Embed Size (px)
Citation preview
Meet the SANRU Myth-Busting Team
Frank the Fact-Finder
Miat the Myth deMystifier
Leon the Legendary Liaison
Felix the First-class Freethinker
Albert the Always-Astute Analyst
Myth Measuring Methodology We will identify statements or claims that have been made about faith-based related work in DR Congo in general, and SANRU in particular.
A myth-buster will propose how to test the myth through the factual data collection and analysis.
The panelist will present the research results, and conclude whether the myth is confirmed, busted, or plausible.
Myth Testing Results
The myth statement is shown to be false (the myth is busted) The myth statement is shown to be true (the myth is confirmed) The myth statement is shown to be possibly or probably true, but could not be fully confirmed at this time (the myth is plausible).
A Short History of SANRU In 1981, USAID funded the Basic Rural Health Project to develop 50 decentralized health zones. The project became known as SANRU (Santé Rurale).
USAID and the MOH selected the Protestant Church of Congo (ECC) Medical Office to manage SANRU.
SANRU I/II (1981-91) helped create 100 health zones with Mr. Nlaba, Dr. Miatudila & Dr. Baer providing leadership.
In 2000, IMA World Health and ECC proposed the SANRU III project with USAID funding to begin rebuilding health zones.
From 2000-2010, IMA and ECC successfully managed several large projects for the MOH and donors (USAID and World Bank).
In 2011 SANRU was registered as a National NGO.
SANRU currently serves as Principal Recipient for Global Fund Malaria & HIV projects, and for GAVI CSO.
Myth Statement #1: DR Congo has the largest faith-based health network in Africa.
Working Definitions
• Faith-Based Health Networks: Loose, informal networks of all faiths, including all organizations that provide healthcare services and support.
• Christian Health Associations: Formal networks of Christian groups for coordination and advocacy, e.g. CCIH and Christian Health Association of Malawi, Zambia, etc.
• FBO: Faith-Based Organizations, e.g. Salvation Army, CRS and World Vision.
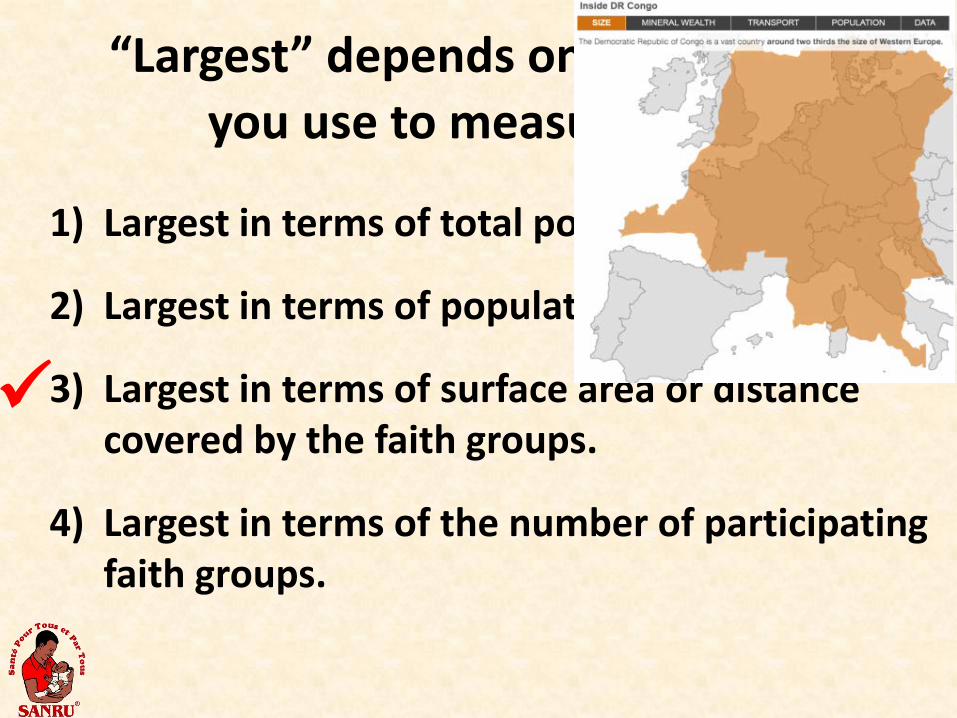
“Largest” depends on what terms you use to measure size.
1) Largest in terms of total population involved.
2) Largest in terms of population density.
3) Largest in terms of surface area or distance covered by the faith groups.
4) Largest in terms of the number of participating faith groups.
1
2
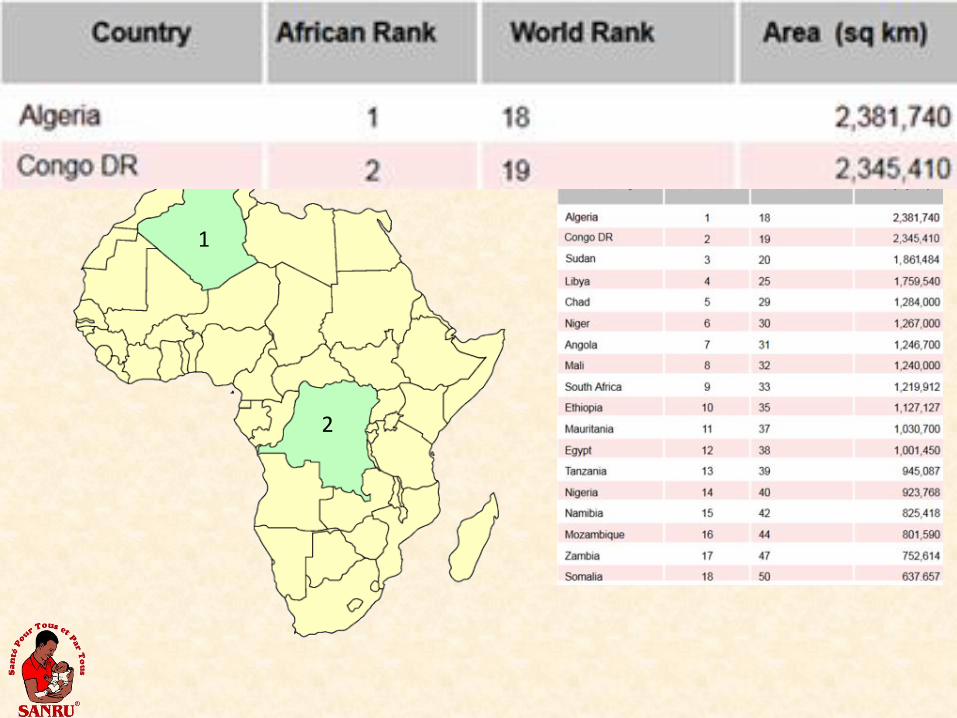
The Two Largest Countries in Africa (in terms of size)
Health for All and By All
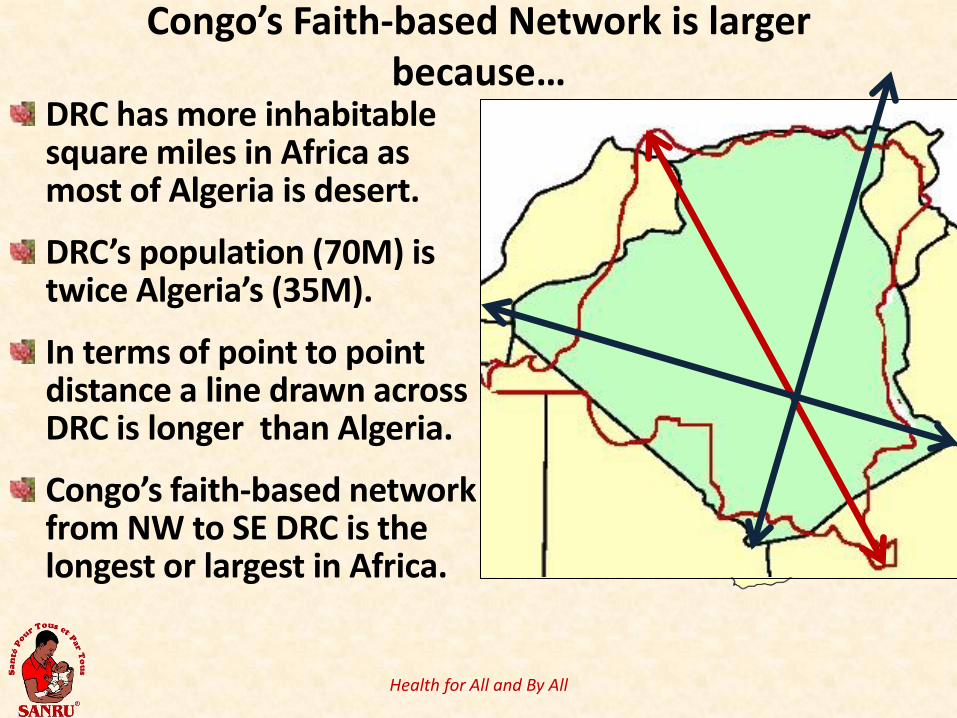
Congo’s Faith-based Network is larger because…
DRC has more inhabitable square miles in Africa as most of Algeria is desert.
DRC’s population (70M) is twice Algeria’s (35M).
In terms of point to point distance a line drawn across DRC is longer than Algeria.
Congo’s faith-based network from NW to SE DRC is the longest or largest in Africa.
Myth #1: DR Congo has the largest faith-based health network in Africa
Conclusion: From the perspective of measuring “large” in terms of distances DRC’s faith-based network is the largest in Africa.
BTW, in terms of population size, Nigeria, with a population of 180,000,000 would be the largest faith-based network in Africa.
Myth Statement #2: 40% of health care in DR Congo is provided through faith-based
managed health facilities.
Playing broken telephone: assessing faith-inspired health care provision in Africa
by Jill Olivier & Quentin Wodon
• It is commonly stated that faith-inspired institutions (FIIs) provide from 30 to 70 per cent of all health care provision in Africa.
• This article tracks the sources of such statements, highlighting a process of ‘broken telephone’ whereby estimates are passed on and frequently distorted…
• Our testing of this myth is not intended to debunk the conclusions of this article, but rather to examine this issue within the context of DR Congo.
Measuring Health Care Coverage Approach 1 for General Reference Hospitals (HGR): Each HGR provides secondary care to the catchment population for a Health Zone. A HZ is similar to what WHO calls a “health district.” Approach 2 for Health Centers (HC): Each HC provides primary care to the population for a designated catchment area. Our approach will try to calculate population served by each of these approaches.
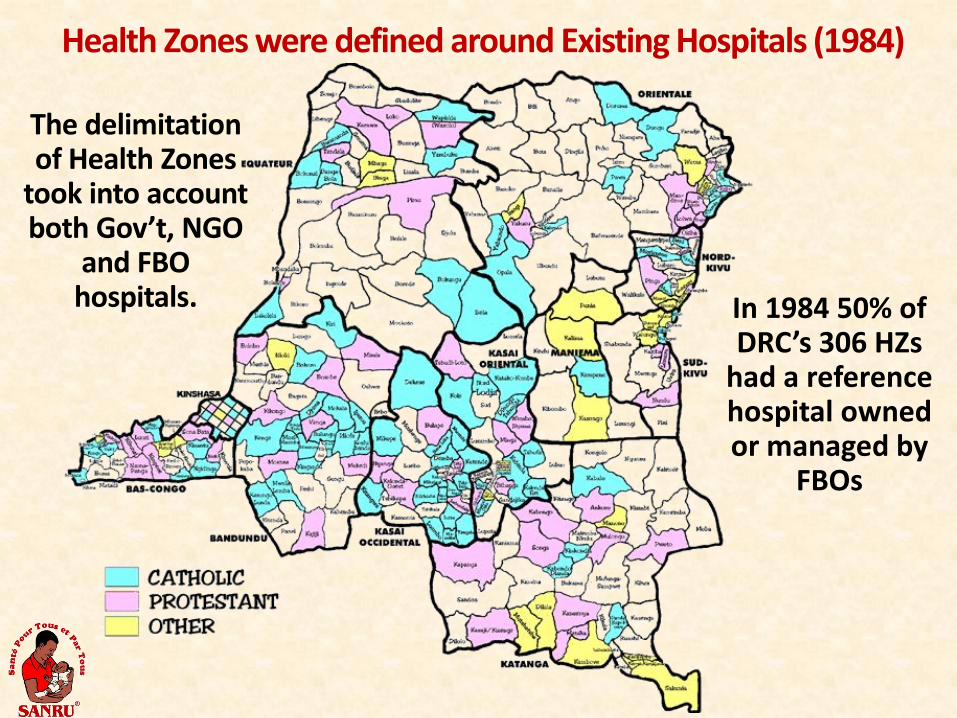
Health Zones were defined around Existing Hospitals (1984)
In 1984 50% of DRC’s 306 HZs
had a reference hospital owned or managed by
FBOs
The delimitation of Health Zones
took into account both Gov’t, NGO
and FBO hospitals.
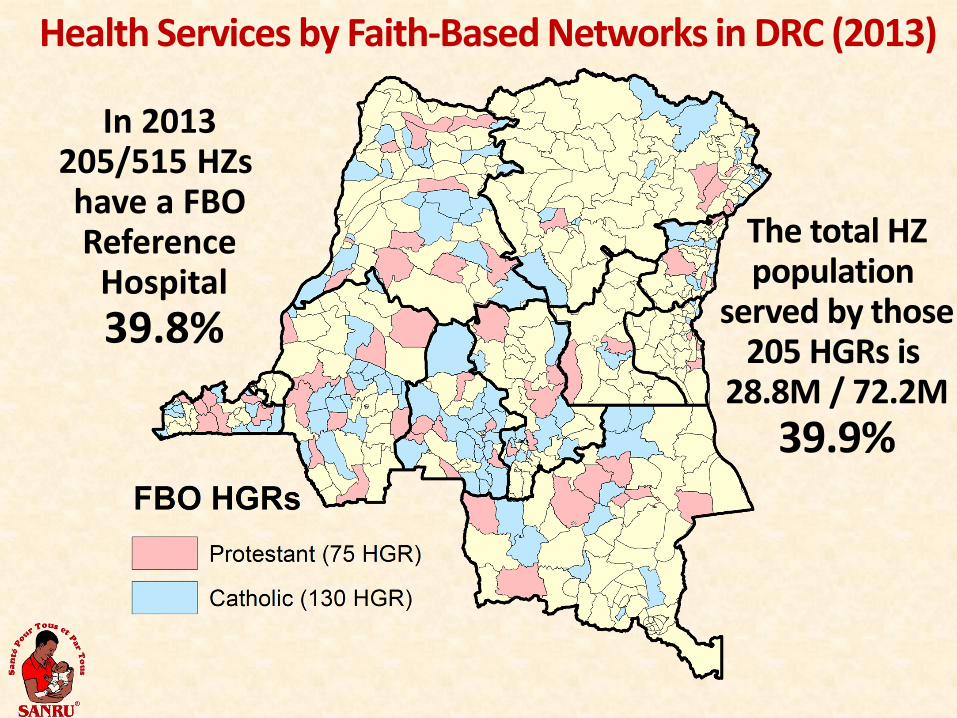
Health Services by Faith-Based Networks in DRC (2013)
In 2013 205/515 HZs have a FBO Reference
Hospital 39.8%
The total HZ population
served by those 205 HGRs is
28.8M / 72.2M 39.9%
Health Care from Faith-based Health Centers The MOH of Congo estimates that there are
approximately 8,240 health centers with catchment areas (16 CS x 515 Health Zones + 1 HGR per HZ).
Ownership of health facilities is unfortunately not tracked by the MOH. However from other sources we know that: Caritas reports ~1,900 Catholic-owned facilities ECC-DOM reports ~800 Protestant-owned facilities Kimbanguists, Muslim, Salvation Army and others groups
probably comprise 200-400 additional facilities
Health Care from Faith-based Health Centers Total faith-based owned facilities which serve as publically
accessible health centers is around 3,000 - Catholic – 1,900 - Protestant – 800 - Other – 300 - Total = ~ 3,000
The percentage of health services provided to the population catchment areas associated with those facilities is 3,000/8240 =36.4%
These numbers are, we feel, conservative since they do not include the work of other faith-based health structures which are not officially functioning as PHC health centers.
Myth #2: 40% of health care in DRC is provided through faith-based managed health facilities.
Faith-Based Reference Hospitals provide secondary care for 40% (or more) of the population.
Faith-Based Health Centers provide primary care for at least 36% of the population (more research is needed to firm up the numbers)
Myth 3: SANRU only provides assistance to Protestant-owned health facilities.
Alma Ata – 1978 Principles of Primary Health Care
21
1) Adoption of an Integrated Medicine
approach (aka Primary Health Care) 2) Proposal to create decentralized
health zones 3) Partnership between the MOH and
Churches for the development and management of the health system
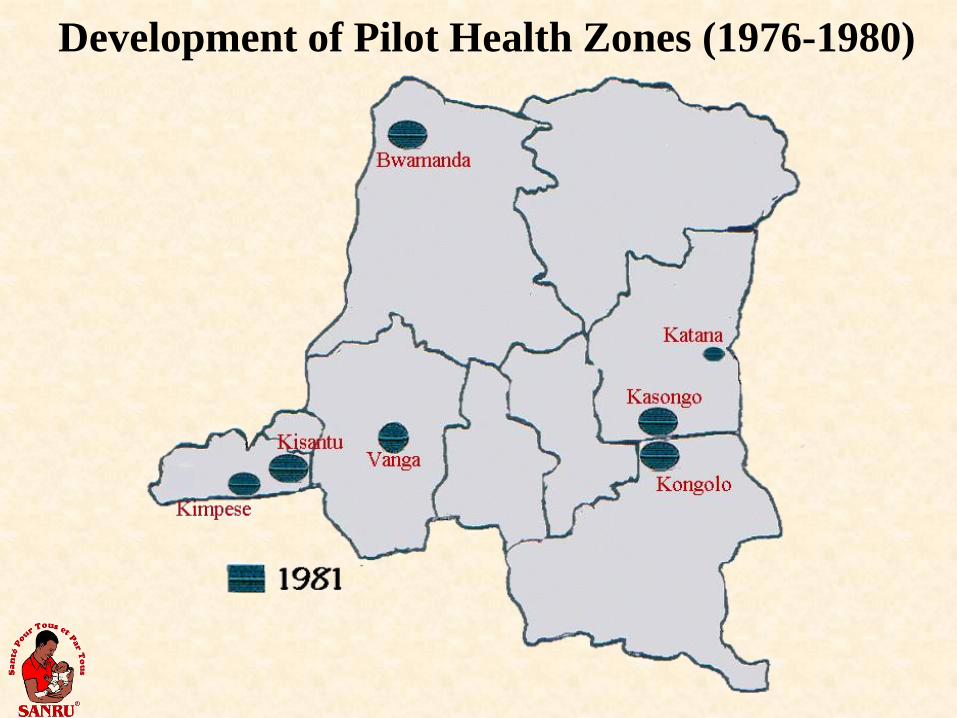
Development of Pilot Health Zones (1976-1980)
Design of the Basic Rural Health Project
SANRU began as a bilateral project (USAID to MOH) with management delegated to the Protestant Church.
This was an unusual arrangement for project implementation, but one that worked extremely well.
Originally the project mandate was to create 50 decentralized health zones around 50 Protestant hospitals.
However, during project startup the vision and mandate of SANRU was expanded to work with all functional hospitals to create HZs.
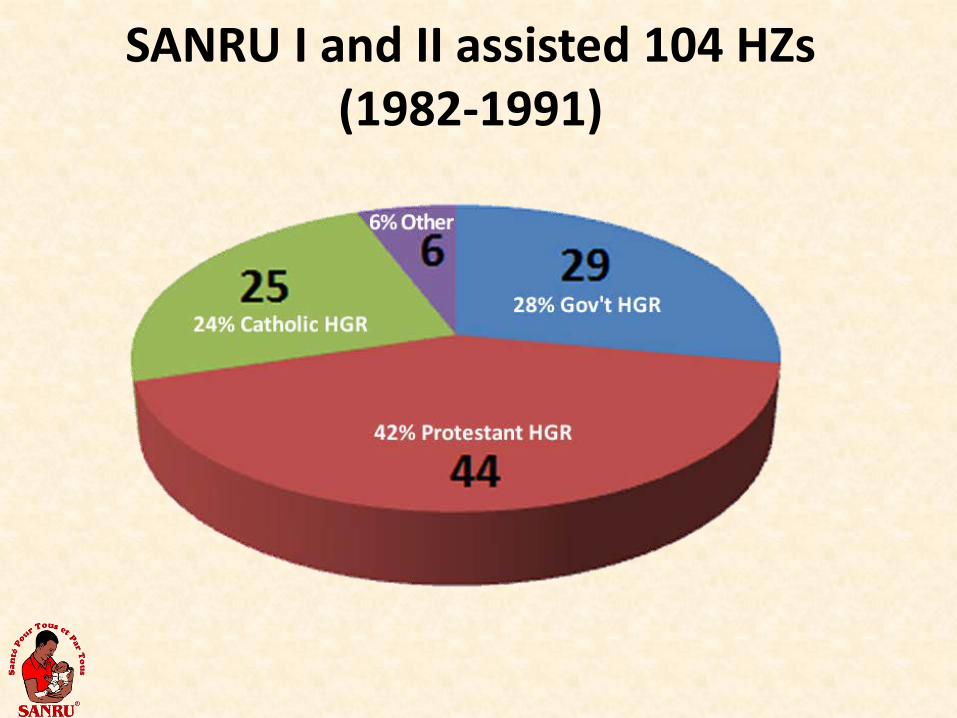
SANRU I and II assisted 104 HZs (1982-1991)
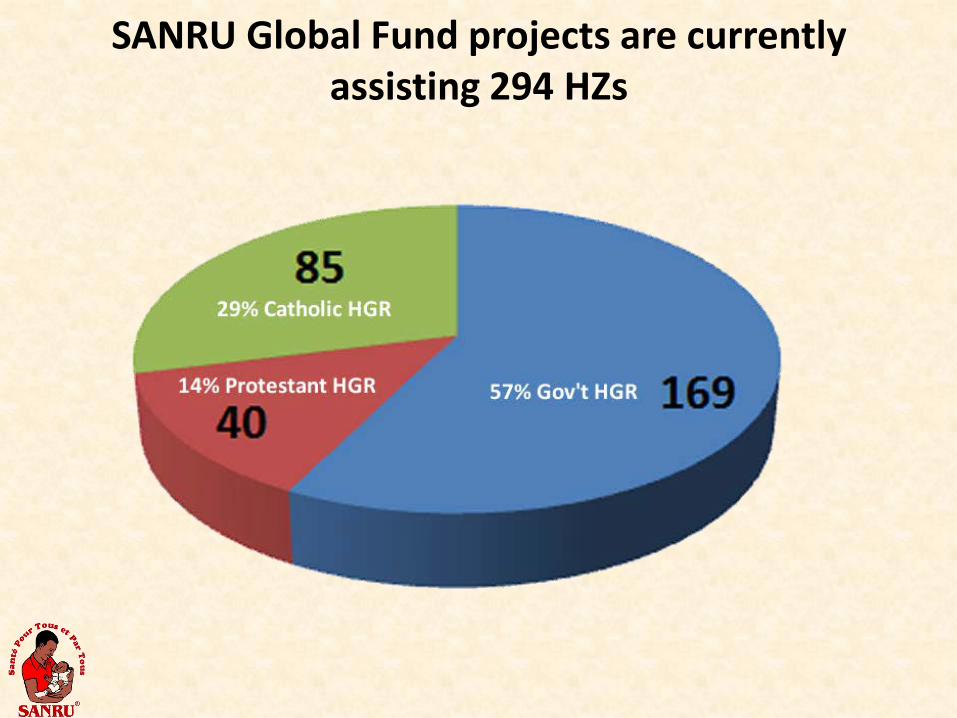
SANRU Global Fund projects are currently assisting 294 HZs
Myth #3: SANRU only provides assistance to Protestant-owned health facilities
SANRU currently provides Global Fund assistance to 294 health zones for malaria and HIV. Only 14% of HZs have Protestant-owned or managed HGRs
Myth Statement #4: In terms of funding, SANRU is the largest Principal Recipient
for Global Fund in Africa.
SANRU’s History of Project Management
• 1981-1991: SANRU I and II
• 2000-2006: SANRU III
• 2006-2010: Project AXxes (USAID)
• 2003-2010: Project PMURR (World Bank)
• 2003-2009: Sub-recipient to UNDP for Global Fund
• 2010-1013: Principal Recipient for Global Fund for Malaria and HIV/AIDS
SANRU and the MOH • SANRU is the most important and largest
partner with the MOH.
• SANRU does not, however, replace the MOH by substitution. SANRU is not a para-MOH.
• SANRU’s role is primarily project implementation, getting resources to HZs.
• This compliments the MOH’s role to develop and coordinate policy, donors and technical protocols.
Myth Statement #4: In terms of funding, SANRU is the largest Principal Recipient
for Global Fund in Africa.
Ways to Measure Global Fund Funding
1) Approved Grant Amounts: These can be very high, yet never disbursed.
2) Amount Disbursed: Actual amount of funding disbursed over time.
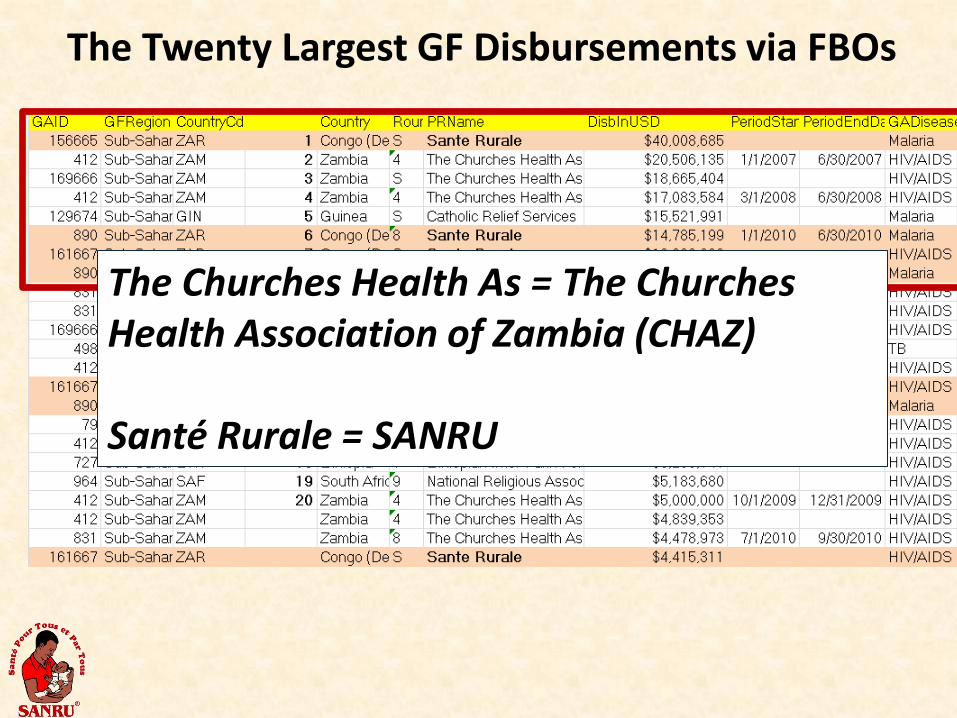
The Twenty Largest GF Disbursements via FBOs
The Churches Health As = The Churches Health Association of Zambia (CHAZ) Santé Rurale = SANRU
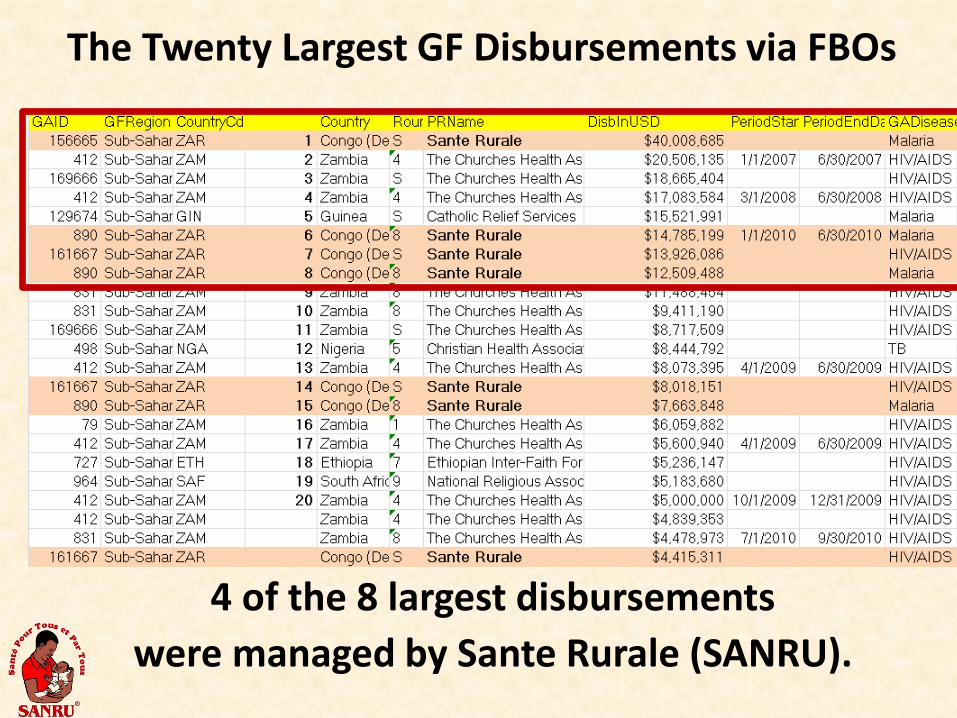
The Twenty Largest GF Disbursements via FBOs
4 of the 8 largest disbursements were managed by Sante Rurale (SANRU).
CHAZ vs SANRU In terms of total funds disbursed CHAZ (Zambia) has received 67 disbursements since 2005 for a total of $187 million, i.e., $24 M/year.
SANRU has received 14 disbursements since 2010 for $114,000 million, i.e., $38 M/year.
The largest current FBO-managed grant is the one held by SANRU Malaria ($40 Million).

Myth #4: SANRU is the largest Faith-Based Principal Recipient for Global Fund in Africa.
SANRU currently manages the largest single disbursement for a GF project (for malaria) and the largest combined total per year of funds disbursed.
Faith-Based Myths in DR Congo Myth Statement #1: DR Congo has the largest faith-based health network in Africa. Myth Statement #2: 40% of health care in DR Congo is provided through faith-based managed health facilities. Myth #3: SANRU only provides assistance to Protestant-owned health facilities Myth #4: SANRU is the largest Faith-Based Principal Recipient for Global Fund in Africa.