Embed Size (px)
Citation preview
Biomarker Development and Disease Pathology in Modern
Healthcare
Gyorgy Marko-Varga
Division of Clinical Protein Science & Imaging, Biomedical Center, Department of Measurement Technology and
Industrial Electrical Engineering,Lund University, BMC C13, SE-221 84 Lund, Sweden,
and First Department of Surgery, Tokyo Medical University,
Tokyo, Japan
Outline
• Disease Biology - Peronalized Medicine• Drug & Clinical Work Flow• IRESSA Study (Asia)• Biomarker Discovery• Biobanking• Technology Platforms• Drug Imaging• Summary
Linking Disease Pathology to
Treatment-Diagnostic Land Marks
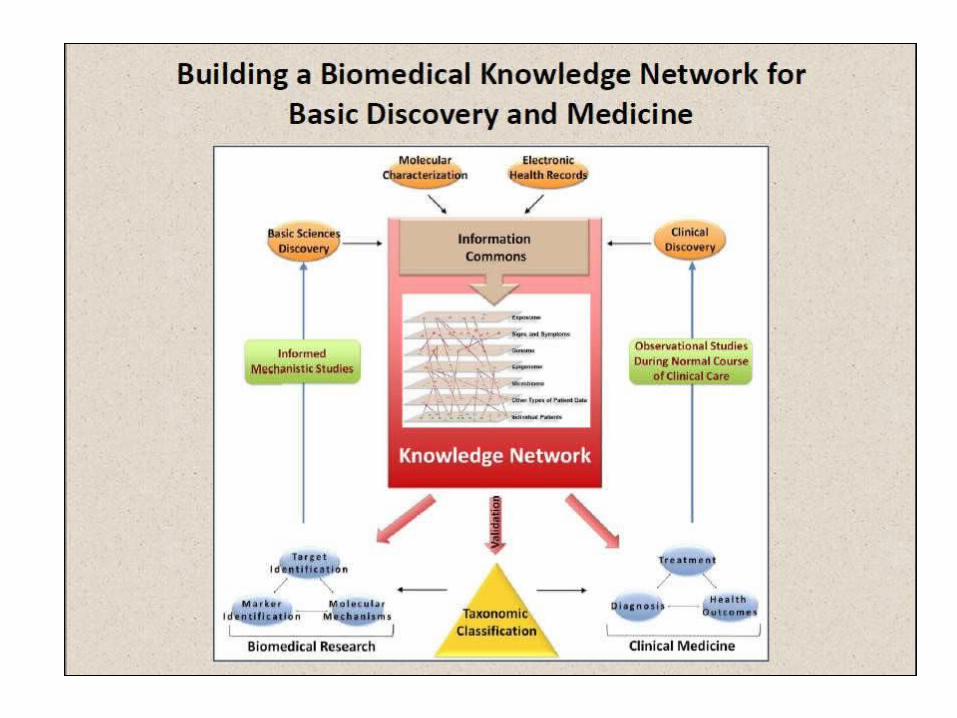
Toward Precision Medicine: Building Knowledge Network for BiomedicalResearch and a New Taxonomy of
Disease
New data network Integrates emerging researchOn the molecular makeup of diseases With clinical data on individual patients
Taxonomy” that defines disease Based on underlying molecular And environmental causes
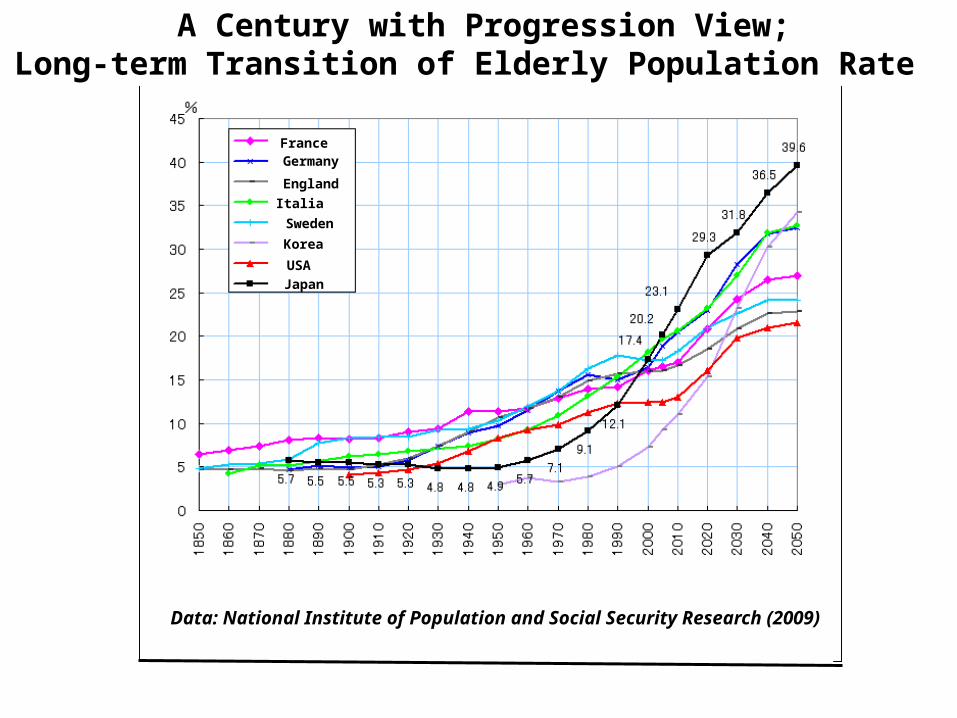
A Century with Progression View;Long-term Transition of Elderly Population Rate
FranceGermany
England
Italia
Sweden
Korea
USA
Japan
Data: National Institute of Population and Social Security Research (2009)
21/09/2004 15
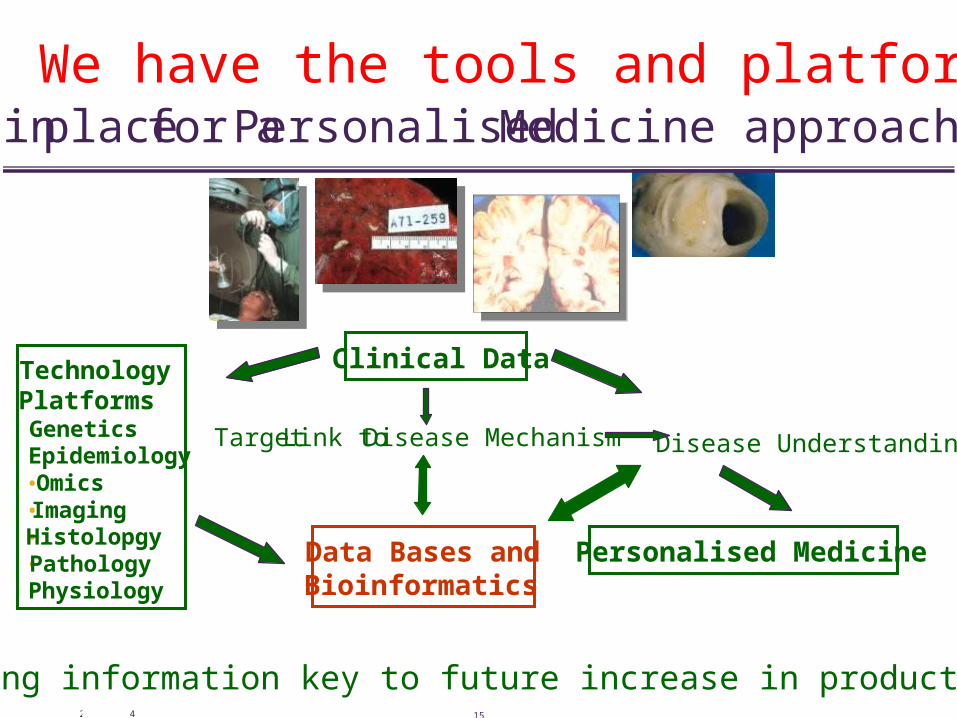
We have the tools and platforms in place for a Personalised Medicine approach
Technology Platforms•Genetics•Epidemiology•Omics•Imaging•Histolopgy•Pathology•Physiology
Data Bases and Bioinformatics
Clinical Data
Target Link to Disease Mechanism Disease Understanding
Sharing information key to future increase in productivity
Personalised Medicine
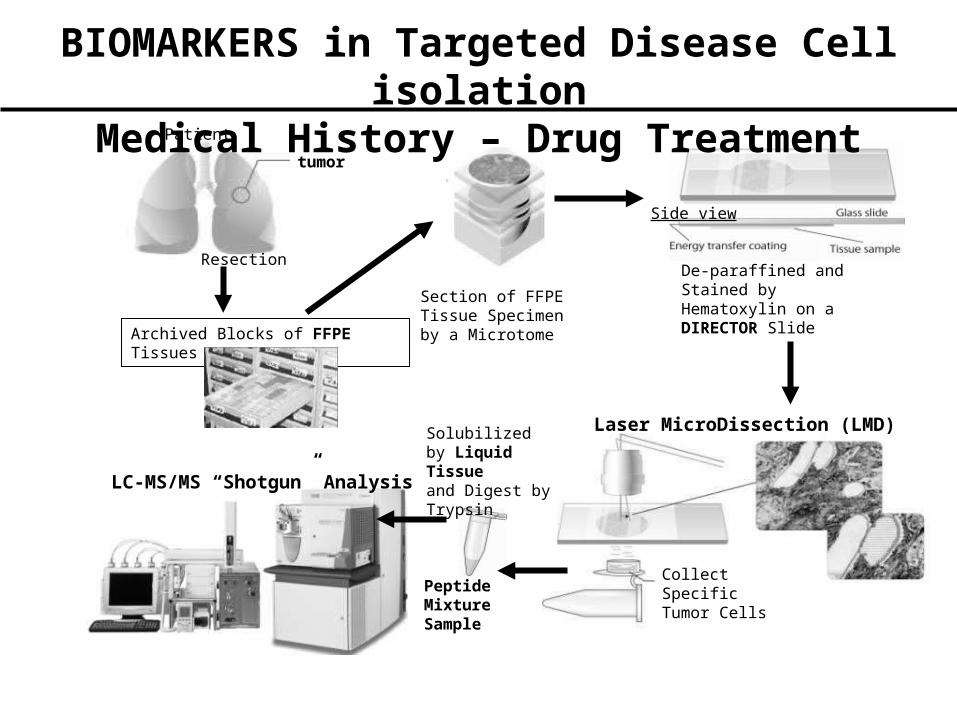
tumor
Section of FFPETissue Specimen by a MicrotomeArchived Blocks of FFPE Tissues
De-paraffined and Stained by Hematoxylin on aDIRECTOR Slide
Laser MicroDissection (LMD)
Collect Specific Tumor Cells
Solubilized by Liquid Tissueand Digest by Trypsin
Peptide Mixture Sample
LC-MS/MS “Shotgun” Analysis
Patient
Side view
Resection
BIOMARKERS in Targeted Disease Cell isolation
Medical History – Drug Treatment
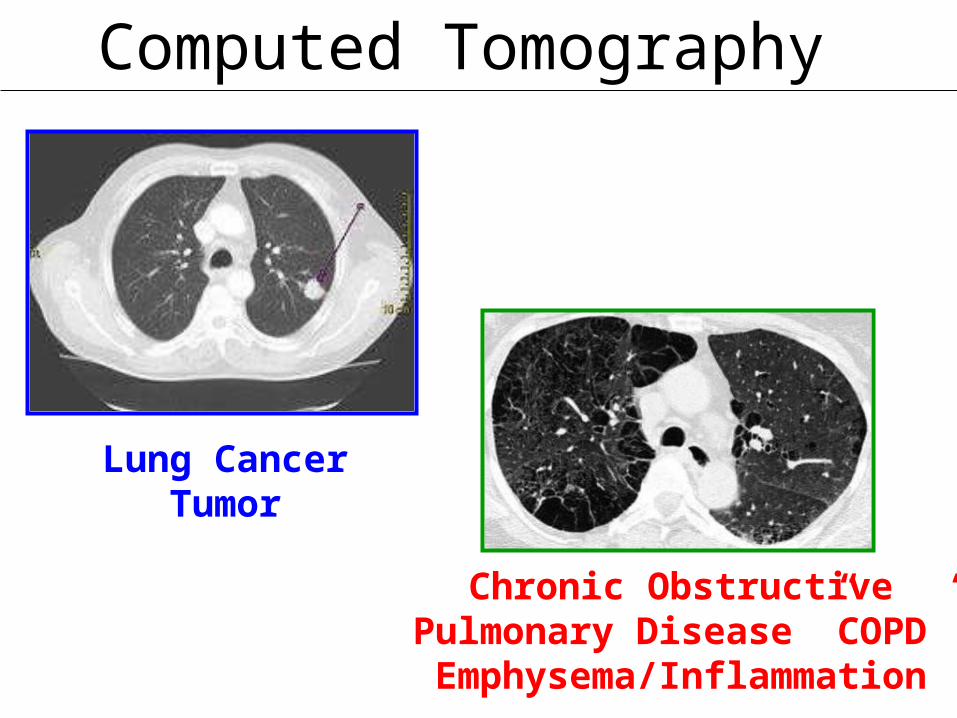
Computed Tomography
Lung CancerTumor
Chronic ObstructivePulmonary Disease ”COPD”Emphysema/Inflammation
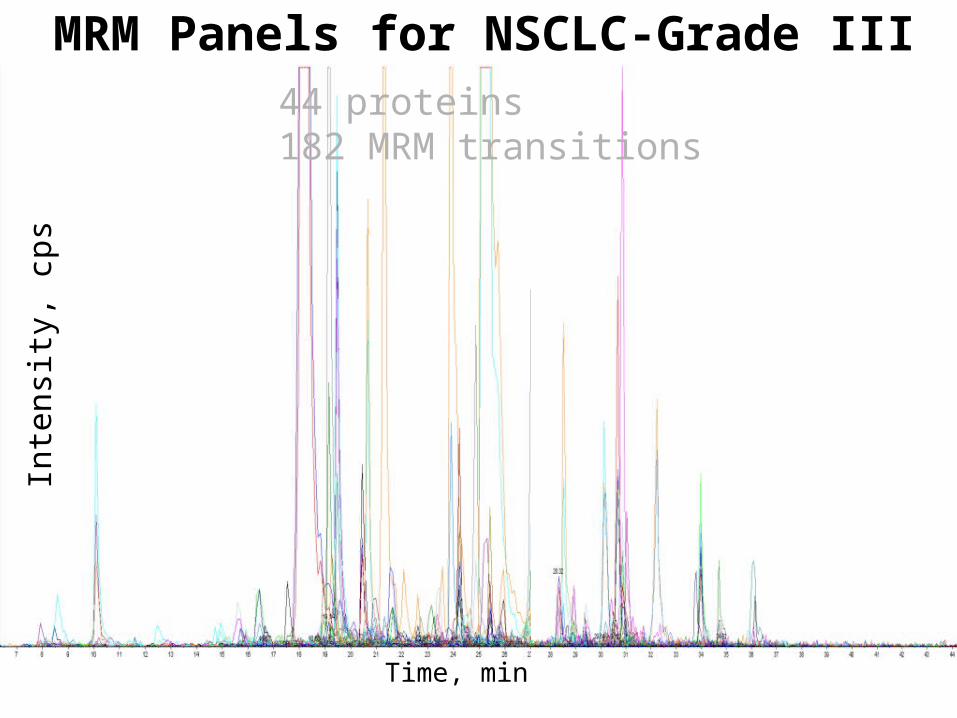
Time, min
Inte
nsi
ty,
cps
44 proteins182 MRM transitions
MRM Panels for NSCLC-Grade III

Localization with Hospital Accesss - both Clinical & Pathology
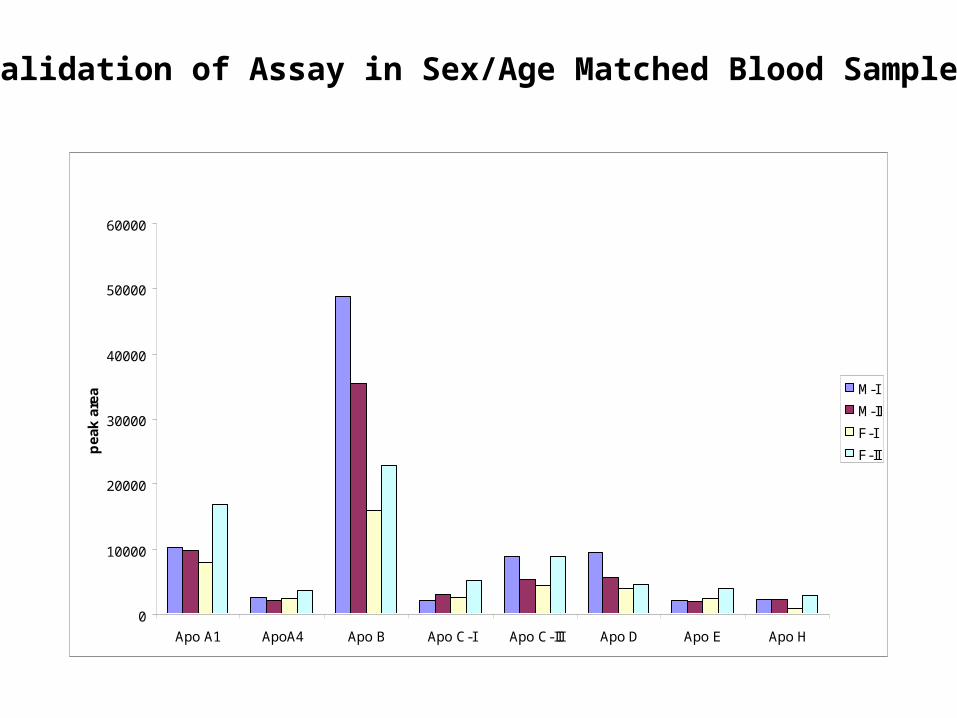
MRM in pooled plasma samples
0
10000
20000
30000
40000
50000
60000
Apo A1 ApoA4 Apo B Apo C-I Apo C-III Apo D Apo E Apo H
pe
ak
are
a M-I
M-II
F-I
F-II
Validation of Assay in Sex/Age Matched Blood Samples
Biobanking – Lung Cancer/ Cardiovascular Diseases/COPD
10 Million Samples – 5 Year Longitudinal Collection
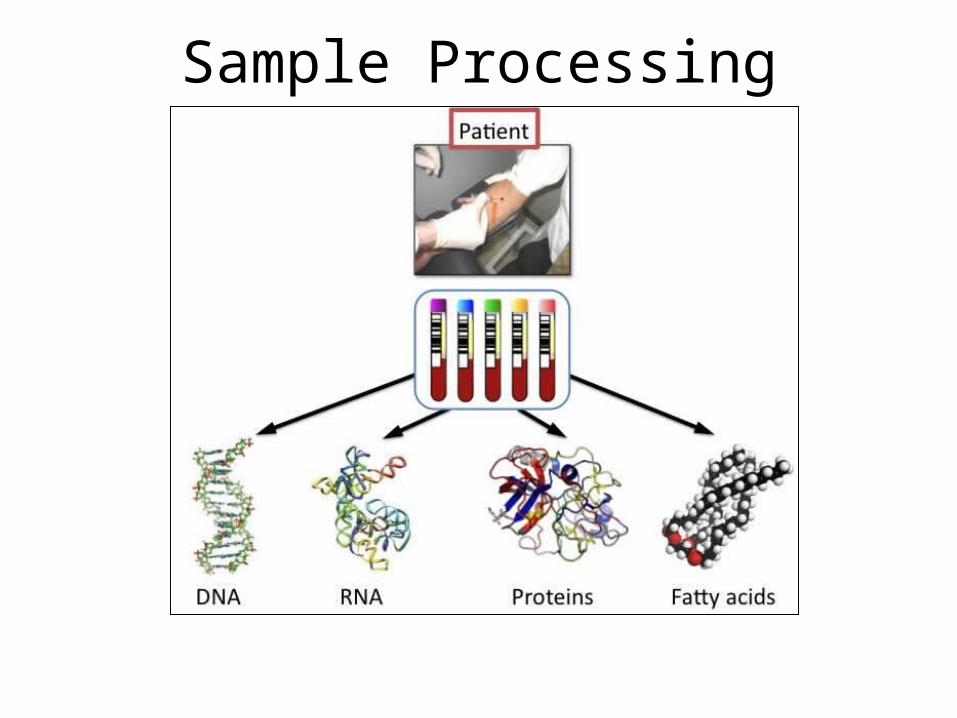
Sample Processing
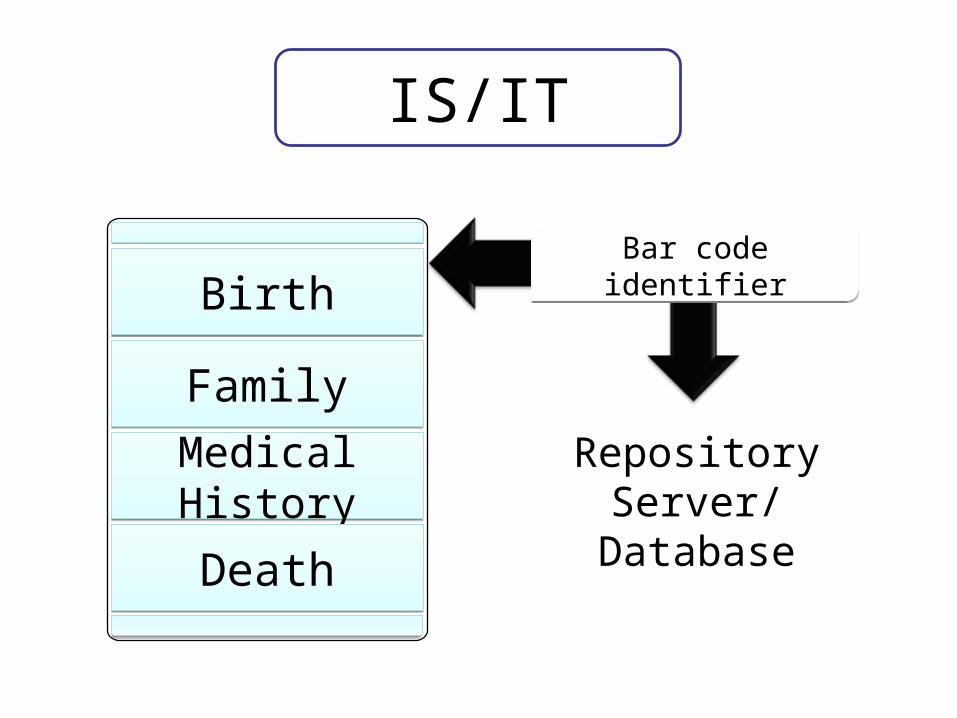
IS/IT
BirthBirth
FamilyFamily
Medical HistoryMedical History
DeathDeath
RepositoryServer/Database
Bar code identifierBar code identifier
Global ProjectGlobal Project
Access code
Access code
Chromosome AnnotationsChromosome Annotations
Reported ValueReported Value
Clinical Delivery & Disease LinkClinical Delivery & Disease Link
Patient BenefitPatient Benefit
Targeted Treatment in Asia
• Asian mutations in the EGFR are found to be as high as 40-60%
• At 10-15% in the western population, a very interesting• Observation that is proving to have medical
consequences for cancer frequency, based on a genetic background
• It is evident in Asian populations that the majority of theNSCLC treated patients with activated mutations achieveda durable and effective response with EGFR TKI-treatment –
Gefitinib (IRESSA) and Erlotinib (TARCEVA)
Case Control Study in Japan• Case-control study in Japan - Observational study of ILD • In a cohort of advanced NSCLC patients receiving treatment either with
gefitinib or other chemotherapy• Planned cohort recruitment about 4000 patients
52 Clinics involved throughout JapanProteomics performed on gefitinib treated patients that develop ILD and controls
Probably the Largest Clinical Proteomics Biomarker Activity
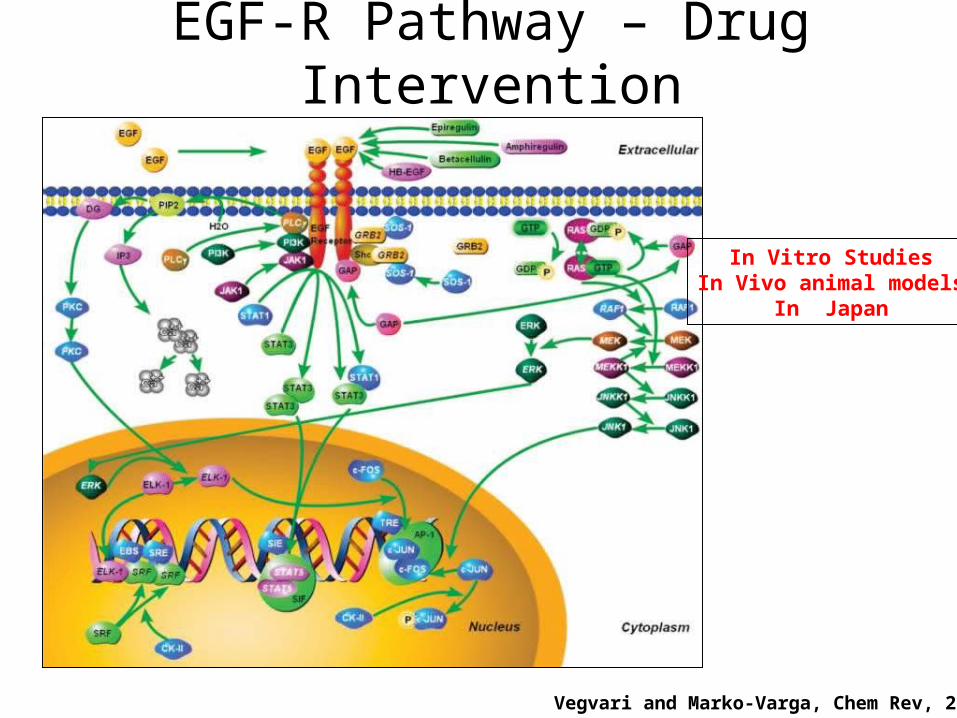
EGF-R Pathway – Drug Intervention
Vegvari and Marko-Varga, Chem Rev, 2010
In Vitro StudiesIn Vivo animal models
In Japan
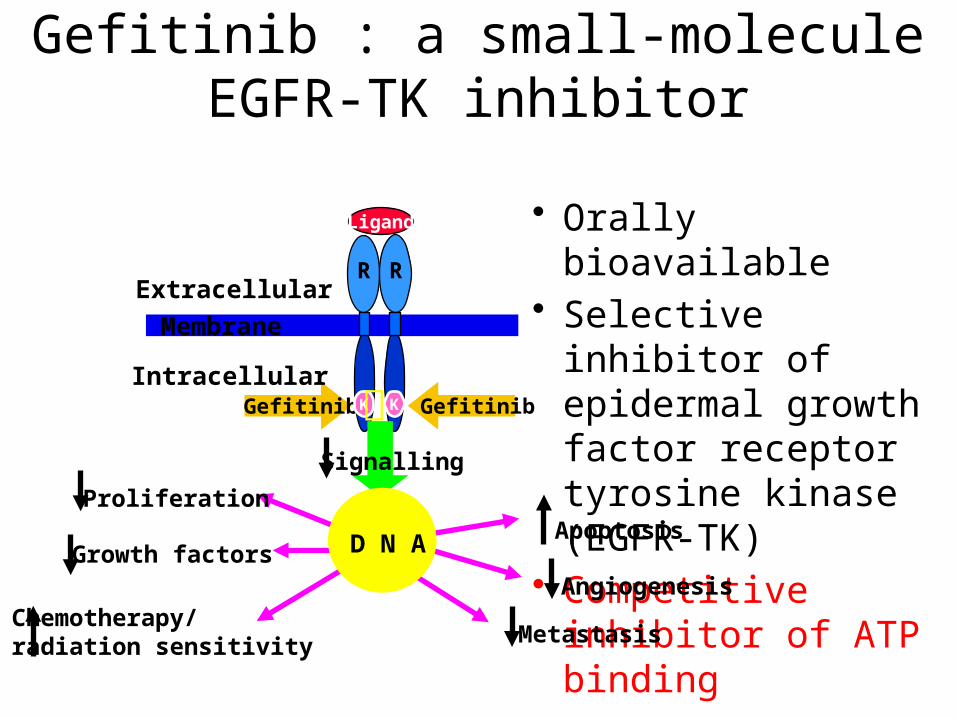
Gefitinib : a small-moleculeEGFR-TK inhibitor
• Orally bioavailable• Selective inhibitor of
epidermal growth factor receptor tyrosine kinase (EGFR-TK)
• Competitive inhibitor of ATP bindingApoptosis
Angiogenesis
R
K
R
GefitinibGefitinib
Ligand
Membrane
Extracellular
IntracellularK
Signalling
Growth factors
Proliferation
MetastasisChemotherapy/radiation sensitivity
D N A
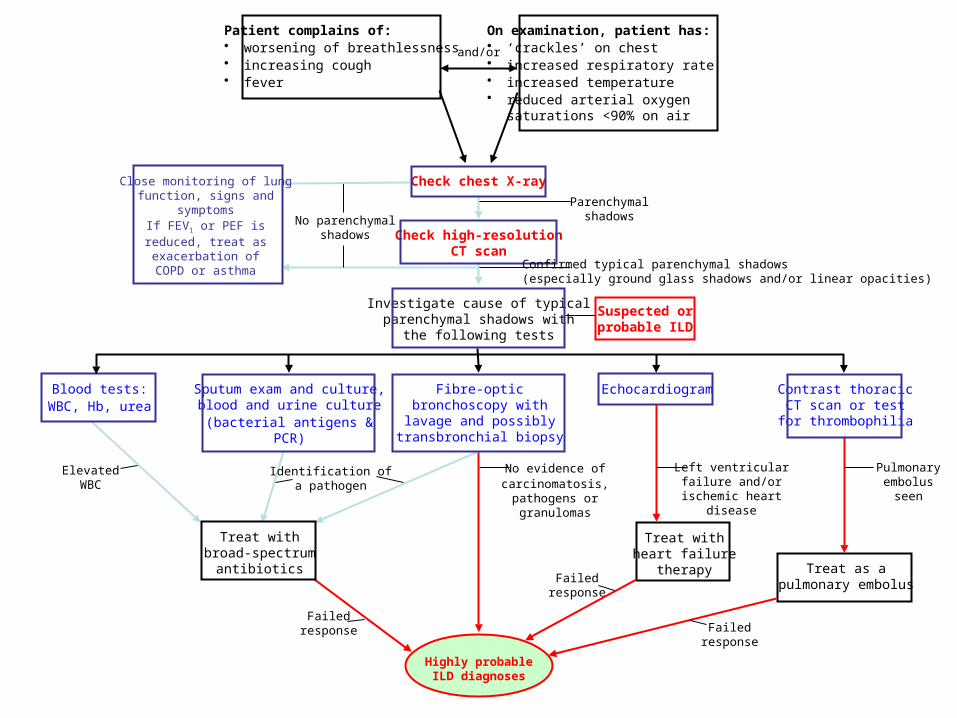
Patient complains of:• worsening of breathlessness• increasing cough• fever
On examination, patient has:• ‘crackles’ on chest• increased respiratory rate• increased temperature• reduced arterial oxygen
saturations <90% on air
Check chest X-ray
Check high-resolutionCT scan
Close monitoring of lungfunction, signs and
symptomsIf FEV1 or PEF isreduced, treat asexacerbation of
COPD or asthma
No parenchymalshadows
Parenchymalshadows
Investigate cause of typicalparenchymal shadows with
the following tests
Suspected orprobable ILD
Confirmed typical parenchymal shadows(especially ground glass shadows and/or linear opacities)
Fibre-opticbronchoscopy withlavage and possibly
transbronchial biopsy
Echocardiogram Contrast thoracicCT scan or test
for thrombophilia
Sputum exam and culture,blood and urine culture(bacterial antigens &
PCR)
Blood tests:WBC, Hb, urea
and/or
No evidence ofcarcinomatosis,
pathogens orgranulomas
Left ventricularfailure and/or
ischemic heartdisease
Pulmonaryembolus
seen
ElevatedWBC
Identification ofa pathogen
Failedresponse
Failedresponse
Failedresponse
Highly probableILD diagnoses
Treat withbroad-spectrum
antibiotics
Treat withheart failure
therapy Treat as apulmonary embolus
p:\proteo_data\...\case\ccs_cs01_01285 2004/11/08 17:23:10 SC1285B
RT: 5.00 - 75.00
5 10 15 20 25 30 35 40 45 50 55 60 65 70 75Time (min)
0
50
100
0
50
100
0
50
100
0
50
100
0
50
100
0
50
100
19.45529.7 47.53
807.4 58.87786.5
20.62575.7
59.82816.2
27.51570.2
67.93757.0
34.93671.5
19.30529.6
38.69881.5
73.33735.2
49.63946.3
57.14853.4
47.45807.8
12.06608.7
9.86580.2
34.68671.5
47.63807.4
65.701248.5
19.34529.6 66.74
725.044.02945.9
42.47808.4
20.39575.7
48.56785.4
59.79816.2
58.87786.5
26.91708.5
34.58671.6
19.22529.7
65.46821.6
10.75485.6
29.37838.728.23
603.043.25807.632.75
613.015.81529.8
23.11570.2
60.73822.1
54.62694.7
63.181248.5
34.60725.4
67.091293.0
46.60837.5
14.23620.7
7.89608.8
36.74725.4
34.69612.9
31.00671.6 45.66
807.569.601292.9
18.09529.8
36.88725.3
26.78688.0
16.63465.8
57.60694.5
65.411086.8
48.16946.4
50.39834.0
12.93462.7
29.09859.5
33.24838.6
39.30725.3 48.18
807.219.34620.5
28.07596.8
40.32585.8
72.041292.8
66.811248.550.86
837.360.18694.4
59.37786.5
17.29530.013.98
608.56.21
638.3
31.77838.7 38.27
725.327.61859.4 31.97
838.839.19585.6
26.28596.8
17.34465.7
62.44984.5
65.29821.8
50.01837.3
71.65894.8
10.37485.6
52.27859.3
58.21776.5
NL: 7.43E6Base Peak F: ITMS + c NSI Full ms [ 450.00-2000.00] MS CCS_CT01_05921
NL: 5.60E6Base Peak F: ITMS + c NSI Full ms [ 450.00-2000.00] MS ccs_ct01_05479
NL: 4.48E6Base Peak F: ITMS + c NSI Full ms [ 450.00-2000.00] MS ccs_ct01_02176
NL: 9.66E6Base Peak F: ITMS + c NSI Full ms [ 450.00-2000.00] MS ccs_ct01_03034
NL: 7.38E6Base Peak F: ITMS + c NSI Full ms [ 450.00-2000.00] MS ccs_ct01_04729
NL: 5.58E6Base Peak F: ITMS + c NSI Full ms [ 450.00-2000.00] MS ccs_cs01_01285
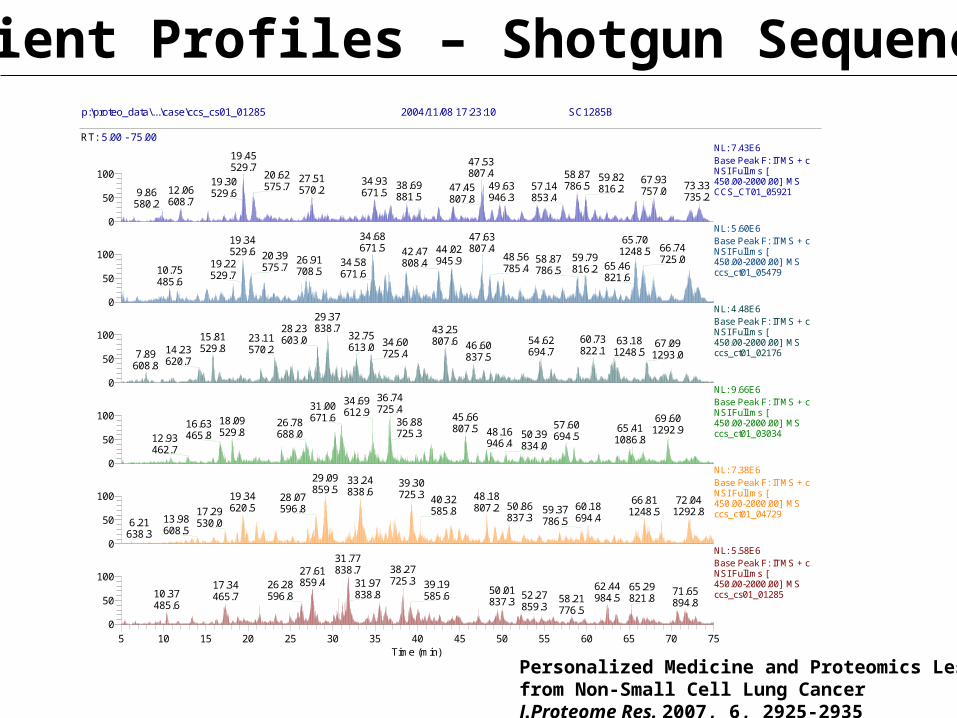
Patient Profiles – Shotgun Sequencing
Personalized Medicine and Proteomics Lessons from Non-Small Cell Lung CancerJ.Proteome Res. 2007, 6, 2925-2935
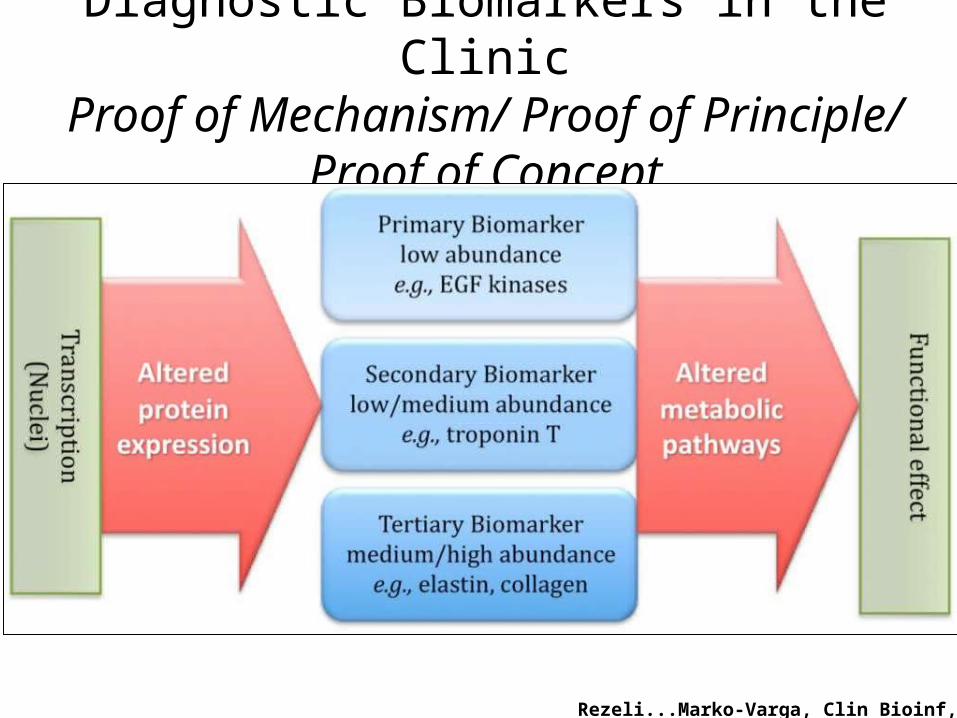
Diagnostic Biomarkers in the ClinicProof of Mechanism/ Proof of Principle/ Proof of Concept
Rezeli...Marko-Varga, Clin Bioinf, 2011
Compound Tissue Imaging
Targeting the “HEART” of the interaction
Drug Target & Drug Compound
25
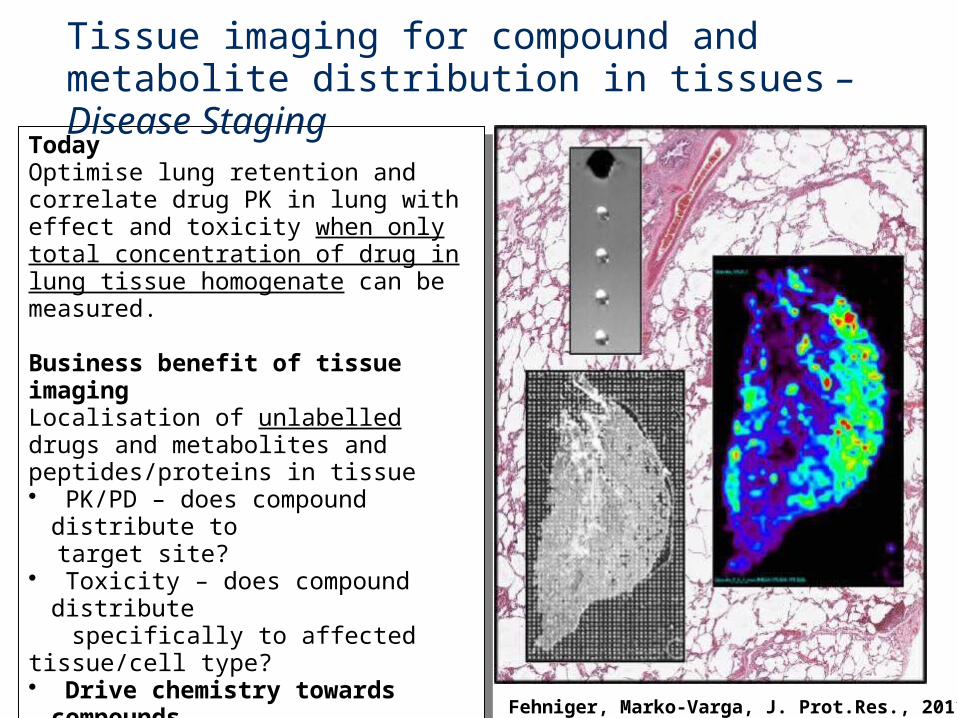
Today Optimise lung retention and correlate drug PK in lung with effect and toxicity when only total concentration of drug in lung tissue homogenate can be measured.
Business benefit of tissue imagingLocalisation of unlabelled drugs and metabolites and peptides/proteins in tissue• PK/PD – does compound distribute to target site? • Toxicity – does compound distribute specifically to affected tissue/cell type?• Drive chemistry towards
compounds with optimal distribution – FIC & BIC• Applicable to
Lung/Liver/Kidney/Brain Pathophysiology
Today Optimise lung retention and correlate drug PK in lung with effect and toxicity when only total concentration of drug in lung tissue homogenate can be measured.
Business benefit of tissue imagingLocalisation of unlabelled drugs and metabolites and peptides/proteins in tissue• PK/PD – does compound distribute to target site? • Toxicity – does compound distribute specifically to affected tissue/cell type?• Drive chemistry towards
compounds with optimal distribution – FIC & BIC• Applicable to
Lung/Liver/Kidney/Brain Pathophysiology
Tissue imaging for compound and metabolite distribution in tissues – Disease Staging
Fehniger, Marko-Varga, J. Prot.Res., 2011,11,3
GRADINGof Disease
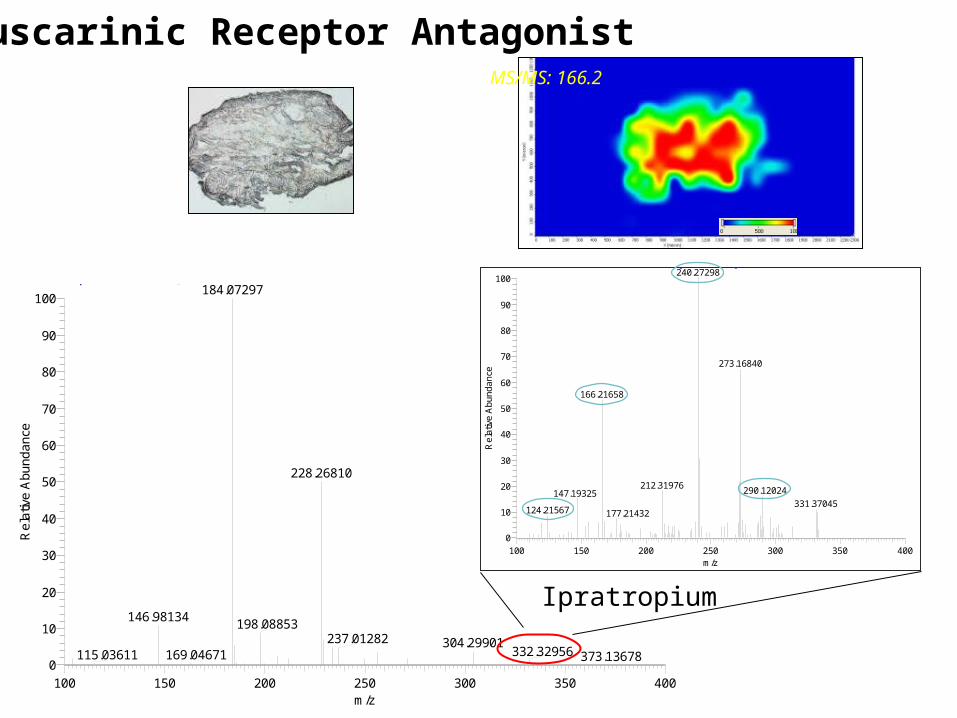
PtN_sample1_slide6A_100629_100um_FTMS_ITMS2_332 #176 RT: 4.87 AV: 1 NL: 1.21E3T: ITMS + c MALDI w Full ms2 [email protected] [90.00-500.00]
100 150 200 250 300 350 400m/z
0
10
20
30
40
50
60
70
80
90
100
Re
lativ
e A
bu
nd
an
ce
240.27298
273.16840
166.21658
212.31976290.12024147.19325
331.37045124.21567 177.21432
PtN_sample1_slide6A_100629_100um_FTMS_ITMS2_332 #387 RT: 10.19 AV: 1 NL: 6.02E6T: FTMS + p MALDI Full ms [100.00-1000.00]
100 150 200 250 300 350 400m/z
0
10
20
30
40
50
60
70
80
90
100
Re
lativ
e A
bu
nd
an
ce
184.07297
228.26810
146.98134198.08853
237.01282 304.29901332.32956169.04671115.03611 373.13678
MS/MS: 166.2
Muscarinic Receptor Antagonist
Ipratropium
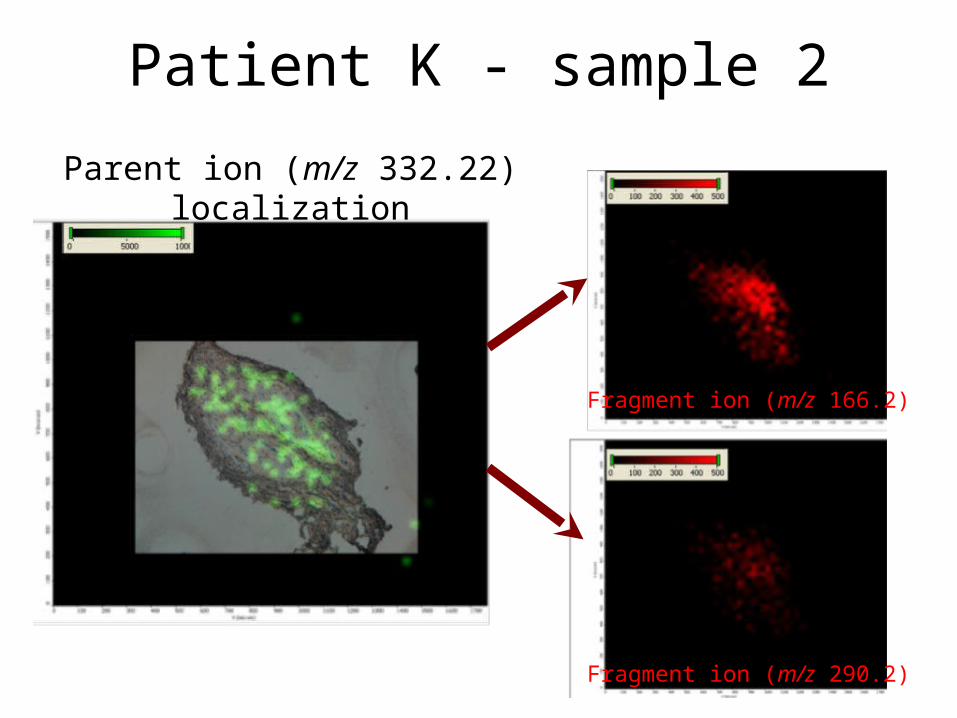
Patient K - sample 2
Parent ion (m/z 332.22)localization
Fragment ion (m/z 166.2)
Fragment ion (m/z 290.2)
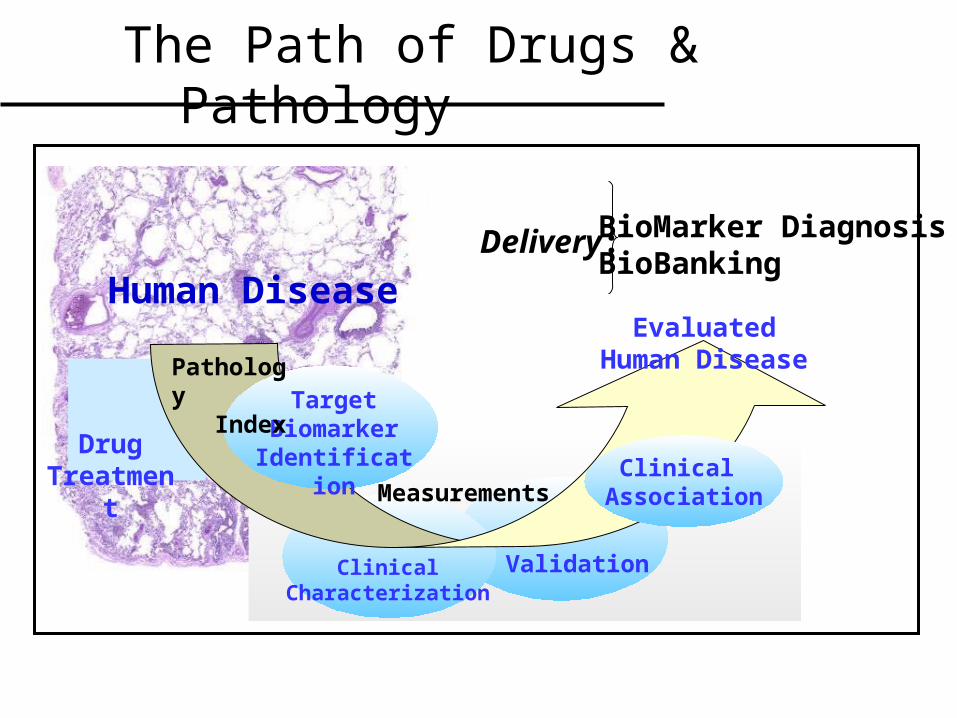
The Path of Drugs & Pathology
Human Disease
Drug Treatment
Delivery: BioMarker DiagnosisBioBanking
ClinicalCharacterization
Validation
Target Biomarker
Identification Measurements
EvaluatedHuman Disease
Clinical Association
Pathology Index
In Summary
• Precision Medicine – Novel Direction• MultiPlex Protein Sequencing Assay
Platform• Personalized Medicine – Mass Spec Drug
Imaging• BioBank – High quality sample archives• Biomarkers – Biology Guidance and
prediction