Embed Size (px)
Citation preview
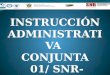
IAC 360°15-12-2015
12.43pm
Great teachers – All this is their work . I am just the reader of their books .
Prof. Paolo castelnuovo
Prof. Aldo Stamm Prof. Mario Sanna
Prof. Magnan

For Other powerpoint presentatioins of “ Skull base 360° ”
I will update continuosly with date tag at the end as I am getting more & more information
click
www.skullbase360.in - you have to login to slideshare.net with Facebook account for downloading.
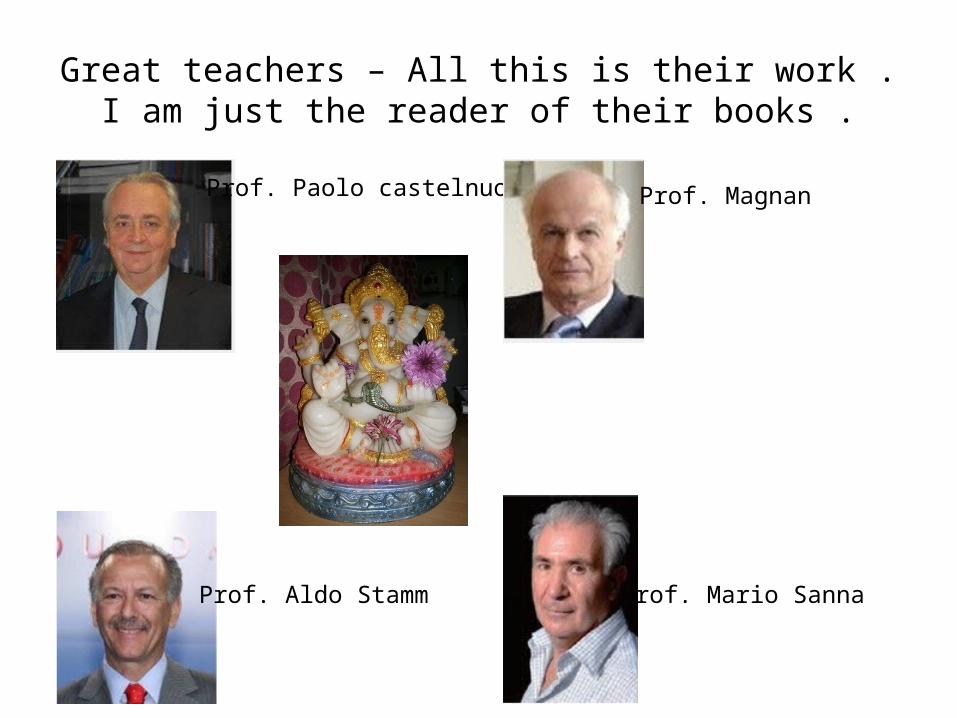
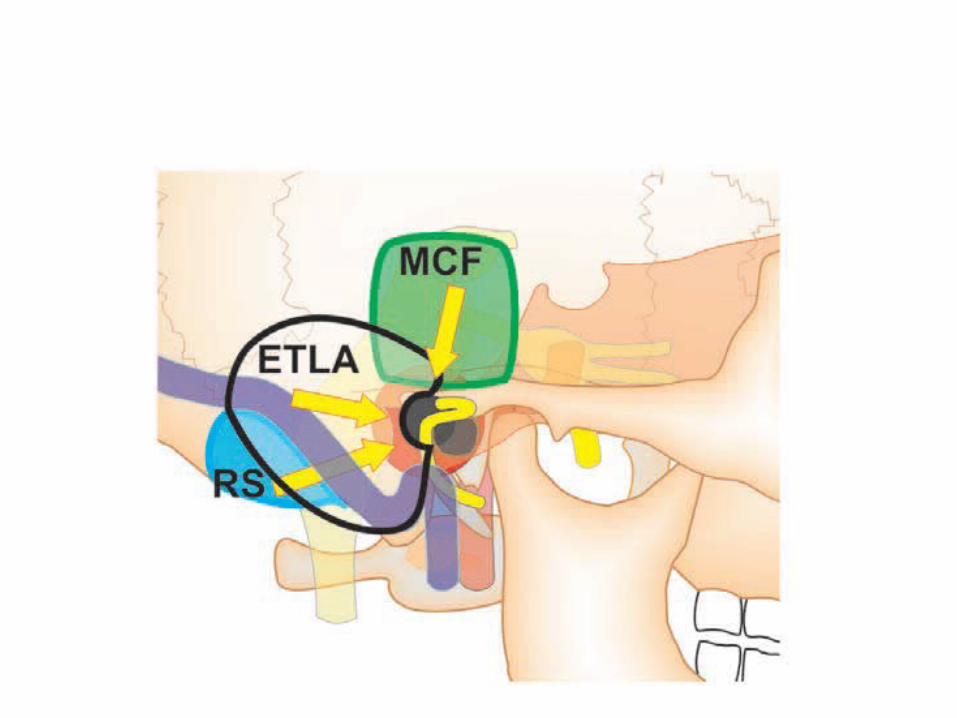
Bottle neck concept – junction of labyrinthine & internal auditory canal facial nerve is narrow [ bottle neck ]
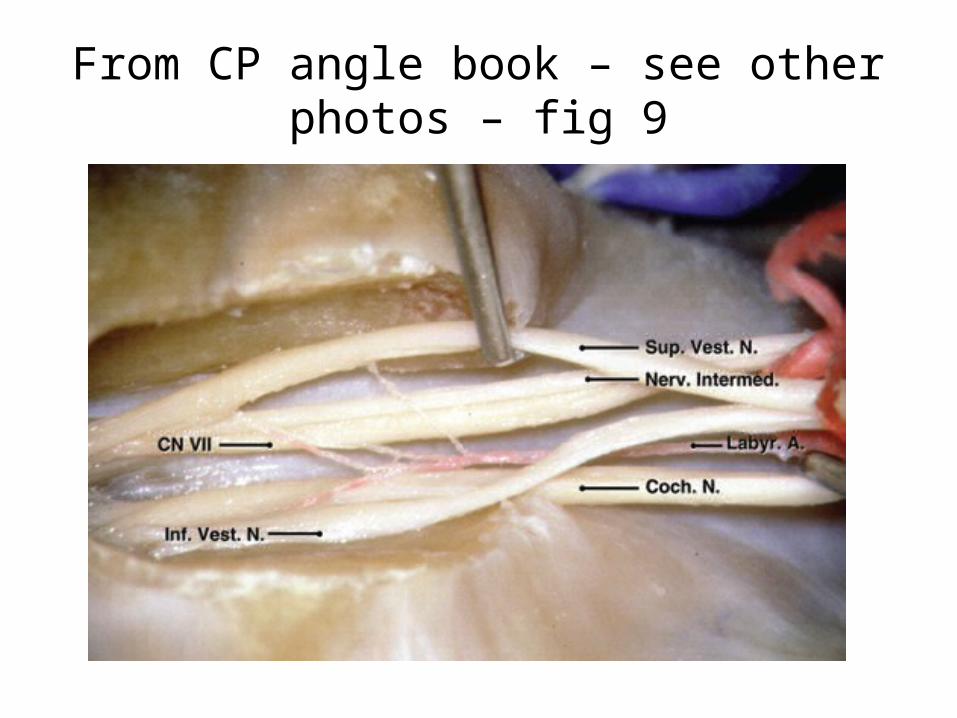
From CP angle book – see other photos – fig 9
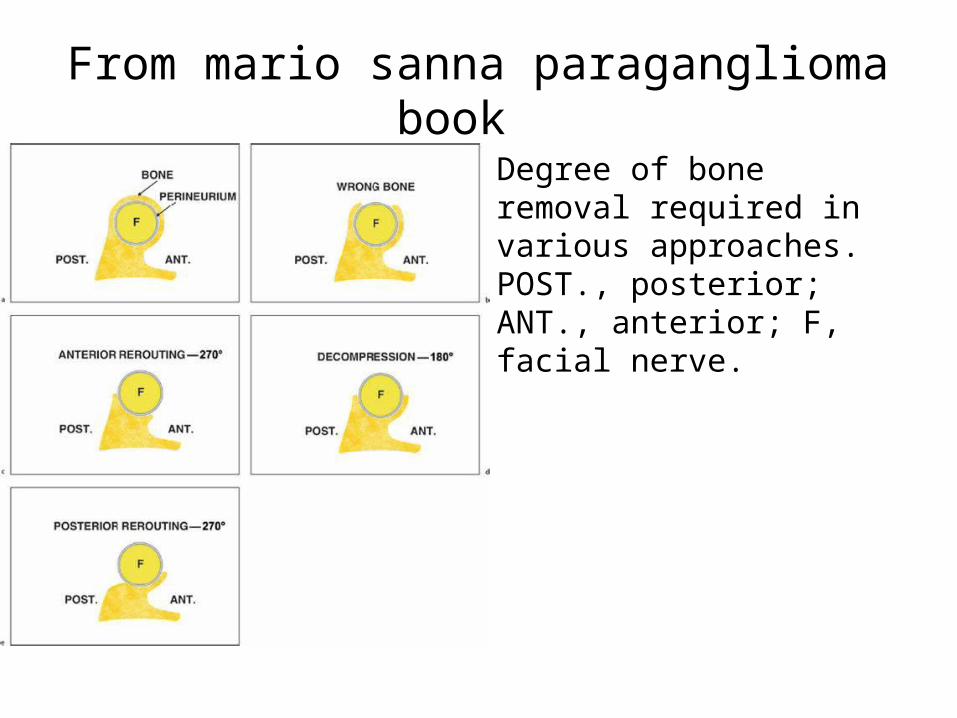
From mario sanna paraganglioma book Degree of bone removal required in various approaches. POST., posterior; ANT., anterior; F, facial nerve.
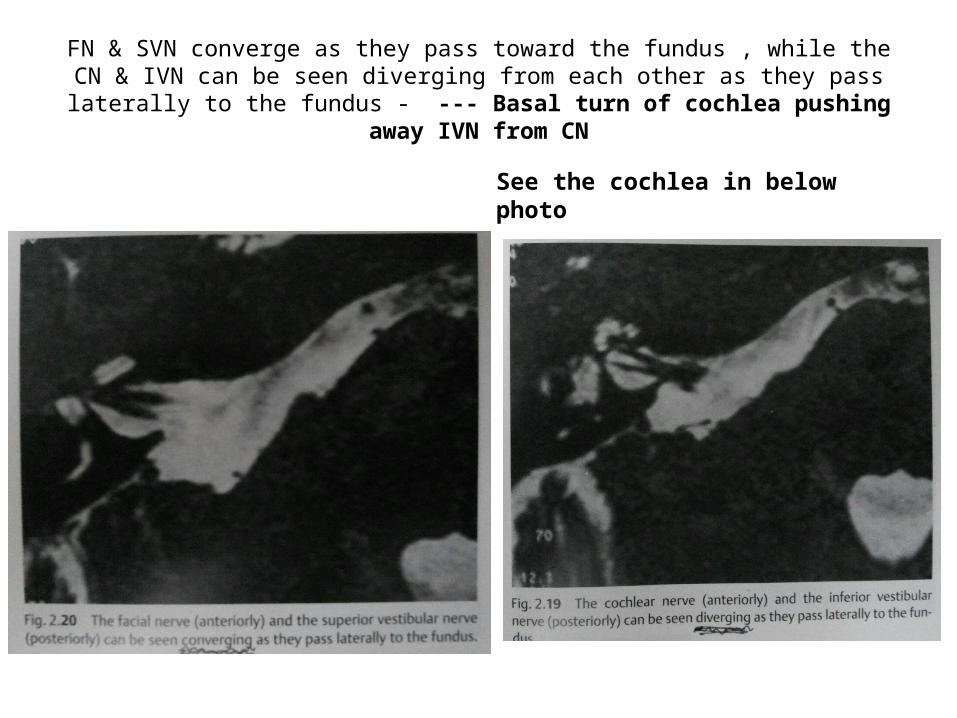
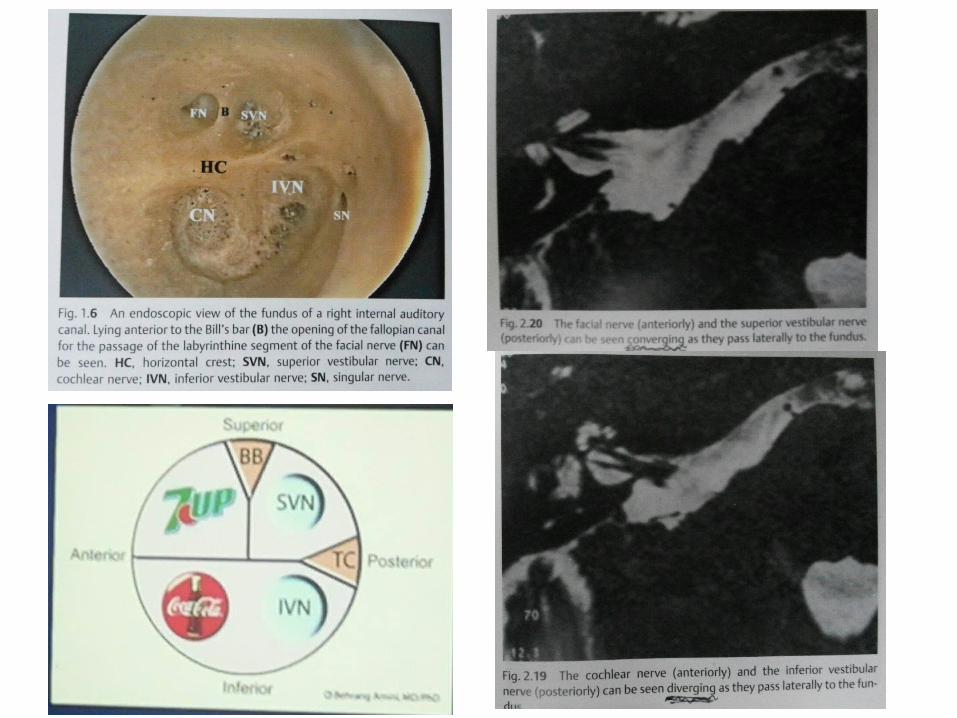
FN & SVN converge as they pass toward the fundus , while the CN & IVN can be seen diverging from each other as they pass laterally to the fundus - ---
Basal turn of cochlea pushing away IVN from CN
See the cochlea in below photo
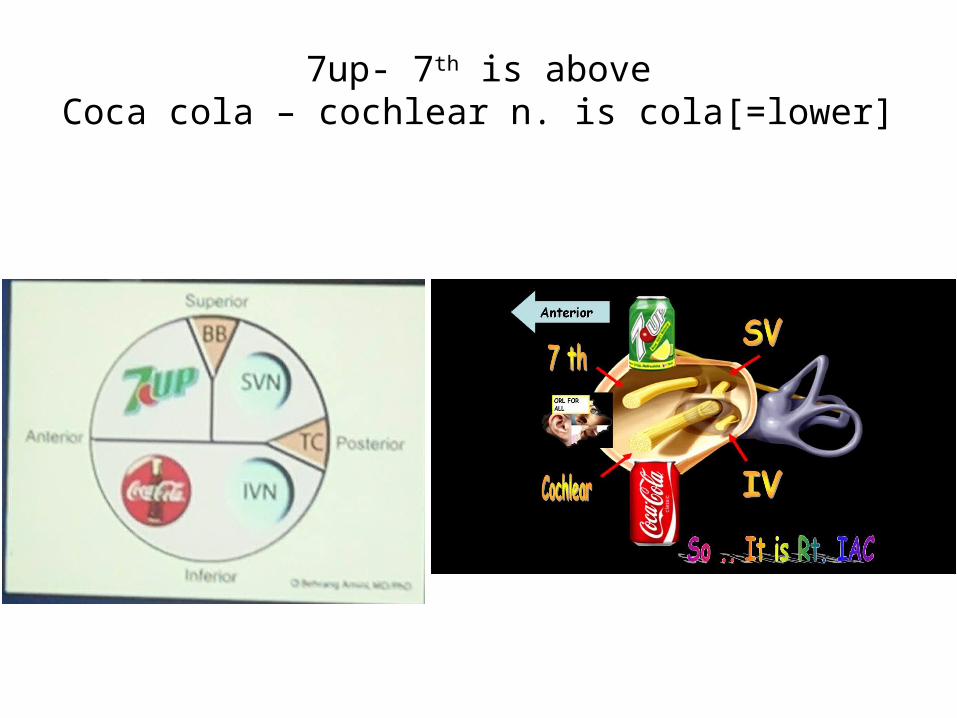
7up- 7th is aboveCoca cola – cochlear n. is cola[=lower]
Translabyrinthine Transpetrous ( = Transapical )
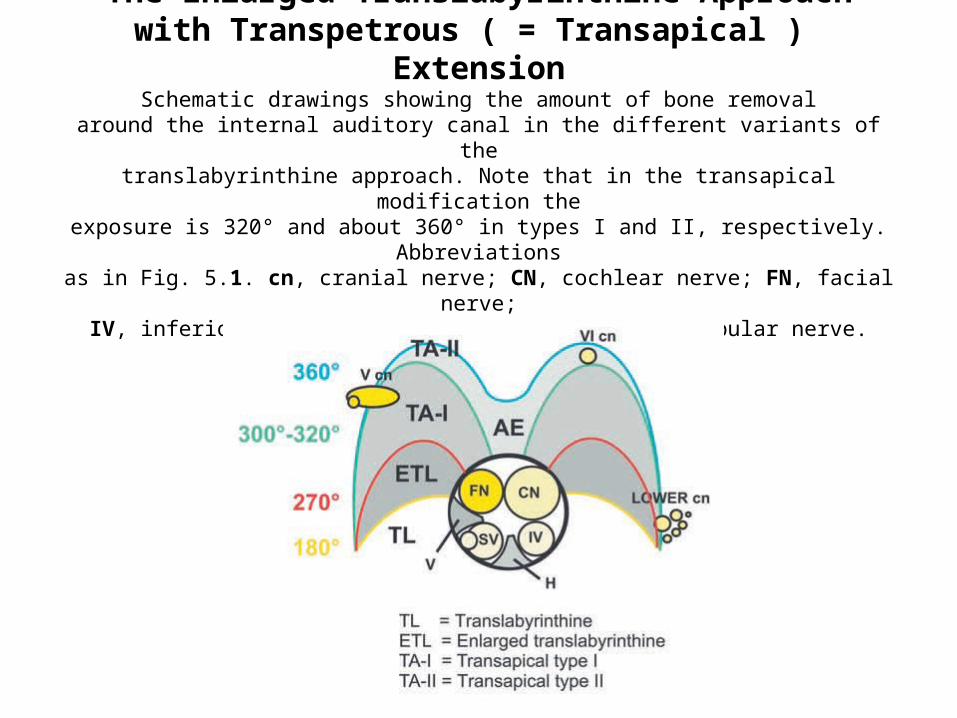
The Enlarged Translabyrinthine Approach with Transpetrous ( = Transapical ) Extension
Schematic drawings showing the amount of bone removalaround the internal auditory canal in the different variants of the
translabyrinthine approach. Note that in the transapical modification theexposure is 320° and about 360° in types I and II, respectively. Abbreviations
as in Fig. 5.1. cn, cranial nerve; CN, cochlear nerve; FN, facial nerve;IV, inferior vestibular nerve; SV, superior vestibular nerve.
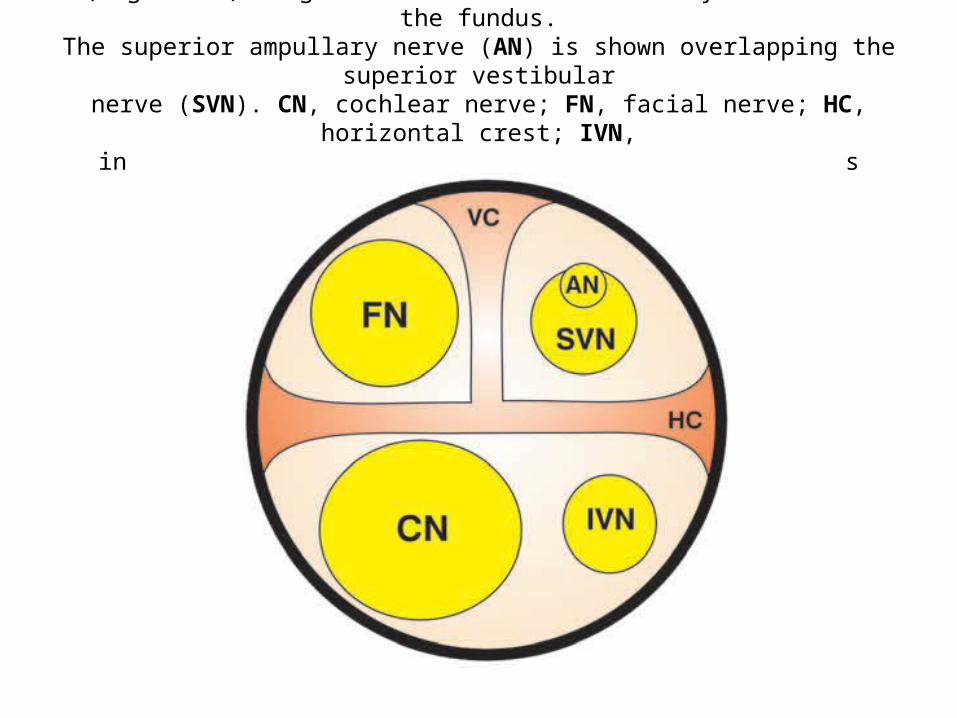
(Right ear) Diagram of the internal auditory canal near the fundus.The superior ampullary nerve (AN) is shown overlapping the superior vestibular
nerve (SVN). CN, cochlear nerve; FN, facial nerve; HC, horizontal crest; IVN,inferior vestibular nerve; VC, vertical crest (Bill’s bar).
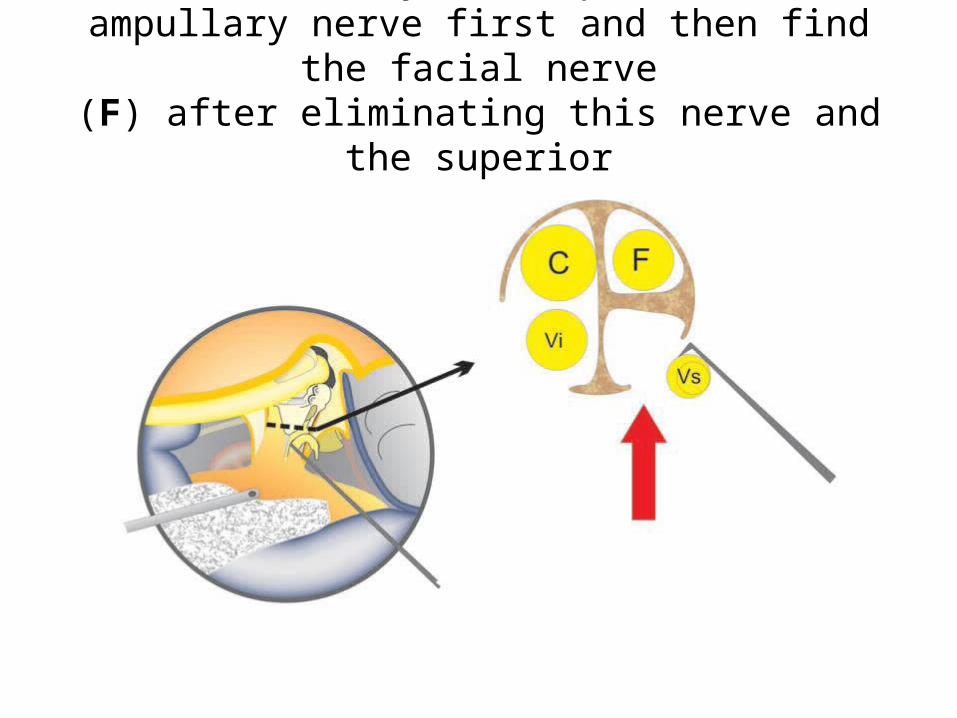
identify the superiorampullary nerve first and then find the facial nerve
(F) after eliminating this nerve and the superiorvestibular nerve (Vs).
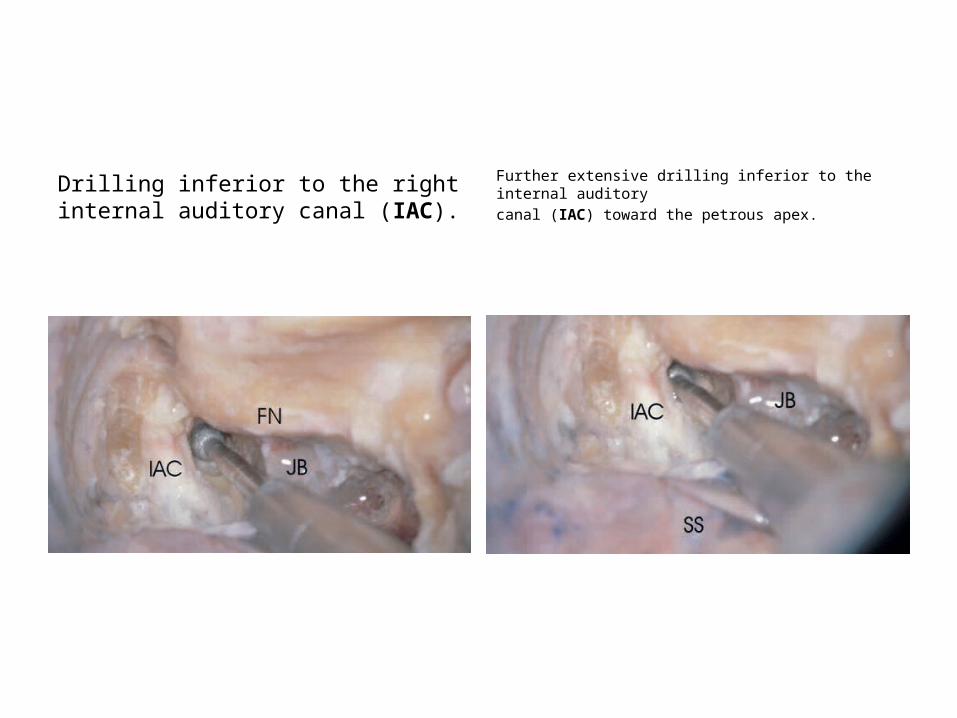
Drilling inferior to the right internal auditory canal (IAC).
Further extensive drilling inferior to the internal auditory canal (IAC) toward the petrous apex.
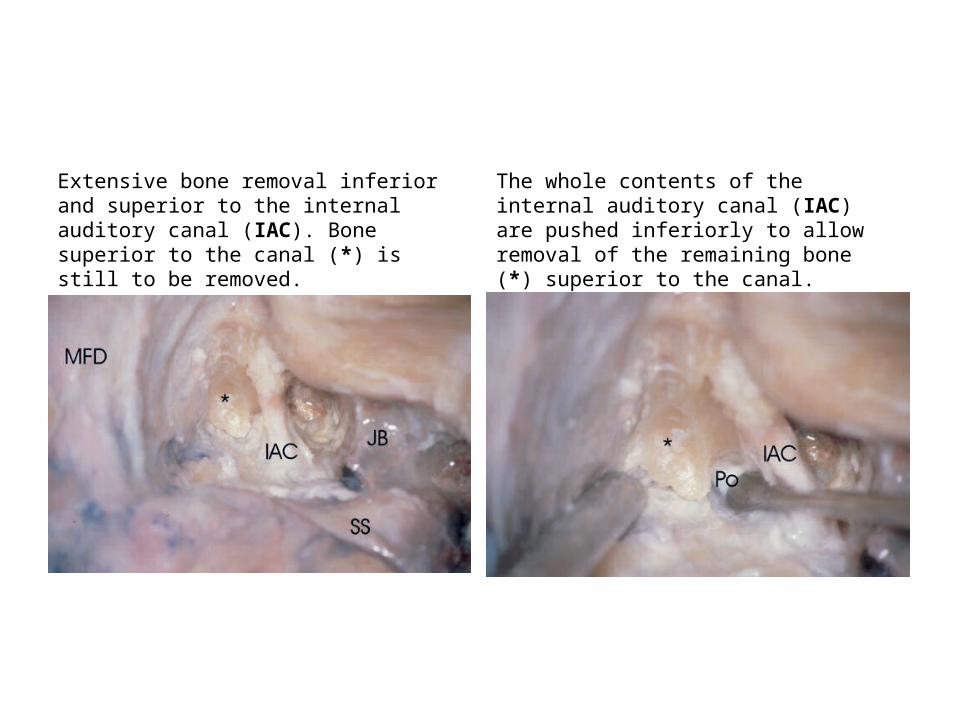
Extensive bone removal inferior and superior to the internal auditory canal (IAC). Bone superior to the canal (*) is still to be removed.
The whole contents of the internal auditory canal (IAC) are pushed inferiorly to allow removal of the remaining bone (*) superior to the canal.
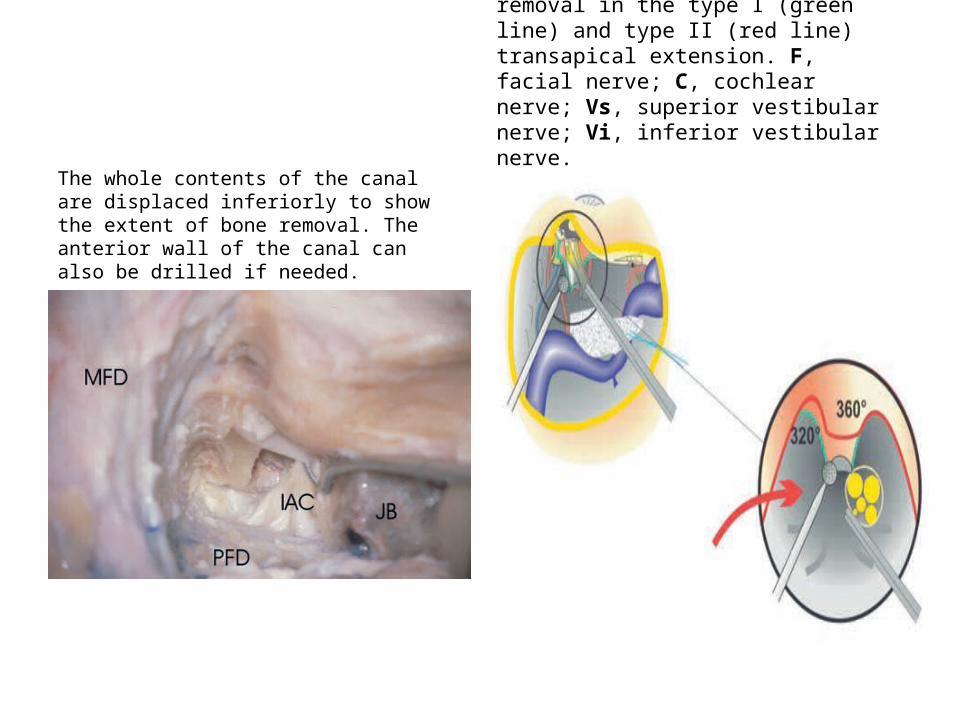
The whole contents of the canal are displaced inferiorly to show the extent of bone removal. The anterior wall of the canal can also be drilled if needed.
Schematic drawing showing the technique and extent of bone removal in the type I (green line) and type II (red line) transapical extension. F, facial nerve; C, cochlear nerve; Vs, superior vestibular nerve; Vi, inferior vestibular nerve.
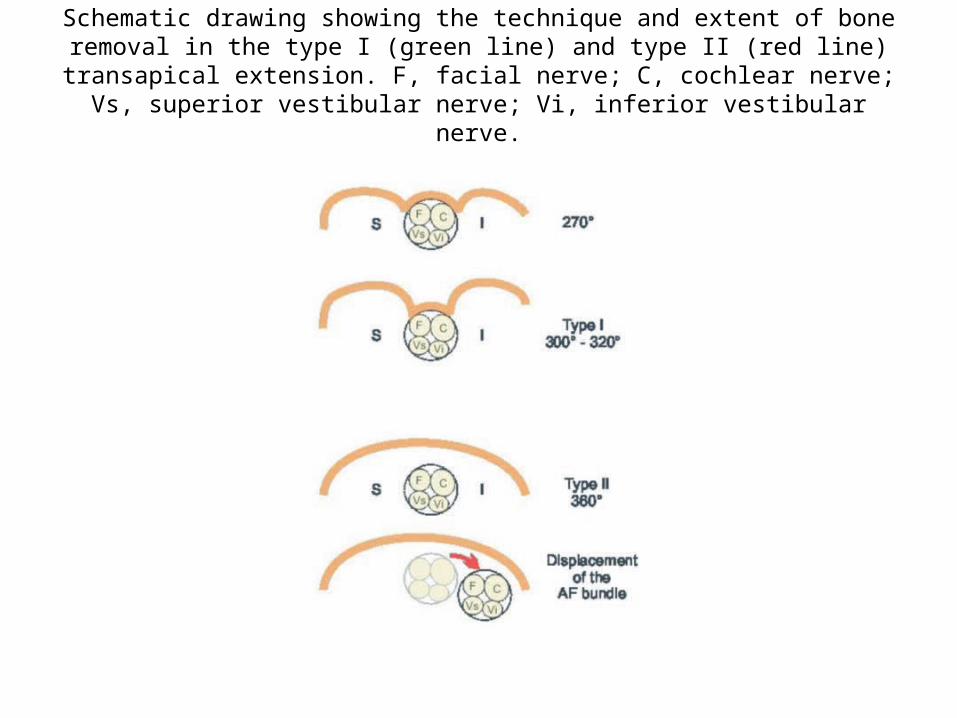
Schematic drawing showing the technique and extent of bone removal in the type I (green line) and type II (red line) transapical extension. F, facial nerve; C, cochlear
nerve; Vs, superior vestibular nerve; Vi, inferior vestibular nerve.
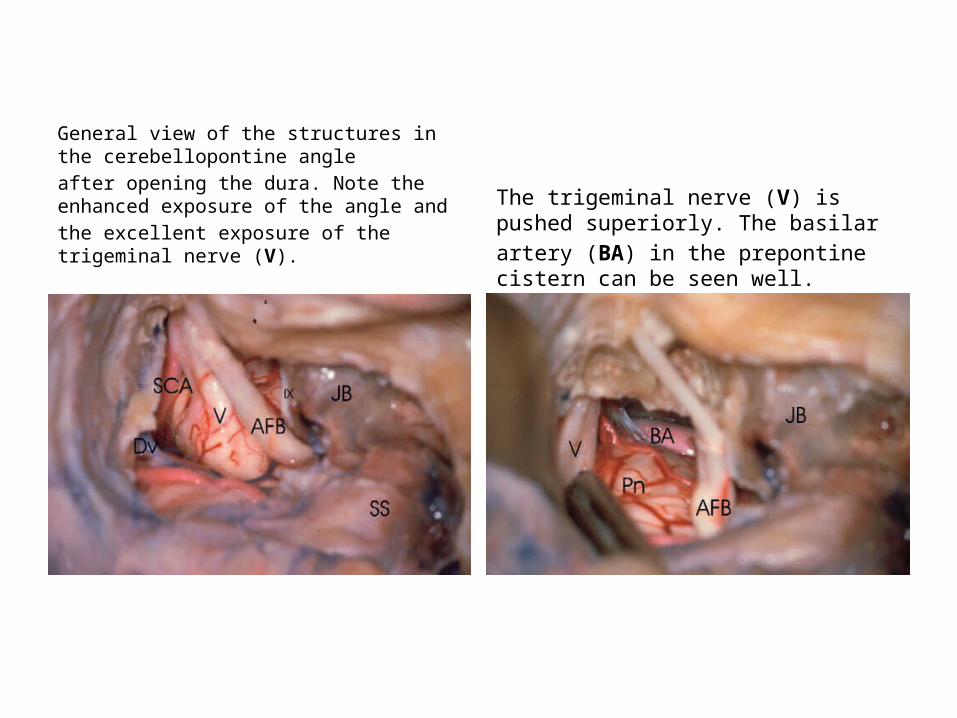
General view of the structures in the cerebellopontine angleafter opening the dura. Note the enhanced exposure of the angle andthe excellent exposure of the trigeminal nerve (V).
The trigeminal nerve (V) is pushed superiorly. The basilarartery (BA) in the prepontine cistern can be seen well.
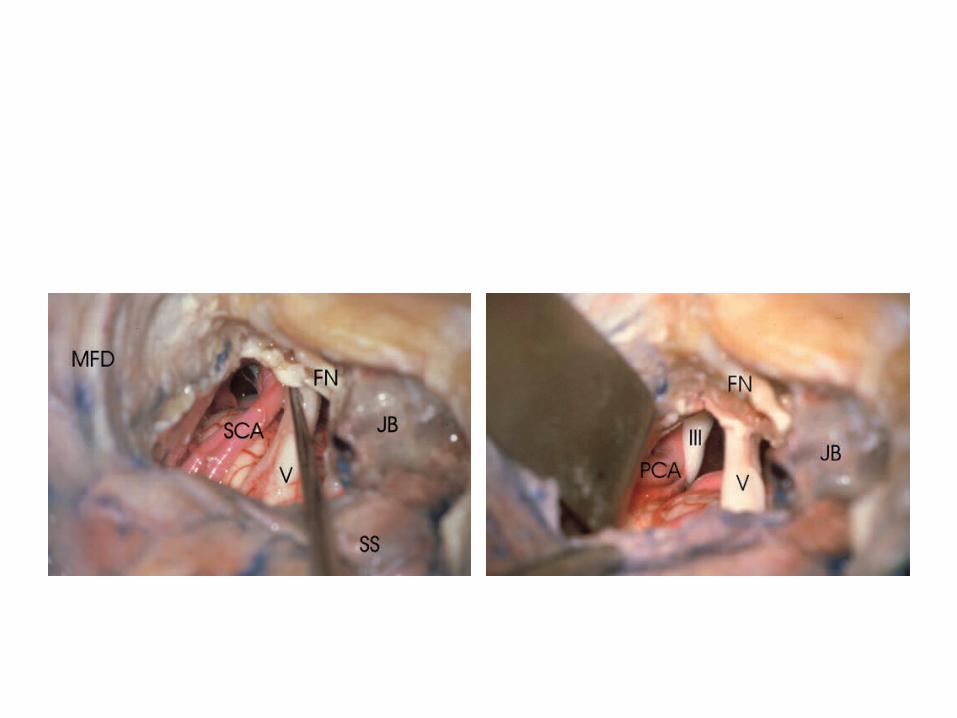
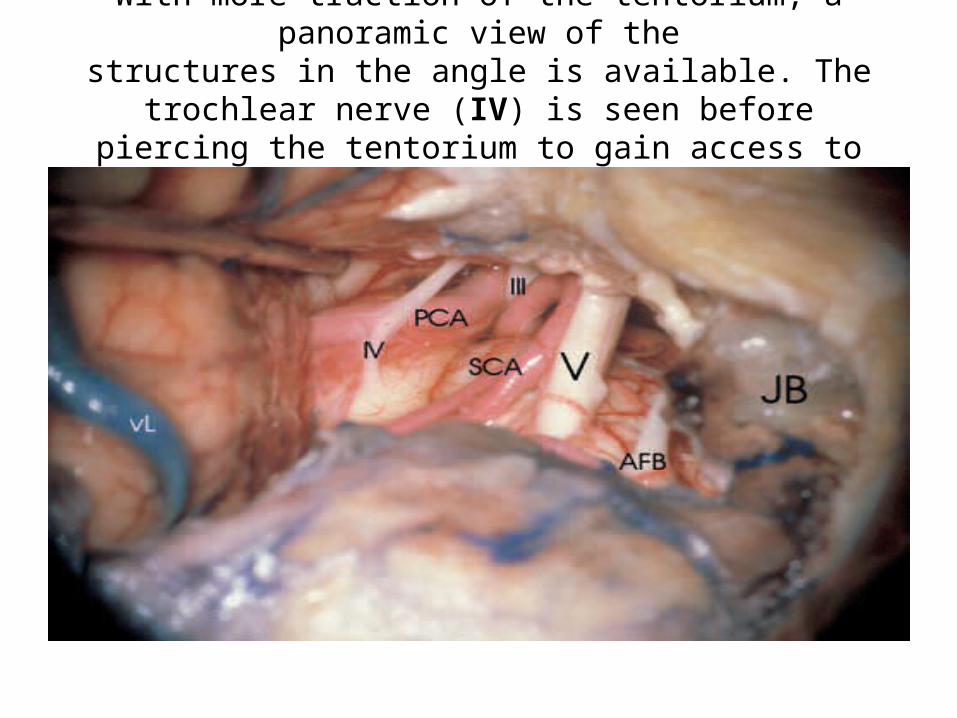
With more traction of the tentorium, a panoramic view of thestructures in the angle is available. The trochlear nerve (IV) is
seen before piercing the tentorium to gain access to the middle fossa.
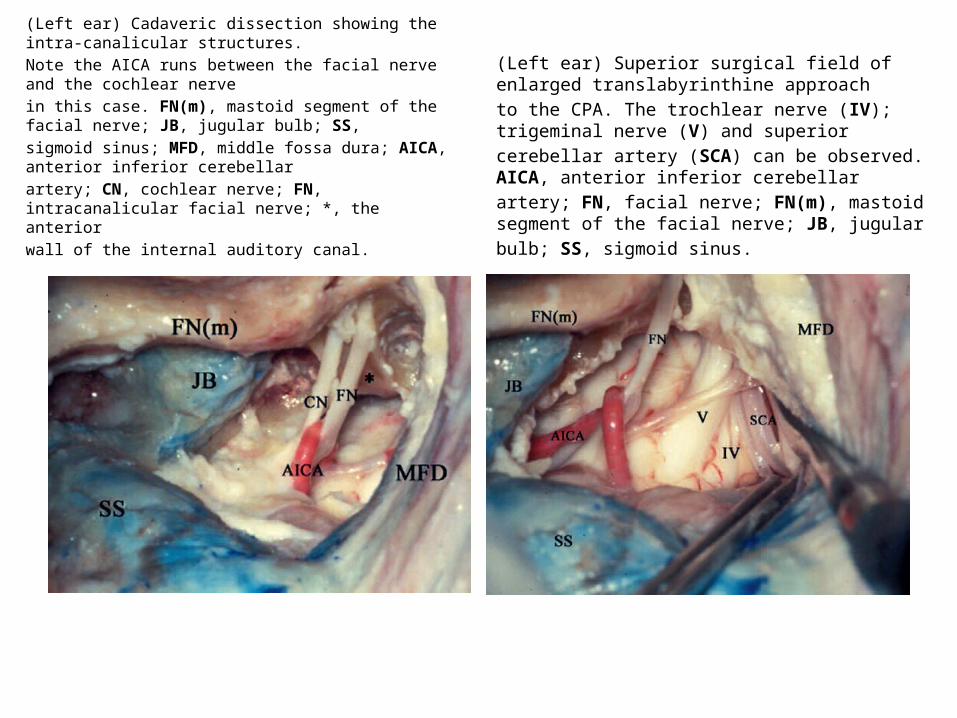
(Left ear) Cadaveric dissection showing the intra-canalicular structures.Note the AICA runs between the facial nerve and the cochlear nervein this case. FN(m), mastoid segment of the facial nerve; JB, jugular bulb; SS,sigmoid sinus; MFD, middle fossa dura; AICA, anterior inferior cerebellarartery; CN, cochlear nerve; FN, intracanalicular facial nerve; *, the anteriorwall of the internal auditory canal.
(Left ear) Superior surgical field of enlarged translabyrinthine approachto the CPA. The trochlear nerve (IV); trigeminal nerve (V) and superiorcerebellar artery (SCA) can be observed. AICA, anterior inferior cerebellarartery; FN, facial nerve; FN(m), mastoid segment of the facial nerve; JB, jugularbulb; SS, sigmoid sinus.
Mohnish grover Cochlear implant radiology lines
Middle cranial fossa approach


For Other powerpoint presentatioins of “ Skull base 360° ”
I will update continuosly with date tag at the end as I am getting more & more information
click
www.skullbase360.in - you have to login to slideshare.net with Facebook account for downloading.