Embed Size (px)
Citation preview
Presented By: Rohin Sharma
(PhD Scholar)
Project Instructor: Dr. Adarsh Kumar
(Associate Professor)
INTRAVENOUS CATHETERIZATION AND TAPING PROCEDURE
Department of Veterinary Surgery and RadiologyD.G.C.N COVAS , CSKHPKV, PALAMPUR (H.P)
Intravenous cannulation is a technique in which a cannula is
placed inside a vein to provide venous access
Introduction :
Venous valves
encourage
unidirectional flow of
blood and prevent
pooling of blood in the
dependent portions of
the extremities; they
also can impede the
passage of a catheter
through and into a
vein
Venous valves
are more
numerous just
distal to the
points were
tributaries join
larger veins and
in the lower
extremities
INDICATIONS:Repeated blood sampling
Intravenous fluid administration
Intravenous medication administration
Intravenous chemotherapy administration
Intravenous nutritional support
Intravenous blood or blood products administration
Intravenous administration of radiological contrast agents
(eg, computed tomography, magnetic resonance imaging,
nuclear imaging)
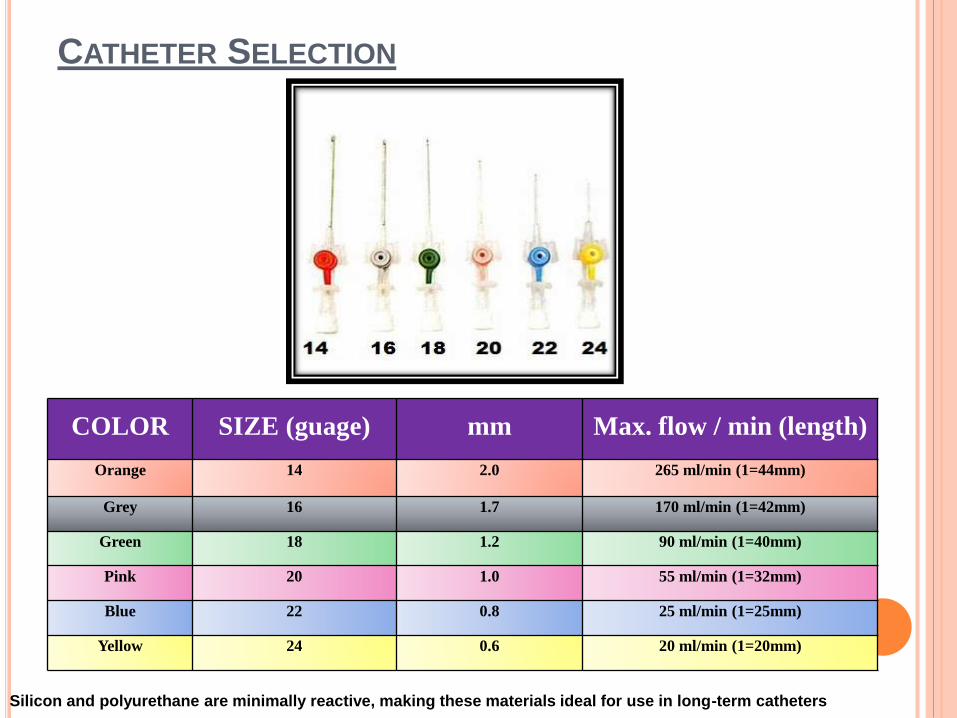
CATHETER SELECTION
COLOR SIZE (guage) mm Max. flow / min (length)
Orange 14 2.0 265 ml/min (1=44mm)
Grey 16 1.7 170 ml/min (1=42mm)
Green 18 1.2 90 ml/min (1=40mm)
Pink 20 1.0 55 ml/min (1=32mm)
Blue 22 0.8 25 ml/min (1=25mm)
Yellow 24 0.6 20 ml/min (1=20mm)
Silicon and polyurethane are minimally reactive, making these materials ideal for use in long-term catheters
EQUIPMENT REQUIRED:
I.V Canula (according to b.wt)
I.V Canula Fixator / Alcohol Wipe / Sterile Gauge Pieces
Thin strips of Adhesive tape (for securing further)
Tourniquet / Shaving Blades / Shaving Razor / Savlon
10-12 ml syringe filled saline / heparinized saline

STEP WISE PROCEDURE
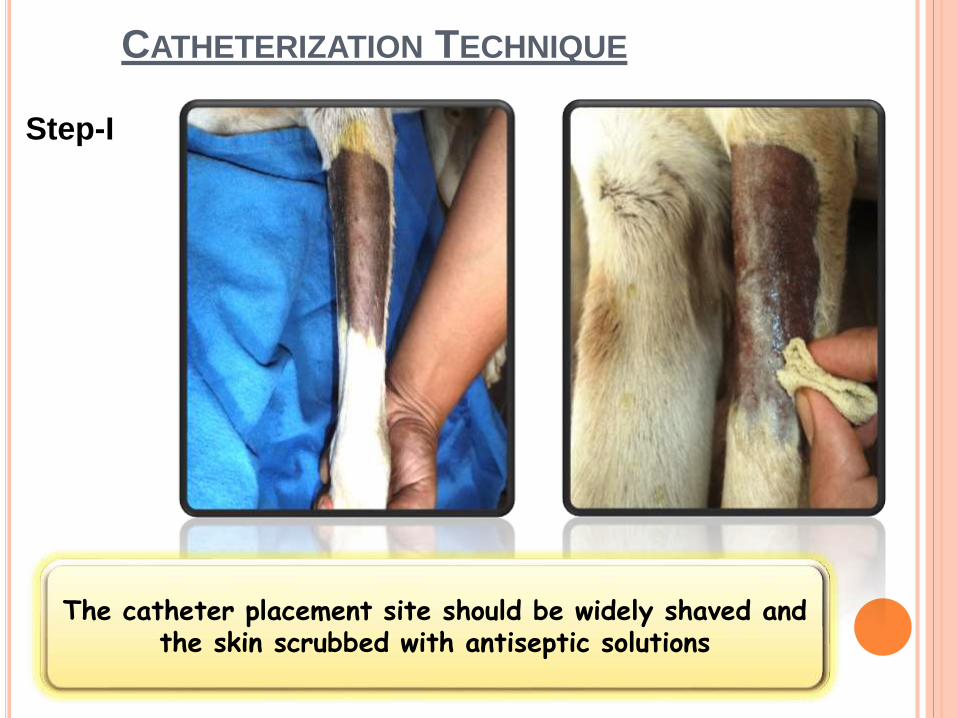
CATHETERIZATION TECHNIQUE
Step-I
The catheter placement site should be widely shaved and the skin scrubbed with antiseptic solutions
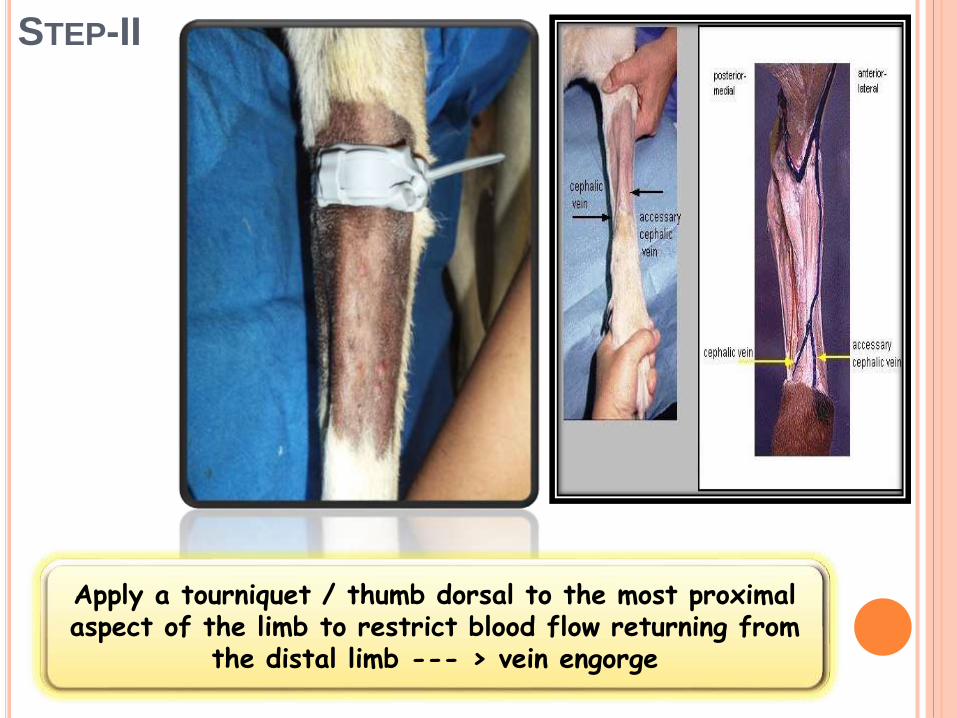
STEP-II
Apply a tourniquet / thumb dorsal to the most proximal aspect of the limb to restrict blood flow returning from
the distal limb --- > vein engorge
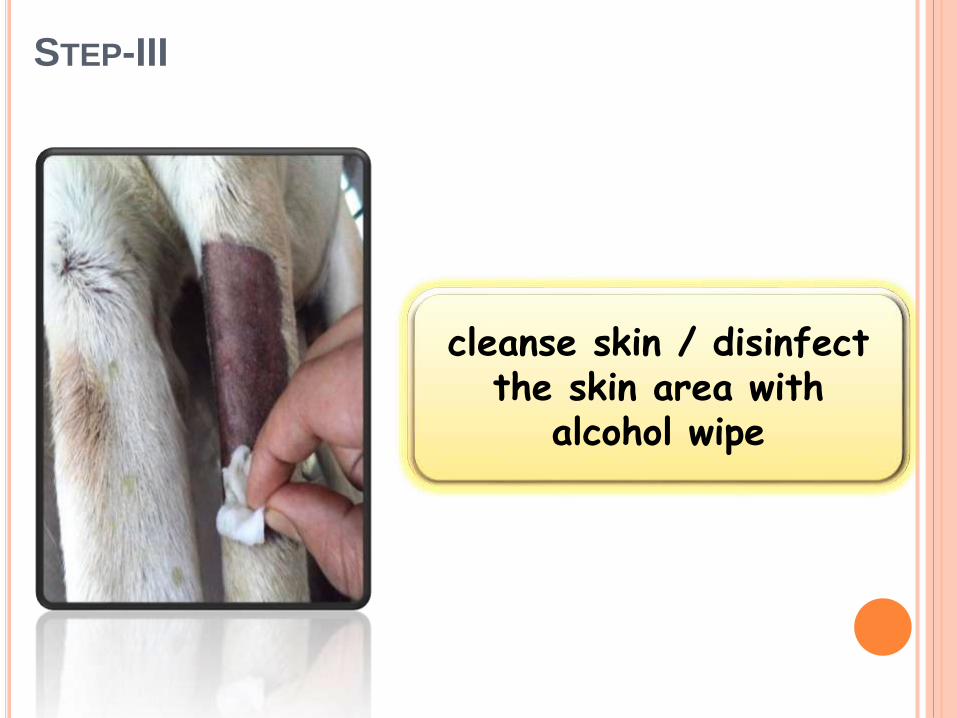
STEP-III
cleanse skin / disinfect the skin area with
alcohol wipe
STEP-IV
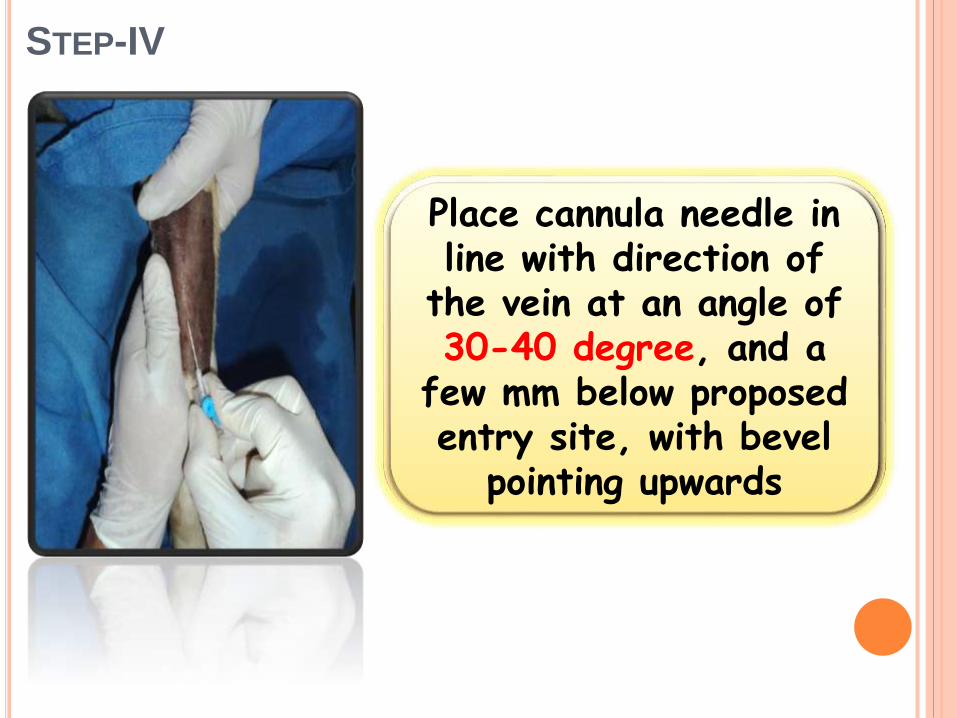
Place cannula needle in line with direction of
the vein at an angle of 30-40 degree, and a
few mm below proposed entry site, with bevel
pointing upwards
STEP-V
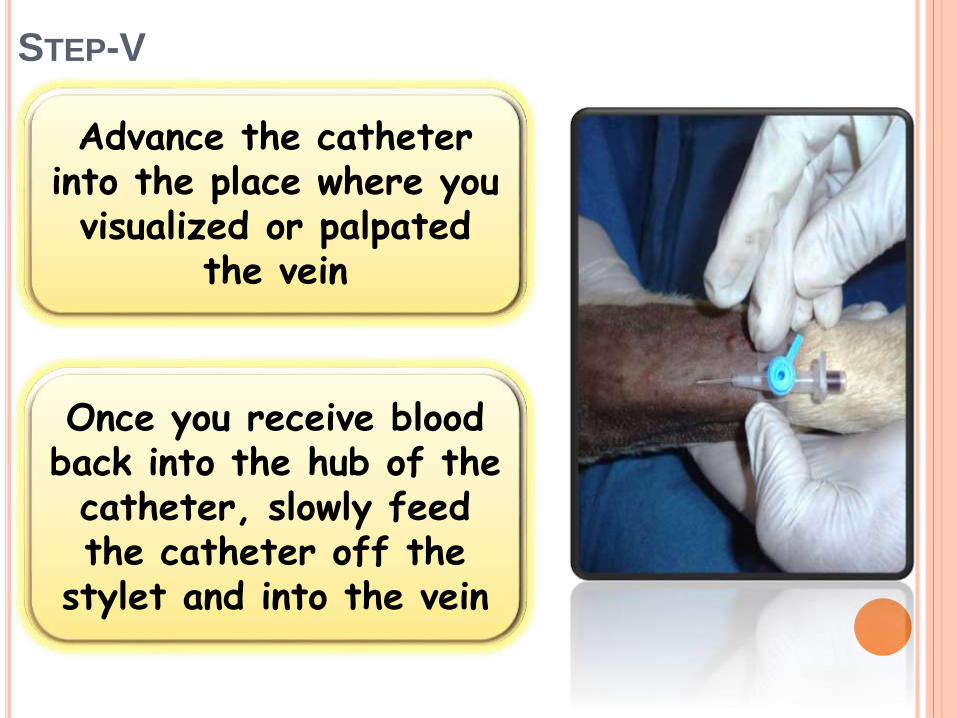
Advance the catheter into the place where you visualized or palpated
the vein
Once you receive blood back into the hub of the catheter, slowly feed the catheter off the
stylet and into the vein
STEP-VI
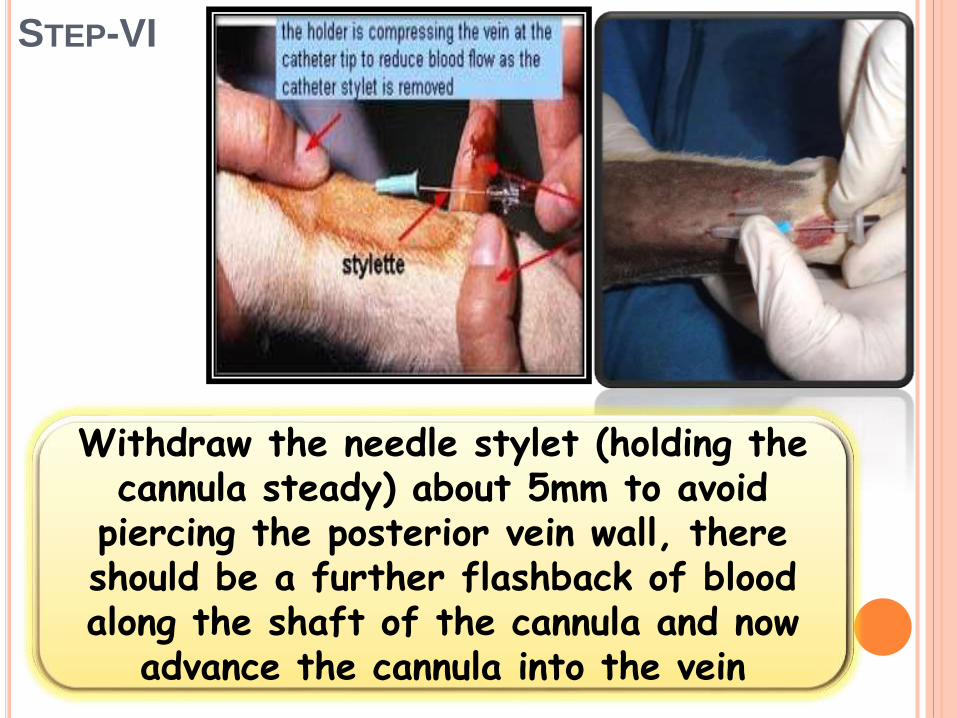
Withdraw the needle stylet (holding the cannula steady) about 5mm to avoid
piercing the posterior vein wall, there should be a further flashback of blood along the shaft of the cannula and now
advance the cannula into the vein
STEP-VII
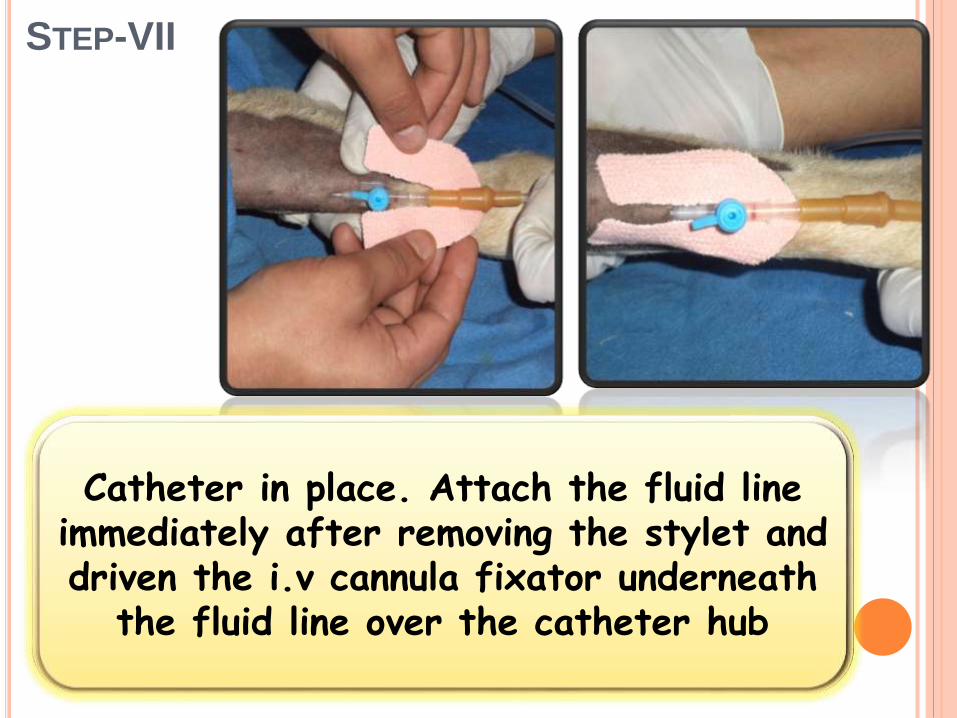
Catheter in place. Attach the fluid line immediately after removing the stylet and driven the i.v cannula fixator underneath
the fluid line over the catheter hub
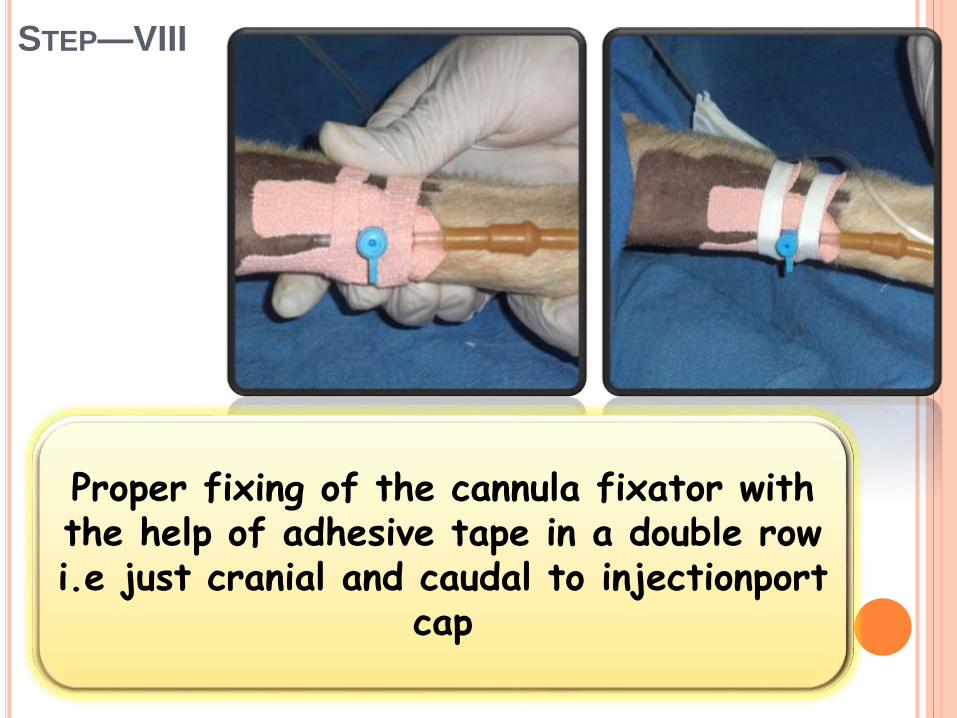
STEP—VIII
Proper fixing of the cannula fixator with the help of adhesive tape in a double row i.e just cranial and caudal to injectionport
cap
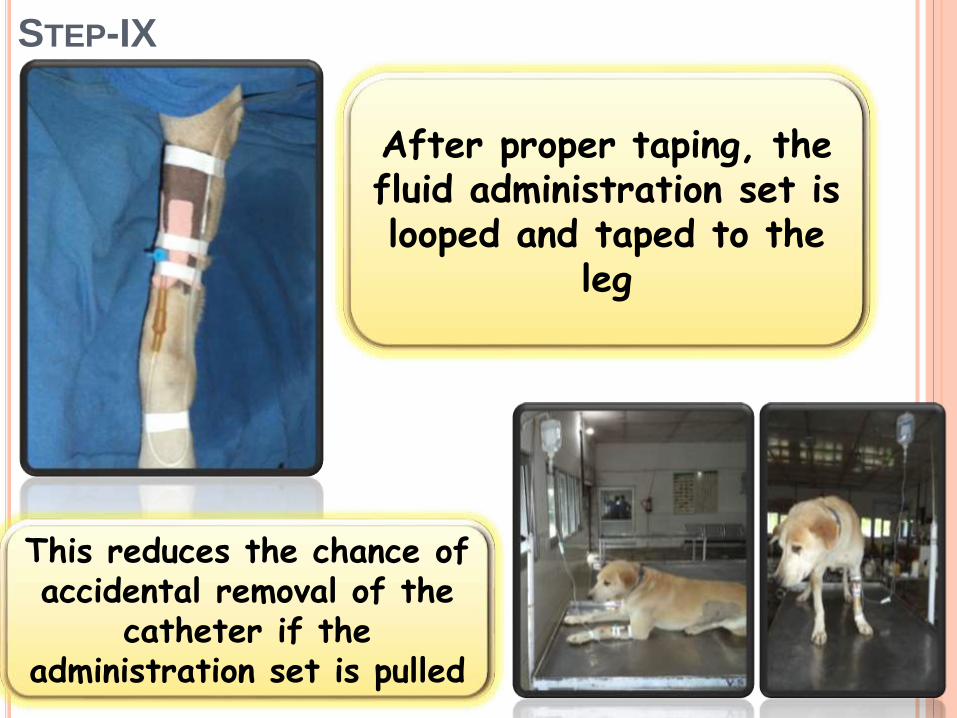
STEP-IX
After proper taping, the fluid administration set is looped and taped to the
leg
This reduces the chance of accidental removal of the
catheter if the administration set is pulled
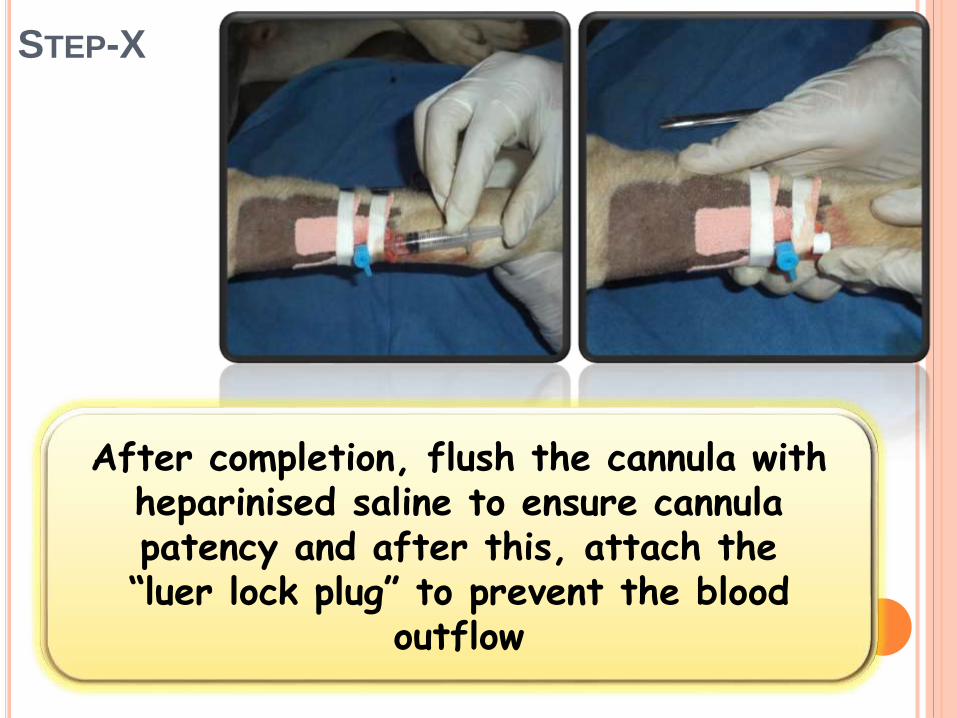
STEP-X
After completion, flush the cannula with heparinised saline to ensure cannula patency and after this, attach the “luer lock plug” to prevent the blood
outflow
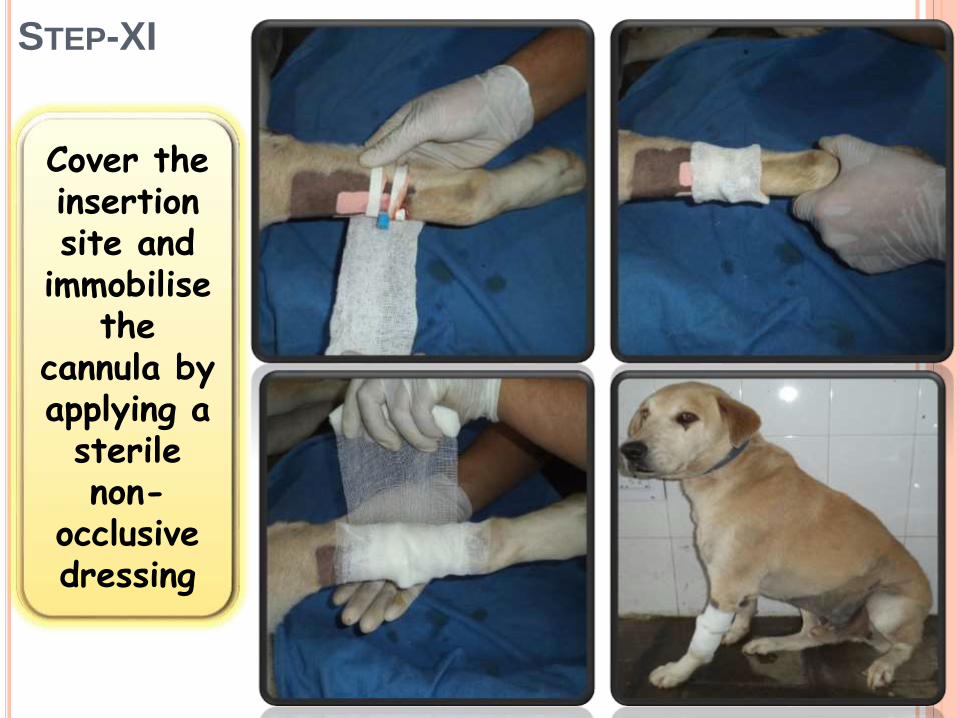
STEP-XI
Cover the insertion site and
immobilisethe
cannula by applying a sterile non-
occlusive dressing

Secure…….. Secure
Scalp vein set
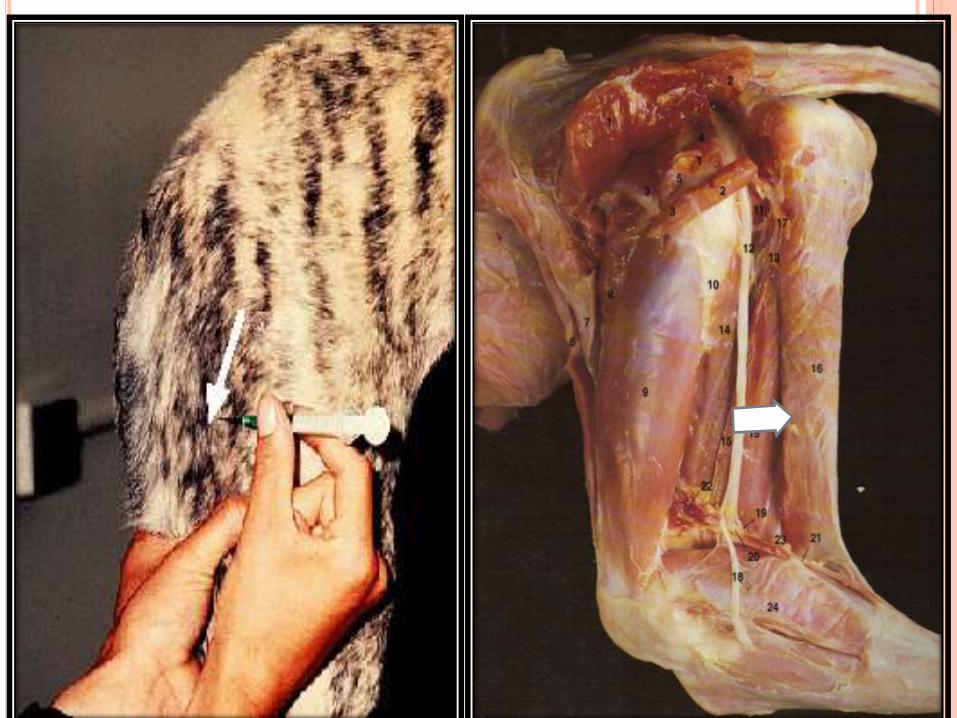
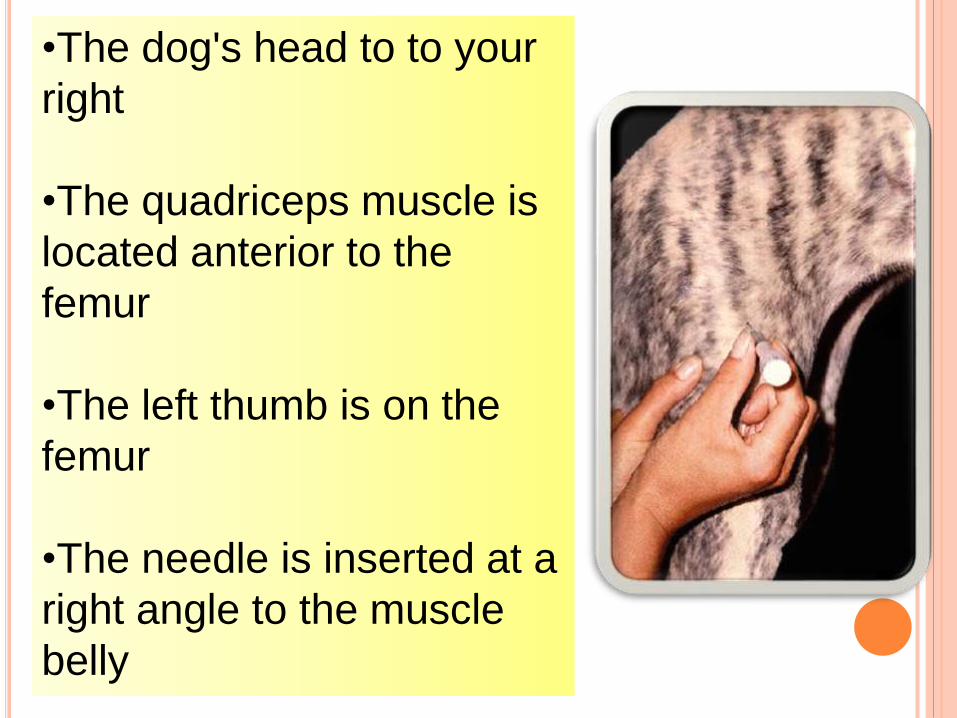
•The dog's head to to your
right
•The quadriceps muscle is
located anterior to the
femur
•The left thumb is on the
femur
•The needle is inserted at a
right angle to the muscle
belly
SECURING THE CANNULA
It is important to secure the cannula to prevent
mechanical phlebitis. This can be done with
clean tape or a special adhesive dressing
Care should be taken to avoid the insertion site. If
the device is located over a joint, the joint should be
immobilised and splinted to prevent movement and
dislodgement of the cannula
CARE OF THE CANNULA
Once sited the cannula should be flushed with
either normal saline or heparinised saline. The
site should be regularly inspected for signs of
phlebitis
Peripheral cannula should be re-sited every 48-
72 hours to reduce the risk of phlebitis, but this
may be difficult in patients with difficult veins
Cannula should not remain in situ for any
longer than necessary to reduce the risks of
infection. Consideration should be given to
resiting them after 48-72 hours
When removing the cannula, pressure should
be applied to the site for at least a minute and
the site should be occluded with a sterile
dressing
CANNULA REMOVAL

















![tmz.vo.llnwd.netEKG pads Endotracheal/nasotracheal tube C] Esophageal obturator Intravenous lines Nasogastric/orogastric tube Urinary catheter Other . ADULT PROTOCOL page 5 of 17tmz.vo.llnwd.net/o28/newsdesk/tmz_documents/... ·](https://img.pdfslide.net/doc/110x75/5a76b4c17f8b9a1b688d7590/tmzvollnwdnetekg-pads-endotrachealnasotracheal-tube-c-esophageal-obturator.jpg)












