Embed Size (px)
Citation preview

Adrenal incidentalomas
Antonia Brooke

To cover……….
• Epidemiology• Chances of progression• Imaging • Assessment of functionality
– Which tests– What is subclinical Cushings, what does it matter, how
to treat
• Implications for our service

Definition
• Adrenal mass >1cm discovered incidentally when investigating for something else
• No clinical syndrome associated or presence of metastatic disease

Background and Incidence• Prevalence around 4% (on CT)
– Increasingly common with age – 1% at 40, 7% at 70• History of malignant disease then metastasis in
50% of cases (frequently bilateral)– 2.5% adenomas are mets
• Bilateral disease differential:– CAH– Hyperplasia– bilateral phaeos – infiltrative diseases (mets) – rare causes

Hormonal secretion• Hormonally active in up to 12%
– Phaeochromocytomas 5% – Cushing’s syndrome / Sub-clinical Cushing’s 5% or
possibly more– Primary hyperaldosteronism / Conn’s syndrome
1% – Androgen secreting / virilising tumour <1%)
• Remaining incidentalomas were ganglioneuromas, myelolipomas, or benign cysts

Follow up - 16 studies over 2-7yrs
Cawood et al EJE 2009
% Mean (%) 95% CIthat↑ size 14.7 8-21
unchanged 68 46-90
that ↓ size 7 -2.4-16.4
Became malignant 0.2 0-0.4
Became functional 0.9 0.5-2.2
Develop Cushings 0.3
Dvp subclinical Cushings 0.3
Dvp phaeo 0.2
Dvp Conns 0

Imaging
• CT better at eliminating malignancy (dedicated CT looking at Hounsfield units (HU) and washout characteristics)– <10HU = benign (sens 71%, spec 100%)
• MRI may characterise phaeos better• FDG-PET good for phaeos and cancer• FNA – consider if cancer history and >10HU on CT
after exclusion of phaeo

Imaging - size• >4cm 90% sensitivity carcinomas
24% specificity (ie only 24% cancer)• >6cm 25% chance of it being carcinoma• <2cm + hypodense then unlikely to grow• If change in size >1cm over 6 months consider
resection• Guidelines suggest:
– NIH: 2 CTs 6M apart– Young et al + UptoDate: 0,6,12,24m– BES: Repeat image – increase in size of 0.8cm over
6-12M consider surgery

Risk of CT
• Abdo CT = 10mSv (adrenal less but about same if delayed washout) = 3.3yrs background radiation
• Lifetime absolute risk of cancer as consequence is 0.048%
• 1 cancer related death for every 5000 scans in those >30yrs

Practical suggestion
• Most have not had dedicated CT (ie bottom of CT chest or CT colon)
• If <4cm do dedicated adrenal CT 6 months after presentation – No need to rescan if no change in size (or <0.8cm)
• If >4cm do dedicated adrenal CT when referred to get characteristics and consider repeat or MRI in a further 6 months if looks benign
• <2cm and no change then discharge2- 4cm monitor clinically for longer?

Function

Biochemistry – initial screen
• 2x 24hr metanephrines or single plasma metanephrine
• Overnight dexamethasone suppression• Renin-aldosterone (if hypertensive or
hypokalaemic)

Phaeo: MetanephrinesUrine • sensitivity and specificity of 91 – 98%) • 4x normal = diagnostic• Cost around £21 each• False positives:
– Drugs (eg amitriptyline, phenoxybenzamine) ?doxazosin ? Mirtazepine – Sleep apnoea
Plasma• If one or more are positive, measure plasma metanephrines (sensitivity
around 80% - higher if inherited, good specificity) – Cost approx £51– Disadv – need to be supine for 20mins– Certain foods leading to high readings: nuts, fruits, potatoes,
tomatoes, beans

Other tests• MIBG scan preoperatively if +ve
• Consider Clonidine suppression test (0.3mg orally) plasma MN at base + after 3 hrs if doubt about diagnosis

Drugs• If suspicion high start alpha blocakade prior to biochemical
confirmation: – Doxazosin 1mg titrated up (even if normotensive)– Phenoxybenzaime 10mg bd up to 20mg qds (more
complete blockade) if • extremely high metanephrines or• initial BP >160/90. • SE: postural hypotension, nasal stuffiness and erectile
problems• Calcium channel blockers if unable to tolerate alpha or beta
blockade• Blocked > 3 weeks prior to surgery

Diagnosis of Phaeo• Consider genetic screening for VHL / RET/ succinate
dehydrogenase (SDH) (+ve in 25%) especially in the young or extra adrenal disease.
• SDHB – strong association with malignancy• 24% have germline mutation even if ‘sporadic’• Familial syndromes less likely to be malignant (unless
SDH)• Follow up > 5 years (long term risk of recurrence 10-
15%)• If large preop tumour consider baseline scan 6M
postop

Conns – RAA ratio• Measure if hypertensive or hypokalaemic• exclude aldosterone antagonists for 6 weeks (and
ideally ACE and Ang II but effect prob minimal)• b blockers suppress renin
– However normal test on treatment is reassuring• Ideally control BP on Ca channel blockers, Doxazosin
and hydralazine• Ensure diet is not salt restricted or load with slow na
for 3 days (120mmol/day = 3 tabs QDS)

RAA cont• Positive = Aldosterone to renin ratio >20
– treat with spironolactone or epleronone• Venous sampling
– If young (<40yrs), lesion >1cm with normal contralateral adrenal then reasonable to not venous sampling
– Only do if patient would consider adrenalectomy (right adrenal vein cannulation is difficult)
– Corrected aldosterone/cortisol ratios of > 4 to 1 = likely unilateral• Untreated aldosterone excess can lead to
– myocardial fibrosis – left ventricular hypertrophy – increased mortality from congestive heart failure – more ischemic events, and increased vascular and clotting
abnormalities

Cortisol

What is subclinical Cushings
• ACTH independent cortisol secretion not fully restrained by pituitary feedback
• Found in up to 20% of adenomas• To make diagnosis:
– Have to have adrenal adenoma– Not cushingoid– Have ACTH independent autonomous secretion

Subclinical Cushings Syndrome
For assymptomatic patients•Overnight dexamethasone suppression test (1mg)
– enzyme inducers (eg anti epileptics) or uncontrolled diabetes
– Pt can eat and drink normally.– Tablet at 11pm then 9am cortisol
<50nmol/l sens>95% spec 70-80%>140nmol/l sens 70% spec >95%

Evidence for harm from cortisol low grade secretion ‘incidentalomas’
• Metabolic complications: – hypertension– obesity– diabetes mellitus– osteoporosis

What’s the evidence
• Lots of retrospective cross sectional studies showing associated risks
• No prospective studies showing link to mortality
• Not likely to progress to clinical Cushings

Tests to detect ACTH independent autonomous secretion
Most surgical studies look for 2 abnormal tests but:• UFC usually normal• Midnight salivary cortisol usually normal• Altered response to overnight dex• ACTH usually low (ACTH <5pg/ml )• Low DHEAS would support diagnosis (but often
normal and declines with age)

But…..
• Virtually impossible to recognise false positives on dex testing
• What should be the cut off….– NIH 138nmol/l– Endo Soc guidelines suggest 50nmol/l for OVERT
Cushings– Why not grey area where consideration to clinical
phenotype is considered (metabolic syndrome and osteoporosis)?

Practical solution
• Overnight dex >138nmol/l– 2nd test of cortisol hypersecretion (eg UFC, ACTH)– Look for metabolic risk– consider adrenalectomy if both positive and young or treat
metabolic risk factors (patient choice?!)
• 50 – 138nmol/l – look at metabolic risk factors (HbA1c, DEXA, lipid profile, BP) and consider treatment at lower threshold than Framlingham
• <50nmol/l – reassure and never repeat

How to treat?• Treat cortisol excess
– Nocturnal metyrapone– Surgical: adrenalectomy
• Treat metabolic complications– Vit D / bisphos– Metformin– Antihypertensives
• GP: No follow up studies beyond 7 yrs so maybe role for GP to monitor metabolic risk factors or be aware of it?

Evidence that adrenalectomy works
• Treating metabolic complications and treating with late night metyrapone – evidence free
• Treating surgically – limited evidence

Main surgical studies
• Erbil: case controlled 28 pts– 11SCS lead to ↓ BP post adrenalectomy↓
• Tsuiki 20pts SCS (followed 15-69M)– 10 adrenalectomy: 8/10 improved– 10 conservative: 5/10 worsened
• Toniati: prospective 45pts SCS (mean FU 8Y)– 23 adrenalectomy: 2/3 N or improved BP and DM– 22 conservative: some worsening

More surgical studies
• Sereg: retrospective uncontrolled followed 9 yrs– 47/125 NON functioning had adrenalectomy– 78 treated conservatively– No benefit
• Chiodini 108pts followed 18-48M– SCS recommend surgery + some pts without had– Surgery – reduced BP

Issues to discuss
• Where are they all?• Can we do a nurse protocol?• What are the most appropriate tests?• How long should they be followed for and
how?• What constitutes a positive test and how
should they be treated?

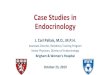
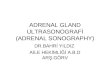
Adrenal imaging




























Adrenocortical cancers
• Incidence 0.5 to 2 per million• Bimodal: childhood and 4th to 5th decade• 1.5 F : 1 M• 60% are secretory
– High DHEAS suggestive (suppressed in adenomas)– Check estradiol in males (more likely malignant)– Allows tumour markers and predict post op
course

• Can be seen in syndromes: CAH, MEN, familial polyposis
• Sporadic mutations in tumor suppressor gene (TP53) seen in 1/3 adrenocortical ca
• Prognosis: <15% at 5 years if locally advanced disease:– Stage 1: 60%– Stage 2: 58%– Stage 3: 24%– Stage 4: 0%

Imaging• >6cm high suspicion of malignancy• 3-6cm repeat imaging in 3-6M• Delayed washout on contrast is suggestive• most are often inhomogeneous, irregular margins• Look for invasion of IVC• Always do CAP and consider bone scan and pet if
in doubt• Don’t ever biopsy (tumour spill)

Surgery• Open adrenalectomy (ESMO clinical practice
guidelines suggests >10 adrenalectomies a year, Dutch studies show improved survival if part of cancer network)
• Laparoscopic can be considered if <8cm and not obviously invasive
• Margin free resection only way to long term survival (hence take kidney, IVC, liver as necessary)

• Consider resection of primary (even if metastatic) as improved survival and endocrinology
• Even seemingly complete resection initially: 50% chance of recurrence
• Surgery for recurrent disease good idea if prolonged disease free interval, particularly if chance of ‘complete’ resection

HIstology• Histology: Challenging as no marker to suggest
malignancy• Weiss score (>3): mitotis, atypical mitoses,
necrosis, venous invasion, capsular invasion, sinusal invasion, nuclear atypia, diffuse architecture and clear cell. Score >3 = suggests malignancy
• Ki67: measure of proliferative activitiy useful• Disease stage and margins most useful predictor

Radiotherapy
• Consider to tumour bed if incomplete resection

Post op treatment - Mitotane• Evidence: case control study: 47 pts on Mitotane
(italy) compared to 130 italian / german pts not offered – improved survival
• Who?– Potential residual disease– Ki67>10%
• Therapeutic mitotane considerably better outcome than non therapeutic
• How long – minimum 2 years

Side effects
• Endocrine• All patients should receive concomitant
glucocorticoids (as adrenolytic) and higher dose (increased metabolic clearance).
• Mitotane increases CBG so measuring cortisol unreliable
• May need thyroxine and testosterone

• Gastrointestinal– Nausea and vomiting– Diarrhoea
• Neurological– Tremor

Chemotherapy – FIRM-ACT NEJM 2012
• FIRM-ACT trial (median survival 12-15M)• Etoposide, Doxorubicin, Cisplatin (and
Mitotane) – response rate 23%• Streptozotocin (Mitotane) – RR 9%• No chemotherapy• No increase in survival but , but better
response rates and progression free survival