Embed Size (px)
DESCRIPTION
TO HELP OUR COUNTRY FUTURE BY A WORD AS A DOCTOR
Citation preview

1
1 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
BRONCHOGENIC CARCINOMA
ESSENTIAL FOR DIAGNOSIS:
New cough or change in chronic cough
Dyspnea , haemoptysis ,anorexia
New or enlarging mass , persistant infiltration , atelectasis or pleural effusion on
CXR
Male ; smoker ;age ˃ 40 years
Cytological finding on sputum ,pleural fluid ,biopsy
RISK FACTORS
Cigarette smoking 90% male ; 80% female---critical in the history
A familial predisposition is recognized
Increased risk in COPD ,sarcoidosis , pulmonary fibrosis , scleroderma
Environmental risk factors:
Asbestosis (( pipe lagging ;electrical wire insulation ))
Chromium
Arsenic
Iron oxides
Radon gas

2
2 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
HISTOLOGY:
1. SCLC==small cell lung cancer 25%
Prone to early haematogenous spread ;rarely amenable to surgery
2. NSCLC==non—small cell lung cancer
Early disease may be cured resection; spread slowly –
Squamous cell ca.--- 25%--- centrally located and spread slowly
Adenocarcinoma ----40%---peripheral nodule or mass
Small cell ca. ------20%--- begins centrally and infiltrate submucosa
Large cell ca.-------10%---peripheral or central
Brocchoalveolar cell ca.----spreads intraalveolar
DIFFERENTIAL DIAGNOSIS:
1. Pneumonia
2. Tuberculosis
3. Lymphoma
4. Metastatic carcinoma
5. Sarcoidosis
6. Foreign body aspiration
7. Benign carcinoid tumour
SIGNS AND SYMPTOMS:
75%--90% are symptomatic at the time of diagnosis.
The presentation depends on:
1. Type of tumour
2. Location of tumour
3. Extent of spread
4. Presence of paraneoplastic syndrome
A. Chest symptoms:
Cough --- new onset or change of the quality and severity of cough in s
smoker who used to have a chronic cough.
Haemoptysis---30%
Dyspnea --------60%

3
3 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
Chest pain------ 40% from bony metastasis or pleural involvement .
LOCAL SPREAD----preesure by the mass over the surrounding structures or
spread to them----from the lymph node 2ry or the mass causing
endobronchial obstruction and postobstructive pneumonia (( unresolving
or recurrent )) .Lung cancer is one of the causes of unresolving pneumonia
or persistent lung opacity in smoker male ˃50yr.
B. Pressure symptoms:
Esophagus ---dysphagia
Trachea ---- stridor , change of the voice , hoarsness
Recurrent laryngeal nerve----- hoarsness of voice
C. Superior vena cava obstruction:
Caused by partial or complete obstruction of SVC.
C/F—
Swelling of the face and neck
Headache ,dizziness ,syncope
Visual disturbance
Facial flushing
Dilated anterior chest wall veins or collateral veins
Brawny eodema
Cyanosis of the face and arms
Bending over or laying down accentuates symptoms.
D/D OF SVC OBSTRUCTION: 1. Superior mediastinal tumors:
Lung ca. , thyroid ca. ,thymoma ,lymphoma ,teratoma , angiosarcoma
2. Aneurysm of the aortic arch
3. Chronic fibrotic mediastinitis---TB ,histoplasmosis ,pyogenic ,methysergide.
4. Constrictive pericarditis
5. Thrombophlebitis 2ry to CVL or pacemaker wire.
For diagnosis:
HISTORY / EXAMINATION
CT SCAN / MRA
CONTRAST VENOGRAPHY

4
4 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
TREATMENT OF SVC: 1) Surgery
2) Chemotherapy
3) External beam radiation
4) Endovascular stenting
5) Venous angioplasty or bypass Horners syndrome-----pancoasts tumour:
Pancoast tumors are lung cancers that begin at the top of the right or left lung and
invade the chest wall. They are also called superior sulcustumors . Apical lung
cancer with invasion of cervical sympathetic chain plexus resulting in:
1. Miosis (( constricted pupil ))
2. Enophthalmos (( sunken eye ))
3. Partial ptosis
4. Ipsilateral loss of sweating (( anhidrosis))
Pancoast tumor causes shoulder ,arm pain (( brachial plexus )) , C8—T2 invasion.
Pain in the shoulder, radiating down the upper inner arm, can be the first sign of a
Pancoast tumor. The patient may have Hoarse of voice or bovine cough with
unilateral recurrent laryngeal nerve palsy and vocal cord paralysis.
D. The patient may present with evidence of metastasis to other systems

5
5 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
Brain – severe headache of recent onset in elder smoker male, convulsion
in a patient above age of 40y with lung opacity in smoker , coma ,gradual
onset of limb weakness of month duration in elder male smoker.
Liver --- vague abdominal pain ,abdominal mass , jaundice.
Adrenal ---lose of weight and apetite with hypoglycemia .
E. Paraneoplastic syndrome: A paraneoplastic syndrome is a disease or symptom that is the consequence of cancer in
the body but, unlike mass effect, is not due to the local presence of cancer cells. These
phenomena are mediated by humoral factors (by hormones or cytokines) excreted by
tumor cells or by an immune response against the tumor. Paraneoplastic syndromes are
typical among middle aged to older patients, and they most commonly present with
cancers of the lung, breast, ovaries or lympSMALL CELL CARCINOMAhatic system
(a lymphoma). Sometimes the symptoms of paraneoplastic syndromes show before the
diagnosis of a malignancy, which has been hypothesized to relate to the disease
pathogenesis.
Commonly seen in small cell lung carcinoma. The patient will show dysfunction of the
central nervous system and endocrine system with out metastasis.
A. ENDOCRINE---
Small cell carcinoma 1.Cushing syndrome---biochemical –low K
2.SIADH
3.Hyperaldosteronism
Squamous carcinoma 1.Hypercalcemia
2.Hyperparathyrodism--Parathyroid hormone-related protein), TGF-α, TNF, IL-1[7]
Bronchial adenoma --
Carcinoid syndrome
B. NEUROLOGICAL-
1. Peripheral neuropathy
2. Subacute sensory neuropathy
3. Guillain-Barré syndrome
4. Eaton-Lambert syndrome
5. Subacute cerebellar degeneration
6. Encephalitis
7. Subacute necrotizing myelopathy
8. Dermatomyositis
9. Subacute motor neuronopathy
1.Peripheral neuropathy is the most common neurologic paraneoplastic syndrome. It is usually a
distal sensorimotor polyneuropathy that causes mild motor weakness, sensory loss, and absent
distal reflexes.
2.Subacute sensory neuropathy is a more specific but rare peripheral neuropathy. Dorsal root
ganglia degeneration and progressive sensory loss with ataxia but little motor weakness develop;
the disorder may be disabling. Anti-Hu, an autoantibody, is found in the serum of some patients
with lung cancer. There is no treatment.

6
6 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
3.Guillain-Barré syndrome, another ascending peripheral neuropathy, is a rare finding in the
general population and probably more common in patients with Hodgkin lymphoma.
4.Eaton-Lambert syndrome is an immune-mediated, myasthenia-like syndrome with weakness
usually affecting the limbs and sparing ocular and bulbar muscles. It is presynaptic, resulting
from impaired release of acetylcholine from nerve terminals. An IgG antibody is involved. The
syndrome can precede, occur with, or develop after the diagnosis of cancer. It occurs most
commonly in men with intrathoracic tumors (70% have small or oat cell lung carcinoma).
Symptoms and signs include fatigability, weakness, pain in proximal limb muscles, peripheral
paresthesias, dry mouth, erectile dysfunction, and ptosis. Deep tendon reflexes are reduced or
lost. The diagnosis is confirmed by finding an incremental response to repetitive nerve
stimulation: Amplitude of the compound muscle action potential increases > 200% at rates > 10
Hz. Treatment is first directed at the underlying cancer and sometimes induces
remission. Guanidine (initially 125 mg po qid, gradually increased to a maximum of 35 mg/kg),
which facilitates acetylcholine release, often lessens symptoms but may depress bone marrow
and liver function. Corticosteroids and plasma exchange benefit some patients.
5.Subacute cerebellar degeneration causes progressive bilateral leg and arm ataxia, dysarthria,
and sometimes vertigo and diplopia. Neurologic signs may include dementia with or without brain
stem signs, ophthalmoplegia, nystagmus, and extensor plantar signs, with prominent dysarthria
and arm involvement. Cerebellar degeneration usually progresses over weeks to months, often
causing profound disability. Cerebellar degeneration may precede the discovery of the cancer by
weeks to years. Anti-Yo, a circulating autoantibody, is found in the serum or CSF of some
patients, especially women with breast or ovarian cancer. MRI or CT may show cerebellar atrophy,
especially late in the disease. Characteristic pathologic changes include widespread loss of
Purkinje cells and lymphocytic cuffing of deep blood vessels. CSF occasionally has mild
lymphocytic pleocytosis. Treatment is nonspecific, but some improvement may follow successful
cancer therapy.
6.Encephalitis may occur as a paraneoplastic syndrome, taking several different forms,
depending on the area of the brain involved.
1. Global encephalitis has been proposed to explain the encephalopathy that occurs most
commonly in small cell lung cancer.
2. Limbic encephalitis is characterized by anxiety and depression, leading to memory loss,
agitation, confusion, hallucinations, and behavioral abnormalities.
Anti-Hu antibodies, directed against RNA binding proteins, may be present in the serum
and spinal fluid. MRI may disclose areas of increased contrast uptake and edema.
7.Subacute necrotizing myelopathy is a rare syndrome in which rapid ascending sensory and
motor loss occurs in gray and white matter of the spinal cord, leading to paraplegia. MRI helps

7
7 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
rule out epidural compression from metastatic tumor—a much more common cause of rapidly
progressive spinal cord dysfunction in patients with cancer. MRI may show necrosis in the spinal
cord.
C. Hypertrophic osteoarthropathy is prominent with certain lung cancers and manifests as
painful swelling of the joints (knees, ankles, wrists, elbows, metacarpophalangeal joints) with
effusion and sometimes fingertip clubbing.
SIGNS:
Cachexia , Anemia ,Lymphadenopathy – suparclavicular and axillary ,clubbing .
Ptosis with atrophy of small muscles of hand on the same side , enophthalmos if apical
Chest ---- may be normal , or signs of consolidation ,or pleural effusion or collapse
Situation in which lung cancer should be a high suspicion:
1. Unexplained unilateral pleural effusion of ˃2 month in elder smoker
2. Unresolving signs of lung consolidation of ˃ 1 month duration
INVESTIGATION:
Routine --- CBC ,RFT ,LFT, BLOOD SUGER ,S. CALCIUM , LDH ,ALP
CBC--- complete blood count
RFT ----renal function test
LFT----liver function test
LDH---lactic dehydrogenase
ALP----alkaline phosphokinase
1. Sputum cytology---highly specific but insensitive
2. Serum tumor markers ----are neither sensitive nor specific
3. Tissue or cytology specimen is needed for diagnosis.
Tissue diagnosis may not necessary prior to surgery in some cases where the
lesion is enlarging or the patient will undergo Surgical resection regardless of the
outcome of biopsy
4. Pulmonary function tests are required in all NSLC patients prior to surgery.
Preoperative FEV1 ˃2 L is adequate to undergo surgery.
Estimate of postresection FEV1 is needed if ˂ 2L preoperative.

8
8 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
5. Imaging studies
Nearly all patients have abnormal findings on CXR or CT SCAN
Pleural effusion
Peripheral circular opacity
Hilar adenopathy and mediastinal thickening (( squamous))
Infiltrates single or multiple nodules (( alveolar))
Central or peripheral masses ((large cell))
Consolidation
Lung collapse
Bony secondaries

9
9 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
CT scan of chest through the adrenal glands :
May not be necessary if patient has obvious M1 disease
IV iodine contrast enhancement is not essential but is recommended in probable
mediastinal invasion.
Is the most important modality in staging to determine the resectibility of the
tumour.
For staging ,Brain MRI , Abdominal CT or radionuclide bone scanning should be
targeted to symptoms and signs.
Recommended tests for selected patients:
1. Ultra sound liver/CT liver with contrast
Abnormal clinical evaluation
Increased LFT
Abnormal non contrast CT

10
10 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
2. MRI brain /CT brain with contrast
CNS symptoms
Abnormal clinically
3. Radionuclide bone scan
Increase ALP
Increase calcium
Bony pain
4. Pulmonary function test
Lung resection
Thoracic radiotherapy
5. Quantative radionuclide perfusion
Lung scan or exercise testing to evaluate maximum o2 consumption.
DIAGNOSTIC PROCEDURES:
1. Bronchoscopy---tissue diagnosis(10%—90%) and operability
2. Percutaneous fine needle aspiration---sensitivity 50%--90% for peripheral lesions
and superficial lymph nodes.
3. Thoracocentesis can be diagnostic in malignant effusion ((65%))
4. Thoracoscopy ---is preferred to pleural biopsy if pleural fluid cytology non
diagnostic after two thoracocentensis
5. Mediastinoscopy
Treatment SUMMARY: NSCLC
Excision is the treatment of choice for peripheral tumors with no metastatic
spread stage I / II 25%
Curative radiotherapy is an alternative if respiratory reserve poor
Chemotherapy and radiotherapy—for more advanced disease.
It is staged with TNM international staging system.
SCLC
Are nearly always disseminated at presentation
They may respond to chemotherapy
SATGING OF THE LUNG CANCER:
T---PRIMARY TUMOUR
T0----no evidence of primary tumour
Tx----malignant cells in the bronchial secretion but not visualized
Tis--- carcinoma in situ
T1---- ≤ 3cm , surrounded by lung or visceral pleura ,in lobar or more distal airway
T2 --- ˃ 3cm , or any size either involves a main bronchus “ ˃ 2 cm distal to the
carina” , OR any size invades the visceral pleura , OR has associated atelectasis ,
obstructive pneumonitis extending to the hilum but not all the lung.

11
11 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
T3---- any size with direct extension into the chest wall ,diaphragm ,mediastinal
pleura ,parietal pericardium , OR tumor in the main bronchus ˂ 2cm distal to
carina with out involving the carina , OR atelectasis or obstructive pneumonitis
involving the entire lung
T4---- any size , with invasion of mediastinum ,heart ,great vessels ,trachea
,oesophagus , vertebral body , carina or malignant effusion ((pleura&pericardium))
Or satellite tumor nodules within the ipsilateral lobe of the lung.
N----REGINAL NODES
Nx---------------------------cant be assessed
No---------------------------none involved “ mediastinoscopy “
N1--------------------------- peribrochial / ipsilateral hilum / both
N2---------------------------I-mediastinal /subcarinal
N3-------------------------- contralateral mediastinal/ hilum /supraclavicular (ips/contra)
M----DISTANT METASTASIS
Mo--------------none
M1--------------present
STAGE
TUMOUR
LYMPH NODE
METASTASIS survival
I.
Tis, T1 or T2 Limited local disease
NO
MO 74%
II.
T1 // T2 T3 Limited local diseae w ipsilateral hilar/ locally invasive
N1 N0
MO 55% MO 39%
III a
T3 T1---T3 Limited local disease w perbronchial /locally with invasive subcarinal
N1 N2
MO 22% MO
III b
T1-----T4 T4 Contralateral LN ,supraclavicular ,malignant effusion
N3 N0---N2
MO MO
IV
T1-----T4 Distant metastases
No-N3
M1

12
12 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014

13
13 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
TREATMENT:
NON SMALL CELL LUNG CANCER (( NSCLC))
A. Stage I / II ------------------------ cured surgically
B. Stage III A ------------------------ may benefit from surgery( multimodal protocols)
C. Stage III B ------------------------ resection surgery after multimodal protocols
D. Stage IV ------------------------- palliative
Neo adjuvant chemotherapy
1. Administration in advance of surgery / radiation therapy
2. Widely used in stage III A and III B
Adjuvant chemotherapy
a) Administration of drugs following surgery / radiotherapy
b) Stage III A // III B who can’t be treated surgically
c) Multidrug platinum based therapy shows a trend toward improved survival in I and IIe

14
14 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
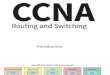
STAGE IIA STAGE IIB

15
15 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
STAGE III A

16
16 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
STAGE III B
STAGE IV
Performance status & symptom control in stage III B & IV may be improved by chemotherapy.
Pleural drainage and pleurodesis—
For symptomatic pleural effusion

17
17 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
Palliative--- radiotherapy=== external beam : used for
a) Bronchial obstruction
b) SVC obstruction
c) Haemoptysis
d) Bony pain
e) Brain metastasis
SVC OBSTRUCTION------- Dexamethazone , Radiotherapy , SVC stent
Endobronchial therapy-------
a) Tracheal stenting
b) Cryotherapy
c) Laser
d) Brachytherapy (( radioactive source ))
Chemotherapy in SCLC:
Limited stage disease ------------------ cisplatin/ etoposide 50%--70%complete response
Extensive disease ------------------ cisplatin / etoposide 15%--40% complete response
Remissions last 6---8 months
Median survival 4 months after recurrence to
a) Cyclophosphamde + Doxorubicin + Vincristin +Etopside
b) Cisplatin + radiotherapy
PROGNOSIS:
NSCLC 50% 2yr with out spread
10% 2yr with spread
SCLC 3 months if untreated
1 ½ year if treated
DRUGS MAY BE USED:
Codeine Bronchodilator analgesics steroids antidepresent

18
18 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014

19
19 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014
OTHER OPTIONS OF TREATMENT:
1.Laser therapy
2.Cryosurgery
3.Photodynamic therapy
4.Electrotherapy
5.Biological therapy---targeted therapy
They include erlotinib (Tarceva),gefitinib (Iressa), crizotinib (Xalkori) and afatinib (Giotrif).

20
20 BRONCHOGENIC CARCINOMA BY DR MAGDI AWAD SASI 2014