Embed Size (px)
DESCRIPTION
Citation preview
1987 -1995 Kedokteran Umum, UNS1999 - 2003 S2 Kedokteran Klinis, UGM1999 – 2004 Spesialis THT-KL, UGM2009 - ..... Program Doktor FK.UGM2009 – 2012 Konsultan Onkologi Bedah Kepala Leher
1996-1999 : Dokter PTT Puskesmas , Klaten1999 : Staff di Sub Bag Onkologi-Bedah Kepala Leher IK.THT-KL FK UGM / RS. Dr. Sardjito 2006-2012 : Kodik Profesi Bag. IK.THT-KL2013 - : Sekretaris Program Studi PPDS IK.THT-KL
dr. S R Indrasari, M.Kes., Sp.THT-KL(K)Yogyakarta, 15 Juli
Jl. Bogowonto 108B [email protected] ; [email protected]

KARSINOMA NASOFARINGS (KNF)NASOPHARYNGEAL CARCINOMA (NPC)
SUB BAGIAN ONKOLOGI BAGIAN IK. THT-KL FAKULTAS KEDOKTERAN UGM / RS DR SARDJITO
YOGYAKARTA
Why Cancer ?
The burden of Cancer
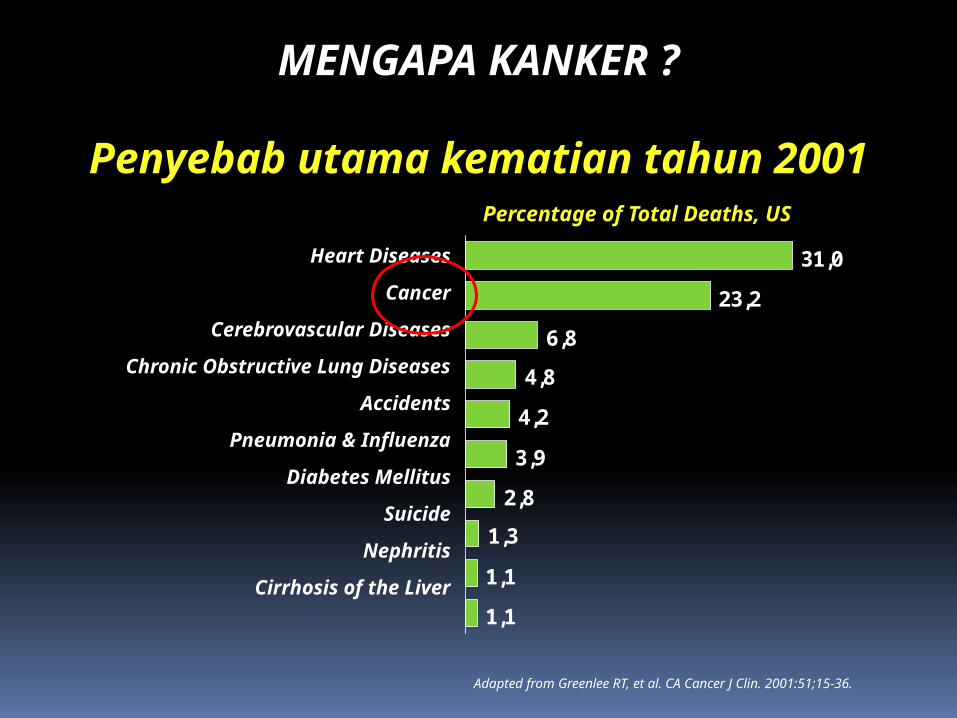
Adapted from Greenlee RT, et al. CA Cancer J Clin. 2001:51;15-36.
Penyebab utama kematian tahun 2001
MENGAPA KANKER ?
1,1
1,1
1,3
2,8
3,9
4,2
4,8
6,8
23,2
31,0
Percentage of Total Deaths, US
Heart Diseases
Cancer
Cerebrovascular Diseases
Chronic Obstructive Lung Diseases
Accidents
Pneumonia & Influenza
Diabetes Mellitus
Suicide
Nephritis
Cirrhosis of the Liver

10 besar keganasan di dunia
1 Lung Breast Lung 1,037,000
2 Stomach Colon/rectum Stomach 798,000
3 Colon/rectum Cervix uteri Breast 796,000
4 Prostate Stomach Colon/rectum 783,000
5 Liver Lung Liver 437,000
6 Mouth/pharynx Ovary Prostate 396,000
7 Esophagus Corpus uteri Cervix uteri 371,000
8 Bladder Liver Mouth/pharynx 363,000
9 Leukemia Mouth/pharynx Esophagus 316,000
10 NHL* Esophagus Bladder 261,000
Total NewRank Males Females Both Sexes Cases
*Non-Hodgkin’s lymphoma. Adapted from Parkin DM, et al. CA Cancer J Clin. 1999;49:39.
Why NPC ?
The burden of NPC
Mengapa Karsinoma nasofarings ?
Keganasan no. 4 di seluruh badan No.1 dari keganasan di Kepala-Leher Insidensi cukup tinggi di Indonesia Mengenai usia produktif Penderita datang pd stadium lanjut Mortalitas tinggi
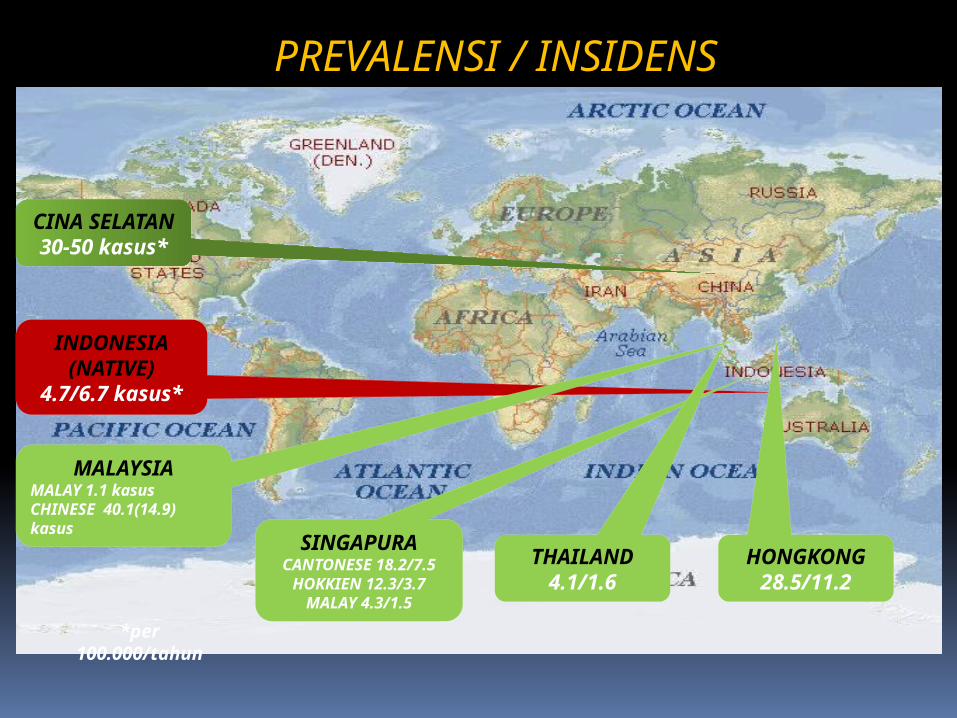
PREVALENSI / INSIDENS
CINA SELATAN
30-50 kasus*
INDONESIA (NATIVE)4.7/6.7 kasus*
MALAYSIAMALAY 1.1 kasusCHINESE 40.1(14.9) kasus SINGAPURA
CANTONESE 18.2/7.5
HOKKIEN 12.3/3.7MALAY 4.3/1.5
THAILAND4.1/1.6
HONGKONG28.5/11.2
*per 100.000/tahun
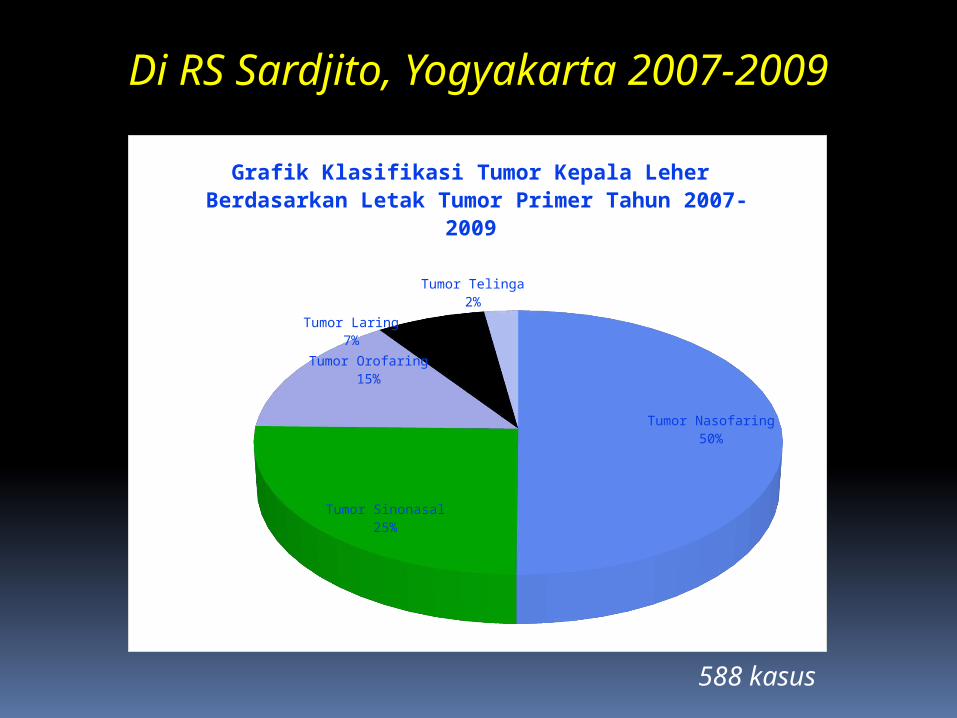
Di RS Sardjito, Yogyakarta 2007-2009
588 kasus
Tumor Nasofaring50%
Tumor Sinonasal25%
Tumor Orofaring15%
Tumor Laring7%
Tumor Telinga2%
Grafik Klasifikasi Tumor Kepala Leher Berdasarkan Letak Tumor Primer Tahun 2007-2009
Tumor Nasofaring Tumor Sinonasal Tumor Orofaring Tumor Laring Carcinoma Auricula
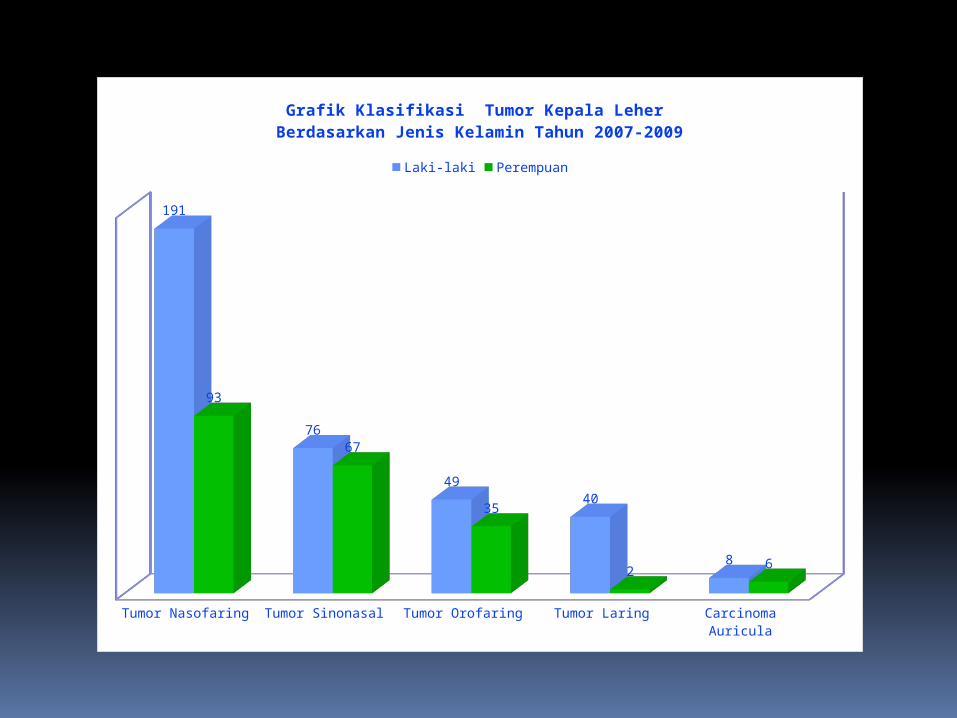
191
76
49
40
8
93
67
35
26
Grafik Klasifikasi Tumor Kepala Leher Berdasarkan Jenis Kelamin Tahun 2007-2009
Laki-laki Perempuan
5-14
15-24
25-34
35-44
45-54
55-64
65-74
75-84
4-14
15-25
26-36
37-47
48-58
59-69
70-80
81-91
7-17
18-28
29-39
40-50
51-61
62-72
73-83
12-24
25-37
38-50
51-63
64-76
77-89
18-27
28-37
38-47
48-57
58-67
68-77
78-87
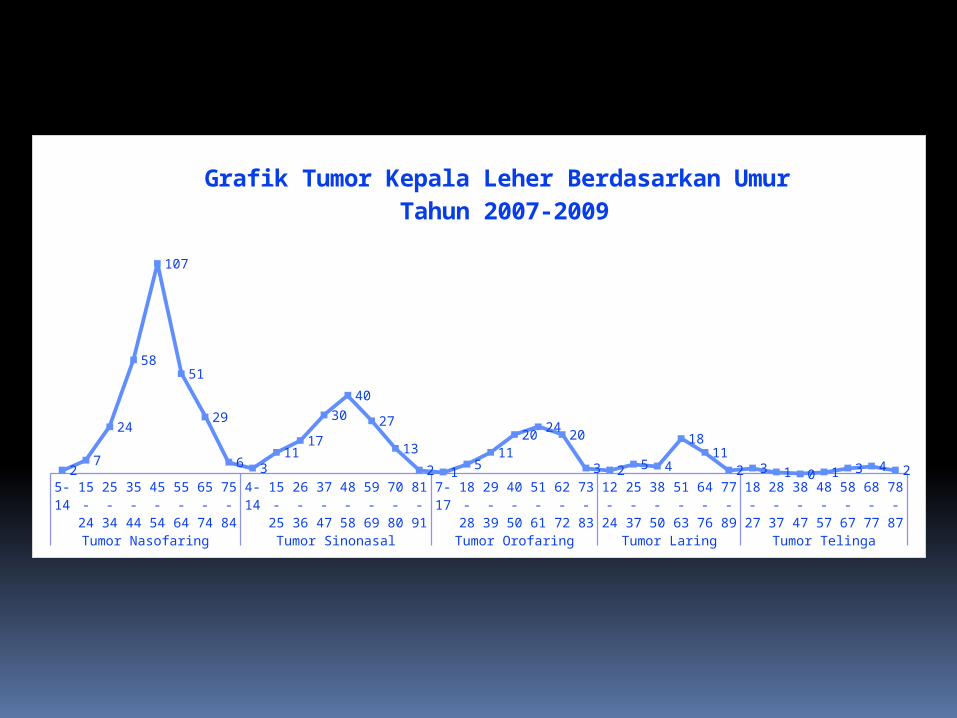
Tumor Nasofaring Tumor Sinonasal Tumor Orofaring Tumor Laring Tumor Telinga
27
24
58
107
51
29
6 311
17
30
40
27
13
2 15
11
2024
20
3 2 5 4
1811
2 3 1 0 1 3 4 2
Grafik Tumor Kepala Leher Berdasarkan Umur Tahun 2007-2009
What is NPC ?
DefinitionCause & Risk factors
Symptoms & signs
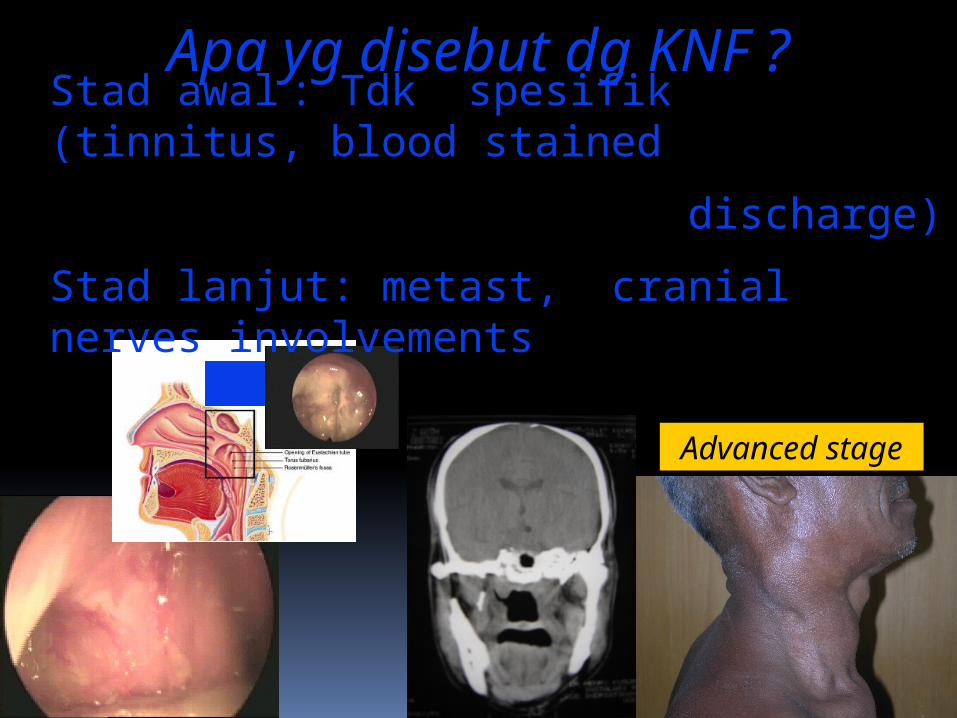
Apa yg disebut dg KNF ?
Advanced stage
Stad awal : Tdk spesifik (tinnitus, blood stained
discharge)
Stad lanjut: metast, cranial nerves involvements
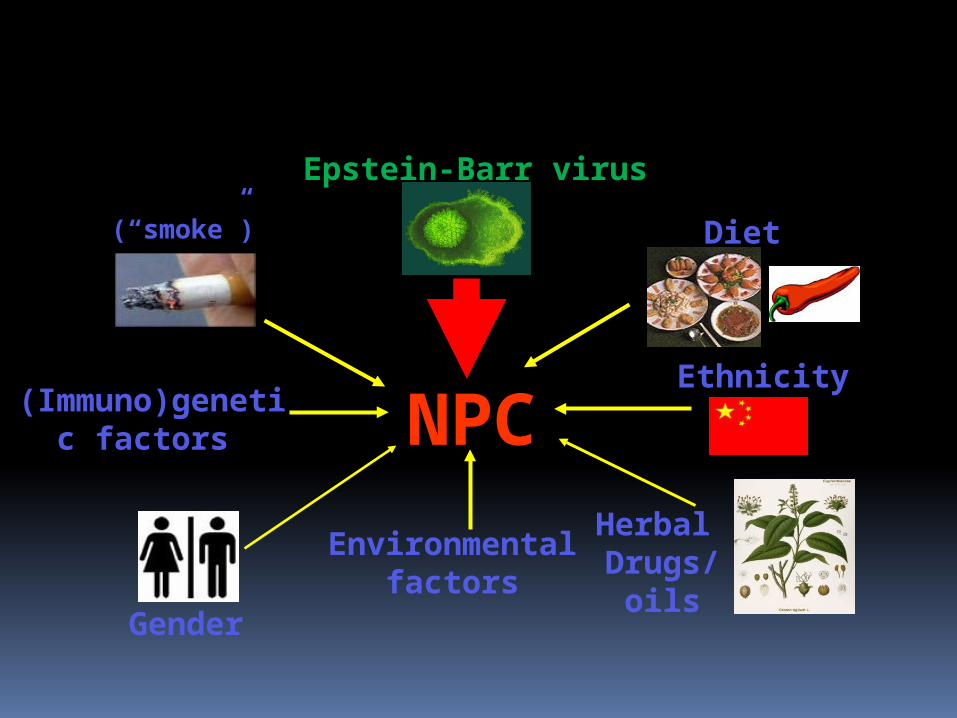
ETIOLOGI & FAKTOR RISIKO
Epstein-Barr virus
NPCEthnicity
Diet(“smoke”)
(Immuno)genetic factors
Gender
Herbal Drugs/
oils
Environmentalfactors
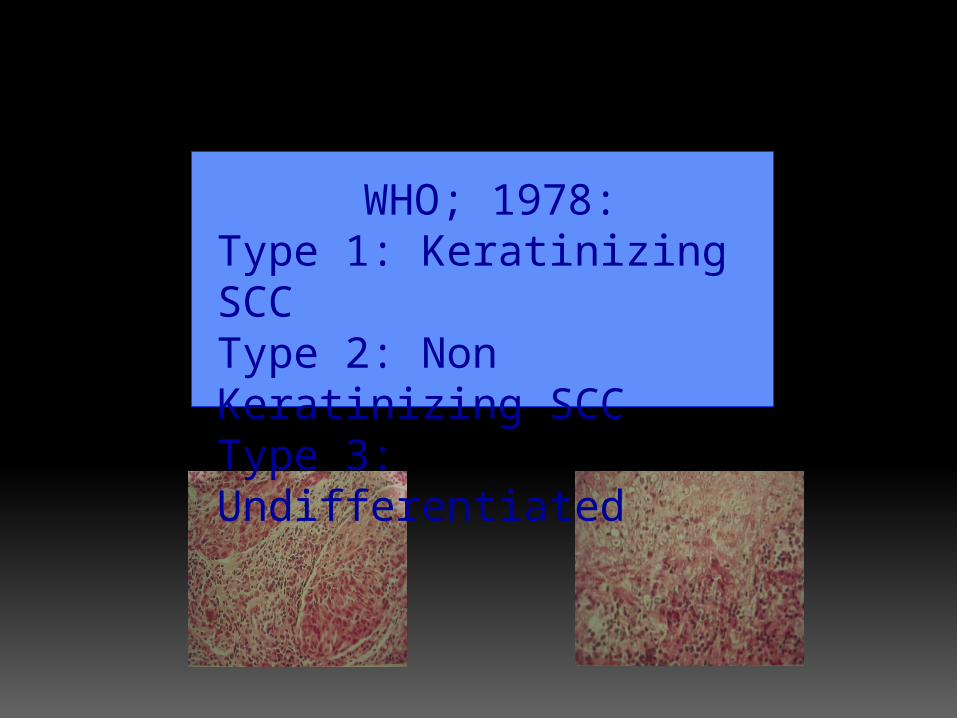
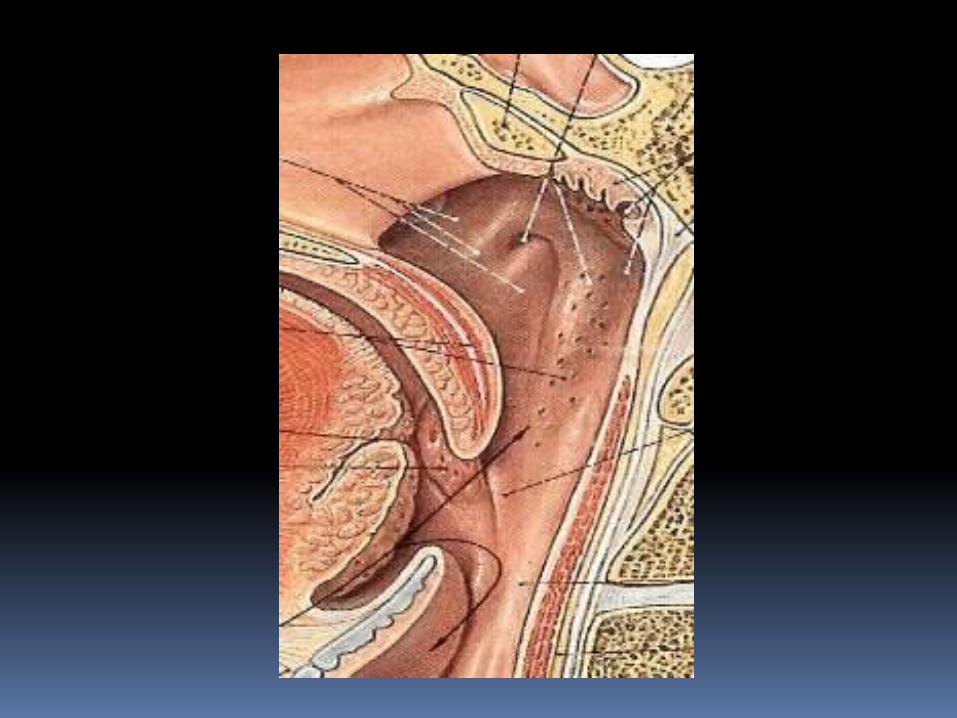
PATOLOGI ANATOMI
WHO; 1978:Type 1: Keratinizing SCCType 2: Non Keratinizing SCCType 3: Undifferentiated
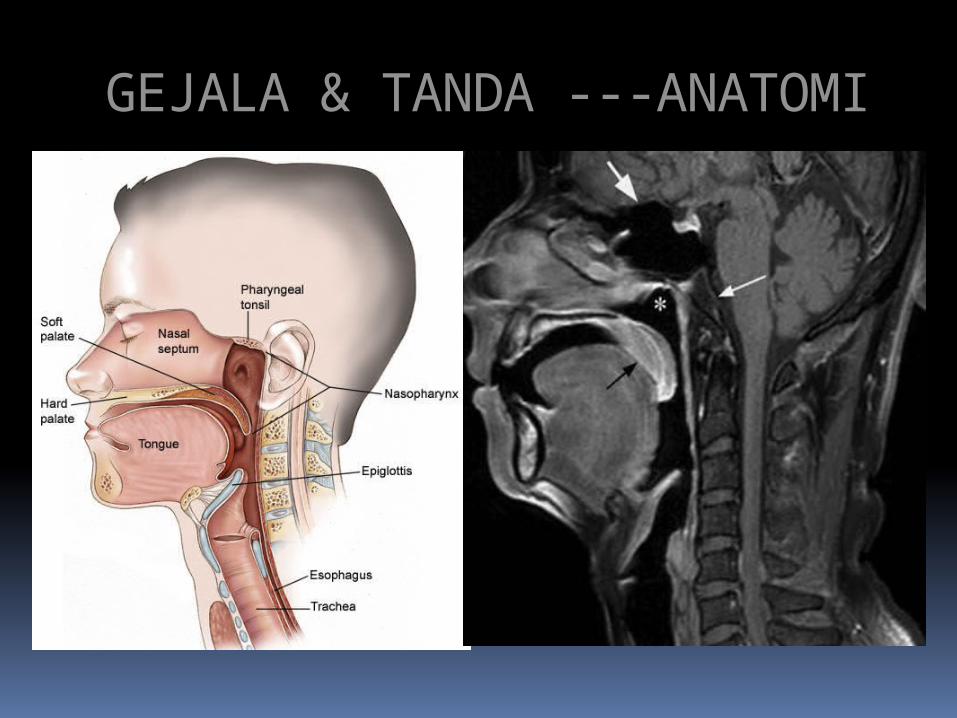
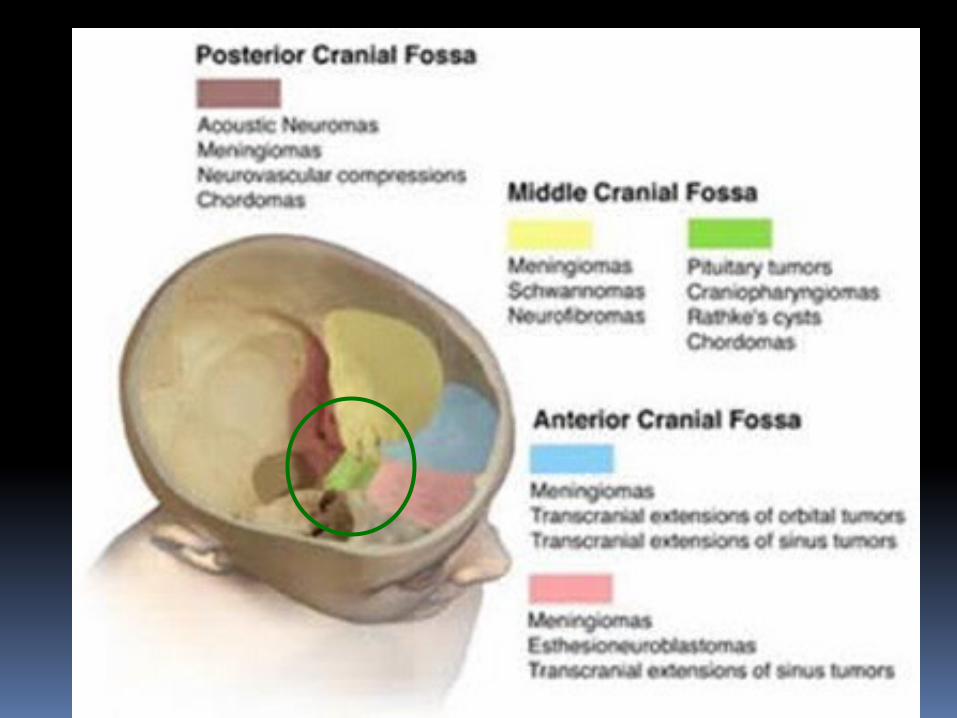
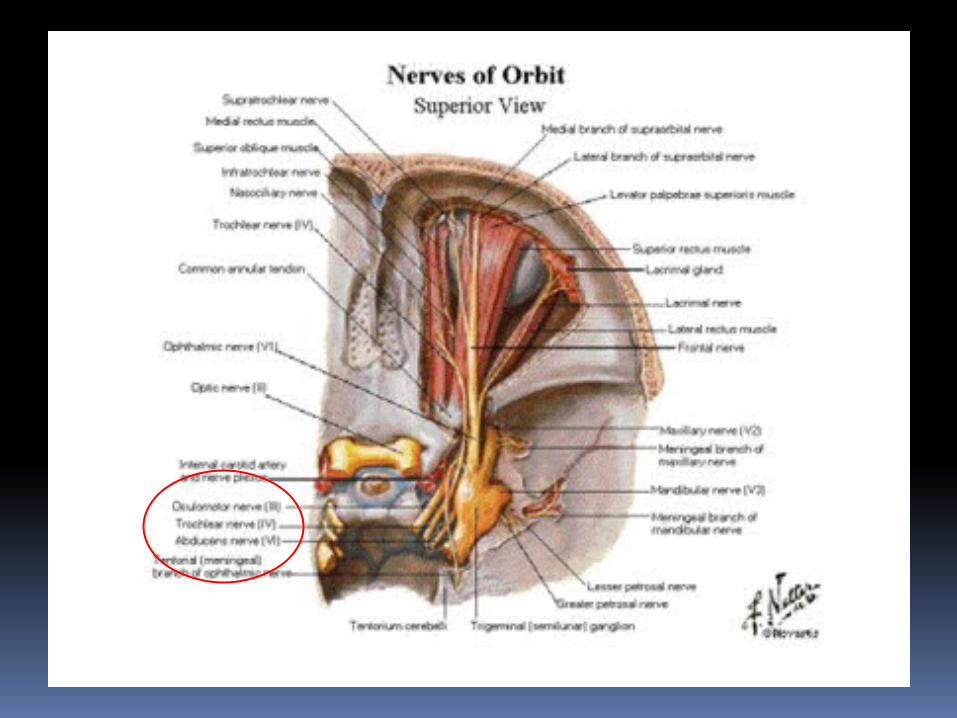
GEJALA & TANDA ---ANATOMI
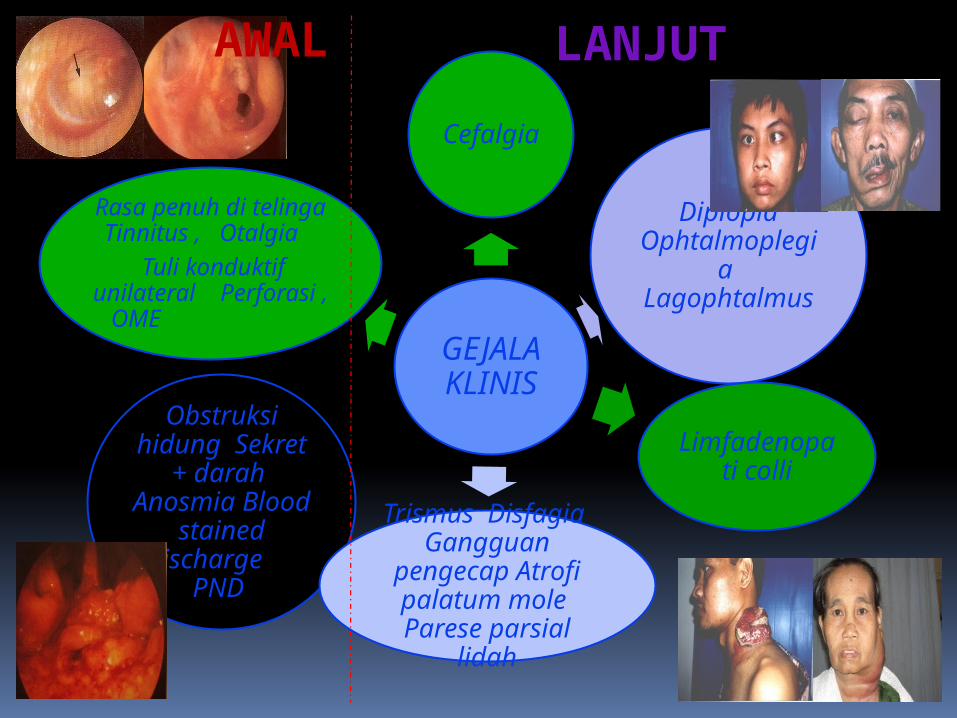
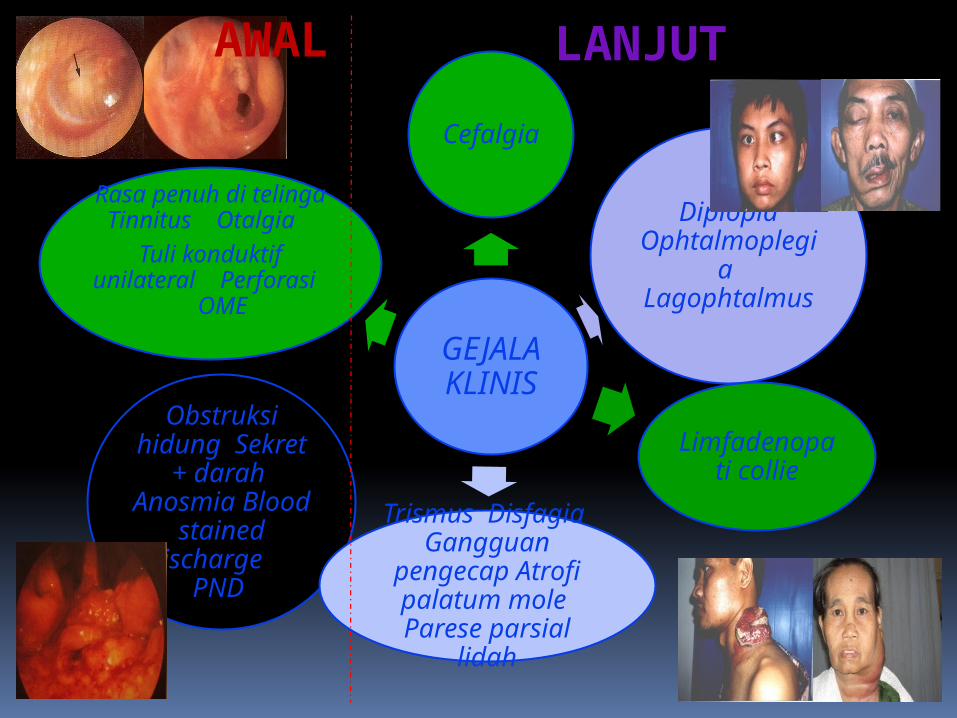
GEJALA KLINIS
Cefalgia
Diplopia Ophtalmoplegia Lagophtalmus
Obstruksi hidung Sekret + darah Anosmia Blood
stained discharge PND Trismus Disfagia Gangguan
pengecap Atrofi palatum mole Parese parsial lidah
Limfadenopati colli
Rasa penuh di telinga Tinnitus , Otalgia
Tuli konduktif unilateral Perforasi , OME
AWAL LANJUT
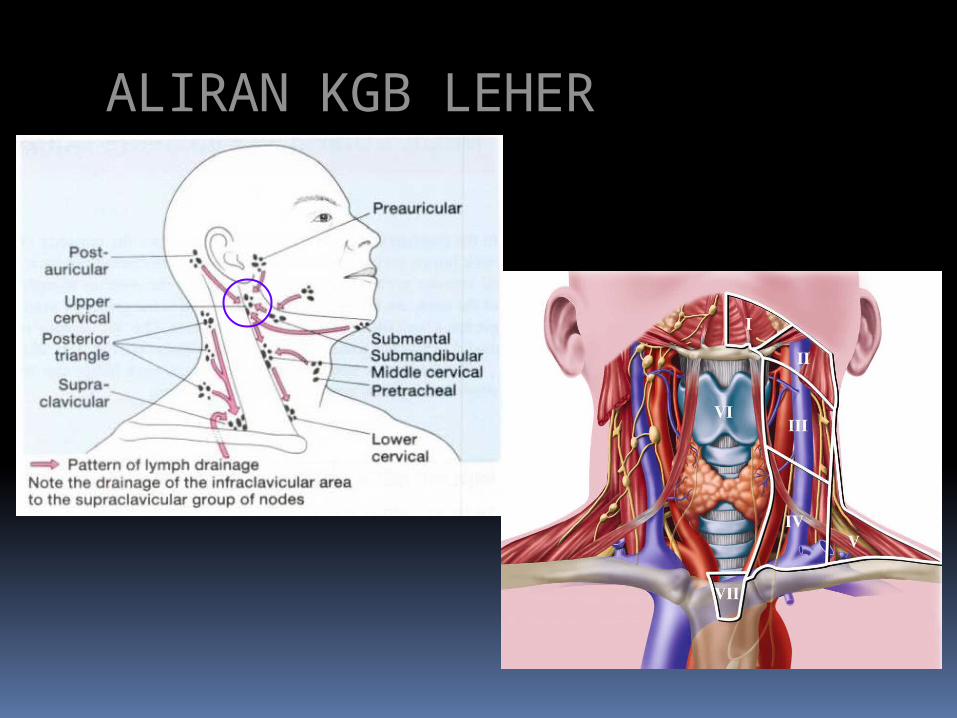
ALIRAN KGB LEHER

DIAGNOSIS
Anamnesis Pemeriksaan Fisik THT Rinoskopi Anterior &
Posterior Endoskopi: Rigid/ Fiber nasopharyngolaryngoscopy
BIOPSI
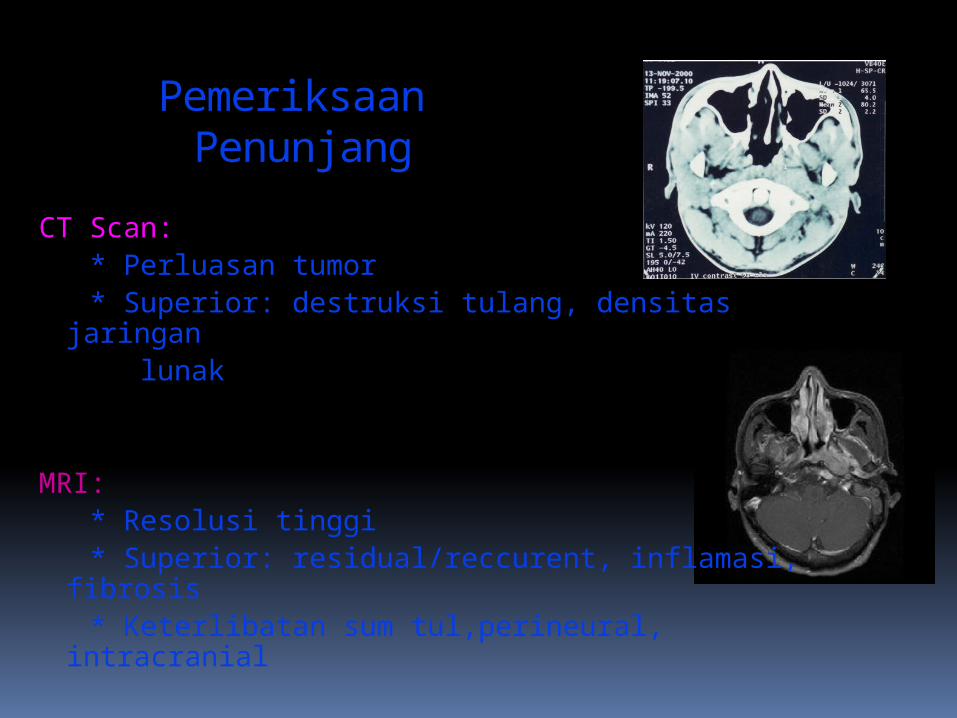
Pemeriksaan Penunjang
CT Scan: * Perluasan tumor * Superior: destruksi tulang, densitas jaringan lunak
MRI: * Resolusi tinggi * Superior: residual/reccurent, inflamasi,
fibrosis * Keterlibatan sum tul,perineural, intracranial
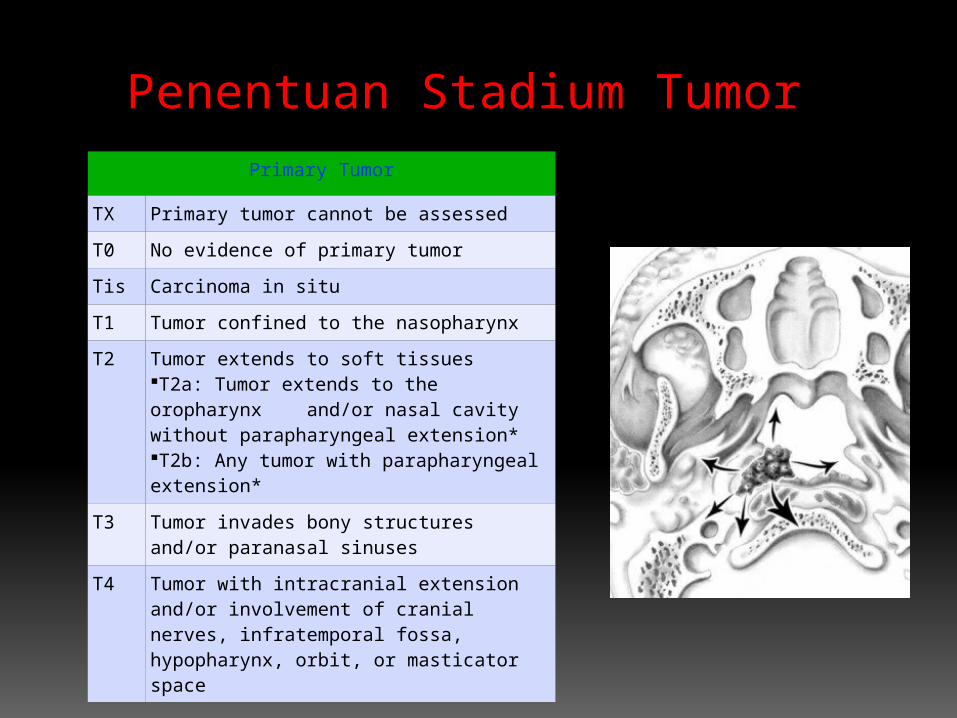
Penentuan Stadium Tumor Primary Tumor
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
Tis Carcinoma in situ
T1 Tumor confined to the nasopharynx
T2 Tumor extends to soft tissuesT2a: Tumor extends to the oropharynx and/or nasal cavity without parapharyngeal extension* T2b: Any tumor with parapharyngeal extension*
T3 Tumor invades bony structures and/or paranasal sinuses
T4 Tumor with intracranial extension and/or involvement of cranial nerves, infratemporal fossa, hypopharynx, orbit, or masticator space
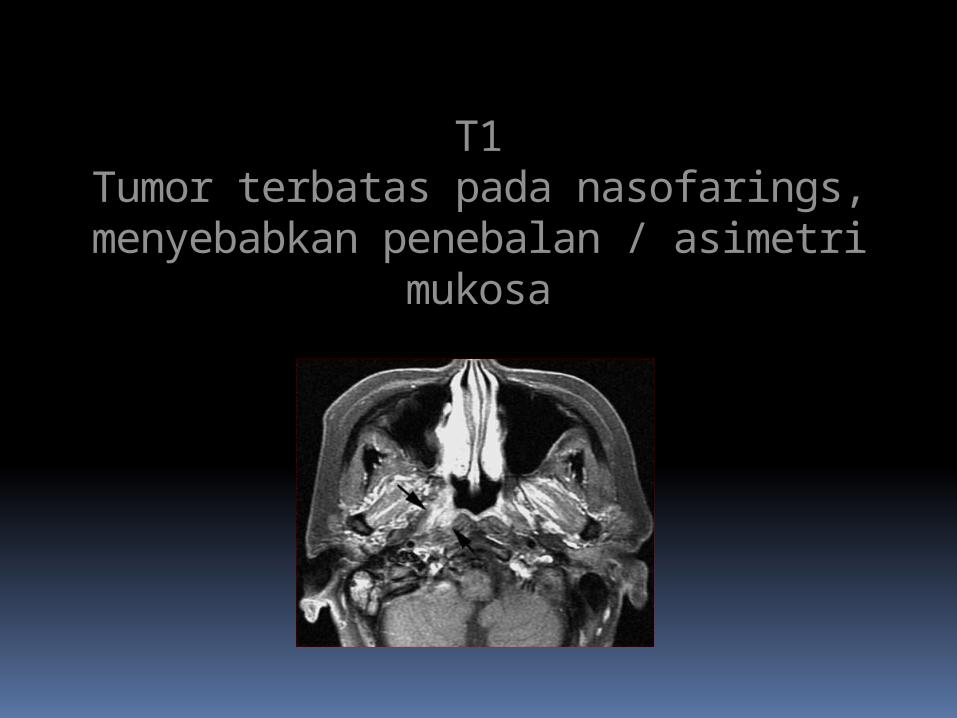
T1Tumor terbatas pada nasofarings, menyebabkan
penebalan / asimetri mukosa
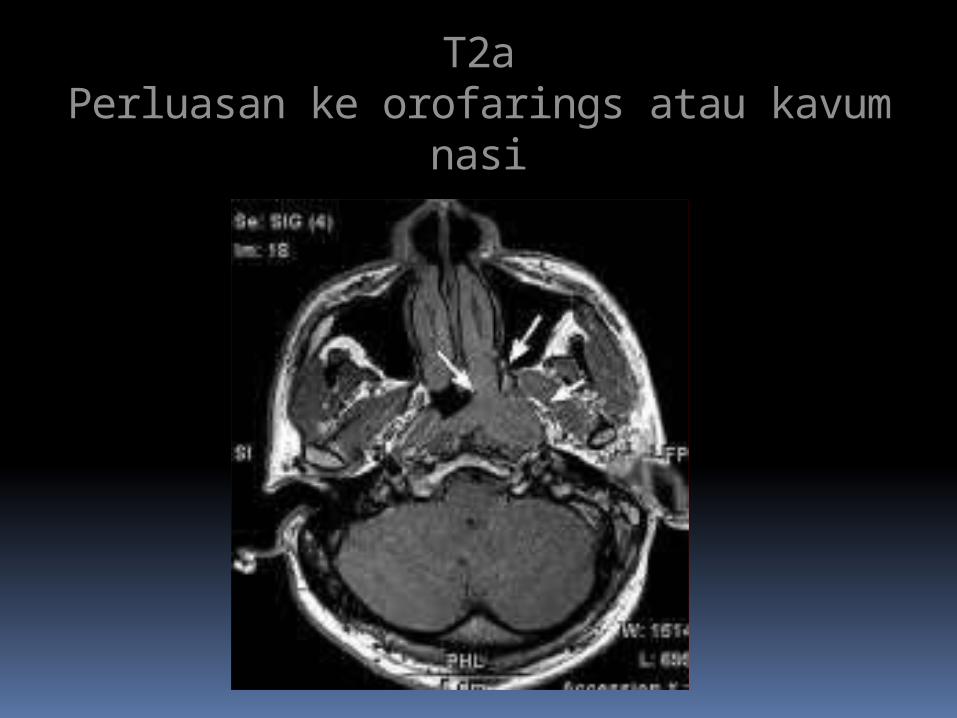
T2aPerluasan ke orofarings atau kavum nasi
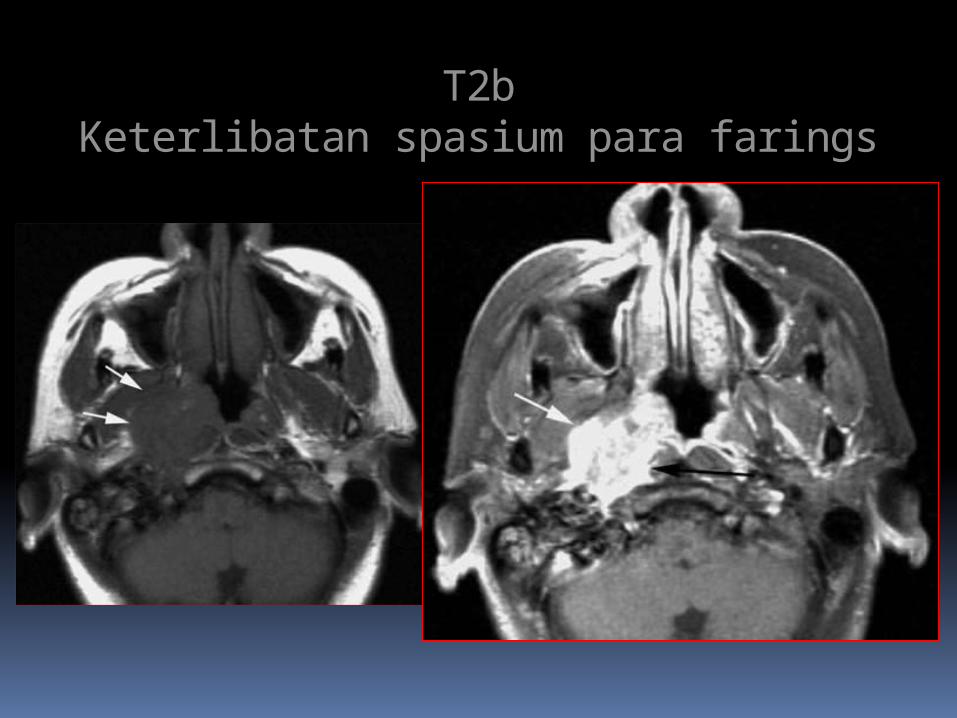
T2bKeterlibatan spasium para farings
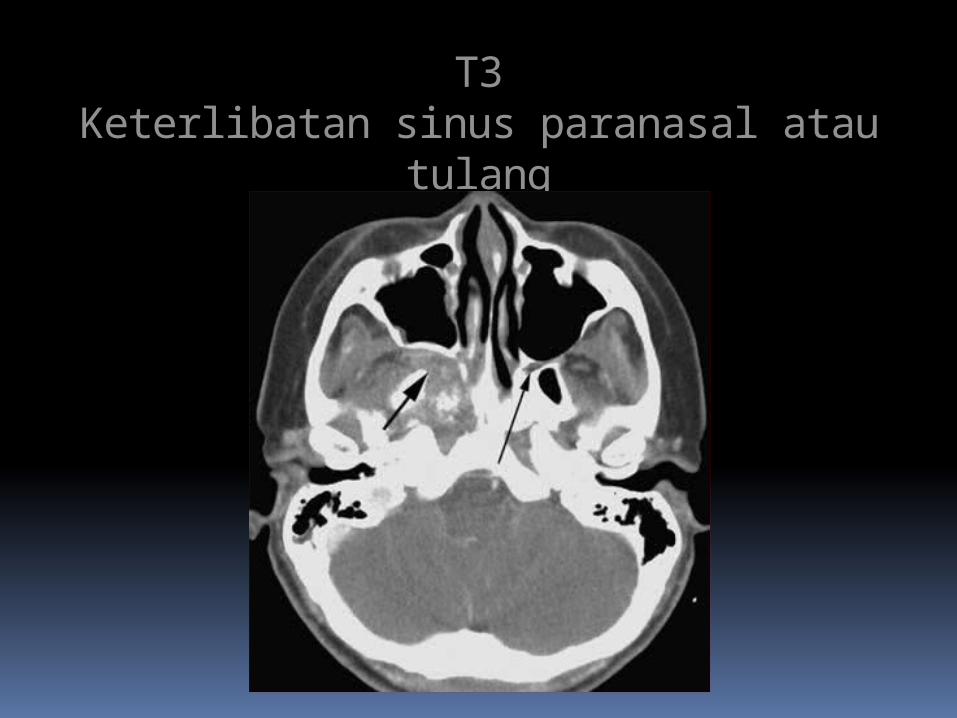
T3Keterlibatan sinus paranasal atau tulang
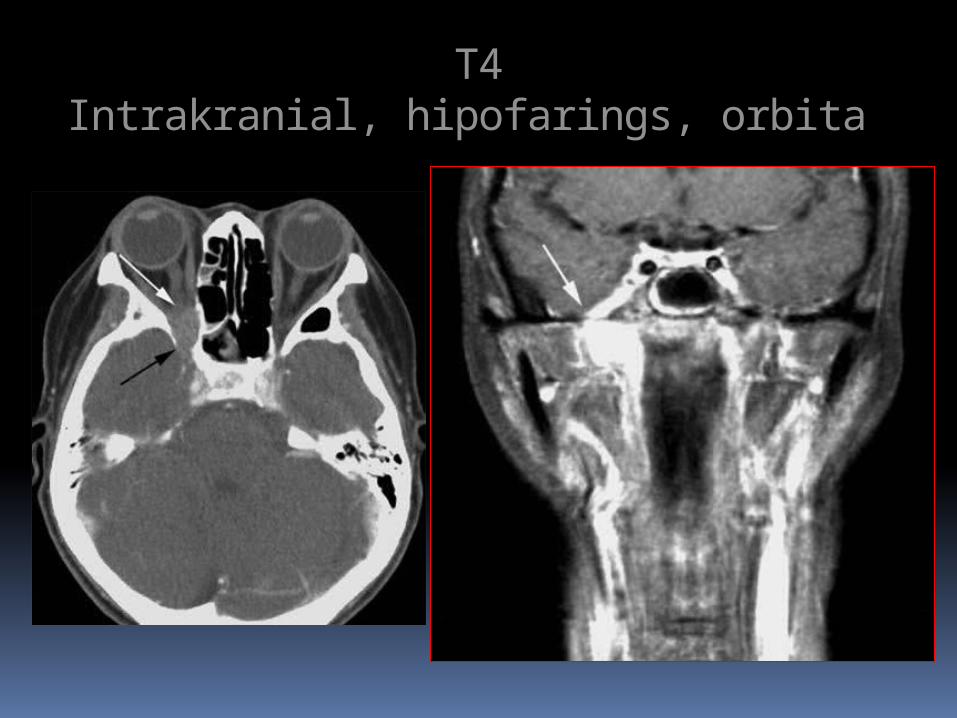
T4Intrakranial, hipofarings, orbita
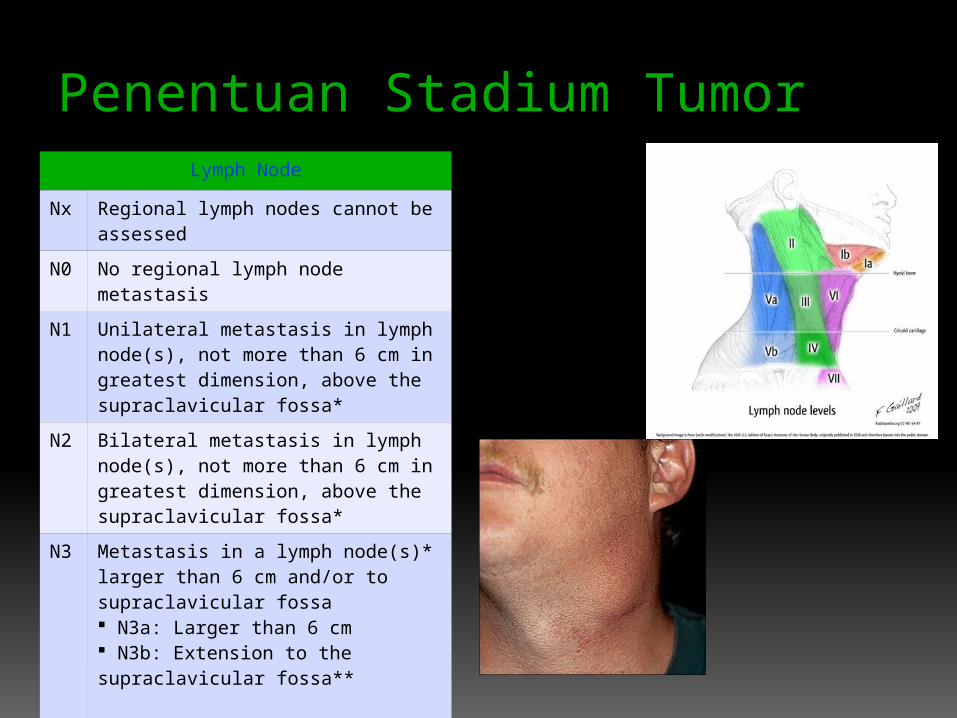
Penentuan Stadium Tumor Lymph Node
Nx Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasis
N1 Unilateral metastasis in lymph node(s), not more than 6 cm in greatest dimension, above the supraclavicular fossa*
N2 Bilateral metastasis in lymph node(s), not more than 6 cm in greatest dimension, above the supraclavicular fossa*
N3 Metastasis in a lymph node(s)* larger than 6 cm and/or to supraclavicular fossa N3a: Larger than 6 cm N3b: Extension to the supraclavicular fossa**
* [Note: Midline nodes are considered ipsilateral nodes.]** [Note: Supraclavicular zone or fossa is relevant to the staging of nasopharyngeal carcinoma and is the triangular region originally described in the Ho-stage classification for nasopharyngeal cancer. It is defined by three points: (1) the superior margin of the sternal end of the clavicle; (2) the superior margin of the lateral end of the clavicle; and, (3) the point where the neck meets the shoulder. Note that this would include caudal portions of Levels IV and V. All cases with lymph nodes (whole or part) in the fossa are considered N3b.]
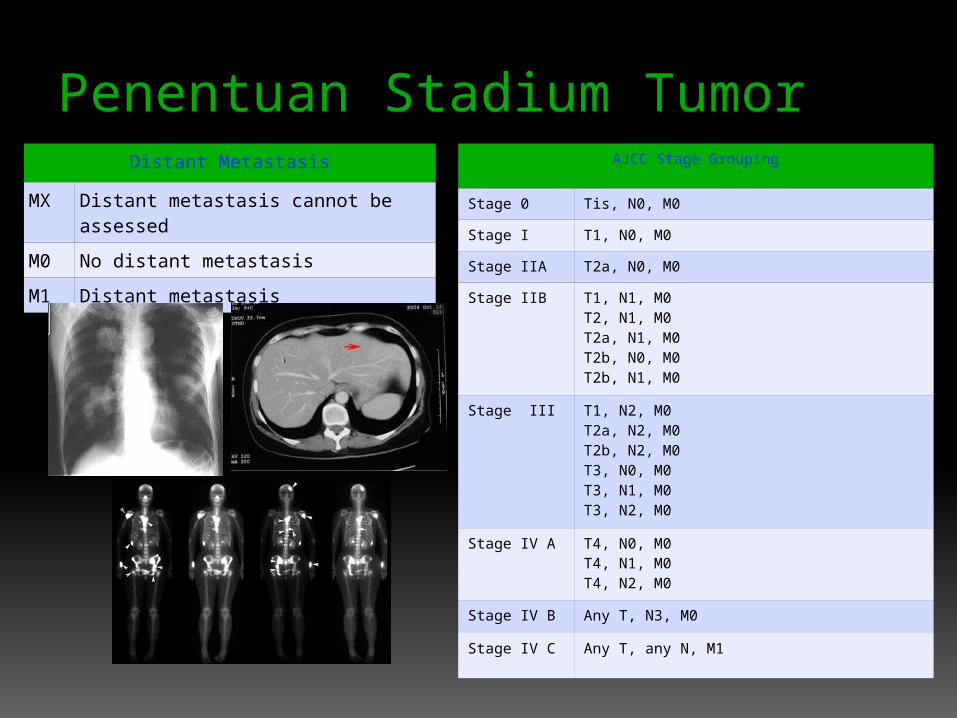
Penentuan Stadium Tumor Distant Metastasis
MX Distant metastasis cannot be assessed
M0 No distant metastasis
M1 Distant metastasis
AJCC Stage Grouping
Stage 0 Tis, N0, M0
Stage I T1, N0, M0
Stage IIA T2a, N0, M0
Stage IIB T1, N1, M0 T2, N1, M0 T2a, N1, M0 T2b, N0, M0 T2b, N1, M0
Stage III T1, N2, M0 T2a, N2, M0 T2b, N2, M0 T3, N0, M0 T3, N1, M0 T3, N2, M0
Stage IV A T4, N0, M0 T4, N1, M0 T4, N2, M0
Stage IV B Any T, N3, M0
Stage IV C Any T, any N, M1
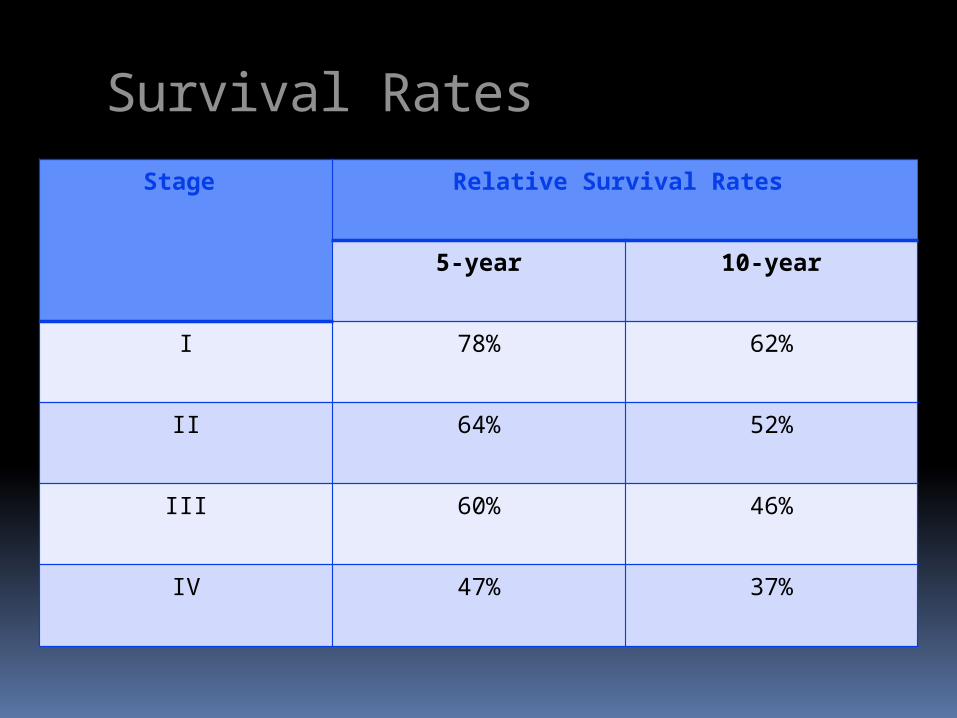
Survival RatesStage Relative Survival Rates
5-year 10-year
I 78% 62%
II 64% 52%
III 60% 46%
IV 47% 37%

PENATALAKSANAAN•Radioterapi
Stadium I & II
•Kemoradiasi
Stadium III, IVa & b
•Kemoterapi
Stadium IVc
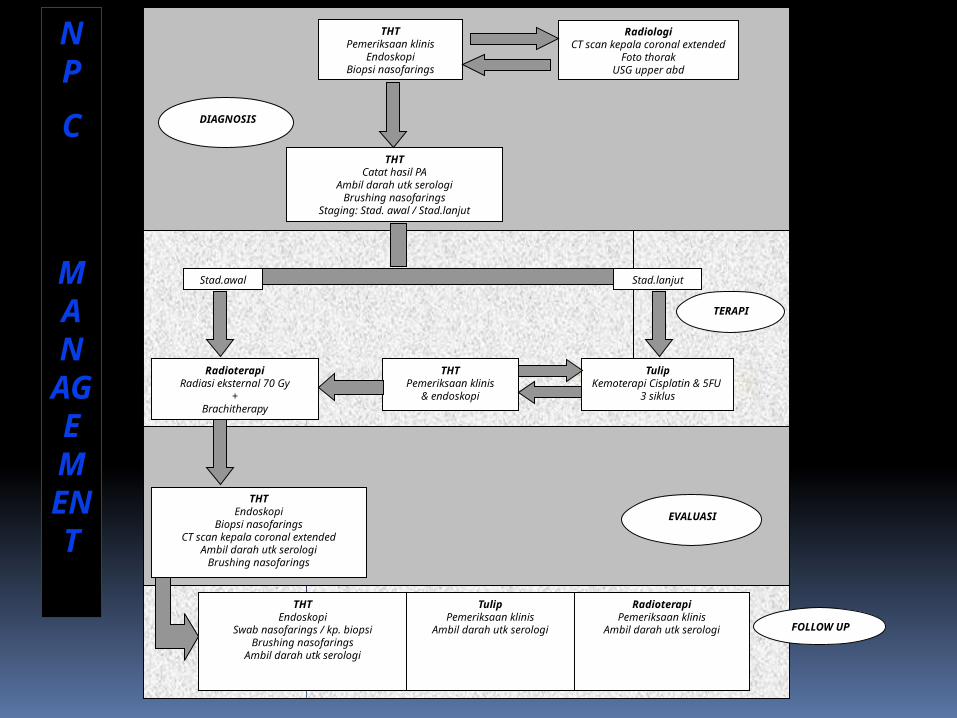
Stad.awal
RadiologiCT scan kepala coronal
extendedFoto thorak
USG upper abd
THTPemeriksaan klinis
EndoskopiBiopsi nasofarings
Stad.lanjut
THTCatat hasil PA
Ambil darah utk serologiBrushing nasofarings
Staging: Stad. awal / Stad.lanjut
RadioterapiRadiasi eksternal 70 Gy
+Brachitherapy
TulipKemoterapi Cisplatin &
5FU 3 siklus
THTPemeriksaan klinis
& endoskopi
THTEndoskopi
Biopsi nasofaringsCT scan kepala coronal extended
Ambil darah utk serologiBrushing nasofarings
TulipPemeriksaan klinis
Ambil darah utk serologi
THTEndoskopi
Swab nasofarings / kp. biopsiBrushing nasofarings
Ambil darah utk serologi
RadioterapiPemeriksaan klinis
Ambil darah utk serologi
DIAGNOSIS
TERAPI
EVALUASI
FOLLOW UP
NP
C
MANAGEMENT

2
weeks
Potentially DO Diagnosis
Early stage
Advanced stage
Radiotherapy Chemotherapy
Radiotherapy
Response Assessment
Follow-up
12 weeks
12 weeks
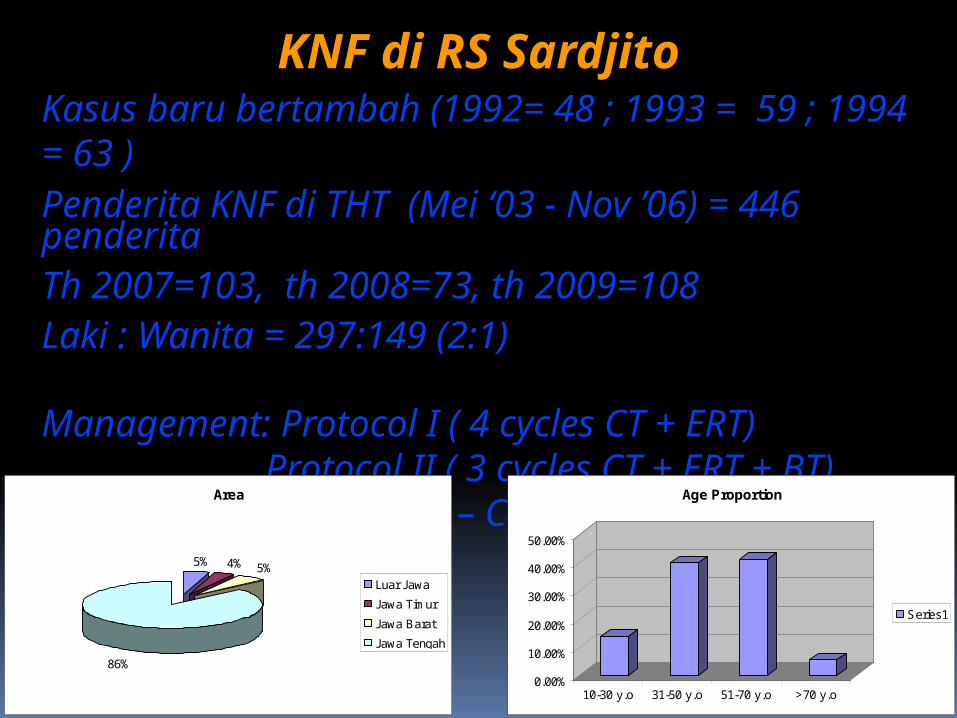
Kasus baru bertambah (1992= 48 ; 1993 = 59 ; 1994 = 63 ) Penderita KNF di THT (Mei ‘03 - Nov ’06) = 446 penderitaTh 2007=103, th 2008=73, th 2009=108Laki : Wanita = 297:149 (2:1)
Management: Protocol I ( 4 cycles CT + ERT) Protocol II ( 3 cycles CT + ERT + BT) Protocol III – Concurrent Chemoradiation
KNF di RS Sardjito
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
10-30 y.o 31-50 y.o 51-70 y.o >70 y.o
Age Proportion
Series1
Area
5% 4% 5%
86%
Luar Jawa
Jawa Timur
Jawa Barat
Jawa Tengah

Sardjito’s standard therapy protocols(Advanced stage)
Protocol I:
Chemotherapy :Neoadjuvant.CisPlatinum : 80 mgr/m2 body surface5 Fu : 800 mgr/m2 body surface 4 cycles
Radiotherapy :Cobalt 606600 – 7000 cGy
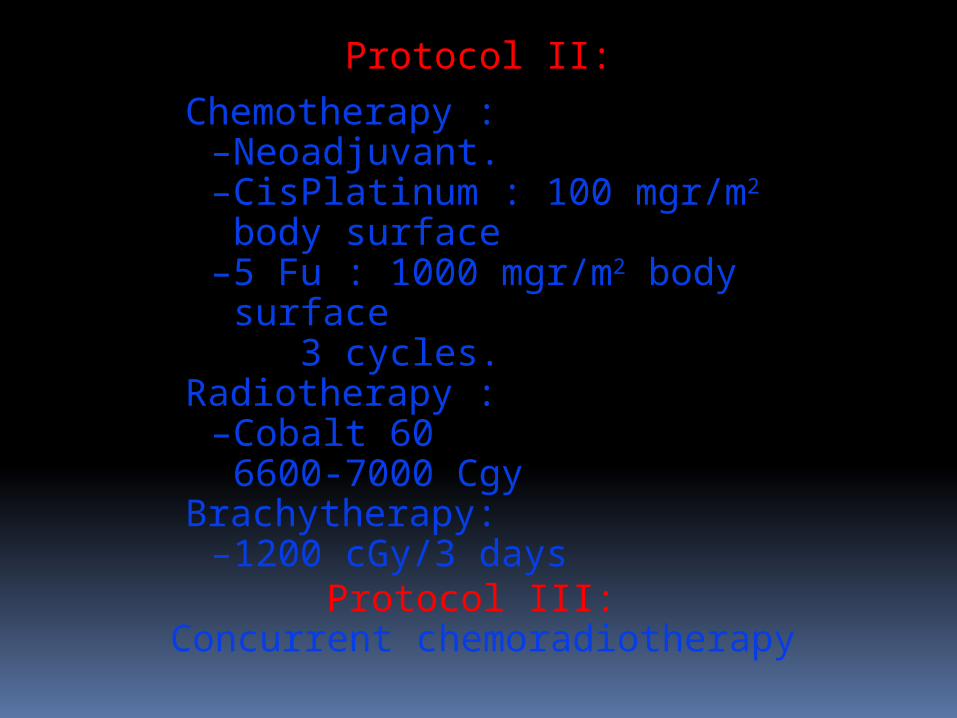
Protocol II:
Chemotherapy :–Neoadjuvant.–CisPlatinum : 100 mgr/m2 body
surface–5 Fu : 1000 mgr/m2 body surface
3 cycles.Radiotherapy :
–Cobalt 606600-7000 Cgy
Brachytherapy:–1200 cGy/3 days
Protocol III: Concurrent chemoradiotherapy
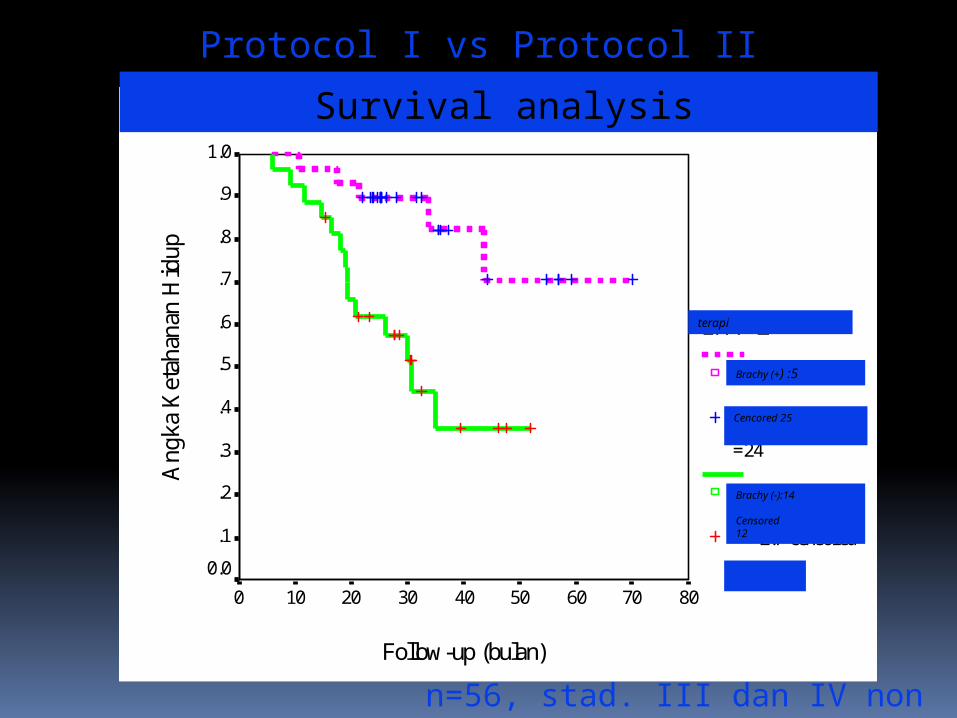
log rank=8,60; p=0,003
Follow-up (bulan)
80706050403020100
Ang
ka K
etah
anan
Hid
up1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
LMP 2
< 2.7=5
< 2.7-censored
=24
>= 2.7=14
>= 2.7-censored
=13
terapi
Brachy (+) :5
Brachy (-):14
Censored12
Cencored 25
n=56, stad. III dan IV non metastasis
Protocol I vs Protocol II
Survival analysis
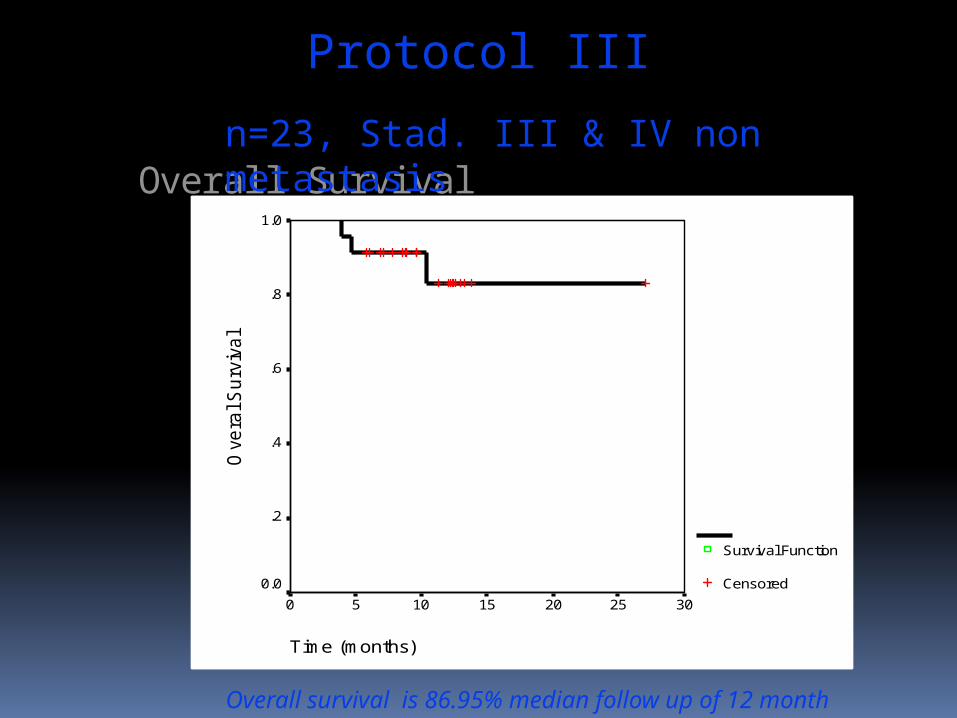
Overall Survival
Time (months)
302520151050
Ove
ral S
urv
iva
l1.0
.8
.6
.4
.2
0.0
Survival Function
Censored
Overall survival is 86.95% median follow up of 12 month
n=23, Stad. III & IV non metastasis
Protocol III
Photodynamic Therapy in Recurrent or Residual Disease of Nasopharyngeal
Carcinoma After Standard Therapy in Sardjito Hospital Yogyakarta:
5-year Experience
Sagung Rai Indrasari1, Camelia Herdini1, Bambang Hariwiyanto1, Tan IB2
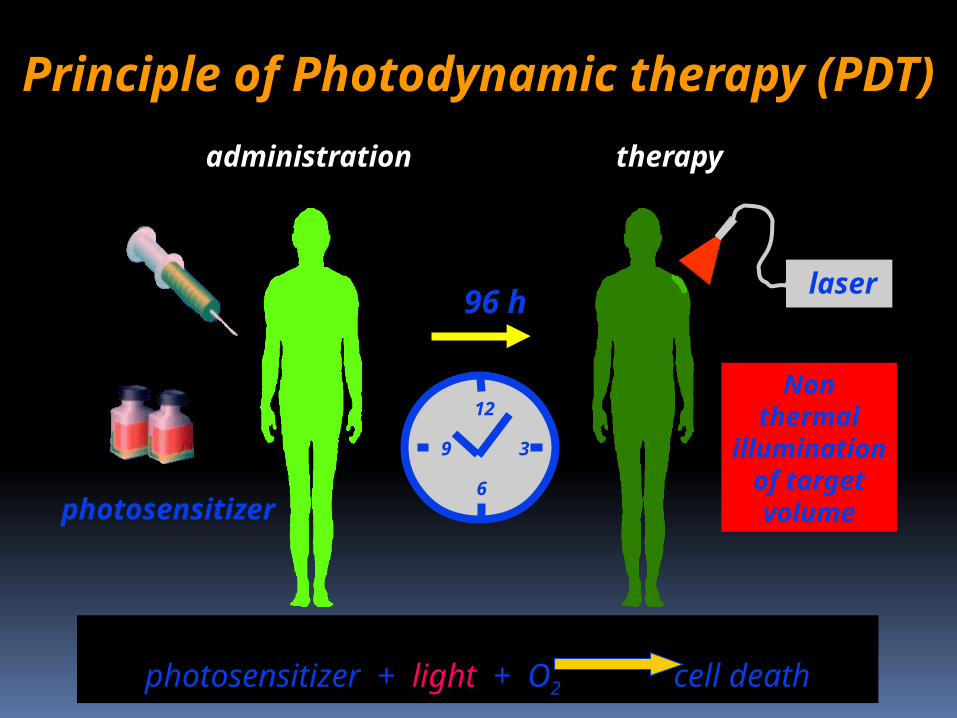
administration
photosensitizer
laser
therapy
96 h
12
6
9 3
Non thermal illumination
of target volume
Principle of Photodynamic therapy (PDT)
photosensitizer + light + O2
cell death
42
Follow Up (Months)
4035302520151050
Cu
m S
urv
iva
l1.0
.9
.8
.7
.6
.5
.4
.3
.2
.1
0.0
Survival Function
Censored
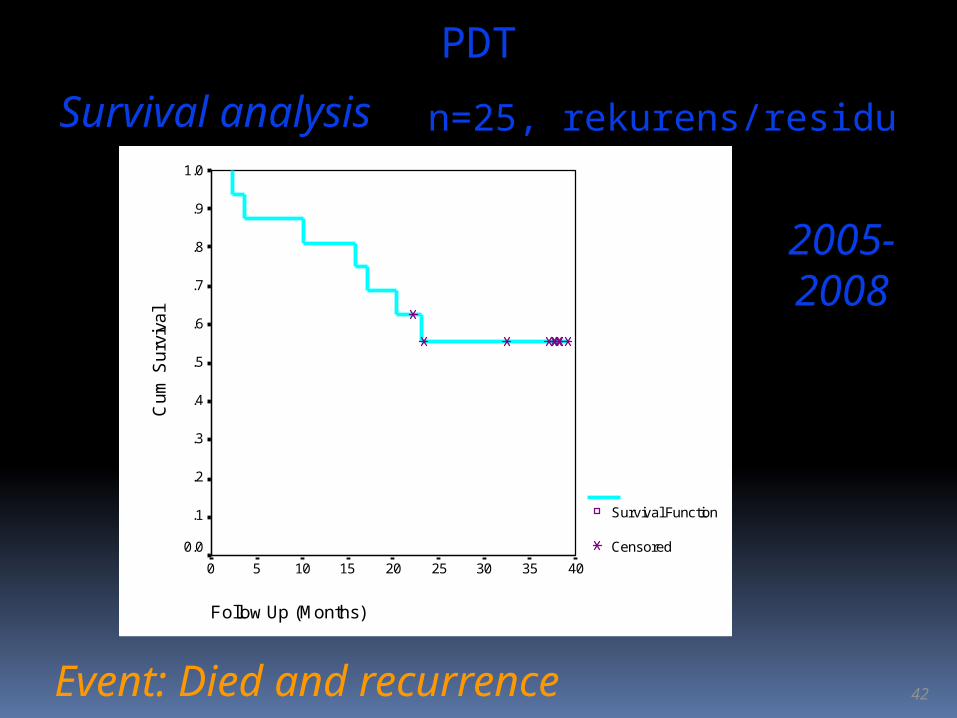
Survival analysis
Event: Died and recurrence
n=25, rekurens/residu
2005-2008
PDT
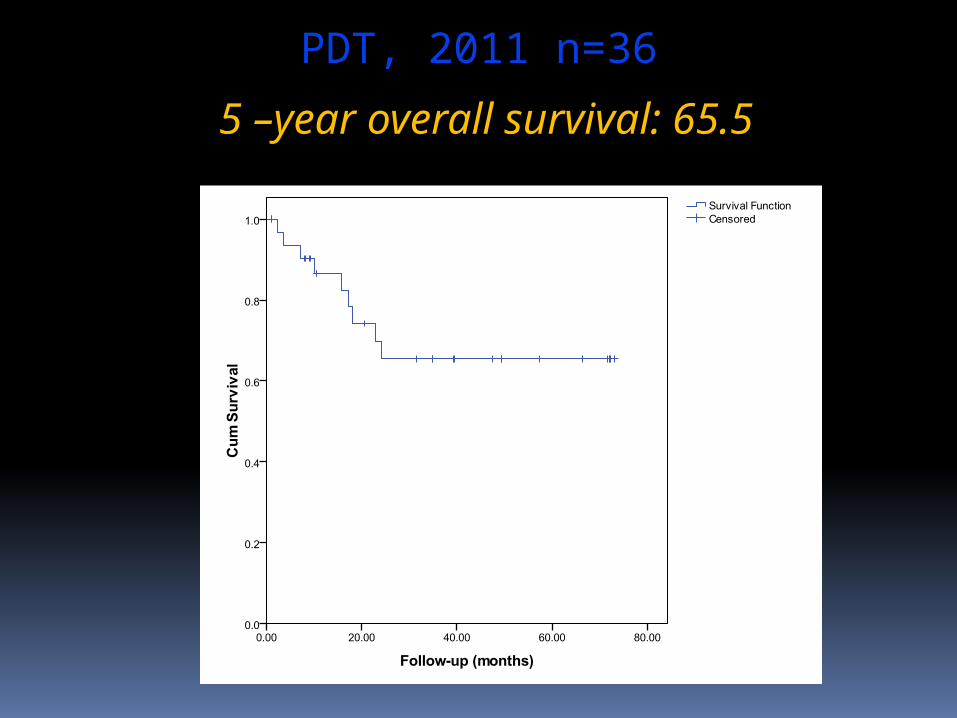
5 –year overall survival: 65.5
PDT, 2011 n=36
Advanced stage diseases need longer treatment
time potentially DO !
In advanced diseases, treatment results are poor
Important !
Diagnosis in early stage
NO DELAY !!
Delay in the diagnosis & treatment of NPC:Patient delayProfesional delay:
Gagal mengidentifikasi gejala & tanda kecurigaan kanker
System delay:Waktu yg diperlukan utk mendpt pelayanan
kesehatan primer / RSWaktu yg diperlukan utk referal ke pelayanan
tertier
EARLY DIAGNOSISAWARENESS
(of symptoms and signs)
Stadium dini Stadium lanjut
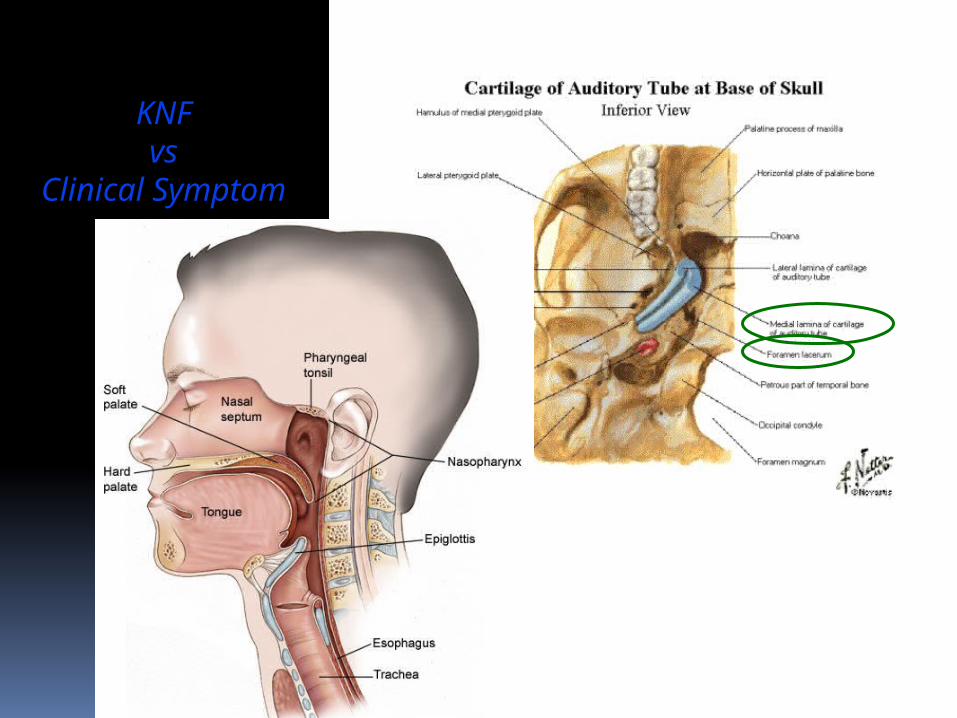
KNFvs
Clinical Symptom
GEJALA KLINIS
Cefalgia
Diplopia Ophtalmoplegia Lagophtalmus
Obstruksi hidung Sekret + darah Anosmia Blood
stained discharge PND Trismus Disfagia Gangguan
pengecap Atrofi palatum mole Parese parsial lidah
Limfadenopati collie
Rasa penuh di telinga Tinnitus Otalgia
Tuli konduktif unilateral Perforasi OME
AWAL LANJUT
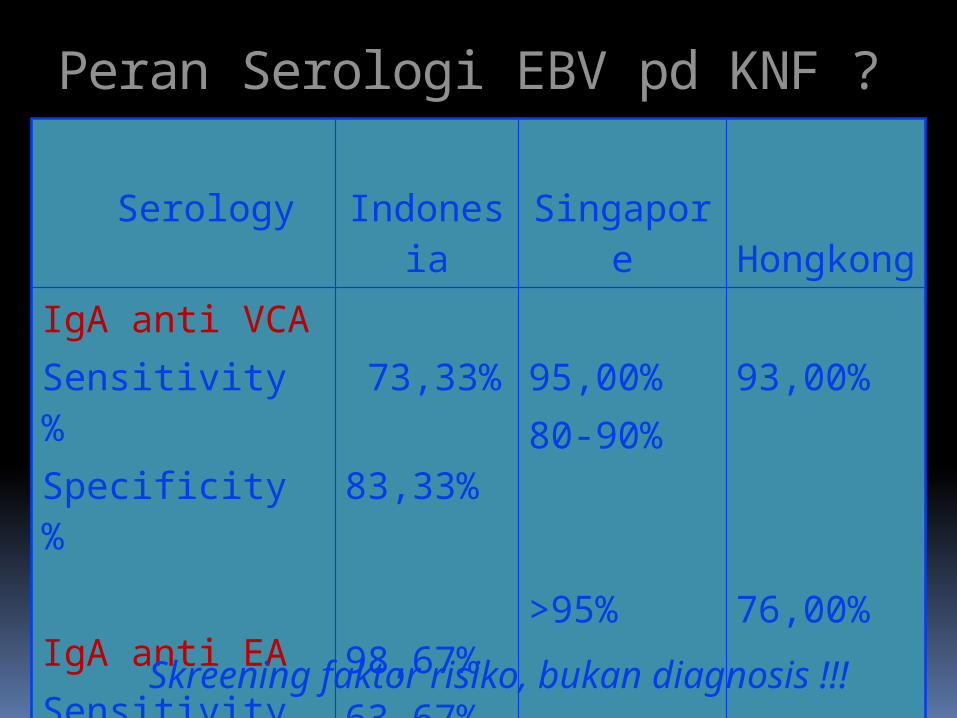
Peran Serologi EBV pd KNF ?
Serology
Indonesia
Singapore Hongkon
gIgA anti VCASensitivity %Specificity %
IgA anti EASensitivity %Specificity%
73,33% 83,33%
98,67% 63,67%
95,00%80-90%
>95%
93,00%
76,00%
Skreening faktor risiko, bukan diagnosis !!!
Early diagnosis- “difficult”
Tumor : non specific symptoms sub mucosal
Medical expert : low index of suspiciousness technical exam of nasopharynx
Deteksi dini pada penderita dg faktor risiko
Annual physical examination Special attention to upper aerodigestive
tract and neck with digital examination of oral cavity
Referral for evaluation of unexplained symptoms
Follow-up for patient with risk factor
Stupp R, Vokes EE. Current Cancer Therapeutics. 3rd ed. 1998;165.
Skreening penderita dengan risiko
Rendahnya tingkat partisipasi penderita berisiko dlm program skreening
Kondisi subklinis/tanpa gejala yg lama
Faktor waktu dan perlu edukasi di seting di pelayanan kesehatan primer
Pd umumnya tdk berhasil krn:
Schantz SP, et al. Cancer: Principles & Practice of Oncology. 6th ed. 2001;797-860.
UPAYA PENCEGAHANJaga daya tahan tubuh
Cegah ISPA
Skrining pasien risiko tinggi
Kurangi makanan dengan pengawet
Kurangi pemakaian alat rumah tangga yang mengandung karsinogen
Hindari rokok (aktif + pasif), terutama di sekitar anak-anak
KEYPOINTS
•KNF kasus terbanyak di kepala leher
•Stadium dini prognosis lebih baik
•Skrining pasien risiko tinggi
•Rekuren terjadi < 1 tahun
•Follow up rutin: KEHARUSAN
•Program kewaspadaan

TERIMA KASIH
















![Nasopharyngeal Carcinoma [Ind] - Fix 19](https://img.pdfslide.net/doc/110x75/55cf9043550346703ba47221/nasopharyngeal-carcinoma-ind-fix-19.jpg)










