Embed Size (px)
Citation preview

Hepatorenal syndrome
Speaker: Dr.S.Ragavendra Preceptors: Dr. Ashutosh Biswas
Dr. Anoop SarayaDr. Sandeep
Mahajan

2
Overview• Historical Perspective
• Definition of Hepatorenal syndrome(HRS)
• Types of HRS
• Natural History
• Pathogenesis
• Prevention
• Management
• Conclusion

Historical Perspective… Association between kidney dysfunction and liver diseases-
Frerichs (1877). Observed oliguria with ascites
Absence of urinary protein and low urinary sodium excretion- Hecker and Sherlock (1956)
Functional nature- Koppel et al (1960). Done kidney Tx from HRS patients
Recovered renal dysfunction after liver Tx- Iwasuki et al (1970)
Later, Schroeder et al - renal vasoconstriction in HRS

4
Hepatorenal syndrome (HRS)
International ascites club defined HRS as a syndrome that occurs in patients with cirrhosis, portal hypertension and advanced liver failure, characterized by impaired renal function with marked abnormalities in the arterial circulation and activity of endogenous vasoactive systems
Is a functional disorder
Kidneys - histologically normal
Arroyo V et al, Hepatology 1996;23:164e76

5
International ascites club (IAC) diagnostic criteria
Major Criteria:o Chronic or acute liver disease with advanced hepatic failure and
portal hypertensiono Low GFR ~ S.cr >1.5mg/dl or 24 hr creatinine clearance <40ml/mino Absence of shock, ongoing bacterial infections, and current or
recent Rx with nephrotoxic drugso Absence of GI fluid losseso Absence of renal fluid losses in response to diuretic therapyo No sustained improvement in renal function after diuretic
withdrawal and expansion of plasma volume with 1.5 liters of isotonic saline
o Proteinuria <500mg/day, and no USG e/o obstructive uropathy or parenchymal renal disease
Arroyo et al, Hepatol, 1996

6
International ascites club (IAC) diagnostic criteria
Minor criteriao Urine volume <500ml/dayo Urine sodium <10mmol/Lo Urine osmolality > Plasma osmolalityo Serum Na <130mmol/Lo Urine RBC <50/hpf
Arroyo et al, Hepatol, 1996

New IAC diagnostic criteria 2007
Salerno et al, Gut 2007

8
Rationale for the proposed diagnostic criteria for HRS
Serum creatinine (> 1.5 mg%) to establish reduced GFR – consensus
Volume expansion to exclude pre-renal causes
Volume replacement: saline vs albumin
Shock preceding renal failure – a pointer towards “ATN”
Transient AKI due to sepsis – should resolve with antibiotics
Nephrotoxic drugs – commonly used

9
Stage Migration

10
Rationale for the proposed diagnostic criteria for HRS
Intrinsic renal disease and obstructive uropathy to be ruled out
Urine volume, Urine Na, urine : plasma osmolality
–
o Parameters traditionally used to differentiate
functional renal failure from ATN
o Removed from the revised diagnostic criteria
o Reason: parameters not exclusive for either of
the entities

11
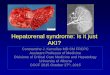
Causes of pseudo hepatorenal syndrome

12
Types of HRS Type-1 HRS:
Rapidly progressive reduction of renal function as defined by
doubling of the initial S.cr to a level >2.5 mg/dL in < 2 wk
o Clinical pattern: acute renal failure
Type-2 HRS:
Moderate renal failure (S.cr ranging from 1.5 to 2.5 mg/dL)
with a steady or slowly progressive course
o Clinical pattern: refractory ascites
Salerno et al, Gut 2007

13
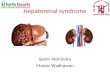
Type 1 vs Type 2 HRS

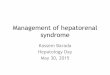
Probability of survival: Type 1 vs Type 2
Alessandria et al, Hepatol 2005

15
Type 3 HRS Recently defined type 85% of end-stage cirrhotics - intrinsic renal
disease on Kidney Bx Allessandria C. Hepatology 2005
Cirrhotics + pre existing renal dysfunction can develop superimposed HRS
Renal histology may be required to accurately diagnose cause of renal failure
May require liver-kid transplant. Never studied in therapeutic trials.

16
Type 4 HRS
> 50 % of ALF develop HRS.
Rarely refractory ascites and PHT
Very poor prognosis esp. if ALF acetaminophen-
related.
Pathophysiology ? similar. Lack of studies.
Moore K; Eur J Gastroentrol Hepatol.1999

17
S.creatinine: prognostic value
MELD o Score based on creatinine, bilirubin, INRo Predicts mortality in patients undergoing TIPSo Organ allocation based on the scoreo Gives an idea about the requirement of RRT post LTo Predicts short term and long term survival in ESLDo Predicts mortality in variceal bleeding, sepsis and
alcoholic hepatitiso Predicts mortality in HCC resection, cardiac and
abdominal surgerieso Refinements - ∆MELD, MELD-Na

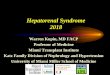
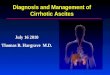
Pathophysiology

Pathogenesis
Gines and Schrier, N Engl J Med, 2009

20
Pathogenesis

Endogenous vasoactive factors
Arch intern med 1993

Peripheral vasodilation hypothesis
Arroyo V et al, J Hepatol 2008

Changes in cardiac output
Ruiz-del-Arbol et al, Hepatol 2005
N = 66 nonazotemic cirrhotic patients
40% developed HRS during the study follow up of 1 year

Modified peripheral vasodilation hypothesis
Arroyo V et al, J Hepatol 2008

Regional hemodynamics
Guevara et al, Hepatol 1998

26
Adrenal dysfunction
Tsai et al, Hepatol 2006

Multiorgan failure & HRS
Arroyo V et al, J Hepatol 2007

28
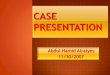
Cirrhosis to HRS: Natural progression
Ramon Planas et al, Clin Gastroenterol Hepatol 2006
DH RA
Type 1 Type 2

Ascites to HRS: Natural progression
Gines et al, Gastroenterol 1993
18%
39%

Prevention

Prevention of HRS SBP: IV albumin administration
Severe acute alcoholic hepatitis: Oral pentoxyphylline
Low protein ascites: Norfloxacin as 1o SBP prophylaxis
Large volume paracentesis: IV albumin to prevent paracentesis induced circulatory dysfunction (PICD)

32
Arroyo V, et al N Engl J Med 1999;341:407

Prevention of HRS SBP: IV albumin administration
Arroyo V, et al N Engl J Med 1999;341:407
Severe acute alcoholic hepatitis: Oral pentoxyphylline
Akriviadis E et alGastroenterology 2000
Low protein ascites: Norfloxacin as 1o SBP prophylaxis
Large volume paracentesis: IV albumin to prevent PICD

Management

Management of HRS Liver transplantation is the only definitive
treatment option
Renal failure at time of transplant has poorer outcomes
Bridge to Liver Transplantation needed

36
Initial Management checklist
Admission to monitored care setting with Vitals montiroing
Central line placement for CVP helpful, not mandatory
Routine blood and urine investigations Abdominal USG Diagnostic paracentesis Discontinue diuretics Plasma expansion with albumin Evaluation for Orthoptic liver transplantation

Pharmacologic therapy

Randomized trials on type 1 or type 2 HRS Treatments compared:
1. Terlipressin (+ albumin) vs no intervention, albumin or NA + albumin
2. Octreotide + albumin vs albumin
3. Terlipressin + albumin given as continuous or bolus infusion

N=376


41
Other drugs Noradrenaline + albumin
o Results similar to terlipressino Cheapero 0.1 mcg/kg/min infusion (max 0.7)
Alessandria et al, J hepatology 2007
Midodrine and octreotideo Oral α adrenergic agonist + long acting s/c somatostatin
analogueo Direct vasoconstrictor + inhibits endogenous vasodilatorso 5 mg tds + 100mcg tds s/co Given along with albumino OPD use. Not studied for Type 2
Angeli p;Hepatology.1999

42
Other drugs Misoprostol
o Synthetic-PGE1o Patients have low urinary levels of vasodilatory
prostaglandinso Evidence poor
Gines;J Hepatol.1993
Renal vasoconstrictor antagonistso Saralasin - Angitensin II receptor antagonist -worsening hypotension, abandoned
o Endothelin antagonists- non specific tezosentan Endothelin A receptor antagonist(BQ123)
Soper CP;Lancet.1996

TIPS(Transjugular intrahepatic portosystemic
shunting) Few studies available (case series)
Decreases portal pressure and consequently reduces renal sympathetic activity
Improvement in renal function and survival noted compared to no treatment (but may take several weeks)
Careful patient selection needed to optimize safety and efficacy
Guevara et al,hepatology 1998;28:416-22

Renal replacement therapy
Paucity of datao Optimal method not knowno Impact on prognosis not knowno No studies in comparison with medical Rx
To be used in patients with an urgent indication of HD and for patients with no response to vasoconstrictor therapy
Available studies:o Keller et al, Ren Fail, 1995 – retrospective analysis, n = 26, better
survivalo Witzke et al, J Gastroenterol Hepatol, 2004 – prospective
observational study, n = 30, RRT not predictive of improved survival

45
Artificial hepatic support
Detoxification treatment ~ form of artificial extracorporeal liver support.
Considered to be a bridge to liver transplantation Liver dialysis devices –
o Molecular Adsorbents Recirculation System
(MARS)
o Single Pass Albumin Dialysis (SPAD)
o Prometheus system

46
Molecular adsorbent recirculating system (MARS)
Most frequently used albumin dialysis system
Dialysate recirculated and perfused online through charcoal and anion exchanger columns
Improve systemic hemodynamics and renal perfusion.
Better than HD for sodium,creatinine, bilirubin and PT

47
MARS

Liver transplantation
Treats the causative organ dysfunction
1 yr survival rate: not on HD – 78.8% , on HD – 73.7%
survival with s.cr at similar MELD scores (at 15-17 and 24-40)
Similar 2 yr and 5 yr survival among non HRS and HRS LT
Beneficial outcomes with renal protective immunosuppression
Schmitt et al, Transpl Int 2009
Sharma et al, Liver Transpl 2009
Jeyarajah et al, Transplantation 1997
Lopez Lago et al, Transplant Proc 2007


Liver-Kidney transplantation
Usual norms:o Preoperative HRS/ ATN usually don’t need KTPo Many times 1o renal disease can be managed
medically
Factors contributing to renal failure:o Improved medical management leading to
better survivalo Long waiting time for transplanto Post-LT calcineurin inhibitors

Liver-Kidney transplantation
Issues to be addressed pre-LT:o Will the ARF reverse?o Is there a way to predict who will recover?o What is the acceptable degree of recovery?
Patients of HRS who required prolonged HD (> 4 - 8 wks) may require KLT and better outcomes have been reported
Ruiz et al, Arch Surg 2006

Liver-Kidney transplantation
Tanriover et al, Transplantation 2008

53
Summary

54
Conclusion
Prevention is utmost important
Low threshold to diagnose and investigate renal failure in presence of liver dysfunction.
Early diagnosis and timely therapeutics can increase life expectancy for HRS patients while these are waiting for liver transplantation as a definitive treatment.

55
THANK YOU

56
Ques to be answered Definitions.. Fluid therapy Cvp based? Do pts develop structural changes? Therapy lacunae?

SummaryDecompensated cirrhosis with renal failure
Rule out pre-renal causes: stop diuretics, volume expansion (NS or albumin), CVP measurement
Rule out intrinsic and obstructive renal disease: urine analysis, USG KUB, check out nephrotoxic drugs
Surveillance for sepsis, low threshold for antibiotics usage
Medical mx to increase urine output and improvizing KFT, optimization of diuretics and management of refractory ascites,
dialyze as per clinical indication
TIPS/List for LT

Triple therapy vs Terlipressin
Type I (n=23) Type II (n=14)
HRS (n=37)
Terlipressin (n=12)Triple (n=11) Triple (n=10) Terlipressin (n=4)

Terlipressin in Type I HRS
Variable Pre-treatment Post-treatment p-value
Urine output 275.5±184.4 1169.4±790.7 0.02
S Creatinine 2.9±1.0 2.6±1.9 0.3
Blood urea 118.7±38.8 118.8±88.1 0.9
Urine sodium 21.7±12.9 72.3±36.7 0.02
Albumin 2.7±0.6 2.8±0.5 0.4

Triple therapy in Type I HRS
Variable Pre-treatment Post-treatment p-value
Urine output 335.0±247.3 1061.0±645.8 0.02
S Creatinine 3.7±1.7 3.2±3.1 0.4
Blood urea 137.9±45.8 138.4±71.8 0.1
Urine sodium 26.9±22.3 53.8±23.1 0.01
Albumin 2.3±0.6 2.7±0.7 0.06

Terlipressin in Type II HRS
Variable Pre-treatment Post-treatment p-value
Urine output 495.0±313.1 (200-1000)
1310.0±636.7 (200-2500)
0.01
S Creatinine 2.0±0.3 (1.5-2.5) 1.3±0.7 (0.7-2.7) 0.02
Urine sodium 10.4±9.2 (1-30) 51.3±34.7 (8-126) 0.008

Triple therapy in Type II HRS
Variable Pre-treatment Post-treatment p-value
Urine output 512.5±295.5 (150-800)
1675.0±670.2 (700-2200)
0.06
S Creatinine 2.0±0.4 (1.6-2.4) 1.4±0.7 (0.8-2.4) 0.1
Urine sodium 11.7±12.1 (1-29) 103.5±36.1 (78-129) 0.1

HRS-I: terlipressin vs triple therapy
Variable p-value
Increase in urine output 0.5
Decrease in S. creatinine 0.3
Increase in 24 hour urine sodium
0.3

Variable p-value
Increase in urine output 0.4
Decrease in S. creatinine 0.8
Increase in 24 hour urine sodium
0.1
HRS-II: terlipressin vs triple therapy