Embed Size (px)
DESCRIPTION
Like it soon...!!
Citation preview

EMPYEMAPyothorax / Purulent Pleuritis / Empyema Thoracis
Prepared By:Sharmin Susiwala

Definition:“ Pleural empyema (also known as
a pyothorax or purulent pleuritis) is an accumulation of pus in the pleural cavity. ”
Empyema itself is not disease it is actually a condition complicated by another disease

Etiology:o 2ndry to Bacterial Pneumonia Parapneumonic
effusion (non-infected Pleural Effusion) infected (complicated) paraneumonic effusion Empyema.
o Other causes include:-o Empyema thoracis can be caused by a number of
different organisms, including bacteria, fungi, and amoebas, in connection with pneumonia.
o Common cause is pulmonary infection as a result of aerobic bacteria such as Streptococcus pneumonia, Staphylococcus aureus, E. coli, Klebsiella pneumoniae, Hoemophilus influenzae.
o Chest trauma(blunt chest wound, chest surgery, lung abscess, or a ruptured esophagus)
o Septicaemia (very rare blood borne infection) o Subdiaphragmatic causes as liver abscess

o Iatrogenic: In rare cases, empyema can occur after a needle is inserted through the chest wall to draw off fluid in the pleural space for medical diagnosis or treatment (thoracentesis).

Stages: There are three stages:
1. Exudative (Acute)
2. Fibrinopurulent(Transitional)
3. Organizing(Chronic)
Stage -1: “Exudative”- Sterile pleural fluid develops secondary to inflammation
without fusion of the pleura; swelling of pleural membranes- Approximately in 7 days.
Stage- 2: “Fibrinopurulent”- Thick,Opaque fluid with positive culture (pus) - Deposition of thin fibrin layer over the pleura.- Progressive loculation and formation of pouches in the
pleura.- From 7 day to 21 days.

Stage-3 : “Organizing”- scarring of the pleural space may lead to lung
entrapment - Presence of very thick pus- after 21 days

Clinical Features:
Symptoms of pleural empyema may vary in severity. Typical symptoms include: Chest pain, which worsens when you breathe in
deeply (pleurisy) Dry cough Excessive sweating, especially night sweats Fever and chills General discomfort, uneasiness, or ill feeling
(malaise) Shortness of breath

Weight loss (unintentional) Clubbing may be present in cases of a chronic nature. There is a dull percussion note and reduced breath
sounds on the affected side of the chest. In severe cases, the patient may become dehydrated,
cough up blood, greenish–brown sputum, or run a fever as high as 105F, or even fall into a coma

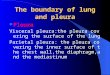
Diagnosis: Chest X-ray. C-T scan. Thoracentesis Pleural fluid Gram stain and culture

On chest X-ray, empyema thoracis will appear as a cloudy or opaque area.

Diagnosis is confirmed by thoracentesis Thoracentesis : This is a procedure which involves the insertion of a needle into the
pleural cavity through the back between the ribs on the infected side, and a sample of fluid is withdrawn
It is performed under local anesthetics If the patient has empyema, there will be leukocytosis, a high level
of protein, and a very low level of blood sugar.

This is the most useful test that conducts analysis of aspirated pleural fluid which shows:
transudative effusions: lactate dehydrogenase (LD) levels less than 200 IU and protein levels less than 3 g/dl
exudative effusions: ratio of protein in pleural fluid to serum greater than or equal to 0.5, LD in pleural fluid greater than or equal to 200 IU, and ratio of LD in pleural fluid to LD in serum greater than or equal to 0.6
empyema: acute inflammatory white blood cells and microorganisms
empyema or rheumatoid arthritis: extremely decreased pleural fluid glucose levels.

Management: Effective management require:
1. Control of infection and sepsis by antibiotics.
2. Evacuation of pus from pleural space.
3. Obliteration of the empyema cavity. Delay in drainage increase mortality from 3.4% to
16%. Empyema is treated using a combination of
medications and surgical techniques Early-course: aspiration, Abx, and sometimes
fibrinolytic therapy.
Late-course: continuous drainage or surgical debridement & decortication.

Antibiotic therapy: Dependent on identification of causative organism Appropriate therapy requires isolation of organism
from blood, pleural fluid or sputum Empiric therapy should be based on local epidemiology and should cover S. pneumonia, S. pyogenes and S. aureus
Treatment with medication involves intravenously administering a two-week course of antibiotics.
It is important to give antibiotics as soon as possible to prevent first-stage empyema from processing to its later stage.
The antibiotics most commonly used are penicillin and vancomycin

Drainage of Empyema First step in treating acute empyema Performed under general anesthesia Done for the dependent rib Open all the intact cyst that leads to conversion of
empyema with free pus Then place intercostal tube for drainage and close
the wound Antibiotics should continue for 6 weeks Includes:
Intercostal tube thoracostomy.Intrapleural instillation of streptokinase .V.A.T.S.Rib Resection Drainage.Eloesser Flap

Rib Resection Drainage;• Performed under general anesthesia • when the pus is thick and loculated • Open all the intact cyst that leads to conversion of empyema
with free pus • Then place intercostal tube for drainage and close the
wound • Antibiotics should continue for 6 weeks Chest Tube
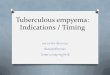
Fibrinolytic Therapy : Studies used Streptokinase or Urokinase Most effective in the early fibrinopurulent stage and
may make surgical drainage unnecessary Life-threatening complications rare Potential adverse effects includes: Bleeding
Bronchopleural fistula Fibrinolytic Therapy

Rib resection drainage

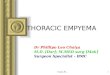
Videoscopic Assisted Thoracoscopy Surgery (VATS) : Minimally invasive Can be used at any stage Advantages includes: Allowance of direct visualization of pleura
and lung Optimal placement of chest tube Fibrinolysis & decortication can be performed. Retrospective case reviews suggest children with failure of
conventional CT therapy exhibit improvement after VATS especially if performed early Videoscopic Assisted Thoracoscopy Surgery (VATS)
Thoracostomy : Open drainage with pleural peel decortication Excision of the thick fibrous pleural rind and removal of
infectious material Longer & complicated procedure Reserved for late presenting empyema with significant fibrous
pleural rind, complex empyema & chronic empyema

Eloesser Flap Drainage

Decortication

Complications: Rupture into the lung;
BronchoPleural fistula Spread to the subcutaneous tissue;
Empyema Niscitanes Septicaemia & septic shock.