Embed Size (px)
Citation preview

Dr.Niharika Singh Gandhi Medical College Bhopal


There is observation of hepatic progenitor cell features in hepatocellular neoplasms at an early stage (dysplastic nodules) or advanced tumours with mixed hepatocellular and cholangiocellular phenotypes.

The 4th edition of the WHO classification of tumours of the digestive system


Regenerative hepatocellular nodules
Boundaries consist usually of fibrous septa, collapsed reticulin strands, multilobular areas of parenchymal collapse, atrophic hepatic plates, other nodules or a combination of the above.

Acetaminophen Toxicity

29 days
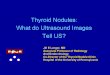
Serial biopsies from native liver during its recovery phase following auxiliary transplantation
Acute necrosis with sparing of periportal hepatocytes results in an initial phase of hepatocellular proliferation, acute inflammation and reticulin collapse with parenchymal nodular transformation.

Acute liver failure due to acetaminophen overdose
146 days

350 days
Resolution of inflammation, matrix reabsorption and hepatic plates remodelling and growth lead eventually to full reconstitution of the liver mass, involution of the graft and withdrawal of immunosuppression.

Regenerative nodule in nodular regenerative hyperplasia. The nodular area is flanked by atrophic plates with condensation of reticulin fibres but no bridging fibrosis.

Regenerative nodule in advanced stage chronic hepatitis C. The nodular area is surrounded by bridging fibrous septa..
In chronic hepatitis C, the nodules are of small size due to porto-portal and porto-central bridging with loss of the vascular anatomical relationships .Two cell- thick hepatic plates are often present, and there may be deposition of granules of copper-binding protein at the interface with the fibrous septa which is an indirect sign of advanced fibrosis may be helpful in the interpretation of core needle biopsy specimens, in which nodule formation is not readily apparent due to the small size of the sample or the large size of the nodules or both.

Primary biliary cirrhosis.Bridging fibrosis linking up portal tracts generate a ‘jigsaw puzzle’ pattern rather than round nodules.

Primary sclerosing cholangitis. Marked segmental hypertrophy and lateral atrophy lead to severe distortion of the lobar anatomy.

Benign hyperplastic regenerative proces secondary to a local abnormality of blood flow due to a vascular malformation such as:
Budd–Chiari syndrome, hereditary haemorrhagic telangiectasia, portal vein thrombosis/ atresia, congenital portosystemic shunt.
Polyclonality, increased ANGPT1/ANGPT2 ratio. Usually solitary, but multiple vascular malformations and
coexist with intracranial tumour. Develops in noncirrhotic livers of women 30–40 years
FNH is usually the easiest to differentiate, due to its architecture and bland appearance of lesional hepatocytes.

Macroscopically, FNH can range in size from a few mm to several cm. It usually shows a pale, micronodular and firm parenchymal surface, with or without a central scar.There is usually no capsule, the periphery of the lesion merging with the adjacent liver .

Microscopically, it consists of nodules of benign-looking hepatocytes separated by fibrous septa containing a ductular reaction, a lymphoid infiltrate and aberrant vascular structures.

A 32-year-old woman transplanted for glycogen storage disease type 1. A 10-mm hepatocellular adenoma showed diffuse staining for glutamine synthetase.
No nuclear or cytoplasmic staining for β-catenin was identified.
Please note background liver on the right hand side showing normal glutamine synthetase expression by perivenular hepatocytes.
52-year-old woman. Liver resection for focal nodular hyperplasia. The pattern of glutamine synthetase is typically ‘map like’.

An important practical point is the identification of a regenerative nodule in a core needle biopsy specimen, as the changes can be very subtle and easily overlooked.
Signs representing that the needle has hit a regenerative area:
1)Two-cell-thick hepatic plates in biopsy cores from adult patients.2)Thin hepatic plates sometimes in a parallel configuration.3)Sinusoidal dilatation without other accompanying features of venous outflow blockage.4)Few focal deposits of copper binding protein on the orcein/ Victoria blue stain without other signs of biliary pathology. *A full clinical history, close correlation with imaging findings and ideally an adequate sample of lesional tissue along with a separate sample of non-lesional tissue to assess the status of background liver should be the basis for the histological interpretation of liver nodules.

DYSPLASTIC NODULES Nodules of relatively small size, up to about
10–15 mm,identified in cirrhotic livers, and showing atypical histological features without fulfilling the criteria of HCC.
These nodules are thought to be HCC precursors, based mainly on the following observations:
Their occurrence in livers affected elsewhere by overt HCC. The identification of small nodular lesions with atypical features
and containing foci of overt HCC (nodule-in-nodule pattern).
Similarities at molecular level with HCC. Clinicopathological studies based on biopsy and clinical follow-up
suggesting their transformation into HCC. Change in their vascular supply. Histologically,associated with the presence of unpaired
arteries and sinusoidal capillarisation marked by the CD34 immunohistochemical marker.

Additional stains, which can be of help in identifying the porto-lobular relationship, are immunohistochemistry for cytokeratins (e.g. Ker 7) glutamine synthetase
*To highlight portal regions and centrilobular venules, respectively.
Degree of sinusoidal capillarisation by CD34 immunostaining.

Arterialisation is exploited radiologically by demonstrating contrast uptake in arterial phase and rapid washout in the venous phase to the point that demonstration of arterialisation by one or two imaging modalities is considered to be sufficient for the diagnosis of HCC without the need of histological confirmation.
The use of liver biopsy is therefore confined to lesions with atypical features on imaging.
According to a recent consensus paper, dysplastic nodules are further subdivided into
Low-grade lesions: may be indistinguishable from large regenerative nodules, differing only by the focal presence of some of the dysplastic changes.
High-grade lesions:nodules may be indistinguishable from early HCC probably because they represent part of a continuum.

Macroscopically, dysplastic nodules are distinct from the background liver in terms of their size, appearance, colour, texture and/or bulging cut surface.
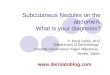
Dysplastic nodule in cirrhotic liver showing a nodule- in nodule pattern. The line of triangles marks the boundary of the nodule against the background liver. The arrow indicates an area of increased cell density.

• Changes in Nodule in Nodule pattern include 1)Siderosis2)Copper/copper-binding protein deposits3) Steatosis4)Clear cell change5)Mallory–Denk bodies6)Increased trabecular thickness7)Pseudoglandular structures8)Nuclear hyperchromasia or irregularity
of the nuclear contour,9)Cytoplasmic basophilia10) Increased proliferative rate within areas of a nodule
or compared with background liver and loss of the reticulin stroma.

11)Large cell change, originally called liver cell dysplasia : Present in association with chronic liver disease Hepatocytes show large atypical nuclei with preserved nuclear cytoplasmic ratio. Risk of development of HCC, particularly in patients with viral hepatitis, Associated with cholestasis and senescence More than one pathogenesis . 12)Small cell change Areas of increased cell density due to a reduction in hepatocyte size Increased
nuclear– cytoplasmic ratio Associated with nuclear hyperchromasia Irregularity of the nuclear contour. True precursor of HCC. A relationship between small cell change and progenitor cells has been
proposed on the basis of a similar immunohistochemical profile. Small cell change and large cell change are part of a constellation of histological
changes which may indicate an increased risk of HCC. The general view is that these changes should at least be mentioned in a
histology report as they may indicate an increased risk of HCC.

Recent molecular studies have led to the introduction of an immunohistochemical panels including:
Heat-shock protein 70, Glypican 3 Glutamine synthetase Deemed to be useful in differentiating dysplastic nodules
from overt HCC.
• Clathrin heavy chain and annexin-A2 have been shown to improve the performance of this panel.
Gene expression profiling has recently produced a prognostic gene expression signature to predict the development of HCC.
Lack of staining with all markers high-grade dysplastic noduleStaining for one marker well-differentiated HCC but does not
exclude a high-grade dysplastic noduleStaining for two or three markers well-differentiated HCC

Rather than separating categorically dysplastic nodules from HCC, the currently accepted view is that HCC development and the transition between dysplasia and HCC can be defined by three phases :

Hepatocellular adenoma
Benign neoplasm of hepatocytes Risk factors- Exposure to oestrogens . Exposure to androgens. Glycogen storage disorders. Familial adenomatous polyposis. Can be single or multifocal, in which case the term ‘adenomatosis’ may apply.HCAs vary in size and are usually fairly well circumscribed, with a soft cut surface often similar to background liver, although in many cases areas of haemorrhage, necrosis or fibrosis may be present.Immunohistochemistry for serum amyloid A or C-reactive protein is usually helpful, as they are both strongly expressed in inflammatory adenoma, ,in contrast to FNH or background liver which are negative.

Hepatocellular adenoma subclassification
Category Histological features
Clinical features
β-catenin mutated
Pseudacinus formation, atypia
Malignant transformation, bleeding. usually in men.
HNF1 mutated Steatosis, FABP deficient
Bleeding
Inflammatory adenoma (formerlytelangiectatic FNH)IL6ST gene mutations
Intralesional lymphocytosis, ductules(ck7+ve) and sinusoidal dilation (telangiectasia) SAA and CRP positive
Bleeding, a percentage bearsβ-catenin mutation. Systemicsyndrome. Associated with alcohol,metabolic syndrome
Unclassified Nonspecific features Variable

Hepatocellular carcinoma More common in males. Risk factors: Hepatitis B and C virus infection Alcohol Aflatoxin Patients taking anabolic steroids Children with inherited metabolic conditions such as tyrosinaemia, hypercytrullinaemia, biliary atresia, Byler’s disease, BSEPdeficiency and a-1-ATdeficiency.
Term ‘satellite’ is commonly used to describe the presence of small tumoural nodules in the vicinity of the main mass.

Microscopically: Resemble to normal hepatocytes. Can be very heterogeneous Characterised by areas with different growth patterns and degree of differentiation. Tumour cells are often arranged in trabecular,pseudoacinar or solid pattern. Well-differentiated HCC Resembles normal hepatocytes with a similar nuclear–cytoplasmic ratio, similar nucleolated nuclei, well-demarcated cell borderseosinophilic cytoplasm.The cytoplasm may show steatosis or
clarification, and sometimes accumulation of Mallory–Denk bodies, or eosinophilic globular inclusions.
Formation of canalicular bile plugs is a diagnostic feature of HCC, although nonlesional cholestatic hepatocellular rosettes may become entrapped within the tumour and mistaken for a tumour component.
• HCC can grow inside large bile ducts

HCC can grow into three main patterns -Nodular,infiltrative pattern and diffuse pattern.
1) The nodular pattern is the one usually observed in cirrhotic liver and consists of an expanding mass well demarcated from the surrounding tissue often by interposition of a capsule and with a multilobulated cut surface.
2) The infiltrative pattern is usually observed in noncirrhotic livers and consists of a large mass which occupies a good proportion of a lobe or more than one lobe. The term ‘massive’ also applies to tumours of this size. There is often involvement of large portal vein branches.
3) HCC in a diffuse pattern is rare, usually observed in cirrhotic Livers and consists of multiple nodules which may mimic the cirrhotic nodules, may not be visible on imaging and difficult to identify macroscopically. The term ‘cirrhotomimetic’ is often used to describe this pattern.

Regression of fibrosis does not eliminate the risk of HCC. HCC can occur in chronic viral hepatitis at a precirrhotic stage.
Cirrhosis is the main risk factor for HCC, but HCC can arise in noncirrhotic livers. This may occur in the context of the metabolic syndrome, or other factors (iron overload, past exposure to HBV, androgens), and occasionally without any signs of liver disease.
HCC tends to be larger in noncirrhotic patients than in cirrhotic ones, partly due to surveillance programmes in patients with chronic liver disease, leading to its identification at a relatively early stage.
Of note cholangiocarcinoma has been described in non-biliary cirrhosis.
In non-cirrhotic liver the differential diagnosis is usually with other primary epithelial or non-epithelial tumours(focal nodular hyperplasia, hepatocellular adenoma, cholangiocarcinoma, angiomyolipoma) or with metastases.

Some patients, however,may not have any risk factor or sign of liver injury .
The fibrolamellar variant of HCC is a well-recognised entity, which affects young adults, without
underlying history of liver disease. Characterised by Fibrous stroma Large Hepatoid tumour cells Eosinophilic cytoplasm Cytoplasmic inclusions Scanty mitotic activity. A recent series has shown that fibrolamellar carcinoma does
not have a better survival than conventional HCC in children. Peculiar radiological and histological characteristics, spread and
behaviour, and its pathogenesis remains obscure.

The histological appearance of HCA and well-differentiated HCC can overlap considerably. Of note, well differentiated HCC can appear very bland, and HCA secondary to hormonal stimulation can show marked atypia, but regresses following hormonal withdrawal.
There are no individual diagnostic histological features or immunohistochemical markers that can be used reliably and in isolation to distinguish between HCA and well-differentiated HCC.
The diagnosis of HCC in cirrhosis is now clinical in most cases; the role of histology in the diagnosis of dysplastic nodule and early HCC depends on local clinical practice.
The inflammatory/telangiectatic variant may need to be differentiated from FNH. The distinction between HCA and HCC may be challenging.

Other variants include Lymphocyte-rich Clear cell, scirrhous Sclerosing HCC. The term mixed or combined hepatocholangiocellular carcinoma refers to tumours
with mixed hepatocholangiocellular phenotype, or tumours with progenitor cell features.
Lack of bile, no demonstrable canaliculus formation or Hep-Par 1 expression by IHC, in the presence of mucus production, cytoplasmic staining for CEA, CA19-9 and biliary cytokeratins favour cholangiocarcinoma.
The presence of adenocarcinoma with a typical tubulo-glandular pattern, in a core needle biopsy from a lesion clinically suspected as HCC, raises the possibility of a mixed (combined) hepatocellular-cholangiocarcinoma.It can occur in non-biliary cirrhosis, and simulate clinically HCC.

Staining for CEA using a polyclonal antibody or CD10 is the most commonly used method to demonstrate canaliculus formation, but its expression is not hepatocellular specific.
Two recent studies have shown excellent specificity of BSEP expression in distinguishing between HCC and its extrahepatic mimics.
Glypican-3 may complement Hep-Par-1 in the diagnosis of poorly differentiated HCC , but it is expressed in non-neoplastic liver parenchyma and extrahepatic tumours , and should not be used in isolation.
Expression of stem cell markers,biliary cytokeratins and a gene expression profile similar to hepatoblast identifies a subtype of HCC with poor prognosis .

Angiomyolipoma Mimic histologically hepatocellular carcinoma. Diagnosis : HMB 45 Positive.
Many extrahepatic primary tumours infiltrating the liver can simulate hepatocellular carcinoma.Histologically and in particular
Adrenal cortical carcinoma Neuroendocrine tumours Renal cell carcinoma Melanoma Hepatoid adenocarcinoma (e.g. gastric origin). Clinical evidence of an extrahepatic primary and
immunohistochemistry are often sufficient for the diagnosis, but in some cases, the extrahepatic primary is too small to be detected clinically (e.g. neuroendocrine tumours), or the tumour is poorly differentiated and does not fit with any specific immunohistochemical profile.
Poorly differentatiated tumours of intestinal origin, and germ cell tumours may be associated with high serum levels of alpha-fetoprotein.

Future directions Recent studies using high-throughput molecular
techniques have classifiied HCC into subcategories associated with specific aetiologies and specific molecular pathways.
The application of genomic profiling to the investigation of HCC associated with rare conditions such as BSEP deficiency may lead to the identification of alternative carcinogenic pathways .
Proteomics profiling of liver tumours appears promising in identifying biomarkers, which can be exploited at diagnostic histological level or clinically for noninvasive diagnosis or to direct treatment .



















![Nodules & placards [Mode de compatibilité]](https://img.pdfslide.net/doc/110x75/5875f8651a28ab1a6c8bcb4a/nodules-placards-mode-de-compatibilite.jpg)