Embed Size (px)
Citation preview
Lennard Funk
Atraumatic InstabilityWhat is it?
Should we Operate?@thearmclinic
www.wrightington.comwww.wrightington.com
www.wrightington.comwww.wrightington.com
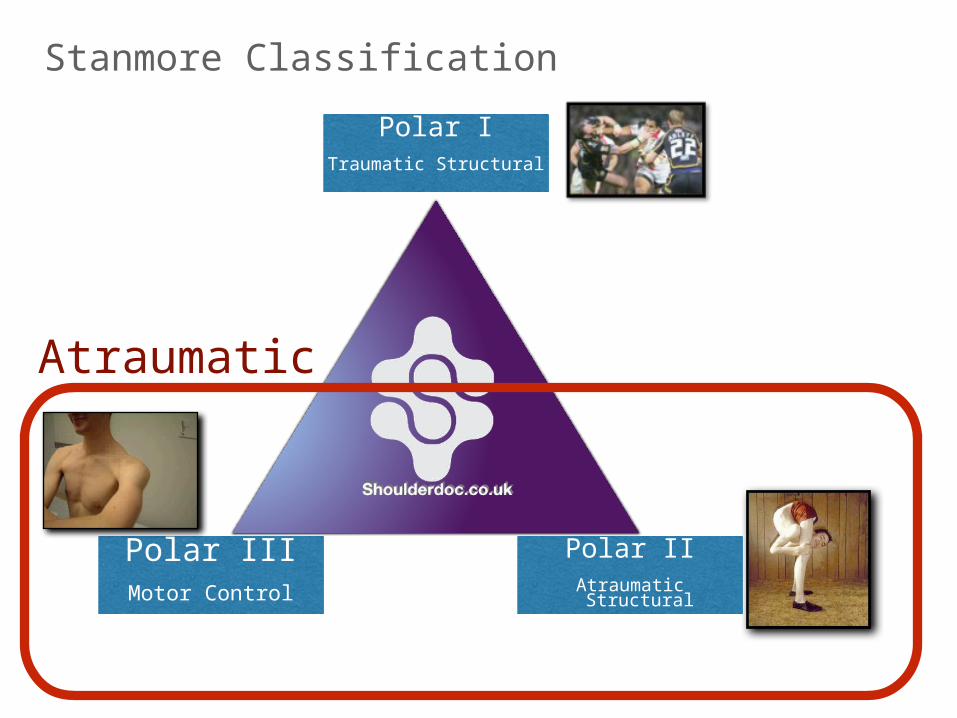
Stanmore ClassificationPolar I
Traumatic Structural
Polar IIAtraumatic Structural
Polar IIIMotor Control
Atraumatic
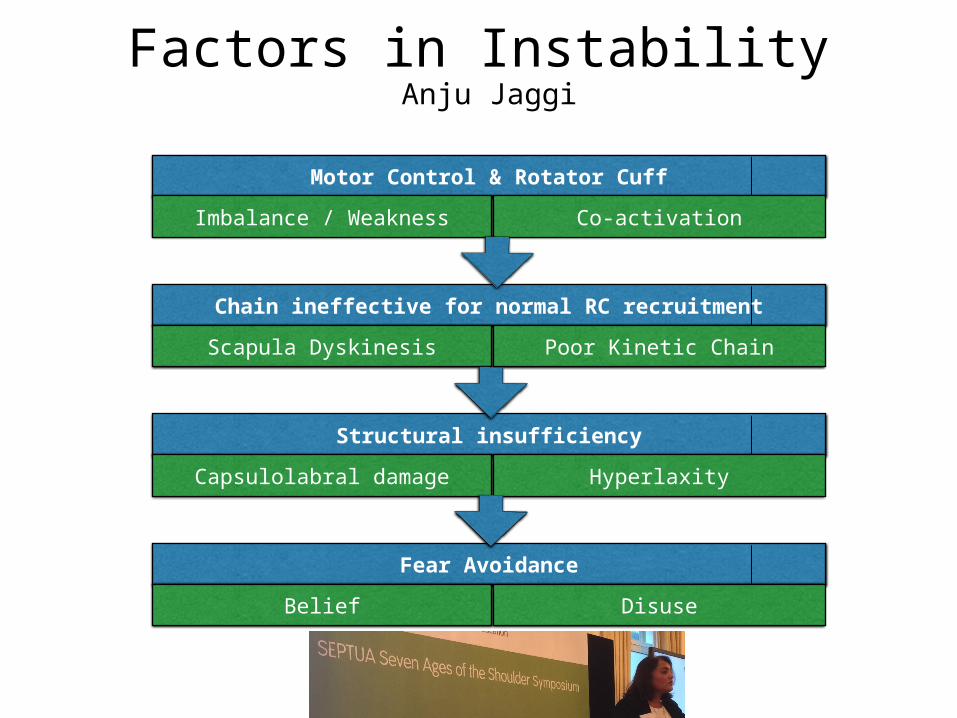
Factors in InstabilityAnju Jaggi
Motor Control & Rotator Cuff
Imbalance / Weakness Co-activation
Chain ineffective for normal RC recruitment
Scapula Dyskinesis Poor Kinetic Chain
Structural insufficiency
Capsulolabral damage Hyperlaxity
Fear Avoidance
Belief Disuse
www.wrightington.comwww.wrightington.com
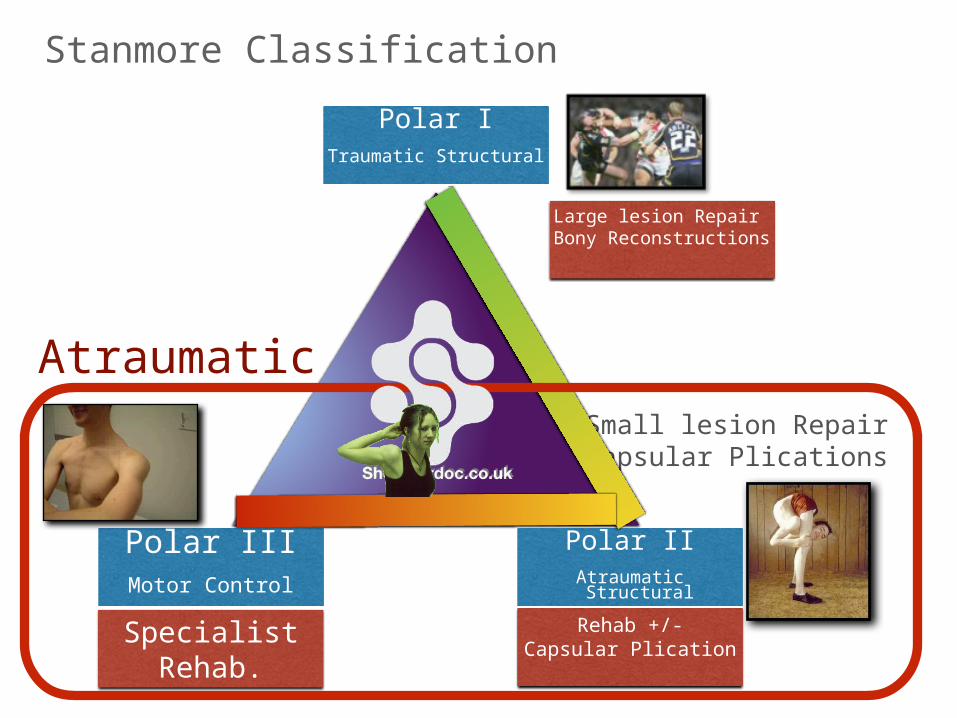
Stanmore Classification
Small lesion RepairCapsular Plications
Polar ITraumatic Structural
Polar IIAtraumatic Structural
Polar IIIMotor Control
Large lesion RepairBony Reconstructions
Rehab +/-Capsular Plication
SpecialistRehab.
Atraumatic
www.wrightington.comwww.wrightington.com
RehabOptimise:
CoreScapulaKinetic ChainPsychologyProprioception
www.wrightington.com
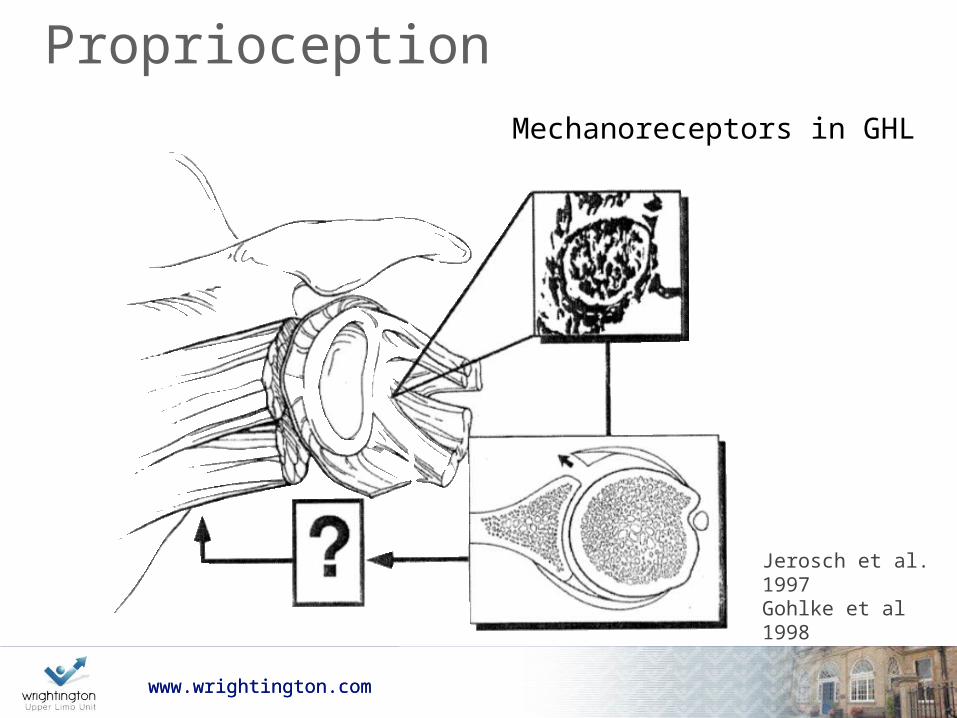
Proprioception
www.wrightington.com
Mechanoreceptors in GHL
Jerosch et al. 1997Gohlke et al 1998
www.wrightington.comwww.wrightington.com
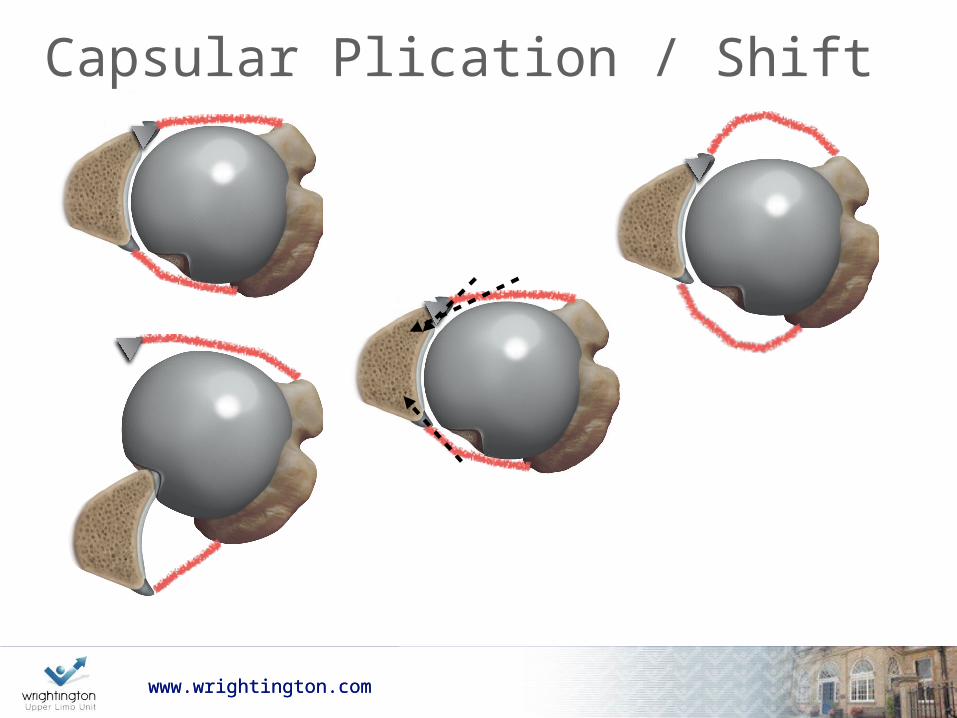
Capsular Plication / Shift
www.wrightington.com
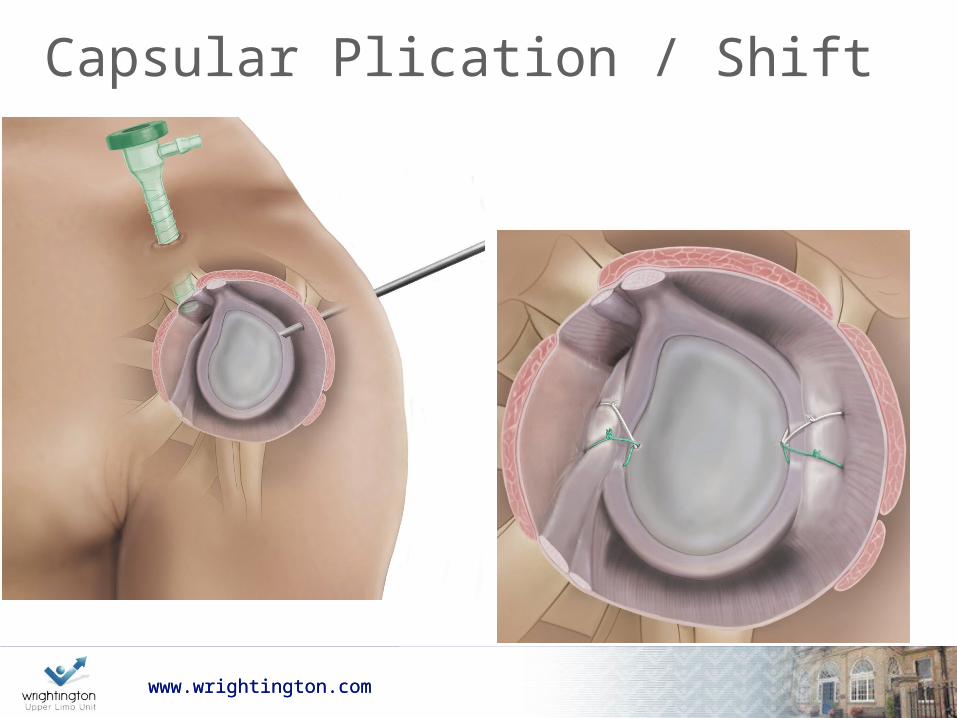
Capsular Plication / Shift
www.wrightington.com
www.wrightington.comwww.wrightington.com
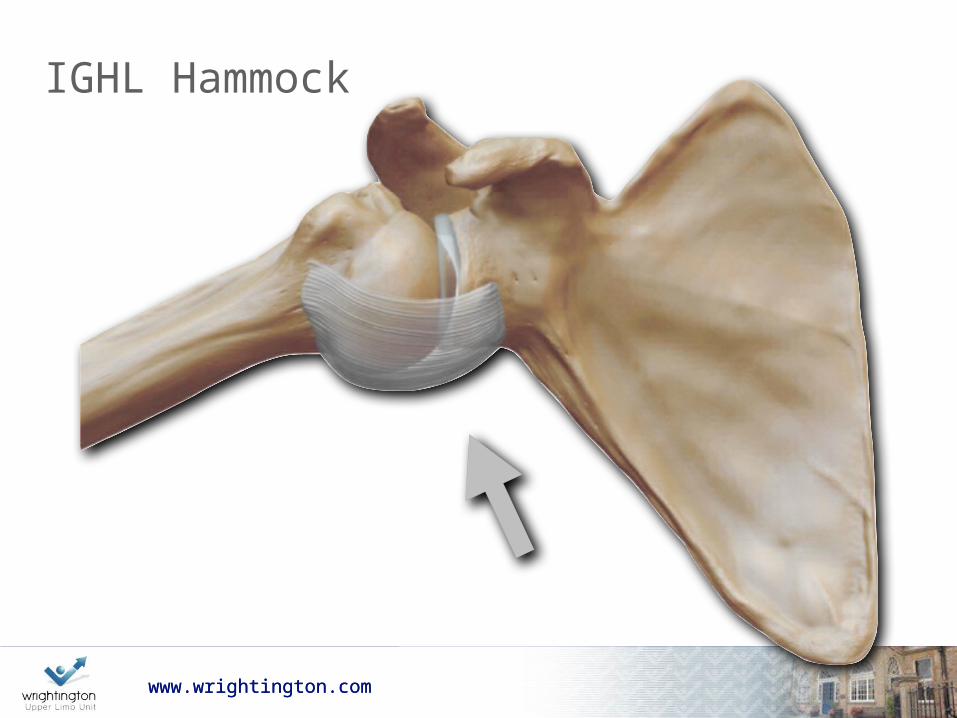
IGHL Hammock
www.wrightington.comwww.wrightington.com
Capsular Plication
www.wrightington.com
Post-op Rehab ER Sling for comfort (approx. 3 weeks) Avoid forcing or stretching Proprioceptive Scapula Core Functional
www.wrightington.com
www.wrightington.comwww.wrightington.com
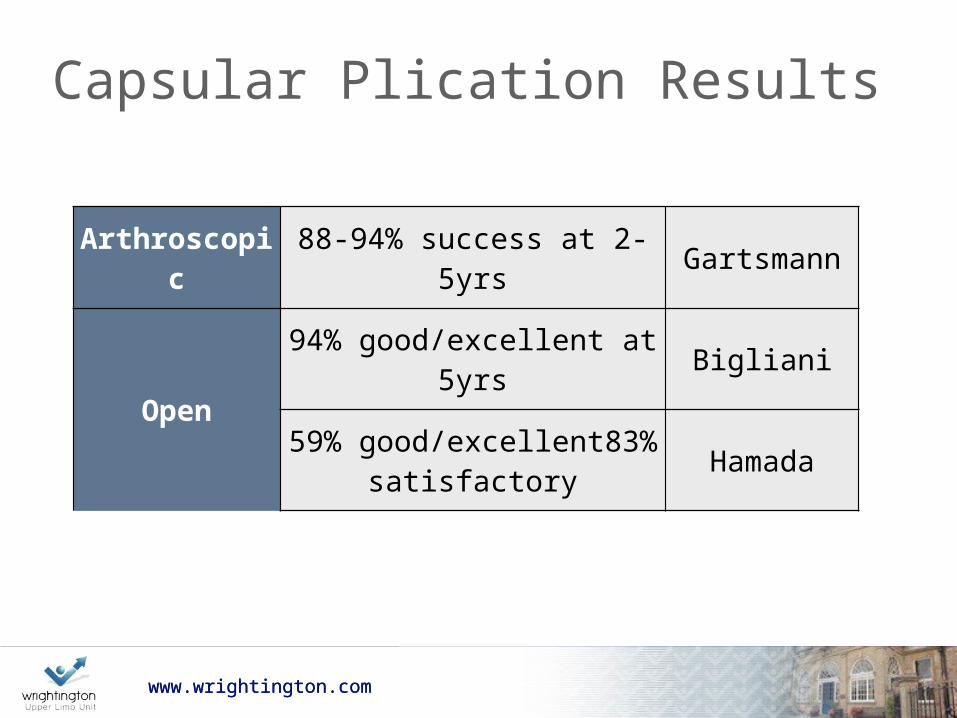
Capsular Plication Results
Arthroscopic 88-94% success at 2-5yrs Gartsmann
Open
94% good/excellent at 5yrs Bigliani
59% good/excellent83% satisfactory Hamada
www.wrightington.comwww.wrightington.com
Arthroscopic Plication Audit
Clinical outcome of arthroscopic capsular plication for atraumatic instability (Stanmore II) of the shoulder by a single surgeon, with >12 month follow-up.
Tablot, Carter & Funk, BESS 2012
www.wrightington.comwww.wrightington.com
Patients• 23 patients (16 )
• Average age 27 (19 – 41 years)
• Follow-up – 15.6 months (range 4 - 40 months)
• Previous Thermal Capsular Shrinkage: 6
• Average Pre-Op Specialist Physio: 5.4 months
www.wrightington.comwww.wrightington.com
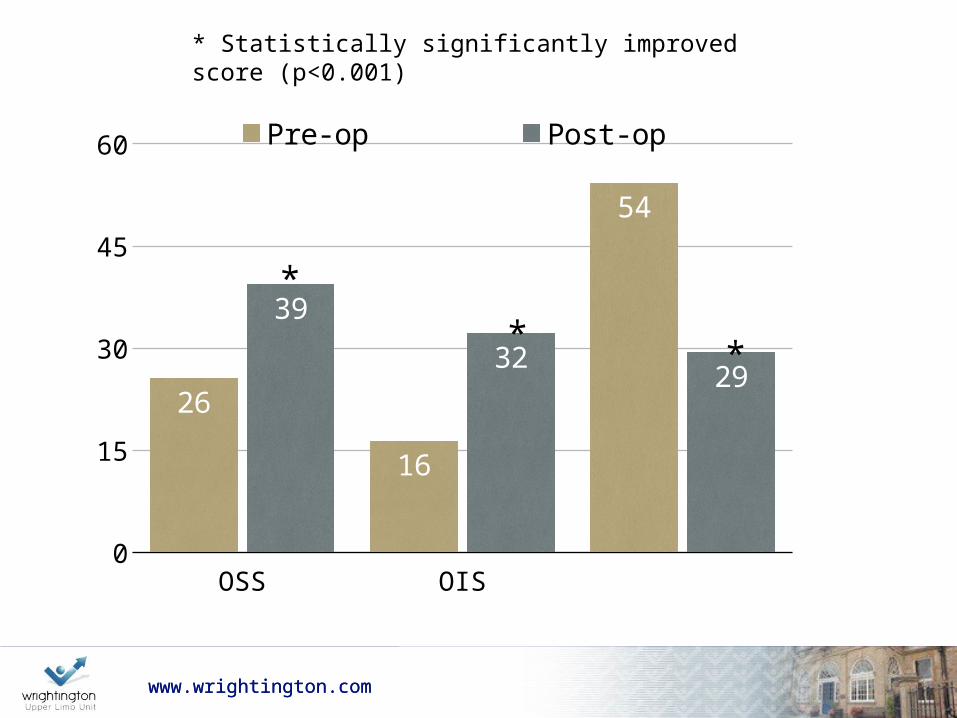
* Statistically significantly improved score (p<0.001)
OSS OIS DASH0
15
30
45
60
26
16
54
3932 29
Pre-op Post-op
* *
*
www.wrightington.comwww.wrightington.com
Patient Satisfaction
• Pre-op: 3.2/10
• Post-op: 8.6 / 10
• with average 82.4% improvement in symptoms
www.wrightington.comwww.wrightington.com
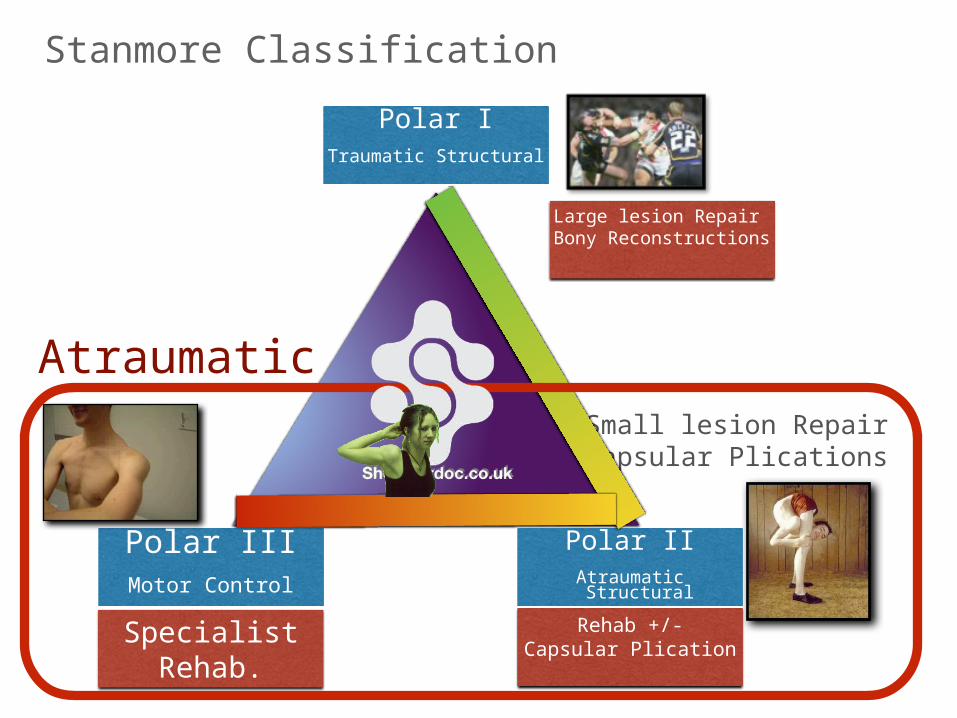
Stanmore Classification
Small lesion RepairCapsular Plications
Polar ITraumatic Structural
Polar IIAtraumatic Structural
Polar IIIMotor Control
Large lesion RepairBony Reconstructions
Rehab +/-Capsular Plication
SpecialistRehab.
Atraumatic
Atraumatic shoulder instabilityRandomized Controlled TrialDoes stabilisation surgery followed by
physiotherapy improve short & long term outcomes compared with physiotherapy
alone?
Associate Professor Karen Ginn
Associate Professor Karen GinnMs Anju JaggiDr Susan AlexanderProfessor Len FunkProfessor Rob Herbert
Karen GinnRob Herbert
Anju JaggiSusan AlexanderLen Funk
Clinical Trial
aima robust randomised controlled clinical trial to determine whether
surgical intervention followed by physiotherapy improves outcomes in patients suffering from atraumatic shoulder instability associated with capsulolabral damage compared with physiotherapy alone
designdouble blind (patient & physiotherapist) randomised controlled
clinical trialsham-controlled surgical arm
in order to account for the strong placebo effect associated with “the high levels of stress and rituals involved with surgery”
Dowrick & Bhandari 2012
ethics approval granted data collection commenced April 2013
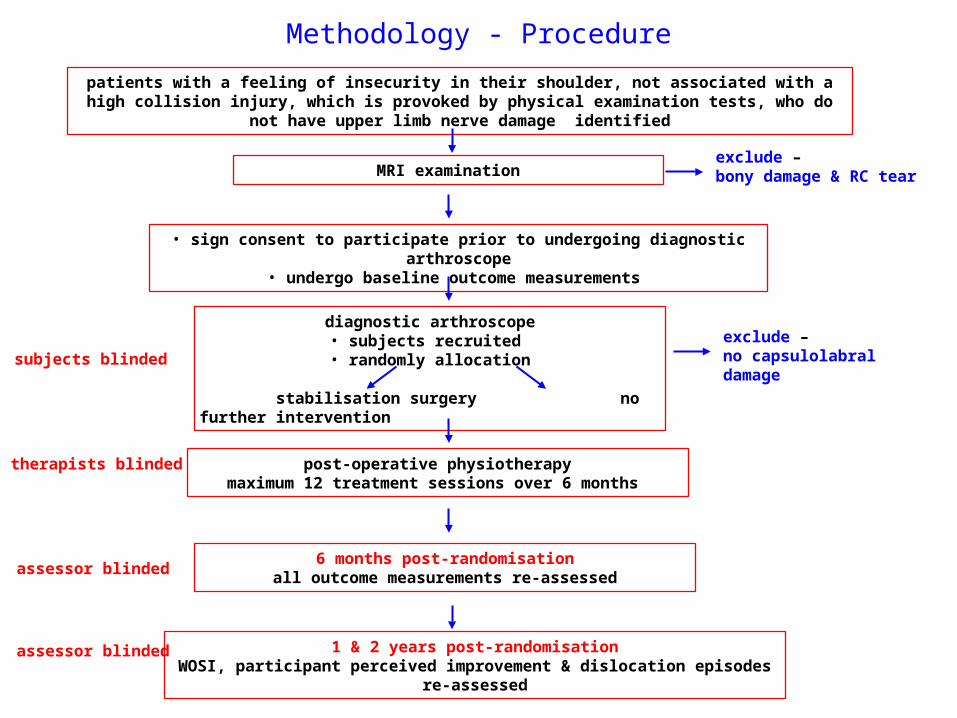
Methodology - Procedurepatients with a feeling of insecurity in their shoulder, not associated with a high collision injury, which
is provoked by physical examination tests, who do not have upper limb nerve damage identified
MRI examination
• sign consent to participate prior to undergoing diagnostic arthroscope• undergo baseline outcome measurements
diagnostic arthroscope• subjects recruited • randomly allocation
stabilisation surgery no further intervention
post-operative physiotherapymaximum 12 treatment sessions over 6 months
6 months post-randomisationall outcome measurements re-assessed
1 & 2 years post-randomisationWOSI, participant perceived improvement & dislocation episodes re-assessed
exclude – bony damage & RC tear
exclude – no capsulolabral damage subjects blinded
therapists blinded
assessor blinded
assessor blinded
www.wrightington.comwww.wrightington.com
References:1. Altchek DW, Warren RF, Skyhar MJ, Ortiz G. T-plasty modification of the Bankart procedure for
multidirectional instability of the anterior and inferior types. J Bone Joint Surg Am . 1991;73: 105-12.Abstract/FREE Full Text
2. Bak K, Spring BJ, Henderson JP. Inferior capsular shift procedure in athletes with multidirectional instability based on isolated capsular and ligamentous redundancy. Am J Sports Med . 2000;28: 466-71.Abstract/FREE Full Text
3. Flatow EL, Miniaci A, Evans PJ, Simonian PT, Warren RF. Instability of the shoulder: complex problems and failed repairs: Part II. Failed repairs. Instr Course Lect . 1998;47: 113-25.Medline
4. Gerber C. Observations on the classification of instability. In: Warner JJP, Iannotti JP, Gerber C, editors. Complex and revision problems in shoulder surgery . Philadelphia: Lippincott-Raven; 1996. p 9-18.
5. Pagnani MJ, Warren RF, Altchek DW, Wickiewicz TL, Anderson AF. Arthroscopic shoulder stabilization using transglenoid sutures. A four-year minimum followup. Am J Sports Med . 1996;24: 459-67.
6. Jobe FW, Tibone JE, Pink MM, Jobe CM, Kvitne RS. The shoulder in sports. In: Rockwood CA Jr, Matsen FA 3rd, editors. The shoulder . 2nd ed. Philadelphia: WB Saunders; 1996. p 1214-38.
7. Neer CS 2nd. Involuntary inferior and multidirectional instability of the shoulder: etiology, recognition, and treatment. Instr Course Lect . 1985;34: 232-8
8. Pollock RG, Owens JM, Flatow EL, Bigliani LU. Operative results of the inferior capsular shift procedure for multidirectional instability of the shoulder. J Bone Joint Surg Am . 2000;82: 919-28



![]Y]989]R^ `X89ZV^U`T#RD8VP]U^9]T]PW PY]^]P8YaR]^9RT7]U`b · cluding rotator cu! tendinopathy, rotator cu! tears, traumatic, atraumatic and acquired shoulder instability, , scapular](https://img.pdfslide.net/doc/110x75/5ffa2b31c650512cba751436/y989r-x89zvutrd8vpu9tpw-pyp8yar9rt7ub-cluding-rotator-cu-tendinopathy.jpg)