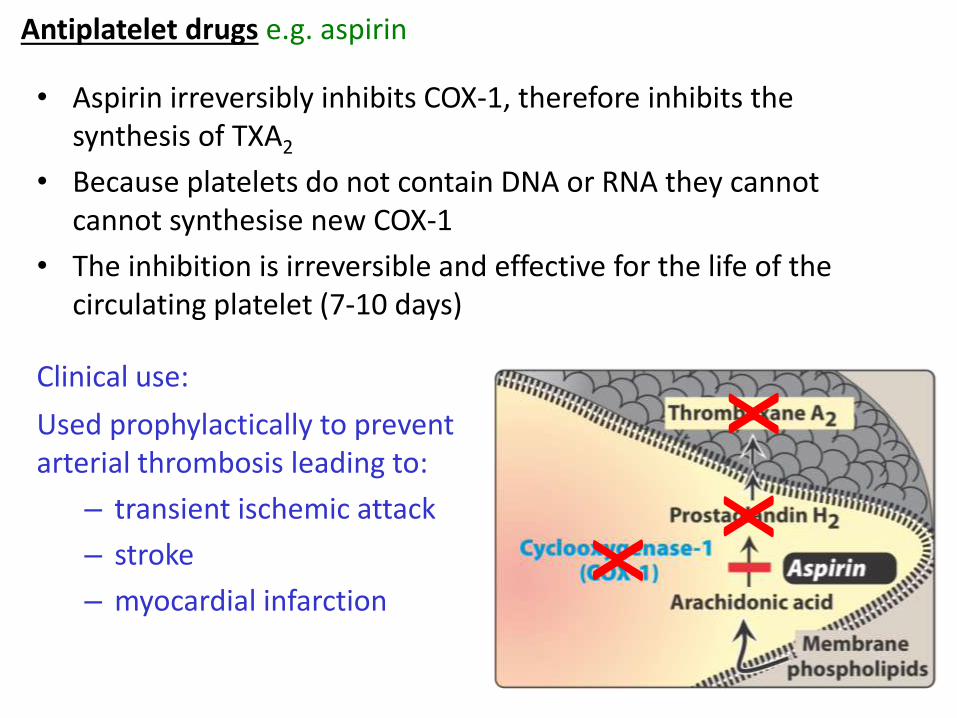
Antiplatelet drugs e.g. aspirin
• Aspirin irreversibly inhibits COX-1, therefore inhibits the synthesis of TXA2
• Because platelets do not contain DNA or RNA they cannot cannot synthesise new COX-1
• The inhibition is irreversible and effective for the life of the circulating platelet (7-10 days)
Clinical use:
Used prophylactically to prevent arterial thrombosis leading to:
– transient ischemic attack
– stroke
– myocardial infarction
xx
x
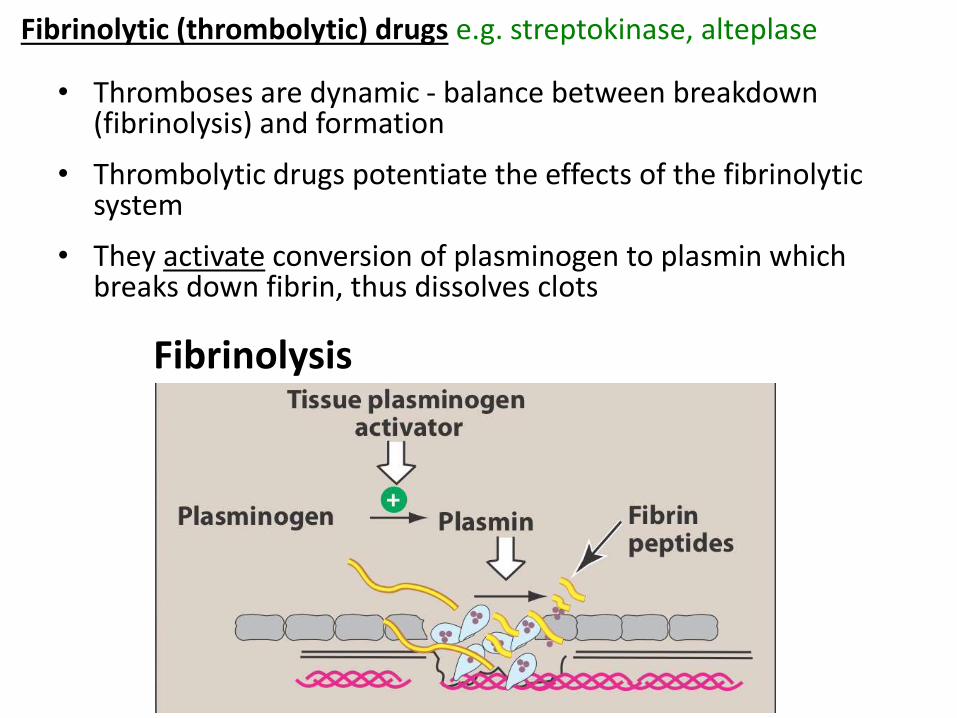
• Thromboses are dynamic - balance between breakdown (fibrinolysis) and formation
• Thrombolytic drugs potentiate the effects of the fibrinolyticsystem
• They activate conversion of plasminogen to plasmin which breaks down fibrin, thus dissolves clots
Fibrinolytic (thrombolytic) drugs e.g. streptokinase, alteplase
Fibrinolysis
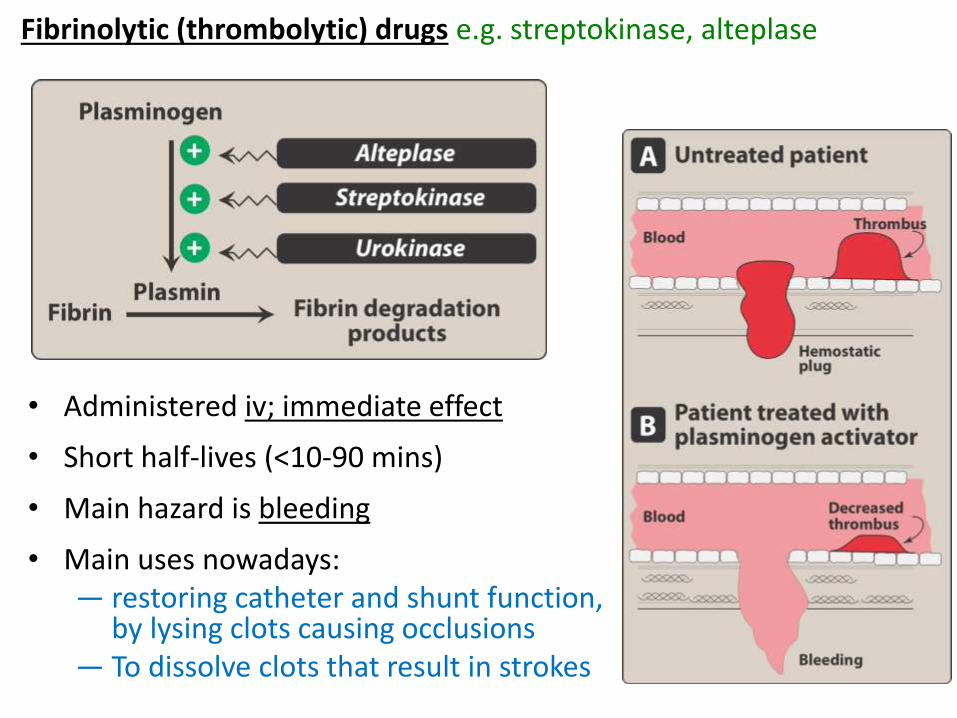
• Administered iv; immediate effect
• Short half-lives (<10-90 mins)
• Main hazard is bleeding
• Main uses nowadays:— restoring catheter and shunt function,
by lysing clots causing occlusions— To dissolve clots that result in strokes
Fibrinolytic (thrombolytic) drugs e.g. streptokinase, alteplase
Key points
Think back through the presentation and write some of the key points you have learned in your own words
• …
• …
• …
• …
Key points
• Heparin works by activating antithrombin III, a naturally occurring inhibitor of clotting factors
• Warfarin works by inhibiting vitamin K reductase
• Heparin is immediately effective, warfarin can take 1-2 days to be effective
• Heparin must be administered parenterally, warfarin orally
• Thrombolytic agents stimulate fibrinolysis by activating conversion of plasminogen to plasmin (which breaks down fibrin)
• Aspirin inhibits COX mediated production of TXA2 , inhibitingTXA2 mediated platelet aggregation
Recommended reading
Rang, Dale, Ritter and Flower. Pharmacology. Relevant sections within the chapter ‘Haemostasis and thrombosis’.
Golan et al. Principles of Pharmacology. Relevant sections within the chapter ‘Pharmacology of Haemostasis and Thrombosis’.
Additional images come from Lippincott's Illustrated Review Pharmacology