Embed Size (px)
Citation preview
CHEST TRAUMA
REFRESHMENT FOR
EMERGANCY DOCTORS
Hussein Elkhayat,MD
Cardiothoracic surgery department
Faculty of medicine
Assiut university
7 july 2014 El-eiman general hospital , Assiut
Think about chest trauma
All multiple trauma patients have chest trauma
till proven otherwise
•If there is head injury and abdominal trauma
there is also chest trauma. (Therefore if CT
scanning the other two scan the chest as well)
Most injuries to the chest, both blunt and
penetrating, do not require surgery.
Only about 10% of chest injuries actually
require operative management.
All cardiothoracic injuries should be
considered lethal until proven otherwise.
PATHOPHYSIOLOGY
Cardiothoracic trauma can be classified as
penetrating or blunt.
Penetrating wounds of the chest such as
gunshot and stab wounds can directly injure
any or all structures in the trajectory of the
missile or weapon, causing rib fractures,
pneumothorax, hemothorax, or pulmonary or
cardiac injury. In contrast, low-velocity
penetrating trauma does not generally damage
surrounding structures not directly injured.
Blunt forces applied to the chest wall cause
injury by three mechanisms:
Rapid deceleration
Direct impact
Compression of the chest by a very heavy
object impedes ventilation and may result in
traumatic asphyxia
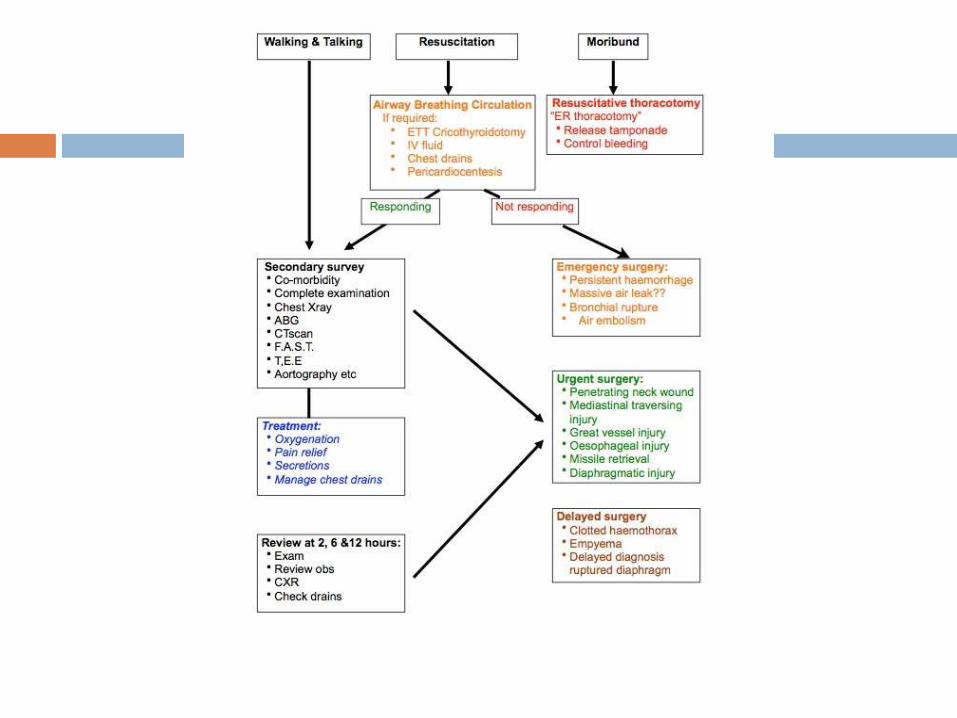
First Glance/Triage/Primary Survey
Walking/Talking can proceed directly to secondary survey
Moribund - a decision will need to be taken as to whether they are unsalvageable (e.g. dismemberment) or salvageable by emergency thoracotomy.
When to do a resuscitative ("E.R.") thoracotomy?Rarely is it indicated, even more rarely is it successful. It is almost never useful in blunt trauma. Successful outcome has been reported with the following:
◦Cardiac arrest due to tamponade or exsanguination
◦Young patient
◦Penetrative trauma to pericardium
◦Signs of life during transit to hospital
Resuscitation required - standard
ABC
•Airway
•BreathingAs part of assessment and treatment of breathing and circulation the insertion of chest drains should be considered.
•Circulation
Rapid clinical evaluation
Age , co morbidities
Mechanism of trauma
Site of pain / bleeding
Examination
Inspection , palpation , auscultationUsually percussion in difficult to perform in noisy busy trauma service
Secondary Survey
•ABG
•Chest Xray
•Cervical Spine Xray
•Limb Xrays
•Angiography as indicated
Focused abdominal ultrasound
•CT scan - this has replaced some of the above in certain circumstances. CT is part of the secondary survey and should not be done of bleeding, unstable patients or those undergoing resuscitation. Unstable patients should be resuscitated adequately which may mean operating before full radiological assessment.
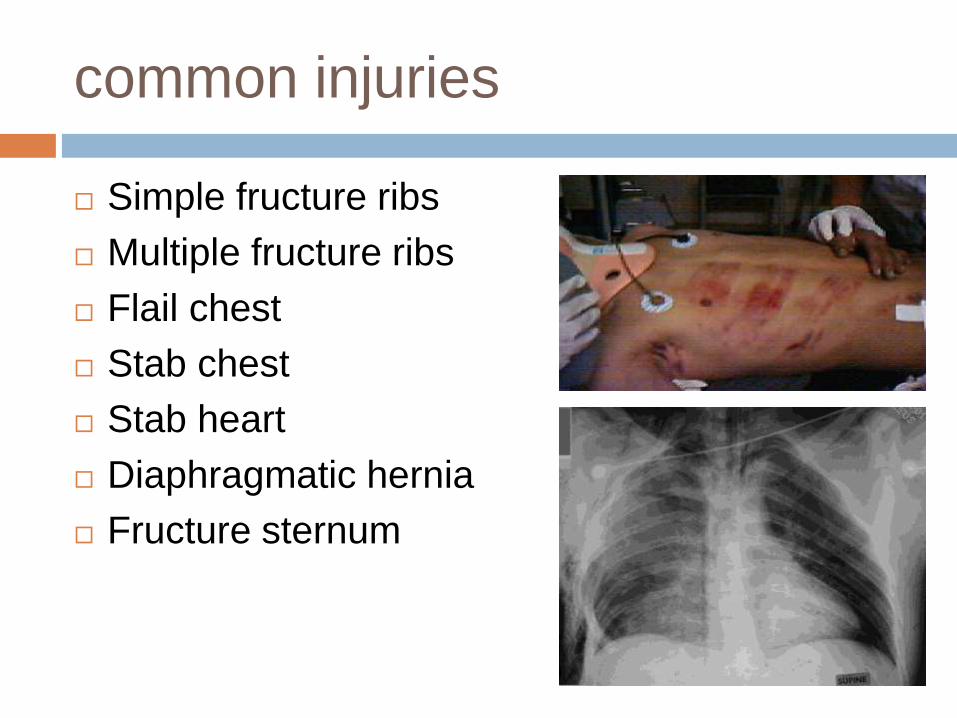
common injuries
Simple fructure ribs
Multiple fructure ribs
Flail chest
Stab chest
Stab heart
Diaphragmatic hernia
Fructure sternum
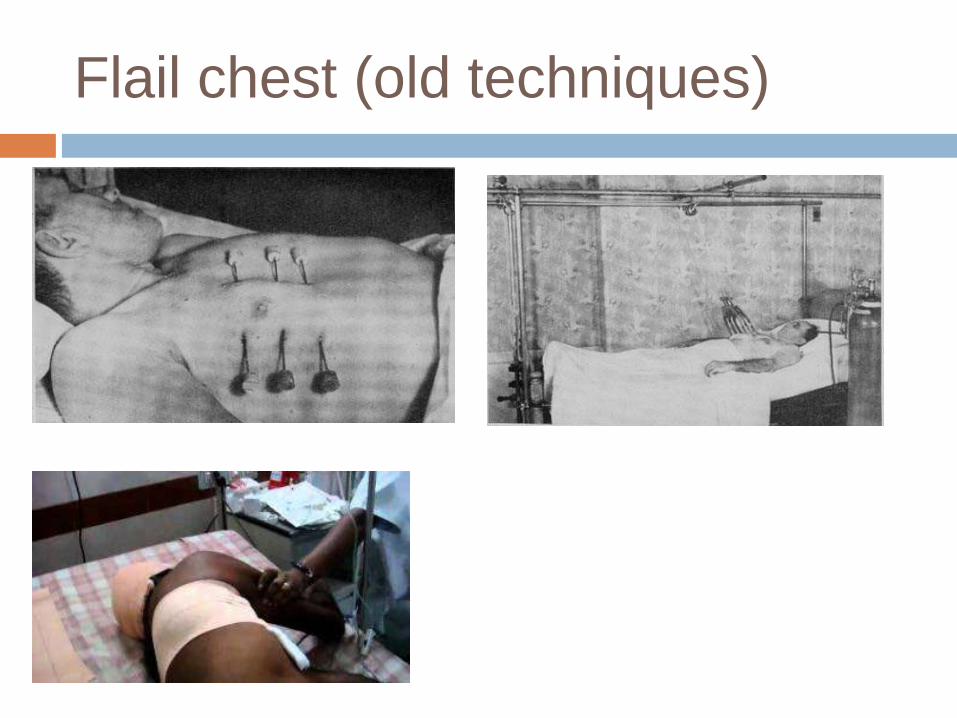
Flail chest (old techniques)
Fail chest (new modalities)
Proper analgesia ( thoracic epidural , opioids ,
nerve block)
Internal pneumatic fixation (using endotracheal
tube and ventilator with PEEP) in pt. with head
trauma or unfit for surgery now
SURGICAL fixation using wires or plates in pt.
who will undergo thoracotomy for another
reason, sever deformity or indentation of the
ribs in lung parenchyma .
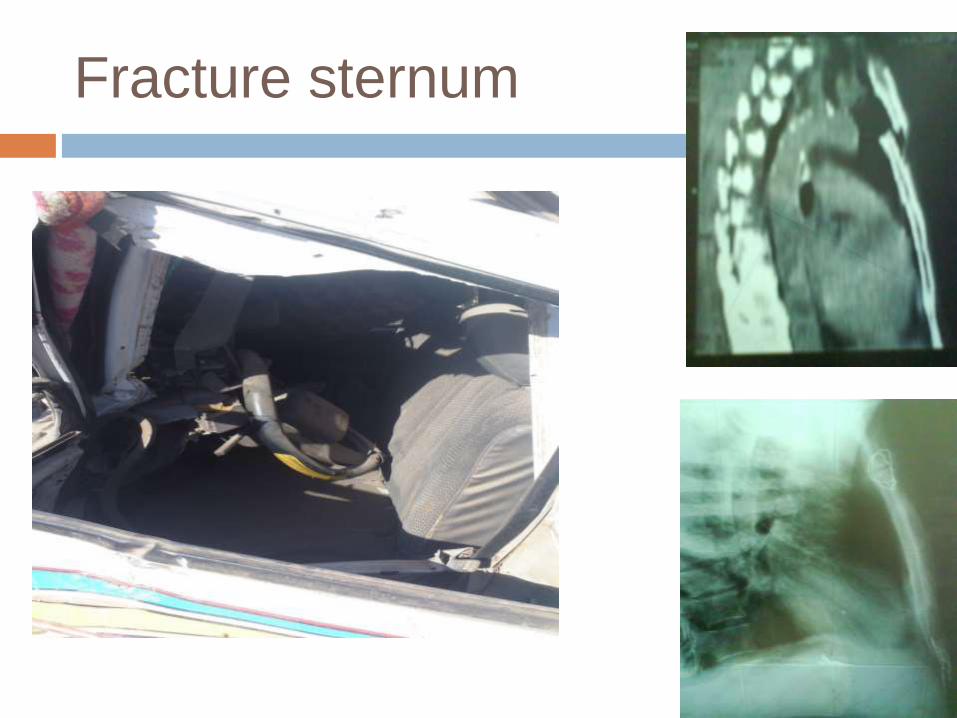
Fracture sternum
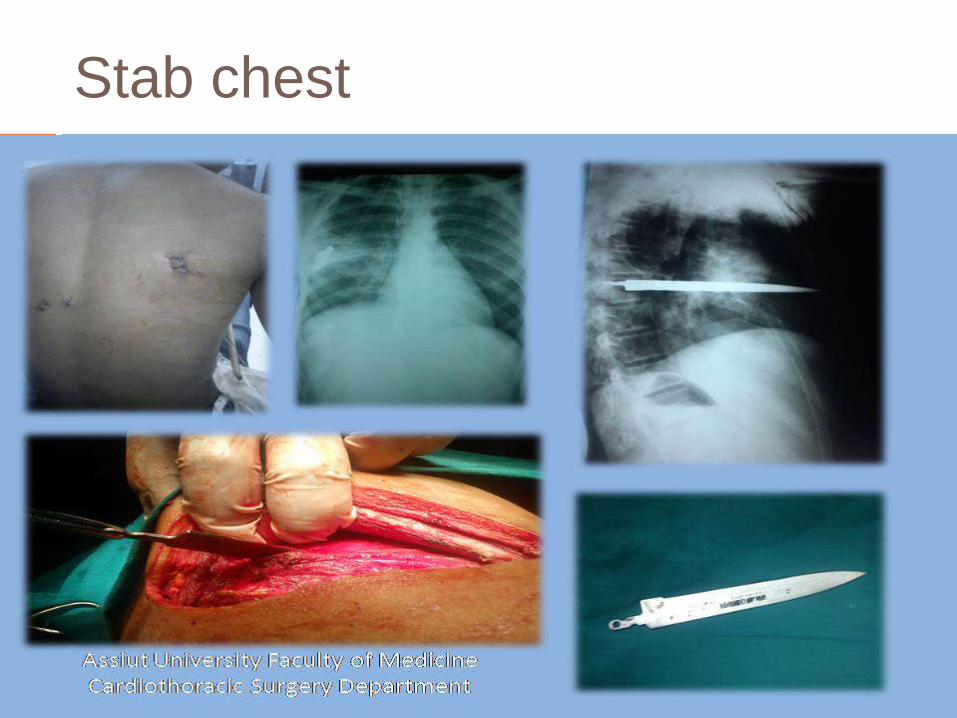
Stab chest
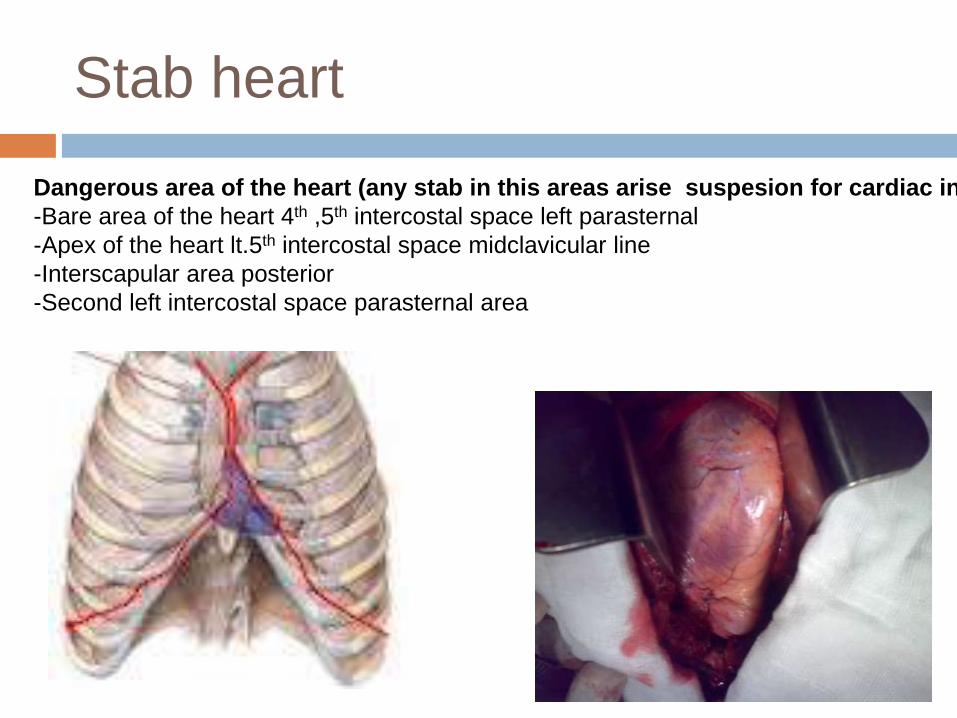
Stab heart
Dangerous area of the heart (any stab in this areas arise suspesion for cardiac injury)
-Bare area of the heart 4th ,5th intercostal space left parasternal
-Apex of the heart lt.5th intercostal space midclavicular line
-Interscapular area posterior
-Second left intercostal space parasternal area
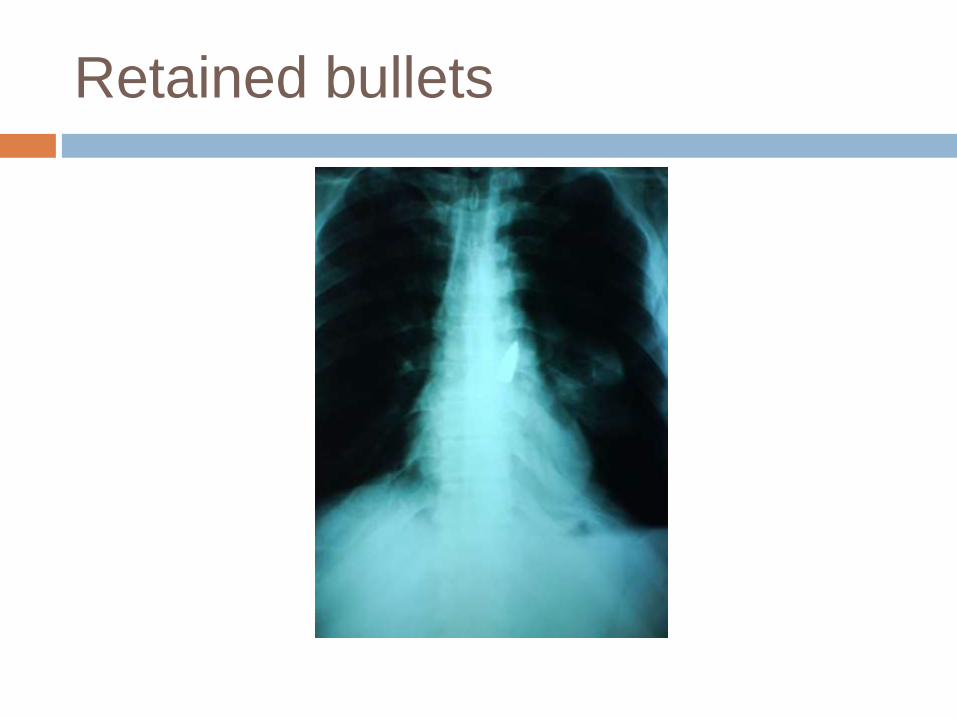
Retained bullets
A trauma patient in shock, associated with theabsence of breath sounds and/or dullness onone side of the chest, should be treated formassive hemothorax until proven otherwise.
Most cases of hemothorax can be adequatelytreated by a tube thoracotomy and restorationof circulating blood volume.
More than 50% of fracture ribs can’t be seenon chest x ray film (clinical evaluation is themost important parameter)
History of chest trauma, physical examination
findings of Beck’s triad (distended neck veins,
hypotension, and muffled heart tones), or
pulsus paradoxus indicate the diagnosis of
pericardial tamponade.
Immediate treatment of cardiac tamponade in
trauma consists of aggressive fluid
replacement and open surgical drainage.
Echocardiography is the diagnostic method of
choice in patients with ECG abnormalities or
unexplained cardiovascular instability following
blunt cardiac trauma.
Thoracic CT with contrast has emerged as the
initial test of choice to diagnose aortic injury in
the setting of an abnormal mediastinum noted
on CXR.
The most common error in diaphragmatic
trauma is failure to suspect the possibility of
diaphragmatic injury.
Esophageal trauma is lethal if unrecognized
because it will lead to mediastinitis and
bacterial necrosis due to contamination of the
mediastinal space by esophageal contents.
Lower rib fractures are associated with injuries
to the spleen and liver.
As a general rule, younger patients with
flexible chest walls are less likely to have rib
fractures.
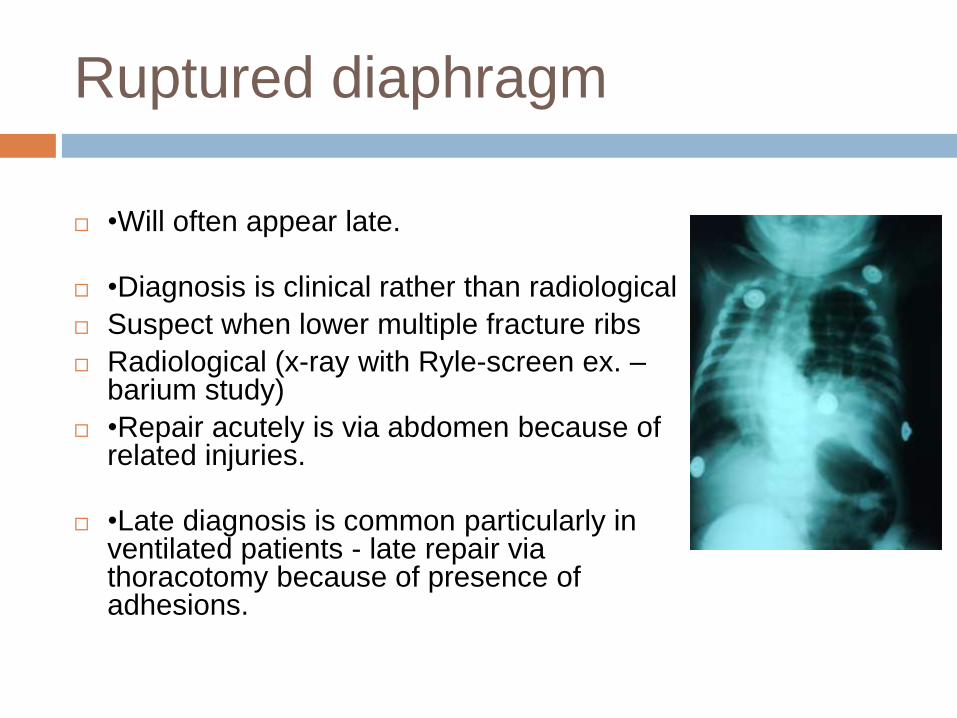
Ruptured diaphragm
•Will often appear late.
•Diagnosis is clinical rather than radiological
Suspect when lower multiple fracture ribs
Radiological (x-ray with Ryle-screen ex. –barium study)
•Repair acutely is via abdomen because of related injuries.
•Late diagnosis is common particularly in ventilated patients - late repair via thoracotomy because of presence of adhesions.
When not to admit patient with
chest trauma
Every patient with relevant chest trauma need
admission and follow up for at least 24 hr.
Patient can be followed up on out patient clinic
in case of young age with simple in place
fracture ribs with tolerable pain from near
discrete
Patient refuse admission should sign informed
consent regarding the need for follow up and
possibility of complications
When to put in a chest drain
without prior chest Xray?
If there is possible chest trauma and breathing is laboured or there is cardiac instability.
•Be prepared to place bilateral emergency drains "on spec"
•If you think about it!
•Emergency drains should be placed with caution via the axillary "triangle of safety" without a trocar.
When to put in a chest drain on the
basis of a CXR post trauma?
•Any post-traumatic pneumothorax.
•massive post-traumatic subcutaneous emphysema??
•Haemothorax
•The above are particularly important if a procedure is to be performed under general anaesthetic and positive pressure ventilation.
What if a drain stops working?
Mechanical factor
Procedure factor
Patient factor
Prophylactic chest drains
In general prophylactic chest drains are not recommended. The exceptions are:
•known chest injury where ambulance transfer is required,
•known chest injury where operative procedures (e.g. fracture fixation) are to be performed under general anaesthetic with positive pressure ventilation,
•where needle thoracentesis has been performed, with positive or negative result, and positive pressure ventilation is required.
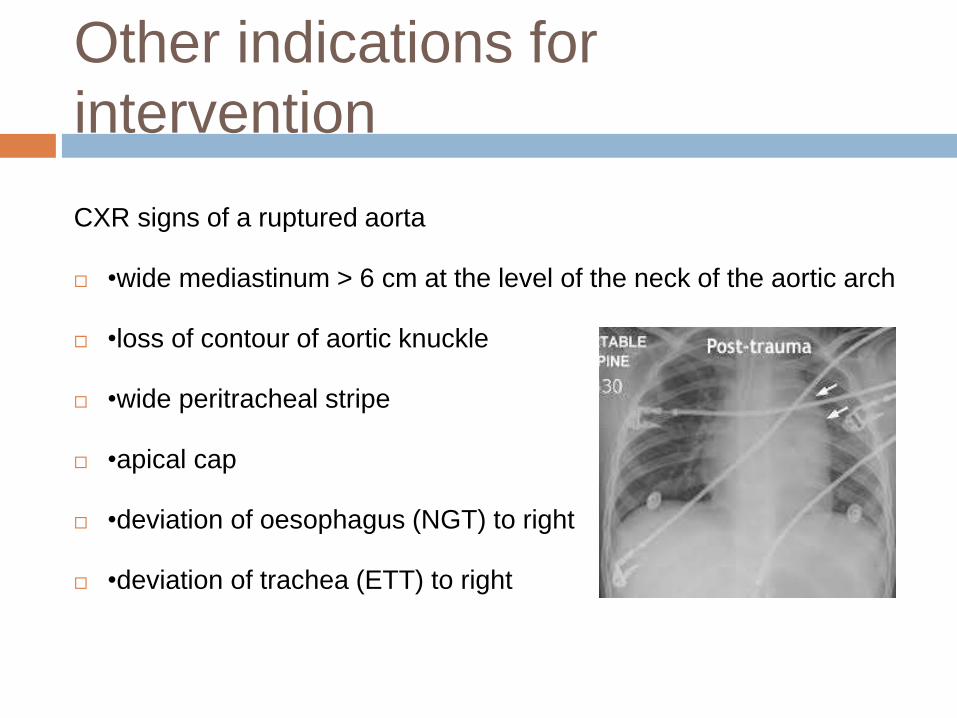
Other indications for
intervention
CXR signs of a ruptured aorta
•wide mediastinum > 6 cm at the level of the neck of the aortic arch
•loss of contour of aortic knuckle
•wide peritracheal stripe
•apical cap
•deviation of oesophagus (NGT) to right
•deviation of trachea (ETT) to right
Review
Chest injury patients should have a formal review few hours after admission with repeat
•Chest Xray,
•Blood gases and
•Clinical appraisal
All patients with chest drains should have daily chest Xrays.
Medical treatment for isolated
chest trauma
Analgisics : NSAIDs , opioids , nerve block
Bronchodilators : used for treatment of
pulmonary contusions
ICU admission for pain control and chest care
in case of very old fragile patients .
Medical treatment for patient with
chest tube
Antibiotics : prophylaxis , usually first
generation cephalosorin
Analgesics : NSAIDs , opioids , nerve block
Bronchodilators : used for treatment of
pulmonary contusions
ICU admission for pain control and chest care
in case of very old fragile patients
Medical treatment for patient
underwent emergency thoracotomy
Antibiotics : covering gram +ve, -ve, anerobes
Analgesics : NSAIDs , opioids , nerve block during thoracotomy.
Bronchodilators : used for treatment of pulmonary contusions
Transximic acid ( cyclocapron )
Expectorant
ICU admission for high volume blood loss patients , pain control and chest care in case of very old fragile patients and for mechanical ventilation for patients with flail segement after fixation.
When to discharge patient with
chest trauma
Clinical : tolerable pain
Examination: - equal air entery
- no spasm or crepetus
Investigation : - clear lung fields , no
pericardial collection in case of heart injury
Drains : - less that 50 cc / 24 hr.
When to remove chest tube in
traumatized ventilated patient
Examination: - equal air entery
- no spasm or crepetus
Investigation : - clear lung fields
Drains : - less that 50 cc / 24 hr.
in absence of portable CXR in the ICU and
difficulty to discover recollection or
pnemonthorax in unstable patients , chest tube
left in place until patients general conditions
improves with consultation of staff member in
charge as regard removal
How to insert a chest tube
http://www.nejm.org/doi/full/10.1056/NEJMvcm
071974
Thank u