Embed Size (px)
Citation preview
Case Study 10
Christy C
Sheila M
Sydney T
The Toxic Invasion of Bacteria
Streptococcus pyogenes
Case Summary
☤ Age: 40
☤ Intravenous drug user
☤ Cellulitis found in right arm with large area inflamed and oozing
☤ Several weeks of experiencing fever and dizziness
☤ Cardiac exam shows abnormal EKG and systolic murmur
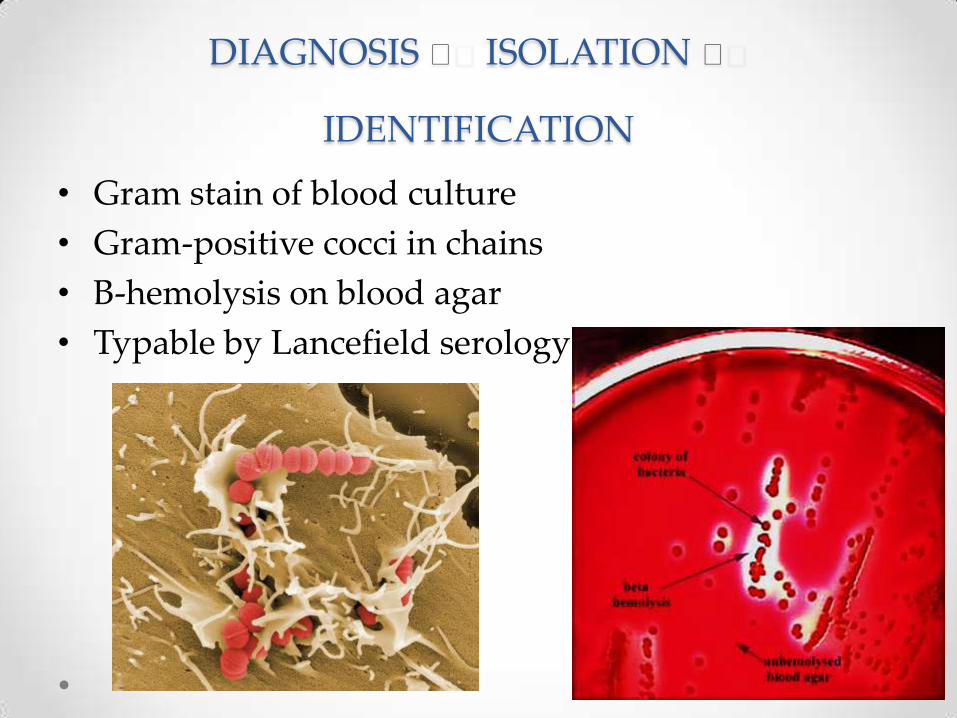
DIAGNOSIS 🔬 ISOLATION 🔬
IDENTIFICATION
• Gram stain of blood culture
• Gram-positive cocci in chains
• Β-hemolysis on blood agar
• Typable by Lancefield serology
Lancefield Serology
• The classification system of hemolytic Streptococci into groups, according to their action on blood cells
• Established in the 1930s by the renowned American microbiologist, Rebecca Lancefield
Lancefield Serology Classification
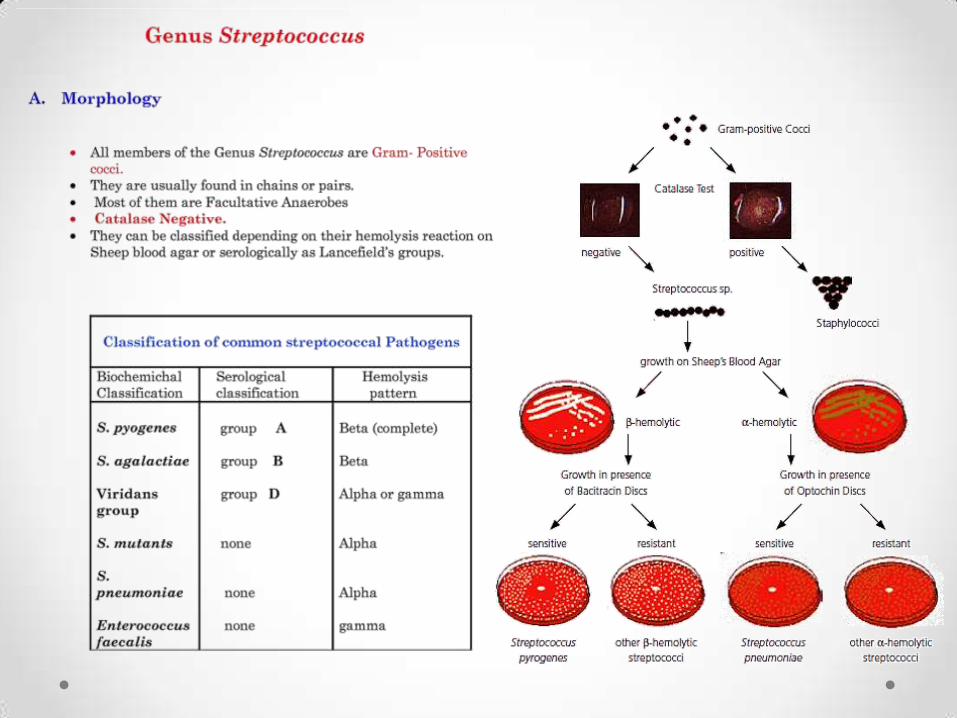
• Streptococci divide in one plane and thus occur in pairs or in chains or varying lengths
• The metabolism of S. pyogenes is fermentative
• The organism is a catalase-negative, aerotolerant anaerobe
• Requires enriched medium containing blood in order to grow
• Group A streptococcus (GAS) typically have a capsule composed of hyaluronic acid and exhibit beta hemolysis on blood agar
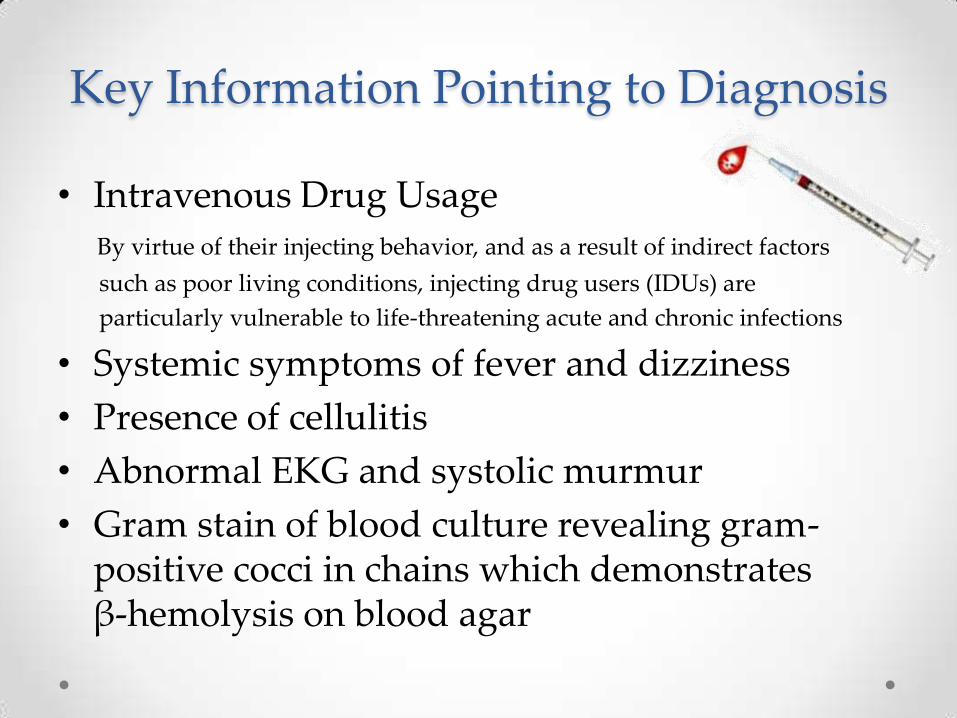
Key Information Pointing to Diagnosis
• Intravenous Drug Usage
By virtue of their injecting behavior, and as a result of indirect factors
such as poor living conditions, injecting drug users (IDUs) are
particularly vulnerable to life-threatening acute and chronic infections
• Systemic symptoms of fever and dizziness
• Presence of cellulitis
• Abnormal EKG and systolic murmur
• Gram stain of blood culture revealing gram-positive cocci in chains which demonstrates β-hemolysis on blood agar
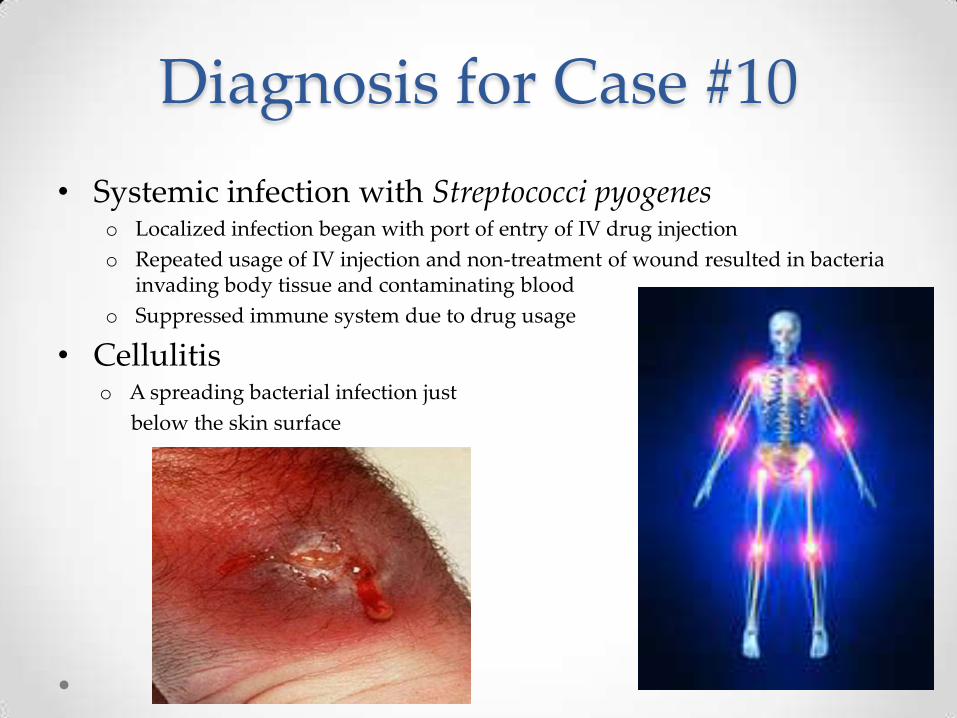
Diagnosis for Case #10
• Systemic infection with Streptococci pyogenes o Localized infection began with port of entry of IV drug injection
o Repeated usage of IV injection and non-treatment of wound resulted in bacteria invading body tissue and contaminating blood
o Suppressed immune system due to drug usage
• Cellulitiso A spreading bacterial infection just
below the skin surface
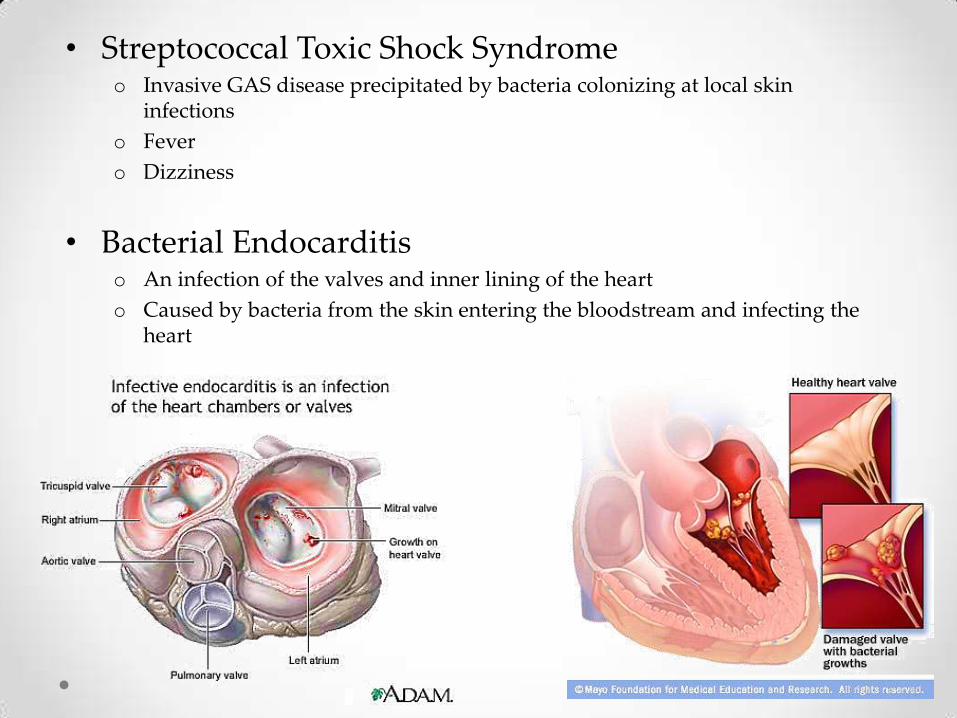
• Streptococcal Toxic Shock Syndromeo Invasive GAS disease precipitated by bacteria colonizing at local skin
infections
o Fever
o Dizziness
• Bacterial Endocarditiso An infection of the valves and inner lining of the heart
o Caused by bacteria from the skin entering the bloodstream and infecting the heart
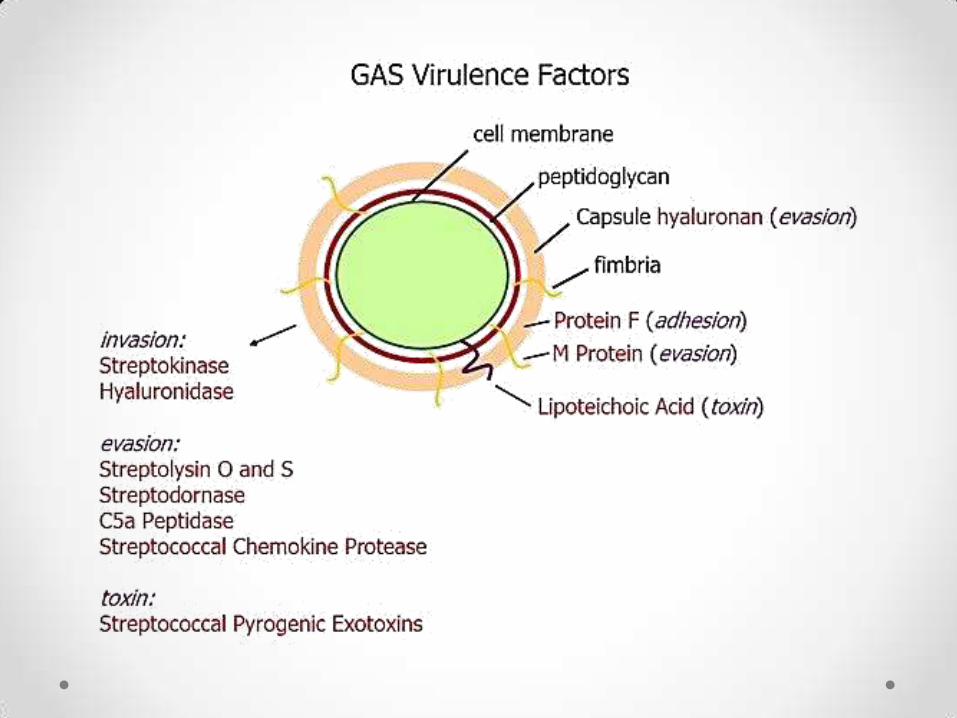
Virulence Factors
• M proteino Inhibits phagocytosis
• Lipoteichoic acido Adherence
• Hyaluronic acid capsuleo Immunological disguise & inhibits phagocytosis
• Invasionso Streptokinase enzyme catalyzes the conversion of plasminogen to plasmin
o Hyaluronidase enzyme that catalyzes the hydrolysis of hyaluronic acid
• Pyrogenic (erythrogenic) toxino Systemic toxic shock syndrome
Epidemiology
According to a report from the Centers for Disease Control and Prevention (CDC)
o Approximately 9,000-11,500 cases of invasive GAS disease occur each year in the United States
o Streptococcal TSS and necrotizing fasciitis each accounted for approximately 6-7% of cases
o More than 10 million noninvasive GAS infections
(primarily throat and superficial skin infections) occur annually
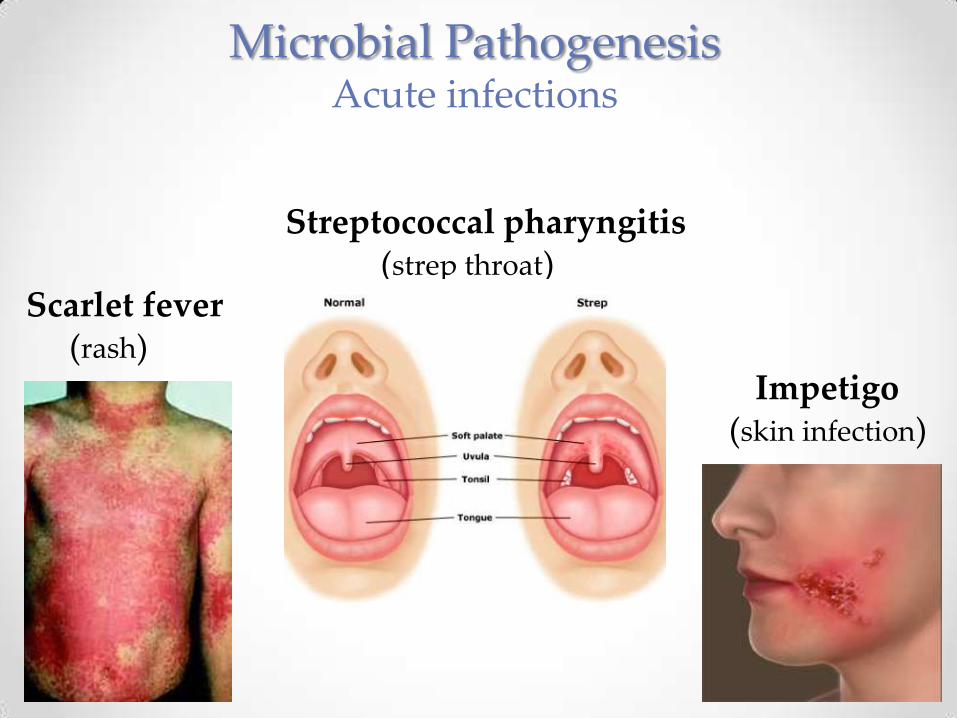
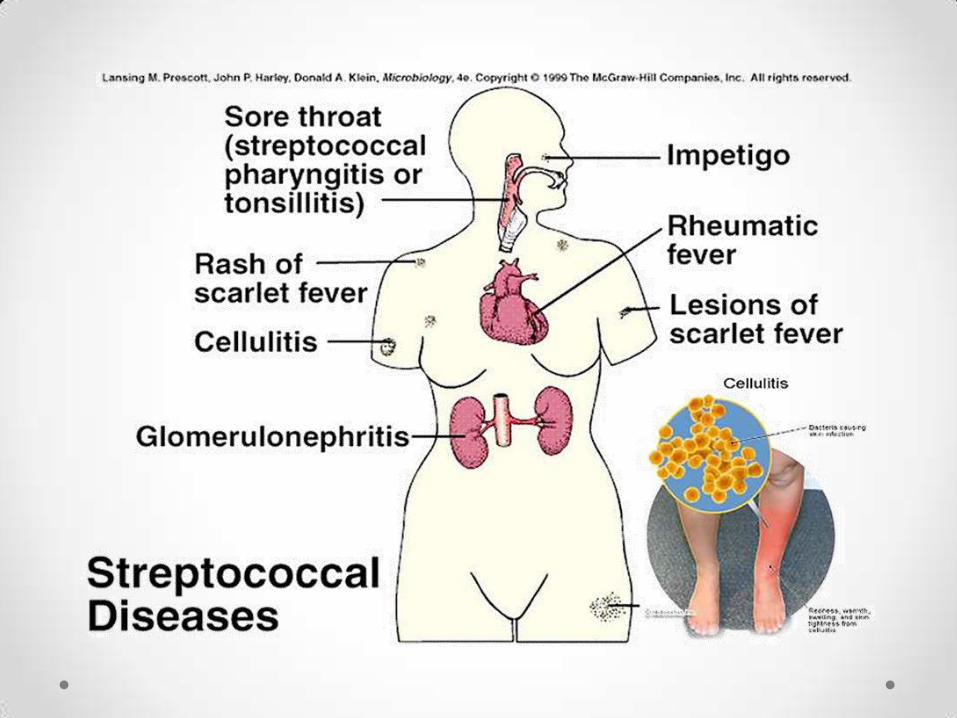
Microbial PathogenesisAcute infections
Streptococcal pharyngitis (strep throat)
Scarlet fever (rash)
Impetigo (skin infection)
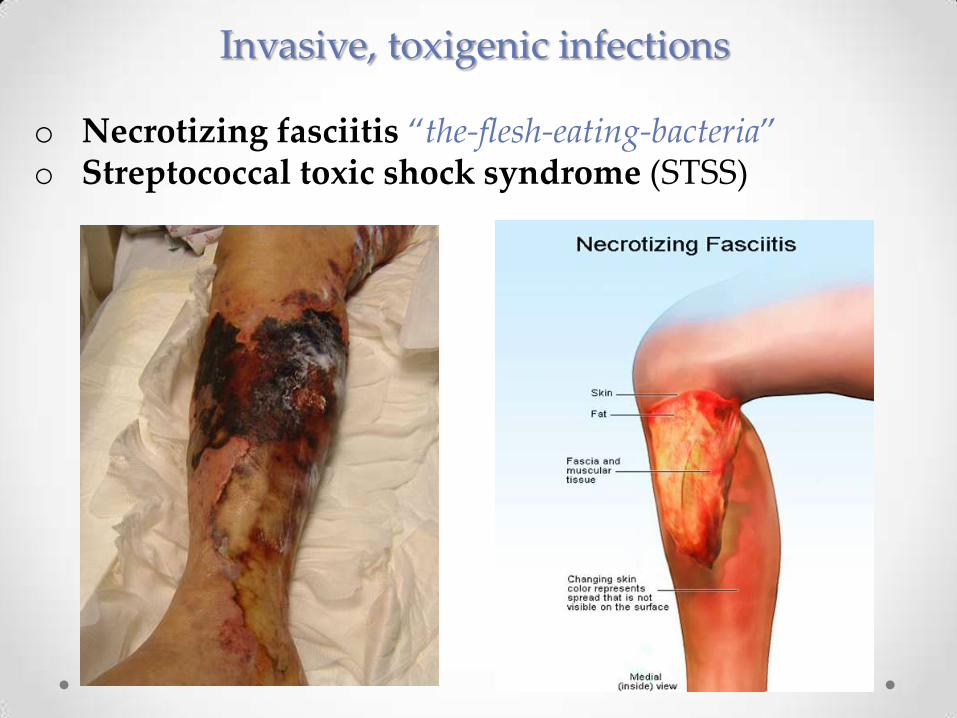
Invasive, toxigenic infections
o Necrotizing fasciitis “the-flesh-eating-bacteria”o Streptococcal toxic shock syndrome (STSS)
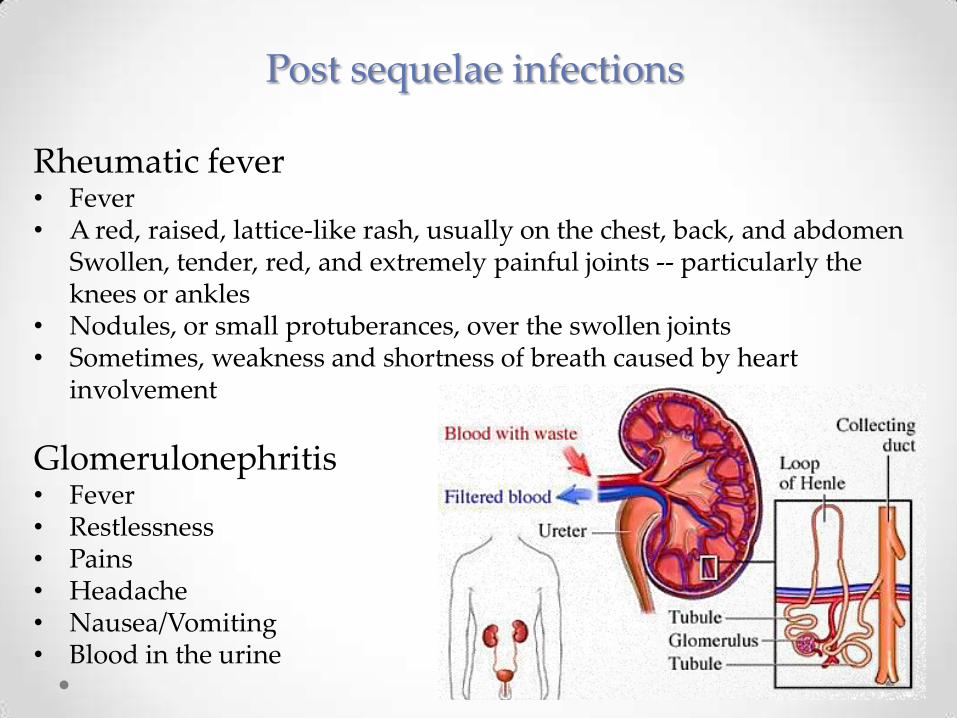
Post sequelae infections
Rheumatic fever • Fever • A red, raised, lattice-like rash, usually on the chest, back, and abdomen
Swollen, tender, red, and extremely painful joints -- particularly the knees or ankles
• Nodules, or small protuberances, over the swollen joints • Sometimes, weakness and shortness of breath caused by heart
involvement
Glomerulonephritis • Fever• Restlessness• Pains• Headache • Nausea/Vomiting• Blood in the urine
Treatment• Penicillin is still uniformly effective, although a
combination of penicillin and clindamycin is recommended in the rare event that the organism is resistant to one or the other
• Recommended duration of antibiotic therapy is 14 days however; therapy may be individualized
• High doses of intravenous drug therapy are recommended for those with STSS along with the addition of supportive care in an intensive care unit
• Endocarditis requires further cardiogram testing and is essential in monitoring and controlling the disorder
Prognosis
Symptomatic and functional recovery is expected following an ongoing rehabilitation care plan contingent upon compliance by the
patient to include completion of antimicrobial drug therapy paired with the
improvement of personal hygiene

Prevention
• Through good hygiene & hand washing
• Through good house keeping
• Cover mouth or nose when coughing or sneezing
• Do NOT share personal items
• Administering proper first aid & treatment aseptically
• Stay up to date on vaccines
References
o Case, Funke, Tortora, Microbiology, An Introduction, Eleventh Edition, Pearson Education, Inc., 2013
o “Group A Streptococcal.” National Center for Immunization and Respiratory Diseases: Division of Bacterial Diseases 2008.” Centers for Disease Control and Prevention (CDC), Disease Info:
<http://www.cdc.gov/ncidod/dbmd/diseaseinfo/groupastreptococcal_g.htm>
o Todar, PhD. Kenneth. “Streptococcus pyogenes and Streptococcal disease.” Textbook of Microbiology 16 Oct. 2013
<http://www.textbookofbacteriology.net/streptococcus_3.html>