Embed Size (px)
Citation preview

Curso de Medicina
TraumANATOMIA:
trauma
RAQUIMEDULAR
2014
Leão HZ (Professor de Morfologia – ULBRA)
Juan Zambon(Acadêmico de Medicina – ULBRA)
Patrícia Comberlato(Acadêmica de Odontologia – PUCRS)
Quino

DOIS MINUTOS

Aspectos anatômicos da coluna
vertebral e medula espinal
• The bony spinal column encases and
protects the spinal cord. The spinal cord is
40–45 cm in length,cylindrical in shape,
starts at the base of the brain, exiting
through the foramen magnum, and
terminates in the conus medullaris at
roughly L1–L2, although this can range
from T12 to L3.
Legome, 2011

Aspectos anatômicos da coluna
vertebral e medula espinal
• The cauda equina emanate from the cona
medullaris.
• The spinal cord is divided into neurological
units, labeled after vertebral levels, i.e., C1,
C2, etc. However, within the spinal cord, a
C8 neurological level exists. This is not true
of the bony spine.
Legome, 2011

Aspectos anatômicos da coluna
vertebral e medula espinal
• The spinal cord gives off 31 spinal nerves,
(8 cervical, 12 thoracic, 5 lumbar, 5 sacral,
1 coccygeal).
• Spinal nerves consist of anterior (ventral)
and posterior (dorsal) nerves, containing
efferent and afferent axons, respectively.
These nerves exit the spinal column through
bony foramina.
Legome, 2011

Aspectos anatômicos da coluna
vertebral e medula espinal
• From C1 to C7, the nerve roots exit the
spinal column above the corresponding
vertebra. At theC7 vertebra, C8 roots exit
below the vertebra.
• All roots caudal to C7 exit inferior to the
vertebra.
Legome, 2011

Aspectos anatômicos da coluna
vertebral e medula espinal
• Fusiform enlargements of the spinal cord
exist in the cervical as well as the lower
thoracic/upper lumbar regions. The
enlargements give rise to the brachial and
lumbo-sacral plexuses that innervate the
arms and legs respectively. The amount of
space not occupied by the cord is reduced at
these levels. Consequently, the cord is more
easily compressed in these locations.Legome, 2011

Aspectos anatômicos da coluna
vertebral e medula espinal
• The most commonly injured spinal cord
level is C5, whereas the thoracolumbar
junction (T12–L1) is the most frequent
lumbar level.
• Transection of the cord above C5 causes
tetraplegia. Respiratory failure may occur if
the transection is superior to C4.
Legome, 2011

Aspectos anatômicos da coluna
vertebral e medula espinal
• Mirroring the brain, the cord is covered by
three meningeal layers, the pia, arachnoid,
and dura maters.
Legome, 2011

Sistema vascular
• Vascular supply of the spinal cord is
divided into anterior and posterior vessels.
--- Arterial
• Both the anterior and posterior circulation
systems of the cord receive contributions
from the radicular and medullary arteries
Legome, 2011

Sistema vascular
--- Arterial
1. Anterior arterial vessel: The anterior spinal
artery (from the union of the vertebral
arteries), runs the entire length of the cord
in the midline, supplies the anterior
circumferential two thirds of cord and the
central gray matter.
Legome, 2011

Sistema vascular
--- Arterial
2. Posterior arterial vessels supply the
remaining third circumferential of posterior
cord. The anastomotic flow between the
anterior and posterior arterial systems is
poor. Both arterial systems contribute to a
net-like arterial plexus surrounding the
thoracic, distal cervical, and proximal
lumbar cord.
Legome, 2011

Sistema vascular
--- Arterial
While redundancy in the arterial supply of
this area exists, this area is felt to be at
greater risk of ischemia than the very upper
and lower ends of the cord during episodes
of hypotension.
Legome, 2011

Pós e
Pré-atlântica
Legome, 2011

Sistema vascular
--- Venous
• The venous system of the cord follows the
arterial system, draining into the internal
and external venous plexuses.
• The internal venous plexus passes
superiorly and communicates with the dural
sinuses and vertebral veins in the skull.
• The external venous plexus lies on the
external surface of the vertebrae.
Legome, 2011

Legome,
2011

Medula espinal
• The cord itself is made up of gray and white
matter. White matter concentration is greatest
in the cervical spinal segments (as a
consequence of the large density of axonal
fibers).
• The butterfly-shaped gray matter sits
centrally and contains the nerve cell bodies
and their processes, whereas the white matter
is a collection of the myelinated ascending
and descending axonal fibers known as tracts.
Legome, 2011

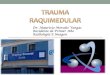
Magnetic resonance
imaging provides the
best visualization of
the soft tissues,
spinal cord,
and spinous
ligaments
Legome, 2011

At this time, MRI cannot predict neurological status at 6
weeks in cases of cord hemorrhage, edema, and contusion.
If a patient is very unstable, check a cross-table lateral
cervical spine X-ray. It will provide basic information about
the cervical spine.
None of these
diagnostic studies
are therapeutic
Legome, 2011

Medula espinal
• Multiple tracts exist.
• Important spinal cord tracts are the posterior
columns (medial and lateral), spinothalamic
tract, and corticospinal tract. The tracts are
named for their origins (i.e., corticospinal
tract starts in the cortex, travels to the spine)
Legome, 2011

Legome, 2011

Legome, 2011

Spinal cord injury terminology
• Tetraplegia (formerly known as
quadriplegia) is injury to the spinal cord in
the cervical region with associated loss of
muscle strength in all four extremities.
• It can be complete – lacking sensory and
motor, or incomplete – having one or both
of these neurologic functions partially or
completely intact.
Legome, 2011

Spinal cord injury terminology
• Paraplegia is injury to the spinal cord in the
thoracic, lumbar, or sacral regions,
including the cauda equina and conus
medullaris, sparing the upper extremities.
Legome, 2011

Pathology of spinal cord injury
• Spinal cord injury can be sustained through
multiple mechanisms.
The spinal cord suffers two distinct
injuries:
• the initial or primary injury and
• a later secondary insult.
Legome, 2011

Pathology of spinal cord injury
The following list details the common
mechanisms (primary injuries) leading to
tissue damage:
• 1. Destruction from direct trauma.
• 2. Compression by bone fragments,
hematoma, or disk material.
• 3. Ischemia from damage or impingement
on the spinal arteries.
Spinal cord edema could ensue secondary to any
of the above.Legome, 2011

Pathology of spinal cord injury
The phenomenon of the secondary insult is
still not entirely clear, but the various
pathways are better understood now.
Currently, secondary injury is believed to
be a highly complex combination of
• cord hypoxia,
• calcium efflux,
• cell apoptosis,
• free radicals,
• and generalized inflammation.Legome, 2011

T2-weighted magnetic
resonance imaging
(MRI) image of C4–C5
complete cord
transection. C3–C5
subluxation with
anterolisthesis of
C4 and C5 and
concurrent
retrolisthesis of C5 on
C6. An epidural
hematoma is visible,
along with prevertebral
and posterior
paraspinous soft tissue
hematoma/edema.

Obrigado por participarem





![Trauma raquimedular [autoguardado]](https://img.pdfslide.net/doc/110x75/5878625d1a28ab18098b678f/trauma-raquimedular-autoguardado.jpg)