Embed Size (px)
Citation preview
Colon CancerBy
Noha El-Baghdady, M.Sc
Colon and rectal cancer are the 3rd leading cause of cancer death in men and
women
Risk Factors
1- Genetic Predisposition2- IBD 3- Tobacco 4- Sedentary life style5- Obesity6- Diet7- Family history
Risk Factors
• Age 50 or older.• A family history of cancer of the colon or rectum.• A personal history of cancer of the colon, rectum, ovary,
endometrium, or breast.• A history of polyps (small pieces of bulging tissue) in the
colon.• A history of ulcerative colitis (ulcers in the lining of the large
intestine) or Crohn disease.• Certain hereditary conditions, such as familial adenomatous
polyposis and hereditary nonpolyposis colon cancer.
Prevention Strategies
1- Fiber Supplementation ….
Decreases Fecal bile acids; decreases transit time, binds to fecal mutagens, dilutes fecal material.
Prevention Strategies
2- Dietary fat Reduction
Decreases fecal bile acids; may reduce consumption of carcinogenic heterocyclic amines associated with meat preparation.
Prevention Strategies
3- Calcium supplementation Reduces the proliferative response to fatty acids and bile acids.
4- Cyclooxygenase inhibition Decreases cox-2 mediated free radical formation; may inhibit growth factor synthesis in response to tumor promoters
Chan AT, Giovannucci EL, Meyerhardt JA et al. Long-term use of aspirin and nonsteroidal anti-inflammatory drugs and risk of colorectal cancer. JAMA. 2005; 294:914-23.Wactawski-Wende J, Kotchen JM, Anderson GL, Calcium plus vitamin D supplementation and the risk of colorectal cancer. N Engl J Med. 2006; 354:684-96.Hawk ET, Levin B. Colorectal Cancer Prevention. J Clin Oncol. 2005; 23:378-91.
Possible signs of colon cancer include a change in bowel habits or blood in the stool
• A change in bowel habits.• Blood (either bright red or very dark) in
the stool.• Diarrhea, constipation, or feeling that the
bowel does not empty completely.• Stools that are narrower than usual.• Frequent gas pains, bloating, fullness, or
cramps.• Weight loss for no known reason.• Feeling very tired.• Vomiting.
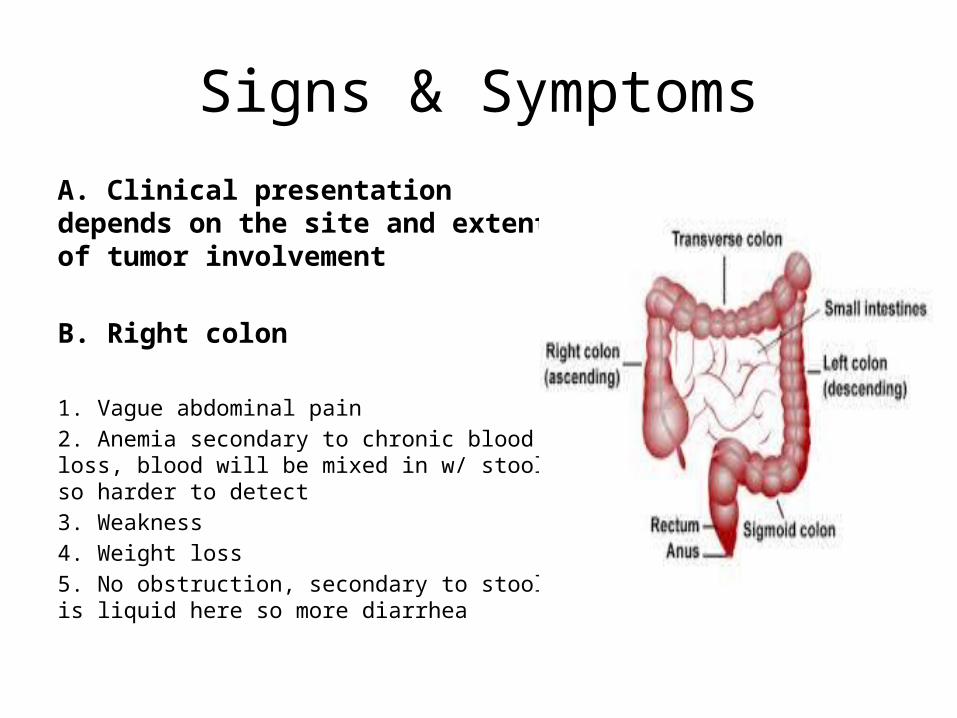
Signs & Symptoms
A. Clinical presentation depends on the site and extent of tumor involvement
B. Right colon
1. Vague abdominal pain2. Anemia secondary to chronic blood loss, blood will be mixed in w/ stool so harder to detect3. Weakness4. Weight loss5. No obstruction, secondary to stool is liquid here so more diarrhea
Signs & SymptomsC. Left colon
1. Constipation alternating with diarrhea secondary to obstruction2. Secondary to pressure against the obstruction that causes stool to liquefy3. Blood will be on the stool (coating)4. Abdominal pain5. Obstructive symptoms (nausea/vomiting)
D. Rectum
1. Changes in bowel movements2. Rectal fullness3. Urgency,4. Bleeding (bright red blood)
DiagnosisA. Medical and family history for:
1. Signs/symptoms2. Inflammatory bowel disease3. Colorectal cancer or polyps
B. Physical examination for:1. Lymphadenopathy2. Hepatomegaly3. Masses or ascites4. Women should undergo appropriate evaluations to rule out breast, ovarian, endometrial cancers
C. ColonoscopyD. Biopsy of any detected lesions
E. CT scan of chest/abdomen/pelvis
DiagnosisF. PET scan only if potential surgically curable metastatic disease
G. CBC with platelets, LFTs, creatinine
Diagnosis
H. Carcinoembryonic antigen (CEA) level1. May be useful in monitoring colorectal cancer response to treatment2. Normal < 33. Normal in smokers 0-64. CEA can be higher with ↑ SrCr, hepatic dysfunction or chemo (5-FU) so may see an increase in CEA and then a decrease after a few months of treatment
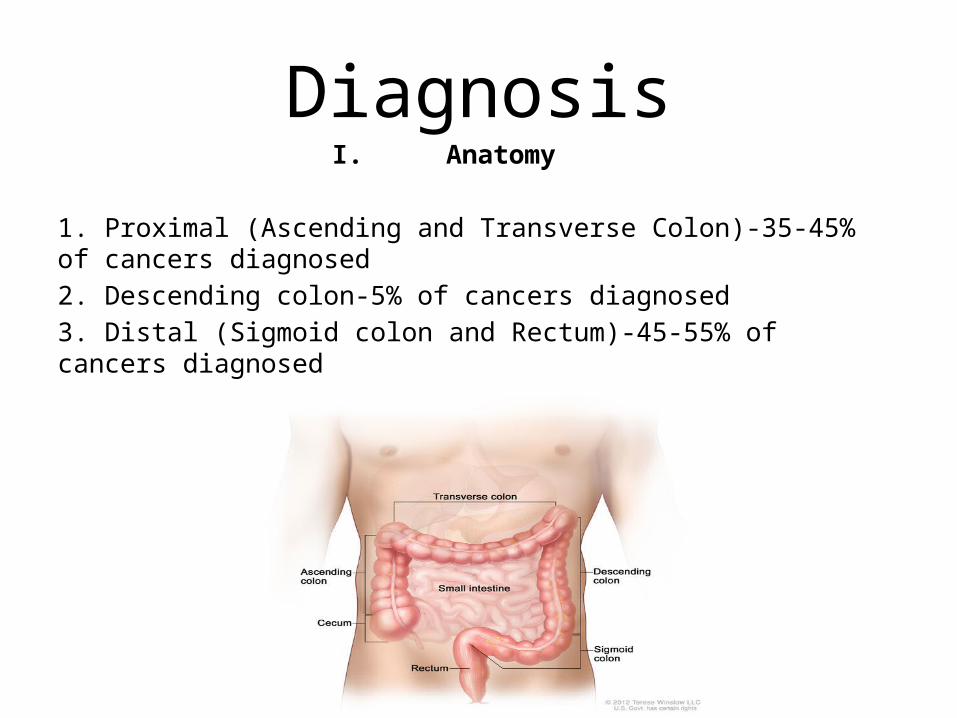
DiagnosisI. Anatomy
1. Proximal (Ascending and Transverse Colon)-35-45% of cancers diagnosed2. Descending colon-5% of cancers diagnosed3. Distal (Sigmoid colon and Rectum)-45-55% of cancers diagnosed
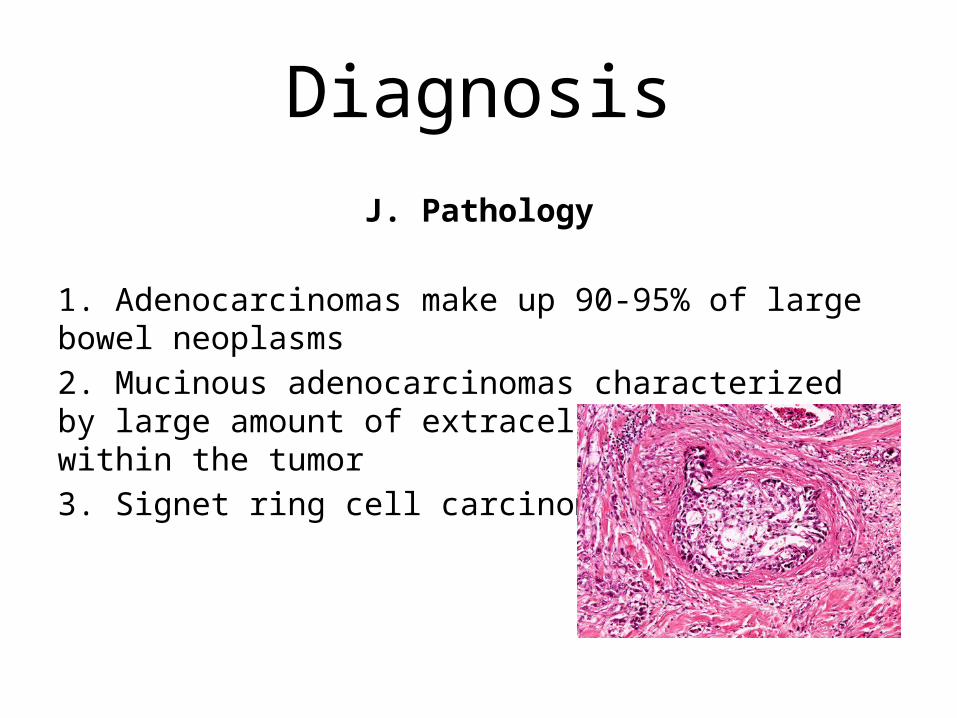
DiagnosisJ. Pathology
1. Adenocarcinomas make up 90-95% of large bowel neoplasms2. Mucinous adenocarcinomas characterized by large amount of extracellular mucus within the tumor3. Signet ring cell carcinoma
Diagnosis
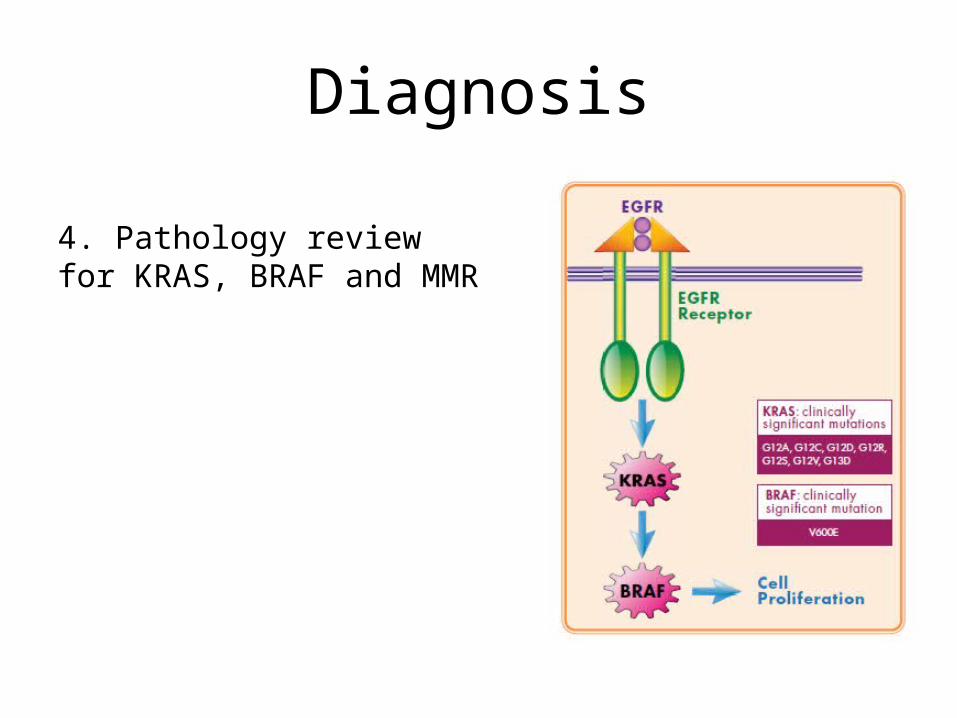
4. Pathology review for KRAS, BRAF and MMR
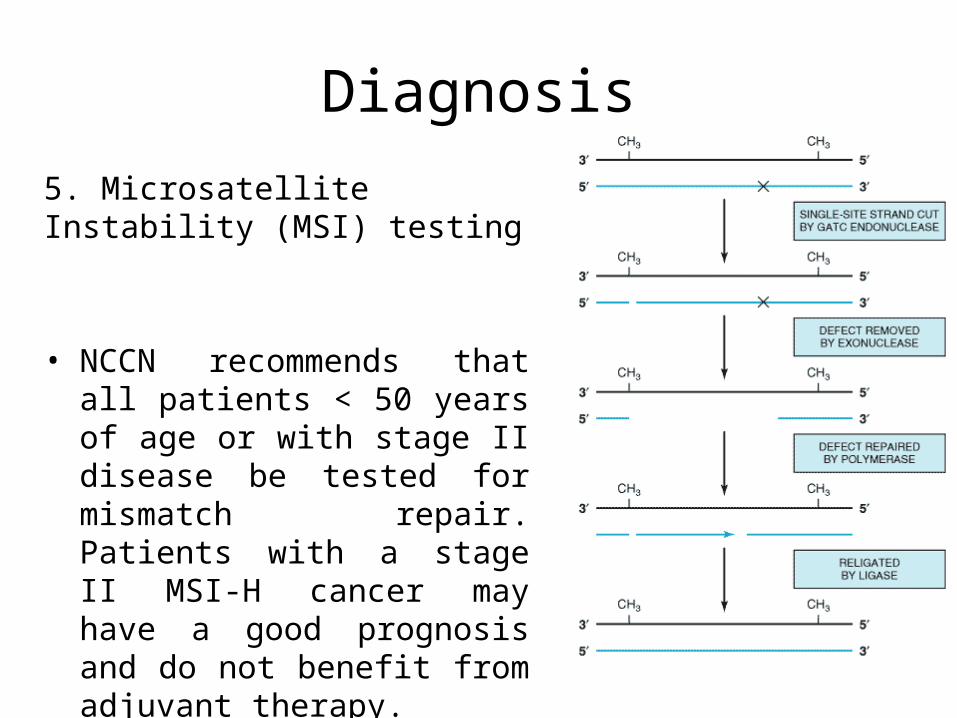
Diagnosis5. Microsatellite Instability (MSI) testing
• NCCN recommends that all patients < 50 years of age or with stage II disease be tested for mismatch repair. Patients with a stage II MSI-H cancer may have a good prognosis and do not benefit from adjuvant therapy.
Diagnosis
• MMR as well as other high risk features for recurrence are to be evaluated when determining whether adjuvant therapy is indicated for stage II colorectal cancers and do not benefit from 5-FU adjuvant therapy.
• Several studies have demonstrated that colorectal adenocarcinomas demonstrating microsatellite instability (MSI) exhibit loss expression of one or more of the mismatch repair (MMR) enzymes MLH1, MSH2, PMS2 and MSH6, which can be assessed by IHC.
Defective DNA mismatch repair (dMMR)1) Associated with colon cancers in the proximal (right side) colon, poor differentiation, mucinous histology, lymphocytic infiltration and diploid DNA contents2) Measured by microsatellite instability (MSI) or testing for loss of genes involved in DNA mismatch repair – MLH1, SMH2, MSH6, and PMS2• High-level MSI (MSI-H) and loss of protein expression of MLH1
and MSH2 have similar prognostic ability3) Stage II colorectal cancers with dMMR (MSI-H, loss of MLH1 or MSH2) do not benefit from 5-fluororuacil based adjuvant chemotherapy.4) MMR as well as other high risk features for recurrence are to be evaluated when determining whether adjuvant therapy is indicated for stage II colorectal cancers
Tests and procedures for diagnosis
• Physical exam and history : An exam of the body to check general signs of health.
• Digital rectal exam : The doctor or nurse inserts a lubricated, gloved finger into the rectum to feel for lumps or anything else that seems unusual.
• Fecal occult blood test: A test to check stool.• Barium enema : A series of x-rays of the lower gastrointestinal
tract. A liquid that contains barium is put into the rectum. The barium coats the lower gastrointestinal tract and x-rays are taken. This procedure is also called a lower GI series.
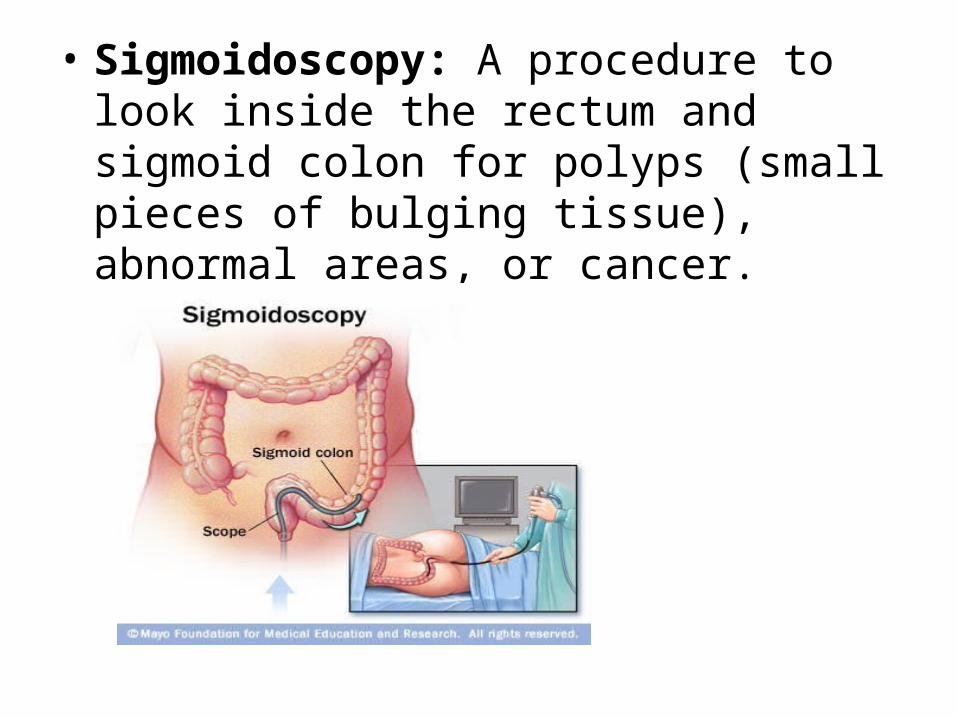
• Sigmoidoscopy: A procedure to look inside the rectum and sigmoid colon for polyps (small pieces of bulging tissue), abnormal areas, or cancer.
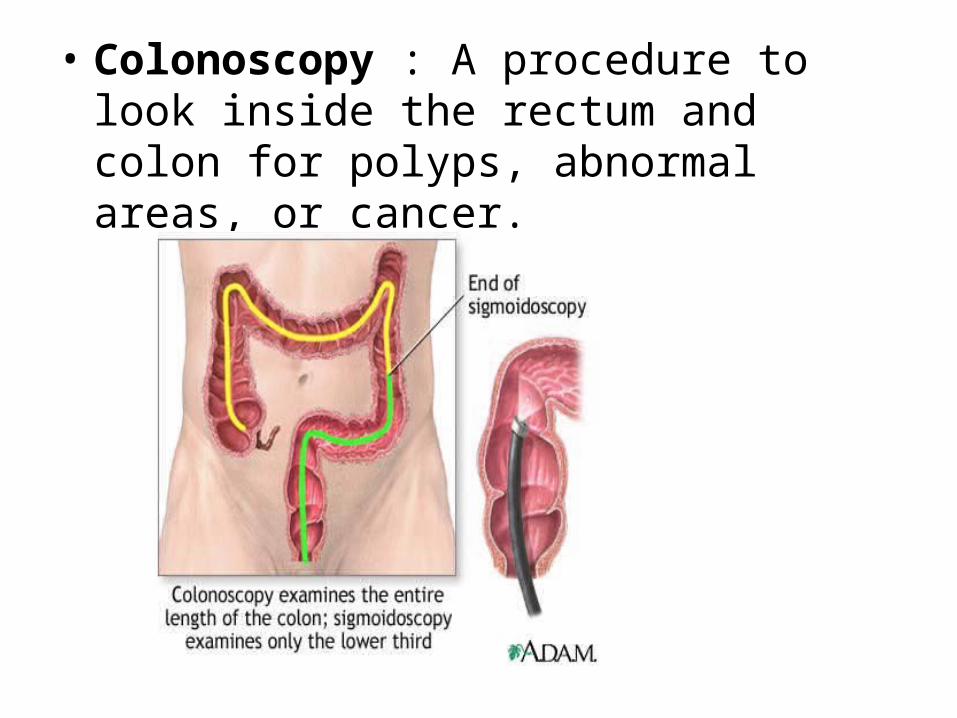
• Colonoscopy : A procedure to look inside the rectum and colon for polyps, abnormal areas, or cancer.
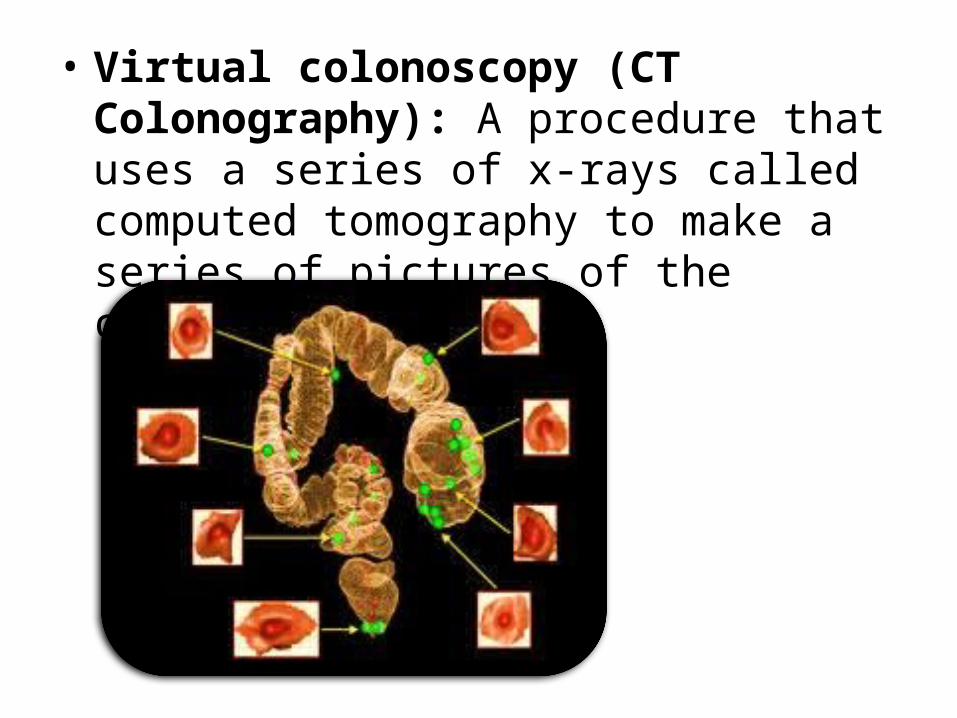
• Virtual colonoscopy (CT Colonography): A procedure that uses a series of x-rays called computed tomography to make a series of pictures of the colon.
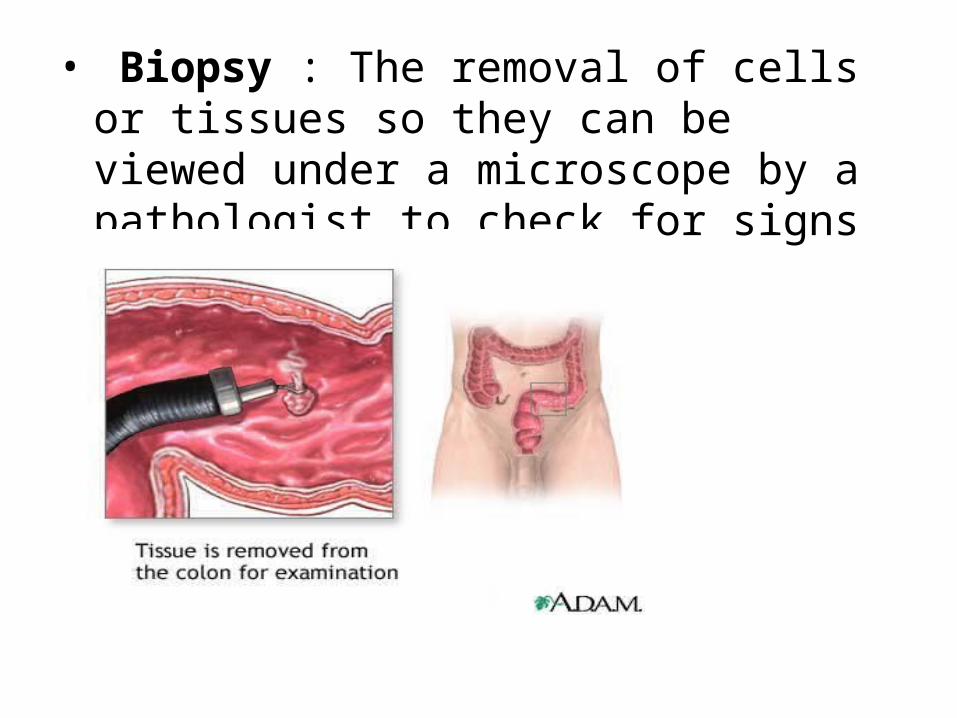
• Biopsy : The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer.
The prognosis• The stage of the cancer.• Whether the cancer has blocked or
created a hole in the colon.• Whether there are any cancer cells
left after surgery.• The blood levels of
carcinoembryonic antigen (CEA) before treatment begins.
• Whether the cancer has recurred.• The patient’s general health.
Treatment ‘depends on the following’
• The stage of the cancer.• Whether the cancer
has recurred.• The patient’s general
health.
Tests and procedures used in the staging process
• CT scan.• MRI (magnetic resonance imaging)• PET scan (positron emission tomography scan)• Chest x-ray• Lymph node biopsy• Complete blood count (CBC)• Carcinoembryonic antigen (CEA) assay

Treatment
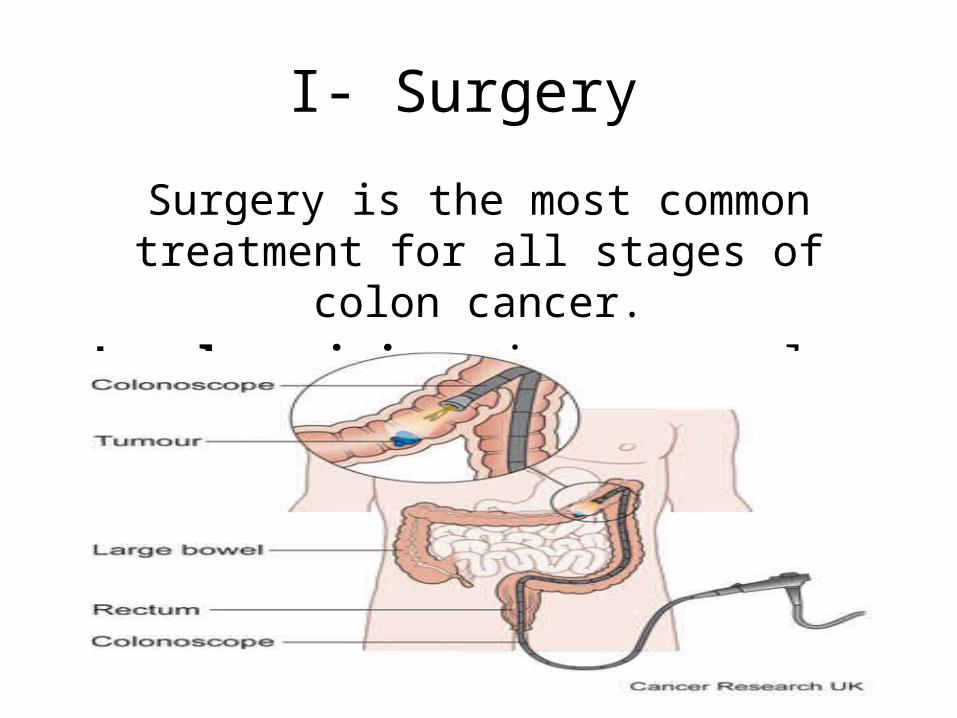
I- Surgery
Surgery is the most common treatment for all stages of colon cancer.
• Local excision: in very early stage.
I- Surgery
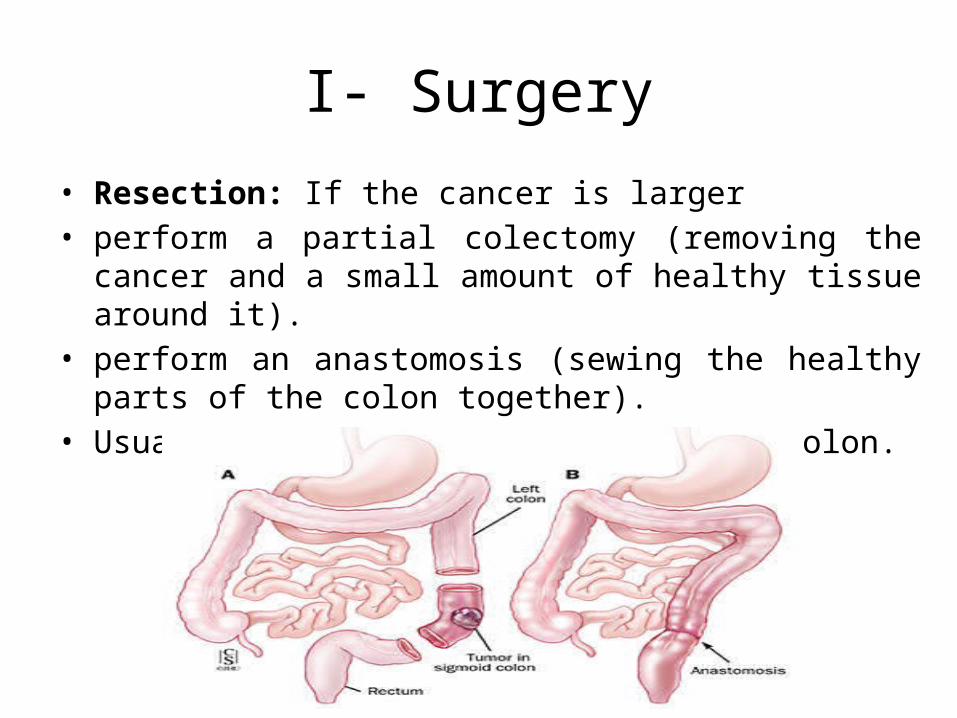
• Resection: If the cancer is larger• perform a partial colectomy (removing the cancer and a small
amount of healthy tissue around it).• perform an anastomosis (sewing the healthy parts of the colon
together). • Usually remove lymph nodes near the colon.
• Radiofrequency ablation: The use of a special probe with tiny electrodes that kill cancer cells.
• Cryosurgery (Cryotherapy): A treatment that uses an instrument to freeze and destroy abnormal tissue.
I- Surgery
II-Radiation therapyRadiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them
from growing.
II-Radiation therapy
a. Administered prior to or following surgery in patients with curable disease
1) Neoadjuvant - utilized to improve resectability of primary tumor (decrease risk for positive margins and increase opportunity for LAR resection) and to decrease risk of local recurrence.2) Adjuvant – used to decrease risk of local recurrencea) Radiation alone after surgery has been found to be inferior to concurrent radiation and chemotherapy in rectal cancer3) Utilized in patients with metastatic disease for symptom reduction (pain, bleeding) for both colon and rectal cancer
II-Radiation therapy
Complicationsa. Acute toxicity1) Thrombocytopenia/leukopenia2) Dysuria, diarrhea, abdominal cramping, proctitisb. Chronic toxicity1) Can be persist for months following discontinuation of XRT• Diarrhea• Small bowel disease• Proctitis• Enteritis
III- Chemotherapy
III- Chemotherapy
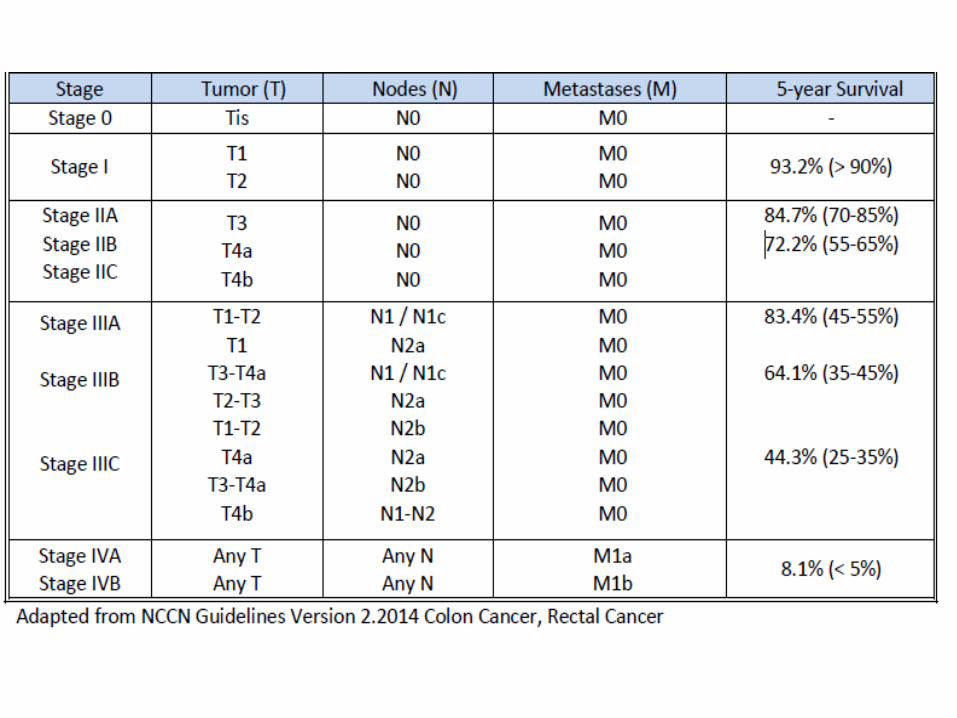
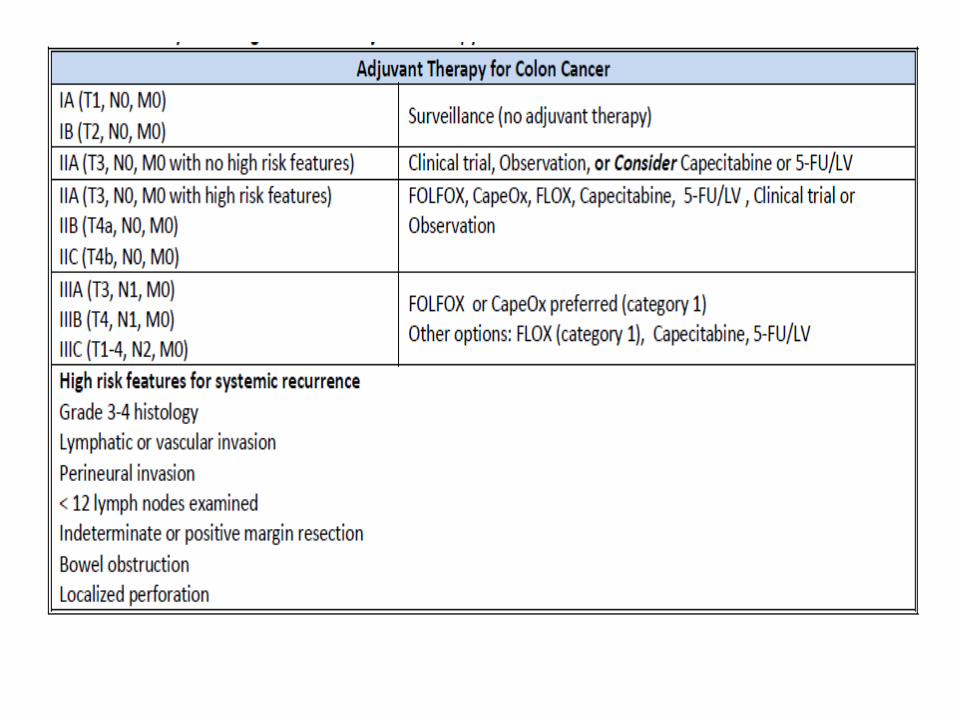
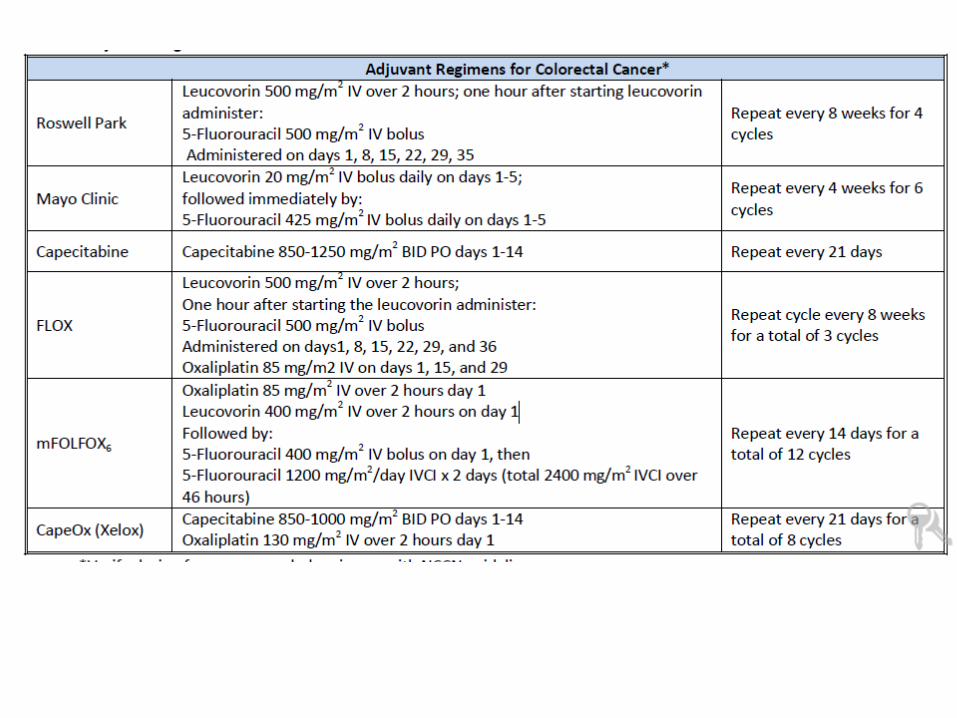
Treatment Regimens for adjuvant Colon Cancer
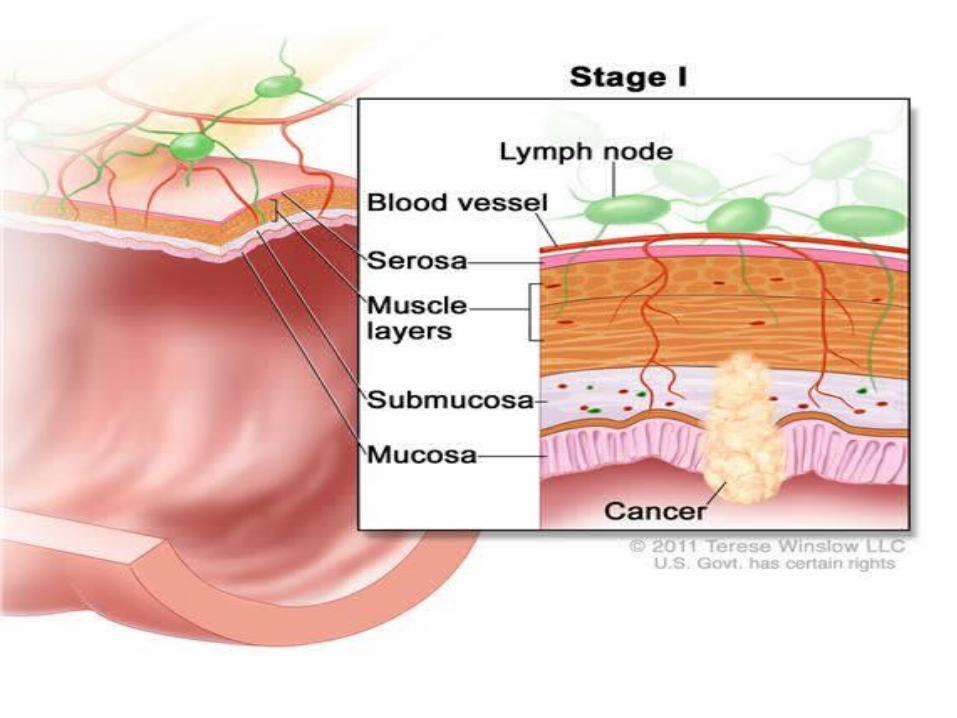
Stage I
• Surgical excision of primary tumor and removal of regional lymph nodes
• No adjuvant chemotherapy
High risk Stage II Disease
The NCCN guidelines include :
1- Grade 3, 4 histology.2- lymphovascular invasion.3- Perineural invasion.4- < 12 lymph nodes examined.5- Positive margins after surgical resection.6- Bowel obstruction, or localized perforation.
High risk Stage II Disease
• the number of lymph nodes:• If fewer than 12 lymph nodes are removed and examined, the
risk of recurrence is higher and the overall survival lower. In studies, the 5-year overall survival (OS) correlates to the number of lymph nodes removed (1-7 LNs = 49.8% OS, 8-12 LNs = 56.2%, >12 LNs = 63.4%).
• It is not clear if this is because examining more lymph nodes in these patients would have found their tumors to be stage III, or because the surgical removal was less than complete, or perhaps both. We don't know for sure, but this finding often drives the decision to use adjuvant chemotherapy in patients with fewer than 12 LNs removed.
High risk Stage II Disease
• Positive margin:
A positive margin has been defined as 1) Tumor <1 mm from the transected margin.2) Tumor <2 mm from the transected margin3) Tumor cells present within the diathermy of the transected
margin.
III- ChemotherapyTreatment Regimens for adjuvant Colon Cancer
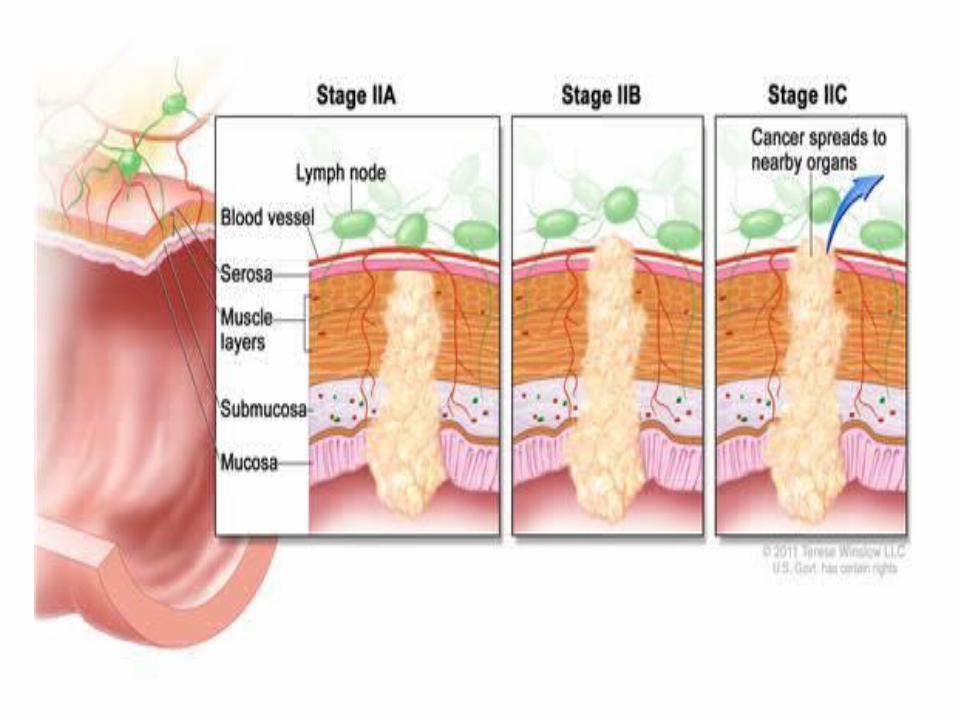
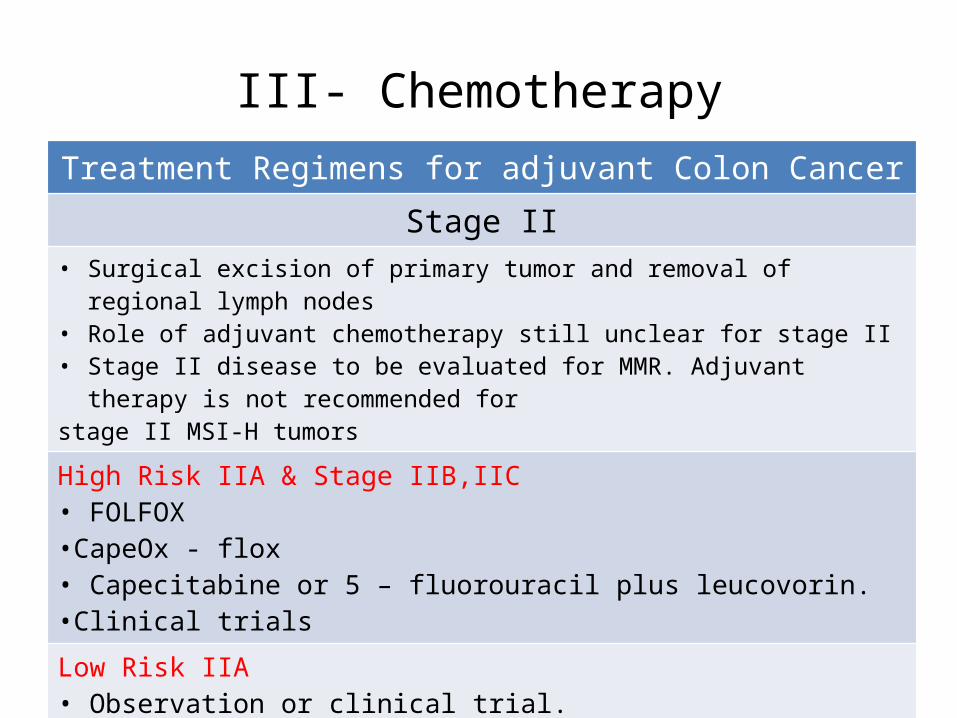
Stage II• Surgical excision of primary tumor and removal of regional lymph nodes• Role of adjuvant chemotherapy still unclear for stage II• Stage II disease to be evaluated for MMR. Adjuvant therapy is not recommended forstage II MSI-H tumorsHigh Risk IIA & Stage IIB,IIC• FOLFOX •CapeOx - flox• Capecitabine or 5 – fluorouracil plus leucovorin.•Clinical trials
Low Risk IIA• Observation or clinical trial.•Capecitabine, 5- fu/leuc.
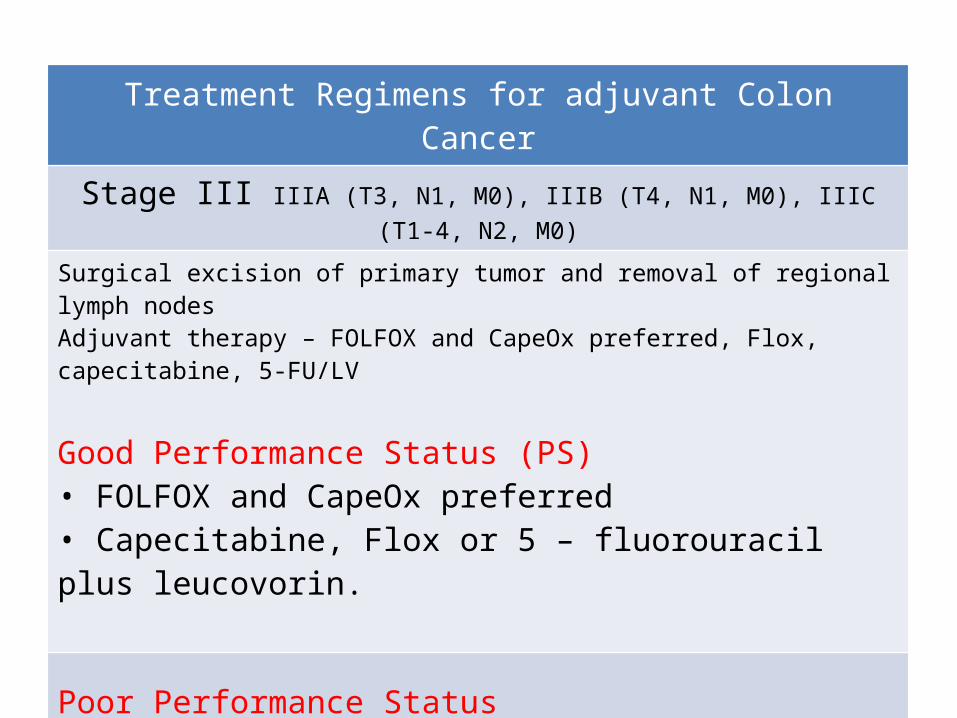
Treatment Regimens for adjuvant Colon Cancer
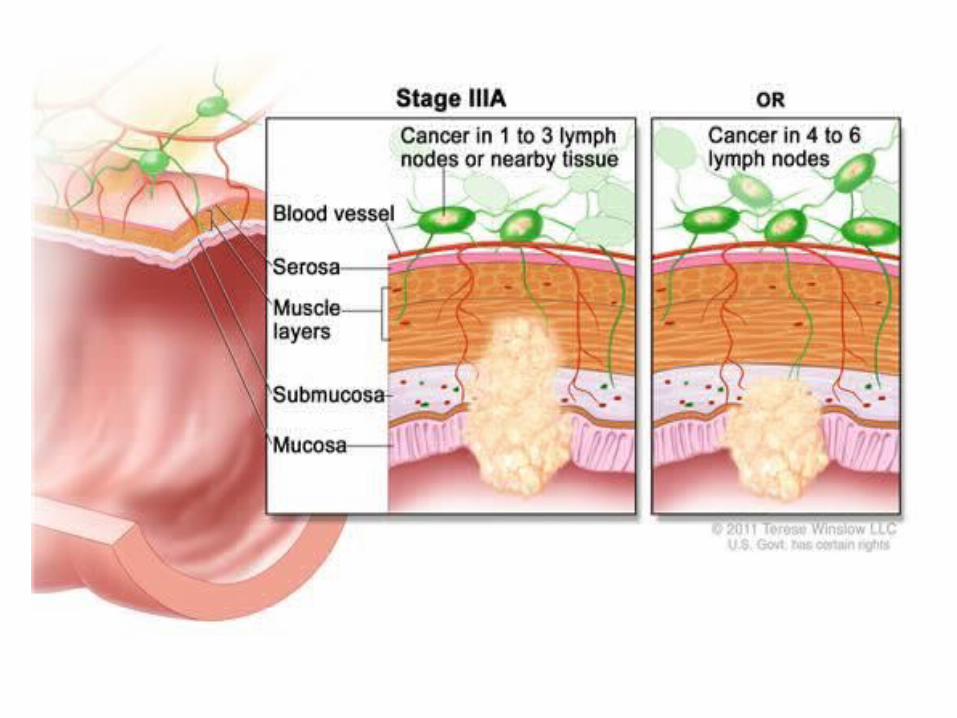
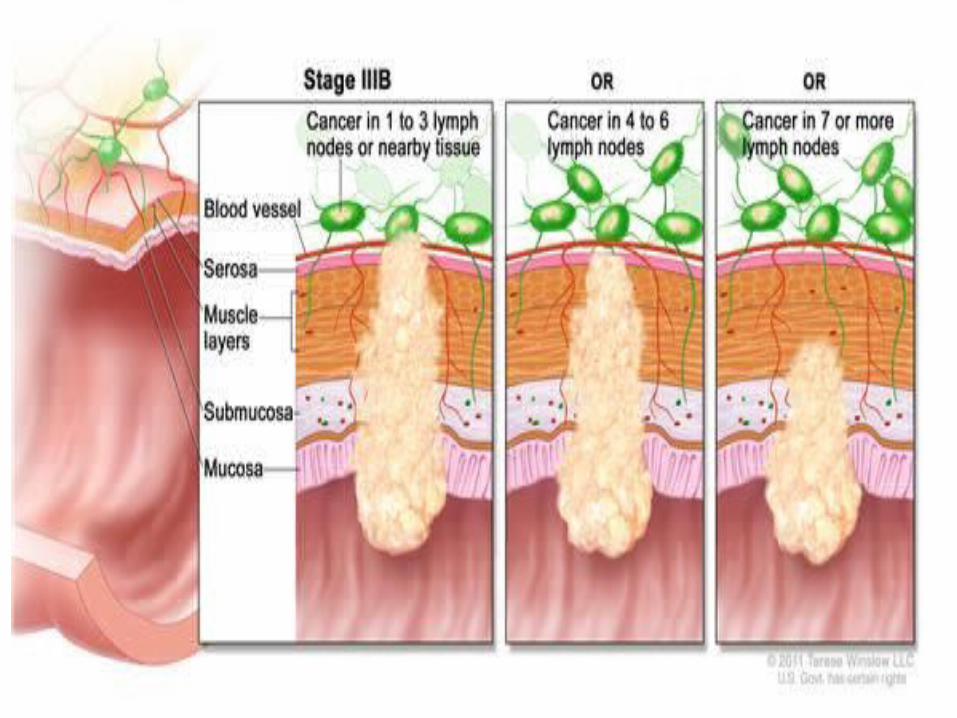
Stage III IIIA (T3, N1, M0), IIIB (T4, N1, M0), IIIC (T1-4, N2, M0)
Surgical excision of primary tumor and removal of regional lymph nodesAdjuvant therapy – FOLFOX and CapeOx preferred, Flox, capecitabine, 5-FU/LV
Good Performance Status (PS)• FOLFOX and CapeOx preferred• Capecitabine, Flox or 5 – fluorouracil plus leucovorin.
Poor Performance Status• Capecitabine.
PRINCIPLES OF ADJUVANT THERAPY5-FU-based regimens standard of care
1) Schedule of 5-FU/LV administration does not affect efficacy, but toxicities may be differenti. Mayo Clinic regimen - more commonly associated with leucopenia and stomatitisii. Roswell Park regimen - more commonly associated with diarrheaiii. Infusional 5-FU/LV may have less toxicity vs. bolusiv. Capecitabine equally effective to bolus 5-FU/LVv. Addition of oxaliplatin increased benefit (a) FOLFOX is superior to fluoropyrimidine therapy alone for stage III(b) FOLFOX is reasonable for high-risk stage IIvi. Irinotecan not used in the adjuvant settingvii. No targeted agents are approved for use in the adjuvant setting
PRINCIPLES OF ADJUVANT THERAPY
• Adjuvant therapy begins 4 to 8 weeks after surgery and lasts for 6 months
• FOLFOX is superior to 5-FU/leucovorin for patients with stage III colon cancer.
• Capecitabine/oxaliplatin is superior to bolus 5-FU/ leucovorin for patients with stage III colon cancer.
PRINCIPLES OF ADJUVANT THERAPY
• FLOX is an alternative to FOLFOX or CapeOx but FOLFOX or CapeOx are preferred.
• Capecitabine appears to be equivalent to bolus 5FU/leucovorin in patients with stage III colon cancer.
• A survival benefit has not been demonstrated for the addition of oxaliplatin to 5-FU/leucovorin in stage II colon cancer.
• FOLFOX is reasonable for high-risk stage II patients and is not indicated for good- or average-risk patients with stage II.
PRINCIPLES OF ADJUVANT THERAPY
• A benefit for the addition of oxaliplatin to 5-FU/leucovorin in patients age 70 and older has not been proven.
• Bevacizumab, cetuximab, panitumumab, or irinotecan should not be used in the adjuvant setting for patients with stage II or III colon cancer outside the setting of a clinical trial.
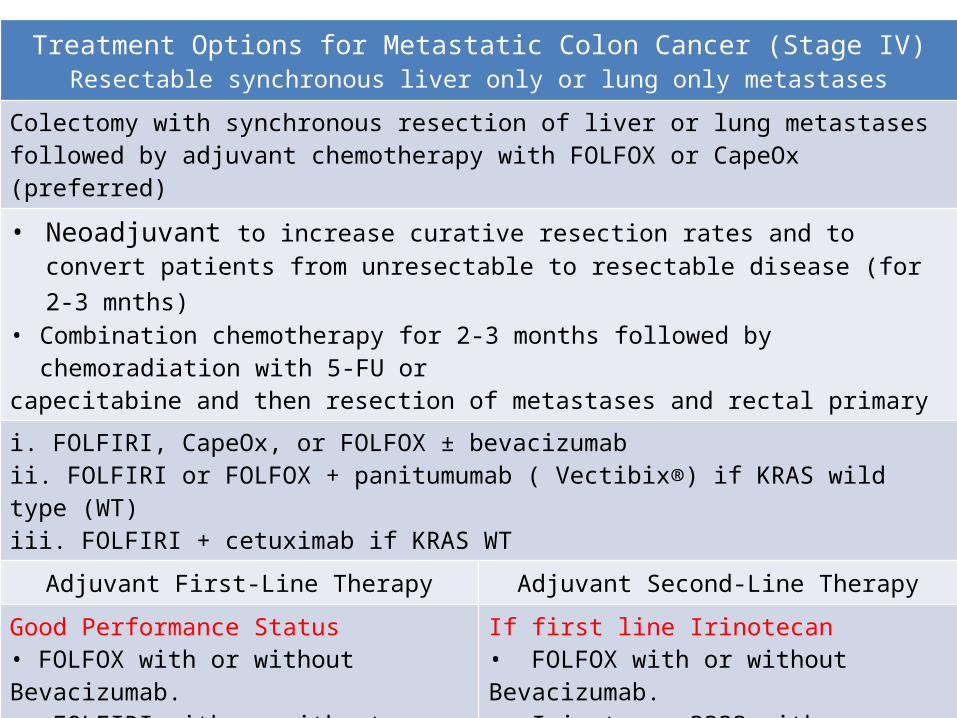
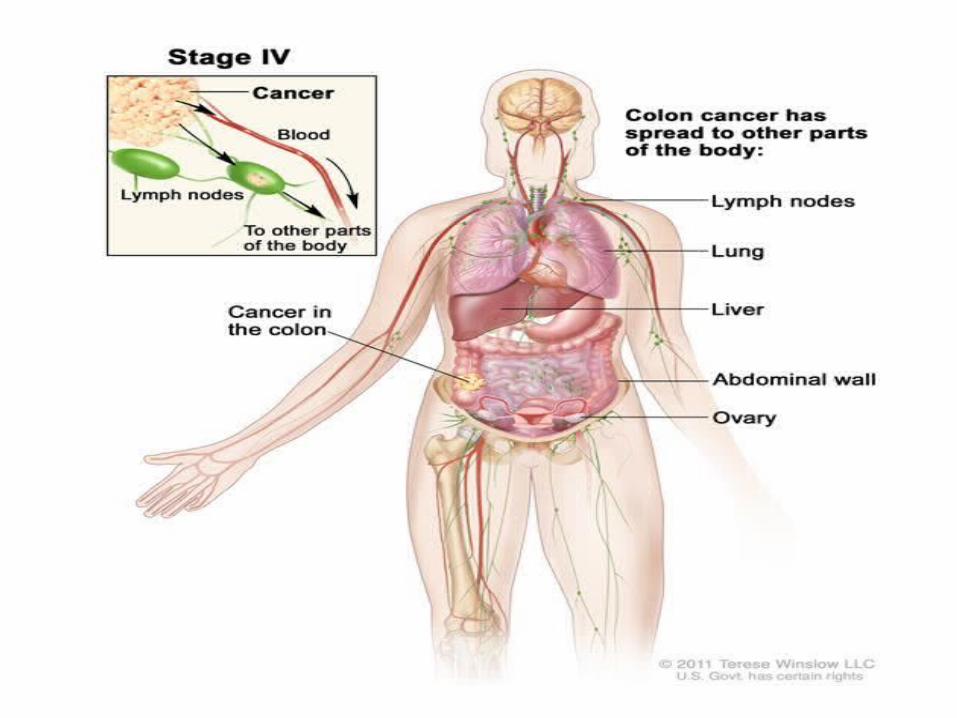
Treatment Options for Metastatic Colon Cancer (Stage IV)Resectable synchronous liver only or lung only metastases
Colectomy with synchronous resection of liver or lung metastases followed by adjuvant chemotherapy with FOLFOX or CapeOx (preferred)
• Neoadjuvant to increase curative resection rates and to convert patients from unresectable to resectable disease (for 2-3 mnths)
• Combination chemotherapy for 2-3 months followed by chemoradiation with 5-FU orcapecitabine and then resection of metastases and rectal primary
i. FOLFIRI, CapeOx, or FOLFOX ± bevacizumabii. FOLFIRI or FOLFOX + panitumumab ( Vectibix®) if KRAS wild type (WT)iii. FOLFIRI + cetuximab if KRAS WT
Adjuvant First-Line Therapy Adjuvant Second-Line Therapy
Good Performance Status• FOLFOX with or without Bevacizumab.• FOLFIRI with or without Bevacizumab.• 5-FU + Leucovrin with bevacizumab
If first line Irinotecan• FOLFOX with or without Bevacizumab.• Irinotecan ???? with or without Cetuximab.• Capecitabine or 5-FU + Leucovorin
Poor Performance Status• Capecitabine or 5-FU + Leucovorin with or without Bevacizumab.
If first line Oxaliplatin• FOLFIRI with or without Bevacizumab.• Irinotecan with or without Cetuximab.
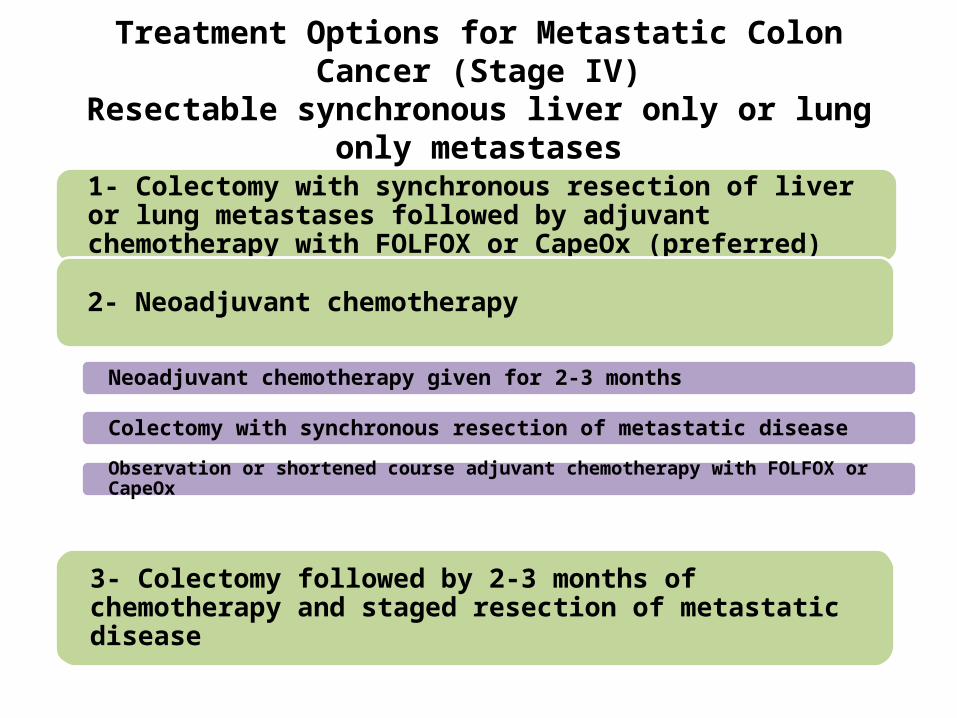
Treatment Options for Metastatic Colon Cancer (Stage IV)Resectable synchronous liver only or lung only metastases
1- Colectomy with synchronous resection of liver or lung metastases followed by adjuvant chemotherapy with FOLFOX or CapeOx (preferred)
2- Neoadjuvant chemotherapy
Neoadjuvant chemotherapy given for 2-3 months
Colectomy with synchronous resection of metastatic disease
Observation or shortened course adjuvant chemotherapy with FOLFOX or CapeOx
3- Colectomy followed by 2-3 months of chemotherapy and staged resection of metastatic disease
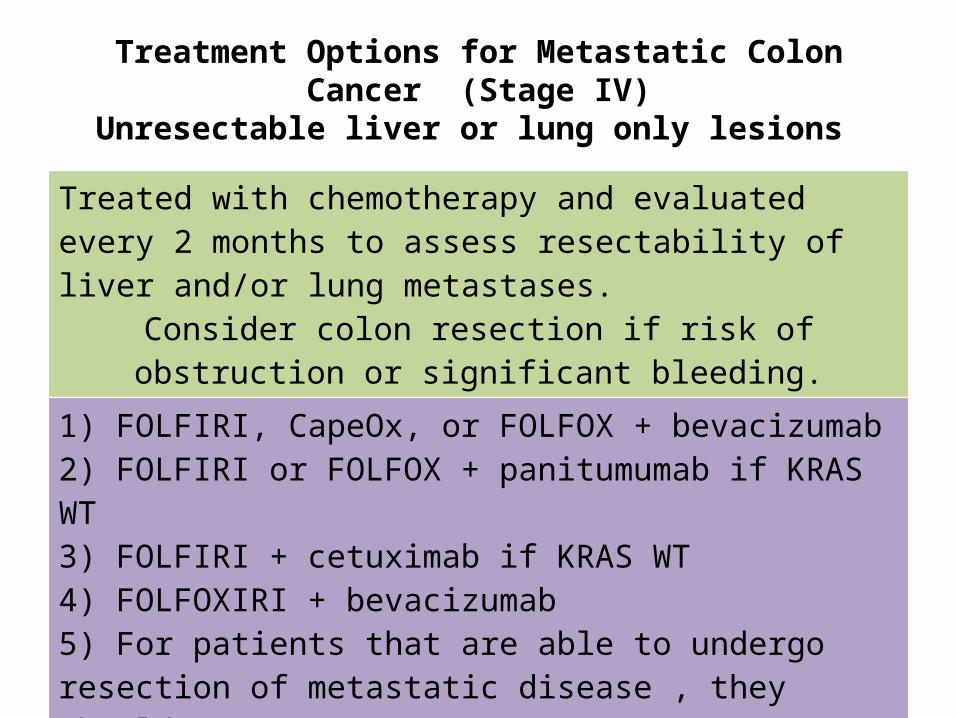
Treatment Options for Metastatic Colon Cancer (Stage IV)Unresectable liver or lung only lesions
Treated with chemotherapy and evaluated every 2 months to assess resectability of liver and/or lung metastases.
Consider colon resection if risk of obstruction or significant bleeding.
1) FOLFIRI, CapeOx, or FOLFOX + bevacizumab2) FOLFIRI or FOLFOX + panitumumab if KRAS WT3) FOLFIRI + cetuximab if KRAS WT4) FOLFOXIRI + bevacizumab5) For patients that are able to undergo resection of metastatic disease , they shouldreceive 6 months of adjuvant therapy with an active regimen for advanced disease,observation, or shortened course of chemotherapy
Based on the information presented, create a care plan for this patient’s colon cancer; includes:
a)The patient’s drug and non drug-related needs and problemsb)The goals of therapyc)A treatment plan specific to the patient that includes strategies to
prevent adverse effects of chemotherapyd)A follow-up plan to determine whether the goals have been
achieved and the adverse effects of chemotherapy have been minimized.
e)A plan for treatment options when the initial therapy is no longer achieving the goals of therapy.
Creating a care plan

Scenarios
Scenario 1
• MM 55 years old patient admitted to the hospital complaining of non- stop diarrhea after investigations patient diagnosed as Cancer colon with no signs of metastatic disease.
• Q 1, it is appropriate for him to undergo surgical resection for his colon cancer??
YesNo
Scenario 1
• MM 55 years old patient admitted to the hospital complaining of non- stop diarrhea after investigations patient diagnosed as Cancer colon with no signs of metastatic disease.
• Q 1, it is appropriate for him to undergo surgical resection for his colon cancer??
YesNo
Scenario 1
• After surgery .. The surgical wound has completely healed. He presents to the medical oncologist’s office for a discussion about whether or not he should receive adjuvant chemotherapy. The pathology for the primary tumor was determined to be a Stage IIIA (T2 N1 M0). His performance status is a 1.
• Q 2, Should he receive adjuvant Chemotherapy ?? Yes No
Scenario 1
• After surgery .. The surgical wound has completely healed. He presents to the medical oncologist’s office for a discussion about whether or not he should receive adjuvant chemotherapy. The pathology for the primary tumor was determined to be a Stage IIIA (T2 N1 M0). His performance status is a 1.
• Q 2, Should he receive adjuvant Chemotherapy ?? Yes No
Scenario 1
• Q 3, What adjuvant therapy do you recommend LD receive?
FOLFOXFOLFIRIFOLFOX + bevacizumabFOLFIRI + bevacizumab
Scenario 1
• Q 3, What adjuvant therapy do you recommend LD receive?
FOLFOXFOLFIRIFOLFOX + bevacizumabFOLFIRI + bevacizumab
Answer Explanation • Given that MM has stage III disease, the recommendation is for MM to
receive adjuvant chemotherapy for 6 months with either FOLFOX or CapeOx(preferred regimens). Other options include FLOX, capecitabine, or 5-FU/LV.
• Observation and clinical trials are not recommended for stage III disease.
Scenario 1
• Q 4, Would your recommendation change if the pathology revealed a stage IIA (T3 N0 M0)? What additional information is needed to make this decision?
THANK YOUCancer











