Embed Size (px)
Citation preview

Cell Injury – Cell Injury and Cell Death

Most forms of disease state begin with cell injury and consequently loss of cellular function.
Cell injury is defined as- a variety of stresses a cell encounters as a result of changes in its internal and external environment.
The cellular response to injury varies and depends upon Type of cell and tissue invovled Extent of injury Type of injury

Cell ProliferationCells are classified according to their proliferative potentialinto
a. Labile cells .b. Stable cells. c. Permanent cells.

Labile cells:- These are continuously dividing cells which
pass directly from M to G1 phase of the cell cycle.
They are of short life span.-Examples are epidermis of the skin, surface epithelium of gastro-intestinal and genito-urinary system and hemopoietic cells of the bone marrow.

Stable cells: - Normally, these cells undergo few postnatal divisions but
are capable of division when activated or after injury ( pass from Go to G1).
They include hepatocytes, renal tubular cells, glandular cells, and mesenchymal cells e.g smooth muscle, osteoblasts, cartilage cells, endothelium and connective tissue cells.
Injury of these cells is followed by complete regeneration if the supporting framework is preserved.

Permanent cells: These cells have left the cell cycle and CANNOT
undergo mitotic division in postnatal life. Permanent cells are found in the central nervous
system and heart.
Once they are destroyed, they cannot regenerate.


The cells which have the capacity to multiply through out their life:
A. Stable cells B.Permanent cells C.Labile cells D.None of the above Ans. ‘C’ [Ref. Harshmohan 3rd Ed Pg 135]

In a 50-year-old woman found to be positive for hepatitis A antibody, the serum aspartate aminotransferase (AST) level was 275U/L and that of alanine aminotransferase (ALT) was 310U/L. A month later, these enzyme levels have returned to normal. At the end of the month after infection, in which part of the cell cycle are most of the hepatocytes going to be?
a. G0 b. G1 c. S D. G2 e. M
Ans. A Hepatocytes are quiescent (stable) cells that can re-enter the cell cycle and
proliferate in response to hepatic injury. The liver can partially regenerate itself. Acute hepatitis results in hepatocyte necrosi, marked by AST and ALT elevations.

Cellular Responses To Injury1. Cellular Adaptation- the cell may adapt to the
change and revert back to normal after the stress removal
2. Sub Cellular changes- the residual effects may persist in the cell as evidence of injury.
3. Intracellular accumulations- metabolites may accumulate within the cell.
4. Reversible cell injury- injury may recover5. Irriversible cell injury- the cell dies.

Etiology of cell injury
Genetic cause Acquired causes

Acquired causes
Based on underlying agent: Hypoxia and ischaemia Physical agents Chemical agents and drugs Microbial agents Immunologic agents Nutritional derangement Psychological factors

Hypoxia and ischaemia
Deficiency of oxygen or hypoxia results in failure to carry out cellular activities.
Most common, causes of hypoxia are:Reduced supply of blood to cells- ischaemiaOxygen deprivation can result from other causes like-
anaemia, carbon monoxide poisoning, cardiorespiration insufficiency and increase in demand of tissues

Physical agents
Mechanical trauma Thermal trauma Electricity Radiation rapid changes in atmospheric pressure

Chemical agents
Chemical poisons: cyanide, arsenic,mercury. Strong acid and alkalis Insecticides and pesticides High oxygen concentration Hypertonic glucose and salt Alcohol and narcotic drugs Theraputic drugs

Microbial agents
Infection caused by Bacteria Rickettsiae Viruses Fungi Protozoa Metazoa Parasites

Immunologic agents
Immunity is a double edged sword :Hypersensitivity reactionsAnaphylatic reactions Autoimmune diseases

Nutritional derangements
Nutritional deficiency diseases : deficiency of nutrients ( eg. Starvation), of protein
calorie ( eg. Marasmus, kwashiorkor)Of minerals ( eg. Anaemia)
Nutritional excessObesityAtterosclerosisHeart diseaseHypertension

Psycologic factors
Mental stress Strain Anxiety Overwork Frustration


Pathogenesis of ischaemic and hypoxic injury
Reversible cell injuryIrreversible cell injury

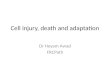
Reversible cell injury
HYPOXIA/ISCHAEMIA
↓ ATP
↓ Intercellular pH (cytosol)
Damaged sodium pump
(membrane)
↓ Protein synthesis (RER)
Ultrastructural/Functional Changes
REVERSIBLE CELL INJURY


Irreversible cell injury
2 essential features: Inability of the cell to reverse mitochondrial
dysfunctionDisturbance in cell membrane function
In addition: depletion of proteins, leakage of lysosomal enzymes into cytoplasm, reduced intracellular pH and further reduction in ATP.

Mitochondrial dysfunction
Continued hypoxia leads to influx of large amount of Calcium ions.
Normal Ca ions – in ECF 10-3 M (millimoles) Cytosole 10-7 M
Leads to mitochondrial dysfunction
Morphological mitochondrial changes: Vacuoles in mitochondria Deposition of amorphous Ca in mitochondrial matrix.


The first step inhibited due to hypoxic injury is: a. Oxidative phosphorylation b. Glycogenesis c. Detachment of ribosomes from RER d. Cell shrinkage
Ans. A The first point of attack of hypoxia id the cells aerobic respiration, i.e. oxidative phosphorylation by mitochondria ATP production is decreased → Na-K Pump stops → more Na inside → cell becomes hyperosmolar → water enters → swelling of cell → bleb formation → along with this ribosomes also detach. This process is reversible if O2 is supplied.

Membrane damage
Membranes in general and plasma membrane Mechanism:
Accelerated degradation of membrane phospholipids.Cytoskeletal damageToxic oxygen radicalsHydrolytic enzymesSerum estimation of liberated intracellular enzymes


MEMBRANE DAMAGE
Nuclear changes (Pyknosis, Karyolysis,
Karyorrhexis)
Cell Death(myelin figures)
Serum enzyme estimation ( SGOT,
LDH)
Libration of intacellular enzymes



Reversible and irreversible injury
See Ch. 1, p. 9,Fig. 1-9


The characteristic feature of hypoxic irreversible injury is/are:
a. Vacuolization of mitochondria b. Swelling of lysosomes c. Calcium densities d. All of the above
Ans. D

Cellular swelling and fatty change are example of: a. Reversible injury b. Irreversible injury c. Cellular swelling is reversible but fatty change is
irreversible d. None of the above
Ans. A Fatty change is an indicator of reversible cell injury, manifested by appearance of small or large lipid vacuoles in cytoplasm and occurs with hypoxia. Basically seen in cells involved in fat metabolism as in liver.

Free radical- mediated cell injury
Ischaemic reperfusion injury Radiolysis of water Chemical toxicity Hyperoxia (toxicity due to oxygen therapy) Cellular aging Killing of exogenous biologic agents Inflammatory damage Destruction of tumor cells Chemical carcinogenesis Atherosclerosis


Generation of oxygen radicals begins within mitochondrial inner membrane.
When cytochrome oxidase catalyses of oxygen (O2 ) to water (H2O)
Intermediates between O2 and H2O are:Superoxide oxygen O’2 : 1 electroneHydrogen peroxide H2O2 : 2 electronesHydroxyl radical OH- : 3 electrones


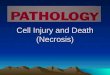
IONISING RADIATION
H2O
Radiolysis
OH-
Proliferating, cells(eg. Epithelial cells)
Non-Proliferating cellsEg. neuron
DNA Damage Lipid peroxidation
Inhibition of DNA
replication
Cell membrane
damage
Apoptosis Necrosis
CELL DEATH
Mechanisms of cell injury by ionising radiation

The histopathological manifestation of oxygen toxicity is due to:
a. Oxygenation of nucleic acid b. Oxygenation of cell organelles except (a) c. Free of oxygen redical d. Oxygenation of cell membrane
Ans. C When patients are subjected to high oxygen concentrations, the free oxygen radicals which are released interact with cell organelles and autocatalytic reactions are initiated resulting in mutation or cell death rather than in oxygenation

Morphology of irreversible cell injury (cell death)
Cell death is a state of irreversible injury
In living body it may occur as:Local or focal change (autolysis, necrosis and
apoptosis)Changes that follow( gangrene and pathologic
calcification)End of life ( somatic death)

Autolysis / self digestion Disintegration of the cell by its own
hydrolytic enzymes liberated from lysosomes
It is rapid in some tissues rich in hydrolytic enzymes such as pancreas and gastric mucosa.
Morphologically , autolysis is identified by : Homogeneous and eosinophilic cytoplasm Loss of cellular details Remains of cell as debris

NECROSIS Defined as- focal death along
with degradation of tissue by hydrolytic enzymes librated by cells, accompanied by inflammation.
2 essential features: Cell digestion by lytic
enzymes Denaturation of proteins

Morphologic changes in necrosis: Cytoplasmic
Homogenous and intensely eosinophilic Occasionally: vacuolation or dystrophic calcification
Nuclear Pyknosis- condensation of nuclear chromatin Karyolysis – undergo dissolution Karyorrhexis- fragmentation into many clumps

3) Disappearance of nuclear chromatin is called as: A. Pyknosis B. Karyolysis C. Karyorhexis D. None Ans. (A) (Ref: Robbin’s –7th Ed/Pg 29, 30) pyknosis, characterized by nuclear shrinkage &
increased basophilia. Here. the DNA apparently condenses into a solid, shrunken basophilia mass.

The fading of cellular chromatin is a. Karyolysis b. Karyorrhexis c. Pyknosis d. Cytolysis
Ans. A [Ref: Robbin’s 7th Ed Pg 29, 30] Nuclear changes assume one of the 3 patterns, all due to the
non-specific breakdown of the DNA. Karyolysis: the basophilia of the chromatin may fade,
presumably due to the DNAse activity. Pyknosis: it is characterized by the nuclear shrinkage and
increased basophilia; the DNA condenses into a solid shrunken mass.

Pyknosis is characterized by a. Nuclear basophilia b. Nuclear Shrinkage
c. Nucleus disintegration d. Nucleolus disintegration
Ans. B

A glassy homogenous, increased eosinophilia with moth eaten appearance in a cell is indicated of:
a. Reversible fatty change b. Reversible hypoxia
c. Necrosis d. B and C
Ans. C These are the characteristic features of a necrotic cell which is coupled with nuclear changes – Pyknosis, keryolysis, keryohyrrexia.

Karyolysis leads to: a. Decreased eosinophilia b. Increased eosinophilia c. Decreased basophilia d. Increased basophilia Ans. C Due to karyolysis the basophila decreases but a
necrotic cell in initial stages is characterized by increased eosinophilia. Increase in basophilia is typical of pyknosis

Types of necrosis
5 types : Coagulative necrosis Liquefaction (colliquative) necrosis Caseous necrosis Fat necrosis Fibrinoid necrosis

Coagulative necrosis
Most common type Caused by irreversible focal injury, mostly from
sudden cessation of blood flow (ischaemia)and less often from bacterial and chemical agents
Organs affected are: heart, kidney and spleen.

Gross appearance
Foci of coagulative necrosis:
In early stages: pale, firm, and slightly swollen.
With progression: become more yellowish, softer, and shrunken.

Microscopically
Hallmark of coagulative necrosis: conversion of normal cells into their ‘tombstones’ i.e. outlines of the cells are retained so that the cell type can still be recognised but their cytoplasm and nuclear details are lost.
Necrosed cells are swollen and appear more eosinophillic than normal

Microscopic changes are the result of: Denaturation of proteins Enzymatic digestion of the cell.
Eventually, the necrosed focus is infiltrated by inflammatory cells and
The dead cells are phagocytosed leaving granular debris and fragments of cells.

Myocardial infarct is an example of: a. Coagulation necrosis b.Liquefactive necrosis c. Caseous necrosi d. Cell death nut not of necrosis
Ans. A

Hypoxic death leads to: a. Coagulation necrosis b.Liquefactive necrosis c. Caseous necrosis d. Cell death nut not of necrosis
Ans. A

Coagulation necrosis is seen in all cells (except in): a. Liver b. Heart c. Brain d.
Lungs Ans. C The process of coagulative necrosis is
characteristic of hypoxic death of cells in all tissues except the brain.

Coagulative necrosis is seen in: a. Brain b. Breast c. Liver d. All Ans. C

Coagulative necrosis is typically seen with: a. Focal bacterial infections b. Hypoxic death c. Loss of tissue architecture d. All of the above Ans. B Coagulative necrosis is associated with hypoxic death and
maintenance of tissue architecture in all the cells of the body except in brain where characteristically liquefaction necrosis is seen and tissue architecture is lost. Caseous necrosis is typically seen in TB where tissue architecture is partially lost.

Liquefaction ( colliquative) necrosis
It occurs commonly due to ischaemic injury and bacterial or fungal infections.
It occurs due to degradation of tissue by the action of powerful hydrolytic enzymes.
Common eg. Infarct brain and abscess cavity.

Liquefaction necrosis is commonly seen ina. Brain b. Lung c. Liver d. Spleen
Ans. A

Caseous necrosis
Found in the centre of foci of tuberculous infection.
It is a combined feature of coagulative and liquefactive necrosis.

Grossly
Foci of caseous necrosis, as the name implies, resemble dry cheese and are soft, granular and yellowish.
This appearence is partly attributed to the histotoxic effects of lipopolysaccharides present in the capsule of the tubercle bacilli, Mycobacterium tuberculosis.

Microscopically
The necrosed foci are structureless, eosinophilic and contain granular debris.
The surrounding tissue shows characteristic granulomatous iflammatory reaction consisting of epitheloid cells with interspersed giant cells of langhan’s or foreign body type and peripherally lymphocytes.

5) Caseation necrosis is suggestive of- A. Tuberculosis B. Sarcoidosis
C. Leprosy D. Mid line lethal granuloma
Ans. 'A'(Ref: Harsh Mohan, Ed. 2nd Pg-35)

Fat necrosis
It is a special form of cell death occurring at two anatomically different locations but morphologically similar lesions.
These are:Following pancreatic necrosisTraumatic fat necrosis commonly in breast

Fat necrosis in either of the 2 instances results in hydrolylsis of neutral fat present in adipose cells into glycerol and free fatty acids.
The damaged adipose cells assume cloudy appearance when only free fatty remain behind , after glycerol leaks out.
The leaked out free fatty acids, complex with Ca to form Ca soaps (sponification)

Grossly
Appears as yellowish-white and firm deposits.
Ca soap imparts the necrosed foci firmer and chalky white appearance.

Microscopically
The necrosed fat cell has a cloudy appearance
Surrounded by inflammatory reaction.
Formation of calcium soaps is identified in the tissue sections as amorphous, granular and basophilic material.

Fibrinoid necrosis
It is characterized by the deposition of fibrin-like material which has the staining properties of fibrin.
It is encountered in various examples of immunologic tissue injury (eg. Autoimmune diseases, arthus reaction), artioles in hypertension, peptic ulcer etc.


Microscopically
Identified by brightly eosinophilic, hyaline-like deposition in the vessel wall or on the luminal surface of a peptic ulcer
Local haemorrhages may occur due to rupture of these blood vessels.

Which of the following is correctly matched a. Caseating necrosis – Tuberculosis b.Caseation - yellow fever c. Fat necrosis – Pancreatitis d. Gumma –
infarction
Ans. A & C

Hypoxic death leads to a. Liquef active necrosis b. Coagulative
necrosis c. Caseous necrosis d. Fat necrosis
Ans. B

Apoptosis
Apoptosis is a form of ‘coordinated and internally programmed cell death’ which is of significance in variety of physiologic pathologic conditions.
Apoptosis in Greek meaning ‘falling off’ or ‘dropping off’.

Morphologic changes Shrinking of cell : with dense cytoplasm and almost normal
organelles. Convolution of cell membrane with formation of membrane-
bound near-spherical bodies called apoptotic bodies containing compacted organelles.
Chromatin condensation around the periphery of nucleus No acute inflammation. Phagocytosis of apoptotic bodies by macrophages

Molecular mechanisms of apoptosis
Initiators of apoptosis1. Absence of stimuli eg. Hormone, growth
factors, cytokines.2. Activators of programmed cell death.
Eg. TNF receptors.3. Intracellular stimuli eg. Heat, radiation,
hypoxia etc. Regulators of apoptosis.eg. bcl-2, p53,
caspases, bax etc.

Progammed cell death.1. Fas receptor activation- leads to activation of
caspase and subsequent proteolysis.2. Ceramide generation- hydrolysis of plasma
membrane ceramide is generated which further leads to mitochondrial injury.
3. DNA damage- produced by various agents such as ionising radiation,
chemotherapeutic agents, activated oxygen species lead to apoptosis
DNA damage affects nuclear protein p53 which induces the synthesis of cell death protein bax.

Phagocytosis The dead apoptotic cells and their fragments
possess cell surfacereceptors which facilitate their identification by adjucent phagocytes.

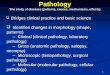
Initiators of apoptosis(transmembrane, intracellar)
Regulators of apoptosis(bcl-2, others)
Programmed cell death
Fas receptor activation (cytotoxic T cells)
DNA damage (radiation, chemotherapy, free radicals
Caspases
ceramideP53Bax
Mitochondrial injury DNA damage
APOPTOSIS
PHAGOCYTOSIS
MECHANISM OF
APOPTOSIS


Physiologic Processes
1. Development of embryo2. Physiologic involution of cells in hormone-
dependent tissues eg. Endometrial shedding.3. Normal cell destruction followed by
replacement proliferation eg. Intestinal epithelium

Pathologic processes
1. Cell death in tumor2. Cell death by cytotoxic T cells.3. Cell death in viral infections4. Pathologic atrophy of organ and tissues on withdrawal
of stimuli eg. Atrophy of kidney or salivary glandon obstruction of ureter or ducts respectively.
5. Cell death in response to injurious agents involved in causation of necrosis eg. radiation., hypoxia and mild thermal injury
6. Pgrogressive depletion of CD4+ T cells in AIDS

Apoptosis is suggestive of:
A. Liquefaction degeneration. B. Coagulation necrosis. C. Neoangiogenesis. D. Epithelial dysplasia.Ans. B (Ref: Rubin 3rd / 13, 14; Anderson 10th)

Cytoplasmic cytochrome C is associated with: A. Glycolysis B. Apoptosis C. Drug metabolization D. All Ans. (B) (Ref: Robbin ‘s-7th Ed/Pg 29, 30)

'Physiologic programmed cell death' is termed as
a. Apoptosis b. Lysis c. Autolysis d. Autopsy
Ans. A

Apoptosis is a pathological process associated with: a. Cellular hyperplasia b. Cellular dysplasia
c. Cellular death d. Cellular hypertrophy
Ans. C

About apoptosis, true statement is: a. Injury due to hypoxia b. Inflammatory reaction is present c. Councilman bodies is a type of apoptosis d. All of these
Ans. C

Gene inhibiting apoptosis is: a. bcl2 b. P53 c.Ras d. N-myc
Ans. A



Gangrene
Gangrene is a potentially life-threatening condition caused by a critically insufficient blood supply (necrosis).
This may occur after an injury or infection, or in people suffering from any chronic health problem affecting blood circulation.
The primary cause of gangrene is reduced blood supply to the affected tissues, which results in cell death.
Diabetes and long-term smoking increase the risk of suffering from gangrene.

3 types of gangrene
Dry Wet Gas In either type of gangrene, coagulation necrosis
undergo liquefaction by the action of putrefactive bacteria.

Dry gangrene
Dry gangrene is a form of coagulative necrosis that develops in ischemic tissue, where the blood
supply is inadequate to keep tissue viable. Dry gangrene is often due to peripheral artery disease, but can
be due to acute limb ischemia. The limited oxygen in the ischemic limb limits
putrefaction and bacteria fail to survive. The affected part is dry, shrunken and dark reddish-black. The line of separation usually brings about complete
separation, with eventual falling off of the gangrenous tissue if it is not removed surgically, a process called autoamputation.

Wet gangrene
Wet, or infected, gangrene is characterized by thriving bacteria and has a poor prognosis (compared to dry gangrene) due to septicemia resulting from the free communication between infected fluid and circulatory fluid.
The tissue is infected by saprogenic microorganisms eg.Clostridium perfringens or Bacillus fusiformis , which cause tissue to swell and emit a fetid smell.
Wet gangrene usually develops rapidly due to blockage of venous (mainly) and/or arterial blood flow.

The affected part is saturated with stagnant blood, which promotes the rapid growth of bacteria.
The toxic products formed by bacteria are absorbed, causing systemic manifestation of septicemia and finally death.
The affected part is edematous, soft, putrid, rotten and dark

Gas gangrene
Gas gangrene is a bacterial infection that produces gas within tissues. It can be caused by Clostridium, most commonly alpha
toxin producing Clostridium perfringens, or various non-clostridial species.
Infection spreads rapidly as the gases produced by bacteria expand and infiltrate healthy tissue in the vicinity.
Because of its ability to quickly spread to surrounding tissues, gas gangrene should be treated as a medical emergency.

Gas gangrene is caused by bacterial exotoxin-producing clostridial species, which are mostly found in soil.
These environmental bacteria may enter the muscle through a wound and subsequently proliferate in necrotic tissue and secrete powerful toxins.
These toxins destroy nearby tissue, generating gas at the same time.
A gas composition of 5.9% hydrogen, 3.4% carbon dioxide, 74.5% nitrogen, and 16.1% oxygen was reported in one clinical case.
Progression to toxemia and shock is often very rapid.

Gangrene is the death of a part accompanied by
a. Suppuration b. Putrefaction c. Calcification d. Coagulation
Ans. B [Ref. Harshmohan 3rd Ed Pg 40] Gangrene is a form of necrosis of tissue
with superadded putrefaction.

Gangrene is defined as: a. Necrosis of body parts b. Coagulative necrosis of body parts c. Necrosis with putrefaction d. All are true
Ans. C

Metastatic calcification Metastatic calcification is
deposition of calcium salts in otherwise normal tissue, because of elevated serum levels of calcium.
Occur because of deranged metabolism as well as increased absorption or decreased excretion of calcium and related minerals, as seen in hyperparathyroidism.

Dystrophic Calcification
Dystrophic calcification is caused by abnormalities or degeneration of tissues resulting in mineral deposition, though blood levels of calcium remain normal.
Metastatic calcification is often found in many tissues throughout a person or animal, whereas dystrophic calcification is localized.

Dystrophic calcification are calcifications seen ina. Skin layers b. Salivary glands
c . Normal tissues d. Dead tissue
Ans. D [Ref. Harshmohan 3rd Ed Pg 42] Dystrophic calcification occurs in dead and
degenerated tissues. Calcium metabolism and serum calcium level are normal. Commonly occurs in different types of necrosis, infarcts, thrombi, hematomas etc.

Metastatic calcifications are seen in a. Hypoparathyroidism b.Vitamin D deficiency c.Hypercalcemia d.All the above Ans. C

Necrotic cells and tissue attract: a. Polyostotic calcification b. Dystrophic calcification c. Anatropic calcification d. None of the above
Ans. B If necrotic cells and cellular debris are not promptly
destroyed and reabsorbed, they tend to attract calcium salts and become mineralized. This is known as dystrophic calcification (Other modes of calcification are not defined modes of calcification).

Dystrophic calcification is commonly seen in: a. Hyperparathyroidism b.Vitamin D deficiency c. Atheromatous plaque d. Lungs
Ans. C

Metastatic calcification occurs in all except: a. Kidney b.Atheroma c. Fundus of stomach d.Wall of IVC
Ans. B

THANK YOU