Embed Size (px)
Citation preview

Prevention of Breast Cancer Breast Diseases Fourth Edition, chapter 6
screening
• reduce mortality but not the incidence• cost effective only among women for whom breast cancer is common (2-
3/1000 per year)
Hormonal and cytotoxic treatment
• significant survival benefits
Life style
• as well as surgical and medical therapeutic interventions
Management options for women at significantly increased risk of breast cancer
• Take no action
• Try to reduce risks:
◦ Plan family early
◦ Avoid OCP and HRT use
◦ Good diet and regular exercise
◦ Delaying menarche
◦ Artificial early menopause (oophorectomy or treatment with goserelin)
◦ Anti-oestrogen therapy (tamoxifen)
Tamoxifen:
the agent of choice for preventive therapy, especially in:
premenopausal high-risk women atypical hyperplasia
lobular carcinoma in situ (LCIS)
Overview of four large trials:
1. 43% reduction in ER-positive invasive cancer
2. no impact on ER-negative disease
3. a reduced incidence in the period after active treatment was completed, with an additional 38% reduction in years 6–10.
4. As side effects were minimal in the post-treatment period, the risk–benefit ratio has improved with longer follow-up
Selective estrogen receptor modulators(SERMs)

Raloxifen: a marked decrease in breast cancer incidence a greater benefit than tamoxifen direct comparison with tamoxifen in the STAR trial at 81 months
indicated that the risk ratio of raloxifene:tamoxifen was 1.24 for invasive cancer and 1.22 for non-invasive disease
Adverse events were less common: endometrial cancer, endometrial hyperplasia and thromboembolic events.
a significant decrease in ER-positive breast cancers
lasofoxifene and arzoxifene
None of the SERMs has demonstrated any impact on oestrogenreceptor-negative tumors.
particularly in BRCA1/2 carriers about 40 years of age reduce subsequent breast cancer risk by approximately 50% Early menopause and Long HRT
salpingo-oophorectomy
2842 women with mutation247: prophylactic mastectomy, no breast cancer to date1372: no prophylactic mastectomy98 (7.1%) diagnosed with breast cancerSalpingo-oophorectomy reduced breast cancer risk in 1372 women with
intact breasts in:BRCA1 carriers from 20 →14%BRCA2 carriers from 23 →7%Ovarian cancer mortality fell with oophorectomy from3–0.4% HR 0.21 (95% CI 0.06–0.80)
Role of prophylactic mastectomy and salpingo-oophorectomy in BRCA mutation carriers.
Aromatase inhibitors (AI)
overall reduction of 50%compared to tamoxifen suggesting a potential 75% reduction overall.
Other agents Bisphosphonates
30% lower breast cancer incidence. may have a greater effect in ER-negative breast cancer
Metformin: in women with type 2 diabetes have shown a reduced risk of breast
cancer
Aspirin: a chemopreventive effect of aspirin for a number of cancers about 10% reduction of breast cancer risk for aspirin and a possibly a
little more for Ibuprofen.
Other NSAIDs COX-2 inhibitors statins
Regular screening Annual mammographic breast screening will identify over 60% of
cancers in young women, but interval cancers do occur.
economic grounds in young age group
MRI is limited to very high-risk women: BRCA1/2 and TP53 mutation carriers aged 30–49 very high-risk individuals without mutations
MRI scanning for women at high risk.
Three studies (from the United Kingdom, the Netherlands and Canada) have shown MRI to be a better screening tool than mammography.
The UK study used 949 women aged 35–49 years with a strong family ∗history or proven genetic mutation. Thirty-five cancers were found by annual screening
• 77% detected by MRI
• 40% detected by mammography
• 94% detected by either MRI or mammography
• Mammography was more specific (93%) than MRI (81%)
Prophylactic surgery reduces the risk of breast cancer in BRCA mutation carriers
by 90% psychosocial and emotional issues Nipple-sparing mastectomy with reconstruction skin and nipple-areola sparing mastectomy and areola
sparing mastectomy
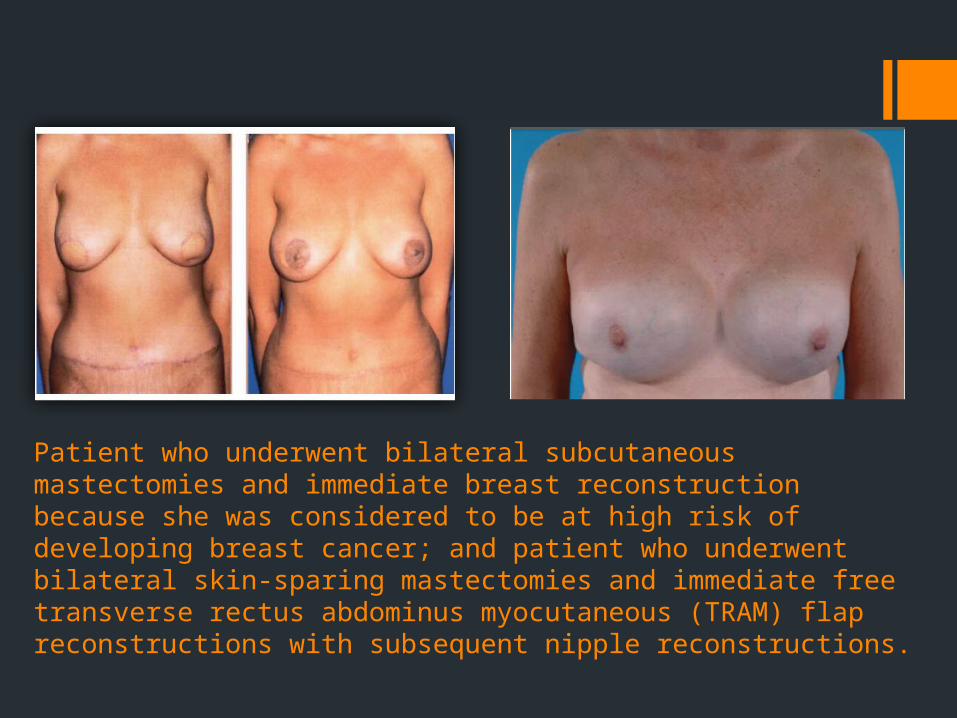
Patient who underwent bilateral subcutaneous mastectomies and immediate breast reconstruction because she was considered to be at high risk of developing breast cancer; and patient who underwent bilateral skin-sparing mastectomies and immediate free transverse rectus abdominus myocutaneous (TRAM) flap reconstructions with subsequent nipple reconstructions.
Ovarian cancer
Transvaginal ultrasound CA125 Annual Pelvic examination
in general the sensitivityis only found to be 60% with no reduction in mortality.
Women who carry a BRCA1/2 mutation should be advised to undertake bilateral salpingo-oophorectomy once their family is complete.

Men with BRCA1 and BRCA2 mutations
BRCA2 mutation carriers lifetime risk of breast cancer, 6–8% compared with 0.1% for men who are not carriers.
risk of prostate cancer is increased to 4.7 times higher breast screening annual prostate screening from age 40 (blood PSA level)
BRCA1 carriers are probably not at any increased risk of cancer overall.

Thanks for your attention…