Embed Size (px)
Citation preview


Asthma Phenotypes and Endotypes
Gamal Rabie Agmy, MD, FCCP Professor of chest Diseases, Assiut university

Definition of Asthma
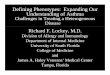
A chronic inflammatory disorder of the airways
Many cells and cellular elements play a role
Chronic inflammation is associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness, and coughing
Widespread, variable, and often reversible airflow limitation

Source: Peter J. Barnes, MD
Asthma Inflammation: Cells and Mediators

Asthma is a complex disease or a syndrome
that includes several disease variants.
The term asthma, like ‘arthritis’, equates to a
definition of grouped clinical and physiological
characteristics. These characteristics could
identify syndromes, phenotypes or even
multiple diseases rather than a single disease.

◙ For revealing the complexity and the
heterogeneity of this disease, asthma patients
were grouped into subtypes called phenotypes.
◙ Term ‘phenotype’ describes subtypes of
asthma focused on ‘clinically observable
characteristics’ of a disease.




Therefore, there are many ‘definitions’ for asthma phenotypes,
many of which are related to differences in symptoms and
severity rather than to differences in underlying mechanisms. but
this kind of subtyping does little to help understand prognosis
and target therapy.
When a link can be made between clinical characteristics and
molecular pathways, the term endotype can be introduced
to describe distinct subtypes with a defining etiology and
consistent pathobiologic mechanisms.

The definition of a true phenotype (or endotype)
requires an underlying pathobiology with
identifiable biomarkers and genetics .
Gene-expression profiling allows definition of
expression signatures to characterize patient
subgroups, predict response to treatment, and
offer novel therapies.

Th2-associated asthma
These patients are characterized by atopy,
eosinophilic inflammation and favorable response
to corticosteroids.
Early-onset allergic asthma
Late-onset persistent eosinophilic asthma
Exercise induced asthma

Early-onset allergic asthma
Clinical characteristics:
This group of asthmatic patients developed their disease in
childhood, and maintained their symptoms into adulthood. .
The majority of early-onset allergic asthma is mild but that
an increasing complexity of immune processes leads to
greater severity.
Most people with asthma are likely to have this phenotype.
Positive skin prick tests, specific IgE antibodies in serum,
eosinophilia in the peripheral blood .

Genetics:
Early-onset allergic patients commonly have a
family history of asthma, suggesting a genetic
component.
►Several Th2 cytokine SNPs
►higher numbers of mutations in TH2-related genes
(IL4, IL13, IL4Rα ) associated with greater severity
of disease.

Biomarkers:
Positive SPT, elevated IgE/elevated FeNO
Th2 cytokines IL-4 ,IL-5 , IL-9, IL-13, and periostin measured in
sputum, BAL, serum and bronchial biopsies.
Treatment responses:
►Corticosteroid-responsive.
►Th2 Targeted therapy:
Anti IgE (omalizumab)in Severe allergic asthma.
Anti–IL-13( lebrikizumab) in Allergic asthma with dominant IL-
13 activation . Surrogate marker predicting better response is
high circulating levels of periostin. .

Inhaled IL-4Rα antagonist . Surrogate
marker predicting better response is IL-4
receptor a polymorphism.

Late-onset persistent eosinophilic asthma
Clinical characteristics:
The majority of this group develops disease in adult
life, often in the late 20s to 40s.
Severe from onset, Severe exacerbations with persistent
sputum eosinophilia (>2%), despite corticosteroid therapy.
less clinical allergic responses( non atopic) than early-
onset asthma.
It is often associated with sinus disease.

Genetics:
Few patients in this group have a family
history of asthma.
little is known regarding the genetics of adult
onset persistent asthma.

Biomarkers:
Lung eosinophilia. Persistent sputum eosinophilia (≥2%)
The lack of clinical allergy in this phenotype suggests that the TH2
process differs from and is probably more complex than the one
associated with the early-onset allergic phenotype but the presence
of IL-13 and IL-5 in the lower airways confirm Th2 pathway.
Some individuals show sputum neutrophilia intermixed with their
eosinophilic process. This mixed inflammatory process implies
that there are interactions of additional immune pathways with
TH2 immunity, including activation of pathways related to IL-33
and IL-17 .
Elevations in FeNO

Treatment responses:
• persistent eosinophilia in late-onset disease inspite of ICS implies that
the TH2 process in this type of asthma is refractory to corticosteroids
but high systemic doses of corticosteroids are generally able to
overcome this refractoriness in late-onset asthma.
• IL-5 targeted therapy may show much better efficacy in this
endotype, compared in early-onset allergic asthma patients, as IL-5
dependent eosinophilia may be more important in this potential
endotype. (decreasing exacerbations and systemic corticosteroid
requirements)
• IL-4 and IL-13 targeted therapy pathway.

AERD is probably a subendotype or a similar endotype. It is an
acquired condition on top of an intrinsic or less frequently
allergic asthma and thus, despite its peculiar sensitivity to
NSAIDs, still has major overlap with these conditions.
Clinical characteristics :
• AERD is frequently progressive severe asthma starts late in
life and is associated with eosinophilia and sinus disease
Polyposis.
• Response to aspirin challenge
Aspirin exacerbated airway disease
(AERD)

Genetics :
• LT-related gene polymorphisms.
• Gene-expression study identified upregulation of periostin a potent
regulator of fibrosis and collagen deposition has also been identified
in polyps of and in airway epithelial cells of patients with AIA.
Overexpression of periostin has been associated with accelerated cell
growth and angiogenesis(subtype).
Biomarkers:
high cysteinyl leukotriene level.

Treatment responses :
• Many patients require systemic corticosteroids to control
their sinusitis and asthma.
• Leukotriene modifiers especially 5-LO inhibitors can have a
robust impact on the AERD subset.
• Downregulation of periostin after treatment of asthmatic
patients with corticosteroids suggests that normalization of
periostin expression is a part of the therapeutic effects of
corticosteroids. This opens a possibility of specifically
targeting periostin in future therapies for nasal polyps and
asthma

Clinical characteristics:
• Exercise induced asthma refers to asthma whose symptoms
are experienced primarily after exercise. EIA is a milder
form of TH2 asthma.
• Consistent with a relationship to TH2 processes, EIA
common in atopic athletes and high percentages of
eosinophils and mast cells and their mediators .
Exercise induced asthma

Biomarkers:
• Th2 cytokines and cysteinyl leukotriene
Genetics:
• No distinct genetic factors .
Treatment responses:
• Leukotriene modifiers high LTE4/FENO ratio is Surrogate
marker predicting better response.
• IL-9 targeted therapy has been shown effective on patients
of this group, which implies that Th2 immunity is involved in
the pathophysiology of EIA.

The lack of efficacy of Th2 targeted therapy suggests that a
subgroup of asthma develops in the absence of Th2 immunity.
Little is understood about the non Th2 asthma and its related
molecular elements.
• Obesity-related asthma
• Neutrophilic asthma
• Smoking asthma
Non Th2-associated asthma

Whether obesity is a driving component in asthma development
or a mere confounder or comorbidity of its presence remains
controversial.
It is likely that obesity differentially impacts asthma that
develops early in life, as compared to later in life, being a more
prominent independent contributor in later onset disease.
So a distinct obesity-related asthma phenotype seems to occur
only in non-TH2 asthma.
, ..

Clinical characteristics :
Patients in this group are commonly women, obese, late onset
(mid-40s), less allergic (obesity is neither a risk factor for atopy
nor a risk factor for allergic asthma).with a high burden of
symptoms.

Biomarkers:
High expression of non Th2 mediators such as tumor
necrosis factor (TNF)-a, IL-6 .
Hormones of obesity, such as adiponectin, leptin, and resistin
either alone or in association with increased oxidative stress.
Elevations in an endogenous inhibitor of iNOS, asymmetric
dimethyl arginine (ADMA).
lower amounts of FeNO, fewer eosinophils.

Treatment responses:
Patients of this subgroup usually respond poorly to corticosteroids.
Bariatric surgery induced weight loss was associated with profound
improvements in lung function and symptoms in obese asthma.
However, the effect of weight loss on bronchial hyper responsiveness
was only shown in late-onset, nonallergic (non-Th2) asthma patient,
consistent with late onset obese asthma being a separate endotype. This
is further supported by the increase in ADMA in association with
worsening severity and control in late onset obese asthma only.

Clinical characteristics and biomarkers:
It remains controversial whether neutrophilia is an independent driving
component, a synergistic factor with eosinophilia or just a consequence of
corticosteroid therapy.
Still unclear whether this represents a unique form of asthma or just a
different stage of severity or persistent bacterial colonization or infection of
the airways on the background of a previously eosinophilic asthma.
Airway pathophysiology in neutrophilic asthma is characterized by (fixed)
airflow limitation more trapping of air, thicker airway walls (as
measured by CT) .

Novel mechanisms implicated in the pathogenesis of
noneosinophilic asthma involve the activation of innate immune
responses with a possible role of bacteria, viruses.
Neutrophilia can also co-exist with eosinophilia, and this identifies
the people with the most severe asthma and emphasizes the
complexity of the immunobiology of severe asthma in which
multiple different innate and adaptive immune pathways and cells
may have roles.
Impaired nuclear recruitment of histone deacetylase (HDAC).
The role of TH17 immunity

Biomarkers:
IL-8, IL-17A, LTB4, and possibly IL-32.
IL-1 and TNF-α pathways are upregulated and associated with
neutrophilic inflammation in a sputum gene-expression study.
low levels of FeNO.

Treatment responses:
Corticosteroids are less effective in patients of this subgroup.
Macrolide antibiotics may have some efficacy on neutrophilic
asthma, By modulating the innate immune response in the
lung, by reducing the expression of neutrophilic markers .
Restoration of HDAC 2 nuclear recruitment with theophylline.
Anti-TNF-α responsive( infliximab )
The efficacy of IL-17 targeted therapy in this subtype of
asthma awaits evidence from ongoing clinical trials.

Smoking has a complex relationship with asthma. It is
associated with deteriorating lung function and resistance to
corticosteroids.
Smoking asthma has been associated with neutrophilia in lung
tissue.
It is unknown if smoking asthma is a subtype of neutrophilic
asthma or an independent endotype . Since not all smoking
asthma is accompanied by neutrophilia, it is more likely that
there is only a partial overlap between neutrophilic asthma and
smoking asthma.

Some reports have suggested that smoking is associated with
elevated total IgE and that active smoking may increase the risk of
sensitization to workplace allergens.
However, little is understood regarding the role of genetics,
biomarkers or pathobiology.
FeNO levels are decreased by smoking and could help to
differentiate asthmatic subjects from non-asthmatic subjects.
Treatment responses
Quitting smoking
Restoration of HDAC 2 nuclear recruitment with theophylline.

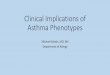
The intensity of the colors represents the range of severity; the relative sizes
of the subcircles suggest relative proportions of affected individuals

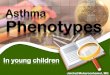
Lötvall et al.2011 proposed endotyping asthma into six classes
depending on several parameters used to define an endotype.
Aspirin sensitive asthma
Allergic asthma (adults)
Severe late-onset hypereosinophilic
ABPM
API-positive preschool wheezer
Asthma in cross country skiers

The principle of personalized or individualized medicine is to
'bring the right drug to the right patient at the right dose', such
that therapeutic efficacy is maximized and the side effects are
kept to a minimum.

The consideration of disease endotypes in treatment design
should be able to bridge the present era of treating asthma
based on family history, patient characteristics and laboratory
test, to the future era of personalized medicine where
treatment scheme will be based on individual biological data
such as genomic, proteomic and metabolic profiles.