Embed Size (px)
Citation preview
CLINICAL PHARMACY IN CLINICAL PHARMACY IN CARDIOLOGYCARDIOLOGY
ISCHEMIC HEART DISEASEISCHEMIC HEART DISEASE
There are 35 risk factors for development of IHD 3 most important ones are –
““big triplebig triple””
hypercholesterolaemiahypercholesterolaemia arterial hypertensionarterial hypertension
smokingsmoking
95 % of patients with IHD are observed to have aterosclerotic changes in coronary arteries
Angina, or angina pectoris, is the medical term used to describe the temporary chest discomfort that occurs when the heart is not getting enough blood
The heart is a muscle (myocardium) and gets its blood supply from the coronary arteries.
Blood carries the oxygen and nutrients the heart muscle needs to keep pumping.
When the heart does not get enough blood, it can no longer function at its full capacity.
When physical exertion, strong emotions, extreme temperatures, or eating increase the demand on the heart, a person with angina feels temporary pain, pressure, fullness, or squeezing in the center of the chest or in the neck, shoulder, jaw, upper arm, or upper back. This is angina, especially if the discomfort is relieved by removing the stressor and/or taking sublingual (under the tongue) nitroglycerin.
The discomfort of angina is temporary, meaning a few seconds or minutes, not lasting hours or all day.
An episode of angina is not a heart attack. Having angina means the patient have an increased risk of having a heart attack.
A heart attack is when the blood supply to part of the heart is cut off and that part of the muscle dies (infarction).
Angina can be a helpful warning sign if it makes the patient seek timely medical help and avoid a heart attack.
Prolonged or unchecked angina can lead to a heart attack or increase the risk of having a heart rhythm abnormality. Either of those could lead to sudden death.
Not all chest pain is angina. Pain in the chest can come from a number of causes, which range from not serious to very serious Chest pain can be caused by:
acid reflux (gastroesophageal reflux disease, GERD),
upper respiratory infection,
asthma, or
sore muscles and ligaments in the chest (chest wall pain)
If chest pain is severe and/or recurrent, the patient should see a healthcare provider.
Life-threatning symptoms: chest pain +
sweating,
weakness,
faintness,
numbness or tingling,
nausea
Pain that does not go away after a few minutes
Pain that is of concern in any way
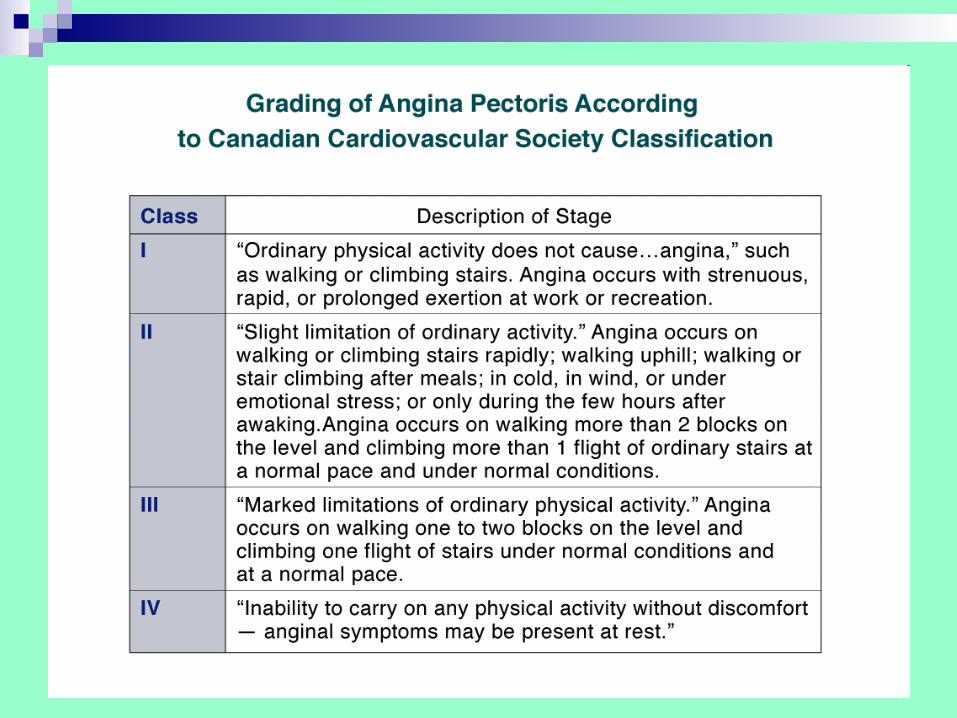
Angina is classified as one of the following two types:
Stable angina People with stable angina usually have angina symptoms on a regular
basis. The episodes occur in a pattern and are predictable.
For most people, angina symptoms occur after short bursts of exertion.
Stable angina symptoms usually last less than five minutes.
They are usually relieved by rest or medication, such as nitroglycerin under the tongue.
Unstable angina Angina symptoms are unpredictable and often occur at rest.
This may indicate a worsening of stable angina, but sometimes the first time a person has angina it is already unstable.
The symptoms are worse in unstable angina - the pains are more frequent, more severe, last longer, occur at rest, and are not relieved by nitroglycerin under the tongue.
Unstable angina is not the same as a heart attack, but it warrants an immediate visit to the healthcare provider or a hospital emergency department. The patient may need to be hospitalized to prevent a heart attack.
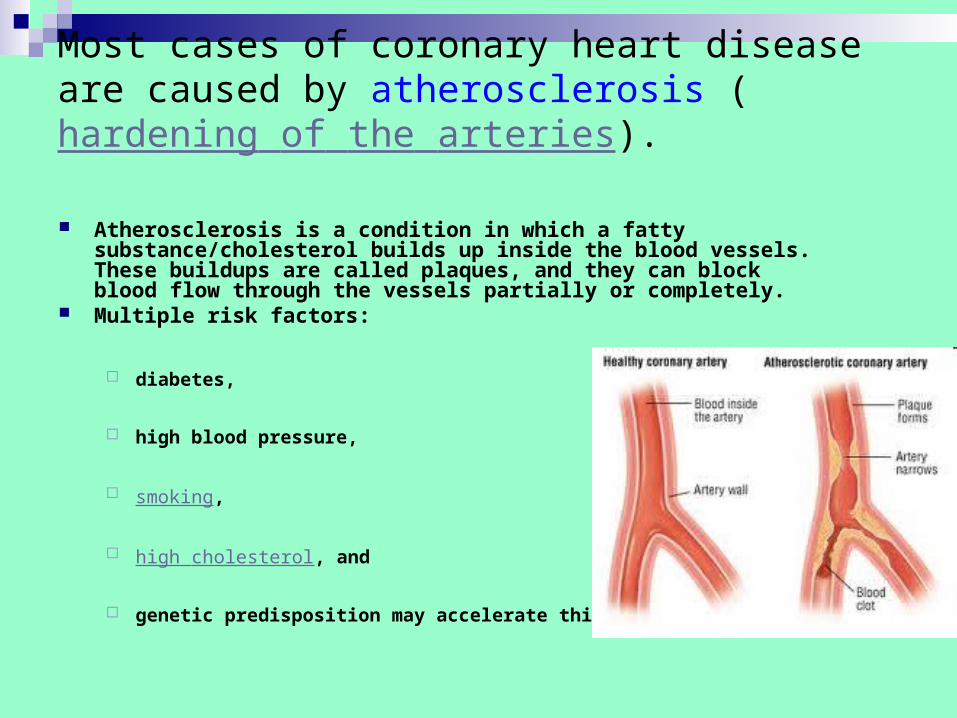
Most cases of coronary heart disease are caused by atherosclerosis (hardening of the arteries).
Atherosclerosis is a condition in which a fatty substance/cholesterol builds up inside the blood vessels. These buildups are called plaques, and they can block blood flow through the vessels partially or completely.
Multiple risk factors:
diabetes,
high blood pressure,
smoking,
high cholesterol, and
genetic predisposition may accelerate this build up.
Coronary Artery Spasm Another cause of unstable angina is coronary artery spasm.
Spasm of the muscles surrounding the coronary arteries causes them to narrow or close off temporarily. This blocks the flow of blood to the heart muscle for a brief time, causing angina symptoms.
This is called variant angina or Prinzmetal angina.
This is not the same as atherosclerosis, although some people have both conditions.
The symptoms often come on at rest (or during sleep) and without apparent cause.
Cocaine use/abuse can cause significant spasm of the coronary arteries and lead to a heart attack.
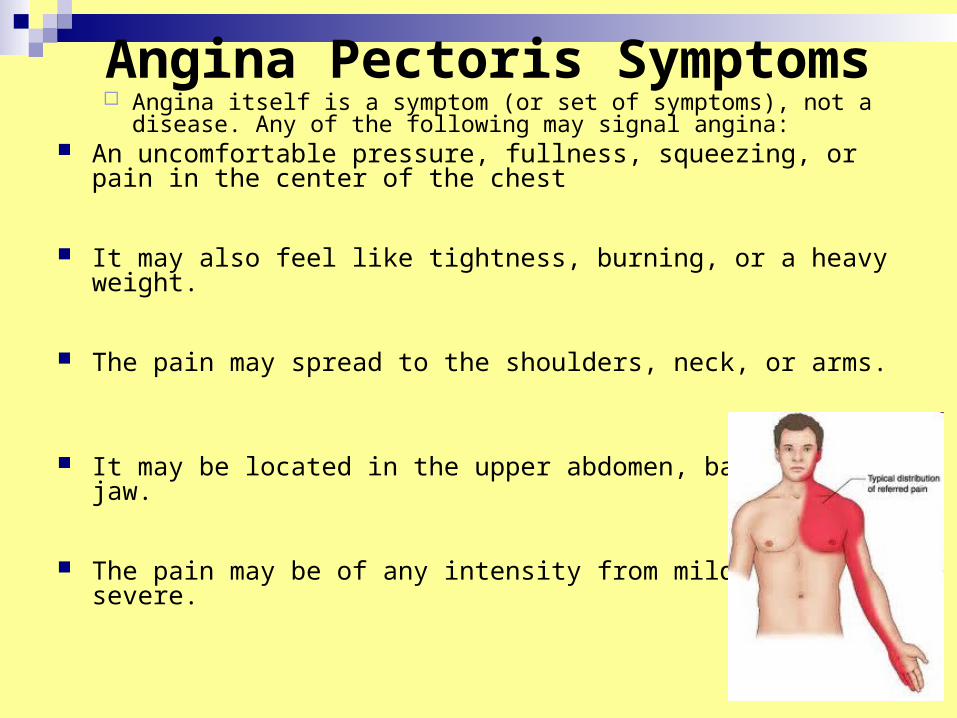
Angina Pectoris Symptoms Angina itself is a symptom (or set of symptoms), not a disease. Any of
the following may signal angina: An uncomfortable pressure, fullness, squeezing, or pain in the
center of the chest
It may also feel like tightness, burning, or a heavy weight.
The pain may spread to the shoulders, neck, or arms.
It may be located in the upper abdomen, back, or jaw.
The pain may be of any intensity from mild to severe.
Other symptoms may occur with an angina attack:
Shortness of breath
Lightheadedness
Fainting
Anxiety or nervousness
Sweating or cold, sweaty skin
Nausea
Rapid or irregular heart beat
Pallor (pale skin)
Feeling of impending doom These symptoms are identical to the signs of an impending heart attack described by the
American Heart Association. It is not always easy to tell the difference between angina and a heart attack, except angina only lasts a few minutes and heart attack pain does not go away.
AntianginalAntianginal ((coronary activecoronary active)) drugsdrugs
a group of drugs which using different mechanisms even out irregularities between myocardium need in oxygen and it’s blood supply by coronary arteries
clinically it is manifested by removal or prevention of angina attacks (improvement of disease current) and increasing of patients’ tolerance to physical load
ANTIANGINALANTIANGINAL ( (CORONARY CORONARY ACTIVEACTIVE) ) DRUGSDRUGS
І. І. Nitrates and sidnonims which are close to the Nitrates and sidnonims which are close to the first onesfirst ones
ІІ. ІІ. BetaBeta--blockersblockersІІІ. ІІІ. Calcium channel blockers (CCBs):Calcium channel blockers (CCBs): ІУ. ІУ. Activators of potassium channelsActivators of potassium channels
• Hypercholesterolemia drugs• Antiplatelets and anticoagulants • Drugs with metabolic influence on miocardium

NITRATESNITRATES nitroglycerinnitroglycerin
isosorbidisosorbid dinitratedinitrate isosorbidisosorbid-5--5-mononitratemononitrate
MECHANISM OF ACTION MECHANISM OF ACTION OF NITRATESOF NITRATES
• Interaction with sulfhydryl (SH-) groups (nitrate receptors) inside cells of vascular smooth muscles
• Stimulation of formation of endothelial factor of relaxation of vessels (ЕRF) – nitrogen oxide (NO)
• Decreasing of ionized Са2+ contents
• Relaxation, dilation of vessels, including coronary vessels
MECHANISM OF ACTION MECHANISM OF ACTION OF NITRATESOF NITRATES
• Decreasing of tone of venules – decreasing of preloading (income of blood into heart during diastole) – decreasing of work of left ventricle and heart output• Decreasing of tone of arterioles – decreasing of afterloading (decreasing of arterial pressure, end diastolic pressure in left ventricle and it’s volume, decreasing of tension of myocardium wall• decreasing of heart need in oxygen • improvement of blood float in ischemic zone of myocardium – redistribution of coronary blood circulation with increasing of perfusion of subendocardial areas• dilation of large coronary vessels if they are in spasm or narrowed with aterosclerotic mass • development of anastomoses between arteries in myocardium (in case of prolonged administration)
NITROGLYCERINENITROGLYCERINE• TabletsTablets (under the tongue)• 1 % alcohol or oil solutionsolution (under the tongue)• aerosolaerosol
Latent period - 2-3 min Duration of action - 20-30 min
• ampoulesampoules 1 % solution – intravenously dropply 0,01% solution
• prolongedprolonged forms of nitroglycerine: trinitrolong, sustak, nitrong, ointment, plaster
• Nitroglycerin is taken only when the patient actually has symptoms or expect to have them. Slow - or long-acting nitroglycerin can be used as a preventative treatment for angina but not until beta blockers are tried first.
NitroglycerineNitroglycerineUnique transdermal system in a form of
plaster
SIDE EFFECTS OF SIDE EFFECTS OF NITROGLYCERINENITROGLYCERINE
burstingbursting, , pulsating headachepulsating headache
decreasing of arterial pressuredecreasing of arterial pressure ((heartbeatheartbeat, , dizzinessdizziness, , collapsecollapse))
skin rednessskin redness, , feeling of feverfeeling of fever
Contraindications for Contraindications for nitroglycerine usenitroglycerine use
• Close-angled form of glaucoma
• increasing of intracranial pressure, stroke
• acute myocardium infarction (in case of presence of hypotension and collapse)
PROLONGED FORMS OF PROLONGED FORMS OF NITROGLYCERINENITROGLYCERINE
• Trinitrolong – polymer films (0,001 g or 0,002 g of nitroglycerine) action develops immediately, lasts for 3-5 hours
• Sustac Sustaс-mite (contains 0,0026 g of nitroglycerine) and Sustac-forte (0,0064 g of nitroglycerine)
beginning of action – after 10 min, maximal action – after 1 hour, duration of action – 4-5 hours
• Nitrong – microcapsule form of nitroglycerine of prolonged action
latent period – 30-60 min, maximal effect - after 3-4 hours,
action duration - 6-8 hours
Other nitratesOther nitratesNitrosorbid – isosorbid dinitrate
latent period 30-50 min, duration of action – 4-6 hours and more
With sublingual administration of the drug latent period grows short to 3-5 min
• buccal form (Dinitrolslrbilong)• tablets of prolonged action (Isoket-retard)
• ointment• aerosol
• drugs for intravenous introduction
Isosorbid-5-mononitrate - pharmacologically active metabolite of isosorbid dinitrate
duration of action - from 6 till 24 hours

Iso Mak Retard 20mgIso Mak Retard 40mg Isomak Retard 60mg(isosorbid dinitrate)
IsoketIsoketIsosorbid dinitrateIsosorbid dinitrate
SYDNONIMINSSYDNONIMINSMolsidomineMolsidomine – – corvatoncorvaton - -
sydnopharmsydnopharm is metabolized in liver forming a substance – SIN-1a which contains free
NО group (doesn’t need previous interaction with SH-groups) • nitrogen oxide stimulates guanilatecyclase that activates synthesis of cGMP
• cGMP causes dilation of vessels
2 mg of molsidomine= 0,5 mg of nitroglycerine
MolsidomineMolsidomine• latent period - 20 min (5-10 min – if administered
sublingually), action duration - 6 hours. • can be used for prophylaxis and releasing angina
attacks in patients with glaucoma (doesn’t increase intraocular pressure)
• indicated for patients who make breaks in using nitrates to decrease tolerance towards them
• doesn’t lead to development of tolerance (doesn’t need previous combining with drugs containing SH- groups)
• absence of withdrawal syndrome
BETA-BLOCKERSBETA-BLOCKERSUsing in AnginaUsing in Angina
• blockade of 1-adrenoreceptors of heart: decreasing of power and frequency of heart contractions and as follows cardiac need in oxygen
• decreasing of thrombocyte aggregation and prevention of clotts formation
• increasing of diastole duration – improvement of coronary vessels saturation with blood – improvement of perfusion of ischemic areas of myocardium
• Decreasing of calcium ions accumulation – releasing of cardiac muscle tension, improvement of metabolic processes, increasing of ATP synthesis
• in case of acute myocardium infarction – increasing of blood supply of ischemic areas of heart, decreasing of size of infarction seat, prevention of development of cardiac arrhythmias

AnaprilinAnaprilin β1- β 2 adrenoblocker

Vasocardin Vasocardin 100 100 mgmgMethoprolol tartrateMethoprolol tartrate

NebivololNebivololbeta-blocker that also causes vasodilation by stimulating the release beta-blocker that also causes vasodilation by stimulating the release
of nitric oxideof nitric oxide
• Beta blockers are taken every day, regardless of whether the patient is having symptoms, because they are proven to prevent heart attacks and sudden death.
Calcium channel blockers1. Derivatives of difenilalkilamin (verapamil)
2. Derivatives of benzothiazepine (dylthiazem)
3. Derivatives of dyhydropyridine (nifedipin, amlodipin, nimodipin)
Drugs of 1 and 2 groups dominantly influence on heart (depress automatism of sinus node, conductivity through conductive heart system), show antiarrhythmic, antianginal and hypotensive action.
Derivatives of dyhydropyridine (group of nifedipin) – decrease blood pressure and cause dilation of coronary vessels, cause reflective tachycardia
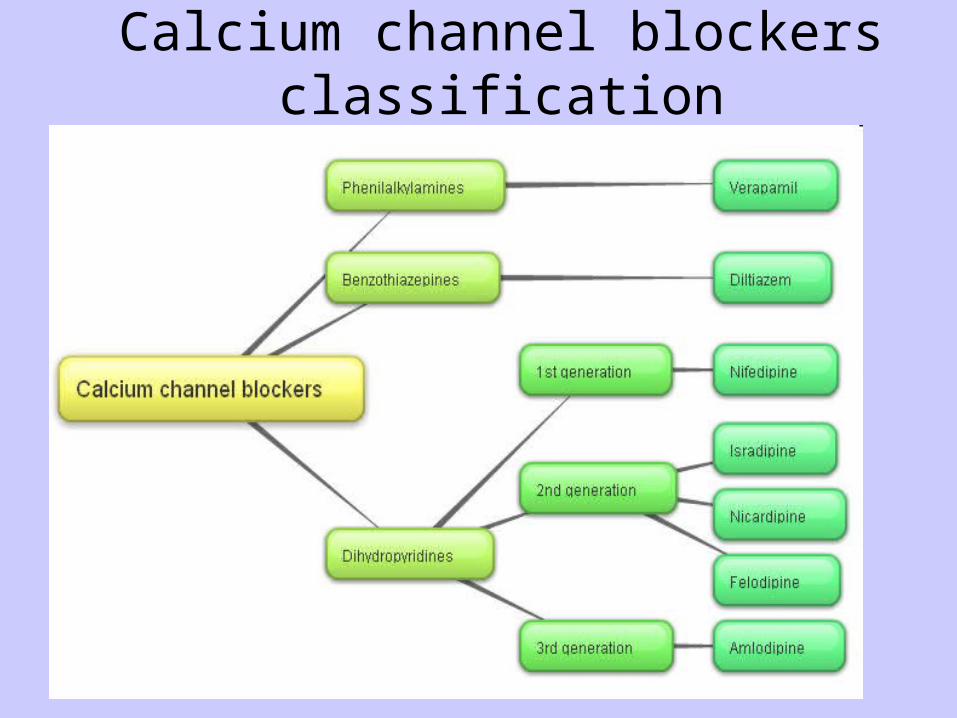
Calcium channel blockers classification
Nifedipin Nifedipin -- corinfarcorinfar - - fenigidinfenigidin - - adalateadalate
Doesn’t depress conductivity in myocardium,has a weak antiarrhythmic action
Maximal concentration of the drug in blood occurs after 45-60 min after administration orally and after 2-3 min – if administered
sublingually Effect lasts for 4-6 hours
Antagonists of calcium ionsAntagonists of calcium ions – derivatives of dyhydropyridine of ІІ ІІ generationgeneration (amlodipinamlodipin, isradipin, nicardipin)
• almost don’t cause tachycardiaalmost don’t cause tachycardia• areare indicated for prolonged treatment of indicated for prolonged treatment of
patients with stable anginapatients with stable angina • aren’t indicatedaren’t indicated in case of non stable anginain case of non stable angina
((long lasting latent periodlong lasting latent period))
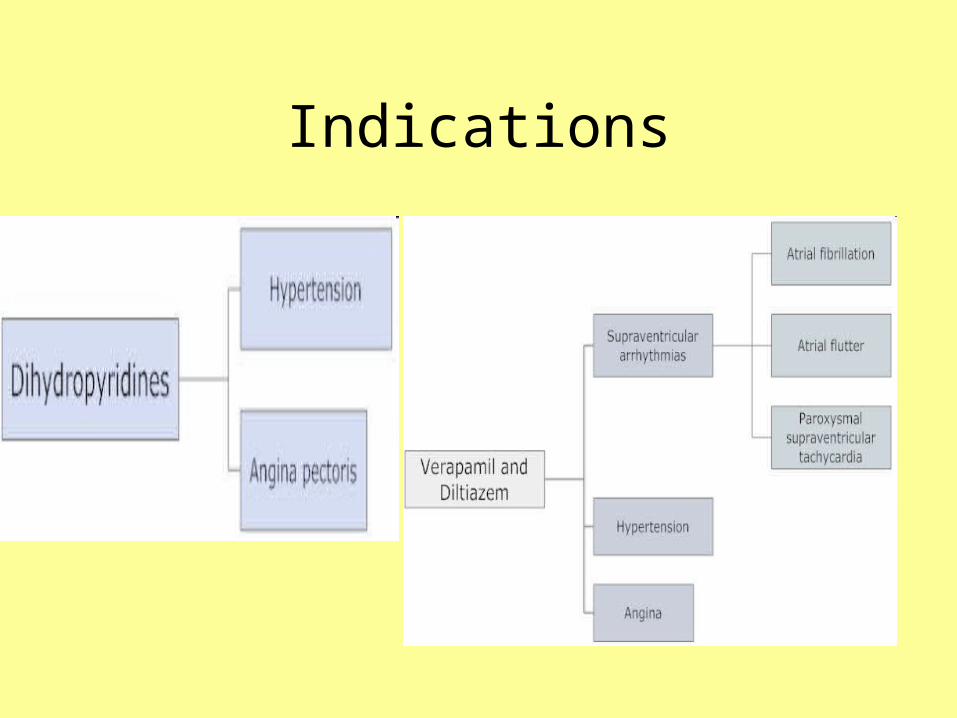
Indications

Nifedipin (Са2+ ions antagonist of dyhydropyrydine series)

Nifedipin (
• Calcium channel blockers are used primarily when beta blockers cannot be used and/or the patient is still having angina with beta blockers. Calcium channel blockers also lower blood pressure and certain ones slow heart rate. Calcium channel blockers have to be taken every day.
Common side effects of calcium channel blockers
include:• headache, • constipation, • rash, • nausea, • flushing, • edema (fluid accumulation in tissues), • drowsiness, • low blood pressure, and • dizziness. • Sexual dysfunction, overgrowth of gums, and liver dysfunction also
have been associated with calcium channel blockers. Verapamil (Covera-HS, Verelan PM, Calan) and diltiazem (Cardizem LA, Tiazac) worsen heart failure because they reduce the ability of the heart to contract and pump blood.
POTASSIUM-CHANNEL POTASSIUM-CHANNEL ACTIVATORACTIVATORSS
NICORANDIL NICORANDIL IkorelIkorel
• activates Са2+-depending potassium channels• causes relaxation of smooth muscles of vessels – coronary, arteriolar and venous vasodilation • improvement of blood supply of myocardium,
decreasing of pre- and afterloads of heart, decreasing of myocardial need in oxygen, separation of ischemic damage zone
Antiplatelet agentsCommonly prescribed include:• Aspirin• Ticlopidine• Clopidogrel• Dipyridamole
Acetylsalicylic acidAcetylsalicylic acid
• 80-100 mg per day – as antiplatelet drug, decreases risk of development of acute myocardial infarction and decreases mortality of patients with IHD
• Helps prevent clotting in patients who have had a heart attack, unstable angina, ischemic strokes, TIA (transient ischemic attacks, or "little strokes") and other forms of cardiovascular disease.
• Usually prescribed preventively when plaque buildup is evident but there is not yet a large obstruction in the artery.
Common types of cholesterol-lowering drugs
include:• statins • resins • nicotinic acid (niacin) • gemfibrozil • clofibrate
• Various medications can lower blood cholesterol levels. They may be prescribed individually or in combination with other drugs. They work in the body in different ways. Some affect the liver, some work in the intestines and some interrupt the formation of cholesterol from circulating in the blood.
Reason for Medication• Used to lower LDL ("bad") cholesterol, raise HDL
("good") cholesterol and lower triglyceride levels
Choose good nutrition Reduce blood cholesterol Lower high blood pressure Be physically active every day Aim for a healthy weight Manage diabetes Reduce stress Limit alcohol Stop smoking
ACUTE MYOCARDIAL ACUTE MYOCARDIAL INFARCTIONINFARCTION
• one of the main reasons of disablement and mortality of people of employed age in many world countries, including Ukraine
• men suffer from MI almost 5 times more often than women
• Mortality of patients with MI during first two hours starting from the beginning of the process makes around 50 % of all mortal cases connected with MI
• the most often death causes – acute cardiac-vascular insufficiency (angina pectoris, lung edema, cardiogenic shock), heart rupture, heavy cardiac arrhythmia
• other complications of MI – thrombosis and emboli, acute and chronic heart aneurisms, Dresler’s syndrome, chronic cardiac insufficiency
TREATMENT OF MYOCARDIAL INFARCTION
threethree stagesstages• Immediate treatment – decreasing pain and treatment of
heart beats arrest• Early treatment – separation of zone of infarction seat and
prevention of early life threatening complications (cardiac arrhythmias, acute cardiac insufficiency)
• Further treatment – prevention and therapy of late complications of MI, prophylaxis of recurrent MI and death of the patients
TREATMENT OF ACUTE MYOCARDIAL TREATMENT OF ACUTE MYOCARDIAL INFARCTIONINFARCTION
Releasing of pain and Releasing of pain and cardiogenic shock prophylaxiscardiogenic shock prophylaxis
• nitroglycerin (1 tablet under the tongue every 7-10 min.) • Neuroleptanalgesia (fentanil with droperidol), morphine,
omnopon, promedol (in combination with atropine, dimedrol, aminasine)
• nitrous oxide in combination with neuroleptics• in case of remaining pain – non narcotic analgesics in
combination with antihistamine and neuroleptic drugs• to increase arterial pressure during cardiogenic shock –
intravenously dropply dopamine (drugs of choice), noradrenalin, mesaton
• sometimes glucocorticosteroids are used
TREATMENT OF ACUTE MIOCARDIAL INFARCTION (cont’d)
Size limitationSize limitation of infarction seatof infarction seat
• Intravenous dropply introduction of 0,01 % nitroglycerin solution
• Administration of -blockers
TREATMENT OF ACUTE MYOCARDIAL TREATMENT OF ACUTE MYOCARDIAL INFARCTION (cont’d)INFARCTION (cont’d)
Treatment and prophylaxis of heart Treatment and prophylaxis of heart arrhythmiasarrhythmias
Treatment of ventricular arrhythmias – i.v. slowly 0,2 % solution of xycain, novocainamid intramuscularly
• Prophylaxis of ventricular extrasystole and tachycardia – magnesium sulfate (intravenous dropping introduction of 4-5 % solution),
-adrenoblockers• Arrhythmias of atrial origin – heart glycosides, antagonists
of calcium channels• Bradycardia - isadrin, atropine sulfate, alupent (i.v.)
TREATMENT OF ACUTE MYOCARDIAL INFARCTION (cont’d)
CORRECTION OF BLOOD CLOTTINGCORRECTION OF BLOOD CLOTTING
• thrombolytic drugsthrombolytic drugsstreptokinase (1,5 mln OD), urokinase (2 mln OD), aktilise –
recombinant tissue activator of plasminogen (100 mg) intravenous• after performing of thrombolytic therapy – intravenous introduction of heparin, at first 10 000 OD, after 1000 OD per
hour during 24-48 hours • anticoagulants of indirect actionanticoagulants of indirect action
• acetylsalicylic acidacetylsalicylic acid (80-100-300 mg per day)
Treatment of heart insufficiencyTreatment of heart insufficiency • i.v. furosemid (40-120 mg); i.v. dropply nitroglycerine (12-20 hours),
morphine• i.v. dropply dopamin and dobutamin • heart glycosides – in tachysystolic form of scintillating arrhythmia or
fluttering of atria with moderate left-ventricular insufficiency
General measuresGeneral measures• oxygen inhalation• correction of acid-base balance
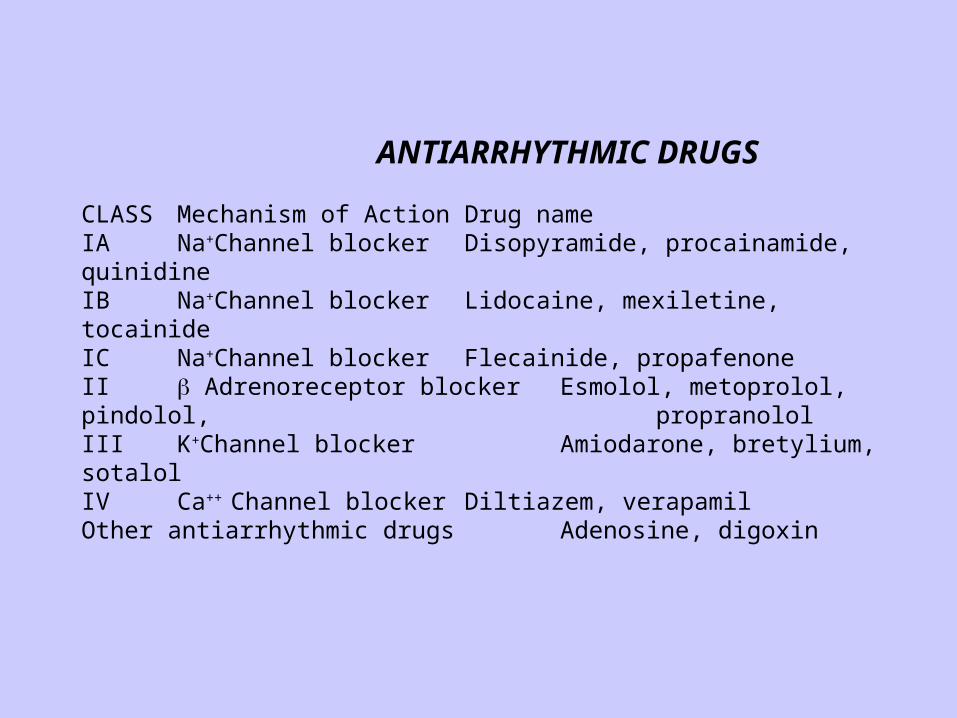
ANTIARRHYTHMIC DRUGS
CLASS Mechanism of Action Drug nameIA Na+Channel blocker Disopyramide, procainamide, quinidineIB Na+Channel blocker Lidocaine, mexiletine, tocainideIC Na+Channel blocker Flecainide, propafenoneII Adrenoreceptor blocker Esmolol, metoprolol, pindolol,
propranolol III K+Channel blocker Amiodarone, bretylium, sotalolIV Ca++ Channel blocker Diltiazem, verapamilOther antiarrhythmic drugs Adenosine, digoxin