Embed Size (px)
Citation preview
Complications inCardiothoracicSurgeryAVOIDANCE AND TREATMENT
Editor
Alex G. Little, MDThe Elizabeth Berry GrayChairman and ProfessorDepartment of SurgeryWright State University School of MedicineDayton, Ohio

Complications in Cardiothoracic Surgery
AVOIDANCE AND TREATMENT

Complications inCardiothoracicSurgeryAVOIDANCE AND TREATMENT
Editor
Alex G. Little, MDThe Elizabeth Berry GrayChairman and ProfessorDepartment of SurgeryWright State University School of MedicineDayton, Ohio
© 2004 by Futura, an imprint of Blackwell Publishing
Blackwell Publishing, Inc./Futura Division, 3 West Main Street, Elmsford, New York 10523, USABlackwell Publishing, Inc., 350 Main Street, Malden, Massachusetts 02148-5020, USABlackwell Publishing Ltd, 9600 Garsington Road, Oxford OX4 2DQ, UKBlackwell Publishing Asia Pty Ltd, 550 Swanston Street, Carlton, Victoria 3053, Australia
All rights reserved. No part of this publication may be reproduced in any form or by anyelectronic or mechanical means, including information storage and retrieval systems, withoutpermission in writing from the publisher, except by a reviewer who may quote brief passages in a review.
04 05 06 07 5 4 3 2 1
ISBN: 0-87993-427-1
Complications in cardiothoracic surgery : avoidance and treatment /editor, Alex G. Little. — 1st ed.
p. ; cm.Includes bibliographical references and index.
ISBN 0-87993-427-11. Heart—Surgery—Complications. 2. Chest—Surgery—Complications.[DNLM : 1. Thoracic Surgical Procedures—adverse effects. 2.
Intraoperative Complications—prevention & control. 3. PostoperativeComplications—prevention & control. WF 980 C73683 2004] I. Little,—Alex G.
RD597.C645 2004617.4′1201—dc22
2003024723
A catalogue record for this title is available from the British Library
Acquisitions: Steven KornProduction: Julie ElliottTypesetter: Graphicraft Limited, Hong Kong, in 9.5/12pt PalatinoPrinted and bound by MPG Books Ltd, Bodmin, Cornwall, UK
For further information on Blackwell Publishing, visit our website:www.blackwellfutura.com
The publisher’s policy is to use permanent paper from mills that operate a sustainable forestrypolicy, and which has been manufactured from pulp processed using acid-free and elementarychlorine-free practices. Furthermore, the publisher ensures that the text paper and cover boardused have met acceptable environmental accreditation standards.
Notice: The indications and dosages of all drugs in this book have been recommended in themedical literature and conform to the practices of the general community. The medicationsdescribed do not necessarily have specific approval by the Food and Drug Administration foruse in the diseases and dosages for which they are recommended. The package insert for eachdrug should be consulted for use and dosage as approved by the FDA. Because standards forusage change, it is advisable to keep abreast of revised recommendations, particularly thoseconcerning new drugs.
Contents
List of contributors, viiIntroduction, ixAcknowledgments, x
Part I General complications
1 Complications of thoracic incisions, 3Norman J. Snow, MD, Malek G. Massad, MD, and Alexander S. Geha, MD, MS
2 Respiratory complications of thoracic operations, 36Hani Shennib, MD
3 Arrhythmias following cardiothoracic operations, 48Adam E. Saltman, MD, PhD and Joseph LoCicero III, MD
Part II Complications of general thoracic surgery
4 Complications of pulmonary resection, 67Stephen J. Burke, MD and L. Penfield Faber, MD
5 Complications of tracheobronchial resection, 92Douglas J. Mathisen, MD
6 Complications of lung volume reduction procedures, 108Robert J. Burnett, MD and Douglas E. Wood, MD
7 Complications of lung transplantation, 128Paul F. Waters, MD, FRCS(C), FACS
8 Pleural space problems, 135Sudish Murthy, MD, PhD and Thomas W. Rice, MD
9 Complications of chest wall reconstruction, 155M. Bulent Tirnaksiz, MD and Claude Deschamps, MD
10 Complications of esophageal resection, 161Richard J. Battafarano, MD, PhD and Nasser K. Altorki, MD
11 Complications of esophageal reconstruction, 173Alex G. Little, MD
v
vi Contents
12 Complications of antireflux surgery, 183Riivo Ilves, MD, FRCS(C), FACS and Mark R. Dylewski, MD
13 Complications of esophageal instrumentation, 202Donald E. Low, MD
14 Complications of mediastinal surgery, 230Thomas A. D’Amico, MD
Part III Cardiac surgery
15 Complications of coronary artery bypass surgery, 257Nader Moazami, MD and Hendrick Barner, MD
16 Complications of cardiopulmonary bypass and cardioplegia, 280Lawrence L. Creswell, MD
17 Complications of aortic surgery, 349Thoralf M. Sundt, III, MD and Whitney M. Burrows, MD
18 Complications of valvular surgery, 362Jeffrey T. Sugimoto, MD, Anthony D. Bruno, MD, and Karen A. Gersch, MD
19 Postpericardiotomy syndrome, 385William A. Gay, Jr., MD
20 Pulmonary and pleural complications after cardiac surgery, 390Jeffrey E. Everett, MD
21 Neurological complications in cardiac surgery, 405George J. Koullias, MD, PhD and John A. Elefteriades, MD
Index, 437
Nasser K. Altorki, MDAttending Cardiothoracic Surgeon, Professor of Cardiothoracic Surgery, Department ofCardiothoracic Surgery, New York-PresbyterianHospital-Cornell Medical Center, New York, NY
Hendrick Barner, MDProfessor of Surgery, Department of Surgery,Division of Cardiothoracic Surgery, WashingtonUniversity School of Medicine, St. Louis, MO
Richard J. Battafarano, MD, PhD Assistant Professor of Surgery, Division ofCardiothoracic Surgery, Department of Surgery,Washington University School of Medicine, St. Louis, MO
Anthony D. Bruno, MDChief Resident in General Surgery, CreightonUniversity Medical Center, Omaha, NE
Stephen J. Burke, MDFellow, Division of Cardiothoracic Surgery, Rush-Presbyterian-St. Luke’s Medical Center,Chicago, IL
Robert J. Burnett, MDChief Resident, Division of CardiothoracicSurgery, University of Washington, Seattle, WA
Whitney M. Burrows, MDAssistant Professor of Surgery, Division ofThoracic Surgery, University of Maryland,Baltimore, MD
Lawrence L. Creswell, MDAssociate Professor of Surgery, Division ofCardiothoracic Surgery, University of MississippiMedical Center, Jackson, MS
Thomas A. D’Amico, MDAssociate Professor of Surgery, Department ofSurgery, Division of Cardiovascular and ThoracicSurgery, Duke University Medical Center,Durham, NC
Claude Deschamps, MDProfessor of Surgery, Division of General ThoracicSurgery, Mayo Clinic and Mayo Foundation,Rochester, MN
Mark R. Dylewski, MDDivision of Cardiovascular Surgery, West FloridaHospital, Pensacola, FL
John A. Elefteriades, MDProfessor of Surgery (Cardiothoracic), YaleUniversity School of Medicine; Chief ofCardiothoracic Surgery, Yale-New HavenHospital, New Haven, CT
Jeffrey E. Everett, MDAssistant Professor, Department of Surgery,Division of Cardiothoracic Surgery, University of Iowa Health Care, Iowa City, IA
L. Penfield Faber, MDDirector of Thoracic Surgery, Department of Cardiovascular-Thoracic Surgery, Rush-Presbyterian-St. Luke’s Medical Center; Professor of Surgery, Rush Medical CollegeChicago, IL
William A. Gay, Jr., MDProfessor of Surgery, Department of Surgery,Division of Cardiothoracic Surgery, WashingtonUniversity School of Medicine, St. Louis, MO
Alexander S. Geha, MD, MSProfessor and Chief, Division of CardiothoracicSurgery, The University of Illinois College ofMedicine at Chicago, Chicago, IL
Karen A. Gersch, MDChief Resident in General Surgery, CreightonUniversity Medical Center, Omaha, NE
Riivo Ilves, MD, FRCS(C), FACS Director of General Thoracic Surgery, AlbanyMedical Center Hospital; Professor of Surgery,Albany Medical Center, Albany, NY
George J. Koullias, MD, PhDResident in Cardiothoracic Surgery, Yale-NewHaven Hospital, Yale University School ofMedicine, New Haven, CT
Alex G. Little, MDThe Elizabeth Berry Gray Chairman and Professor,Department of Surgery, Wright State UniversitySchool of Medicine, Dayton, OH
List of contributors
vii
viii List of Contributors
Joseph LoCicero III, MDProfessor and Chair, Department of Surgery,University of South Alabama College of Medicine,Mobile, AL
Donald E. Low, MDHead, Section of General Thoracic Surgery,Virginia Mason Medical Center; ClinicalInstructor, Department of Surgery, University ofWashington School of Medicine, Seattle, WA
Malek G. Massad, MDAssociate Professor of Surgery, Division ofCardiothoracic Surgery, Director, Heart and LungTransplant Programs, The University of IllinoisCollege of Medicine at Chicago, Chicago, IL
Douglas J. Mathisen, MDChief of Thoracic Surgery, Massachusetts GeneralHospital; Hermes Grillo Professor of ThoracicSurgery, Harvard Medical School, Boston, MA
Nader Moazami, MDAssistant Professor of Surgery, Department ofSurgery, Division of Cardiothoracic Surgery,Washington University School of Medicine, St.Louis, MO
Sudish Murthy, MD, PhDDepartment of Thoracic and CardiovascularSurgery, The Cleveland Clinic Foundation,Cleveland, OH
Thomas W. Rice, MDHead, Section of Thoracic and CardiovascularSurgery, The Cleveland Clinic Foundation,Cleveland, OH
Adam E. Saltman, MD, PhDAssociate Professor of Surgery and Physiology,Department of Cardiothoracic Surgery, Universityof Massachusetts Memorial Medical Center,Worcester, MA
Hani Shennib, MDProfessor, Department of Surgery, McGillUniversity, Montreal, Quebec, Canada
Norman J. Snow, MDProfessor of Surgery, Division of CardiothoracicSurgery, Section Chief, General Thoracic Surgery,The University of Illinois College of Medicine atChicago; Chief, Thoracic Surgery, West SideVeterans Administration Hospital, Chicago, IL
Jeffrey T. Sugimoto, MDProfessor of Surgery, Vice-Chairman Departmentof Surgery, Chief, Cardiothoracic Surgery,Creighton University Medical Center, Omaha, NE
Thoralf M. Sundt, III, MDSenior Associate Consultant, Division ofCardiovascular Surgery, Mayo Clinic; AssociateProfessor of Surgery, Mayo Medical School,Rochester, MN
M. Bulent Tirnaksiz, MDFellow in General Thoracic Surgery, Division of General Thoracic Surgery, Mayo Clinic andMayo Foundation, Rochester, MN
Paul F. Waters, MD, FRCS(C), FACSProfessor of Surgery, Mount Sinai School ofMedicine, New York, NY
Douglas E. Wood, MDProfessor and Chief, Section of General ThoracicSurgery, Endowed Chair, Lung Cancer Research,University of Washington, Seattle, WA
Introduction
Cardiothoracic surgery, including operative techniques and postoperativecare, can and should be read about in the several available textbooks by bothresidents in training and active practitioners. This activity provides the fund ofknowledge which is the foundation of surgical competence. However, it is thepractical experience gained in the operating room and on the wards dealingwith complications and deviations from the typical or average scenario thatmatures and fully develops a surgeon. The typical textbook demonstrates the‘right’ or standard way to do things and the implicit assumption is that if these guidelines are followed then the patient and the surgeon’s life will be complication free. This is not the case and reminds me of the observationthat good results come from experience and experience is gained by makingmistakes. The goal of this book is to minimize the frequency of surgical complica-tions and maximize the outcome when they do occur by allowing the reader tolearn from the operative and clinical experience of those who have gone beforeso that each generation can collectively stand on the shoulders of the precedinggeneration without the need to learn from one’s own complications.
This book is therefore designed less to address indications for operationsthan how to carry them out and provide postoperative care without complica-tions. While the authors of the various chapters address the correct or rightway to perform operations and care for patients after surgery, they have alsobeen tasked to address and emphasize specific do’s and don’t s for both intraoperative techniques and postoperative care that will reduce the incidence ofcomplications. As some complications, alas, are inevitable, also addressed arethe issues of timely recognition and appropriate treatment of complicationswhen they do occur despite best efforts.
In sum, I hope the reader will see and use this book as a supplement to, not a replacement for, standard text books and operative atlases and that it willcontribute to an ongoing commitment to excellence in cardiothoracic surgery.
ix

Acknowledgments
The editor is grateful to the authors of the various chapters who have sacrificedprofessional and personal time to produce their thoughtful and well-writtenchapters.
Two people deserve my special thanks. The first is Steven Korn, an incred-ibly patient, supportive and wise Publisher without whose encouragementand friendship this book would not have occurred.
Secondly, special thanks go to Lorraine Rinaldi my Administrative Assist-ant for many years. Her energy, zeal and commitment to excellence in this project have been invaluable and always appreciated.
x

PART I
General complications


CHAPTER 1
Complications of thoracic incisions
Norman J Snow, Malek G Massad, Alexander S Geha
Introduction
The history of thoracic incisions dates to the Hippocratic era when trephina-tion of empyema cavities was first reported. Subsequent reports primarily docu-mented the use of incisional drainage of chest infections since intrapleuralsurgery was inevitably associated with respiratory failure due to open pneumo-thorax. Evolution of thoracic incisions evolved gradually until our avoidanceof intrapleural surgery was overcome by recognition of the safety of endo-tracheal intubation, positive pressure ventilation and the ability to operatesafely within the pleural cavity.
The choice of which incision to use is guided by such considerations as thesurface landmarks, a knowledge of intrathoracic anatomy and the relation-ships between the two. Incisions performed anteriorly are rarely useful foroperations on dorsal organs such as the bronchus, the esophagus or the aorta.Conversely anteriorly placed incisions are often appropriate for operations onthe anterior pulmonary hilum, the pericardium and the heart. The guidingprinciple regarding the choice of a thoracic incision should be the provision of adequate exposure necessary to accomplish the operation safely balancedby the approach which least disrupts the thoracic anatomy and least impairsthoracic function. Cosmetic considerations are important in certain situations.
Widely accepted surgical principles such as the use of Langer’s lines of ten-sion for placement of incisions, gentle handling of tissues, pinpoint hemostasiswhen employing electrocautery and precise anatomic closure are encouraged.
Sternotomy incisions
Median sternotomyThe road to the heart is only two or three centimeters in a direct line, but it has takensurgery nearly 2400 years to travel it [Hehrlein] [1].
The median vertical sternal approach was first suggested by Milton in 1897[2]. At the time when cardiac operations were performed through a transversebilateral thoracotomy, Shumaker reported use of the vertical sternotomy incision for pulmonary valvulotomy [3,4], and Blalock used it for the samelesion in some of his initial cases [5]. In 1956 Julian and coworkers from our
3
4 Chapter 1
institution described their initial experience for intracardiac proceduresrequiring hypothermia and inflow occlusion. A year later, they described its use in four patients with intracardiac lesions that required extracorporealcirculation and advocated its use for these purposes [5–7]. Julian et al. stressedthe importance of firm closure and the use of non-absorbable sutures [5].
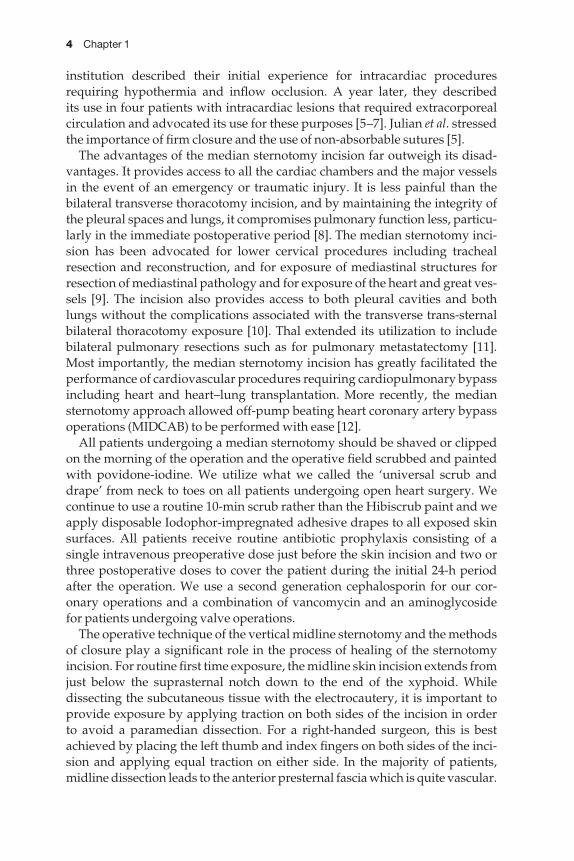
The advantages of the median sternotomy incision far outweigh its disad-vantages. It provides access to all the cardiac chambers and the major vesselsin the event of an emergency or traumatic injury. It is less painful than thebilateral transverse thoracotomy incision, and by maintaining the integrity ofthe pleural spaces and lungs, it compromises pulmonary function less, particu-larly in the immediate postoperative period [8]. The median sternotomy inci-sion has been advocated for lower cervical procedures including trachealresection and reconstruction, and for exposure of mediastinal structures forresection of mediastinal pathology and for exposure of the heart and great ves-sels [9]. The incision also provides access to both pleural cavities and bothlungs without the complications associated with the transverse trans-sternalbilateral thoracotomy exposure [10]. Thal extended its utilization to includebilateral pulmonary resections such as for pulmonary metastatectomy [11].Most importantly, the median sternotomy incision has greatly facilitated theperformance of cardiovascular procedures requiring cardiopulmonary bypassincluding heart and heart–lung transplantation. More recently, the mediansternotomy approach allowed off-pump beating heart coronary artery bypassoperations (MIDCAB) to be performed with ease [12].
All patients undergoing a median sternotomy should be shaved or clippedon the morning of the operation and the operative field scrubbed and paintedwith povidone-iodine. We utilize what we called the ‘universal scrub anddrape’ from neck to toes on all patients undergoing open heart surgery. Wecontinue to use a routine 10-min scrub rather than the Hibiscrub paint and weapply disposable Iodophor-impregnated adhesive drapes to all exposed skinsurfaces. All patients receive routine antibiotic prophylaxis consisting of a single intravenous preoperative dose just before the skin incision and two orthree postoperative doses to cover the patient during the initial 24-h periodafter the operation. We use a second generation cephalosporin for our cor-onary operations and a combination of vancomycin and an aminoglycoside for patients undergoing valve operations.
The operative technique of the vertical midline sternotomy and the methodsof closure play a significant role in the process of healing of the sternotomyincision. For routine first time exposure, the midline skin incision extends fromjust below the suprasternal notch down to the end of the xyphoid. While dissecting the subcutaneous tissue with the electrocautery, it is important toprovide exposure by applying traction on both sides of the incision in order to avoid a paramedian dissection. For a right-handed surgeon, this is bestachieved by placing the left thumb and index fingers on both sides of the inci-sion and applying equal traction on either side. In the majority of patients,midline dissection leads to the anterior presternal fascia which is quite vascular.

Complications of thoracic incisions 5
Exposure of one of the edges of the pectoralis major muscle on either side alertsthe surgeon that the incision is deviating from the midline. In some patients,the pectoral muscles are well developed and enlarged so that the midline incision will inadvertently cut through them. As the anterior presternal fasciais exposed, the sternochondral junctions on both sides of the sternum are palp-ated with the left thumb and index fingers. Once the midline of the sternum isoutlined, the submanubrial and subxyphoid spaces are developed using bluntdissection with the fingertip. The incision is carried upward a short distanceunder the skin into the deep cervical fascia and the interclavicular ligamentformed by fibers of the superior sternoclavicular ligament from each side istransected. Venous plexuses near the suprasternal notch are identified andclipped or ligated. A constantly present venous plexus overlying the sterno-xyphoid junction is identified and cauterized. The sternotomy incision is thenperformed, using the oscillating Stryker saw for cutting the sternum. The cord-less battery-driven saw is practical and easy to handle without the fear of crosscontamination during connection and handling. Once the sternum is divided,bleeding from the sternal edges is controlled. Pinpoint hemostasis of the anterior presternal fascia is achieved with the electrocautery under visionwhereas the edges of the posterior sternal fascia on both sides are cauterizedthroughout the length of the sternum to assure control of all the bleeding sites.Bleeding from the bone marrow is controlled with bone-wax, although wehave found that rubbing the sternal marrow on both sides with Gel-foam provides good control of bleeding without the added risk of infection or othercomplications [13]. The thymus and pericardium are divided with the electro-cautery and the venous branches at the inferior border of the innominate veinare clipped or ligated. It is important to preserve the viability of the presternalsoft tissues to maintain maximum tissue viability between the skin and thesternum. Discriminatory use of the electrocautery also plays an important rolein minimizing the amount of burned tissue and decreasing the rate of infec-tions. Nishida and colleagues utilized the technique of pinpoint hemostasis onpresternal soft tissues on over 3000 patients who underwent a median ster-notomy and achieved a sternotomy wound infection rate as low as 0.16% [14].For spreading of the sternal edges and exposure of the anterior mediastinalstructures, it is advisable to use a sternal retractor with blades designed to distribute evenly the traction along the cut sternal edges rather than using theregular rib spreader [11]. The retractor should not be placed too high along thesternum to avoid injury to the innominate vein or the brachial plexus [11].When procedures require exposure of the posterior plate of one or both sternaledges such as during internal mammary artery harvest, the sternal edgesshould not be forcefully retracted upwards in order to avoid sternal and ribfractures or dislocations.
At the conclusion of the operation, the sternal edges are checked again forany bleeding source. In patients undergoing coronary bypass operations withthe internal mammary artery, the mammary artery bed is checked and anyactive bleeding is controlled. The sternum is re-approximated with six to eight
6 Chapter 1
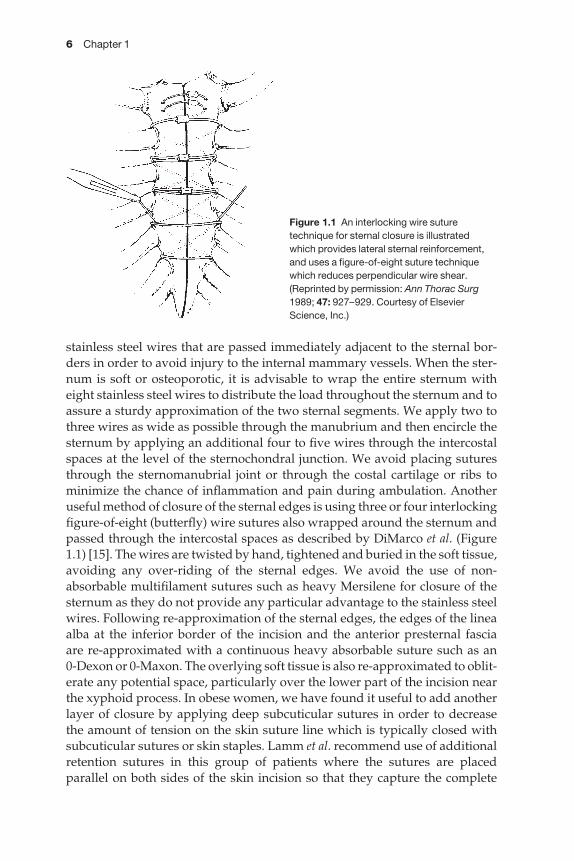
stainless steel wires that are passed immediately adjacent to the sternal bor-ders in order to avoid injury to the internal mammary vessels. When the ster-num is soft or osteoporotic, it is advisable to wrap the entire sternum witheight stainless steel wires to distribute the load throughout the sternum and toassure a sturdy approximation of the two sternal segments. We apply two tothree wires as wide as possible through the manubrium and then encircle thesternum by applying an additional four to five wires through the intercostalspaces at the level of the sternochondral junction. We avoid placing suturesthrough the sternomanubrial joint or through the costal cartilage or ribs tominimize the chance of inflammation and pain during ambulation. Anotheruseful method of closure of the sternal edges is using three or four interlockingfigure-of-eight (butterfly) wire sutures also wrapped around the sternum andpassed through the intercostal spaces as described by DiMarco et al. (Figure1.1) [15]. The wires are twisted by hand, tightened and buried in the soft tissue,avoiding any over-riding of the sternal edges. We avoid the use of non-absorbable multifilament sutures such as heavy Mersilene for closure of thesternum as they do not provide any particular advantage to the stainless steelwires. Following re-approximation of the sternal edges, the edges of the lineaalba at the inferior border of the incision and the anterior presternal fascia are re-approximated with a continuous heavy absorbable suture such as an 0-Dexon or 0-Maxon. The overlying soft tissue is also re-approximated to oblit-erate any potential space, particularly over the lower part of the incision nearthe xyphoid process. In obese women, we have found it useful to add anotherlayer of closure by applying deep subcuticular sutures in order to decrease the amount of tension on the skin suture line which is typically closed withsubcuticular sutures or skin staples. Lamm et al. recommend use of additionalretention sutures in this group of patients where the sutures are placed parallel on both sides of the skin incision so that they capture the complete
Figure 1.1 An interlocking wire suturetechnique for sternal closure is illustratedwhich provides lateral sternal reinforcement,and uses a figure-of-eight suture techniquewhich reduces perpendicular wire shear.(Reprinted by permission: Ann Thorac Surg1989; 47: 927–929. Courtesy of ElsevierScience, Inc.)

Complications of thoracic incisions 7
suprasternal tissue including fascia, subcutaneous fat, and skin [16]. This willplace the tension on the retention sutures that are then removed 1–2 weeksafter the operation.
All dressings are kept for 24 h after the operation and the patients areallowed to shower by the third or fourth postoperative day. In obese women orin women with large breasts, we recommend that they wear a supportivebrassiere or corset immediately after the operation in order to minimize lateraltension on the incision generated by pendulous breasts and to keep the lowerpart of the incision covered for the initial few days after the operation. Phys-ical therapy is initiated during the early postoperative period, commencingwith a range of motion exercises of both upper extremities. The patients areinstructed to avoid any extraneous activity or active exercises involving theupper extremities or shoulders, and to avoid lifting heavy objects for at least6–8 weeks from the time of their operation. Delayed healing of part or all of thesternum has been observed a year or more after the operation manifesting asan audible or palpable click on physical examination.
Sternal wound complications occur infrequently with an estimated incid-ence of 1–5% depending on the series [7,17,18]. When they do occur, they areassociated with a substantial morbidity and mortality. Minor complicationsinclude skin separation and superficial soft tissue seroma or infection withoutbone involvement. These usually respond to conservative treatment such asoral or intravenous antibiotics, local drainage and debridement and frequentwound care (Table 1.1). Once the infection clears and healthy granulation tis-sue starts forming, the wound may be closed secondarily. Major complicationsinclude sternal dehiscence, acute mediastinitis and sternal osteomyelitis. Theyusually require more extensive management including systemic antibiotics,wound and sternal debridement and tissue coverage of the wound. These can have grave consequences and are associated with a mortality of 5–27%depending on the series reported [7,17,18]. In a large series of patients under-going open heart procedures through median sternotomy, Breyer and associ-ates compared the incidence of minor and major sternal complications inpatients whose sternum was closed with wire and those whose sternum wasclosed with heavy Dacron sutures and found no difference. A theoretical con-cern is that eradication of a deep infection would be more difficult in presenceof the multifilament braided sutures. However, this was not shown to be true
Table 1.1 Guidelines for the surgical management of median sternotomy complications.
Median sternotomy complication Recommended treatment
Skin disruption, intact anterior presternal fascia Drainage, debridement, wound careIntact skin, sternal separation, no infection Sternal rewiring, Robicsek techniqueSkin disruption, sternal separation, no infection Sternal rewiring, continuous irrigationSternal dehiscence, mediastinitis Sternal debridement, muscle flap coverageChronic osteomyelitis of sternum Partial/ complete resection and local coverage
8 Chapter 1
in their series. Major complications occurred in 0.8% of the patients whose sternum was closed with wire and in 0.9% of those whose sternum was closedwith Dacron [17].
Many predisposing factors for sternal complications have been implicated.These can be classified into preoperative factors, intraoperative factors, andpostoperative factors [14,19]. Although it is difficult to control preoperativefactors such as diabetes, obesity, chronic obstructive lung disease, previouschest radiation, immunosuppressed state, renal failure or other comorbid con-ditions, the surgeon can have direct impact on the intraoperative factors suchas strict aseptic technique, precise midline osteotomy, selection of good clos-ure material, optimal hemostasis, prophylactic antibiotics, meticulous atraum-atic surgical technique and avoidance of prolonged operative time [14,20].Finally, certain factors or complications may arise in the postoperative periodand may lead to sternal instability or disruption such as external cardiac compression, mediastinal bleeding requiring re-exploration and prolongedmechanical ventilatory support.
Sternal dehiscence is associated with one or more of the following: anunusual amount of incisional pain, skin incision separation, serous or cloudydrainage through the separated sternal edges, a clicking sound upon move-ment of the upper trunk or upper extremities, and an otherwise unexplainedfever or leukocytosis. Physical examination often demonstrates a clickingsound that is elicited by exerting pressure on one of the two sternal edges orless frequently palpable separation of the sternal edges [7]. Early postoperativesternal instability may lead to skin separation, ingress of bacteria, and sub-sequent wound infection [21]. In extreme cases, paradoxical movement of the chest on deep inspiration may be visible to the examining physician. Thealmost uniformly painful unstable sternum has a cardiac tamponade and flailchest effect on the cardiac and respiratory functions [22]. These acutely illpatients can be retrieved from a progressive downhill course characterized bylow cardiac output, atelectasis, and progressive respiratory failure [22].
Based on the physical examination alone, it is sometimes difficult to deter-mine the extent of tissue and sternal involvement and radiographic examina-tion is helpful. An upright chest radiograph in the posteroanterior and lateralprojections or sternal views may show evidence of sternal overriding, separa-tion or fracture. A broken or loosened wire may also suggest a sternal problem.Identification of a vertically oriented midsternal lucency on plain radiographmay be the first clue to the diagnosis of sternal separation [23]. However, as many as 30% of patients may develop such a midsternal stripe followingmedian sternotomy without having sternal separation, and therefore its visualization does not necessarily indicate impending sternal dehiscence but rather warrants a careful clinical evaluation of the operative site [24].Computed axial tomography (CAT scan) of the chest may also show sternalseparation, a non-drained substernal fluid collection, or bone resorption suggestive of osteomyelitis. A white blood cell tagged nuclear scan may alsodemonstrate increased uptake in the sternum suggestive of osteomyelitis.
Complications of thoracic incisions 9
The diagnosis of sternal wound infection is often supported by bacteriologicassays with Gram stain and cultures. Staphylococcus aureus and S. epidermidisare the two principal offending microorganisms. Gram-negative organismsand enteric flora have been also cultured from sternal wounds, particularlyPseudomonas aeruginosa, Klebsiella, Serratia marcescens and enterobacter. Morerecently, we have been encountering resistant organisms such as methicillin-resistant S. aureus (MRSA) and vancomycin-resistant enterococcus (VRE).Systemic antibiotics are started empirically until the offending organism(s) are identified and the proper bacterial antibiotic sensitivity results becomeavailable.
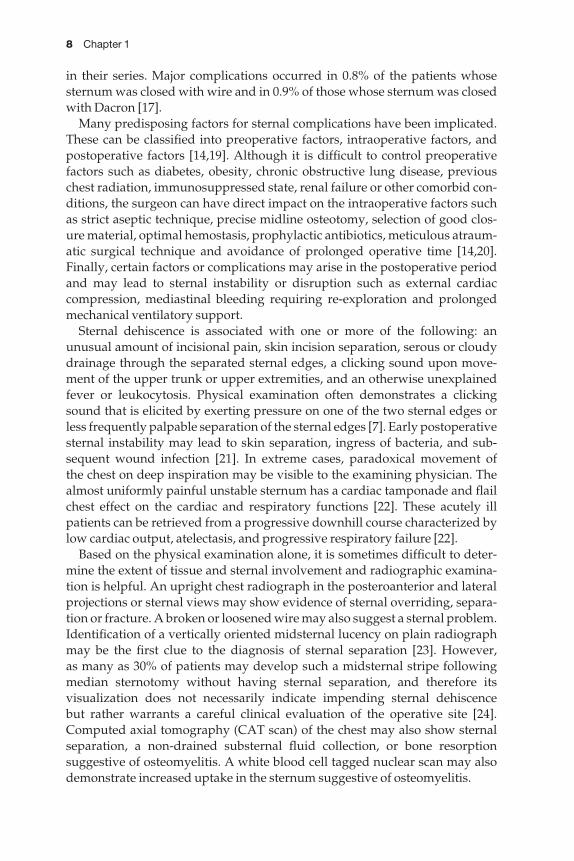
It has been our observation and that of others [7] that in almost everyinstance of sternal separation, the wires cut through a sternal edge. Once thesternal dehiscence is complicated by wound infection, important therapeuticprinciples include: mandatory wide drainage, debridement and coverage ofthe sternal wound, adequate ventilatory support and prolonged systemicantibiotic coverage. When dehiscence of the sternal closure is detected early,the sternum is still viable and the infection has not deepened into the medi-astinum, an attempt may be made at rewiring the sternum utilizing theRobicsek weaving technique (Figure 1.2) [25]. The chest incision is then closedafter thorough irrigation with antibiotic or a diluted povidone iodine contain-ing solution [26]. Continuous irrigation of the mediastinal space with anantibiotic solution through an irrigation suction system for a period of 3–5days has been advocated with satisfactory results [8,27–29]. However, whenthis conservative approach fails or when radical debridement makes primary
Figure 1.2 Conventional Robicsek sternalweave. (Reprinted by permission: J ThoracCardiovasc Surg 1977; 73: 267–268. Courtesyof Mosby, Inc.)

10 Chapter 1
closure of the wound impossible, then muscle flap coverage is indicated [30].In most instances, the actual sternal involvement is more severe than what isanticipated clinically. Signs of cartilage or bone resorption secondary to osteo-chondritis or acute osteomyelitis mandate removal of much, if not all of thesternum. We have found it useful to co-ordinate the operative care with theplastic surgeons beforehand in order to plan single-stage coverage [30–33].Several options are available for the surgical team for adequate coverage of theanterior mediastinal structures following sternal debridement or resection.These include pedicled and free myocutaneous flaps and omentum and arelisted in Table 1.2 [6,30,33–35].
Chronic osteomyelitis of the sternum is a very serious complication, particu-larly in patients with prosthetic valves. A prolonged course (4–6 weeks) ofintravenous antibiotics may bring the infection under control. However, it issometimes advisable to proceed with total or subtotal resection of the infectedsternum or sternal segment with excision of the cartilage of the adjacent ribs. Utilization of a muscle flap might be necessary to secure coverage of the exposed mediastinal structures. A chronic draining sinus or sinuses from a healed sternum have been observed several months following median sternotomy, some of which may be attributed to an underlying foreign bodysuch as an adjacent wire or suture. This may be associated with surroundingcellulitis and tissue inflammation. Treatment entails obtaining cultures fromthe draining site and administration of oral or intravenous antibiotics.Frequently, this condition requires local debridement of the sternal segmentalong with removal of the foreign body followed by local coverage.
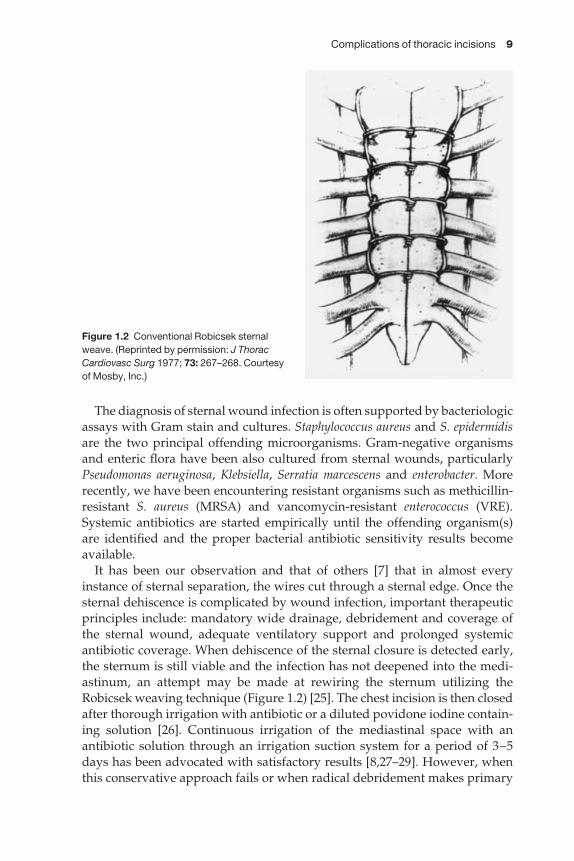
A rare complication is the occasional patient who presents weeks to monthsafter the operation with a partial separation of the sternum and a healed skin incision (Figure 1.3a). In these instances, Robicsek et al. recommend amodification of the sternal weaving closure technique in which the separatedpart of the sternum, often being the lower end, is exposed. An osteotomy ismade on one side of the sternum to realign the sternal segments and two weav-ing wires are passed along each of the two sternal borders in the area of sternalseparation. This allows easy approximation of the two halves, that are thenunited by three or four transverse wire sutures buttressed by this peristernalweave (Figure 1.3b). Detaching the sternal edges from the pectoralis majormuscles on either side and re-approximating them over the sternum will
Table 1.2 Available tissue transfer for coverage of anteriormediastinum following sternal debridement.
Left and/or right pectoralis major muscle or myocutaneous flapLeft and/or right rectus abdominis muscle or myocutaneous flapLeft or right latissimus dorsi muscle or myocutaneous flapFree muscle transfer (rectus abdominis, latissimus)OmentumSkin and soft tissue of anterior chest wall
Complications of thoracic incisions 11
provide adequate soft tissue coverage of the re-wired sternum for proper healing [36].
Incisional hernias develop in about 4% of patients undergoing operationsthrough median sternotomy [37]. These are usually located in the linea alba near the lower border of the xyphoid process. The main predisposing factors are wound infections, use of absorbable suture material, obesity andpulmonary complications. In one series, 35% of these hernias became symp-tomatic and required a later repair [37].
Median sternotomy complications also occur in children following openheart surgery. The same principles of management apply with some modifica-tions. In reconstructing sternotomy wounds in female patients, wide mobil-ization of the pectoralis major muscles is relatively contraindicated to preventdamage to the undeveloped breast buds [38]. Closure of the wound with limited mobilization only of the sternal edge of the adjacent pectoral cutaneoustissue or a rectus abdominus muscle or myocutaneous flap may be moreappropriate.
Figure 1.3 (a,b) Modified sternum weave applied in partial sternal separation. (a) Before repair. (b) After repair. (Reprinted by permission: J Thorac Cardiovasc Surg 1998; 116: 361–362. Courtesy of Mosby, Inc.)

12 Chapter 1
Redo sternotomyThe redo sternotomy or re-sternotomy incision is utilized for cardiac patho-logy that requires reoperative intervention. The need for this approach hasincreased over the past two decades since an increasing number of patients areundergoing a second (or third, fourth) coronary revascularization procedure.Reoperations are also utilized in patients with prosthetic valve complications,and in patients who have previously undergone a commissurotomy or valverepair and who return for valve replacement. The use of the re-sternotomyincision has also increased among infants and children who undergo cor-rective operations for congenital heart defects after they have been managedinitially with palliative procedures. The re-sternotomy incision is also utilizedto provide access to the in-patients with previous heart or heart–lung trans-plants who require re-transplantation. The re-sternotomy incision may also be utilized for debulking of previously resected retrosternal or mediastinaltumors. The approach also provides access to both pleural spaces and bothlungs and may be utilized for resection of recurrent benign and malignant pul-monary disease. At our center, about 15% of adult cardiac surgical proceduresand 25% of congenital cardiac procedures are performed through a previoussternotomy incision.
When a re-sternotomy is contemplated, attention should be given to aproper history and physical examination. It is important to obtain the previousoperative report which provides a ‘road map’ for the surgeon. If the previoussternotomy was for a coronary bypass or a valve operation, it is important to know whether the internal mammary artery or arteries were used. A planechest radiogram in the posteroanterior and lateral positions will identify theproximity of the heart to the sternum. It may also identify the course of theinternal mammary artery through previously applied clips at the dividedmammary branches. It will also provide information about the number of sternal wires and the technique of sternal closure; whether the previous ster-notomy incision was paramedian and required weaving wire(s) for closure orwhether figure-of-eight butterfly sutures have been placed.
In the operating room, it is advisable that percutaneous defibrillating padsbe placed in the event the patient develops ventricular tachycardia or fibrilla-tion and becomes unstable before dissecting the heart away from the sur-rounding pericardium and mediastinal structures. It is also advisable to have a guide wire placed in the common femoral artery prior to the sternotomy in order to access the femoral vessels for cannulation for cardiopulmonarybypass or for intra-aortic balloon pump placement if needed. The chest isentered through the previous sternotomy scar. Prior to initiating the ster-notomy, minimizing ventilation with high tidal volumes and positive-endexpiratory pressures serves to avoid displacement of the heart towards theoperative incision [38]. In most redo operations, the sternum is divided withthe use of an oscillating cast cutter or occasionally a Lebsche knife. Garrett andMathews have described the technique of retaining the sternotomy wires after untwisting to provide upward traction on the sternum and to limit the

Complications of thoracic incisions 13
depth of penetration of the oscillating saw [39]. We have found this technique helpful, particularly in second and third-time redo operations or in the elderlypatient with osteoporosis or a brittle sternum. The suprasternal area is dis-sected with the electrocautery to expose the manubrium over its most superiorportion. Dissection commences over the lower part of the incision to re-exposethe linea alba and xyphoid. With upward and lateral traction on the costal archand xyphoid, the retrosternal space is freed to a safe distance that will allowdivision of the lower end of the sternum with the oscillating saw. The anteriorperiosteal plate and spongiosa of the sternum are then divided with the oscil-lating saw starting from the lower sternal edge upwards. Once this is done, theposterior periosteum of the sternum is divided in a similar fashion starting atthe lower end of the sternum. After the retrosternal space is entered, upwardtraction is applied on either side of the sternal edges and with gentle down-ward countertraction with a sponge or forceps, the mediastinal tissues are dissected away from the sternum. The dissection is continued laterally on both sides of the sternal edges until about an inch or more of the costal margin is exposed. It is helpful to enter one or both pleural spaces, as that frees the mediastinal structures and facilitates the dissection. The sternal spreader is then placed. The heart and major vessels are then exposed in a systematicfashion starting at the diaphragm, the right atrium and aorta. It is advisable to delay total mobilization of the left side of the heart until cardiopulmonarybypass is instituted and occasionally until the heart is arrested to minimizebleeding and tearing of the epicardial surfaces.
The main complications relating to the redo sternotomy include major car-diac lacerations and injury to the native coronary vessels or to the previouslyimplanted coronary bypass grafts, intraoperative hemorrhage during bypasswith subsequent development of bleeding diathesis, and multiple sternal frac-tures with postoperative sternal instability. It is therefore important to inspectall the dissected surfaces for hemostasis prior to heparinization and again after reversal of heparin and before closure of the sternal incision. When thesternum is brittle or has one or more fractures or is off center we apply figure-of-eight wire sutures around the fracture or around the area where the incision is off center [8]. When the sternum is too thin and osteoporotic or when thesternotomy cut was paramedian rather than in the midline, vertical wires are woven in and out laterally alongside the sternal borders as described byRobicsek [25]. The encircling wires are then applied around the Robicsek wiresto decrease the amount of tension on the sternum and to minimize the chancethat the encircling wires cut through the thinned out sternum (Figure 1.2).
Bilateral submammary vertical sternotomy incisionOne disadvantage of the median sternotomy incision is the clearly visible ver-tical scar in the skin since the incision is at right angles to Langer’s lines [8].Moreover, and for unknown reasons, the sternal region is known for a highincidence of hypertrophied and keloid scars [8]. The bilateral submammaryskin incision in women and young females provides a nice alternative. With

14 Chapter 1
the patient supine, an anterior incision is made along the inferior skin creasesof both breasts and joined transversely. The skin and subcutaneous tissue flapsare raised to expose the sternum which is divided vertically. The main limitationof this exposure is the need for retraction of the subcutaneous tissues of the an-terior chest wall and both breasts in addition to the sternal spreader. The inci-sion may also require suction drains to be placed in the subcutaneous spaces toavoid hematomas. This incision provides an aesthetic scar that is not as appar-ent as the vertical scar and can be obscured by a brassiere or a swim suit top.
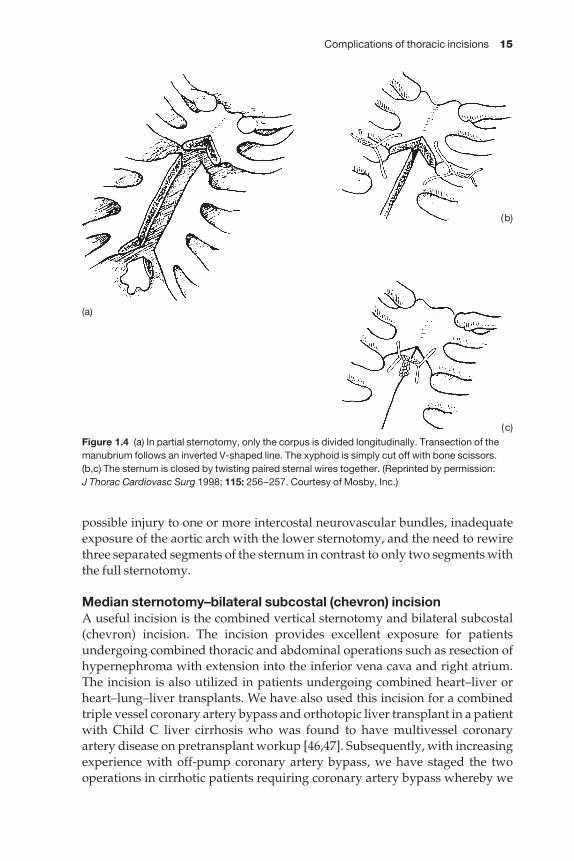
Partial sternotomyIn 1949, Holman and Willete reported on the use of the partial or incompletevertical sternotomy with transection of the sternum at the second intercostalspace for pericardiectomy [5,40]. The same approach was also applied forremoval of lesions of the anterior mediastinum, such as substernal thyroidadenoma, and for exposure of the trachea and upper thoracic esophagus[41,42]. The partial sternotomy incision may be modified to provide exposureof the anterior superior mediastinum, aorta and arch (partial upper ster-notomy or manubrial split) or to provide exposure of the heart through a par-tial lower sternotomy. To achieve this latter exposure, the lower sternum is split vertically up to the second intercostal space with bilateral transection of the sternum at the top of the incision [43,44]. A variety of operations may beperformed through this approach, including coronary bypass operations,resection of left ventricular aneurysms, valve operations, closure of atrial andventricular septal defects, resection of atrial myxomas and combined cardiacoperations [44,45]. A standard sternal retractor is inserted to spread the lowersternal edges. With the lower sternotomy, exposure of the aorta and the mostsuperior part of the operative field may be enhanced by lifting the intact uppersternomanubrial segment with a Rultrac retractor (Rultrac, Inc., Mentor, OH,USA) or a Favaloro Type retractor [44]. Sternal closure is usually done withstandard peristernal wires. An additional set of two vertical wires are appliedto approximate the upper and lower sternal segments. Alternatively, a figure-of-eight wire is placed around the transversely transected sternal segment forthe same purpose. Walterbusch recommends transecting the manubriumalong an inverted V-shaped line (Figure 1.4) [45]. This provides the advantageof cannulating the aorta near the pericardial fold superiorly, and prevents horizontal dislocation of the sternal coaptation.
The main advantage of the partial sternotomy is less postoperative paincompared with full sternotomy or anterolateral thoracotomy, particularlywith the lower sternotomy when the manubrium and both clavicular heads aswell as the attachments of the first and second ribs remain intact. Other potential advantages include decreased blood loss compared with completesternotomy and a shorter skin incision with a better aesthetic appearance of the scar. These advantages make the partial sternotomy a worthwhile altern-ative to complete sternotomy [43]. The main disadvantages of the partial sternotomy are the need to sacrifice one or both internal mammary arteries,
Complications of thoracic incisions 15
possible injury to one or more intercostal neurovascular bundles, inadequateexposure of the aortic arch with the lower sternotomy, and the need to rewirethree separated segments of the sternum in contrast to only two segments withthe full sternotomy.
Median sternotomy–bilateral subcostal (chevron) incisionA useful incision is the combined vertical sternotomy and bilateral subcostal(chevron) incision. The incision provides excellent exposure for patientsundergoing combined thoracic and abdominal operations such as resection ofhypernephroma with extension into the inferior vena cava and right atrium.The incision is also utilized in patients undergoing combined heart–liver orheart–lung–liver transplants. We have also used this incision for a combinedtriple vessel coronary artery bypass and orthotopic liver transplant in a patientwith Child C liver cirrhosis who was found to have multivessel coronaryartery disease on pretransplant workup [46,47]. Subsequently, with increasingexperience with off-pump coronary artery bypass, we have staged the twooperations in cirrhotic patients requiring coronary artery bypass whereby we
Figure 1.4 (a) In partial sternotomy, only the corpus is divided longitudinally. Transection of themanubrium follows an inverted V-shaped line. The xyphoid is simply cut off with bone scissors.(b,c) The sternum is closed by twisting paired sternal wires together. (Reprinted by permission: J Thorac Cardiovasc Surg 1998; 115: 256–257. Courtesy of Mosby, Inc.)
(a)
(b)
(c)

16 Chapter 1
perform the coronary bypass on a beating heart and follow that by the livertransplant at a separate setting.
The bilateral subcostal incision is made about one and a half inches belowthe costal margin. The incision is extended to the left side either halfway to themidclavicular line for exposure of the liver and upper midline abdominalstructures or all the way to the anterior axillary line for exposure of the entireupper abdomen. The incision is then extended as a midline vertical sternotomyto expose the anterior mediastinum and heart. Retraction is achieved by apply-ing a standard sternal spreader and an upper arm or Book–Walter retractor toexpose the abdominal organs. Wound closure entails standard closure of themedian sternotomy along with closure of the bilateral subcostal portion andre-approximation of the abdominal musculature. The retrosternal space isdrained through two chest tubes exteriorized through the upper abdominalwall. It is important to re-approximate the linea alba in the midline with heavynon-absorbable sutures and follow that with another layer to re-approximatethe anterior presternal fascia and soft tissue. The skin closure is completedwith surgical clips or inverted mattress nylon sutures. It is advisable to keepthe skin clips or sutures for 3–4 weeks to avoid skin separation and wounddehiscence, particularly in the immunosuppressed transplant patient.
Thoracotomy incisions
Posterolateral thoracotomyThe posterolateral thoracotomy is the standard approach to a variety ofintrathoracic operations such as pulmonary resection, esophageal surgery,aortic reconstruction and posterior mediastinal surgery. It offers wide expos-ure but requires division of large groups of chest wall muscles, including thelatissimus dorsi, occasionally the serratus anterior, trapezius, and rhomboids.
Prevention of complications begins with proper positioning of the patienton the operating table. Padding all exposed surfaces is mandatory. Thisincludes lateral malleolus, elbow, hip and knee. Neurological injury due to pressure-induced ischemia or necrosis is wholly preventable. We preferpadded cloth bolsters rather than the ‘bean bag’ because of concerns regardingthe prolonged exposure of vulnerable prominences to the rigid surface of thisdevice. There are no definitive data favoring one method over the other and itremains an issue of personal preference. Care must be taken to avoid hyperex-tension of the arm at the shoulder joint. Brachial plexus stretch injuries areoften disabling and can be avoided if proper positioning is utilized. An ‘air-plane device’ or cloth blankets are both suitable to support the ipsilateral arm ifattention is given to arm position and protection of exposed surfaces. Foampadding placed under the dependent arm and contiguous to body surfaceareas at risk is useful and effective. An axillary roll is placed under the thoraxboth to protect against brachial plexus injury and to elevate the thorax off thetable to permit adequate respiratory excursion of the dependent lung. Thismay be important with single lung ventilation. Postoperative examination is
Complications of thoracic incisions 17
routine to assess for cutaneous or neurological injuries, both to intervene earlyand to satisfy quality assurance concerns.
The technique of the incision may have consequences postoperatively.Meticulous hemostasis is most important, especially in this incision whichdivides large muscle masses. Use of the electrocautery is common and oneshould avoid the production of excess ‘char’ and necrotic tissue so as to min-imize the possibility of subsequent wound infection. Blood vessels may retractinto the muscle and later bleed, so patient and methodical cautery use is best.
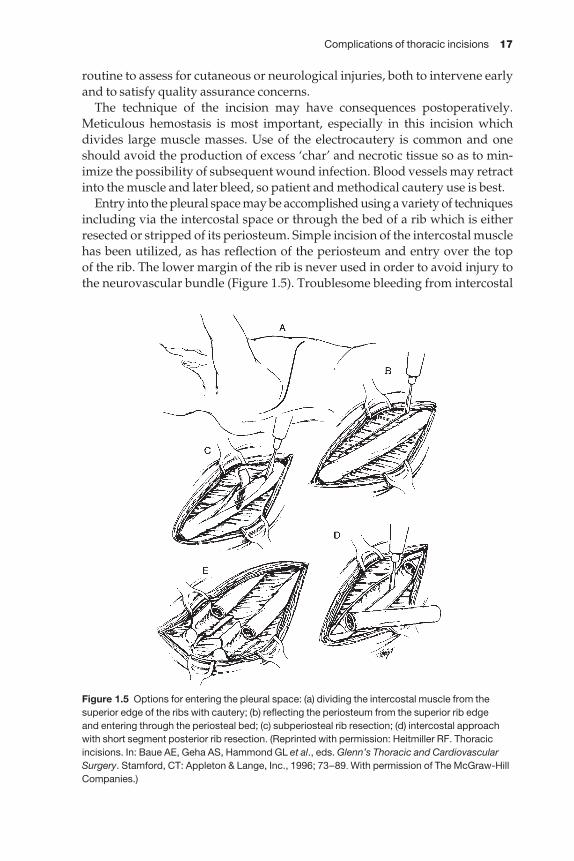
Entry into the pleural space may be accomplished using a variety of techniquesincluding via the intercostal space or through the bed of a rib which is eitherresected or stripped of its periosteum. Simple incision of the intercostal musclehas been utilized, as has reflection of the periosteum and entry over the top of the rib. The lower margin of the rib is never used in order to avoid injury tothe neurovascular bundle (Figure 1.5). Troublesome bleeding from intercostal
Figure 1.5 Options for entering the pleural space: (a) dividing the intercostal muscle from thesuperior edge of the ribs with cautery; (b) reflecting the periosteum from the superior rib edge and entering through the periosteal bed; (c) subperiosteal rib resection; (d) intercostal approachwith short segment posterior rib resection. (Reprinted with permission: Heitmiller RF. Thoracicincisions. In: Baue AE, Geha AS, Hammond GL et al., eds. Glenn’s Thoracic and CardiovascularSurgery. Stamford, CT: Appleton & Lange, Inc., 1996; 73–89. With permission of The McGraw-HillCompanies.)

18 Chapter 1
vessel injury and neurogenic pain (intercostal neuralgia) from intercostal nerveinjury may thus be prevented. Intercostal artery bleeding is not an uncommonsource of hemorrhage requiring reoperation after thoracotomy [48]. The bleed-ing may not be readily apparent due to impaired visibility, so placement of asponge inside the pleural cavity under the incision to assess for hemorrhage isuseful. Rib resection is seldom utilized unless fibrosis and adhesions limitentry into the chest or the rib is needed for a bone graft [49]. During reoperat-ive thoracotomy, rib removal offers increased exposure for safe dissection ofpleural adhesions and adherent lung. There is some evidence to suggest thatintercostal space entry results in less pain due to intercostal neuralgia than ribresection [50].
Excessive retraction of the ribs during thoracotomy predisposes to tearingand bleeding at the costo-vertebral angle. Division of the posterior rib withexcision of a 1 cm length will allow the rib to ‘hinge’ and avoid traction at theangle which probably causes the bleeding. This is not associated with measur-able morbidity and may actually reduce postoperative pain associated with arib fracture and painful respiratory motion at the fracture site.
The posterolateral thoracotomy has been associated with considerable post-operative pain and some disability. Division of the shoulder girdle muscula-ture results in at least transient muscle dysfunction. Significant neurologicalpathology has been seen after posterolateral thoracotomy in children resultingin shoulder asymmetry and electromyographic evidence of injury to nerves of the serratus and latissimus dorsi muscles. The deficits were seen more fre-quently in children operated upon within the first year of life. The higher theincision, the more frequent was the incidence of sequelae. Fortunately, mostwere not functionally significant but there is the potential for abnormal jointwear. The authors concluded that the incisions should be as low as possible to avoid denervating significant muscle mass and operations should be per-formed after the first year of life if possible [51]. Another report examining thesequelae of thoracotomy in children documented a surprising incidence ofbreast and pectoral maldevelopment after anterolateral thoracotomy [52].Placing the incision in the seventh intercostal space anteriorly, below the levelgenerally thought that breast migration might occur in adulthood, shouldavoid this complication, as will elevating the pectoralis muscle from the chestwall rather than incising and therefore denervating it.
Closure of the posterolateral thoracotomy, and indeed all thoracic incisions,should be as meticulous and as attentive to detail as the opening. Restorationof chest wall integrity and strength minimizes postoperative disability andpain. We prefer large no. 2 absorbable pericostal sutures. These are placedcarefully around the ribs so as to avoid the neurovascular bundle, since encir-clement of the bundle will aggravate intercostal neuralgia. We have not drilledthe sutures through the ribs. If there is a rib fracture, two choices are available:either excision of a short segment of rib to eliminate painful motion, or place-ment of pericostal sutures on either side of the fracture in a figure-of-eightfashion to tightly ‘splint’ and immobilize it. An anatomic layered closure is
Complications of thoracic incisions 19
preferred, both to strengthen the incision and to insulate against leakage offluid or air into the chest wall. We prefer subcuticular closure of the skin andnormally utilize a running technique. Monofilament absorbable sutures seemto incite less erythema and local cutaneous reaction than the braided suturewhich we previously employed. Daily inspection of the incision permits earlyrecognition of a wound infection and early intervention may limit the extent ofthis complication. Full-thickness infections and dehiscence of a thoracotomyare very rare, even when the thoracotomy is performed for drainage of infec-tions or resection of infected tissue.
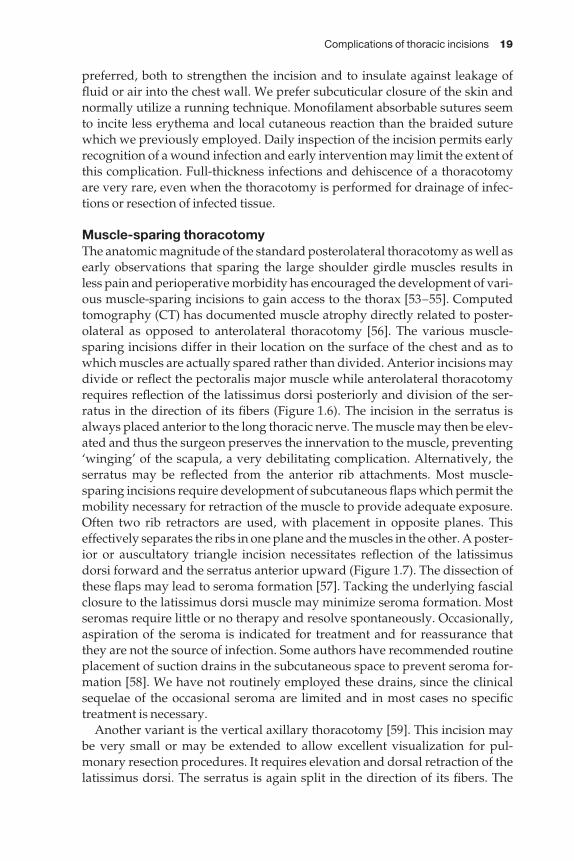
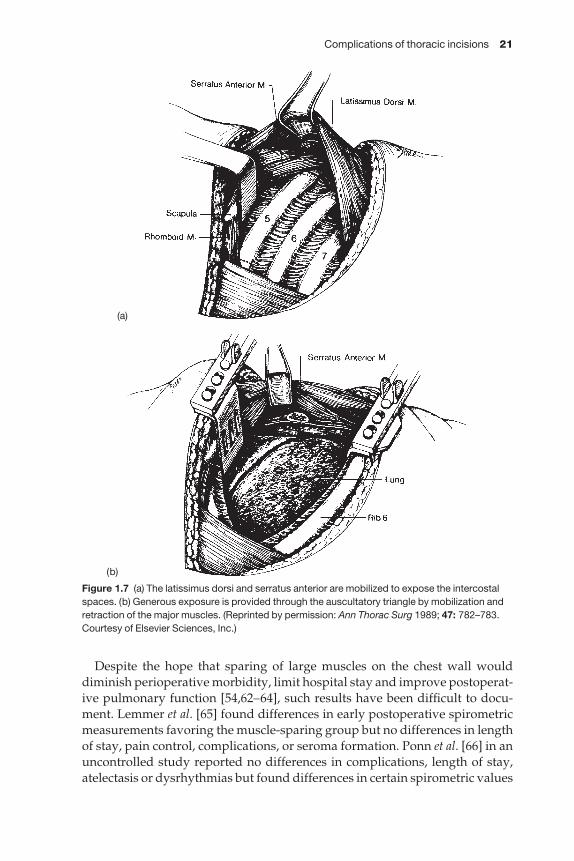
Muscle-sparing thoracotomyThe anatomic magnitude of the standard posterolateral thoracotomy as well asearly observations that sparing the large shoulder girdle muscles results in less pain and perioperative morbidity has encouraged the development of vari-ous muscle-sparing incisions to gain access to the thorax [53–55]. Computedtomography (CT) has documented muscle atrophy directly related to poster-olateral as opposed to anterolateral thoracotomy [56]. The various muscle-sparing incisions differ in their location on the surface of the chest and as towhich muscles are actually spared rather than divided. Anterior incisions maydivide or reflect the pectoralis major muscle while anterolateral thoracotomyrequires reflection of the latissimus dorsi posteriorly and division of the ser-ratus in the direction of its fibers (Figure 1.6). The incision in the serratus isalways placed anterior to the long thoracic nerve. The muscle may then be elev-ated and thus the surgeon preserves the innervation to the muscle, preventing‘winging’ of the scapula, a very debilitating complication. Alternatively, theserratus may be reflected from the anterior rib attachments. Most muscle-sparing incisions require development of subcutaneous flaps which permit themobility necessary for retraction of the muscle to provide adequate exposure.Often two rib retractors are used, with placement in opposite planes. Thiseffectively separates the ribs in one plane and the muscles in the other. A poster-ior or auscultatory triangle incision necessitates reflection of the latissimusdorsi forward and the serratus anterior upward (Figure 1.7). The dissection ofthese flaps may lead to seroma formation [57]. Tacking the underlying fascialclosure to the latissimus dorsi muscle may minimize seroma formation. Mostseromas require little or no therapy and resolve spontaneously. Occasionally,aspiration of the seroma is indicated for treatment and for reassurance thatthey are not the source of infection. Some authors have recommended routineplacement of suction drains in the subcutaneous space to prevent seroma for-mation [58]. We have not routinely employed these drains, since the clinicalsequelae of the occasional seroma are limited and in most cases no specifictreatment is necessary.
Another variant is the vertical axillary thoracotomy [59]. This incision maybe very small or may be extended to allow excellent visualization for pul-monary resection procedures. It requires elevation and dorsal retraction of thelatissimus dorsi. The serratus is again split in the direction of its fibers. The
20 Chapter 1
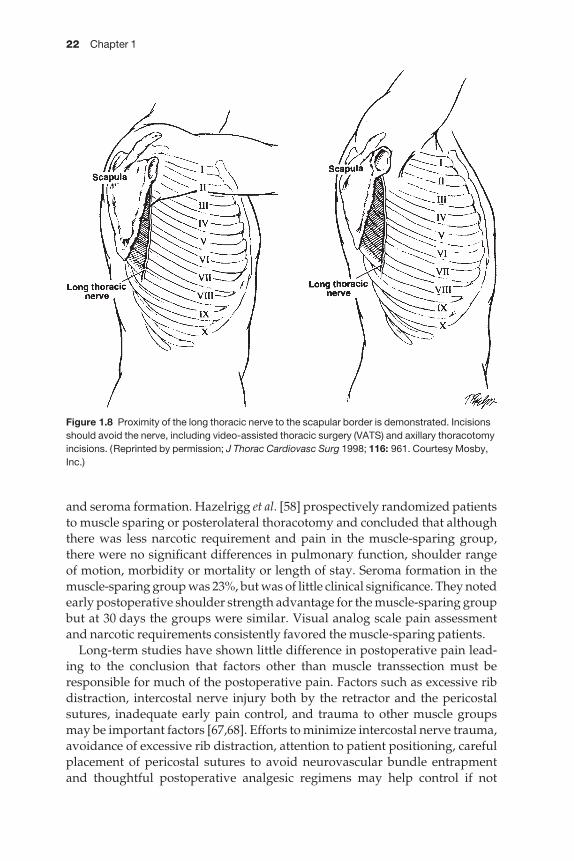
long thoracic nerve may be vulnerable to injury and a thorough knowledge ofits anatomy is necessary. The nerve is closest to the anterior border of thescapula at the level of the higher intercostal spaces. Therefore placement of cer-tain thoracic incisions must be carefully planned in order to avoid nerve injuryand subsequent winging of the scapula (Figure 1.8). If the serratus is to bedivided, it is mandatory to do so as low as possible. Division below the scapu-lar tip assures sufficient innervated and functional muscle mass to prevent theloss of scapular support. Winging of the scapula occurs when there is a loss ofserratus muscle tension which pulls the scapula downward and the counter-balancing muscles dominate. This results in outward and upward scapularrotation. Positioning the arm posteriorly moves the scapula dorsally, thus fur-ther exposing the long thoracic nerve to operative trauma. Salazar et al. havestudied the long thoracic nerve in cadavers and proposed guidelines to min-imize the potential for its injury [60].
Scapular winging, shoulder pain and inability to raise or rotate the shoulderforward result in significant morbidity, patient distress and prolonged disabil-ity [61]. Prevention is paramount.
Figure 1.6 (a) Dissection and mobilization of the latissimus dorsi muscle so it can be retractedrather than divided. (b) The serratus anterior has been divided in the direction of its fibers toexpose the intercostal space. (Reprinted by permission: J Thorac Cardiovasc Surg 1990; 99: 592.Courtesy of Mosby, Inc.)
(a)
(b)
Complications of thoracic incisions 21
Despite the hope that sparing of large muscles on the chest wall woulddiminish perioperative morbidity, limit hospital stay and improve postoperat-ive pulmonary function [54,62–64], such results have been difficult to docu-ment. Lemmer et al. [65] found differences in early postoperative spirometricmeasurements favoring the muscle-sparing group but no differences in lengthof stay, pain control, complications, or seroma formation. Ponn et al. [66] in anuncontrolled study reported no differences in complications, length of stay,atelectasis or dysrhythmias but found differences in certain spirometric values
Figure 1.7 (a) The latissimus dorsi and serratus anterior are mobilized to expose the intercostalspaces. (b) Generous exposure is provided through the auscultatory triangle by mobilization andretraction of the major muscles. (Reprinted by permission: Ann Thorac Surg 1989; 47: 782–783.Courtesy of Elsevier Sciences, Inc.)
(a)
(b)
22 Chapter 1
and seroma formation. Hazelrigg et al. [58] prospectively randomized patientsto muscle sparing or posterolateral thoracotomy and concluded that althoughthere was less narcotic requirement and pain in the muscle-sparing group,there were no significant differences in pulmonary function, shoulder range of motion, morbidity or mortality or length of stay. Seroma formation in themuscle-sparing group was 23%, but was of little clinical significance. They notedearly postoperative shoulder strength advantage for the muscle-sparing groupbut at 30 days the groups were similar. Visual analog scale pain assessmentand narcotic requirements consistently favored the muscle-sparing patients.
Long-term studies have shown little difference in postoperative pain lead-ing to the conclusion that factors other than muscle transsection must beresponsible for much of the postoperative pain. Factors such as excessive ribdistraction, intercostal nerve injury both by the retractor and the pericostalsutures, inadequate early pain control, and trauma to other muscle groupsmay be important factors [67,68]. Efforts to minimize intercostal nerve trauma,avoidance of excessive rib distraction, attention to patient positioning, carefulplacement of pericostal sutures to avoid neurovascular bundle entrapmentand thoughtful postoperative analgesic regimens may help control if not
Figure 1.8 Proximity of the long thoracic nerve to the scapular border is demonstrated. Incisionsshould avoid the nerve, including video-assisted thoracic surgery (VATS) and axillary thoracotomyincisions. (Reprinted by permission; J Thorac Cardiovasc Surg 1998; 116: 961. Courtesy Mosby,Inc.)
Complications of thoracic incisions 23
eliminate some of these common operative sequelae. Landreneau and col-leagues [69] have concluded that the principal advantage of muscle-sparingincisions is the preservation of the large muscle groups that may be used asrotational flaps for patients requiring tissue transfers to augment suture linesand to fill infected spaces. We currently employ muscle-sparing incisions as often as possible. Only rarely does concern for the adequacy of exposurecause us to convert from an anterolateral or auscultatory triangle muscle-sparing incision to a conventional incision with muscle division. All types ofpulmonary resections, decortications, mediastinal procedures and simplebiopsies are routinely accomplished with muscle-sparing techniques.
Thoracoabdominal incisionThe left thoracoabdominal incision has been utilized for many years whenexposure of the lower thorax and upper abdomen is required. The incision is performed by extending the intercostal incision, usually in the 7th or 8thinterspace, across the costal arch into the abdomen. The diaphragm is incisedradially to avoid damage to the phrenic nerve and resultant diaphragmaticdysfunction. The most frequent clinical scenario involves resection of the middle or lower esophagus and the proximal stomach. The advantages of thisincision include excellent exposure, the ability to operate upon varying lengthsof stomach or esophagus, and the fact that it affords a single position and inci-sion [70]. The major problem associated with this approach is the propensityfor infection at the level of costal arch transection. The infection presents witherythema, fluctuance and often a purulent draining sinus at the site. There may be systemic signs of infection including fever, leukocytosis and malaise.The cartilage derives its principal blood supply from the perichondrium, andsurgical disruption may render the cartilage segment ischemic and subject to infection, after which it behaves as a foreign body. The cartilage should be divided sharply, since overuse of the electrocautery will cause necrosis ofthe cartilage and further predispose it to infection. Superficial infections can be locally drained and treated with conventional techniques such as wet to dry saline dressing changes. However, deeper infections and those with aninfected sequestrum of cartilage must be surgically drained and the cartilageexcised. There is controversy regarding whether the entire costal arch must beexcised if the infection involves the 6th through 10th cartilages because of thecommon tissue involved [71,72]. In our experience, sequential debridement of individual sinus tracts is usually unsuccessful in eradicating the infectionwithin the costal arch. Wide total or subtotal excision of the arch with primaryclosure (with or without muscle flap coverage) is preferred. Suction drainageis usually employed after debridement. Prevention of this vexing problemmay be possible by employing several strategies, including appropriate use of perioperative prophylactic antibiotics (short course, intravenously adminis-tered beginning within 1 h of the incision). A precise anatomic closure shouldinclude secure restoration of the costal arch with absorbable suture which virtually eliminates the suture as a nidus for chronic infection. Excision of a
24 Chapter 1
short segment of the transected cartilage eliminates malunion and painfulmotion at the site as well as an ischemic sequestrum. A secure closure utilizingthe diaphragmatic sutures to close the abdominal and chest wall muscles helps to prevent herniation of abdominal viscera through a weakened area bydrawing the diaphragm up to the undersurface of the costal arch [70].
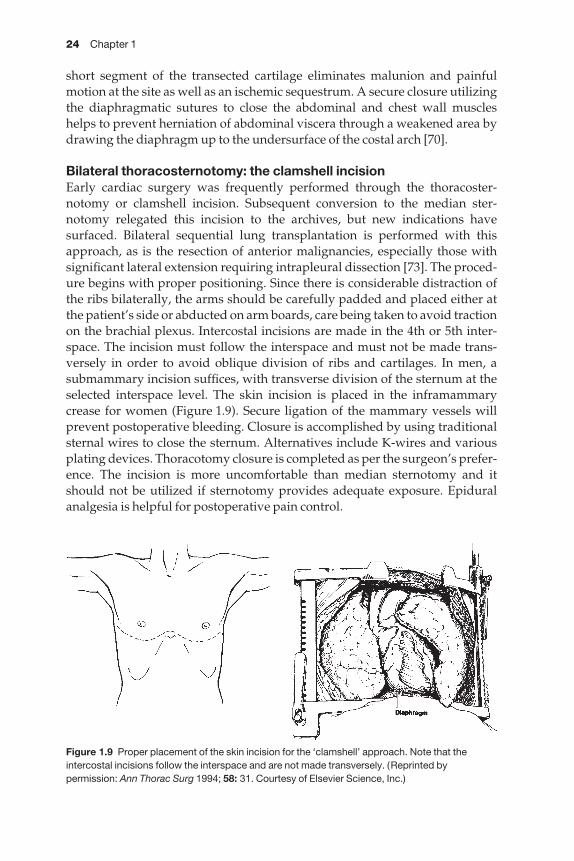
Bilateral thoracosternotomy: the clamshell incisionEarly cardiac surgery was frequently performed through the thoracoster-notomy or clamshell incision. Subsequent conversion to the median ster-notomy relegated this incision to the archives, but new indications havesurfaced. Bilateral sequential lung transplantation is performed with thisapproach, as is the resection of anterior malignancies, especially those withsignificant lateral extension requiring intrapleural dissection [73]. The proced-ure begins with proper positioning. Since there is considerable distraction ofthe ribs bilaterally, the arms should be carefully padded and placed either atthe patient’s side or abducted on arm boards, care being taken to avoid tractionon the brachial plexus. Intercostal incisions are made in the 4th or 5th inter-space. The incision must follow the interspace and must not be made trans-versely in order to avoid oblique division of ribs and cartilages. In men, asubmammary incision suffices, with transverse division of the sternum at theselected interspace level. The skin incision is placed in the inframammarycrease for women (Figure 1.9). Secure ligation of the mammary vessels willprevent postoperative bleeding. Closure is accomplished by using traditionalsternal wires to close the sternum. Alternatives include K-wires and variousplating devices. Thoracotomy closure is completed as per the surgeon’s prefer-ence. The incision is more uncomfortable than median sternotomy and itshould not be utilized if sternotomy provides adequate exposure. Epiduralanalgesia is helpful for postoperative pain control.
Figure 1.9 Proper placement of the skin incision for the ‘clamshell’ approach. Note that theintercostal incisions follow the interspace and are not made transversely. (Reprinted bypermission: Ann Thorac Surg 1994; 58: 31. Courtesy of Elsevier Science, Inc.)
Complications of thoracic incisions 25
Complications specific to this approach include mammary vessel hemor-rhage, and sternal overriding. The former is preventable by careful operativetechnique, and the latter has occurred rarely, but can be painful and cosmetic-ally unappealing. Secure wiring of the sternal bone should be all that is neededto avoid this complication, but some authors have favored placing K-wiresinto the sternum to eliminate the possibility [74].
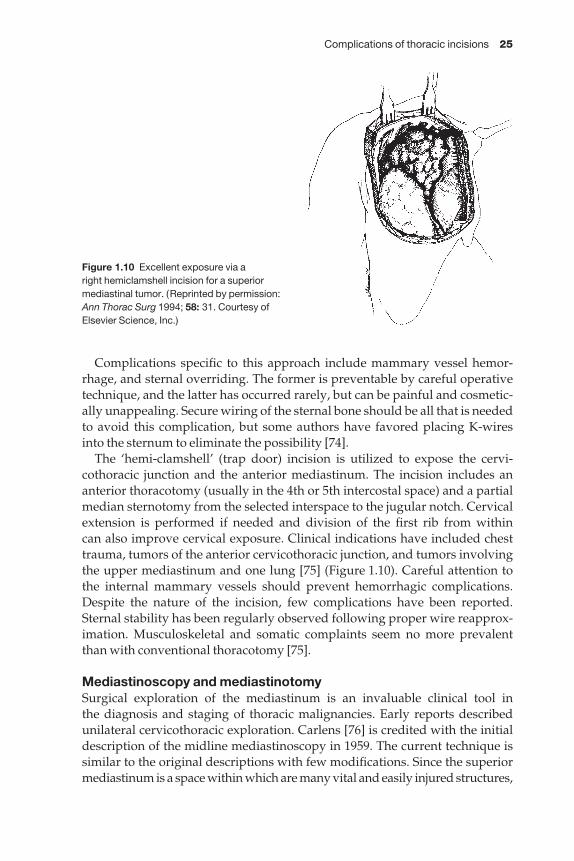
The ‘hemi-clamshell’ (trap door) incision is utilized to expose the cervi-cothoracic junction and the anterior mediastinum. The incision includes ananterior thoracotomy (usually in the 4th or 5th intercostal space) and a partialmedian sternotomy from the selected interspace to the jugular notch. Cervicalextension is performed if needed and division of the first rib from within can also improve cervical exposure. Clinical indications have included chesttrauma, tumors of the anterior cervicothoracic junction, and tumors involvingthe upper mediastinum and one lung [75] (Figure 1.10). Careful attention to the internal mammary vessels should prevent hemorrhagic complications.Despite the nature of the incision, few complications have been reported.Sternal stability has been regularly observed following proper wire reapprox-imation. Musculoskeletal and somatic complaints seem no more prevalentthan with conventional thoracotomy [75].
Mediastinoscopy and mediastinotomySurgical exploration of the mediastinum is an invaluable clinical tool in the diagnosis and staging of thoracic malignancies. Early reports describedunilateral cervicothoracic exploration. Carlens [76] is credited with the initialdescription of the midline mediastinoscopy in 1959. The current technique issimilar to the original descriptions with few modifications. Since the superiormediastinum is a space within which are many vital and easily injured structures,
Figure 1.10 Excellent exposure via a right hemiclamshell incision for a superiormediastinal tumor. (Reprinted by permission:Ann Thorac Surg 1994; 58: 31. Courtesy ofElsevier Science, Inc.)

26 Chapter 1
adequate training and experience, as well as surgical patience are necessary toavoid catastrophic complications. Mediastinoscopy is begun with a transverseincision just above the sternal notch. It proceeds in the avascular midline planeto the pretracheal space which is developed by blunt dissection. Injuries to thetrachea, pulmonary artery, azygous vein, bronchus, left recurrent laryngealnerve and even the aorta have been described. The overall complication rate is about 3%, with less than a 1% mortality rate. Serious complications with lasting sequelae are 0.5% or less. Thorough knowledge of the anatomy, suctiondissection of the lymph nodes so they appear in relief and consistent and aspiration prior to biopsy (to assess for bleeding potential) should preventcatastrophic complications. Although most problems are not caused by theincision per se, but by the operative adventure within, their occurrence is to beacknowledged and avoided.
The two most common incisional complications are wound infection and tumor seeding. Fortunately, both are quite rare. Wound infection occurs in approximately 0.1–0.15% of cases [77,78]. Mediastinal extension of the infection has been reported only sporadically. Our preference has been to closethe platysma with an absorbable 3–0 suture and to perform a running sub-cuticular skin closure. Most isolated mediastinoscopy procedures are todayperformed on an out-patient basis. When erythema and swelling occur, we advise warm compresses and oral antibiotics. Rarely does the incisionrequire open drainage but this can be safely accomplished with no significantside-effects.
Tumor implantation in the mediastinoscopy incision is exceedinglyunusual. An early analysis showed an incidence of 0.12% in over 6400 cases[79]. Neither cell type nor stage of disease seem to influence occurrence oftumor implantation. Both chemotherapy and radiation have been used to treatthis complication, but the numbers are too small to assess efficacy [80]. Bothdirect implantation secondary to tumor extraction and hematogenous deposi-tion in the wound have been implicated. In at least one case the medi-astinoscopy was actually negative although the patient had tumor in thesubcarinal fatty tissue. Due to the paucity of information it is not possible tostate how to avoid this complication.
The report of parasternal mediastinotomy by McNeill and Chamberlain [81]in 1966 was the first of many to demonstrate the utility of this incision to pro-vide access to the superior mediastinum. The procedure is performed throughthe second or third intercostal space, depending on the site of the target lesion.Generally the costal cartilage is removed and mediastinal entry occurs via thebed of the cartilage, which we prefer to excise since it leaves patients with little,if any morbidity or disability. Reassurance is offered that the small bulge withforced exhalation or Valsalva maneuver is of no consequence.
Extrapleural or intrapleural examination, either directly or with a medi-astinoscope, results in high diagnostic yields. If the lung is not biopsied orinjured, chest tubes are not required. Catheter aspiration of air, with a Valsalvamaneuver supplied by the anesthesiologist, evacuates the ambient air. Closure

Complications of thoracic incisions 27
is with absorbable suture to the pectoralis muscle, subcutaneous tissue andskin.
Most Chamberlain operations are performed as out-patient procedures.Admission is advised if there are complications, pneumothorax, or slow anes-thetic recovery [82]. As with mediastinoscopy, complications after mediastino-tomy are uncommon. Superficial wound infection has been reported in as highas 2.4% of cases. Local measures almost always suffice, particularly if there isno retained cartilage sequestrum. Other complications are hemorrhage, pneu-mothorax, and recurrent laryngeal nerve injury, but these are independent ofthe incision itself. There is essentially no mortality reported for this procedure.A postoperative upright chest X-ray should be performed to assess for pneu-mothorax and bleeding after both mediastinoscopy and mediastinotomy.
Thoracoscopy or video-assisted thoracic surgery incisionsVideo-assisted thoracic surgery (VATS) allows operative exposure via a smallcamera and monitor linkage so that only small incisions are required. Multipleports are placed so that operating instruments can be introduced into the pleural cavity. The ostensible advantages include shorter length of stay, fasterrecovery and return to work, less systemic inflammatory response, and lesspain and disability when compared with standard thoracotomy access. VATSdoes not depend upon an airtight seal as does laparoscopy. In fact, pneumoth-orax is necessary if the lung is to fall away from the chest wall to provide ade-quate exposure. The camera is usually inserted first, after which working portsmay be placed under direct vision for safety. These rigid instruments often fulcrum on the rib and periosteum and as such may be the source of consider-able postoperative pain, presumably because of their injury to the periosteum.Some studies have suggested that there is little difference between post-thoracotomy pain and pain following VATS [83,84]. One could speculate thatsmaller instrumentation might be less traumatic to insert and manipulate.Wound infections do occur in VATS incisions [85,86], as does port site implan-tation of metastasis [87]. Extraction within an endobag should virtually elim-inate the port site recurrence. All nodules with malignant potential should beremoved within the bag. Overall the complication rate is 4–5% followingVATS. Most are minor in nature [86]. An unexpectedly high rate of dehis-cences, hernias and wound infection has been associated with the anterior thoracotomy used for ‘minimally invasive’ coronary artery bypass grafting[88–90]. Wound ischemia due to internal mammary artery harvesting has been implicated as a cause. It may be that median sternotomy is preferable tominithoracotomy, whether the operation is conducted with or without theheart lung machine. We have occasionally noted subcutaneous emphysemaafter VATS. As these small incisions are sometimes difficult to close with precision, we have opted for a heavy 0-Vicryl closure of the chest wall muscles,usually placing them in a figure-of-eight fashion. Air-tight closure and ade-quate pleural drainage should prevent troublesome subcutaneous air in themajority of patients.
28 Chapter 1
Miscellaneous complicationsLung herniaHerniation of the lung through the intercostal space is an uncommon cause ofpost-thoracotomy pain. It is produced by chest wall trauma, either societal orsurgical. Loss of chest wall integrity may be due to the primary injury or dehis-cence of a thoracotomy. Interestingly, traumatic hernias rarely present early,perhaps due to muscle spasm and splinting of the area which mask the herniabulge. The hernias are often located anteriorly, since there is less chest wallmusculature in this location and because the interspaces are wider. It may bedifficult to distinguish pain secondary to lung hernia from intercostal neural-gia. The parietal pleura is innervated by the intercostal nerves and there isoverlap between the two syndromes [91]. Pain is located over a soft, spongyswelling on the chest wall which is maximally appreciated during forced exha-lation. Quiet breathing may mask the hernia and physical examination andradiography should be performed with a Valsalva maneuver (Figure 1.11).Plane radiography, especially tangentially across the swelling, or CT willdemonstrate the hernia, although physical examination is sufficient for clinicaldecision making [92]. Prevention is preferable to repair. Careful closure andavoidance of wound infection should diminish the incidence. Small (< 5 cm)defects which are asymptomatic or minimally so, may be managed safely non-operatively. Enlargement, persistent symptoms and large size are clinicallyproblematic and repair is usually indicated. Wound closure can be effectedusing local tissues such as rib struts, periosteal flaps, fascia or muscle. If this isnot possible, prostheses such as Gore-Tex or Marlex mesh may be implanted toobdurate the defect.
Figure 1.11 Subcutaneous air is seen withinan intercostal hernia in a patient taking steroidswho had undergone an anterior thoracotomyfor lung biopsy. (Reprinted by permission:Chest 1995; 107: 878. Courtesy AmericanCollege of Chest Physicians.)
Complications of thoracic incisions 29
Neurological sequelae of thoracotomyWhen neurological complications are seen after surgery on the thoracic aorta,spinal cord ischemia is thought to be the cause. However, non-aortic surgeryinvolving a posteriorly placed thoracotomy can also result in paraplegia [93],meningitis [94] and subarachnoid-pleural fistula with pneumocephalus [95].The principal causal factor is excessive traction with resultant bleeding at thecosto-vertebral junction. Attempts at control lead to disruptive dissection, useof cautery and packing. There have been reported instances of migration andswelling of topical oxidized cellulose resulting in a mass effect within the spinalcanal. Cautery-induced trauma, ligation of intercostal arteries and epiduralhematoma formation have also been implicated in the development of post-thoracotomy paraplegia. The incidence of paraplegia after thoracotomy at theUniversity of Maryland was 0.08% over a 40-year period [93]. Recognition ofpostoperative neurological damage must be made quickly to minimize per-manent sequelae. Routine neurological assessment in the recovery room orICU is mandatory. Since most thoracotomy patients are now extubated ‘early’if not in the operating room, opportunity exists for rapid diagnosis. Once thephysical examination confirms injury, urgent magnetic resonance imaging orCT scan is indicated, followed by timely consultation with the spine service. If indicated, operative intervention is immediately carried out. Despite all bestefforts, complete neurological reversal is seldom achieved.
The hazards of operating in the costo-vertebral recess must be appreciated if such misadventures are to be avoided. Excessive retraction and bleeding can be avoided in most instances by dividing the posterior rib and allowing itto hinge rather than tear at the costo-vertebral angle. Should bleeding occurdespite careful operative technique, then minimal topical hemostatic celluloseshould be applied and intercostal ligation should be avoided if at all possible.
Thoracic infection and antibioticsThe incidence of wound infection in thoracotomy incisions is low. A MayoClinic series [96] noted an infection rate of 1.6%. Factors influencing the incid-ence of thoracotomy infection include the length of surgery, immune status of the patient and the size of the infecting inoculum. Presence of prostheticmaterial and any devitalized tissue adversely affects the clinical course.Optimization of the patients’ nutrition and immune status as well as limitingthe surgical and perioperative factors are the goal of the surgeon. Several earlyobservations encouraged the routine use of prophylactic antibiotics andclaimed that such a practice was responsible for the low infection rate [97,98].More recent studies have shown that the routine use of properly administeredsystemic antibiotics prior to thoracotomy reduces the wound infection rate[99,100]. The timing of the antibiotic administration is important, since delayafter inoculation decreases the efficacy. We begin the intravenous antibioticinfusion in the operating room so we are assured that the drug has circulatedwithin 1 h of the thoracic incision. Some authors differentiate between woundinfection (well controlled with antibiotics) and other thoracic infections such

30 Chapter 1
as empyema or pneumonia. It may be that the two require different considera-tions, such as preoperative cultures or vigilance that infections elsewhere onthe patient are properly addressed. If there is endobronchial obstruction withdistal pneumonitis, we obtain preoperative sputum cultures and plan the peri-operative antibiotic regimen accordingly [101]. Short courses of antibiotics(one to four doses) are as effective as prolonged use [102] and may obviatesome of the sequelae such as Clostridium difficile colitis and antibiotic resist-ance. Our current protocol includes the preoperative treatment of any docu-mented infections (bronchitis, post obstructive pneumonia, skin infections),preoperative antibacterial soap for in-patients and out-patients as well asintravenously administered antibiotics (usually cefazolin) in the operatingroom and for 24–48 h postoperatively. Special consideration is accordedpatients submitted to esophageal resection, since their flora may be differ-ent and require coverage for upper aerodigestive tract organisms [103].Cephalosporins with anaerobic coverage are utilized, with or without con-comitant metronidazole. Body hair is clipped immediately prior to the operation. A betadine skin preparation is used in surgery, and dressings aremaintained for 48 h in the ICU or recovery area. There is a tendency for person-nel to neglect to scrutinize the wound if the wound dressing is connected to thechest tube dressing and the two dressings should be separated. With thoracicwound infections there may be erythema, swelling, pain and drainage.Intraoperatively, efforts are made to avoid or contain spillage of contaminatedmaterial. We routinely utilize antibiotic irrigation prior to closure, although nostudies have found this to be necessary.
Drainage of an infected area and application of wet to dry dressings usuallysuffice for superficial wound infections. Deeper infections require mechanicaldebridement of all necrotic tissue and excision of infected bone or cartilage.Healing by secondary intention or secondary wound closure are both satisfact-ory when the wound is clean. Dehiscence of a thoracotomy incision may becaused by local infection, inadequate surgical technique or compromise of thepatient’s ability to heal [104]. Recognition is facilitated by careful observationwith notation of a widening of the intercostal spaces, often made worse bycoughing. There may be a fluid wave or subcutaneous air beneath the incision.Respiratory insufficiency may ensue in patients with marginal respiratory sta-tus. Unless there is frank necrosis or infection, thoracotomy wounds whichbreak down are usually closed primarily after debridement and cleansing.
Occasionally open packing is necessary. Monofilament absorbable suturesare used to prevent chronic infections from the sutures themselves.Satisfactory healing of a thoracotomy dehiscence can be expected followingsurgical repair.
References
1 Hehrlein FW, Herrmann H, Kraus J. Complications of median sternotomy in cardiovas-cular surgery. J Cardiovasc Surg (Torino) 1972; 13: 390–393.
Complications of thoracic incisions 31
2 Milton H. Mediastinal surgery. Lancet 1897; 1: 872–875.3 Shumaker HB, Lurie PR. Pulmonary valvulotomy. J Thorac Surg 1953; 25: 173–186.4 Julian OC, Dye WS, Grove WJ et al. Hypothermia in open heart surgery. Arch Surg 1956;
73: 493–502.5 Julian OC, Lopez-Belio M, Dye WS et al. The median sternal incision in intracardiac
surgery with extracorporeal circulation: a general evaluation of its use in heart surgery.Surgery 1957; 42: 753–761.
6 Brown AH, Braimbridge MV, Panagopoulos P et al. The complications of median ster-notomy. J Thorac Cardiovasc Surg 1969; 58: 189–197.
7 Stoney WS, Alford WC Jr, Burrus GR et al. Median sternotomy dehiscence. Ann ThoracSurg 1978; 26: 421–426.
8 Ochsner JL, Mills NL, Woolverton WC. Disruption and infection of the median ster-notomy incision. J Cardiovasc Surg (Torino) 1972; 13: 394–399.
9 Grillo HC. Surgical treatment of postintubation tracheal injuries. J Thorac Cardiovasc Surg1979; 78: 860–875.
10 Falor WH, Traylor R. Extended indication for the median sternotomy incision. Am Surg1982; 48: 582–583.
11 Heitmiller RF. Thoracic incisions. In: Baue AE, Geha AS, Hammond GL, Laks H,Naunheim KS, eds. Glenn’s Thoracic and Cardiovascular Surgery, 6th edn. Stamford, CT:Appleton & Lange, Inc., 1996; 73–89.
12 Oz MC, Argenziano M, Rose EA. What is ‘minimally invasive’ coronary bypass sur-gery? Experience with a variety of surgical revascularization procedures for single vesseldisease. Chest 1997; 112: 1409–1416.
13 Robicsek F, Masters TN, Littman L et al. The embolization of bone wax from sternotomyincisions. Ann Thorac Surg 1981; 31: 357–359.
14 Nishida H, Grooters RK, Soltanzadeh H et al. Discriminate use of electrocautery on themedian sternotomy incision: a 0.16% wound infection rate. J Thorac Cardiovasc Surg 1991;101: 488–494.
15 DiMarco RF Jr, Lee MW, Bekoe S et al. Interlocking figure-of-eight closure of the sternum.Ann Thorac Surg 1989; 47: 927–929.
16 Lamm P, Godje OL, Lange T et al. Reduction of wound healing problems after mediansternotomy by use of retention sutures. Ann Thorac Surg 1998; 66: 2125–2126.
17 Breyer RH, Mills SA, Hudspeth AS et al. A prospective study of sternal wound complica-tions. Ann Thorac Surg 1984; 37: 412–416.
18 Serry C, Bleck PC, Javid H et al. Sternal wound complications: management and results. J Thorac Cardiovasc Surg 1982; 80: 861.
19 Kontos GJ Jr, Starr MG, Orszulak TA. Etiology of mediastinal infection after cardiacsurgery. In: Salem TJV, ed. Mediastinal and Sternal Infections. Cardiac Surgery: State of theArt Review. Philadelphia: Hanley and Belfus, Inc., 1988; 519–530.
20 Shafir R, Weiss J, Herman O et al. Faulty sternotomy and complications after median ster-notomy. J Thorac Cardiovasc Surg 1988; 96: 310–313.
21 Demmy TL, Park SB, Liebler GA et al. Recent experience with major sternal wound com-plications. Ann Thorac Surg 1990; 49: 458–462.
22 Sommerhaug RG, Wolfe SF, Red DA et al. Infected median sternotomy wounds. AnnThorac Surg 1987; 43: 461 (letter).
23 Adams GW, Ravin CE. Midline lucency following median sternotomy. Chest 1983; 83:793–794.
24 Escovitz ES, Okulski TA, Lapaywker MS. The midsternal stripe: a sign of dehiscence fol-lowing median sternotomy. Radiology 1976; 121: 521–524.
32 Chapter 1
25 Robicsek F, Cook JW, Rizzoni W. Sternoplasty for incomplete sternum separation. J Thorac Cardiovasc Surg 1998; 116: 361–362.
26 Angelini GD, Lamarra M, Azzu AA et al. Wound infection following early repeat ster-notomy for postoperative bleeding. An experience utilizing intraoperative irrigationwith povidone iodine. J Cardiovasc Surg (Torino) 1990; 31: 793–795.
27 Grossi EA, Culliford AT, Krieger KH et al. A survey of major infectious complications ofmedian sternotomy: a review of 7,949 consecutive operative procedures. Ann Thorac Surg1985; 40: 214–223.
28 Wong PS, Youhana A, Magee PG et al. Primary closure of infected sternum. Ann ThoracSurg 1993; 56: 1005–1006.
29 Bryant LR, Spencer FC, Trinkle JK. Treatment of median sternotomy infection by medi-astinal irrigation with an antibiotic solution. Ann Surg 1969; 169: 914–920.
30 Cohen M, Silverman NA, Goldfaden DM et al. Reconstruction of infected median ster-notomy wounds. Arch Surg 1987; 122: 323–327.
31 Miller JI, Nahai F. Repair of the dehisced median sternotomy incision. Surg Clin NorthAm 1989; 69: 1091–1102.
32 Pearl SN, Dibbell DG. Reconstruction after median sternotomy infection. Surg GynecolObstet 1984; 159: 47–52.
33 Weinzweig N, Yetman R. Transposition of the greater omentum for recalcitrant mediansternotomy wound infections. Ann Plast Surg 1995; 34: 471–477.
34 Tizian C, Borst HG, Berger A. Treatment of total sternal necrosis using the latissimusdorsi muscle flap. Plast Reconstr Surg 1985; 76: 703–707.
35 Trotter MC, Ilabaca PA, Economides NG et al. Muscle flaps for repair of dehisced orinfected sternotomy wounds. J Tenn Med Assoc 1994; 87: 511–513.
36 Robicsek F, Cook JW, Rizzoni W. Sternoplasty for incomplete sternum separation. J Thorac Cardiovasc Surg 1998; 116: 361–362.
37 Davidson BR, Bailey JS. Incisional herniae following median sternotomy incisions: theirincidence and etiology. Br J Surg 1986; 73: 995–996.
38 Stahl RS, Kopf G. Sternotomy infections in infants. Ann Thorac Surg 1990; 50920: 337 (letter).
39 Garrett HE Jr, Mathews J. Reoperative median sternotomy. Ann Thorac Surg 1989; 48: 305.40 Holman E, Willete F. The surgical correction of constrictive pericarditis. Surg Gyncol
Obstet 1949; 89: 129–144.41 Orringer MB. Partial median sternotomy: anterior approach to the upper thoracic eso-
phagus. J Thorac Cardiovasc Surg 1984; 87: 124–129.42 Gitter R, Daniel TM, Kesser BW et al. Membranous tracheobronchial injury repaired with
gastric serosal patch. Ann Thorac Surg 1999; 67: 1159–1160.43 Zwart H. Partial sternotomy: a mini approach for a maxi exposure. J Thorac Cardiovasc
Surg 1997; 114: 686 (letter).44 Moreno-Cabral. Mini-T sternotomy for cardiac operations. J Thorac Cardiovasc Surg 1997;
113: 810–811 (letter).45 Walterbusch G. Partial sternotomy for cardiac operations. J Thorac Cardiovasc Surg 1998;
115: 256–257 (letter).46 Massad M, Benedetti E, Pollak R et al. Combined coronary bypass and orthotopic liver
transplantation: technical considerations. Ann Thorac Surg 1998; 65: 1130–1132.47 Benedetti E, Massad M, Chami Y, Wiley T, Layden M. Is the presence of surgically treat-
able coronary artery disease a contraindication to liver transplantation. Clin Transplant1999; 13 (Part 1): 59–61.
48 Sirbu H, Busch T, Aleksic I et al. Chest re-exploration for complication after lung surgery.Thoracic Cardiovascular Surg 1999; 47: 73–76.
Complications of thoracic incisions 33
49 Kittle CF. Which way in? The thoracotomy incision. Ann Thorac Surg 1988; 45: 234.50 Weinberg JA, Krause AR. Intercostal incisions in transpleural operations. J Thorac Surg
1950; 19: 769–778.51 Emmel M, Ulbach P, Herse B et al. Neurogenic lesions after posterolateral thoracotomy in
young children. Thorac Cardiovasc Surg 1996; 44: 86–91.52 Cherup L, Siewers R, Futrell J. Breast and pectoral muscle maldevelopment after antero-
lateral and posterolateral thoracotomies in children. Ann Thorac Surg 1986; 41: 492–497.53 Bethancourt DM, Holmes EC. Muscle sparing thoracotomy. Ann Thorac Surg 1988; 45:
337–339.54 Horowitz MD, Ancalmo N, Ochsner JL. Thoracotomy through the auscultatory triangle.
Ann Thorac Surg 1989; 47: 780–781.55 Noirclerc M, Dor V, Chauvin G et al. Extensive thoracotomy without muscle section. Ann
Chir Cardiovasc 1973; 12: 181–184.56 Frola C, Serrano J, Cantoni S et al. CT findings of atrophy of chest wall muscle after thora-
cotomy: relationship between muscles involved and type of surgery. Am J Roentgenol1995; 164: 599–601.
57 Mitchell RL. The lateral limited thoracotomy incision: standard for pulmonary opera-tions. J Thor Cardiovasc Surg 1990; 99: 590–596.
58 Hazelrigg S, Landrenau R, Boley J et al. The effect of muscle-sparing versus standard pos-terolateral thoracotomy on pulmonary function, muscle strength and postoperativepain. J Thorac Cardiovasc Surg 1991; 101: 394–401.
59 Fry W, Kehoe T, McGee J. Axillary thoracotomy. Amer Surgeon 1990; 460–463.60 Salazar J, Ditz J, Tseng E et al. Relationship of the long thoracic nerve to the scapulan tip:
an aid to prevention of proximal nerve injury. J Thorac Cardiovasc Surg 1998; 116: 960–964.61 Kauppila L, Vastamaki M. Latrogenic serratus anterior paralysis long-term outcome in
26 patients. Chest 1996; 109: 31–34.62 Van Raemdonck D, Coosemans W, Lerut T. Vertical axillary thoracotomy: a muscle spar-
ing approach for routine thoracic operations. Acta Chirurgie Belgica 1993; 93: 207–211.63 Siegel T, Steiger Z. Axillary thoracotomy. SGO 1982; 155: 725–727.64 Khan I, McManus K, McCraith A, McGuigan J. Muscle sparing thoracotomy: a bio-
mechanical analysis confirms preservation of muscle strength but no improvement inwound discomfort. Eur J Cardiothorac Surg 2000; 18: 656–661.
65 Lemmer J, Gomez M, Symreng T et al. Limited lateral thoracotomy. Arch Surg 1990; 125:873–877.
66 Ponn R, Ferneini A, D’Agostino R et al. Comparison of late pulmonary function after posterolateral and muscle-sparing thoracotomy. Ann Thorac Surg 1992; 53: 675–679.
67 Ashour M. Modified muscle-sparing posterolateral thoracotomy. Thorax 1990; 45:935–938.
68 Benedetti F, Vighetti S, Ricco C et al. Physiologic assessment of nerve impairment in pos-terolateral and muscle-sparing thoracotomy. J Thorac Cardiovasc Surg 1998; 115: 841–847.
69 Landrenau R, Pigula F, Luketich R et al. Acute and chronic morbidity differencesbetween muscle-sparing and standard lateral thoracotomies. J Thorac Cardiovasc Surg1996; 112: 1346–1350.
70 Heitmiller R. Results of standard left thoracoabdominal esophagogastrectomy. SeminThorac Cardiovasc Surg 1992; 4: 314–319.
71 Talucci R, Webb W. Costal chondritis: the costal arch. Ann Thorac Surg 1983; 35: 318–321.72 McLaughlin J, Hankins J. Thoracic infections. In: Cordell RA, Ellison RG, eds. Complica-
tions of Intra Thoracic Surgery. Boston: Little Brown and Co., 1979; 335–345.73 Bains M, Ginsberg R, Jones W et al. The Clamshell incision: an improved approach to
bilateral pulmonary and mediastinal tumor. Ann Thorac Surg 1994; 58: 30–33.

34 Chapter 1
74 Wright C. Transverse sternothoracotomy. Chest Surg Clinics N America 1996; 6: 149–156.75 Lardinois D, Sippel M, Gugger M et al. Morbidity and validity of the hemiclamshell
approach for thoracic surgery. Eur J Cardiothorac Surg 1999; 16: 194–199.76 Carlens E. Mediastinoscopy. A method for inspection and tissue biopsy in the superior
mediastinum. Dis Chest 1959; 36: 343.77 Foster E, Munro D, Dobell A. Mediastinoscopy. Ann Thorac Surg 1972; 13: 273–286.78 Puhakka H. Complications of mediastinoscopy. J Laryngol Otol 1989; 103: 312–315.79 Ashbaugh D. Mediastinoscopy. Arch Surg 1970; 100: 568–573.80 Al-Sotyani M, Maziak D, Shamji F. Cervical mediastinoscopy: incisional metastasis. Ann
Thorac Surg 2000; 69: 1255–1257.81 McNeill T, Chamberlain J. Diagnostic anterior mediastinal exploration. Ann Thorac Surg
1966; 2: 532.82 Olak J. Parasternal mediastinotomy (Chamberlain procedure). Chest Surg Clin N America
1996; 6: 31–39.83 Furrer M, Rechsteiner R, Eigenmann C et al. Thoracotomy and thoracoscopy: postoper-
ative pulmonary function, pain and chest wall complaints. Eur J Cardiothorac Surg 1997;12: 82–87.
84 Hutter J, Miller K, Moritz E. Chronic sequelae after thoracoscopic procedures for benigndiseases. Eur J Cardiothor Surg 2000; 17: 687–690.
85 Yim A, Liv H. Complication and failures of video-assisted thoracic surgery: experiencefrom two centers in Asia. Ann Thorac Surg 1996; 61: 538–541.
86 Kaiser L, Bavaria J. Complications of thoracoscopy. Ann Thorac Surg 1993; 56: 796–798.87 Yim A. Port-site recurrence following video-assisted thoracoscopic surgery. Surg Endosc
1995; 9: 1133–1135.88 Pagni S, Salloum E, Tobin GR et al. Serious wound infections after minimally invasive
coronary bypass procedures. Ann Thorac Surg 1998; 66: 92–94.89 Hake U, Hilker M. Deep wound infection following minithoracotomy for coronary
bypass grafting. Ann Thorac Surg 1999; 67: 595.90 Ng P, Chua A, Swanson M. Anterior thoracotomy wound complications in minimally
invasive direct coronary bypass. Ann Thorac Surg 2000; 69: 1338–1340.91 DiMarco A, Oca O, Renston J. Lung herniation. A cause of chronic chest pain following
thoracotomy. Chest 1995; 107: 877–879.92 Minai O, Hammond G, Curtis A. Hernia of the lung: a case report and review of the liter-
ature. Connecticut Med 1997; 61: 77–81.93 Attar S, Hankins J, Turney S et al. Paraplegia after thoracotomy: Report of five cases and
review of the literature. Ann Thorac Surg 1995; 59: 1410–1416.94 Saldana R, Srikrishna S, Pais P et al. Pyogenic meningitis after posterolateral thoraco-
tomy. Ann Thorac Surg 1996; 62: 1573–1574.95 Brown W, Symbas P. Pneumocephalus complications, routine thoracotomy: symptoms,
diagnosis and management. Ann Thorac Surg 1995; 59: 234–236.96 Trastek V, Pairolero P, Allen M, Deschamps C. Unusual complications of pulmonary
resection. Chest Surg Clinc N America 1992; 2: 853–860.97 Bryant LR, Dillon M, Mobin-Uddin K. Prophylactic antibiotics in noncardiac thoracic
operations. Ann Thorac Surg 1975; 19: 670–676.98 Cooper D. Incidence of postoperative infection and the role of antibiotic prophylaxis in
pulmonary surgery: a review of 221 consecutive patients undergoing thoracotomy. Chest1981; 75: 154–160.
99 Aznar R, Mateu M, Miro JM et al. Antibiotic prophylaxis in non cardiac thoracic surgery:cefazolin v. placebo. Eur J Cardiothorac Surg 1991; 5: 515–518.

Complications of thoracic incisions 35
100 Kvale P, Ranga V, Kopacz M. Pulmonary resection. Southern Med J 1977; 70 (Suppl. I):64–68.
101 Ferdinand B, Shennib H. Postoperative pneumonia. Chest Surg Clin N Am 1998; 8:529–539.
102 Olak J, Jeyasingham K, Forrester-Wood C et al. Randomized trial of one-dose versus sixdose cefazolin prophylaxis in elective general thoracic surgery. Ann Thorac Surg 1991; 51:956–958.
103 Sharpe D, Renwick P, Matthews K, Moghissi K. Antibiotic prophylaxis in oesophagealsurgery. Eur J Cardiothorac Surg 1992; 6: 5561–5564.
104 Douglas J. Complications related to patient positioning, thoracic incisions and chest tubeplacement. In: Wolfe W, ed. Complications in Thoracic Surgery. St Louis: Mosby Year Book,1992; 76–87.
CHAPTER 2
Respiratory complications of thoracic operations
Hani Shennib
Postoperative atelectasis
The incidence of postoperative atelectasis or lung collapse varies from 6% to 76% based on the clinical and radiological criteria for assessment and on methods of surveillance [1–8] Plate-like atelectasis after thoracic surgery is quite frequent and usually associated with minimal clinical findings.However, in patients with borderline lung function atelectasis may lead to other serious sequela such as cardiac arrhythmia, pneumonia and respiratoryfailure. On the other hand, major collapse involving the whole lung or lobe can lead to significant shunt and decompensation.
Susceptibility to atelectasisThoracic surgical patients are particularly vulnerable to pulmonary atelectasisas they are subjected both to general anesthesia and a thoracotomy [9–17]. Lossof upper airway reflexes, endotracheal intubation and active lung collapse inthe course of many routine thoracic surgical procedures predispose to postop-erative atelectasis. Administration of narcotic analgesics and postoperativepain impair respiratory mechanics, and accentuate atelectasis. Furthermore,pneumo and hemothorax, which often develop in the absence of adequatepleural drainage, may contribute to postoperative lung collapse. Retention ofsecretions within the airway secondary to inability to cough, pain, loss of lungcompliance, and vocal cord dysfunction are all factors that would induce orcompound atelectasis. Certain procedures are associated with a major risk ofatelectasis and these include sleeve pulmonary resections, lung transplanta-tion, and major chest wall resections.
At a cellular level [14,15,17,18], atelectasis alters lung host defenses byimpairing mucociliary function, pulmonary macrophage phagocytic, bacteri-cidal and lymphocyte activity, thus impairing the lung host defenses andtherefore making the patient susceptible to pneumonia [19–23]. Intraoperat-ively, atelectasis may occur due to malpositioning of an endotracheal tube,inadequate suctioning of endotracheal secretions, inadvertent creation of con-tralateral pneumothorax from pleural holes, and from unexplained airwayreactivity. This may occur and progress intraoperatively and hence it is imper-ative that a chest radiograph be done on arrival to the recovery room. More
36

Respiratory complications of thoracic operations 37
important, however, is to have excellent rapport between the anesthesiologistand surgeon during the procedure to recognize ventilation difficulties encoun-tered during surgery. Any hypoxia or decrease in measured end-tidal carbondioxide should be investigated. Usually malpositioning of the endotrachealtubes can be avoided or corrected by the choice of the appropriate tube sizeand confirmation of its location by prompt bronchoscopy.
Atelectasis may not be apparent on the initial postoperative radiograph.Oxygen which is routinely administered postoperatively will accentuateatelectasis as it displaces normally inhaled nitrogen, resulting in diffusionatelectasis [24]. Atelectasis should be suspected when the chest radiographshows evidence of volume loss with increased opacification, diaphragmaticelevation and mediastinal shift. In patients with asthma and severe chronicobstructive pulmonary disease (COPD) it may take a longer time for hyper-inflated lung segments to collapse. This is also true for patients with major airway obstruction, and chest radiographs may not be the most sensitive wayto identify this. Surgeons must adopt a vigilant routine for assessing post-operative chest radiographs themselves, as often, radiologists are less familiarwith surgical techniques and may misinterpret postoperative images. Surgicaltechniques such as creation of a pleural tent or temporary diaphragmatic even-tration by phrenic nerve injection may be reported incorrectly by radiologistdue to lack of operative information. Radiologically, it may be difficult to dif-ferentiate between atelectasis, pneumonia, and pulmonary infarction [25–27].Shift of the mediastinum towards the atelectatic side helps differentiatebetween loss of lung volume and a pleural fluid collection which causes a contralateral shift. Clinical manifestations of atelectasis such as low-gradetemperature and mild elevation of the white blood cell count also appearequally with pneumonia.
Pulmonary infarction is notoriously misinterpreted and its associated lungconsolidation is usually interpreted as pneumonia and treated as such. Earlieron, it may manifest clinically and radiologically as atelectasis. Clipping or ligat-ure of segmental veins are often tolerated quite well. Inadvertent interruptionof lobar veins, on the other hand, due to technical error or when lobar torsionoccurs, results in full opacification of the lobe and will appear radiographic-ally as a rounded and well-demarcated consolidated lobe. Remarkably, a bronchoscopic examination is often inconclusive and mild indentation of the affected bronchus due to some rotation may be undetected. It is henceimportant to differentiate atelectasis early after surgery from other more serious pulmonary complications.
Management of atelectasis consists of anticipation, prevention and treat-ment [5,6,18,26,28–45]. It is important to identify those patients that are at high risk of atelectasis preoperatively. The obese, elderly, those with COPD,patients with restrictive chest wall or lung disease and those with head and necksurgery which affects the vocal cords, must be prepared and educated aboutpostoperative respiratory therapy protocols prior to surgery. Such educationand a physiotherapy program should be pursued vigorously in the postoperative
38 Chapter 2
period with specific therapeutic measures added for any underlying disease.For example, asthma and COPD patients may benefit from an intensified regimen of pre- and postoperative steroid and bronchodilator prophylaxis.
Postoperative optimization of analgesia, preferably by administration ofregional epidural analgesics, must be considered with all major operations.Patient-controlled intravenous analgesics are superior to uncontrolled intra-venous and subcutaneous analgesic administration. The negative effects ofoverdose, albeit less, will still lead to somnolence and reduction of overallpatient activity.
The main objective of postoperative physiotherapy is the incremental im-provement in overall cardiovascular and chest function. Incentive spirometrytechniques and other methods to improve respiratory mechanics are mosteffective in clearing the bronchopulmonary tree from secretions, expandingthe lung, and decreasing the risk of atelectasis. The administration of inhaledbronchodilators may improve the efficacy of clapping, vibration and otherchest physiotherapy techniques when given before surgery. The literature isfull of studies comparing the efficacy of one method of chest physiotherapywith another. Regardless, chest physiotherapy has been shown to minimizethe risk of postoperative atelectasis. The use of mucolytic agents remains con-troversial, but we do use it occasionally in patients with recurrent airwayobstruction due to thick inspissated secretions.
When atelectasis is established, aggressive chest physiotherapy should be continued. Incentive inspirometry is superior to the old blow bottles andcauses better expansion of collapsed lung segments by alveolar recruitment.Several European centres have experience with the use of non-invasivemechanical ventilators for the treatment of major atelectasis. Intermittent, positive pressure breathing by pressure-cycled ventilators pushes a deter-mined volume of air to a preset pressure. Contraindication for such a therapyincludes bullous emphysema, and massive or persistent air leak. Side-effectsof this ventilator modality such as abdominal distension and bloating have notbeen reported; however, controlled studies to substantiate the efficacy of thismethod are lacking. While some single-arm reports suggest a benefit in theincidence of pulmonary complication, one randomized study failed to showan advantage of intermittent positive pressure breathing over incentiveinspirometry for prevention of pulmonary complications following open heartsurgery. Caution should be exercised in subjecting patients who have had asleeve resection as disruption of a bronchial anastomosis may cause an airleak. The presence of major lobar atelectasis or atelectasis of lesser extent, inpatients with borderline lung function, warrants prompt use of fiberopticbronchoscopy for diagnosis and therapy. In addition to permitting anatomicinspection for possible technical problems, it may be possible to identify andremove major obstructions due to retained secretions. The performance ofdeep bronchial secretion sampling for culture and sensitivity will also help todetermine the need for administering antibiotics.
Respiratory complications of thoracic operations 39
In patients with compromised neurological status, the use of fiberopticbronchoscopy to clear airways of secretions, particularly following aggressivephysiotherapy, may be beneficial. Hypoxic patients require continuous oxy-gen monitoring and administration. Excessive utilization of suctioning in thecourse of fiberoptic bronchoscopy can lead to significant hypoxia. This can beremedied promptly by discontinuing the suctioning and if needed by purgingoxygen through the working channel of the bronchoscope.
On occasion, when retained secretions lead to repeat respiratory failure,prolonged endotracheal intubation and/or re-intubation, it is advisable toconsider performing tracheostomy to facilitate pulmonary toilet. Percutane-ous tracheostomy can be easily performed in the intensive care unit and hasbecome increasingly the technique of choice in some centres.
Postoperative pneumonia
This is one of the most common and potentially devastating of all postoperat-ive complications. It has the same risk factors described previously for otherpulmonary complications. In addition, its risk is higher following right asopposed to left pneumonectomy after extensive lung and chest wall resectionand with prolonged operative time and increased transfusion requirement[5–7,46–52].
The diagnosis and treatment of postoperative pneumonia are extremelydifficult [53–56], primarily because of the overlap in symptoms, hematologicaland radiological changes between atelectasis and pneumonia. Often it is over-or underdiagnosed. Delayed treatment of postoperative pneumonia may leadto rapid progression to respiratory failure and death. It is hence advocated thataggressive antibiotic therapy be promptly initiated whenever the classic triadof fever, elevated white blood count and a radiological infiltrate manifest. This becomes even more pertinent in the presence of progressive decline in gasexchange. In the absence of reliable bacterial culture results, it is advocated to commence antibiotics on empiric basis. Immediate deep sample Gram stains and bacterial cultures must be obtained by endotracheal suction or bronchoscopy. Initial antibiotic therapy should cover Haemophilus influenzae,Staphylococcus aureus, Streptococcus pneumoniae, Enterobacteriaceae includingKlebsiella pneumoniae, Escherichia coli and Pseudomonas eroginosa. The utilizationof ampicillin and an aminoglycoside or a third-generation cephalosporin arecurrently the golden standard.
While prevention of postoperative pneumonia has traditionally entailedadministration of prophylactic doses of antibiotics [57,58], current regimensfor thoracic surgery are outdated and rather reflect a general surgery practiceaimed at decreasing wound infections [8]. Currently used second-generationcephalosporins are less likely to be effective in preventing bronchopneumoniaor empyema. Wound infections in thoracic incisions on the other hand areunusual due to the excellent chest wall blood supply.
40 Chapter 2
Acute respiratory failure
Acute adult respiratory failure following a cardiothoracic procedure is definedas respiratory decompensation requiring intubation and mechanical ventila-tion any time after initial extubation or failure to discontinue mechanical ventilation within 48 h of completing surgery. While there is a variation in the overall incidence of pulmonary complications following cardiothoracicsurgery, the incidence of this serious respiratory complication ranges between5% and 14%. The significance of development of respiratory failure followingthoracic surgery is its associated mortality. Bush et al. reported that 14% of allpatients ultimately required tracheostomies and 8% died. Ginsberg reportedthat 40–70% of all postoperative deaths after lung resections were attributed to respiratory complications [10]. Bousamara reported that up to 10% ofpatients undergoing lung volume reduction surgery may require prolongedmechanical ventilation [59] and Markos also reported an incidence of 10% ofrespiratory failure in patients undergoing lung resection for lung cancer [60].Preoperative risk factors for pulmonary complications include smoking his-tory, sputum production, obesity, old age and impaired cardiopulmonaryfunction. Clearly, the patients overall and preoperative pulmonary functionalstatus will contribute to determining any added risk of mortality from re-spiratory failure. As we operate on older frail patients with boderline lungfunctions, mortality will probably increase.
Many factors contribute to the development of postoperative respiratoryfailure. Several insults occur routinely during surgery and may contribute to such injury: lung collapse during single lung ventilation, manipulation ofthe lung during dissection and positive pressure ventilation are contributorsand prime the lung for membrane leakage following surgery. Redistribution of lung perfusion following major resection, early postoperative mechanicalventilation, excessive intravenous fluid and blood administration, silent aspira-tion, medications and cardiac events may also contribute to the developmentof capillary leak in the early postoperative period. Despite early extubation,lung injury often progresses over a few days following operation so that aninjury may only manifest itself 48–72 h after. Frequently, this renders differen-tial diagnosis of the etiology (pneumonia, embolism, cardiogenic, etc.) morecomplex. Existing underlying cardiopulmonary disease renders diagnosis andmanagement of respiratory failure more difficult (e.g. pulmonary fibrosisorganizing pneumonia, aortic valve and coronary artery disease).
Moderate improvement in outcome of post-thoracotomy respiratory failurehas recently been reported due to advances in supportive care [61–83]. Newconcepts which may have contributed to such improvement include min-imization of inspired oxygen, avoiding hyperinflation, avoiding recruitment–rerecruitment, the use of airway pressure release ventilation, inverse ratio ventilation, permissive hypercapnea, better fluid management and intermit-tent utility of the prone position. The administration of antibiotics, antifungals,steroids, anti-inflammatory agents and surfactant have not shown convincing
Respiratory complications of thoracic operations 41
benefits. Inhaled nitric oxide, on the other hand, has been shown to lead toimprovement in hemodynamics and gas exchange.
Post-pneumonectomy pulmonary edema
This is the most dreaded and poorly understood complication following pneu-monectomy. Flooding of the remaining lung with edematous transudatebrings immediate respiratory failure and a mortality that is higher than 80%.Fortunately, it only occurs in less than 5% of all pneumonectomy patients [84]. It was originally described by Gibbon [85] in the early 1940s but onlyrecently has it been recognized as a distinct entity. While originally it wasassumed to be secondary to fluid overload, today it is thought to be of multi-factorial etiology and probably related to some direct form of pulmonary vas-cular endothelial injury from increased capillary pressure and flow throughthe remaining lung. Progressive baro-trauma from mechanical ventilation inthe course of supportive therapy accentuates this alveolar–capillary damage[86].
In an attempt to identify risk factors for post-pneumonectomy pulmonaryedema Delaurier [84] et al. reviewed the course of 291 pneumonectomy cases and identified 13 patients who developed post-pneumonectomy edema following right pneumonectomy. The extent of surgery and duration of theoperation were noted as risk factors for its development. Not surprisingly,excessive pleural drainage from patients with this form of injury was noted incomparison with patients who did not develop post-pneumonectomy edema.This occurred despite conservative fluid intake. Administration of blood prod-ucts such as fresh frozen plasma, higher mechanical ventilation pressures during surgery, and performance of redo thoracotomy for completion pneu-monectomy were considered additional risks [87].
Usually, post-pneumonectomy edema develops in the first 48–72 h after an otherwise routine uncomplicated pneumonectomy. Dyspnea and oxygenrequirement progress rapidly leading to admission to the intensive care unitfor mechanical ventilation. Physical examination and early chest radiographsare usually unremarkable; with rapid progression, examination will reveal the presence of diffuse lung crepitations and crackles and chest radiographswill manifest whiteout of the lung. Administration of diuretics is often of littlevalue. Insertion of a pulmonary artery catheter and measurement of wedgepressure will suggest low-pressure edema. Care must be taken as expansion ofa pulmonary artery balloon catheter in the course of hemodynamic measure-ment temporarily occludes a significant amount of the cross-sectional area ofthe single remaining pulmonary artery. This significant increase in pulmonaryartery resistance may result in significant hemodynamic compromise and a drop in arterial pressure. Diagnosis is often made after exclusion of other pulmonary complications such as pulmonary embolism, bacterial and viralpneumonia and aspiration pneumonia. A bronchoscopy often reveals frothyclear bronchial secretions and bronchoalveolar lavage and bacterial workup
42 Chapter 2
are often negative. Perfusion scans or enhanced spiral computed tomographyscans will rule out the presence of pulmonary embolism.
Despite the lack of convincing evidence that excessive fluid intake is respons-ible for post-pneumonectomy pulmonary edema, caution about administer-ing intravenous fluids following pneumonectomies should be practised and itis advisable that in the course of supporting these patients with mechanicalventilation, adequate sedation and analgesia be continued until the patient isready to be weaned. Patients actively struggling against the ventilator createabrupt increases in airway pressures and add additional baro-trauma. Supportmust also include rotating patients in bed regularly in order to avoid hydro-static pulmonary congestion. Many treating physicians would give diuretics,however, excessive dehydration may compromise perfusion of peripherallung zones resulting in increased shunting and hypoxia. It is recommendedthat bacterial cultures of sputum be regularly obtained and any specific pneu-monia be treated with the appropriate antimicrobial agent. Prophylacticantibiotics have no proven role, while prophylactic anticoagulation is meritedin most intensive care patients unless contraindicated. Pulmonary vascularrecruitment by utilization of inhaled nitric oxide has been shown to improvegas exchange and may benefit patients with post-pneumonectomy pulmonaryedema. It is also likely that other new therapeutic agents such as prostanoidbased drugs and endothelin receptor antagonists may be of benefit.Extracorporeal membrane oxygenation and liquid ventilation are considered a last resort and should be reserved for younger patients with convincing evidence of lung recoverability. It is likely that liquid ventilation may provesuperior in supporting the lung by avoiding baro-trauma of positive pressureventilation [88–98].
Recurrent laryngeal and phrenic nerve injuries
Even though not traditionally classified under respiratory complications,recurrent laryngeal and phrenic nerve injuries can lead to serious pulmonarysequelae [99]. Recurrent laryngeal injury may occur in the course of mobiliza-tion of the upper thoracic esophagus during esophagectomy or the perform-ance of a long myotomy, during radical left lung pneumonectomy when dissecting around the aortopulmonary window or during aortic surgery onthe left side. Dissection along the tracheo–esophageal groove at the thoracicinlet may result in injury to the right recurrent laryngeal nerve as it swingsaround the right subclavian artery. Orringer has described principles of tech-niques during cervical esophagectomy to avoid recurrent laryngeal nerveinjury which include careful placement of metal retractors for retraction of thetrachea to expose the esophagus. Similarly, cervical tracheal resections requirespecial attention to avoid injuring the recurrent nerve as it turns medially intothe laryngeal muscle [99].
Phrenic nerve injury most commonly occurs in the course of routine primaryor redo cardiac surgery and is attributed to nerve paresis or praxia during high

Respiratory complications of thoracic operations 43
dissection of the internal mammary artery due to tension on the pericardialstay sutures and the topical use of pericardial slush. In general thoracicsurgery, the phrenic nerve may be injured or purposely resected during mobil-ization or radical resection of aggressive mediastinal tumors. When thora-coabdominal procedures require transdiaphragmatic access, it is advisable todivide the diaphragm along the perimeters or radially. Anterior mediastino-tomy (Chamberlain procedure) may result in injury to either of the two nerves.Better visualization and magnification with video-assisted techniques maypotentially decrease the risk of phrenic and laryngeal nerve injuries.
References
1 Canver C, Bhayana J, Lajos T et al. Pulmonary resection combined with cardiac operations.Ann Thorac Surg 1990; 50: 796–799.
2 Deron S, Kotler M. Noncardiac surgery in the cardiac patient. Am Heart J 1988; 116: 831–838.3 Detsky A, Abrams H, Forbath N et al. Cardiac assessment for patients undergoing noncar-
diac surgery. Arch Intern Med 1986; 146: 231–234.4 Freeman W, Gibbons R, Shub C. Preoperative assessment cardiac patients undergoing
noncardiac surgical procedures. Mayo Clin Proc 1989; 64: 1105–1117.5 Anderson WH, Dossett BE, Hamilton GL. Prevention of postoperative pulmonary com-
plications; use of isoproterenol and intermittent positive pressure breathing on inspiration.JAMA 1963; 186: 763–767.
6 Dales RE, Dionne G, Leech JA et al. Preoperative prediction of pulmonary complicationsfollowing thoracic surgery. Chest 1993; 104: 155–159.
7 Deslauriers J, Ginsberg RJ, Dubois P et al. Current operative morbidity associated withelective surgical resection for lung cancer. Can J Surg 1989; 32: 335–339.
8 Massard G, Wihlm J. Postoperative atelectasis. In: Shennib H, ed. Medical Complications ofThoracic Surgery. Chest Surgical Clinic of North America. Philadelphia: W.B. Saunders, 1998,503–528.
9 Foster E, Davis K, Carpenter J et al. Risk of noncardiac operation in patients with definedcoronary disease: The Coronary Artery Surgery Study (CASS) registry experience. AnnThorac Surg 1986; 4: 42–50.
10 Ginsberg R, Hill L, Eagan E et al. Modern thirty-day operative mortality for surgical resec-tions in lung cancer. J Thorac Cardiovasc Surg 1983; 86: 654–658.
11 Goldman L, Caldera D, Nussbaum S et al. Multifactorial index of cardiac risk in noncar-diac surgical procedures. N Engl J Med 1977; 297: 845–850.
12 Kirsh M, Rotman H, Behrent D et al. Complications of pulmonary resection. Ann ThoracSurg 1975; 20: 215–236.
13 Krowka M, Pairolero P, Trastek V et al. Cardiac dysrhythmia following pneumonectomy:clinical correlates and prognostic significance. Chest 1987; 91: 490–495.
14 Lewis J, Bastanfar M, Gavriel F et al. Right heart function and prediction of respiratorymorbidity in patients undergoing pneumonectomy with moderately severe cardiopul-monary dysfunction. J Thorac Cardiovasc Surg 1994; 108: 169–175.
15 Mangano D, Browner W, Hollengerg M et al. Association of preoperative myocardialischemia with cardiac morbidity and mortality in men undergoing noncardiac surgery. N Engl J Med 1990; 323: 1781–1788.
16 Miller D, Orszulak T, Pairolero P et al. Combined operation for lung cancer and cardiacdisease. Ann Thorac Surg 1994; 58: 989–994.
44 Chapter 2
17 Mowry F, Reynolds E. Cardiac rhythm disturbances complicating resectional surgery ofthe lung. Ann Intern Med 1964; 61: 688–695.
18 Tarhan S, Moffit E, Taylor W et al. Myocardial infarction after general anesthesia. JAMA1972; 220: 1451.
19 Gamsu G, Singer MM, Vincent HH et al. Postoperative impairment of mucous transport inthe lung. Am Rev Respir Dis 1976; 114: 673–679.
20 Nelin LD, Rickaby DA, Linehan JH et al. Effect of atelectasis and surface tension on pul-monary vascular compliance. J Appl Physiol 1991; 70: 2401–2409.
21 Nguyen DM, Mulder DS, Shennib H. Altered cellular immune function in the atelectaticlung. Ann Thorac Surg 1991; 51: 76–80.
22 Paul A, Marelli D, Shennib H et al. Mucociliary function in autotransplanted, allotrans-planted and sleeve resected lungs. J Thorac Cardiovasc Surg 1989; 98: 523–528.
23 Shennib H, Mudler DS, Chiu RCJ. The effects of pulmonary atelectasis and reexpansion onlung cellular immune defences. Arch Surg 1984; 119: 274–277.
24 Rothen HU, Sporre B, Engberg G et al. Influence of gas composition on recurrence ofatelectasis after a reexpansion maneuver during general anesthesia. Anesthesiology 1995;82: 832–842.
25 Woodring JH, Reed JC. Types and mechanisms of pulmonary atelectasis. J Thorac Imaging1996; 11: 92–108.
26 Yao Taso T, Huang Tsai Y, Shee Ian R et al. Treatment of collapsed lung in critically illpatients. Chest 1990; 97: 435–438.
27 Young M, Marrie TJ. Interobserver variability interpretation of chest roentgenograms ofpatients with possible pneumonia. Arch Intern Med 1994; 154: 2729–2732.
28 Nagasaki F, Flehinger B, Martini N. Complications of surgery in the treatment of carci-noma of the lung. Chest 1982; 82: 25–29.
29 Patel R, Townsend E, Fountain S. Elective pneumonectomy. Factors associated with mor-bidity and operative mortality. Ann Thorac Surg 1992; 54: 84–88.
30 Rao T, Jocobs K, El-Ete A. Reinfarction following anesthesia in patients with myocardialinfarction. Anesthesiology 1983; 59: 499–505.
31 Reed C, Spinale F, Crawford F. Effect of pulmonary resection on right ventricular func-tion. Ann Thorac Surg 1992; 53: 578–582.
32 Ritchie A, Bowe P, Gibbons J. Prophylactic digitalization for thoracotomy: a reassessment.Ann Thorac Surg 1992; 53: 578–582.
33 Steen P, Tinker J, Tarhan S. Myocardial reinfarction after anesthesia and surgery. JAMA1978; 239: 2566–2570.
34 von Knorring J. Postoperative myocardial infraction. A prospective study in a risk groupof surgical patients. Surgery 1981; 90: 55–60.
35 von Knorring J, Lepantalo M, Lindgren L et al. Cardiac arrhythmias and myocardialischemia after thoracotomy for lung cancer. Ann Thorac Surg 1992; 53: 642–647.
36 Wahi R, McMurtrey M, DeCaro L et al. Determinants of preoperative morbidity and mor-tality after pneumonectomy. Ann Thorac Surg 1989; 48: 33–37.
37 Yokoyama T, Derrick M, Lee A. Cardiac operation with associated pulmonary resection. J Thorac Cardiovasc Surg 1993; 105: 912–917.
38 Handelsman H. Intermittent positive pressure breathing therapy. Health Technol AssessResp 1991; 1: 1–9.
39 Jaworski A, Goldberg SK, Walkenstein MF et al. Utility of immediate post lobectomyfiberoptic bronchoscopy in preventing atelectasis. Chest 1988; 94: 42.
40 Jonhson D, Kelm C, Thomson D et al. The effect of physical therapy on respiratory com-plications following cardiac valve surgery. Chest 1996; 109: 638–644.
Respiratory complications of thoracic operations 45
41 Marini J, Pierson D, Hudson L. Acute lobar atelectasis. A prospective comparison of bronchoscopy and respiratory therapy. Am Rev Respir Dis 1979; 119: 971–978.
42 Pedersen J, Schurizek BA, Melsen NC et al. Is minitracheostomy a simple and safe pro-cedure? A prospective investigation in the intensive care unit. Intensive Care Med 1991; 17:333–335.
43 Shennib H, Baslaim G. Bronchoscopy in the Intensive Care Unit. Chest Surgical Clinic of NorthAmerica. Philadelphia: W.B. Saunders Co., 1996; 345–361.
44 Stiller K, Geake T, Taylor J et al. Acute lobar atelectasis. A comparison of two chest physio-therapy regimens. Chest 1990; 98: 1336–1340.
45 Van Heerden PV, Jacob W, Cameron PD et al. Bronchoscopic insufflation of room air forthe treatment of lobar atelectasis in mechanically ventilated patients. Aneasth IntensiveCare 1995; 23: 175–177.
46 Boushy SF, Billig DM, North LB et al. Clinical course related to preoperative and postoper-ative pulmonary function in patients with bronchogenic carcinoma. Chest 1971; 59: 383.
47 Busch E, Verazin G, Antkowiak JG et al. Pulmonary complications in patients undergoingthoracotomy for lung carcinoma. Chest 1994; 105: 760.
48 Craven DE, Kunches LM, Kilinsky V et al. Risk factors of pneumonia and fatality inpatients receiving continuous mechanical intubation. Am Rev Respir Dis 1986; 133: 792.
49 Deslauriers J, Ginsberg RJ, Piantadosi S et al. Prospective assessment of 30-day operativemorbidity for surgical resections in lung cancer. Chest 1994; 106: 329S.
50 Gaynes R, Bizek B, Mowry-Hanley J et al. Risk factors for nosocomial pneumonia aftercoronary artery bypass graft operations. Ann Thorac Surg 1991; 51: 215.
51 Girabaldi RA, Britt MR, Coleman ML et al. Risk factors for postoperative pneumonia. Am JMed 1981; 70: 677.
52 Harpole DH, Liptay MJ, DeCamp MM Jr. et al. Prospective analysis of pneumonectomy;risk factors for major morbidity and cardiac dysrhythmias. Ann Thorac Surg 1996; 61: 977.
53 Higuchi JH, Coalson JJ, Johanson WG. Bacteriological diagnosis of nosocomial pneumo-nia in primates. Am Rev Respir Dis 1982; 125: 53.
54 Huxley EJ, Viroslav J, Gray WR et al. Pharyngeal aspiration in normal adults and patientswith depressed consciousness. Am J Med 1978; 64: 564.
55 Iwamoto K, Ichiyama S, Shimokata K et al. Postoperative pneumonia in elderly patients:incidence and mortality in comparison with young patients. Intern Med 1993; 32: 274–277.
56 Mitsudomi T, Mizoue T, Yoshimatsu T et al. Postoperative complications after pneu-monectomy for treatment of lung cancer: multivariate analysis. J Surg Oncol 1996; 61: 218.
57 Aznar R, Mateu M, Miro JM et al. Antibiotic prophylaxis in noncardiac thoracic surgery:cefazolin versus placebo. Eur J Cardiothorac Surg 1991; 5: 515.
58 Bernard A, Pillet M, Goudet P et al. Antibiotic prophylaxis in pulmonary surgery. J ThoracCardiovasc Surg 1994; 107: 896.
59 Bousamra M, Presberg KW, Chammas JH. Early and late morbidity in patients undergo-ing pulmonary resection with low diffusion capacity. Ann Thorac Surg 1996; 62: 968.
60 Markos J, Mullan BP, Hillman DR et al. Preoperative assessment as predictor of mortalityand morbidity after lung resection. Am J Resp Dis 1989; 39: 902.
61 Abraham E, Park YC, Covington P et al. Liposomal prostaglandin E1 in acute respiratorydistress syndrome: a placebo-controlled randomized, double-blind multicenter clinicaltrial. Crit Care Med 1996; 24: 10–15.
62 Amato MBP, Barbas CVS, Medeiros DM et al. Beneficial effect of ‘open lung approach’with low distending pressures in ARDS. Am J Respir Crit Care Med 1995; 152: 1835–1846.
63 Anderson HL, Delius RE, Sinard JM et al. Early experience with adult extracorporealmembrane oxygenation in the modern ear. Ann Thorac Surg 1992; 53: 553–563.
46 Chapter 2
64 Anzuete A, Baughman RP, Guntuplli KK et al. Aerosolized surfactant in adults with sepsis-induced ARDS. Exosurf ARDS sepsis study group. N Engl J Med 1996; 334: 1417–1421.
65 Armstrong BW, MacIntyre NR. Pressure-controlled inverse ratio ventilation that avoidsair trapping in the adult respiratory distress syndrome. Crit Care Med 1995; 23: 279–285.
66 Bernard GR, Artigas A, Brigham KL et al. The American–European Consensus Conferenceon ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. AmJ Respir Crit Care Med 1994; 149: 818–824.
67 Broccard AF, Shapiro RS, Schmitz LL et al. Influence of prone position on the extent anddistribution of lung injury in a high tidal volume oleic acid model or ARDS. Crit Care Med1997; 25: 16–27.
68 Brunet F, Mira JP, Belghith M et al. Extracorporeal carbon dioxide removal techniqueimproves oxygenation without causing overinflation. Am J Respir Crit Care Med 1994; 149:1557–1562.
69 Chatte G, Sab JM, Dubois JM et al. Prone position mechanically ventilates patients withsevere acute respiratory distress syndrome. Am J Respir Crit Care Med 1997; 155: 473–478.
70 Dreyfuss D, Soler P, Basset G et al. High inflation pressure pulmonary edema. Respectiveeffects of high airway pressure, high tidal volume and positive end-expiratory pressure.Am Rev Respir Dis 1988; 137: 1159–1164.
71 Dreyfuss D, Soler P, Saumon G. Mechanical ventilation-induced pulmonary edema. CritCare Med 1995; 151: 1568–1575.
72 Falkenhain SK, Reilley TE, Gregory JS. Improvement in cardiac output during airwaypressure release ventilation. Crit Care Med 1992; 20: 1358–1360.
73 Feihl F, Perret C. Permissive hypercapniaahow permissive should we be? Am J Respir CritCare Med 1994; 150: 1722–1737.
74 Gauger PG, Pranikoff T, Schreihner RJ et al. Initial experience with partial liquid ventila-tion in pediatric patients with the acute respiratory distress syndrome. Crit Care Med 1996;24: 16–22.
75 Gerlach H, Pappert D, Lewandowski K et al. Long-term inhalation with evaluated lowdoses of nitric oxide for selective improvement of oxygenation in patients with ARDS.Intens Care Med 1993; 19: 443–449.
76 Hickling KG, Walsh J, Henderson S et al. Low mortality rate of ARDS using low-volume,pressure-limited ventilation with permissive hypercapnia: a prospective study. Crit CareMed 1994; 22: 1568–1578.
77 Hirschl RB, Prannikoff T, Gauger P et al. Liquid ventilation in adults, children and fullterm neonates. Lancet 1995; 346: 1201–1202.
78 Hirschl RB, Prannikoff T, Wise C et al. Initial experience with partial liquid ventilation inadult patients with acute respiratory distress syndrome. JAMA 1996; 275: 383–389.
79 Lewis JF, Jobe AH. Surfactant and the adult respiratory distress syndrome. Am Rev RespirDis 1993; 147: 218–233.
80 Rossaint R, Falke KJ, Lopez F et al. Inhaled nitric oxide for ARDS. N Engl J Med 1993; 328:399–405.
81 Slotman GJ, Burchard KW, D’Arezzo A et al. Ketoconazole prevents acute respiratory failure in critically ill surgical patients. J Trauma 1988; 28: 648–654.
82 Slutsky AS. Barotrauma and alveolar recruitment. Intensive Care Med 1993; 19: 369–371.83 Swissler B, Kemming G, Habler O et al. Inhaled prostacyclin (PG12) versus inhaled nitric
oxide in ARDS. Am J Respir Crit Care Med 1996; 154: 1671–1677.84 Deslauriers J, Aucoin A, Gregoire J. Postpneumonectomy pulmonary edema. In: Shennib
H, ed. Medical Complications of Thoracic Surgery. Chest Surgical Clinic of North America.Philadelphia: W.B. Saunders, 1998; 611–631.
Respiratory complications of thoracic operations 47
85 Gibbon JH, Gibbon MH. Experimental pulmonary edema following lobectomy andplasma infusion. Surgery 1942; 12: 694–704.
86 Jansen JP, Brutel de la Riviere A, Carpentier-Alting MP et al. Postpneumonectomy syn-drome in adulthood. Chest 1992; 101: 1167–1170.
87 Little AG, Langmuir VK, Singer AH et al. Hemodynamic pulmonary edema in dog lungsafter contralateral pneumonectomy and mediastinal lymphatic interruption. Lung 1984;162: 139–145.
88 Mathisen DJ, Kuo EY, Hahn C et al. Inhaled nitrous oxide for adult respiratory distresssyndrome following pulmonary resection. Soc Thoracic Surgeons Annu Meeting 1998; 7: 68(Abstract).
89 Mathru M, Blakeman B, Dries DJ et al. Permeability pulmonary edema following lungresection. Chest 1990; 98: 1216–1218.
90 Nabers J, Hoogsteden HC, Hilvering C. Postpneumonectomy pulmonary edema treatedwith continuous positive airway pressure face mask. Crit Care Med 1989; 17: 102–103.
91 Okada M, Ota T, Okada M et al. Right ventricular dysfunction after major pulmonaryresection. J Thorac Cardiovasc Surg 1994; 108: 503–511.
92 Satur CMR, Robertson RH, DaCosta PE et al. Multiple pulmonary microemboli complicat-ing pneumonectomy. Ann Thorac Surg 1991; 52: 122–126.
93 Shapira OM, Shanian DM. Postpneumonectomy pulmonary edema. Ann Thorac Surg1993; 45: 190–195.
94 Slinger PD. Perioperative fluid management for thoracic surgery. The puzzle of postpneu-monectomy edema. J Cardiothorac Vasc Anesth 1995; 9: 442–451.
95 Turnage WS, Lunn JJ. Postpneumonectomy pulmonary edema. A retrospective analysisof associated variables. Chest 1993; 103: 1646–1650.
96 Van der Werff YD, van der Houwen HK, Heijmans PJM et al. Postpneumonectomy pul-monary edema. A retrospective analysis of incidence and possible risk factors. Chest 1997;111: 1278–1284.
97 Waller DA, Keavey P, Woodfine L et al. Pulmonary endothelial permeability changes aftermajor lung resection. Ann Thorac Surg 1996; 61: 1435–1440.
98 Wittnich C, Trudel J, Zidulka A et al. Misleading ‘pulmonary wedge pressure’ after pneumonectomy: its importance in postoperative fluid therapy. Ann Thorac Surg 1986; 42:192–196.
99 Feins R. Neurological complications in thoracic surgery. In: Shennib H, ed. MedicalComplications of Thoracic Surgery. Chest Surgery Clinic of North America. Philadelphia: W.B.Saunders, 1998; 633–643.

CHAPTER 3
Arrhythmias following cardiothoracicoperations
Adam E. Saltman, Joseph LoCicero III
Cardiac arrhythmia after thoracotomy is not a new problem. Since the firstreports in 1943 [1,2], many communications concerning arrhythmias haveappeared in the literature. For a comprehensive review, the reader is referredelsewhere. They may occur in the atrium or the ventricle, although supravent-ricular arrhythmias are far more common, usually accounting for over 80% ofsuch disorders. Of these, atrial fibrillation occurs most frequently, althoughmultifocal atrial tachycardia and atrial premature complexes are not unusual.The purposes of this chapter are (i) to describe the incidence and characteristicsof cardiac arrhythmias that appear after thoracic surgery, (ii) to explain what is known about the etiology of these dysrhythmias, (iii) to report on which prophylactic regimens are thought currently to be effective against them, and (iv) to instruct the reader as to their treatment.
Incidence and characteristics of postoperative arrhythmias
It has been well documented that cardiac arrhythmias, particularly atrialarrhythmias such as atrial fibrillation or flutter, occur in approximately25–40% of patients undergoing open heart surgery [3]. The incidence of thesearrhythmias following non-cardiac thoracic surgery is a bit more variable,depending upon the specific procedure. Most studies which have addressedthe issue have concluded that postoperative arrhythmias serve as a marker for increased mortality, longer intensive care unit stay and longer length ofhospital stay [4–6], although it is not clear if the arrhythmia itself is an inde-pendent predictor or rather a symptom of the patient’s illness.
SupraventricularAs displayed in Table 3.1, atrial arrhythmias following thoracic surgeryappear in 8–37% (average 20%) of all patients undergoing thoracotomy. Atrialfibrillation (AF) is by far the most common rhythm, accounting for at least 55%of supraventricular arrhythmias. The magnitude of operation plays an import-ant role. After simple exploration or biopsy, anywhere from 4.6 to 23.5% (average 9.3%) of patients suffered an atrial arrhythmia. After lobectomy, the
48
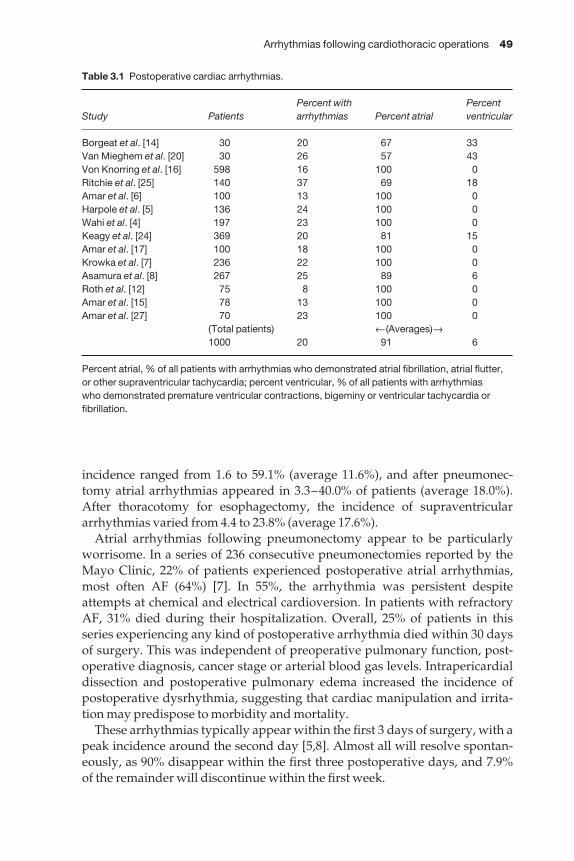
Arrhythmias following cardiothoracic operations 49
incidence ranged from 1.6 to 59.1% (average 11.6%), and after pneumonec-tomy atrial arrhythmias appeared in 3.3–40.0% of patients (average 18.0%).After thoracotomy for esophagectomy, the incidence of supraventriculararrhythmias varied from 4.4 to 23.8% (average 17.6%).
Atrial arrhythmias following pneumonectomy appear to be particularlyworrisome. In a series of 236 consecutive pneumonectomies reported by theMayo Clinic, 22% of patients experienced postoperative atrial arrhythmias,most often AF (64%) [7]. In 55%, the arrhythmia was persistent despiteattempts at chemical and electrical cardioversion. In patients with refractoryAF, 31% died during their hospitalization. Overall, 25% of patients in thisseries experiencing any kind of postoperative arrhythmia died within 30 daysof surgery. This was independent of preoperative pulmonary function, post-operative diagnosis, cancer stage or arterial blood gas levels. Intrapericardialdissection and postoperative pulmonary edema increased the incidence ofpostoperative dysrhythmia, suggesting that cardiac manipulation and irrita-tion may predispose to morbidity and mortality.
These arrhythmias typically appear within the first 3 days of surgery, with apeak incidence around the second day [5,8]. Almost all will resolve spontan-eously, as 90% disappear within the first three postoperative days, and 7.9% of the remainder will discontinue within the first week.
Table 3.1 Postoperative cardiac arrhythmias.
Percent with PercentStudy Patients arrhythmias Percent atrial ventricular
Borgeat et al. [14] 30 20 67 33Van Mieghem et al. [20] 30 26 57 43Von Knorring et al. [16] 598 16 100 0Ritchie et al. [25] 140 37 69 18Amar et al. [6] 100 13 100 0Harpole et al. [5] 136 24 100 0Wahi et al. [4] 197 23 100 0Keagy et al. [24] 369 20 81 15Amar et al. [17] 100 18 100 0Krowka et al. [7] 236 22 100 0Asamura et al. [8] 267 25 89 6Roth et al. [12] 75 8 100 0Amar et al. [15] 78 13 100 0Amar et al. [27] 70 23 100 0
(Total patients) ←(Averages)→1000 20 91 6
Percent atrial, % of all patients with arrhythmias who demonstrated atrial fibrillation, atrial flutter,or other supraventricular tachycardia; percent ventricular, % of all patients with arrhythmias who demonstrated premature ventricular contractions, bigeminy or ventricular tachycardia orfibrillation.

50 Chapter 3
VentricularVentricular arrhythmias, mainly appearing as either burst of extrasystoles or short runs of non-sustained tachycardia, are appearing more commonly asthe acuity of illness and average patient age rise with time. Fortunately, theyare much more rare than supraventricular arrhythmias, appearing in only0–43% (average 6%) of all patients undergoing non-cardiac thoracic surgery ofall types.
Risk factors
Many investigators have attempted to determine the specific risks factors associated with postoperative cardiac arrhythmias. Unfortunately, no com-mon element has emerged. In one study by Melendez and Carlon of 180patients undergoing pneumonectomy, lobectomy, wedge resection or lesserpulmonary procedures, there was a 12% incidence of cardiac ‘complications’[9]. The authors attempted to assign a Cardiopulmonary Risk Index (CPRI: theaddition of the Goldman Cardiac Risk Index [10] to a Pulmonary Risk Indexwhich included obesity, cough, elevated PaCO2, poor spirometric parameters,cigarette smoking and asthma) to each patient. There was no correlationbetween the CPRI and the incidence of cardiac arrhythmias. Furthermore,there was no correlation between postoperative arrhythmias and either theCardiac Risk Index or the Pulmonary Risk Index when considered in isolation.Not too surprisingly, however, preoperative ‘rhythm alteration’, ‘cardiac disease’, an abnormal electrocardiogram and a forced expiratory volume in 1 s (FEV1) < 2.0 correlated positively with postoperative arrhythmias.
This finding was echoed by Hasenbos and colleagues who attempted tocompare differences in postoperative complications between patients givenepidural or intramuscular narcotic pain medication [11]. Although this studyfound no differences in postoperative complications between groups accord-ing to method of pain relief, it did find that patients who were taking ‘cardiacdrugs’ preoperatively had a higher risk of developing arrhythmias in the postoperative period (68% vs. 38%). This study suggests that patients with pre-existing cardiac disease are at higher risk of developing postoperativearrhythmias.
In a search for anatomic risk factors for postoperative complications, Roth et al. attempted to quantify coronary artery calcifications found on chest com-puted tomography (CT) scan and use the Coronary Artery Calcification Index(CAC) to predict the occurrence of postoperative arrhythmias [12]. Althoughthe CAC had 100% sensitivity for postoperative arrhythmias, its positive predictive value was only 23%, making it a weak index by which to screenpatients for this complication. With a negative predictive value of 100%, how-ever, it is helpful to know that a patient with no coronary calcifications presenton chest CT will probably have a smoother postoperative course.
Asamura and associates have undertaken the most complete study to dateon preoperative risk factors for postoperative arrhythmias [8]. They studied

Arrhythmias following cardiothoracic operations 51
267 patients undergoing pneumonectomy, lobectomy bilobectomy, segmen-tectomy or wedge resection, and discovered 63 arrhythmias (23.6% incidence).Of those, 60 (95%) were supraventricular, and of that subset 33 (55%) wereatrial fibrillation. Besides tabulating demographic variables such as sex, age, indication for operation, hypertension and preoperative ECG status, theauthors also made note of the mode of thoracotomy, the extent of the pul-monary resection and the extent of the lymph node dissection. They found thatonly age > 70 years (P < 0.0008) and extent of pulmonary resection (P < 0.0001)were independent predictors for the appearance of postoperative atrialarrhythmias.
There is recent evidence emerging that the side of operation may play a role in the genesis of arrhythmias following thoracic surgery, particularlypneumonectomy. In a series of 115 patients undergoing pneumonectomy,Yellin and Zeligson reported the incidence of dysrhythmias to be 4.2% inpatients undergoing a left-sided operation, compared with 14% in those with aright pneumonectomy (P = 0.05) [13]. This has been supported by some studies[5], but not by others [4,14].
Influence on outcome
A few studies have attempted to correlate the occurrence of postoperativearrhythmias with patient outcome. In a report of 78 patients undergoing pneumonectomy, lobectomy or wedge resection for non-small cell lung cancer, Amar et al. found 13% demonstrated postoperative dysrhythmias [15].Somewhat surprisingly, neither the stage of the tumor, the extent of operation,nor the administration of preoperative radiation therapy influenced survivalat the 30-month follow-up. This may have been due to the small study popula-tion. Survival at 30 months was, however, adversely affected by age > 70 years,perioperative chemotherapy and the occurrence of postoperative supraven-tricular tachycardia. The patients who died during the follow-up period did soas a result of their disease, and not from arrhythmias.
In another study conducted by von Knorring and associates of 598 patientsundergoing resection for lung cancer, atrial tachyarrhythmias occurred in 16% [16]. Of those patients with recurrent episodes, 17% died. This wassignificantly higher than the mortality rate observed in patients with limitedepisodes (2.5%, P < 0.01).
Specific arrhythmias and their mechanisms
It is not currently known what causes atrial dysrhythmias in postoperativethoracic surgical patients. There have been many conjectures, includingincreased sympathetic discharge from postoperative pain, atrial fluid overloadfrom intraoperative and postoperative resuscitation, and even increased atrial pressure from high pulmonary vascular resistance in the patient afterparenchymal resection. In a study of 100 consecutive patients undergoing

52 Chapter 3
pulmonary resection at Memorial Sloan-Kettering Cancer Center, Amar et al.were able to show that patients with high right ventricular pressures (as determined by echocardiography) had a higher incidence of postoperativesupraventricular tachycardias [17]. This was not associated with an elevatedright atrial pressure, however, as measured by a central venous catheter. Also,the right and left atrial chambers were of normal size and did not differbetween groups.
These findings are partially supported by the work of Reed et al., whoshowed that right ventricular function is diminished following pulmonaryresection [18]. They demonstrated that right ventricular end diastolic volumeincreased and ejection fraction decreased during the first 2 days after re-section. In comparison with preoperative values, pulmonary artery systolicpressure and calculated pulmonary vascular resistance did not change. Thiscorresponds to the period of highest risk for postoperative supraventriculartachycardia (SVT). They did not follow these patients out beyond the first 2days, however. Also, for the 20% of patients who exhibited SVT, they did notdiscriminate the right ventricular variables between patients who sufferedSVT and those who did not. Whether this results from a primary myocardialprocess or an alteration in right ventricular loading during the early post-operative period remains unclear. Although the same authors subsequentlyreported that right ventricular preload recruitable stroke work was unchangedduring the first 24 h following surgery, which suggests that right ventricularcontractility per se is unaffected [19].
Atrial premature contractionsAtrial premature contractions (APCs) are characterized by a P wave appearingearlier in the cardiac cycle than anticipated, usually of a different morphologythan the usual sinus P waves (Figure 3.1). This suggests that the ectopic beat originates in atrial tissue outside of the sinoatrial node. If the APC is early,it may encounter a refractory atrioventricular node (AVN), and either noimpulse will be transmitted to the ventricle or the conducted impulse willdepolarize the ventricle with a bundle branch pattern. If the APC enters thesinus node during electrical diastole, it may ‘reset’ the node and delay onset of the next sinus beat.
The causes of APCs are legion, and they have been associated with con-gestive heart failure, electrolyte imbalances, myocardial ischemia and peri-carditis. The use of temporary epicardial atrial wires or a transesophageal electrocardiogram can facilitate their diagnosis.
Atrial fibrillationAtrial fibrillation results from a chaotic, disorganized and irregular beating ofthe atrium at 400–600 times per minute. The sinus node no longer participatesin the pacemaking process. The atrioventricular node, which is incapable oftransmitting impulses so rapidly to the ventricle, blocks most of these beats.The ventricle therefore typically responds to atrial fibrillation by beating irre-
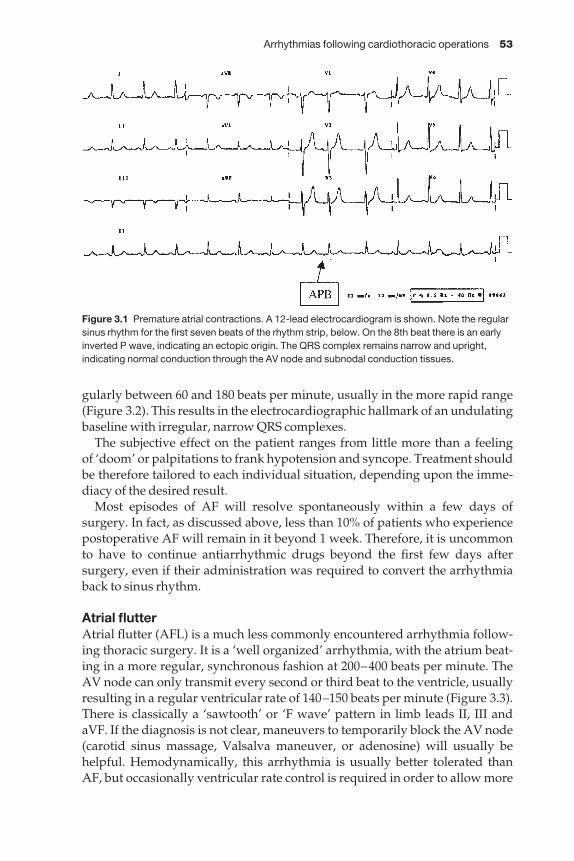
Arrhythmias following cardiothoracic operations 53
gularly between 60 and 180 beats per minute, usually in the more rapid range(Figure 3.2). This results in the electrocardiographic hallmark of an undulatingbaseline with irregular, narrow QRS complexes.
The subjective effect on the patient ranges from little more than a feeling of ‘doom’ or palpitations to frank hypotension and syncope. Treatment shouldbe therefore tailored to each individual situation, depending upon the imme-diacy of the desired result.
Most episodes of AF will resolve spontaneously within a few days ofsurgery. In fact, as discussed above, less than 10% of patients who experiencepostoperative AF will remain in it beyond 1 week. Therefore, it is uncommonto have to continue antiarrhythmic drugs beyond the first few days aftersurgery, even if their administration was required to convert the arrhythmiaback to sinus rhythm.
Atrial flutterAtrial flutter (AFL) is a much less commonly encountered arrhythmia follow-ing thoracic surgery. It is a ‘well organized’ arrhythmia, with the atrium beat-ing in a more regular, synchronous fashion at 200–400 beats per minute. TheAV node can only transmit every second or third beat to the ventricle, usuallyresulting in a regular ventricular rate of 140–150 beats per minute (Figure 3.3).There is classically a ‘sawtooth’ or ‘F wave’ pattern in limb leads II, III and aVF. If the diagnosis is not clear, maneuvers to temporarily block the AV node(carotid sinus massage, Valsalva maneuver, or adenosine) will usually behelpful. Hemodynamically, this arrhythmia is usually better tolerated thanAF, but occasionally ventricular rate control is required in order to allow more
Figure 3.1 Premature atrial contractions. A 12-lead electrocardiogram is shown. Note the regularsinus rhythm for the first seven beats of the rhythm strip, below. On the 8th beat there is an earlyinverted P wave, indicating an ectopic origin. The QRS complex remains narrow and upright,indicating normal conduction through the AV node and subnodal conduction tissues.
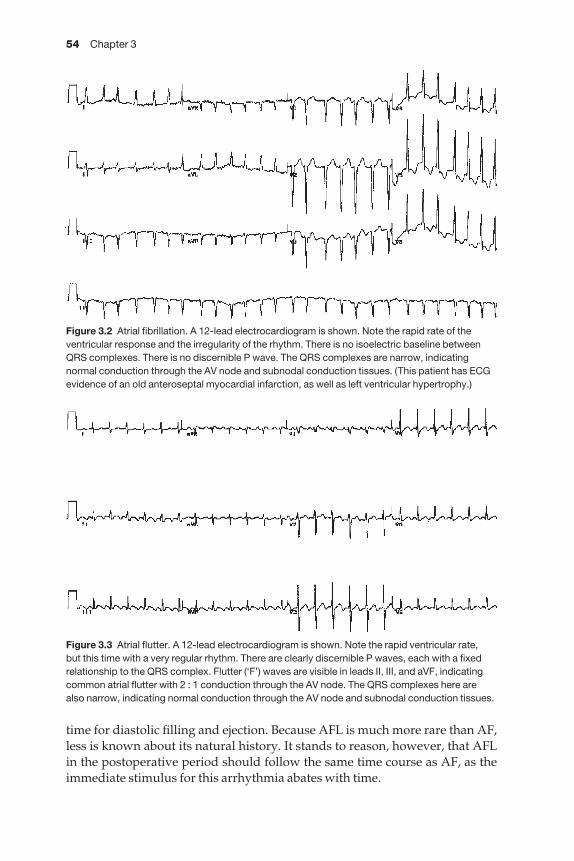
54 Chapter 3
time for diastolic filling and ejection. Because AFL is much more rare than AF,less is known about its natural history. It stands to reason, however, that AFLin the postoperative period should follow the same time course as AF, as theimmediate stimulus for this arrhythmia abates with time.
Figure 3.2 Atrial fibrillation. A 12-lead electrocardiogram is shown. Note the rapid rate of theventricular response and the irregularity of the rhythm. There is no isoelectric baseline betweenQRS complexes. There is no discernible P wave. The QRS complexes are narrow, indicatingnormal conduction through the AV node and subnodal conduction tissues. (This patient has ECGevidence of an old anteroseptal myocardial infarction, as well as left ventricular hypertrophy.)
Figure 3.3 Atrial flutter. A 12-lead electrocardiogram is shown. Note the rapid ventricular rate, but this time with a very regular rhythm. There are clearly discernible P waves, each with a fixedrelationship to the QRS complex. Flutter (‘F’) waves are visible in leads II, III, and aVF, indicatingcommon atrial flutter with 2 : 1 conduction through the AV node. The QRS complexes here arealso narrow, indicating normal conduction through the AV node and subnodal conduction tissues.
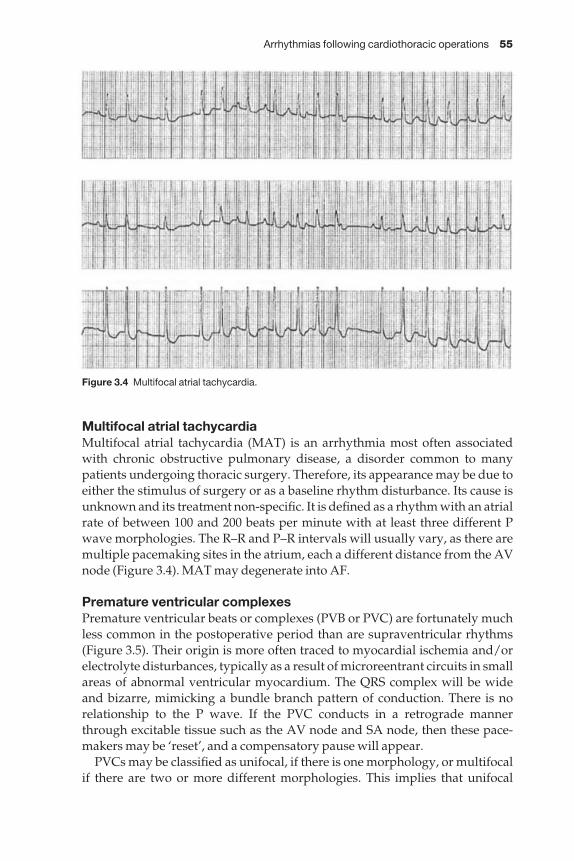
Arrhythmias following cardiothoracic operations 55
Multifocal atrial tachycardiaMultifocal atrial tachycardia (MAT) is an arrhythmia most often associatedwith chronic obstructive pulmonary disease, a disorder common to manypatients undergoing thoracic surgery. Therefore, its appearance may be due toeither the stimulus of surgery or as a baseline rhythm disturbance. Its cause isunknown and its treatment non-specific. It is defined as a rhythm with an atrialrate of between 100 and 200 beats per minute with at least three different Pwave morphologies. The R–R and P–R intervals will usually vary, as there aremultiple pacemaking sites in the atrium, each a different distance from the AVnode (Figure 3.4). MAT may degenerate into AF.
Premature ventricular complexesPremature ventricular beats or complexes (PVB or PVC) are fortunately muchless common in the postoperative period than are supraventricular rhythms(Figure 3.5). Their origin is more often traced to myocardial ischemia and/orelectrolyte disturbances, typically as a result of microreentrant circuits in smallareas of abnormal ventricular myocardium. The QRS complex will be wideand bizarre, mimicking a bundle branch pattern of conduction. There is norelationship to the P wave. If the PVC conducts in a retrograde mannerthrough excitable tissue such as the AV node and SA node, then these pace-makers may be ‘reset’, and a compensatory pause will appear.
PVCs may be classified as unifocal, if there is one morphology, or multifocalif there are two or more different morphologies. This implies that unifocal
Figure 3.4 Multifocal atrial tachycardia.
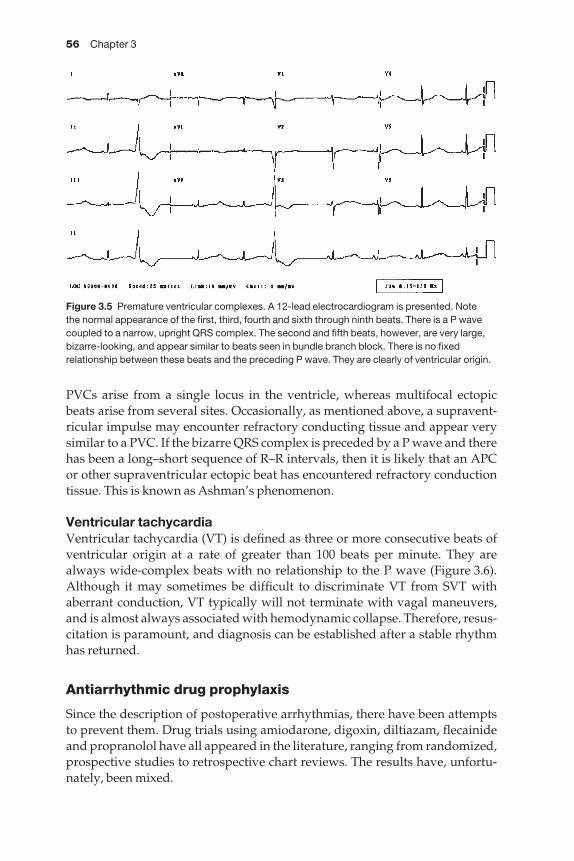
56 Chapter 3
PVCs arise from a single locus in the ventricle, whereas multifocal ectopicbeats arise from several sites. Occasionally, as mentioned above, a supravent-ricular impulse may encounter refractory conducting tissue and appear verysimilar to a PVC. If the bizarre QRS complex is preceded by a P wave and therehas been a long–short sequence of R–R intervals, then it is likely that an APC or other supraventricular ectopic beat has encountered refractory conductiontissue. This is known as Ashman’s phenomenon.
Ventricular tachycardiaVentricular tachycardia (VT) is defined as three or more consecutive beats ofventricular origin at a rate of greater than 100 beats per minute. They arealways wide-complex beats with no relationship to the P wave (Figure 3.6).Although it may sometimes be difficult to discriminate VT from SVT withaberrant conduction, VT typically will not terminate with vagal maneuvers,and is almost always associated with hemodynamic collapse. Therefore, resus-citation is paramount, and diagnosis can be established after a stable rhythmhas returned.
Antiarrhythmic drug prophylaxis
Since the description of postoperative arrhythmias, there have been attemptsto prevent them. Drug trials using amiodarone, digoxin, diltiazam, flecainideand propranolol have all appeared in the literature, ranging from randomized,prospective studies to retrospective chart reviews. The results have, unfortu-nately, been mixed.
Figure 3.5 Premature ventricular complexes. A 12-lead electrocardiogram is presented. Note the normal appearance of the first, third, fourth and sixth through ninth beats. There is a P wavecoupled to a narrow, upright QRS complex. The second and fifth beats, however, are very large,bizarre-looking, and appear similar to beats seen in bundle branch block. There is no fixedrelationship between these beats and the preceding P wave. They are clearly of ventricular origin.
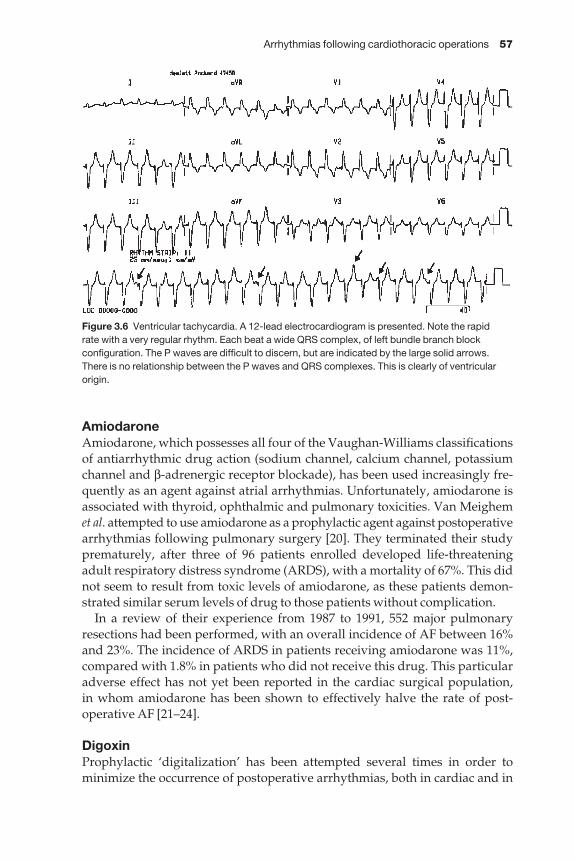
Arrhythmias following cardiothoracic operations 57
AmiodaroneAmiodarone, which possesses all four of the Vaughan-Williams classificationsof antiarrhythmic drug action (sodium channel, calcium channel, potassiumchannel and β-adrenergic receptor blockade), has been used increasingly fre-quently as an agent against atrial arrhythmias. Unfortunately, amiodarone isassociated with thyroid, ophthalmic and pulmonary toxicities. Van Meighemet al. attempted to use amiodarone as a prophylactic agent against postoperativearrhythmias following pulmonary surgery [20]. They terminated their studyprematurely, after three of 96 patients enrolled developed life-threateningadult respiratory distress syndrome (ARDS), with a mortality of 67%. This didnot seem to result from toxic levels of amiodarone, as these patients demon-strated similar serum levels of drug to those patients without complication.
In a review of their experience from 1987 to 1991, 552 major pulmonaryresections had been performed, with an overall incidence of AF between 16%and 23%. The incidence of ARDS in patients receiving amiodarone was 11%,compared with 1.8% in patients who did not receive this drug. This particularadverse effect has not yet been reported in the cardiac surgical population, in whom amiodarone has been shown to effectively halve the rate of post-operative AF [21–24].
DigoxinProphylactic ‘digitalization’ has been attempted several times in order to minimize the occurrence of postoperative arrhythmias, both in cardiac and in
Figure 3.6 Ventricular tachycardia. A 12-lead electrocardiogram is presented. Note the rapid rate with a very regular rhythm. Each beat a wide QRS complex, of left bundle branch blockconfiguration. The P waves are difficult to discern, but are indicated by the large solid arrows.There is no relationship between the P waves and QRS complexes. This is clearly of ventricularorigin.

58 Chapter 3
non-cardiac thoracic surgical patients. In a randomized controlled unblindedstudy of 80 consecutive patients undergoing thoracotomy for esophagectomy,Ritchie et al. randomly assigned half of the patients to receive digoxin and half to receive no treatment [25]. The drug was begun preoperatively and con-tinued postoperatively for 9 days, with serum levels measured and adjustedappropriately. There was no difference in the occurrence of dysrhythmiasbetween the patient groups. The authors did not discriminate between atrialand ventricular arrhythmias. They did, however, clearly demonstrate thatpatients undergoing resection for benign disease had a significantly lower incidence of arrhythmia than did those having an operation for malignancy(0% vs. 39%, P < 0.002).
They extended their findings in a study of 140 patients undergoing thoraco-tomy for pulmonary and esophageal procedures [26]. The overall incidence ofarrhythmias was 37%, with no differences between digoxin-treated patientsand control.
DiltiazemIn a small study of patients undergoing pneumonectomy at memorial Sloan-Kettering Cancer Center, digoxin was compared with diltiazem for post-operative control of arrythmias [27]. Patients on digoxin had an incidence of31% supraventricular arrythmias while those on diltiazem had an incidence of14% (P = 0.09). However, in the subset of patients having an intrapericardialpneumonectomy, diltiazem patients had no supraventricular arrythmias compared with 32% in the digoxin arm (P < 0.005). No patients in the studyhad ventricular tachycardia, although most had occasional ventricular premat-ure beats.
FlecainideIn a randomized, placebo-controlled single-blinded study of 30 patientsundergoing pneumonectomy, lobectomy or decortication, Borgeat et al. deter-mined that flecainide administration immediately following operationresulted in a significant decrease in the use of additional antiarrhythmic drugs[14]. Because these authors did not consider the incidence of atrial arrhythmiasas a separate endpoint, one cannot draw a conclusion about the efficacy offlecainide against this rhythm. There was, however, a significant decrease in the incidence of PVCs. In another study by this same group comparing the postoperative administration of flecainide with digoxin, the same groupshowed that flecainide significantly decreased the incidence of AF (by 50%)and PVCs (by 100%) [28].
PropranololIn 1999, Bayliff and associates conducted a randomized trial of propranolol vs.placebo in patients undergoing a major pulmonary resection [29]. This studywas somewhat flawed because of a large number of patients (142 out of 242)who did not participate in the study. They were able to randomize 99 of the
Arrhythmias following cardiothoracic operations 59
100 patients in the study. Patients in the experimental arm received 10 mg ofpropranolol every 6 h. Arrythmias of any variety occurred in 62% of placebopatients and 72% in the propranolol group. However, rhythms that requiredtreatment were 20% in the placebo patients and 6% in the propranolol patients.Only AF occurred in the propranolol group while every rhythm includingventricular tachycardia was seen in the placebo group. Hypotension andbradycardia were common in the propranolol group at 49% and 25%, respect-ively, while both were significantly less in the placebo group at 26% and 4%,respectively. Although it seemed to be effective, the side-effects argue againstthe routine use of propranolol in thoracic surgery.
Treatment
The treatment of postoperative arrhythmias is controversial. A brief review of the most commonly used medications is presented in Table 3.2, and a suggested treatment algorithm is presented in Figure 3.7. Because atrialarrhythmias are far more common, their management is discussed in somedetail below. In contrast, because the treatment of ventricular arrhythmiasrelies primarily upon resuscitation of the patient from a hemodynamic-ally unstable situation, little else will be said about them. The principles of correcting electrolyte abnormalities and ruling out myocardial ischemiashould be paramount for patients demonstrating ventricular ectopy and/ortachycardia.
Once the diagnosis of an atrial tachyarrhythmia has been established, thefirst priority is to assess hemodynamic stability. If the patient experiences syncope, or if the blood pressure is < 80 mmHg systolic, then synchronouselectrical cardioversion should be performed. The first shock is typically deliv-ered at 200 J, with subsequent shocks at 300 J and 360 J, respectively. For thesyncopal patient, no premedication is required. For the patient who is mentat-ing, however, some sedation should be administered prior to cardioversion.Sometimes this will depress the blood pressure further, requiring intravenousfluid administration.
Table 3.2 Commonly used antiarrhythmic agents.
Drug Class Loading dose Maintenance dose
Adenosine (Unassigned) 6–12 mg rapid i.v. push (None)Digoxin (Unassigned) 1.0–1.5 mg/4 doses/12 h 0.125–0.25 mg/day p.o. or i.v.Procainamide I-A 17 mg/kg (load over 20 min) 2 mg/min i.v. infusionMetoprolol* II 5–10 mg i.v. bolus 5–10 mg i.v. q 1–2 hVerapamil IV 5–10 mg i.v. bolus 5–10 mg i.v. q 1–2 hDiltiazem IV 0.25 mg/kg (load over 10 min) 5–10 mg/min i.v. infusion
‘Class’ refers to Vaughan-Williams classification; i.v., intravenous. *b-Blockers are contraindicatedin patients with bronchospastic disease or known hypersensitivity to the drug.
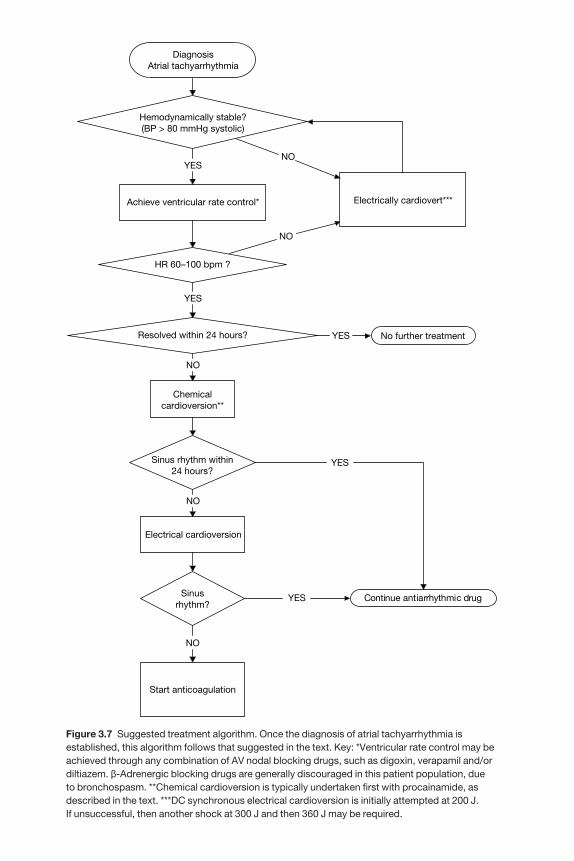
DiagnosisAtrial tachyarrhythmia
Hemodynamically stable?(BP > 80 mmHg systolic)
Electrically cardiovert***Achieve ventricular rate control*
No further treatment
NOYES
YES
Chemicalcardioversion**
Resolved within 24 hours?
NO
NO
Sinus rhythm within24 hours?
Electrical cardioversion
Sinusrhythm?
Continue antiarrhythmic drug
Start anticoagulation
YES
NO
HR 60–100 bpm ?
YES
NO
YES
Figure 3.7 Suggested treatment algorithm. Once the diagnosis of atrial tachyarrhythmia isestablished, this algorithm follows that suggested in the text. Key: *Ventricular rate control may beachieved through any combination of AV nodal blocking drugs, such as digoxin, verapamil and/ordiltiazem. b-Adrenergic blocking drugs are generally discouraged in this patient population, due to bronchospasm. **Chemical cardioversion is typically undertaken first with procainamide, asdescribed in the text. ***DC synchronous electrical cardioversion is initially attempted at 200 J. If unsuccessful, then another shock at 300 J and then 360 J may be required.
Arrhythmias following cardiothoracic operations 61
Ventricular rate controlIf the patient is hemodynamically stable and mentating, then the next priorityshould be to achieve control over the ventricular rate, as it is usually rapid(140–200 beats per minute). Drugs such as digoxin, verapamil, diltiazem ormetoprolol all depress AV nodal conduction, and are most useful here. Manythoracic surgical patients exhibit bronchospasm, however, and therefore β-adrenergic blocking drugs are relatively contraindicated. Furthermore, β-blockers are frequently longer-acting than calcium channel blocking drugsand are not as easy to reverse should an adverse effect appear. For these reasons, this author prefers to use digoxin (0.5-mg i.v. bolus, followed by two0.25-mg i.v. boluses spaced 4 h apart) combined with verapamil (5–10-mg i.v.bolus every 5–10 min) or diltiazem (0.25–0.35 mg/kg i.v. bolus every 5–10 min)to control ventricular rate. If these drugs are not successful, or if the patient’shemodynamics deteriorate, then synchronous cardioversion should be under-taken immediately. Once rate control has been achieved, the patient may be transitioned over to equivalent doses of oral digoxin and verapamil or diltiazem over the next 24 h.
During this period of time, electrolytes such as potassium and magnesiumshould be assayed and repleted. Myocardial ischemia should be ruled out by electrocardiography. In the absence of these factors, the natural history ofpostoperative atrial tachyarrhythmias is self-termination. Therefore, usuallynothing more than a day or two of rate control is required. If the patient does,indeed, spontaneously convert back to normal sinus rhythm over the next 24h, the digoxin and calcium channel blocker can be discontinued and no furthertreatment is required.
CardioversionIf, however, the patient remains in a rate-controlled fibrillation or flutterbeyond 24 h, then cardioversion should be attempted. Usually this is begun as a trial of chemical cardioversion with antiarrhythmic medication. Unfortu-nately, there is no single drug which demonstrated high efficacy at convertingpostoperative AF or AFL to sinus rhythm. The class I-A agents such as pro-cainamide and quinidine exhibit approximately a 30% conversion rate, similarto placebo. The class I-C agents such as flecainide and propafanone claim asomewhat higher conversion rate (about 40–60%), but their use is contraindic-ated in patients recently following a myocardial infarction or with a knowndepressed ejection fractionamany of the patients who are seen on thoracic sur-gical services. The new class III agent, ibutilide, claims a very high conversionrate of approximately 60%, but is associated with both a high relapse rate andalso the appearance of malignant ventricular arrhythmias such as Torsadesde Pointes. One of the older class III agents, d-sotalol, has been shown to beeffective at converting AF to sinus rhythm, but the racemic mixture of d- and l-sotalol has significant β-blocking activity and is relatively contraindicated in thoracic surgical patients.
Despite its relative lack of efficacy, the most often used and recommendeddrug for chemical cardioversion is procainamide. It is easy to load (17 mg/kg

62 Chapter 3
i.v. over 20 min), has relatively few acute limiting side-effects (hypotension,nausea), and is quickly metabolized. Unlike quinidine, which has anticholiner-gic side-effects, procainamide has some antiadrenergic effects, and can there-fore ‘double’ as an AV nodal blocking drug. Once the patient has been given aprocainamide load, they are started on a continuous infusion of 2–4 mg/min.If the patient is taking oral medications, then Procan SR® or ProcanBID® can bestarted by mouth once the loading dose is completed. The infusion is stoppedafter the second oral dose.
If the patient converts to sinus rhythm, then the oral antiarrhythmic drugshould be continued for at least 30 days after surgery. It may then be stoppedas an out-patient, as the risk of relapsing into AF or AFL is extremely unlikelyso far out from operation. If the arrhythmia persists, however, two options areavailable. First, a semielective electrical cardioversion may be undertaken atthis time, with adequate serum levels of antiarrhythmic drug present. Second,the patient may be given anticoagulation with heparin and then maintained onwarfarin.
Typically, if a patient is discharged from the hospital in rate-controlled AFwith adequate anticoagulation, they will spontaneously convert to sinusrhythm as an out-patient. If, however, they remain in AF beyond 30 post-operative days, then they should be at low risk for an out-patient electrical cardioversion, provided they have remained therapeutically anticoagulated.
Summary
Cardiac arrhythmias are common after thoracic surgical procedures. Mostarrhythmias are atrial in origin and typically are not life threatening, althoughthere are some data which suggest that they adversely affect long-term prog-nosis. Their cause remains unclear, although there is some indication thatacute right ventricular overload may contribute. Risk factors for atrial arrhyth-mias following thoracotomy appear to be increasing patient age, extent ofoperation and perhaps side of operation.
These arrhythmias typically occur within the first 2–3 days after surgery,and usually abate by day 6. Treatment should initially be aimed at achievingventricular rate, with the hope that most patients will spontaneously convertback to normal sinus rhythm. Should conservative measures fail at cardiover-sion, then anticoagulation should be instituted and electrical cardioversion canbe attempted, either as an in-patient or later, as an out-patient.
References1 Currens JH, White PD, Churchill ED. Cardiac arrhythmias following thoracic surgery.
N Engl J Med 1943; 229: 360–364.2 Baley CC, Betts RH. Cardiac arrhythmias following pneumonectomy. N Engl J Med 1943;
229: 356–360.3 Ferguson TB Jr. Arrhythmias associated with thoracotomy. In: Wolfe WG, ed. Complica-
tions in Thoracic Surgery. Recognition and Management. St Louis: Mosby, 1992; 28–50.
Arrhythmias following cardiothoracic operations 63
4 Wahi R, McMurtrey MJ, DeCaro LF et al. Determinants of perioperative morbidity andmortality after pneumonectomy. Ann Thoracic Surg 1989; 48: 33–37.
5 Harpole DH, Liptay MJ, DeCamp MM Jr, Mentzer SJ, Swanson SJ, Sugarbaker DJ.Prospective analysis of pneumonectomy: risk factors for major morbidity and cardiac dysrhythmias. Ann Thoracic Surg 1996; 61: 977–982.
6 Amar D, Burt ME, Bains MS, Leung DH. Symptomatic tachydysrhythmias afteresophagectomy: incidence and outcome measures. Ann Thoracic Surg 1996; 61: 1506–1509.
7 Krowka MJ, Pairolero PC, Trastek VF, Payne WS, Bernatz PE. Cardiac dysrhythmia fol-lowing pneumonectomy. Clinical correlates and prognostic significance. Chest 1987; 91:490–495.
8 Asamura H, Naruke T, Tsuchiya R, Goya T, Kondo H, Suemasu K. What are the risk factors for arrhythmias after thoracic operations? A retrospective multivariate analysis of267 consecutive thoracic operations. J Thoracic Cardiovasc Surg 1993; 106: 1104–1110.
9 Melendez JA, Carlon VA. Cardiopulmonary risk index does not predict complicationsafter thoracic surgery. Chest 1998; 114: 69–75.
10 Goldman L, Caldera DL, Nussbaum SR et al. Multifactorial index of cardiac risk in noncar-diac surgical procedures. N Engl J Med 1977; 297: 845–850.
11 Hasenbos M, van Egmond J, Gielen M, Crul JF. Post-operative analgesia by epidural versus intramuscular nicomorphine after thoracotomy. Part II. Acta Anesthesiologica Scand1985; 29: 577–582.
12 Roth BJ, Meyer CA. Coronary artery calcification at CT as a predictor for cardiac complica-tions of thoracic surgery. J Comp Assisted Tomogr 1997; 21: 619–622.
13 Yellin A, Zeligson E. Postpneumonectomy dysrhythmias. Chest 1988; 93: 669 (letter).14 Borgeat A, Biollaz J, Bayer-Berger M, Kappenberger L, Chapuis G, Chiolero R. Prevention
of arrhythmias by flecainide after noncardiac thoracic surgery. Ann Thoracic Surg 1989; 48:232–234.
15 Amar D, Burt M, Reinsel RA, Leung DH. Relationship of early postoperative dysrhythmiasand long-term outcome after resection of nonsmall cell lung cancer. Chest 1996; 110:437–439.
16 von Knorring J, Lepantalo M, Lindgren L, Lindfors O. Cardiac arrhythmias and myocar-dial ischemia after thoracotomy for lung cancer. Ann Thoracic Surg 1992; 53: 642–647.
17 Amar D, Roistacher N, Burt M, Reinsel RA, Ginsberg RJ, Wilson RS. Clinical and echocar-diographic correlates of symptomatic tachydysrhythmias after noncardiac thoracicsurgery. Chest 1995; 108: 349–354.
18 Reed CE, Spinale FG, Crawford FA Jr. Effect of pulmonary resection on right ventricularfunction. Ann Thoracic Surg 1992; 53: 578–582.
19 Reed CE, Dorman BH, Spinale FG. Assessment of right ventricular contractile perform-ance after pulmonary resection. Ann Thoracic Surg 1993; 56: 426–431; discussion 431–432.
20 Van Mieghem W, Coolen L, Malysse I, Lacquet LM, Deneffe GJ, Demedts MG.Amiodarone and the development of ARDS after lung surgery. Chest 1994; 105: 1642–1645.
21 Daoud EG, Strickberger SA, Man KC et al. Preoperative amiodarone as prophylaxisagainst atrial fibrillation after heart surgery. N Engl J Med 1997; 337: 1785–1791.
22 Rady MY, Ryan T, Starr NJ. Preoperative therapy with amiodarone and the incidence ofacute organ dysfunction after cardiac surgery. Anesth Analg 1997; 85: 489–497.
23 Dimopoulou I, Marathias K, Daganou M et al. Low-dose amiodarone-related complica-tions after cardiac operations. J Thorac Cardiovasc Surg 1997; 114: 31–37.
24 Keagy BA, Lores ME, Starek PJ, Murray GF, Lucas CL, Wilcox BR. Elective pulmonarylobectomy: factors associated with morbidity and operative mortality. Ann Thorac Surg1985; 40: 349–352.
64 Chapter 3
25 Ritchie AJ, Bowe P, Gibbons JR. Prophylactic digitalization for thoracotomy: a reassess-ment. Ann Thorac Surg 1990; 50: 86–88.
26 Ritchie AJ, Tolan M, Whiteside M, McGuigan JA, Gibbons JR. Prophylactic digitalizationfails to control dysrhythmia in thoracic esophageal operations. Ann Thorac Surg 1993; 55:86–88.
27 Amar D, Roistacher N, Burt ME et al. Effects of diltiazem versus digoxin on dysrhythmiasand cardiac function after pneumonectomy. Ann Thorac Surg 1997; 63: 1374–1381; dis-cussion 1381–1382.
28 Borgeat A, Petropoulos P, Cavin R, Biollaz J, Munafo A, Schwander D. Prevention ofarrhythmias after noncardiac thoracic operations: flecainide versus digoxin. Ann ThoracSurg 1991; 51: 964–967; discussion 967–968.
29 Bayliff CD, Massel DR, Inculet RI et al. Propranolol for the prevention of postoperativearrhythmias in general thoracic surgery. Ann Thorac Surg 1999; 67: 182–186.
PART I I
Complications of generalthoracic surgery


CHAPTER 4
Complications of pulmonary resection
Stephen J Burke, L Penfield Faber
The avoidance of postoperative complications after pulmonary resectionremains the goal of every thoracic surgeon. Many risk factors may contributeto the development of postoperative complications (Table 4.1). The major complications that more frequently occur are listed in Table 4.2. Intraoperat-ive prevention, prompt diagnosis, and appropriate treatment will decreasemorbidity. The following discussion will review common complicationswhich need to be recognized early and managed efficiently in a busy thoracicservice.
Atelectasis
Partial or complete collapse of a segment of lung due to atelectasis andretained secretions plagues to some degree many pulmonary resections. Theincidence of postoperative atelectasis varies in the literature with a range from10% to 70% [1]. Atelectasis is one of the most common complications followingthoracic surgery; the most average incidence being 20–30%. We reviewed ourcomplications following pulmonary resection from 1 January 1994 to 1 January1999. There were 194 complications in 1243 resections. Nearly 10% of postoper-ative complications requiring further intervention were due to atelectasis orretained secretions (Table 4.3).
67
Table 4.1 Risk factors for postoperative complications.
1 Extensive resection2 Right side vs. left side3 Diagnosis: inflammatory or cancer vs. benign4 Sex: male vs. female5 Adjuvant chemoradiation therapy6 FEV1 < 800 ml7 Dlco < 70%8 Comorbidity: CAD, COPD, poor nutrition9 Preoperative steroid use
10 Postoperative infection11 Prolonged ventilatory support12 Surgical technique
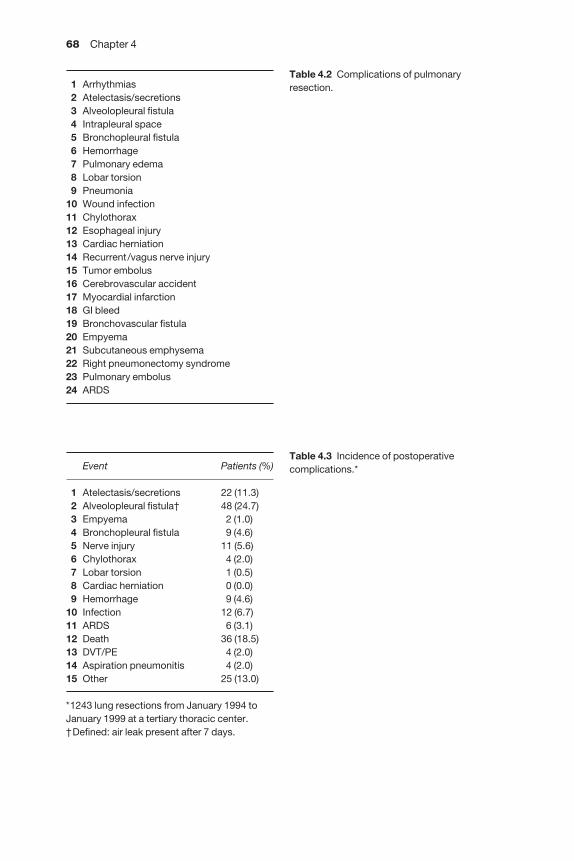
68 Chapter 4
1 Arrhythmias2 Atelectasis/secretions3 Alveolopleural fistula4 Intrapleural space5 Bronchopleural fistula6 Hemorrhage7 Pulmonary edema8 Lobar torsion9 Pneumonia
10 Wound infection11 Chylothorax12 Esophageal injury13 Cardiac herniation14 Recurrent/vagus nerve injury15 Tumor embolus16 Cerebrovascular accident17 Myocardial infarction18 GI bleed19 Bronchovascular fistula20 Empyema21 Subcutaneous emphysema22 Right pneumonectomy syndrome23 Pulmonary embolus24 ARDS
Event Patients (%)
1 Atelectasis/secretions 22 (11.3)2 Alveolopleural fistula† 48 (24.7)3 Empyema 2 (1.0)4 Bronchopleural fistula 9 (4.6)5 Nerve injury 11 (5.6)6 Chylothorax 4 (2.0)7 Lobar torsion 1 (0.5)8 Cardiac herniation 0 (0.0)9 Hemorrhage 9 (4.6)
10 Infection 12 (6.7)11 ARDS 6 (3.1)12 Death 36 (18.5)13 DVT/PE 4 (2.0)14 Aspiration pneumonitis 4 (2.0)15 Other 25 (13.0)
*1243 lung resections from January 1994 toJanuary 1999 at a tertiary thoracic center.†Defined: air leak present after 7 days.
Table 4.2 Complications of pulmonaryresection.
Table 4.3 Incidence of postoperativecomplications.*
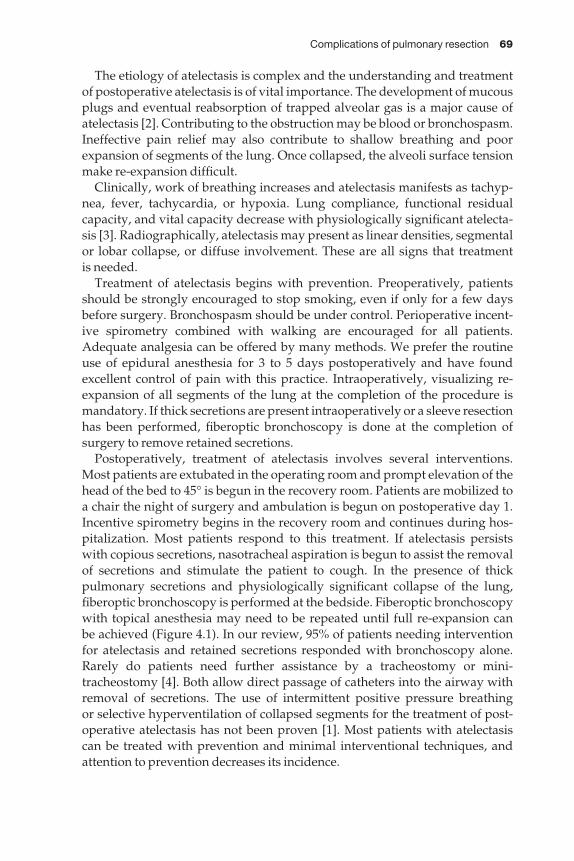
Complications of pulmonary resection 69
The etiology of atelectasis is complex and the understanding and treatmentof postoperative atelectasis is of vital importance. The development of mucousplugs and eventual reabsorption of trapped alveolar gas is a major cause ofatelectasis [2]. Contributing to the obstruction may be blood or bronchospasm.Ineffective pain relief may also contribute to shallow breathing and poorexpansion of segments of the lung. Once collapsed, the alveoli surface tensionmake re-expansion difficult.
Clinically, work of breathing increases and atelectasis manifests as tachyp-nea, fever, tachycardia, or hypoxia. Lung compliance, functional residualcapacity, and vital capacity decrease with physiologically significant atelecta-sis [3]. Radiographically, atelectasis may present as linear densities, segmentalor lobar collapse, or diffuse involvement. These are all signs that treatment is needed.
Treatment of atelectasis begins with prevention. Preoperatively, patientsshould be strongly encouraged to stop smoking, even if only for a few daysbefore surgery. Bronchospasm should be under control. Perioperative incent-ive spirometry combined with walking are encouraged for all patients.Adequate analgesia can be offered by many methods. We prefer the routineuse of epidural anesthesia for 3 to 5 days postoperatively and have foundexcellent control of pain with this practice. Intraoperatively, visualizing re-expansion of all segments of the lung at the completion of the procedure ismandatory. If thick secretions are present intraoperatively or a sleeve resectionhas been performed, fiberoptic bronchoscopy is done at the completion ofsurgery to remove retained secretions.
Postoperatively, treatment of atelectasis involves several interventions.Most patients are extubated in the operating room and prompt elevation of thehead of the bed to 45° is begun in the recovery room. Patients are mobilized toa chair the night of surgery and ambulation is begun on postoperative day 1.Incentive spirometry begins in the recovery room and continues during hos-pitalization. Most patients respond to this treatment. If atelectasis persists with copious secretions, nasotracheal aspiration is begun to assist the removal of secretions and stimulate the patient to cough. In the presence of thick pulmonary secretions and physiologically significant collapse of the lung,fiberoptic bronchoscopy is performed at the bedside. Fiberoptic bronchoscopywith topical anesthesia may need to be repeated until full re-expansion can be achieved (Figure 4.1). In our review, 95% of patients needing interventionfor atelectasis and retained secretions responded with bronchoscopy alone.Rarely do patients need further assistance by a tracheostomy or mini-tracheostomy [4]. Both allow direct passage of catheters into the airway withremoval of secretions. The use of intermittent positive pressure breathing or selective hyperventilation of collapsed segments for the treatment of post-operative atelectasis has not been proven [1]. Most patients with atelectasis can be treated with prevention and minimal interventional techniques, andattention to prevention decreases its incidence.
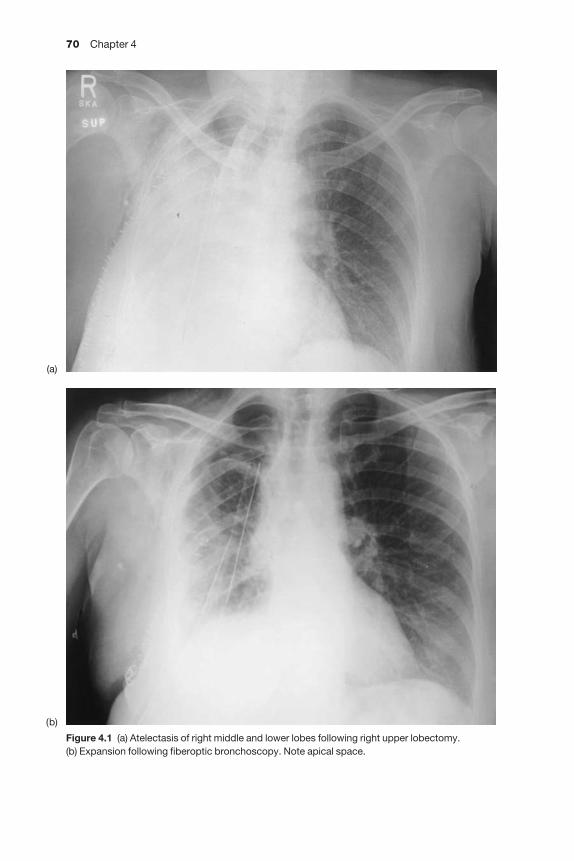
70 Chapter 4
Figure 4.1 (a) Atelectasis of right middle and lower lobes following right upper lobectomy. (b) Expansion following fiberoptic bronchoscopy. Note apical space.
(a)
(b)
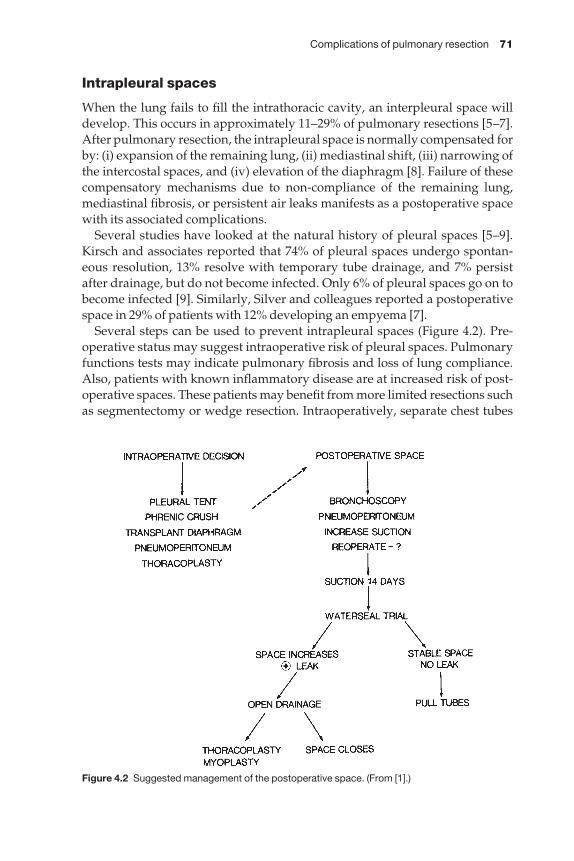
Complications of pulmonary resection 71
Intrapleural spaces
When the lung fails to fill the intrathoracic cavity, an interpleural space willdevelop. This occurs in approximately 11–29% of pulmonary resections [5–7].After pulmonary resection, the intrapleural space is normally compensated forby: (i) expansion of the remaining lung, (ii) mediastinal shift, (iii) narrowing ofthe intercostal spaces, and (iv) elevation of the diaphragm [8]. Failure of thesecompensatory mechanisms due to non-compliance of the remaining lung,mediastinal fibrosis, or persistent air leaks manifests as a postoperative spacewith its associated complications.
Several studies have looked at the natural history of pleural spaces [5–9].Kirsch and associates reported that 74% of pleural spaces undergo spontan-eous resolution, 13% resolve with temporary tube drainage, and 7% persistafter drainage, but do not become infected. Only 6% of pleural spaces go on tobecome infected [9]. Similarly, Silver and colleagues reported a postoperativespace in 29% of patients with 12% developing an empyema [7].
Several steps can be used to prevent intrapleural spaces (Figure 4.2). Pre-operative status may suggest intraoperative risk of pleural spaces. Pulmonaryfunctions tests may indicate pulmonary fibrosis and loss of lung compliance.Also, patients with known inflammatory disease are at increased risk of post-operative spaces. These patients may benefit from more limited resections suchas segmentectomy or wedge resection. Intraoperatively, separate chest tubes
Figure 4.2 Suggested management of the postoperative space. (From [1].)
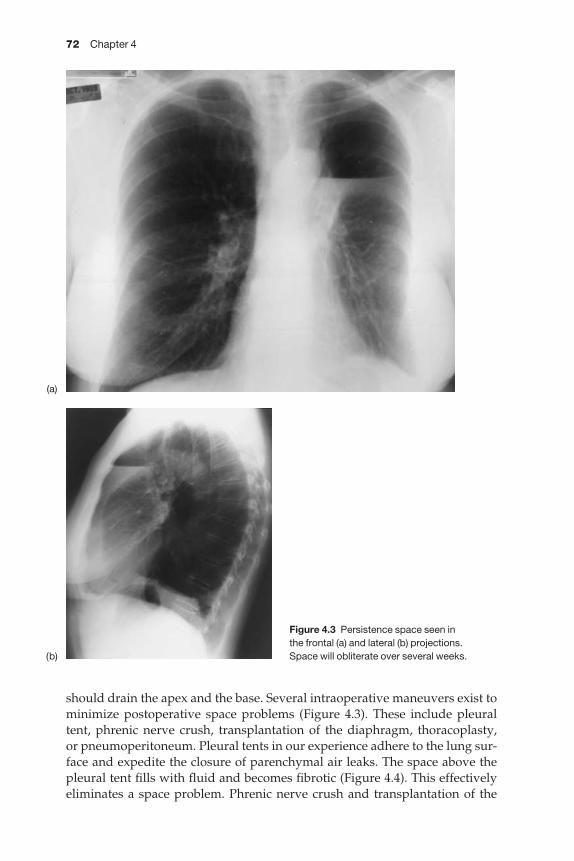
72 Chapter 4
should drain the apex and the base. Several intraoperative maneuvers exist tominimize postoperative space problems (Figure 4.3). These include pleuraltent, phrenic nerve crush, transplantation of the diaphragm, thoracoplasty, or pneumoperitoneum. Pleural tents in our experience adhere to the lung sur-face and expedite the closure of parenchymal air leaks. The space above thepleural tent fills with fluid and becomes fibrotic (Figure 4.4). This effectivelyeliminates a space problem. Phrenic nerve crush and transplantation of the
Figure 4.3 Persistence space seen in the frontal (a) and lateral (b) projections. Space will obliterate over several weeks.
(a)
(b)
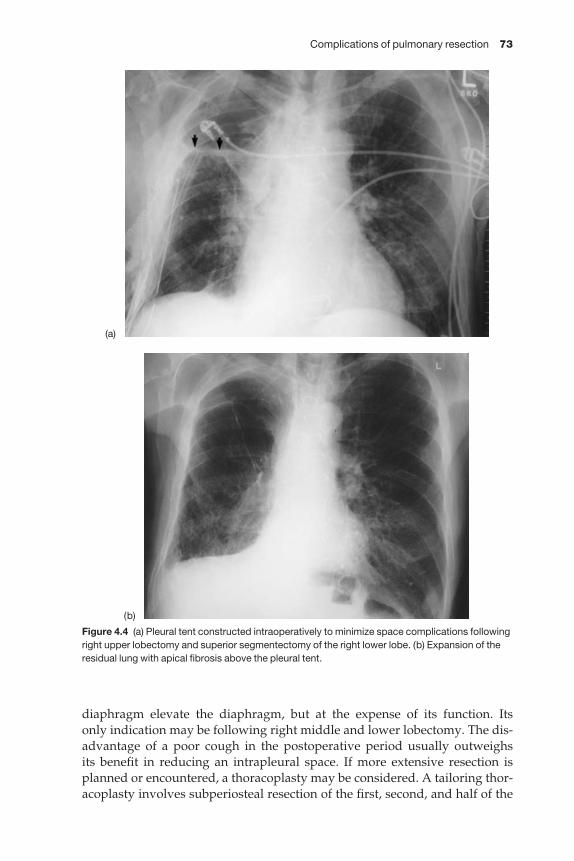
Complications of pulmonary resection 73
diaphragm elevate the diaphragm, but at the expense of its function. Its only indication may be following right middle and lower lobectomy. The dis-advantage of a poor cough in the postoperative period usually outweighs its benefit in reducing an intrapleural space. If more extensive resection isplanned or encountered, a thoracoplasty may be considered. A tailoring thor-acoplasty involves subperiosteal resection of the first, second, and half of the
Figure 4.4 (a) Pleural tent constructed intraoperatively to minimize space complications followingright upper lobectomy and superior segmentectomy of the right lower lobe. (b) Expansion of theresidual lung with apical fibrosis above the pleural tent.
(a)
(b)
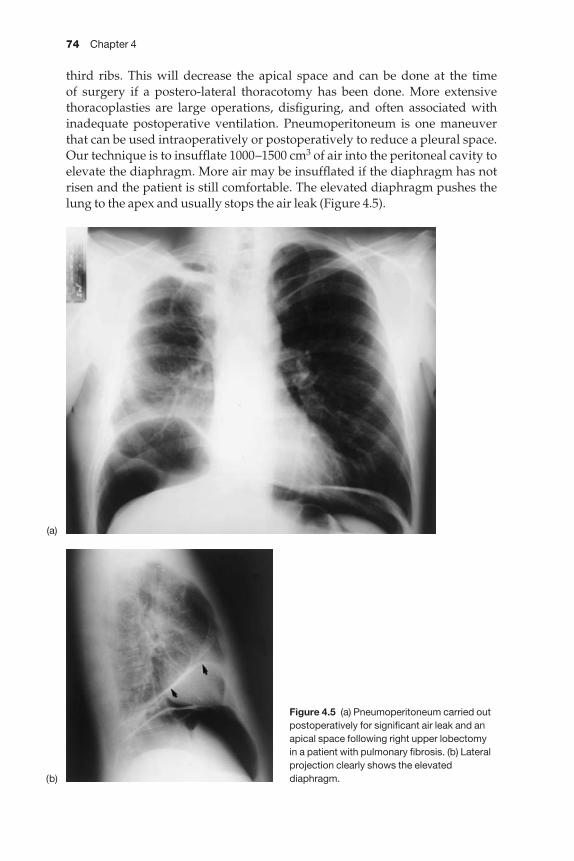
74 Chapter 4
third ribs. This will decrease the apical space and can be done at the time of surgery if a postero-lateral thoracotomy has been done. More extensive thoracoplasties are large operations, disfiguring, and often associated withinadequate postoperative ventilation. Pneumoperitoneum is one maneuverthat can be used intraoperatively or postoperatively to reduce a pleural space.Our technique is to insufflate 1000–1500 cm3 of air into the peritoneal cavity toelevate the diaphragm. More air may be insufflated if the diaphragm has notrisen and the patient is still comfortable. The elevated diaphragm pushes thelung to the apex and usually stops the air leak (Figure 4.5).
Figure 4.5 (a) Pneumoperitoneum carried outpostoperatively for significant air leak and anapical space following right upper lobectomy in a patient with pulmonary fibrosis. (b) Lateralprojection clearly shows the elevateddiaphragm.
(a)
(b)
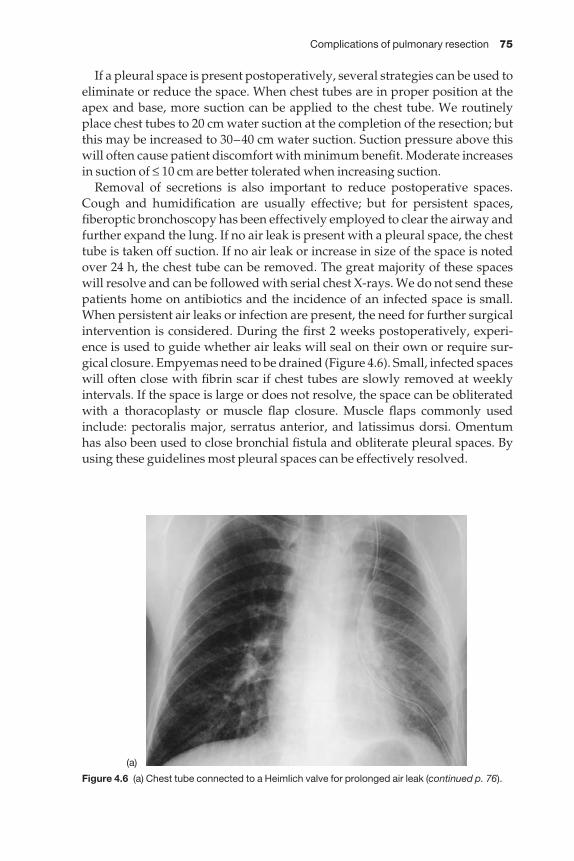
Complications of pulmonary resection 75
If a pleural space is present postoperatively, several strategies can be used toeliminate or reduce the space. When chest tubes are in proper position at theapex and base, more suction can be applied to the chest tube. We routinelyplace chest tubes to 20 cm water suction at the completion of the resection; butthis may be increased to 30–40 cm water suction. Suction pressure above thiswill often cause patient discomfort with minimum benefit. Moderate increasesin suction of ≤ 10 cm are better tolerated when increasing suction.
Removal of secretions is also important to reduce postoperative spaces.Cough and humidification are usually effective; but for persistent spaces,fiberoptic bronchoscopy has been effectively employed to clear the airway andfurther expand the lung. If no air leak is present with a pleural space, the chesttube is taken off suction. If no air leak or increase in size of the space is notedover 24 h, the chest tube can be removed. The great majority of these spaceswill resolve and can be followed with serial chest X-rays. We do not send thesepatients home on antibiotics and the incidence of an infected space is small.When persistent air leaks or infection are present, the need for further surgicalintervention is considered. During the first 2 weeks postoperatively, experi-ence is used to guide whether air leaks will seal on their own or require sur-gical closure. Empyemas need to be drained (Figure 4.6). Small, infected spaceswill often close with fibrin scar if chest tubes are slowly removed at weeklyintervals. If the space is large or does not resolve, the space can be obliteratedwith a thoracoplasty or muscle flap closure. Muscle flaps commonly usedinclude: pectoralis major, serratus anterior, and latissimus dorsi. Omentumhas also been used to close bronchial fistula and obliterate pleural spaces. Byusing these guidelines most pleural spaces can be effectively resolved.
Figure 4.6 (a) Chest tube connected to a Heimlich valve for prolonged air leak (continued p. 76).
(a)
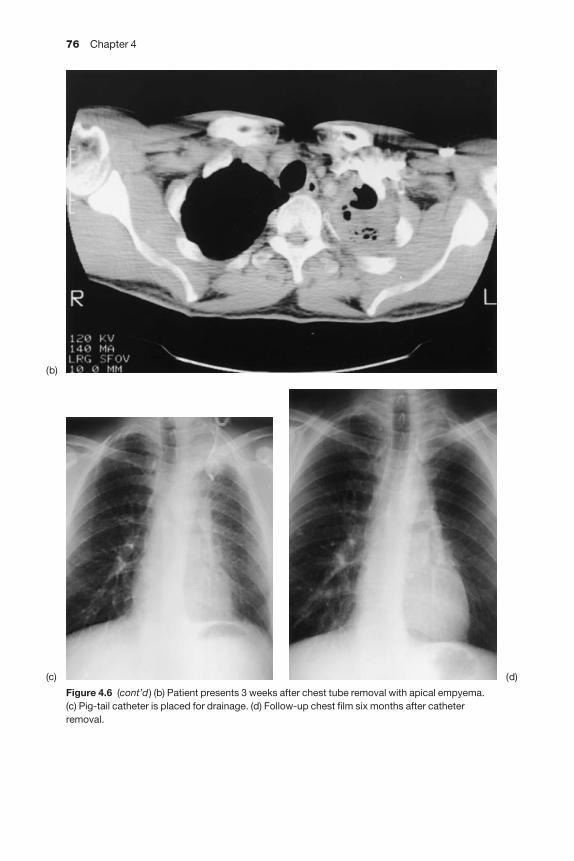
76 Chapter 4
Figure 4.6 (cont’d) (b) Patient presents 3 weeks after chest tube removal with apical empyema.(c) Pig-tail catheter is placed for drainage. (d) Follow-up chest film six months after catheterremoval.
(b)
(c) (d)
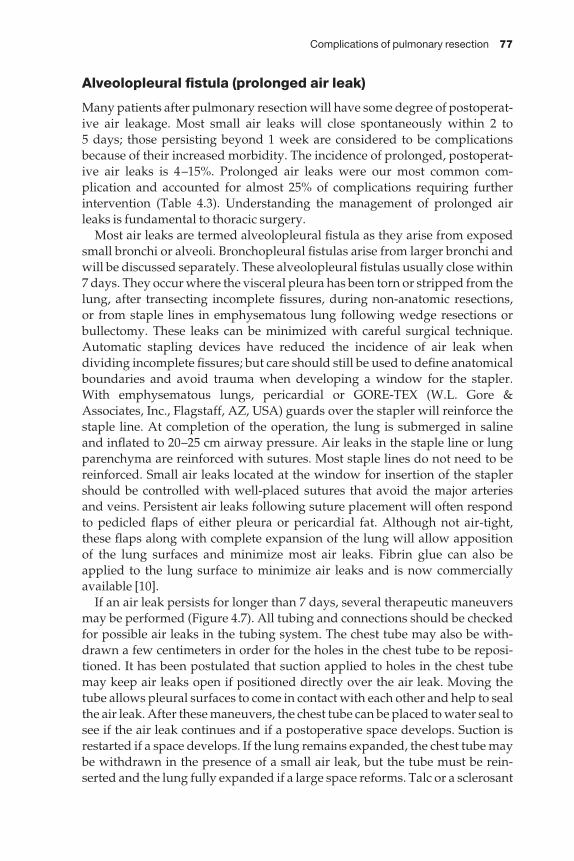
Complications of pulmonary resection 77
Alveolopleural fistula (prolonged air leak)
Many patients after pulmonary resection will have some degree of postoperat-ive air leakage. Most small air leaks will close spontaneously within 2 to 5 days; those persisting beyond 1 week are considered to be complicationsbecause of their increased morbidity. The incidence of prolonged, postoperat-ive air leaks is 4–15%. Prolonged air leaks were our most common com-plication and accounted for almost 25% of complications requiring furtherintervention (Table 4.3). Understanding the management of prolonged airleaks is fundamental to thoracic surgery.
Most air leaks are termed alveolopleural fistula as they arise from exposedsmall bronchi or alveoli. Bronchopleural fistulas arise from larger bronchi andwill be discussed separately. These alveolopleural fistulas usually close within7 days. They occur where the visceral pleura has been torn or stripped from thelung, after transecting incomplete fissures, during non-anatomic resections, or from staple lines in emphysematous lung following wedge resections orbullectomy. These leaks can be minimized with careful surgical technique.Automatic stapling devices have reduced the incidence of air leak when dividing incomplete fissures; but care should still be used to define anatomicalboundaries and avoid trauma when developing a window for the stapler.With emphysematous lungs, pericardial or GORE-TEX (W.L. Gore &Associates, Inc., Flagstaff, AZ, USA) guards over the stapler will reinforce thestaple line. At completion of the operation, the lung is submerged in saline and inflated to 20–25 cm airway pressure. Air leaks in the staple line or lungparenchyma are reinforced with sutures. Most staple lines do not need to bereinforced. Small air leaks located at the window for insertion of the staplershould be controlled with well-placed sutures that avoid the major arteriesand veins. Persistent air leaks following suture placement will often respondto pedicled flaps of either pleura or pericardial fat. Although not air-tight,these flaps along with complete expansion of the lung will allow apposition of the lung surfaces and minimize most air leaks. Fibrin glue can also beapplied to the lung surface to minimize air leaks and is now commerciallyavailable [10].
If an air leak persists for longer than 7 days, several therapeutic maneuversmay be performed (Figure 4.7). All tubing and connections should be checkedfor possible air leaks in the tubing system. The chest tube may also be with-drawn a few centimeters in order for the holes in the chest tube to be reposi-tioned. It has been postulated that suction applied to holes in the chest tubemay keep air leaks open if positioned directly over the air leak. Moving thetube allows pleural surfaces to come in contact with each other and help to sealthe air leak. After these maneuvers, the chest tube can be placed to water seal tosee if the air leak continues and if a postoperative space develops. Suction isrestarted if a space develops. If the lung remains expanded, the chest tube maybe withdrawn in the presence of a small air leak, but the tube must be rein-serted and the lung fully expanded if a large space reforms. Talc or a sclerosant
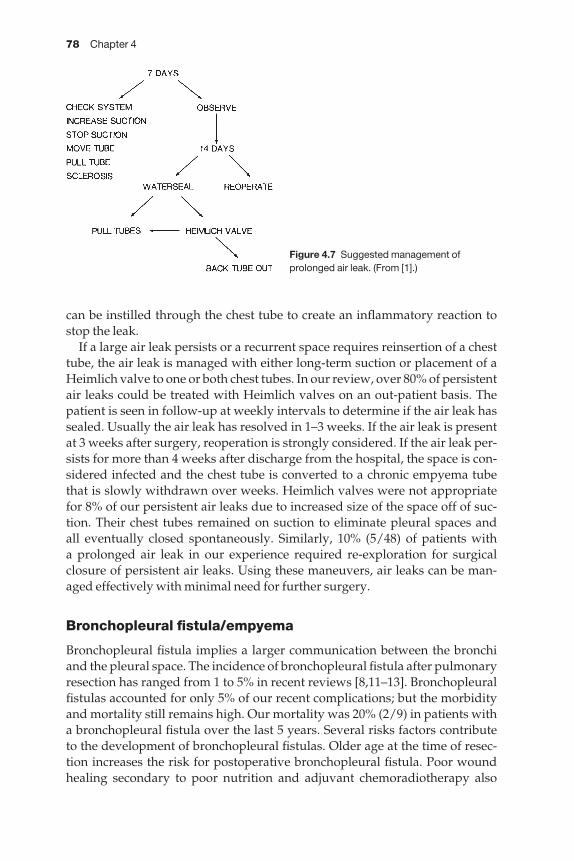
78 Chapter 4
can be instilled through the chest tube to create an inflammatory reaction tostop the leak.
If a large air leak persists or a recurrent space requires reinsertion of a chesttube, the air leak is managed with either long-term suction or placement of aHeimlich valve to one or both chest tubes. In our review, over 80% of persistentair leaks could be treated with Heimlich valves on an out-patient basis. Thepatient is seen in follow-up at weekly intervals to determine if the air leak hassealed. Usually the air leak has resolved in 1–3 weeks. If the air leak is presentat 3 weeks after surgery, reoperation is strongly considered. If the air leak per-sists for more than 4 weeks after discharge from the hospital, the space is con-sidered infected and the chest tube is converted to a chronic empyema tubethat is slowly withdrawn over weeks. Heimlich valves were not appropriatefor 8% of our persistent air leaks due to increased size of the space off of suc-tion. Their chest tubes remained on suction to eliminate pleural spaces and all eventually closed spontaneously. Similarly, 10% (5/48) of patients with a prolonged air leak in our experience required re-exploration for surgical closure of persistent air leaks. Using these maneuvers, air leaks can be man-aged effectively with minimal need for further surgery.
Bronchopleural fistula/empyema
Bronchopleural fistula implies a larger communication between the bronchiand the pleural space. The incidence of bronchopleural fistula after pulmonaryresection has ranged from 1 to 5% in recent reviews [8,11–13]. Bronchopleuralfistulas accounted for only 5% of our recent complications; but the morbidityand mortality still remains high. Our mortality was 20% (2/9) in patients witha bronchopleural fistula over the last 5 years. Several risks factors contribute to the development of bronchopleural fistulas. Older age at the time of resec-tion increases the risk for postoperative bronchopleural fistula. Poor woundhealing secondary to poor nutrition and adjuvant chemoradiotherapy also
Figure 4.7 Suggested management ofprolonged air leak. (From [1].)
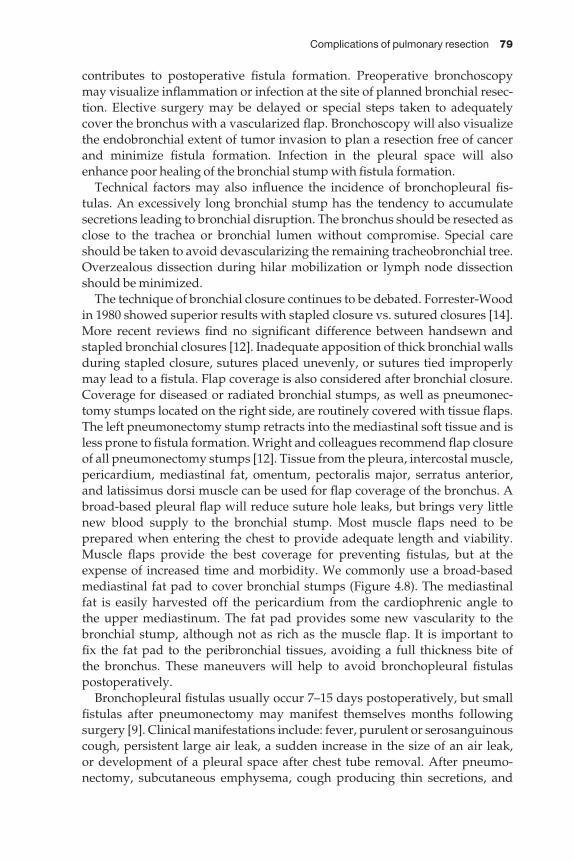
Complications of pulmonary resection 79
contributes to postoperative fistula formation. Preoperative bronchoscopymay visualize inflammation or infection at the site of planned bronchial resec-tion. Elective surgery may be delayed or special steps taken to adequatelycover the bronchus with a vascularized flap. Bronchoscopy will also visualizethe endobronchial extent of tumor invasion to plan a resection free of cancerand minimize fistula formation. Infection in the pleural space will alsoenhance poor healing of the bronchial stump with fistula formation.
Technical factors may also influence the incidence of bronchopleural fis-tulas. An excessively long bronchial stump has the tendency to accumulatesecretions leading to bronchial disruption. The bronchus should be resected asclose to the trachea or bronchial lumen without compromise. Special careshould be taken to avoid devascularizing the remaining tracheobronchial tree.Overzealous dissection during hilar mobilization or lymph node dissectionshould be minimized.
The technique of bronchial closure continues to be debated. Forrester-Woodin 1980 showed superior results with stapled closure vs. sutured closures [14].More recent reviews find no significant difference between handsewn and stapled bronchial closures [12]. Inadequate apposition of thick bronchial wallsduring stapled closure, sutures placed unevenly, or sutures tied improperlymay lead to a fistula. Flap coverage is also considered after bronchial closure.Coverage for diseased or radiated bronchial stumps, as well as pneumonec-tomy stumps located on the right side, are routinely covered with tissue flaps.The left pneumonectomy stump retracts into the mediastinal soft tissue and isless prone to fistula formation. Wright and colleagues recommend flap closureof all pneumonectomy stumps [12]. Tissue from the pleura, intercostal muscle,pericardium, mediastinal fat, omentum, pectoralis major, serratus anterior,and latissimus dorsi muscle can be used for flap coverage of the bronchus. Abroad-based pleural flap will reduce suture hole leaks, but brings very littlenew blood supply to the bronchial stump. Most muscle flaps need to be prepared when entering the chest to provide adequate length and viability.Muscle flaps provide the best coverage for preventing fistulas, but at theexpense of increased time and morbidity. We commonly use a broad-basedmediastinal fat pad to cover bronchial stumps (Figure 4.8). The mediastinal fat is easily harvested off the pericardium from the cardiophrenic angle to the upper mediastinum. The fat pad provides some new vascularity to thebronchial stump, although not as rich as the muscle flap. It is important to fix the fat pad to the peribronchial tissues, avoiding a full thickness bite of the bronchus. These maneuvers will help to avoid bronchopleural fistulaspostoperatively.
Bronchopleural fistulas usually occur 7–15 days postoperatively, but smallfistulas after pneumonectomy may manifest themselves months followingsurgery [9]. Clinical manifestations include: fever, purulent or serosanguinouscough, persistent large air leak, a sudden increase in the size of an air leak, or development of a pleural space after chest tube removal. After pneumo-nectomy, subcutaneous emphysema, cough producing thin secretions, and

80 Chapter 4
increased dyspnea may indicate a bronchopleural fistula. Additional evid-ence of a bronchopleural fistula may be confirmed by chest radiography.Radiographic findings may include: new pleural space; development of an air-fluid level; or, after pneumonectomy, a decrease in the level of fluid on the pneumonectomy side of < 2 cm. These clinical signs suggest the presence of a fistula.
Bronchoscopy should be carried out urgently and often assists with thediagnosis and treatment of bronchopleural fistulas. Large fistulas or completeseparation of the anastomosis can be easily detected. Small fistulas are moredifficult to visualize and may only appear as a back-and-forth motion of secretions, necrotic tissue, inflammation, or granulation tissue at the bronchialstump. Residual tumor, inflammation, or infection of the proximal bronchusare also important to note if bronchial closure is being considered.
Treatment is dependent on the timing and circumstances of the bron-chopleural fistula. Approximately 20–30% of small fistulas will close withdrainage alone following pneumonectomy [9,15]. Results with conservativetreatment are usually better following lobectomy than pneumonectomy.Fistulas after lobectomy are rare and usually occur after bilobectomy ratherthan standard lobectomy. Increased dissection for a bilobectomy may devas-cularize the bronchial stump, stressing the importance of careful closure and bronchial artery preservation in these circumstances. Surgical repair of a lobar bronchial fistula may require resection, if not, pneumonectomy. This
Figure 4.8 Mediastinal fat pad sutured in placed to cover a right pneumonectomy stump. (From [8].)
Complications of pulmonary resection 81
major surgery in a compromised patient and probable infection in the pleuralspace must be carefully weighed against the benefits of surgical closure.Conservative treatment is recommended for lobar bronchial fistula. This con-sists of tube drainage and space closure with a pedicled muscle flap.
Timing is critical when a bronchopleural fistula is diagnosed. The spaceshould be urgently drained with a chest tube to prevent aspiration of fluid intothe remaining lung and appropriate antibiotics are begun to treat the under-lying empyema. Chest tubes are placed to water-seal drainage without suctionto minimize loss of tidal volume. Previously, primary closure of bronchopleu-ral fistulas was recommended after only 48–72 h. With better antibiotics, irriga-tion treatment for empyema, and vascularized stump coverage, reoperationand reclosure of the bronchial stump can be considered up to 14 days after theoriginal pneumonectomy [8]. A single lumen endotracheal tube placed intothe contralateral bronchus under bronchoscopic guidance is used to preventaspiration into the dependent lung during operative positioning. The tech-nique of repair of the bronchial stump includes careful debridement and theuse of monofilament sutures to re-approximate the bronchus. A vascularizedflap, as previously discussed, is then used to cover the bronchial stump.Recently, Landreneau and colleagues have described the technique of video-assisted thoracoscopy (VATS) to treat empyemas [16]. They successfullyclosed the fistula and drained the infection in 98% of patients with VATS treat-ment alone when the empyema was treated early in the ‘fibrinopurulent’phase. Early diagnosis and prompt treatment are paramount in the manage-ment of bronchopleural fistula and associated empyema.
The management of a bronchopleural fistula that occurs several weeks or months after pneumonectomy requires the space to be drained and theinfection controlled. This is best accomplished with the open thoracostomy orEloesser flap [17]. The presence of a chronic bronchopleural fistula requiresdirect closure as the fistula will not heal spontaneously and the pneumonec-tomy space cannot be sterilized until the fistula has healed. Puskas [18]described successful closure of chronic bronchopleural fistulas followingpneumonectomy in 47 patients (85%) using direct suture closure of thebronchial stump in 37 and suturing of tissue flaps over the fistula in 10 patients. All of these bronchial closures were buttressed with vascularizedflaps of omentum, muscle or pleura. At the time of the bronchopleural fistulaclosure, the empyema cavity can also be partially obliterated using myoplastyand thoracoplasty techniques. Any residual cavity that remains can be success-fully sterilized using the Claggett technique [19]. This antibiotic irrigationtechnique can be accomplished after the fistula is closed. It consists of irriga-tion of the empyema space with antibiotics and packing the space with sterilegauze to achieve healthy granulation tissue. When the cavity is clean, thepatient is brought to surgery and the cavity is filled with an antibiotic solutionand the open thoracostomy or Eloesser flap is closed. Approximately 60% ofempyemas can be sterilized with this technique, but a repeat procedure may berequired if the empyema recurs.
82 Chapter 4
A two-stage procedure is advocated by Deschamps [20] for fistula closureand sterilization of a pneumonectomy empyema space. The first stage consistsof opening the thoracotomy incision with debridement and closure of thebronchial fistula and coverage with viable tissue. The empyema cavity is thor-oughly debrided and the cavity is packed open with gauze soaked in Povidoneiodine solution, diluted 20: 1. The packing is changed daily and when healthygranulation appears in the pleural space, the cavity is filled with antibioticsolution and a watertight chest wall closure is obtained. Satisfactory results arenoted to be achieved in 80% of patients.
If antibiotic irrigation and open thoracostomy closure fail to sterilize theempyema cavity, it can be managed with daily packing with expecteddecrease in size of the space by granulation tissue over several months.Pairolero [21] reported the use of muscle flaps along with omentum to achievean 88% success rate in controlling intrathoracic empyema. Extrathoracic mus-cle transpositions, along with omentum, are now the accepted standard of therapy for treatment of the chronic bronchopleural fistula and empyema.The need for thoracoplasty has been significantly decreased with thesedescribed techniques.
Other techniques are available to attempt to close a post-pneumonectomybronchial fistula. If a long bronchial stump is present the trans-sternalapproach can be utilized as described by Baldwin and Mark [22]. The bronchusis approached through the pericardium and stapled and transected. Followingclosure of the bronchus the empyema cavity is treated by antibiotic irrigationtechniques.
Fibrin glue can be used to close a small bronchial fistula up to 4 mm in size.Tissue glue can be made from cryoprecipitate and thrombin. Commerciallymade glues are available. Closure of small fistulas in both pneumonectomyand lobar stumps has been achieved [23]. The glue is instilled throughcatheters passed through the channel of a fiberoptic bronchoscope. This tech-nique is associated with low morbidity and can be the initial therapeuticmaneuver if the procedure is small. Fewer than 10% of our most recent bron-chopleural fistulas were candidates for closure with fibrin glue.
Chylothorax
Chylothorax is a rare complication after pulmonary resection that occurs morecommonly after pneumonectomy than after lobectomy or segmentectomy.Cerfolio and associates found an incidence of < 0.5% for all thoracic cases [24].Chylothorax is more common after esophageal surgery, accounting for almosttwo-thirds of the reported experience. Thoracic duct injury accounted for 2%of our recent complications. Resection of large central tumors and extensivelymphadenectomy increase the possibility of thoracic duct injury.
Knowledge of the anatomy of the thoracic duct may prevent its injury andaid in its treatment. The thoracic duct begins as the cisterna chyli at the level ofthe second lumbar vertebrae, just lateral to the aorta. The most constant loca-

Complications of pulmonary resection 83
tion of the thoracic duct is at the diaphragm where it passes through the aortichiatus with the aorta and azygous vein [25]. Often the favored site for electiveligation of the duct is here during its more constant path through the aortic hia-tus. The thoracic duct then ascends to the right side of the aorta and anterior tothe vertebrae. The duct crosses to the left side at the level of the fifth or sixththoracic vertebrae. It remains posterior to the aortic arch and adjacent to theesophagus before it empties into the junction of the left subclavian and internaljugular veins. Almost 40% of individuals have multiple branches that are mostcommon in the mid-thoracic region. Injury can occur anywhere in the medi-astinum, but this variability makes injury more common. The close proximityto the esophagus and subcarinal space on the right make extensive lympha-denectomy in these areas prone to thoracic duct injury. Damage can also occuron the left side after the duct has crossed the thorax. Mobilization of the leftmain-stem bronchus or removal of lymph nodes along the left tracheo–esophageal groove may injure the thoracic duct. A knowledge of the locationof the thoracic duct may prevent this complication.
A chylous leak can often be diagnosed intraoperatively. Because the patienthas not eaten the day of surgery, chyle from a ductal injury may appear thinand clear rather than milky. If golden-yellow fluid continues to fill the operat-ive space, the surgeon should consider a possible thoracic duct injury andattempt to identify its site. Administration of cream or milk down a nasogas-tric tube may help to identify the leak. Whenever the ductal injury is identifiedintraoperatively, the injury should be repaired with fine interrupted perman-ent sutures.
Many thoracic duct injuries are not identified until postoperatively. Becausepatients often do not eat postoperatively, the classic milky appearance of thepleural drainage is often absent. However, continuation of large amounts of pleural drainage should raise the suspicion of a ductal injury. Chest tubeoutputs measuring > 500 cm3/day are typical of chylous effusions. After thepatient resumes a general diet, the milky appearance of the pleural fluid maybecome evident. It should be analyzed for cholesterol and triglycerides if thediagnosis is in question. Chyle typically has elevated cholesterol and triglyc-eride levels. Staats [26] in 1980 reported if the triglyceride level is > 110 mg/100 cm3, then there is a 99% chance that the effusion is chyle. Similarly, if thetriglyceride level is < 50 mg/100 cm3, there is only a 5% chance that the pleuralfluid is chyle. Large amounts of chest tube drainage confirmed by laboratorystudies can identify chylous effusions.
The initial treatment of a thoracic duct injury is conservative. If not present,chest tubes are placed to drain the involved pleural space completely andallow expansion of the lung. The chest tube output must be accurately meas-ured. A trial with a specialized diet containing no fat and medium-chaintriglycerides may be tried. A more conservative approach is allowing nothingorally and providing complete nutrition by central hyperalimentation. Thesuccess of this conservative approach varies. Cerfolio found non-operativetherapy to be successful in 27% of patients [24]. Others have reported success
84 Chapter 4
in close to half of patients with conservative therapy [8]. We found that 75%responded to non-operative treatment in our last review.
Guidelines for conservative management of thoracic duct injuries arebecoming better defined. Because of the depletion of the patient’s nutritionfrom prolonged drainage and increased risk of infection, conservative man-agement should never exceed 2 weeks’ duration. Earlier surgical interventionhas been advocated by some groups. The Mayo clinic experience suggests thatoutputs > 1000 cm3/day for more than 7 days or any thoracic duct injury afteresophageal surgery should be surgically repaired at 1 week [24]. With the goodresults from surgical ligation and the increased interest in less invasive tech-niques such as thoracoscopy, the trend may be toward earlier intervention atthe time of diagnosis [25].
Surgical management of thoracic duct injuries remains very effective. Thetraditional approach is direct ligation of the duct near the diaphragm througheither a thoracic or abdominal approach. This was first proposed by Lampsonin 1948 and involves mass ligation of the soft tissues that include the thoracicduct between the aorta, azygous vein, and vertebrae at the diaphragm. Clipsshould be avoided because they can injure the duct. Our approach is through a low right thoracotomy, although a left thoracotomy may be used. Surgicalligation is effective in nearly 90–95% of cases. Other approaches have been to enter the chest on the side of the chylous leak. The leak itself is identified and sutured. Identification of the site of leak may be troublesome with thisapproach due to inflamed tissues. Fibrin glue has also been used to seal thor-acic duct leaks and is gaining popularity with thoracoscopic approaches [25].
If primary surgical repair fails in the chest, the thoracic duct may be ligatedthrough the abdomen. In a patient unable to tolerate surgery, pleurodesis maybe attempted but often ineffectively obliterates the pleural space. Pleuroper-itoneal shunts and stops the leak are effective and can prevent malnutrition in patients with advanced cancer causing chylous effusions. These options are rarely needed in postoperative chylous leaks and long term, conservativemanagement should be avoided because of the associated malnutrition, infec-tious complications, and increased mortality.
Cardiac herniation
Cardiac herniation is a rare event after pulmonary resection, but if notpromptly managed is often fatal. The incidence is low and much of our under-standing comes from isolated case reports. We experienced no cases over thelast 5 years. Cardiac herniation is often associated with intrapericardial pneu-monectomy with herniation of the heart through a large pericardial defect.Without prompt recognition and reoperation, death quickly ensues, account-ing for a mortality rate approaching 50% [27]. Understanding of the mech-anism of cardiac herniation may prevent and reduce its mortality.
Cardiac herniation typically occurs shortly after the completion of the pul-monary resection on the operating table or in the immediate postoperative
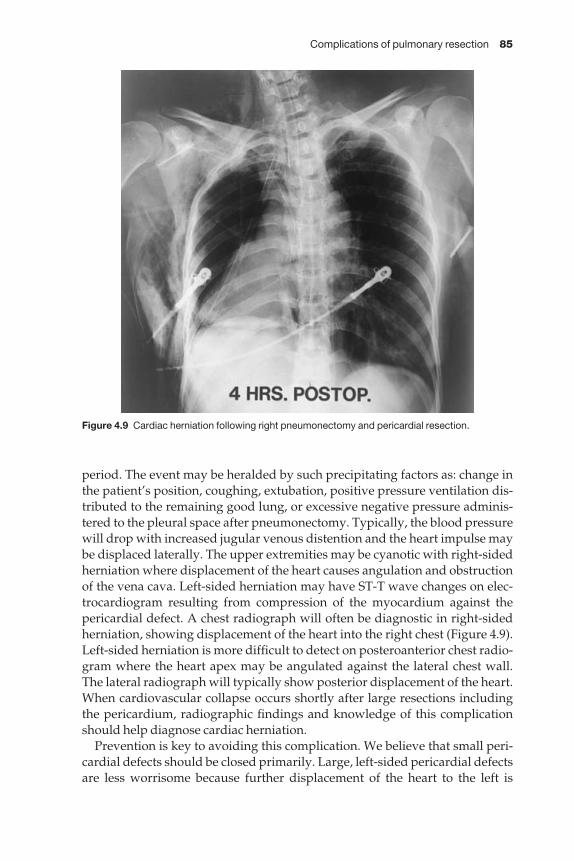
Complications of pulmonary resection 85
period. The event may be heralded by such precipitating factors as: change inthe patient’s position, coughing, extubation, positive pressure ventilation dis-tributed to the remaining good lung, or excessive negative pressure adminis-tered to the pleural space after pneumonectomy. Typically, the blood pressurewill drop with increased jugular venous distention and the heart impulse maybe displaced laterally. The upper extremities may be cyanotic with right-sidedherniation where displacement of the heart causes angulation and obstructionof the vena cava. Left-sided herniation may have ST-T wave changes on elec-trocardiogram resulting from compression of the myocardium against thepericardial defect. A chest radiograph will often be diagnostic in right-sidedherniation, showing displacement of the heart into the right chest (Figure 4.9).Left-sided herniation is more difficult to detect on posteroanterior chest radio-gram where the heart apex may be angulated against the lateral chest wall. The lateral radiograph will typically show posterior displacement of the heart.When cardiovascular collapse occurs shortly after large resections includingthe pericardium, radiographic findings and knowledge of this complicationshould help diagnose cardiac herniation.
Prevention is key to avoiding this complication. We believe that small peri-cardial defects should be closed primarily. Large, left-sided pericardial defectsare less worrisome because further displacement of the heart to the left is
Figure 4.9 Cardiac herniation following right pneumonectomy and pericardial resection.
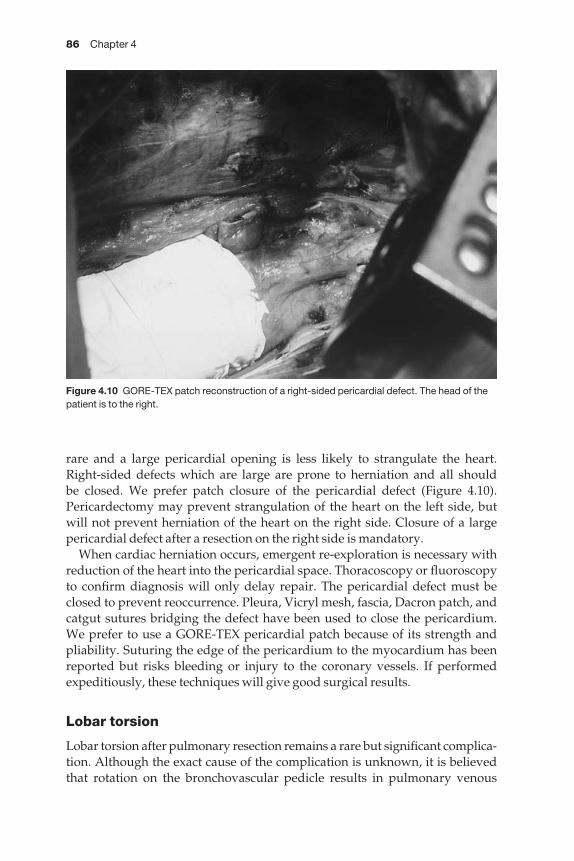
86 Chapter 4
rare and a large pericardial opening is less likely to strangulate the heart.Right-sided defects which are large are prone to herniation and all should be closed. We prefer patch closure of the pericardial defect (Figure 4.10).Pericardectomy may prevent strangulation of the heart on the left side, but will not prevent herniation of the heart on the right side. Closure of a largepericardial defect after a resection on the right side is mandatory.
When cardiac herniation occurs, emergent re-exploration is necessary withreduction of the heart into the pericardial space. Thoracoscopy or fluoroscopyto confirm diagnosis will only delay repair. The pericardial defect must beclosed to prevent reoccurrence. Pleura, Vicryl mesh, fascia, Dacron patch, andcatgut sutures bridging the defect have been used to close the pericardium. We prefer to use a GORE-TEX pericardial patch because of its strength and pliability. Suturing the edge of the pericardium to the myocardium has beenreported but risks bleeding or injury to the coronary vessels. If performedexpeditiously, these techniques will give good surgical results.
Lobar torsion
Lobar torsion after pulmonary resection remains a rare but significant complica-tion. Although the exact cause of the complication is unknown, it is believedthat rotation on the bronchovascular pedicle results in pulmonary venous
Figure 4.10 GORE-TEX patch reconstruction of a right-sided pericardial defect. The head of thepatient is to the right.

Complications of pulmonary resection 87
obstruction and eventual gangrene. Rotation may occur intraoperatively orpostoperatively. Angulation of the bronchus also compromises bronchial arterial circulation and contributes to the lung infarction. Lobar torsion mustbe differentiated from other causes of lobar gangrene such as pulmonary veinthrombosis or pulmonary artery occlusion combined with disruption of thebronchial circulation. Torsion is absent in these cases and circulatory com-promise is usually associated with operative injury. Lobar torsion typicallyinvolves the right middle lobe after a right upper lobectomy. If the transversefissure is complete, the right middle lobe has few attachments to the lower lobeand can move freely. The middle lobe can, then, rotate on its bronchovascularpedicle. Less commonly, lobar torsion can occur on the left side after eitherupper lobectomy or lower lobectomy. In our 5-year review, we identified one case of right middle lobe torsion that required surgical resection. Schulerreviewed lobar torsion and reported a 16% mortality in their 31 cases [28]. If not recognized early, circulatory embarrassment of the lobe can lead toinfarction, lobar gangrene, and increased mortality.
Prevention and early recognition are essential to the management of lobartorsion. In the presence of a complete transverse fissure, the right middle lobe should be secured to the remaining lobe to prevent torsion. Sutures can be used or the distal edges of the lung may be secured with staples. Carefulsurgical technique is mandatory to prevent interrupting circulation to the lung causing lobar gangrene without torsion. At the completion of the resection, the lung should be inspected while fully inflated to prevent intra-operative torsion.
Early recognition of this complication is essential to prevent irreversibleischemia. Clinical symptoms of lobar torsion are few in the early stages. If leftuntreated, these patients become septic and develop fever, massive air leak, or foul smelling sputum or bloody chest tube drainage. A chest radiographtaken postoperatively may show signs of torsion (Figure 4.11). Radiographicfindings may include: hilar displacement, bronchial cut-off, or lobar consolida-tion. Later, the radiograph may show enlargement of the lobe beyond that normally expected from hyperinflation. Over time, the lobe will graduallydecrease in size due to consolidation and have a honeycomb pattern orground-glass appearance [9]. Nuclear perfusion scans and angiography maydemonstrate the obstruction to flow through the main lobar vessels or itsbranches, but are not diagnostic for lobar torsion. Atelectasis and intra-parenchymal hematoma may have the same appearance. Urgent flexible bron-choscopy can be diagnostic and should be considered to identify lobar torsionor more commonly remove mucous plugs from an atelectatic lobe. The bron-choscopic features of lobar torsion are a ‘fish-mouth’ bronchus that allows pas-sage of the bronchoscope, but quickly reobstructs when the bronchoscope isremoved. This compressed bronchus with normal distal airways should raisethe suspicion of lobar torsion and the need for surgical management.
After prompt diagnosis, the treatment of lobar torsion is immediate surgicalre-exploration. If lobar torsion is recognized before pulmonary infarction,
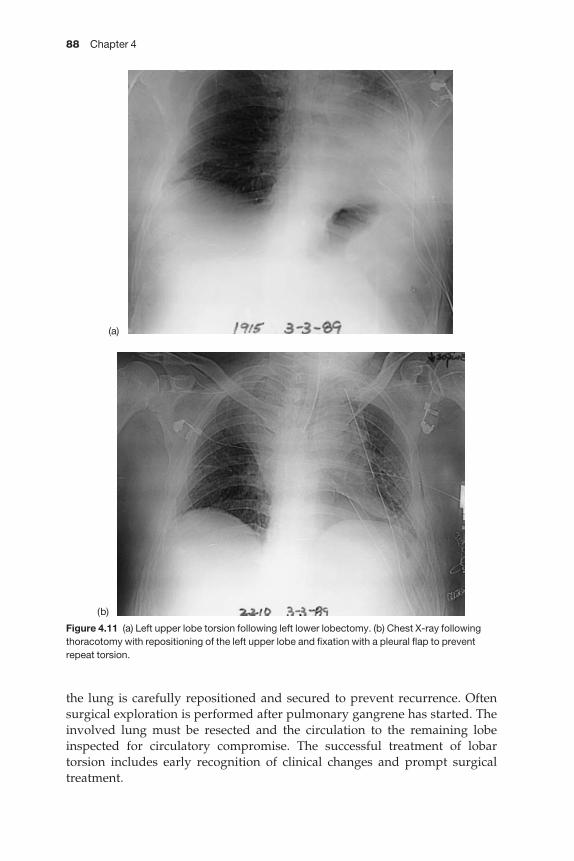
88 Chapter 4
Figure 4.11 (a) Left upper lobe torsion following left lower lobectomy. (b) Chest X-ray followingthoracotomy with repositioning of the left upper lobe and fixation with a pleural flap to preventrepeat torsion.
(a)
(b)
the lung is carefully repositioned and secured to prevent recurrence. Oftensurgical exploration is performed after pulmonary gangrene has started. Theinvolved lung must be resected and the circulation to the remaining lobeinspected for circulatory compromise. The successful treatment of lobar torsion includes early recognition of clinical changes and prompt surgicaltreatment.

Complications of pulmonary resection 89
Nerve injury
The recurrent laryngeal, phrenic and vagus nerves are the nerves most com-monly involved in a thoracic surgical procedure. Each of these nerves can be invaded by a tumor or pathological process and the nerve is resected toachieve a complete resection. Injury to a nerve can also occur with the use ofelectrocautery or resection of tissues in close proximity to the nerve.
The left recurrent laryngeal nerve wraps around the ligamentum arteriosumin the aorto–pulmonary window and can be damaged with lymph node dis-section or during a difficult pneumonectomy. On occasion, the tumor invadesthe vagus nerve above the transverse aortic arch and resection of the vagusnerve with pleurectomy at this level results in vocal cord paralysis. The rightrecurrent laryngeal nerve can be damaged during the superior mediastinallymph node dissection following right-sided lung cancer operations. Shields[29] reported injury to the left recurrent laryngeal nerve in 3/62 patients afterextensive lymph node dissection. Unilateral vocal cord paralysis followingpulmonary resection can be associated acutely with inadequate cough or air-way aspiration. Retained secretions and aspiration can result in significantcomplications, particularly following a pneumonectomy. Signs of vocal cordparalysis include a breathy voice, a poor cough and/or aspiration of liquids.When vocal cord paralysis is known or suspected, fiberoptic visualization ofthe larynx should be carried out to determine the position of the affected vocalcord. A poor cough and aspiration with lateral positioning of the paralyzedvocal cord indicate a need for repositioning of the vocal cord. The paralyzedvocal cord can be repositioned toward the midline by injection of Gelfoampaste into its lateral aspect. This is temporary to achieve an improved coughand to diminish the complications of aspiration. Following discharge thepatients is re-evaluated by fiberoptic techniques and Teflon is then injected forlong-term benefit. Other methods of vocal cord medialization include neuro-muscular transfer and the recently described thyroplasty technique [30].
Sacrifice or injury of the phrenic nerve may manifest itself as an asymp-tomatic elevated diaphragm or an ineffective cough with retained secretions.Special attention must be made to maintain a clear airway in this instance.Injury to a single vagus nerve rarely produces clinical symptoms and the trueincidence of injury to this nerve is unknown. Dissection of apical lung cancerscan result in sacrifice of the Stellate ganglion resulting in a Horner’s syndromeand branches of the brachial plexus can be damaged by resection of the cancer.
The patient should be informed preoperatively of possible nerve damagewhenever extensive central or apical cancers are resected.
References
1 Piccione W, Faber LP. Management of complications related to pulmonary resection. In:Waldhausen JA, Orringer MB, eds. Complications In Cardiothoracic Surgery. Mosby YearBook: St Louis, 1991; 336.
90 Chapter 4
2 Lewis FR. Management of atelectasis and pneumonia. Surg Clin N Am 1980; 67: 1391.3 Stock MC, Downs JB, Gaver PK et al. Prevention of postoperative pulmonary complica-
tions with CPAP, incentive spirometry and conservative therapy. Chest 1985; 87: 151.4 Mastboom WJ, Wobbes T, van den Dries A et al. Bronchial suction by minitracheostomy as
an effective measure against sputum retention. Surg Gynecol Obstet 1991; 173: 187.5 Shields TW, Lees WMM, Fox RT et al. Persistent pleural space following resection for
pulmonary tuberculosis. J Thorac Cardiovasc Surg 1959; 38: 523–536.6 Barker WL, Langston HT, Naffah P. Postresectional thoracic spaces. Ann Thorac Surg 1966;
2: 299.7 Silver AW, Espinas EE, Byron FX. The fate of post-resection space. Ann Thorac Surg 1966; 2:
1311–1326.8 Faber LP, Piccione W. Complication of surgery in the lung cancer patient. In: Mitchell JB,
Johnson DH, Turrisi AT, eds. Lung Cancer: Principles and Practice. Lippincott-Raven, 1996.9 Kirsch MM, Rotman H, Behrendt DM et al. Complications of pulmonary resection. Ann
Thorac Surg 1975; 20: 215.10 Spotnitz WD, Dalton MS, Baker JW et al. Successful use of fibrin glue during 2 years of
surgery at a university medical center. Am Surg 1989; 55: 1660.11 Yano T, Yokoyama H, Fukuyama Y et al. The current status of postoperative complications
and risk factors after a pulmonary resection for primary lung cancer. A multivariate ana-lysis. Eur Cardiothoracic Surg 1997; 11: 445–449.
12 Wright CD, Wain JC, Mathisen DJ, Grillo HC. Post-pneumonectomy bronchopleuralfistula after sutured bronchial closure: incidence, risk factors and management. J ThoracicCardio Surg 1996; 112: 1367–1371.
13 Vester SR, Faber LP, Kittle CF, Warren WH, Jensik RJ. Bronchopleural fistula after stapledclosure of bronchus. Ann Thorac Surg 1991; 52: 1253–1258.
14 Forrester-Wood CP. Bronchopleural fistula following pneumonectomy for carcinoma ofthe bronchus. J Thorac Cardiovasc Surg 1980; 80: 406–409.
15 Wain JC. Management of late postpneumonectomy empyema and bronchopleural fistula.Chest Surg Clin N Am 1996; 6: 529–531.
16 Landreneau RJ, Keenan RJ, Hazelrigg S et al. Thoracoscopy for empyema and hemothorax.Chest 1995; 109: 18–24.
17 Eloesser L. An operation for tuberculosis empyema. Surg Gynecol Obstet 1935; 60: 1096.18 Puskas JD, Mathisen DJ, Grillo HC et al. Treatment strategies for bronchopleural fistula.
J Thorac Cardiovasc Surg 1995; 109: 989.19 Claggett OT, Gerace JE. A procedure for the management of post-pneumonectomy
empyema. J Thorac Cardiovasc Surg 1963; 45: 141.20 Deschamps C, Pairolero PC, Allen MS et al. Early complications: broncholeural fistula and
empyema. Chest Surg Clin N Am 1999; 9: 587–595.21 Pairolero PC, Arnold PG, Piehler JM. Intrathoracic transposition of extrathoracic skeletal
muscle. J Thorac Cardiovasc Surg 1983; 86: 806–809.22 Baldwin JC, Mark JBD. Treatment of bronchopleural fistula after pneumonectomy.
J Thorac Cardiovasc Surg 1985; 90: 813.23 Torre M, Chiesa G, Ravini M et al. Endoscopic gluing of bronchopleural fistula. Ann Thorac
Surg 1994; 58: 901.24 Cerfolio RJ, Allen MS, Deschamps C et al. Postoperative chylothorax. J Thorac Cardiovasc
Surg 1996; 112: 1361–1365.25 Merrigan BA, Winter DC, O’Sullivan GC. Chylothorax. Br J Surg 1997; 84: 15–20.26 Staats RA, et al. The lipoprotein profile of chylous and unchylous pleural effusion. Mayo
Clin Proc 1980; 55: 700.

Complications of pulmonary resection 91
27 Deiraniya AK. Cardiac herniation following intrapericardial pneumonectomy. Thorax1974; 29: 545–552.
28 Schuler JG. Intraoperative lobar torsion producing pulmonary infarction. J ThoracCardiovasc Surg 1973; 65: 951.
29 Shields TW. General features and complications of pulmonary resections. In: GeneralThoracic Surgery. Williams and Wilkins, 1994; 391–414.
30 Carew JF, Kraus DH, Ginsberg RJ. Early complications: recurrent nerve palsy. Chest SurgClinics N Am 1999; 9: 597–608.
CHAPTER 5
Complications of tracheobronchialresection
Douglas J Mathisen
Management of complications of bronchoplasty
Techniques have been developed to allow sleeve resection of any lobe of thelung. These techniques allow both surgery for individuals who could not toler-ate more extensive operations and an improved quality of life because of thepreservation of functioning lung parenchyma. For these reasons, practicingthoracic surgeons should be familiar with technical details of the operation.The technical demands of the operation are such that there is an increased risk of complications. These can be minimized by strict attention to technicaldetails. Complications, however, are inevitable and one should be familiarwith their presentation and management possibilities. Like most surgery, themanagement of complications starts in the operating room, doing everythingpossible to avoid them!
Indications for sleeve lobectomyKnowing the indications for bronchoplasty will help in patient selection andimprove results. The most common indication for sleeve lobectomy is the pres-ence of a neoplasm originating at the origin of a lobar bronchus. The neoplasmcan be either benign or malignant. It is the rare neoplasm that can be managedby endoscopic methods with the expectation of cure. Hamartoma and papil-loma may be the exceptions. One should not be tempted to try laser ablation orremoval of benign or low-grade neoplasms. The biology of these tumors issuch that they always involve the bronchial wall deeply enough that completeremoval or obliteration is impossible. Extensive lasering can lead to bronchialstricturing and also to bronchial perforation, inflammation and growth of theneoplasm, possibly precluding a future bronchoplastic procedure.
There are other conditions that may be amenable to bronchoplastic tech-niques. At the time of thoracotomy, the origin of the bronchus may be found tobe involved with malignant lymph nodes, or positive frozen section marginsmay document direct extension of the primary neoplasm. These are conditionsnot identifiable by bronchoscopy and underscore the need for thoracic sur-geons to be familiar with bronchoplastic techniques. Other indications arepost-traumatic, postinflammatory, and postsurgical strictures.
92
Complications of tracheobronchial resection 93
Evaluation of patients for bronchoplastic procedures
The evaluation of patients for possible bronchoplastic procedures should proceed on many levels. The advanced knowledge provided by thoroughevaluation will help in planning the operation and improving overall results.In addition to general medical evaluation to determine the ability to tolerate apulmonary resection, it is essential to evaluate fully the patient’s pulmonaryfunction, with standard spirometry and quantitative ventilation and perfusionscans. This very important evaluation will determine whether a broncho-plastic procedure is the only option if anatomical findings are unfavorable at thoracotomy. I obtain these tests routinely for all patients if there is anyquestion about their ability to withstand the alternative to sleeve lobectomy,i.e. pneumonectomy.
Bronchoscopy should be performed by the operating surgeon. One shouldnever rely on the observation of others to assess the suitability of a patient for apossible bronchoplastic procedure. The bronchoscopy should reveal the originof the pathology, the extent of involvement, and the quality of the bronchialmucosa. The use of flexible bronchoscopes allows in almost every circum-stance the evaluation of the bronchus distal to the pathology. Even neoplasmsthat protrude into the lumen of the main bronchus and seemingly occlude theentire bronchus can usually be passed by carefully insinuating the tip of thebronchoscope around the periphery of the neoplasm. I believe this is import-ant to try to determine in every patient before thoracotomy. It can be sorted out at thoracotomy by bronchotomy, but this is not ideal and may compromisethe procedure. It is important to assess the bronchial mucosa for inflammatorychanges as well. One should not attempt bronchoplastic procedures throughmucosa that is actively inflamed.
The radiological assessment is very valuable in patients being consideredfor possible bronchoplastic procedures. Standard linear tomograms werequite useful in assessing bronchial pathology, but they have become virtuallyimpossible to obtain. Computed axial tomograms (CT) and spiral CT scanshave supplanted linear tomograms. Although not superior, they are satisfact-ory. They are superior, however, in determining extraluminal involvementand presence of enlarged lymph nodes.
For malignant lesions, mediastinoscopy should be performed to assessinvolvement of mediastinal lymph nodes. Positive nodes may influence thechoice of operation and the need for adjuvant therapy. I believe mediastinos-copy gives additional valuable information. Mediastinoscopy allows someassessment of the proximal mainstem bronchus as well as the main pulmonaryartery. Combining these findings with bronchoscopic findings and pulmonaryfunction tests is very valuable in determining the suitability of bronchoplasty. I prefer to perform mediastinoscopy at the time of thoracotomy or as close to itas possible. The resultant scarring that inevitably follows the procedure cancompromise the mobility of the airway, dissection of the bronchus, and createsome confusion as to what is scarring and what is neoplasm.
94 Chapter 5
Bronchoplasty in the presence of postintubation pneumoniaPostobstructive pneumonia is common in patients with obstructing neo-plasms [1]. It is preferable to try to resolve this before the bronchoplastic procedure. In addition to appropriate intravenous antibiotics and chest physiotherapy, aspiration bronchoscopy is invaluable. This may need to berepeated multiple times to achieve the desired effect. In some cases ‘core-out’of the neoplasm should be done to open the obstruction. Balanced against this goal is the risk of hemorrhage from neoplasms such as carcinoids. In thissituation multiple aspiration bronchoscopies may be preferable. Most otherneoplasms can safely be ‘cored out’ with minimal risk of bleeding [2]. A few days spent relieving postobstructive pneumonia is time well spent. Thegeneral risk of sepsis is reduced, purulent secretions diminished and in-flammation of the bronchial mucosa reduced. All of these diminish the risk ofpostoperative complications.
Anesthetic managementIt is important to perform these operations under optimal conditions. Themanagement of the airway is critical to the safe conduct of the operation. I prefer the use of a double-lumen endotracheal tube whenever possible.Bronchial blockers are alternative solutions, but they do not provide as muchprotection of the opposite lung from spilled secretions and in general are only a consideration for left-sided bronchoplastic procedures. Placement ofdouble-lumen tubes should be done with the aid of a flexible bronchoscopethrough the tube. This minimizes trauma to any neoplasm, reduces the risk of bleeding, and guarantees proper placement. The actual anesthetic shouldallow for extubation in the operating room at the conclusion of the operation. It is preferable not to have these patients intubated and mechanically ventil-ated. I routinely use epidural analgesia on all thoracotomy patients as manyhave difficulty clearing secretions. Maximal pain control helps enormously to allow vigorous coughing and thereby avoid complications from sputumretention.
Surgical technique
Success depends upon precise attention to technical details, gentle handling of the tissues, preservation of blood supply and avoidance of tension on theanastomosis. The technical details are the same as for standard lobectomy untilthe bronchus is reached. Great care must be taken to avoid devascularizationof the bronchus. Avoiding devascularization is important for bronchial heal-ing. A balance must be achieved in lymph node dissection as well, becausenode dissection often interferes with bronchial blood supply. Sharp transec-tion of the bronchus should be accomplished with minimal trauma to theremaining ends of the bronchus. To avoid confusion for the pathologist, it isbest to submit a separate sliver of bronchus from each end for histologicalreview. This practice minimizes sampling mistakes by the pathologist.
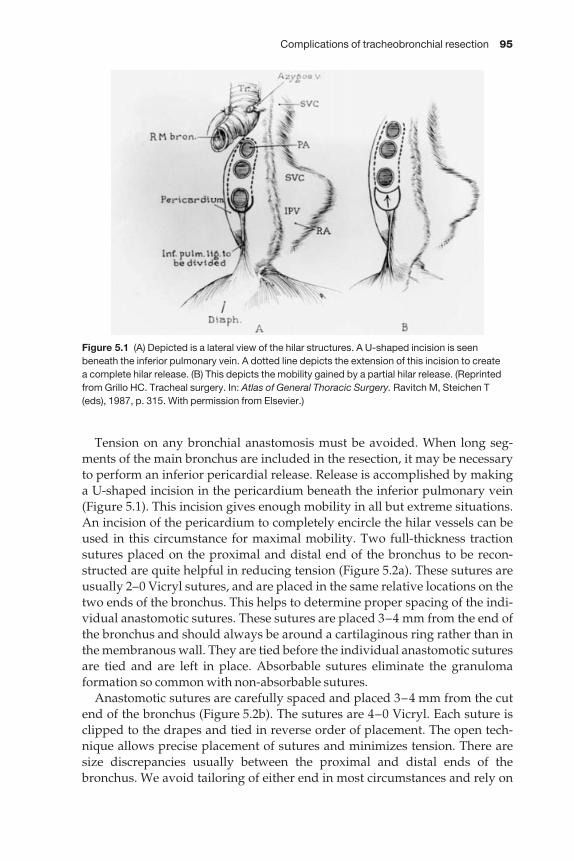
Complications of tracheobronchial resection 95
Tension on any bronchial anastomosis must be avoided. When long seg-ments of the main bronchus are included in the resection, it may be necessaryto perform an inferior pericardial release. Release is accomplished by making a U-shaped incision in the pericardium beneath the inferior pulmonary vein(Figure 5.1). This incision gives enough mobility in all but extreme situations.An incision of the pericardium to completely encircle the hilar vessels can beused in this circumstance for maximal mobility. Two full-thickness tractionsutures placed on the proximal and distal end of the bronchus to be recon-structed are quite helpful in reducing tension (Figure 5.2a). These sutures areusually 2–0 Vicryl sutures, and are placed in the same relative locations on thetwo ends of the bronchus. This helps to determine proper spacing of the indi-vidual anastomotic sutures. These sutures are placed 3–4 mm from the end ofthe bronchus and should always be around a cartilaginous ring rather than inthe membranous wall. They are tied before the individual anastomotic suturesare tied and are left in place. Absorbable sutures eliminate the granuloma formation so common with non-absorbable sutures.
Anastomotic sutures are carefully spaced and placed 3–4 mm from the cutend of the bronchus (Figure 5.2b). The sutures are 4–0 Vicryl. Each suture isclipped to the drapes and tied in reverse order of placement. The open tech-nique allows precise placement of sutures and minimizes tension. There aresize discrepancies usually between the proximal and distal ends of thebronchus. We avoid tailoring of either end in most circumstances and rely on
Figure 5.1 (A) Depicted is a lateral view of the hilar structures. A U-shaped incision is seenbeneath the inferior pulmonary vein. A dotted line depicts the extension of this incision to create a complete hilar release. (B) This depicts the mobility gained by a partial hilar release. (Reprintedfrom Grillo HC. Tracheal surgery. In: Atlas of General Thoracic Surgery. Ravitch M, Steichen T(eds), 1987, p. 315. With permission from Elsevier.)

96 Chapter 5
proper spacing of sutures to make up for any size difference. Some telescopinginevitably occurs, but this has not been a problem in our experience. Occasion-ally, when the entire right main bronchus, upper lobe, middle lobe, andbronchus intermedius are removed, the size discrepancy is too great and theproximal bronchus must be narrowed. Narrowing of the bronchus inevitablycreates a T intersection in the anastomosis. One must pay meticulous attentionto detail to avoid creating a potential area for a fistula. Once all sutures havebeen placed, the traction sutures are tied bringing the two ends together. The individual anastomotic sutures are tied in reverse order of placement(Figure 5.2c).
At the completion of the anastomosis, the operative field is flooded withsaline and the lung ventilated. Any air leaks should be repaired even if itmeans taking the anastomosis down and redoing it. Air leaks from the anasto-mosis demand repair to avoid a fistula. Flexible bronchoscopy should be done at this point to be certain of proper alignment, patency of lobar and seg-mental bronchi, and that there are no loose anastomotic sutures. All of theseproblems are best identified and corrected at this point rather than identifyingthem in the recovery room. Once the integrity of the anastomosis has been
Figure 5.2 (a) Traction sutures replaced in the mid-lateral position. They are placed full thicknessaround a cartilaginous ring about 2–4 mm from the cut end of the bronchus. They should be placed in the same relative position on the proximal and distal bronchus. (b) Individualanastomotic sutures are placed with the knots on the outside. An open technique is preferred to allow precise placement. The first suture is placed posteriorly at ‘6 o’clock’. The sutures areplaced inside the preceding suture and sequentially clipped to the drapes to maintain the properorder. (c) The traction sutures have been tied (not seen in the diagram) first. The anastomoticsutures are tied in reverse order of initial placement. The completed anastomosis is seen.
Complications of tracheobronchial resection 97
confirmed, a pedicled flap of pleura or pericardial fat is developed and passedaround the anastomosis. This may aid in healing, in sealing of small leaks thatmay develop, and in separating the bronchus from the nearby pulmonary artery.
Special mention should be made of patients who are steroid dependent orwho have had prior irradiation over 1 year before surgery. These circum-stances influence bronchial healing and increase the risk of a bronchoplasticprocedure and may preclude surgery. In those circumstances where bron-choplasty is elected, a pedicled intercostal muscle flap at the very least shouldbe used to buttress the anastomosis. When wrapped circumferentially itshould have the periosteum stripped to avoid a ring of bone that may constrictthe bronchus. A pedicled omental flap passed through a substernal tunnel isprobably even better protection than pedicled muscle.
In those circumstances where postoperative irradiation is to be given, it isbest to wait 4–6 weeks after surgery. A bronchoscopy should be done prior toinitiation of radiation therapy to be certain adequate healing has taken place.
Management of complications
The most common postoperative complication is sputum retention and atelec-tasis. Proper antibiotic selection, chest physiotherapy and pain control are veryimportant to managing this problem. Beside aspiration, bronchoscopy withirrigation of the distal airway should be used liberally.
Bronchoscopy should be done in the postoperative period to examine theanastomosis to ascertain whether or not normal healing is taking place. If thebronchial mucosa is ischemic but intact, a bronchoscopy should be done everyfew days to monitor the situation. If the anastomosis appears to remain intact,late stenosis may develop. This may take the form of a fibrotic stricture or ex-uberant granulations. Excessive granulation tissue may be debrided or lasered.A fibrotic stricture may be amenable to repeat dilations with either woven bou-gies through a rigid bronchoscope, pediatric rigid bronchoscopes, or balloondilators. These procedures may need to be repeated to maintain patency andavoid postobstructive pneumonia or atelectasis of the lung. It is possible that apartial stenosis will result and be satisfactory. If recurrent infection, atelectasisor shortness of breath become troublesome, reoperation may be necessary.Sufficient time should be allowed for resolution of postoperative inflammationand fibrosis. A period of 3 months is ideal, but may not be feasible. Reopera-tion and redoing a bronchoplastic procedure may be impossible and com-pletion pneumonectomy may be inevitable. The bronchial stump may bedifficult because of rigidity or short length. A difficult bronchial stump of this nature should be reinforced with a pedicled muscle flap. Bronchial stentshave limited application for stenosis following sleeve lobectomy because ofthe short length of distal bronchus available. A stent would be difficult to seat,maintain patency, and avoid granulation formation.
If bronchoscopic inspection of the anastomosis reveals dehiscence, partialseparation or frank necrosis, surgical intervention is mandatory. Completion
98 Chapter 5
pneumonectomy should be performed in most cases. Attempts to redo orrepair the anastomosis are futile and very risky. If completion pneumonec-tomy is not an option because of certain respiratory insufficiency and the process is caught early enough, an attempted repair can be entertained.Conditions would have to be ideal: no gross infection, no involvement of thepulmonary artery, debridement of devitalized tissues, and no anastomotic tension. I would prefer to wrap this anastomosis with pedicled omentum togive the greatest chance of success and avoid fatal complications.
Development of a bronchopleural fistula is a devastating postoperativecomplication and risks a bronchovascular fistula. If a bronchopleural fistula is suspected, a bronchoscopy should be done to evaluate the anastomosis. Ifthe problem is identified and small, conservative management is possible. Thisincludes proper antibiotics, adequate dependent drainage and possible irriga-tion to help evacuate infected material. A CT with contrast should be done tobe certain that all infection is drained and no residual abscess remains. If anyquestion exists, surgical exploration should be done to assess the problemmore accurately. This may be the only way to avoid a fatal bronchovascularfistula. Long-term drainage may allow closure. If the fistula fails to close afteradequate drainage and sufficient time (minimum 3 months), attempted repaircould be entertained. Debridement, closure with absorbable sutures, and ped-icled omental or muscle flap buttress should be done. The development of abronchopleural fistula may result in late bronchial stenosis as well. This mayinfluence the management of this problem and preclude local repair.
The most dreaded complication following a bronchoplastic procedure is abronchovascular fistula. This problem is clearly one that is best managed byavoiding the problem altogether. It is the reason I wrap every anastomosiswith viable pedicled tissue of some sort. Most bronchovascular fistulas have a ‘herald bleed’ of a significant amount of blood. Any episode of hemo-ptysis after a bronchoplastic procedure should immediately be evaluated.Bronchoscopic findings may be subtle with only an area of granulation tissueor obvious with frank dehiscence. If suspicion of a bronchovascular fistula isconfirmed, immediate surgical intervention is warranted. Delay may be fatal.It is unlikely that anything other than completion pneumonectomy is possiblein this circumstance. It is essential to gain proximal control of the pulmonaryartery before exposing the fistula. The mainstem bronchus may be difficult to close and should be buttressed with at least a pedicled muscle flap in every case. Because of the likelihood of contamination of the pleural space,copious irrigation with saline and an antibiotic solution should be done. Ifgross contamination of the pleural space exists, consideration should be givento postoperative antibiotic irrigation of the pleural space.
Local recurrence of tumor is a complication of sleeve lobectomy. Because of the potential for this, I believe surveillance bronchoscopy twice a year iswarranted in these patients. Early detection may afford an opportunity forresection in some cases.
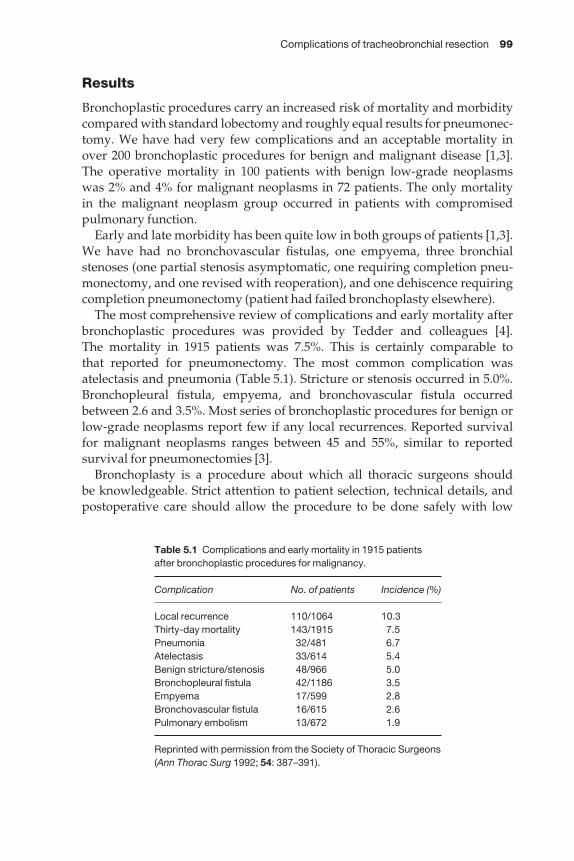
Complications of tracheobronchial resection 99
Results
Bronchoplastic procedures carry an increased risk of mortality and morbiditycompared with standard lobectomy and roughly equal results for pneumonec-tomy. We have had very few complications and an acceptable mortality inover 200 bronchoplastic procedures for benign and malignant disease [1,3].The operative mortality in 100 patients with benign low-grade neoplasms was 2% and 4% for malignant neoplasms in 72 patients. The only mortality in the malignant neoplasm group occurred in patients with compromised pulmonary function.
Early and late morbidity has been quite low in both groups of patients [1,3].We have had no bronchovascular fistulas, one empyema, three bronchialstenoses (one partial stenosis asymptomatic, one requiring completion pneu-monectomy, and one revised with reoperation), and one dehiscence requiringcompletion pneumonectomy (patient had failed bronchoplasty elsewhere).
The most comprehensive review of complications and early mortality afterbronchoplastic procedures was provided by Tedder and colleagues [4]. The mortality in 1915 patients was 7.5%. This is certainly comparable to that reported for pneumonectomy. The most common complication wasatelectasis and pneumonia (Table 5.1). Stricture or stenosis occurred in 5.0%.Bronchopleural fistula, empyema, and bronchovascular fistula occurredbetween 2.6 and 3.5%. Most series of bronchoplastic procedures for benign orlow-grade neoplasms report few if any local recurrences. Reported survivalfor malignant neoplasms ranges between 45 and 55%, similar to reported survival for pneumonectomies [3].
Bronchoplasty is a procedure about which all thoracic surgeons should be knowledgeable. Strict attention to patient selection, technical details, andpostoperative care should allow the procedure to be done safely with low
Table 5.1 Complications and early mortality in 1915 patientsafter bronchoplastic procedures for malignancy.
Complication No. of patients Incidence (%)
Local recurrence 110/1064 10.3Thirty-day mortality 143/1915 7.5Pneumonia 32/481 6.7Atelectasis 33/614 5.4Benign stricture/stenosis 48/966 5.0Bronchopleural fistula 42/1186 3.5Empyema 17/599 2.8Bronchovascular fistula 16/615 2.6Pulmonary embolism 13/672 1.9
Reprinted with permission from the Society of Thoracic Surgeons(Ann Thorac Surg 1992; 54: 387–391).

100 Chapter 5
operative morbidity and mortality. Early identification of potential complica-tions should allow successful management of most and avoidance of fatal out-comes. Because of the excellent survival for low-grade malignancies (> 90%)and good survival for malignant neoplasms (50%) and the improved quality of life from preserved lung parenchyma, bronchoplastic procedures are theprocedure of choice for anatomically suited neoplasms.
Tracheal resection and reconstruction
The goals of tracheal surgery are to resect the diseased segment of trachea and perform an end-to-end reconstruction with a tension-free anastomosis [5].Knowledge of tracheal anatomy, indications for surgery, surgical techniques,release maneuvers to reduce tension and airway management will improvethe chance of success and minimize the risks of complications. Trachealsurgery is relatively uncommon, therefore thoracic surgeons need to be famil-iar with these issues to allow them to manage these problems successfully.Successful outcome will allow patency of the airway, preservation of voice andavoid the need for life-long tracheostomy. As with bronchoplastic proceduresof the main bronchi, the best way to manage complications of tracheal surgeryis to avoid them altogether by achieving a successful surgical outcome.
High-risk conditionsSpecial mention should be made of certain high-risk situations. The burnedtrachea from inhalation is a very difficult situation to manage [6]. A longperiod of time should elapse before any consideration is given to attemptedrepair. The airway is best managed with a tracheostomy or T-tube. Patientselection and timing are critical. Patients that present on high-dose steroidsmust be weaned and a minimum of 4 weeks allowed for normal healing mech-anisms to return. The combination of steroids and anastomotic tension is a prescription for disaster. Massively obese patients, patients at high risk formechanical ventilation and patients with sleep apnea are relative contraindica-tions for reconstruction. Quadriplegic patients are at high risk and must becarefully selected. A condition referred to as idiopathic tracheal stenosis requirescareful patient selection and proper timing of repair. This condition is predom-inantly seen in women and usually presents in the subglottic area. If any degreeof inflammation exists, surgical correction should be delayed until it has sub-sided. Dilation with a rigid bronchoscope provides temporary improvement.
Indications for surgeryThe most common indication for surgical resection remains tracheal stenosisfollowing prolonged mechanical ventilation through an oral endotrachealtube or tracheostomy. Cuff injuries remain the most common problem despitethe advent of ‘low-pressure cuffs’. Overinflated low-pressure cuffs can stilllead to circumferential tracheal injury. It is very important to use the propersize endotracheal or tracheostomy tube. The cuff pressure should be kept as
Complications of tracheobronchial resection 101
low as possible consistent with the needs for ventilation. The cuff pressureshould be checked regularly and deflated periodically to reduce the chance of injury. Excessive traction on tracheostomy tubes is responsible for moststomal injuries leading to stenosis. Lightweight connecting tubing and con-stant nursing vigilance are required to reduce this injury. Neoplasms representthe next most common indication for tracheal resection. Other indicationsinclude post-traumatic, idiopathic, tracheoesophageal fistula, congenitalstenosis, and failed primary repair.
Evaluation of tracheal pathologyThorough preoperative evaluation is invaluable to allow for optimal operativeplanning. Simple radiological studies will allow assessment of the extent ofinvolvement of the airway. Soft tissue X-rays of the neck and linear tomogramswill give excellent detail of the pathology. CT, spiral CT scans and magneticresonance images are alternative exams, but are probably not superior to lineartomograms.
The most important assessment is bronchoscopy. Bronchoscopy is best donein the operating room where emergency rigid bronchoscopy can be done tomanage critical airway stenosis if it develops. Flexible bronchoscopy should be limited to inspection of the area proximal to the stenosis. Manipulation ofthe stenosis may lead to secretions, edema or bleeding which may precipitatecritical airway stenosis. Formal bronchoscopic evaluation is best reserved forthe time of definitive surgical correction. I believe it is best done with a rigidbronchoscope with telescopes for careful inspection. The length and locationof involvement should be carefully measured. The total length of airway andamount of uninvolved airway should also be carefully measured. It is alsoimportant to assess the trachea for the presence of inflammation which is com-mon in many conditions involving the trachea. Allowing the inflammation tosubside may be helpful and allow resection and reconstruction to be achieved.It is thought that as much as half of the adult trachea can be resected and recon-structed, but this is dependent on many factors.
Airway managementPerhaps nothing is more important than airway management. Failure tosecure the airway may lead to a fatal outcome, inappropriate tracheostomy or trauma to the airway precluding future repair. Initial presentation of postin-tubation stenosis is rarely an emergency. Maintaining patients in the uprightposition and application of cool, humidified oxygen will often stabilizepatients and allow airway assessment under optimal circumstances. The airway is best managed in the operating room with skilled anesthesiologists,an operating room team, pediatric and adult rigid bronchoscopes and tra-cheostomy kit available. Patients should be anesthetized with an agent thatallows spontaneous ventilation. This technique requires patience to achievethe depth of anesthesia necessary to allow rigid bronchoscopy, but is clearlysafer than any technique that utilizes paralysing agents. Once an adequate

102 Chapter 5
level of anesthesia has been achieved, an adult rigid bronchoscope is carefullyinserted into the proximal airway to visualize the area of stenosis. A pediatricflexible bronchoscope can be inserted through the rigid bronchoscope toinspect the entire length of the stenosis. All strictures can be dilated by smallwoven bougies and then pediatric bronchoscopes (3.5–7 mm). This is donewith gentle pressure under direct vision. It is almost always possible to dilatestrictures to a 7-mm rigid bronchoscope. A sufficient lumen can be maintainedin most patients for days to weeks following dilation. Tumors can be ‘coredout’ with a bronchoscope. If a tracheostomy is contemplated to manage the air-way, it should be performed through the most damaged portion of the airwayto preserve as much viable trachea as possible for future reconstruction.
Surgical techniqueThe majority of tracheal resections can be performed through a cervical collarincision. A small partial upper sternotomy just beyond the angle of Louis givesadditional exposure of the distal trachea. The important anatomical considera-tions are the recurrent laryngeal nerves located in the tracheo–esophagealgroove, the esophagus posteriorly, and the segmental blood supply that entersthe trachea in the mid-lateral position. Initial dissection is kept right on the tracheal wall. No attempt is made to identify the recurrent nerves as they areoften embedded in scar and easily injured if there is an attempt to identifythem. The trachea should be encircled just proximal or distal to the area ofstenosis. This allows dissection in an area with minimal scarring whichreduces the risk of injury to the esophagus. A tape is passed around the tracheato provide traction and elevation. We prefer to ventilate patients during resec-tion with a sterile endotracheal tube on the operative field inserted into the dis-tal airway connected to sterile tubing which is passed off the operative field tothe anesthesiologists (Figure 5.3a). This allows the endotracheal tube to beremoved allowing for careful inspection of the airway and precise placementof sutures. A conservation point of transection of the airway is determined andthe trachea divided. Further dissection of the airway can be done by elevatingthe transected ends of the airway, again staying very close to the trachea at alltimes. If it appears that resection and reconstruction can be accomplished, thediseased segment is removed. Traction sutures (2–0 Vicryl) are placed in theproximal and distal ends of the trachea in the mid-lateral position (Figure5.3a). They should be placed 3–4 mm from the cut ends and around a trachealcartilage. Individual anastomotic sutures (4–0 Vicryl) are placed starting in themidline posteriorly (Figure 5.3a,b). The sutures are placed so the knots will beon the outside. Each suture is clipped to the drapes to maintain proper order.Once all of the sutures are placed, the neck is flexed and maintained by theanesthesiologist, the oral tube advanced across the anastomosis, and the trac-tion sutures tied. With the traction sutures tied, each anastomotic suture isthen tied in reverse order of placement (Figure 5.3c). This provides the leastamount of tension on the anastomosis. The wound is then flooded with salineand the anastomosis checked for any air leaks. This is done by deflating the
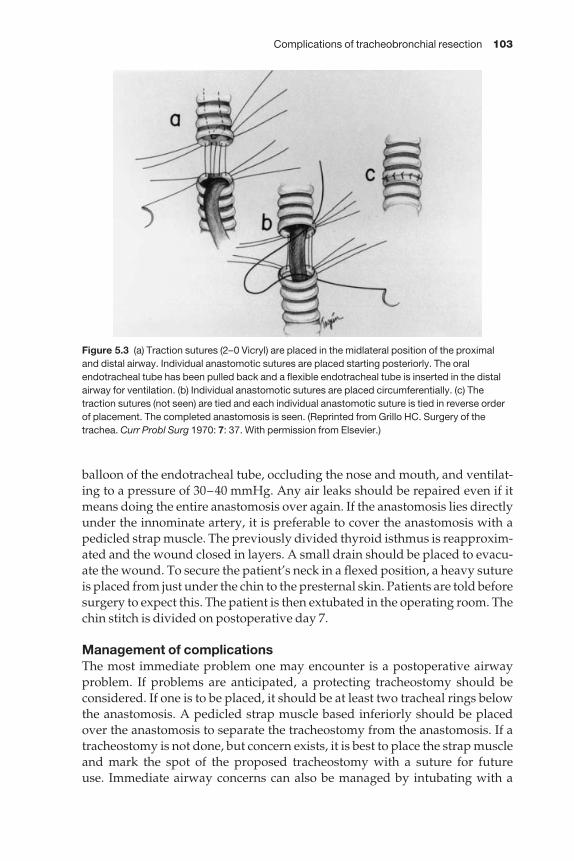
Complications of tracheobronchial resection 103
balloon of the endotracheal tube, occluding the nose and mouth, and ventilat-ing to a pressure of 30–40 mmHg. Any air leaks should be repaired even if itmeans doing the entire anastomosis over again. If the anastomosis lies directlyunder the innominate artery, it is preferable to cover the anastomosis with apedicled strap muscle. The previously divided thyroid isthmus is reapproxim-ated and the wound closed in layers. A small drain should be placed to evacu-ate the wound. To secure the patient’s neck in a flexed position, a heavy sutureis placed from just under the chin to the presternal skin. Patients are told beforesurgery to expect this. The patient is then extubated in the operating room. Thechin stitch is divided on postoperative day 7.
Management of complicationsThe most immediate problem one may encounter is a postoperative airwayproblem. If problems are anticipated, a protecting tracheostomy should beconsidered. If one is to be placed, it should be at least two tracheal rings belowthe anastomosis. A pedicled strap muscle based inferiorly should be placedover the anastomosis to separate the tracheostomy from the anastomosis. If atracheostomy is not done, but concern exists, it is best to place the strap muscleand mark the spot of the proposed tracheostomy with a suture for future use. Immediate airway concerns can also be managed by intubating with a
Figure 5.3 (a) Traction sutures (2–0 Vicryl) are placed in the midlateral position of the proximaland distal airway. Individual anastomotic sutures are placed starting posteriorly. The oralendotracheal tube has been pulled back and a flexible endotracheal tube is inserted in the distalairway for ventilation. (b) Individual anastomotic sutures are placed circumferentially. (c) Thetraction sutures (not seen) are tied and each individual anastomotic suture is tied in reverse orderof placement. The completed anastomosis is seen. (Reprinted from Grillo HC. Surgery of thetrachea. Curr Probl Surg 1970: 7: 37. With permission from Elsevier.)

104 Chapter 5
small uncuffed endotracheal tube. It can be left in for 48 h at which time thepatient should be returned to the operating room and extubated under a lightgeneral anesthetic. Persistent airway problems necessitate placement of a tracheostomy.
Airway problems that develop in the first 24–48 h may be related to edema.This should be managed with racemic epinephrine, 24 h of steroids, and diur-esis. If the problem fails to respond, a small uncuffed endotracheal tube shouldbe placed. This is best done with the aid of a flexible bronchoscope.
Wound infections have been relatively uncommon (< 2%). Concern overinfection is one reason to always try to cover the anastomosis with viable tissue(thyroid isthmus or strap muscle). I always cover the anastomosis with a strapmuscle in diabetics or those patients where a tracheostomy stoma is present.These patients are at slightly greater risk. A superficial wound infection shouldbe managed with dressing changes and antibiotics. Bronchoscopy should bedone to check the integrity of the anastomosis.
The presence of subcutaneous emphysema or an air leak through the wounddrain usually means a small leak in the anastomosis. The patient should bereturned to the operating room and the wound explored. If the leak can beidentified, it should be repaired with a pedicled strap muscle. The anastomosisshould be inspected as well.
The presence of subcutaneous emphysema and respiratory distress usuallyheralds more serious problems with the anastomosis. Dehiscence and separa-tion is a life-threatening problem. Great judgement is required to determinehow best to manage this problem. If the separation is only partial, a tra-cheostomy or T-tube should be placed through the separation. Complete sep-aration is a very serious situation. If enough length of the distal airway exists, it can be secured to the skin as an end-stoma. Insufficient length of the distalairway requires creative solutions to secure the airway. A tracheostomy tubeshould be placed and buttressed with muscle flaps to wall it off from surrounding vascular structures. The proximal airway should be closed orcovered with a muscle flap. A T-tube can be used if the distance of separation isnot too great. Muscle flaps should be utilized to buttress the T-tube.
Late anastomotic stenosis is usually a result of exuberant granulations or stricture from ischemia or slow separation. Granulations are uncommonnow that absorbable sutures are used. Mechanical debridement, lasering, andsteroid ingestion may be utilized to manage the granulations with varyingdegrees of success. Early stricturing can be managed transiently with dilation.If dilation is unsuccessful, a tracheostomy or T-tube may be necessary.Whichever tube is chosen, it should be placed through the most damaged portion of the airway to insure as much viable trachea as possible for futurereconstruction. If recurrent stenosis develops, reoperation is possible in highlyselected patients. A period of at least 3 months should elapse before attemptedresection and reconstruction.
Paralysis of one vocal cord or performance of a suprahyoid laryngeal releasepredisposes patients to aspiration. This is usually a temporary problem.
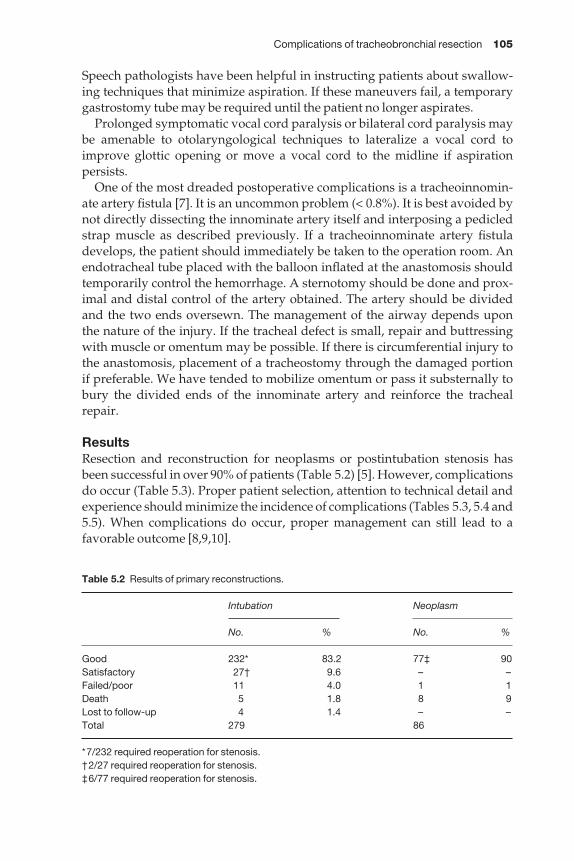
Complications of tracheobronchial resection 105
Speech pathologists have been helpful in instructing patients about swallow-ing techniques that minimize aspiration. If these maneuvers fail, a temporarygastrostomy tube may be required until the patient no longer aspirates.
Prolonged symptomatic vocal cord paralysis or bilateral cord paralysis maybe amenable to otolaryngological techniques to lateralize a vocal cord toimprove glottic opening or move a vocal cord to the midline if aspiration persists.
One of the most dreaded postoperative complications is a tracheoinnomin-ate artery fistula [7]. It is an uncommon problem (< 0.8%). It is best avoided bynot directly dissecting the innominate artery itself and interposing a pedicledstrap muscle as described previously. If a tracheoinnominate artery fistuladevelops, the patient should immediately be taken to the operation room. Anendotracheal tube placed with the balloon inflated at the anastomosis shouldtemporarily control the hemorrhage. A sternotomy should be done and prox-imal and distal control of the artery obtained. The artery should be divided and the two ends oversewn. The management of the airway depends upon the nature of the injury. If the tracheal defect is small, repair and buttressingwith muscle or omentum may be possible. If there is circumferential injury tothe anastomosis, placement of a tracheostomy through the damaged portion if preferable. We have tended to mobilize omentum or pass it substernally tobury the divided ends of the innominate artery and reinforce the trachealrepair.
ResultsResection and reconstruction for neoplasms or postintubation stenosis hasbeen successful in over 90% of patients (Table 5.2) [5]. However, complications do occur (Table 5.3). Proper patient selection, attention to technical detail andexperience should minimize the incidence of complications (Tables 5.3, 5.4 and5.5). When complications do occur, proper management can still lead to afavorable outcome [8,9,10].
Table 5.2 Results of primary reconstructions.
Intubation Neoplasm
No. % No. %
Good 232* 83.2 77‡ 90Satisfactory 27† 9.6 – –Failed/poor 11 4.0 1 1Death 5 1.8 8 9Lost to follow-up 4 1.4 – –Total 279 86
*7/232 required reoperation for stenosis.†2/27 required reoperation for stenosis.‡6/77 required reoperation for stenosis.
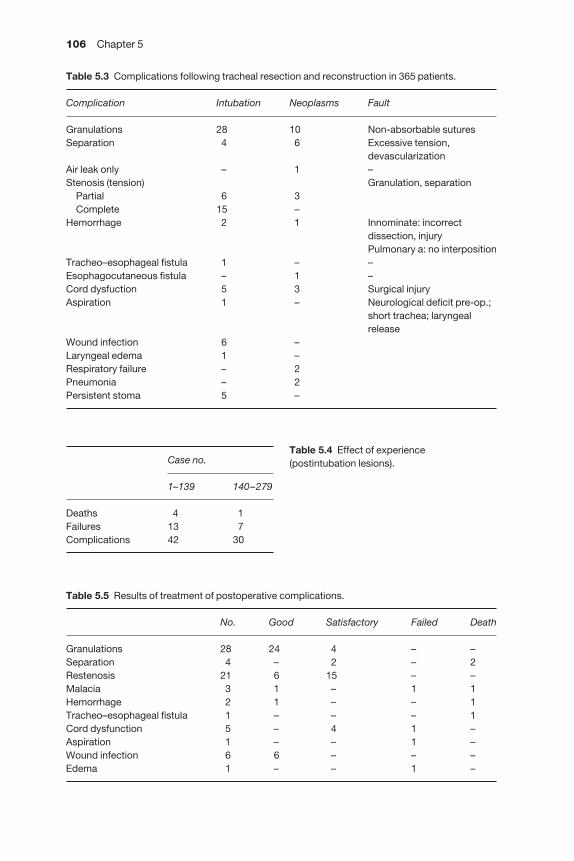
106 Chapter 5
Table 5.5 Results of treatment of postoperative complications.
No. Good Satisfactory Failed Death
Granulations 28 24 4 – –Separation 4 – 2 – 2Restenosis 21 6 15 – –Malacia 3 1 – 1 1Hemorrhage 2 1 – – 1Tracheo–esophageal fistula 1 – – – 1Cord dysfunction 5 – 4 1 –Aspiration 1 – – 1 –Wound infection 6 6 – – –Edema 1 – – 1 –
Case no.
1–139 140–279
Deaths 4 1Failures 13 7Complications 42 30
Table 5.3 Complications following tracheal resection and reconstruction in 365 patients.
Complication Intubation Neoplasms Fault
Granulations 28 10 Non-absorbable suturesSeparation 4 6 Excessive tension,
devascularizationAir leak only – 1 –Stenosis (tension) Granulation, separation
Partial 6 3Complete 15 –
Hemorrhage 2 1 Innominate: incorrectdissection, injuryPulmonary a: no interposition
Tracheo–esophageal fistula 1 – –Esophagocutaneous fistula – 1 –Cord dysfuction 5 3 Surgical injuryAspiration 1 – Neurological deficit pre-op.;
short trachea; laryngeal release
Wound infection 6 –Laryngeal edema 1 –Respiratory failure – 2Pneumonia – 2Persistent stoma 5 –
Table 5.4 Effect of experience (postintubation lesions).
Complications of tracheobronchial resection 107
References
1 Bueno R, Wain JC, Wright CD et al. Bronchoplasty in the management of low grade airwaymalignancies and benign bronchial stenoses. Ann Thorac Surg 1996; 62: 824–829.
2 Mathisen DJ, Grillo HC. Endoscopic relief of malignant airway obstruction. Ann ThoracSurg 1989; 48: 469–475.
3 Gaissert HA, Mathisen DJ, Moncure AC et al. Survival and function after sleeve lobectomyfor lung cancer. J Thorac Cardiovasc Surg 1996; 111: 948–953.
4 Tedder M, Anstadt MP, Tedder S et al. Current morbidity, mortality and survival afterbronchoplastic procedures for malignancy. Ann Thorac Surg 1992; 54: 387–391.
5 Grillo HC, Donahue DM, Mathisen DJ et al. Postintubation tracheal stenosis: treatmentand results. J Thorac Cardiovasc Surg 1995; 109: 486.
6 Muehrcke DD, Grillo HC, Mathisen DJ. Reconstructive airway surgery after irradiation.Ann Thorac Surg 1995; 59: 14.
7 Wright CD. Management of tracheoinnominate fistula. Chest Surg Clin N Am The Trachea1996; 6: 865.
8 Mathisen DJ. Complications of tracheal surgery. Chest Surg Clin N Am. The Trachea 1996; 6:853.
9 Grillo HC, Zannini P, Michelassi F. Complications of tracheal reconstruction. J ThoracCardiovasc Surg 1986; 91: 322.
10 Grillo HC. Complications of tracheal operations. In: Complications of Intrathoracic. Surgery(eds AR Cordell, RG Ellison). Little, Brown Co, Boston, 1979: pp 287.

CHAPTER 6
Complications of lung volume reduction procedures
Robert J Burnett, Douglas E Wood
Introduction
Since the reintroduction by Cooper [1] of Brantigan’s [2–4] original concepts,surgical treatment other than transplantation has emerged as a viable optionfor patients with end-stage emphysema. Although there remains a great dealof controversy surrounding many aspects of this procedure, surgical reductionof hyperinflated emphysematous lungs improves symptoms and pulmonaryfunction in selected patients. The excision of the most severely diseased portions of the lung that occupy space, but provide little or no gas exchange,allows improved function by decreasing small airway resistance and improv-ing chest wall and diaphragmatic mechanics. Volume reduction procedures,or lung volume reduction surgery (LVRS), have been shown to benefit certainpatients by improving the forced expiratory volume in 1 s (FEV1), timed walking distance, oxygen and steroid requirements and overall quality of life[1,5–8]. Additionally, LVRS can be an alternative or bridge to pulmonarytransplantation in patients with end-stage emphysema.
Many of the questions and controversies surrounding LVRS are currentlybeing studied by the National Emphysema Treatment Trial (NETT). In thetrial, patients are evaluated by strict criteria and initially undergo a period of pulmonary rehabilitation before being randomized to LVRS or continuedmedical therapy and rehabilitation. Overall survival and maximum exercisecapacity are the primary outcomes being measured in the trial [9]. Survival is aclinically significant outcome, because patients with severe emphysema have ahigh mortality rate and there have been no studies that evaluate the effect ofLVRS on overall survival. Standardized exercise testing is a way to evaluateimprovements in cardiopulmonary and physical function in a qualitative andreproducible fashion. Secondary outcome parameters for the NETT includequality of life, utility, pulmonary function and gas exchange, radiographicchanges, oxygen requirements, 6-min walk distances and other cardiovas-cular measurements. In addition to these primary and secondary outcomemeasurements, the trial will help to define the subgroups of patients with end-stage emphysema that may benefit from LVRS and which patients are atparticularly high risk of complications.
108
Complications of lung volume reduction procedures 109
It is not the purpose of this chapter to discuss the controversies surroundinglung volume reduction procedures. The focus of this discussion is the preven-tion, identification, and treatment of complications associated with LVRS.Patients with end-stage emphysema have an unpredictable natural history.Most of these patients have a progressive course of their disease with exacerba-tions and hospitalizations accelerating the worsening of symptoms and quality of life. Mortality ranges from 10 to 30% per year and is higher in those patients who have required hospitalizations for complications of theiremphysema. It is likely that any procedure performed routinely on patientswith such severe emphysema is apt to produce significant and potentially life-threatening complications. This becomes particularly true when the operationinvolves violation of the thorax and perturbation of respiratory mechanics.With an understanding of the lessons learned regarding this procedure and about the general intra- and postoperative care of this particular type ofpatient, many complications can be avoided and LVRS can be performed withacceptably low major morbidity and mortality.
Overview of mortality
As pointed out by Cooper [10], there were several reasons why Brantigan’swork in the 1950s failed to gain popularity. In addition to the unsettling notionof removing lung tissue in a patient with existing respiratory dysfunction,there was a lack of objective evidence for the benefit of the operation and a 16%mortality that led to criticism and ultimate failure of acceptance. In 1995,Cooper [1] reported on his first 20 patients to undergo bilateral LVRS viamedian sternotomy in which there were no early or late deaths. In a later seriesreporting the first 150 consecutive patients in 1996, the same group had a mortality of 4% [5]. Similar mortality rates have been reported in other series as well [6–8,11–13]. Recently, Roberts et al. reviewed the mortality of patientsafter LVRS which ranged from 0 to 19%, with a weighted average of 6.8% [13].Summarized at the bottom of Table 6.1 is the composite mortality from sixrecently published series, utilizing lung volume reduction via median ster-notomy or unilateral or bilateral video-assisted thoracic surgery (VATS). Theweighted mortality among this group of series is 4.6%. Although the bestresults and average mortality amongst published reports is approximately 5%,clearly there is a wide range of reported mortality to date, and unreportedmortality rates may be even less favorable. Since LVRS is a palliative pro-cedure directed primarily at the improvement in functional quality of life, it is critical that low mortality rates be maintained in order to sanction rationallyits utilization for patients with end-stage emphysema.
Death after LVRS can result from a variety of complications and can occurearly or late in the postoperative period. Early deaths have been reported as aresult of hemorrhage and myocardial infarction [5]. Respiratory failure canoccur early as a result of profound CO2 retention or massive air leak, or late as aresult of nosocomial respiratory tract infection, either of which can be fatal.
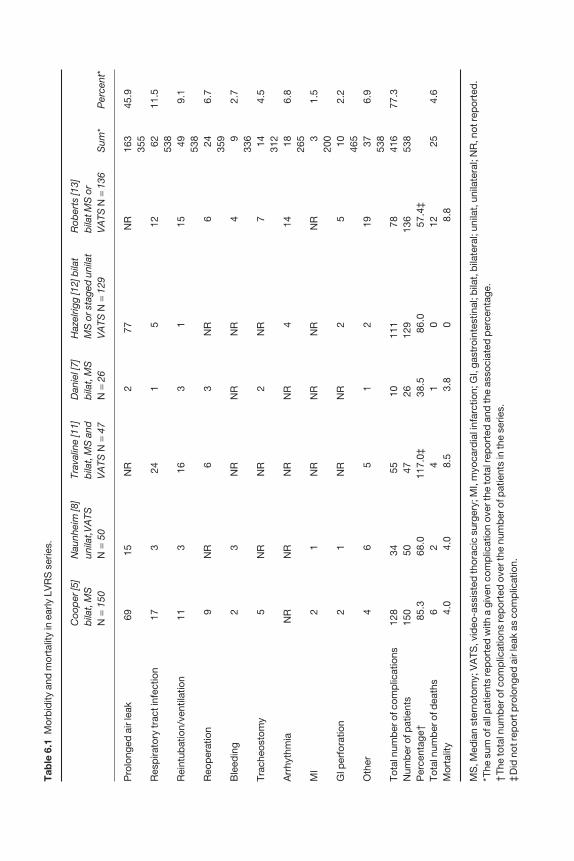
Tab
le 6
.1M
orb
idity
and
mor
talit
y in
ear
ly L
VR
S s
erie
s.
Coo
per
[5]
Nau
nhei
m [8
]Tr
aval
ine
[11]
Dan
iel [
7]H
azel
rigg
[12]
bila
tR
ober
ts [1
3]b
ilat,
MS
un
ilat,
VA
TSb
ilat,
MS
and
bila
t, M
SM
S o
r sta
ged
uni
lat
bila
t MS
or
N=
150
N=
50V
ATS
N=
47N
=26
VA
TS N
=12
9V
ATS
N=
136
Sum
*P
erce
nt*
Pro
long
ed a
ir le
ak69
15N
R2
77N
R16
345
.935
5R
esp
irato
ry tr
act i
nfec
tion
173
241
512
6211
.553
8R
eint
ubat
ion/
vent
ilatio
n11
316
31
1549
9.1
538
Reo
per
atio
n9
NR
63
NR
624
6.7
359
Ble
edin
g2
3N
RN
RN
R4
92.
733
6Tr
ache
osto
my
5N
RN
R2
NR
714
4.5
312
Arr
hyth
mia
NR
NR
NR
NR
414
186.
826
5M
I2
1 N
RN
RN
R
NR
31.
520
0G
I per
fora
tion
21
NR
NR
25
102.
246
5O
ther
46
51
219
376.
953
8To
tal n
umb
er o
f com
plic
atio
ns12
834
5510
111
7841
677
.3N
umb
er o
f pat
ient
s15
050
4726
129
136
538
Per
cent
age†
85.3
68.0
117.
0‡38
.586
.057
.4‡
Tota
l num
ber
of d
eath
s6
24
10
1225
4.6
Mor
talit
y4.
04.
08.
53.
80
8.8
MS
, Med
ian
ster
noto
my;
VA
TS, v
ideo
-ass
iste
d th
orac
ic s
urge
ry; M
I, m
yoca
rdia
l inf
arct
ion;
GI,
gast
roin
test
inal
; bila
t, b
ilate
ral;
unila
t, u
nila
tera
l; N
R, n
ot re
por
ted
.*T
he s
um o
f all
pat
ient
s re
por
ted
with
a g
iven
com
plic
atio
n ov
er th
e to
tal r
epor
ted
and
the
asso
ciat
ed p
erce
ntag
e.†
The
tota
l num
ber
of c
omp
licat
ions
rep
orte
d o
ver t
he n
umb
er o
f pat
ient
s in
the
serie
s.‡
Did
not
rep
ort p
rolo
nged
air
leak
as
com
plic
atio
n.
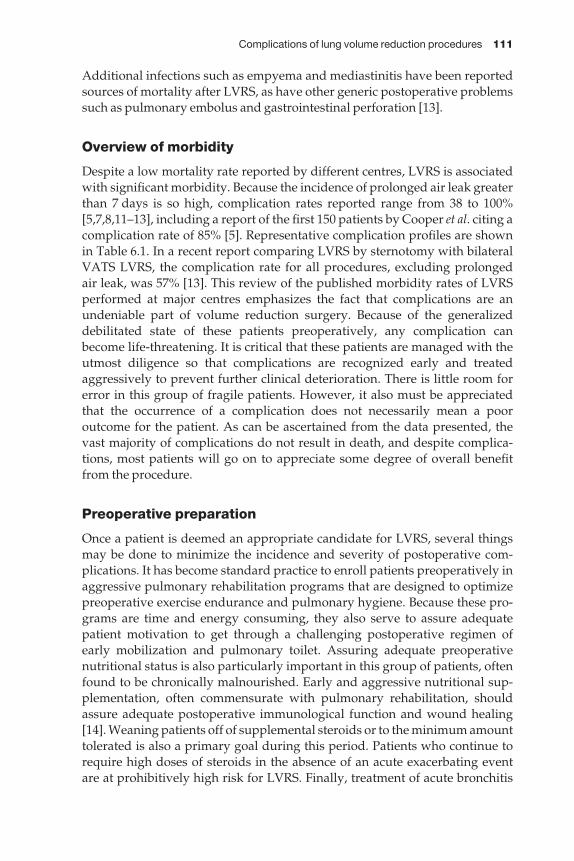
Complications of lung volume reduction procedures 111
Additional infections such as empyema and mediastinitis have been reportedsources of mortality after LVRS, as have other generic postoperative problemssuch as pulmonary embolus and gastrointestinal perforation [13].
Overview of morbidity
Despite a low mortality rate reported by different centres, LVRS is associatedwith significant morbidity. Because the incidence of prolonged air leak greaterthan 7 days is so high, complication rates reported range from 38 to 100%[5,7,8,11–13], including a report of the first 150 patients by Cooper et al. citing acomplication rate of 85% [5]. Representative complication profiles are shownin Table 6.1. In a recent report comparing LVRS by sternotomy with bilateralVATS LVRS, the complication rate for all procedures, excluding prolonged air leak, was 57% [13]. This review of the published morbidity rates of LVRSperformed at major centres emphasizes the fact that complications are anundeniable part of volume reduction surgery. Because of the generalizeddebilitated state of these patients preoperatively, any complication canbecome life-threatening. It is critical that these patients are managed with theutmost diligence so that complications are recognized early and treatedaggressively to prevent further clinical deterioration. There is little room forerror in this group of fragile patients. However, it also must be appreciatedthat the occurrence of a complication does not necessarily mean a poor outcome for the patient. As can be ascertained from the data presented, thevast majority of complications do not result in death, and despite complica-tions, most patients will go on to appreciate some degree of overall benefitfrom the procedure.
Preoperative preparation
Once a patient is deemed an appropriate candidate for LVRS, several thingsmay be done to minimize the incidence and severity of postoperative com-plications. It has become standard practice to enroll patients preoperatively inaggressive pulmonary rehabilitation programs that are designed to optimizepreoperative exercise endurance and pulmonary hygiene. Because these pro-grams are time and energy consuming, they also serve to assure adequatepatient motivation to get through a challenging postoperative regimen of early mobilization and pulmonary toilet. Assuring adequate preoperativenutritional status is also particularly important in this group of patients, oftenfound to be chronically malnourished. Early and aggressive nutritional sup-plementation, often commensurate with pulmonary rehabilitation, shouldassure adequate postoperative immunological function and wound healing[14]. Weaning patients off of supplemental steroids or to the minimum amounttolerated is also a primary goal during this period. Patients who continue torequire high doses of steroids in the absence of an acute exacerbating event are at prohibitively high risk for LVRS. Finally, treatment of acute bronchitis
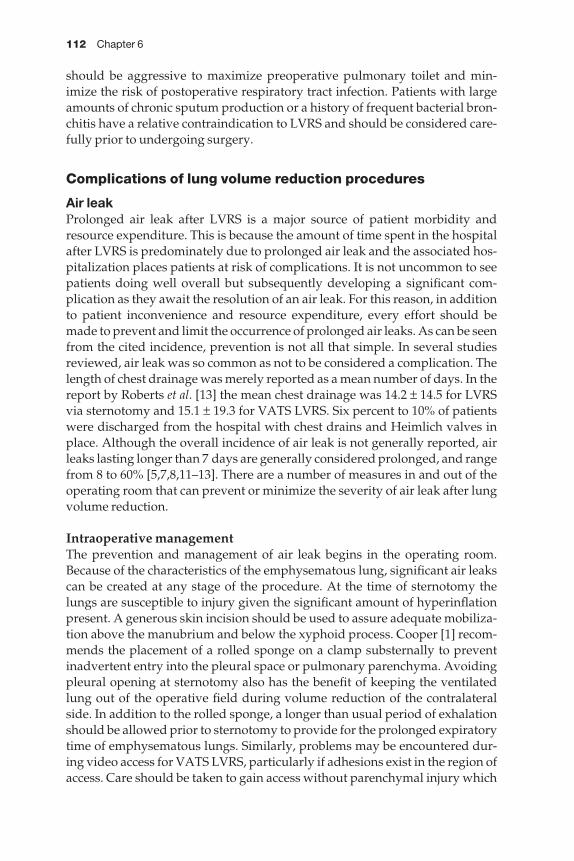
112 Chapter 6
should be aggressive to maximize preoperative pulmonary toilet and min-imize the risk of postoperative respiratory tract infection. Patients with largeamounts of chronic sputum production or a history of frequent bacterial bron-chitis have a relative contraindication to LVRS and should be considered care-fully prior to undergoing surgery.
Complications of lung volume reduction procedures
Air leakProlonged air leak after LVRS is a major source of patient morbidity andresource expenditure. This is because the amount of time spent in the hospitalafter LVRS is predominately due to prolonged air leak and the associated hos-pitalization places patients at risk of complications. It is not uncommon to seepatients doing well overall but subsequently developing a significant com-plication as they await the resolution of an air leak. For this reason, in additionto patient inconvenience and resource expenditure, every effort should bemade to prevent and limit the occurrence of prolonged air leaks. As can be seen from the cited incidence, prevention is not all that simple. In several studiesreviewed, air leak was so common as not to be considered a complication. Thelength of chest drainage was merely reported as a mean number of days. In thereport by Roberts et al. [13] the mean chest drainage was 14.2 ± 14.5 for LVRSvia sternotomy and 15.1 ± 19.3 for VATS LVRS. Six percent to 10% of patientswere discharged from the hospital with chest drains and Heimlich valves inplace. Although the overall incidence of air leak is not generally reported, airleaks lasting longer than 7 days are generally considered prolonged, and rangefrom 8 to 60% [5,7,8,11–13]. There are a number of measures in and out of theoperating room that can prevent or minimize the severity of air leak after lungvolume reduction.
Intraoperative managementThe prevention and management of air leak begins in the operating room.Because of the characteristics of the emphysematous lung, significant air leakscan be created at any stage of the procedure. At the time of sternotomy thelungs are susceptible to injury given the significant amount of hyperinflationpresent. A generous skin incision should be used to assure adequate mobiliza-tion above the manubrium and below the xyphoid process. Cooper [1] recom-mends the placement of a rolled sponge on a clamp substernally to preventinadvertent entry into the pleural space or pulmonary parenchyma. Avoidingpleural opening at sternotomy also has the benefit of keeping the ventilatedlung out of the operative field during volume reduction of the contralateralside. In addition to the rolled sponge, a longer than usual period of exhalationshould be allowed prior to sternotomy to provide for the prolonged expiratorytime of emphysematous lungs. Similarly, problems may be encountered dur-ing video access for VATS LVRS, particularly if adhesions exist in the region ofaccess. Care should be taken to gain access without parenchymal injury which
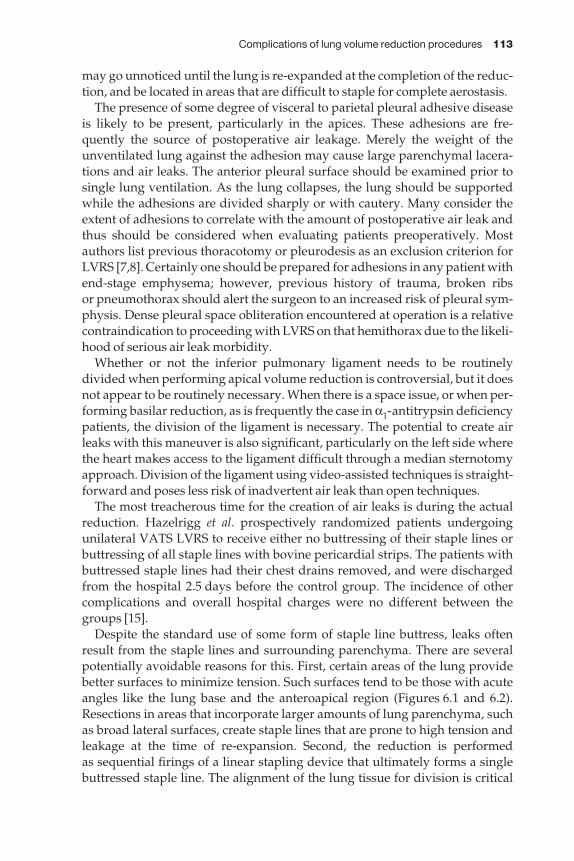
Complications of lung volume reduction procedures 113
may go unnoticed until the lung is re-expanded at the completion of the reduc-tion, and be located in areas that are difficult to staple for complete aerostasis.
The presence of some degree of visceral to parietal pleural adhesive diseaseis likely to be present, particularly in the apices. These adhesions are fre-quently the source of postoperative air leakage. Merely the weight of theunventilated lung against the adhesion may cause large parenchymal lacera-tions and air leaks. The anterior pleural surface should be examined prior tosingle lung ventilation. As the lung collapses, the lung should be supportedwhile the adhesions are divided sharply or with cautery. Many consider theextent of adhesions to correlate with the amount of postoperative air leak andthus should be considered when evaluating patients preoperatively. Mostauthors list previous thoracotomy or pleurodesis as an exclusion criterion forLVRS [7,8]. Certainly one should be prepared for adhesions in any patient withend-stage emphysema; however, previous history of trauma, broken ribs or pneumothorax should alert the surgeon to an increased risk of pleural sym-physis. Dense pleural space obliteration encountered at operation is a relativecontraindication to proceeding with LVRS on that hemithorax due to the likeli-hood of serious air leak morbidity.
Whether or not the inferior pulmonary ligament needs to be routinelydivided when performing apical volume reduction is controversial, but it doesnot appear to be routinely necessary. When there is a space issue, or when per-forming basilar reduction, as is frequently the case in α1-antitrypsin deficiencypatients, the division of the ligament is necessary. The potential to create airleaks with this maneuver is also significant, particularly on the left side wherethe heart makes access to the ligament difficult through a median sternotomyapproach. Division of the ligament using video-assisted techniques is straight-forward and poses less risk of inadvertent air leak than open techniques.
The most treacherous time for the creation of air leaks is during the actualreduction. Hazelrigg et al. prospectively randomized patients undergoing unilateral VATS LVRS to receive either no buttressing of their staple lines orbuttressing of all staple lines with bovine pericardial strips. The patients withbuttressed staple lines had their chest drains removed, and were dischargedfrom the hospital 2.5 days before the control group. The incidence of othercomplications and overall hospital charges were no different between thegroups [15].
Despite the standard use of some form of staple line buttress, leaks oftenresult from the staple lines and surrounding parenchyma. There are severalpotentially avoidable reasons for this. First, certain areas of the lung providebetter surfaces to minimize tension. Such surfaces tend to be those with acuteangles like the lung base and the anteroapical region (Figures 6.1 and 6.2).Resections in areas that incorporate larger amounts of lung parenchyma, suchas broad lateral surfaces, create staple lines that are prone to high tension andleakage at the time of re-expansion. Second, the reduction is performed as sequential firings of a linear stapling device that ultimately forms a singlebuttressed staple line. The alignment of the lung tissue for division is critical
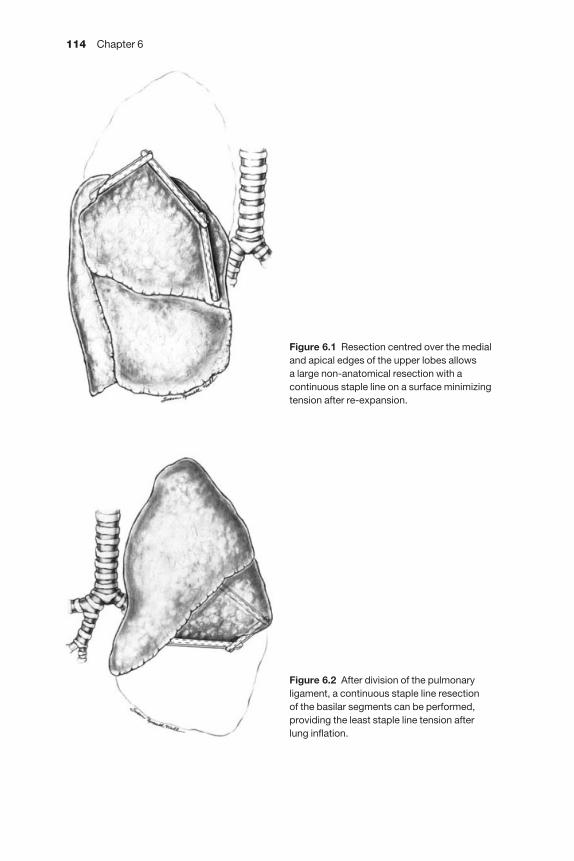
114 Chapter 6
Figure 6.1 Resection centred over the medialand apical edges of the upper lobes allows a large non-anatomical resection with acontinuous staple line on a surface minimizingtension after re-expansion.
Figure 6.2 After division of the pulmonaryligament, a continuous staple line resection of the basilar segments can be performed,providing the least staple line tension after lung inflation.
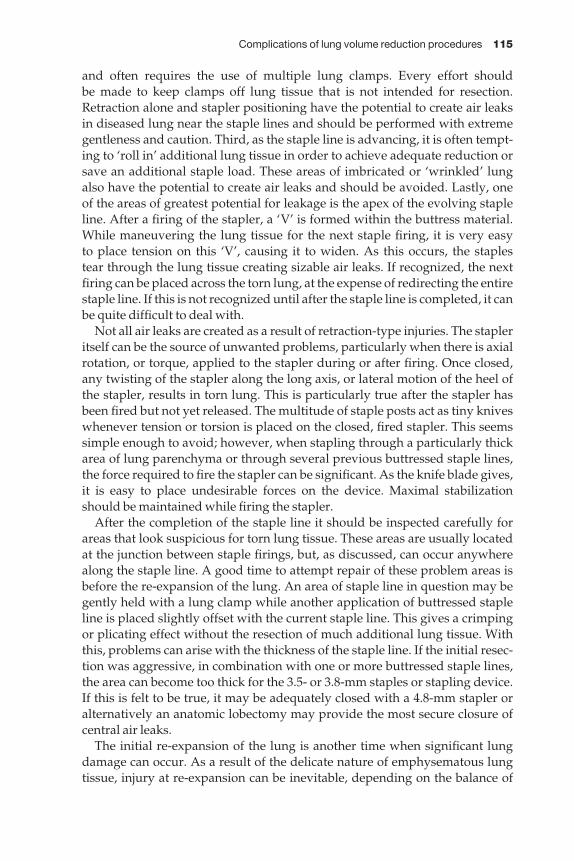
Complications of lung volume reduction procedures 115
and often requires the use of multiple lung clamps. Every effort should be made to keep clamps off lung tissue that is not intended for resection.Retraction alone and stapler positioning have the potential to create air leaks in diseased lung near the staple lines and should be performed with extremegentleness and caution. Third, as the staple line is advancing, it is often tempt-ing to ‘roll in’ additional lung tissue in order to achieve adequate reduction orsave an additional staple load. These areas of imbricated or ‘wrinkled’ lungalso have the potential to create air leaks and should be avoided. Lastly, one of the areas of greatest potential for leakage is the apex of the evolving stapleline. After a firing of the stapler, a ‘V’ is formed within the buttress material.While maneuvering the lung tissue for the next staple firing, it is very easy to place tension on this ‘V’, causing it to widen. As this occurs, the staples tear through the lung tissue creating sizable air leaks. If recognized, the nextfiring can be placed across the torn lung, at the expense of redirecting the entirestaple line. If this is not recognized until after the staple line is completed, it canbe quite difficult to deal with.
Not all air leaks are created as a result of retraction-type injuries. The stapleritself can be the source of unwanted problems, particularly when there is axialrotation, or torque, applied to the stapler during or after firing. Once closed,any twisting of the stapler along the long axis, or lateral motion of the heel ofthe stapler, results in torn lung. This is particularly true after the stapler hasbeen fired but not yet released. The multitude of staple posts act as tiny kniveswhenever tension or torsion is placed on the closed, fired stapler. This seemssimple enough to avoid; however, when stapling through a particularly thickarea of lung parenchyma or through several previous buttressed staple lines,the force required to fire the stapler can be significant. As the knife blade gives,it is easy to place undesirable forces on the device. Maximal stabilizationshould be maintained while firing the stapler.
After the completion of the staple line it should be inspected carefully forareas that look suspicious for torn lung tissue. These areas are usually locatedat the junction between staple firings, but, as discussed, can occur anywherealong the staple line. A good time to attempt repair of these problem areas isbefore the re-expansion of the lung. An area of staple line in question may begently held with a lung clamp while another application of buttressed stapleline is placed slightly offset with the current staple line. This gives a crimpingor plicating effect without the resection of much additional lung tissue. Withthis, problems can arise with the thickness of the staple line. If the initial resec-tion was aggressive, in combination with one or more buttressed staple lines,the area can become too thick for the 3.5- or 3.8-mm staples or stapling device.If this is felt to be true, it may be adequately closed with a 4.8-mm stapler oralternatively an anatomic lobectomy may provide the most secure closure ofcentral air leaks.
The initial re-expansion of the lung is another time when significant lungdamage can occur. As a result of the delicate nature of emphysematous lungtissue, injury at re-expansion can be inevitable, depending on the balance of

116 Chapter 6
the amount of lung resected, staple line location and integrity and strength ofthe tissue. After inspection of the staple line, the anesthesiologist is asked tohand ventilate the patient gently under direct vision, while keeping a watchfuleye on peak inspiratory pressures. Because of the large amount of lung paren-chyma drawn into the staple line, there is tremendous tension on both the stapleline and adjacent lung tissue as the lung expands. It is very important for thesurgeon and anesthesiologist to work very closely during this portion of theoperation. The minimal pressures necessary to achieve modest re-expansionand acceptable gas exchange should be used initially. In open cases it may helpto support the staple line manually to prevent rapid over-expansion. This alsohas the advantage of giving direct tactile feedback regarding lung tension thatmay not relate closely to airway pressures if there are secretions or a malposi-tioned double lumen tube. Once satisfactory ventilation has resumed, atten-tion can turn to the contralateral lung. Some surgeons prefer the feedback ofhand ventilation during this phase, but most important is close communica-tion between the surgeon and the anesthesiologist, assuring adequate ventila-tion without air trapping and allowing two-lung ventilation temporarily asnecessary to improve oxygenation without excessive airway pressures.
At the completion of lung reduction, the hemithorax should be filled withwarm saline solution and the lung should be inspected for areas of air leakage.Although the total absence of leak at this point is not uncommon, small leaksassociated with the staple line may be present. This should be accepted andthis type of leak usually seals within a few days. The goal is to detect largeunsuspected leaks, that are often not associated with the staple line. Largeblebs in areas of lung not resected are frequently the source of such leaks. Thesmell of anesthetic gases during the procedure is a clue to the presence of alarge leak. An excellent way to handle these leaks, when easily accessible, is with additional stapling with buttressed staples. Suture plication with orwithout a pericardial pledgett can reduce the amount of leakage but will rarelymake it stop completely. Another consideration is the use of fibrin glue. Untilrecently, its use was impractical due to the amount of time necessary to obtainthe components from the blood bank. Currently, commercially availablepreparations have made the use of fibrin glue more practical by significantlydecreasing the time to availability and eliminating the transfusion risk. Thismay prove to be beneficial and a decreased length of stay would certainly justify its expense. Recently, in a report by Macchiarini et al., an absorbablesynthetic sealant was used after pulmonary resection in an animal study,significantly reducing the number of animals with postoperative air leak [16].In addition to fibrin glue, the use of commercially available cyanoacrylate glue has been reported in the treatment of air leaks from other etiologies [17].The authors have used fibrin glue successfully to control air leaks after cauterytumor excision or with anatomically difficult air leaks deep within a fissure. If these maneuvers are unsuccessful, if the area is not accessible or if anatomicresection is not appropriate, the leak should be accepted rather than risk wor-sening of the damage with continued efforts at exposure and repair.
Complications of lung volume reduction procedures 117
Maneuvers involving the pleura can be performed when significant air leakor space issues seem likely. Apical pleural tents can be performed with greatease and minimal morbidity or added operating time. They may shorten the time of leakage by eliminating the intrapleural space and allowing approx-imation of lung and suture line with pleura. Pleurectomy or pleural abrasionwhich can be performed to promote adhesions and leak closure would com-plicate performance of a subsequent lung transplant. Therefore, careful con-sideration should be given prior to using these procedures in patients that arecurrent or potential transplant candidates.
Postoperative managementIt is not uncommon to detect an air leak either at the completion of the operative procedure or in the immediate postoperative period despite beingapparently leak-free at the time of chest closure. This is probably due to con-tinued expansion of the lung with increasing tension on the suture line.Management in the peri-extubation period is very important from an air leakstandpoint. It is particularly difficult at this time, because arterial pCO2 levelscan exceed 100 mmHg after combined single-lung ventilation and there will besome sense of urgency to reduce the CO2 level in preparation for extubation.At the completion of the procedure, neuromuscular blockade is reversed, the patient is allowed spontaneous respiration and is then extubated prior to the excitement phase and is supported with mask-assisted ventilation [18].Vigorous coughing at this time is to be avoided as it will frequently cause orworsen an air leak.
Adequate chest drainage is important in the management of postoperativeair leak. We place two thoracic drains on each side, one anteroapical and one in the posterior diaphragmatic sulcus. The routine use of chest tube suction inthis setting is controversial. Some recommend routine suction for 24–48 h,even in the absence of air leak or pneumothorax. Others advocate water seal,with suction applied only for a large pneumothorax or pneumothorax withrespiratory distress. The use of suction for asymptomatic apical air spaces isalso controversial. Some surgeons prefer to maximize lung expansion and sub-sequent pleural approximation as in other pulmonary surgery, while othersprefer to avoid the potential deleterious effects of suction and accept small to moderate apical spaces. Although air leaks have not been shown to be eliminated more quickly without suction in a randomized trial, many thoracicsurgeons firmly believe that less suction or no suction significantly decreasesthe magnitude and duration of postoperative air leak [19]. Regardless, small or moderate air leaks are expected to seal in the first 72–96 h if there is pleuralto pleural apposition. Large air leaks, with continuous leakage throughout therespiratory cycle, are more difficult to manage. Using the minimum amount of suction that maintains lung expansion will also minimize the amount of airleak. Despite this, a significant percentage of the inspiratory volume can be lostto air leak. Occasionally, hypocapnea from this degree of air exchange resultsin a significant respiratory alkalosis. When profound, mechanical ventilatory
118 Chapter 6
support may be required to limit the inspiratory volume. Compensation by theprolongation of the inspiratory time usually results in adequate ventilationand oxygenation. Consideration may be given to reoperation in an effort tolimit the volume of air leakage. The need for surgical re-exploration should be carefully assessed and only undertaken when all non-operative measureshave failed to stabilize the situation. Surgical attempts to treat air leak in thepostoperative period can be very gratifying if a discrete correctable cause of the leak is identified. However, further surgical manipulation of the lung can also result in significant exacerbation of the amount of leakage. Thoracicdrains are removed 24 h after the cessation of air leak. When an air leak is present and the patient is stable, the tube(s) can be connected to a one-wayvalve to allow the patient to be discharged from hospital, with the tube laterremoved in an out-patient visit.
Respiratory tract infection
The incidence of respiratory tract infection after LVRS is significant and can be life-threatening. Comparison of incidence is difficult because of differentdefinitions used. Reports in the literature vary from 4 to 50% [5,7,8,11–13]. Thehigher numbers probably reflect the reporting of all respiratory infectionsincluding upper and lower respiratory tract infections. True bacterial pneumo-nia as reflected by purulent sputum, positive culture, fever, leukocytosis andinfiltrate on radiograph occurs in approximately 4–15% of patients after LVRS.The consequences of pneumonia in this group of patients are severe, withRoberts reporting a mortality of 40% in patients who acquired a postoperativepneumonia [13]. It is our experience that even when patients survive post-operative pneumonia, they obtain subjectively less overall benefit from LVRS. Therefore, efforts to prevent respiratory infections are of paramountimportance in producing favorable results and minimizing mortality.
Prevention of postoperative respiratory infections begins with meticulouspain control in order to minimize the detrimental effects of sternotomy or thor-acoscopy on respiratory mechanics and pulmonary toilet. This starts with theaccurate, reliable preoperative placement of a thoracic epidural catheter. Eventhough a thoracic epidural does not completely block the pain of a median ster-notomy, the amount of oral and parenteral analgesia required is significantlyless when a functioning epidural catheter is utilized. The ability to minimizethe amount of narcotic administration is so important that some recommendthe placement of the catheter under fluoroscopic guidance to assure accurateplacement at the T3–4 level [18]. Incomplete or unilateral blocks are unaccept-able and require catheter adjustment or, if necessary, timely replacement. A few hours of inadequate pain relief, or high-dose systemic narcotics can be profoundly detrimental with regard to pulmonary toilet and overall oxy-genation and ventilation. The complete support of an acute pain managementteam, available around the clock, is necessary to minimize the sequelae of poorpain control or narcotic over-sedation.

Complications of lung volume reduction procedures 119
Sympathetic blockade associated with epidural local anesthetic agentsshould be anticipated. Moderate hypotension may not require treatment, butin an effort to minimize fluid administration, α-agonists such as phenyle-phrine may be used. It is usually possible to wean the α-agonist over the first12–24 h postoperatively. Ketorolac is a useful adjunct to postoperative painmanagement that helps to reduce the amount of narcotic required. In this set-ting, renal function should be followed closely given the relative hypovolemiaand hypotension that many of these patients experience. To prevent renal or gastrointestinal complications, ketorolac should be written for 48–72 hcourses with clinical re-assessment prior to renewal.
If these measures do not adequately control postoperative pain, as deter-mined by adequacy of pulmonary toilet and secretion clearance, some sys-temic narcotic may be required. Oral agents are avoided until the epidural hasbeen removed, which usually coincides with the removal of the chest drains.When a prolonged air leak is present, the epidural may be removed safely afterfour or five postoperative days. Parenteral narcotics are best given as smalldoses of a short-acting agent to prevent respiratory depression. Narcotic usemust be monitored very carefully to avoid over-sedation with subsequent CO2retention and respiratory failure. A very low-dose patient-controlled analgesia(PCA) with continuous monitoring may optimize systemic analgesia. If thereis any hypercapnia by blood gas analysis or the patient is too sedated to per-form pulmonary toilet exercises, the narcotics are stopped and a reversal agentis used if necessary.
Other measures are utilized to maximize pulmonary toilet and thereforeminimize respiratory tract infections. Generous use of nebulized and metereddose β-agonists are used for both bronchodilation and to facilitate secretionmobilization. Incentive spirometry, early mobilization, and chest physio-therapy are routine. The patient is placed upright in a bedside chair post-operatively after arrival from the postanesthesia unit to the intensive care unit.Ambulation is expected on postoperative day 1, which often requires portablesuction devices to maintain chest tube suction. Physical therapists that special-ize in the care of these patients help to assure that they are mobilized safely and regularly despite the amount of associated equipment. When used aggress-ively in a motivated patient, these measures usually suffice for the manage-ment of pulmonary secretions. Occasionally, additional measures such asnaso-tracheal suctioning, fiberoptic bronchoscopy or small-bore tracheotomyas a way to provide pulmonary toilet (Minitrach II; Portex, Keene, NH, USA)are required.
Naso-tracheal suctioning is a profound motivational measure for somepatients and is very effective for the patient who needs occasional assistance inclearing retained secretions. It is not ideal for patients who require frequentsuctioning. If secretions are retained despite naso-tracheal suctioning, fiber-optic bronchoscopy is performed to obtain a sputum specimen as well as fordirected pulmonary toilet. This may be required daily or even twice daily in some patients. If naso-tracheal suctioning or bronchoscopy are required

120 Chapter 6
more frequently than this, a small-bore tracheostomy, or ‘mini-trach’ can beperformed at the bedside through the cricothyroid membrane under localanesthesia. Commercially prepared kits are available for this procedure whichis quick and simple. This sheath provides access for diagnostic and therapeuticmaneuvers with minimal patient discomfort or sequelae.
When respiratory tract infections do occur, they must be treated early andaggressively. Classically, nosocomial pneumonias would be diagnosed onlywhen multiple criteria were present including fever, purulent sputum, posit-ive cultures from a tracheal aspirate or sputum specimen, leukocytosis andinfiltrate on chest radiograph. In this patient population it may not be wise to wait for multiple criteria to be present. If any one of the clinical indicatorsabove is present without an alternative explanation, it is prudent to obtainpromptly a reliable sputum specimen for Gram stain and culture and sensitivity and begin broad-spectrum antibiotics with double coverage forPseudomonas species. Antibiotics are then modified based upon the cultureresults and given for a full 10–14-day course. The mobilization and clearance of secretions remains an important adjunct to antibiotic treatment. Similar to pneumonia prevention strategies, adequate analgesia, patient mobilizationand secretion management interventions should be maximized.
Respiratory failure
The need for reintubation for respiratory failure after LVRS is a particularlyconcerning complication. It is uncommon that a patient dies after LVRS with-out first demonstrating respiratory failure. In the report of Cooper et al. of 150patients, 11 (7%) required mechanical ventilation at some point during theirpostoperative course [5]. Of these, five went on to require tracheostomy andthree ultimately died in hospital. Similarly, in the meta-analysis depicted inTable 6.1, 11.5% of patients required reintubation and ventilation, with anoverall mortality of 4.6%. Thus, respiratory failure with reintubation, althoughnot exceedingly common, carries an associated mortality of approximately40%.
Patients who require reintubation after reduction surgery can be categor-ized into one of three groups: those requiring early reintubation as a result ofanesthetic or pain management difficulty, those requiring early reintubationfor inadequate gas exchange, and those requiring late reintubation for respir-atory failure secondary to respiratory tract infection. These distinctions are useful not only for prognostic reasons, but for treatment strategy as well.
It is not uncommon for patients to demonstrate significant hypercapniaimmediately after the completion of a reduction procedure, with arterial pCO2levels > 80 mmHg. In an effort to minimize barotrauma, hand ventilation is used with caution and the patient is extubated in a deeper anesthetic stage to prevent harsh coughing or gagging. As a result of these maneuvers, gasexchange can be tenuous for a period after extubation. Reintubation may berequired if somnolence, as a result of hypercapnia, results in worsening CO2
Complications of lung volume reduction procedures 121
retention with hemodynamic compromise. Similarly, patients with inade-quate pain relief may experience worsening CO2 retention from hypoventila-tion. Intubation may be required if these conditions cannot be reversed prior tohemodynamic embarrassment. Over-sedation with resultant hypoventilationrequiring reintubation may also be related to systemic narcotic administration.Given a certain component of somnolence from postoperative hypercapnia,even trivial amounts of systemic narcotic may result in early respiratory fail-ure. With an experienced anesthesiologist these problems should rarely neces-sitate reintubation. When it is required, the causative factors may be addressedwith expected successful extubation a few hours after reintubation. Theseevents should not affect overall length of stay or outcome unless associatedbarotrauma has resulted in the development or exacerbation of air leakage.
It is particularly worrisome when patients require reintubation for inade-quate gas exchange in the absence of pain control or over-sedation issues.Oxygenation is rarely a problem after LVRS because of the ability to admin-ister supplemental oxygen. Indeed, relative hyperoxemia at the completion of the procedure may contribute to respiratory depression in patients withchronic hypercapnia. Maintaining arterial oxygen levels close to baseline is aroutine strategy at the time of extubation. Theoretical improvement in ventila-tion as a result of the reduction procedure, in the form of normalization ofdiaphragmatic function and improvement in functional airway obstruction,can be offset by the derangements in respiratory mechanics resulting from the surgical insult. This may not be tolerated by patients who are frequentlytenuous even in the preoperative period. It may therefore be necessary to provide mechanical ventilatory support to assist in reducing CO2 from supra-physiological to normal levels. At this point, some patients will be capable of maintaining adequate ventilation allowing extubation. Meticulous paincontrol and pulmonary toilet are particularly important in keeping these fragile patients extubated.
Some patients will not tolerate weaning of ventilatory support because ofpCO2 retention. In these patients, the perturbations in respiratory mechanicsas a result of the procedure are greater then the early improvements in ventila-tion. The duration of this is variable. Persistent CO2 retention despite the optimization of pain management and pulmonary toilet will usually requireintermediate or long-term ventilatory support. As respiratory mechanics normalize over the ensuing days to weeks, there is hope for separation frommechanical assistance. It has been our experience that early tracheostomy isbeneficial in the management of this group of patients. Tracheostomy helpswith weaning and placement strategies, pulmonary secretion management,and patient comfort issues. We have not experienced problems associated withearly tracheostomy after median sternotomy.
Minimizing the number of patients that require chronic ventilator supportafter LVRS is one of the primary goals of the patient selection process.Although a discussion regarding the preoperative evaluation and screen-ing process is not the focus of this chapter, a few comments as it relates to

122 Chapter 6
postoperative respiratory failure are warranted. There is controversy regard-ing the appropriateness of LVRS in patients with baseline CO2 retention. Therange of resting arterial pCO2 for exclusion from most published series is between 45 and 55 mmHg [1,5,7,13]. Most agree that a resting pCO2 > 55mmHg carries a prohibitive risk of postoperative respiratory failure leading todeath or chronic ventilatory support. Likewise, most agree that a resting pCO2< 45 mmHg correlates with a reasonably low risk of postoperative ventilatoryinsufficiency. There is controversy regarding the management of the signi-ficant number of patients that fall between 45 and 55 mmHg. In 1996, Szekelyet al. published a report of preoperative predictors of operative morbidity andmortality after LVRS [20]. In this analysis, only two preoperative factors cor-related with unacceptable postoperative outcome, as defined by death within6 months or hospitalization ≥ 21 days. These factors were poor performanceon a 6-min walk test and resting pCO2 > 45 mmHg, with the latter being a 10-fold negative predictor. Conversely, a European study published in 1998reported on 80 patients undergoing LVRS, 22 of whom had resting hyper-capnia > 45 mmHg [21]. Although the mortality in patients with hypercapniawas 9.1% vs. 5.2% in those with normal CO2 levels, this did not reach statisticalsignificance. ICU stays and duration of chest drainage were similar, andimprovement in FEV1 at 3 months favored the group with hypercapnia pre-operatively. It appears that the group of patients with resting arterial pCO2between 45 and 55 mmHg may gain significant benefit from LVRS but be athigher risk of postoperative respiratory failure. It may be wise to considerthese patients at higher risk and counsel them accordingly. It also may be pru-dent to consider these patients only if there are no other extenuating circum-stances, such as poor target areas for resection, high steroid dose, advancedage, significant sputum production or malnutrition. It is our general feelingthat even when no single overt exclusionary criterion exists, one or more ‘borderline’ conditions in combination with marginal resting hypercapnia is arelative contraindication to LVRS. It is the intention of the NETT investigatorsto address these issues.
Nosocomial pneumonia is the likely etiology in patients who experience laterespiratory failure requiring reintubation and mechanical ventilation. Earlyand aggressive treatment of hospital-acquired respiratory tract infections isrequired for patient salvage. Despite these efforts, late nosocomial pneumoniaresulting in respiratory failure carries a poor prognosis, often resulting in prolonged intubation, sepsis, multiorgan failure and death.
Hemorrhage
Significant bleeding can occur during LVRS independent of operative ap-proach. Although bleeding from sternotomy or VATS port sites can be trouble-some, it is rarely significant enough to require transfusion or reoperation. Mostbleeding of clinical significance originates at the buttressed staple line whichcan be life threatening on occasion. Hemorrhage can be intraparenchymal,
Complications of lung volume reduction procedures 123
intrapleural or both. Bleeding is frequently from major pulmonary arterial or venous branches and tends to occur when staple lines are too close to thehilum or major fissure or when staple lines are stressed by a large amount ofparenchyma. Vascular injury can be a result of linear or rotational forces on theclosed or closing stapler in a mechanism similar to that which results in airleakage, as previously discussed. When the bleeding is across the staple lineinto the pleural space, it can frequently be controlled with additional firings ofthe reinforced stapler, or by direct suture ligature. Similarly, when a parenchy-mal hematoma appears after stapling, attempts should be made to control thesource of hemorrhage and thus limit the size and functional significance of thehematoma. These maneuvers may be difficult using video-assisted techniquesand may require conversion to an open procedure to control the hemorrhage.Despite meticulous technique and careful inspection of staple lines, both re-operations and intraoperative mortalities have been described as a result ofmajor hemorrhage. It is difficult to extrapolate the exact incidence of post-operative hemorrhage requiring transfusion, re-exploration or death. Studiesthat do report the complication in the form of re-operation generally show a0–5% incidence with reported mortality < 1% [13].
Cardiac complications
Patients who undergo LVRS are at risk of the same perioperative cardiac com-plications as other thoracic surgery patients. Most patients who are candidatesfor reduction surgery are also at high risk of cardiac disease based on age, sex,smoking and sedentary lifestyle. Unfortunately, because exercise tolerance inthese patients is limited by pulmonary function, few patients present with a history of myocardial infarction (MI) or anginal symptoms. In one recentreport, 10 (11%) of 90 patients had one or more perioperative cardiac eventsincluding atrial fibrillation (n = 3), supraventricular tachycardia (n = 3), con-gestive heart failure (n = 4), myocardial ischemia (n = 2), and premature vent-ricular beats (n = 1) [21]. The overall incidence of perioperative acute MI is low, reported between 0 and 2% [5,7,8,11–13]. The low incidence of MI andother cardiac events is attributed to the aggressive screening process that mostcentres employ prior to LVRS and the fact that patients with significant cardiacdisease detected preoperatively are generally not offered surgical treatmentoptions. On the other hand, self-selection may occur prior to presentation forpossible LVRS due to the high baseline ‘stress’ of dyspneic patients, eliminat-ing patients with concomitant coronary artery disease (CAD).
In 1997, Thurnheer and associates reported on the incidence of CAD inpatients being evaluated for LVRS [24]. Of 46 patients eligible for LVRS by other criteria, 44 underwent coronary angiography. All patients with a history of CAD and 15% of patients without a history of CAD demonstratedsignificant disease, emphasizing the prevalence of CAD in this patient popula-tion. Echocardiography with and without dobutamine stress has been used asa screening tool prior to LVRS [22]. Despite the hyperinflation of the lungs,
124 Chapter 6
images were obtained that satisfactorily assessed wall motion abnormalities,ejection fraction, valvular function and right heart abnormalities that mightsuggest pulmonary hypertension or cor pulmonale. Correlation betweenechocardiographic findings and catheterization results revealed that normalright heart findings on echocardiographic examination obviated the need forright heart catheterization. Correlation with results of coronary angiographywere less reliable, however, with a sensitivity and specificity of 60 and 83%,respectively [22]. Although the authors concluded that all patients being evalu-ated for LVRS should be screened for cardiac disease using function and/orinvasive studies, many centres reserve functional testing for patients withsymptoms, signs, or ECG evidence of CAD. Patients should routinely undergosurface echocardiographic evaluation to identify right heart abnormalities andproceed to right heart catheterization if such abnormalities are discovered.Functional evaluation by dobutamine stress echocardiography or dipyri-damole thallium-201 perfusion scintigraphy should be performed in selectedpatients, followed by coronary angiography when indicated. Only by suchaggressive evaluation will it be possible to maintain such low perioperativecardiac morbidity in this high-risk population.
When cardiac complications do occur, they are treated in a fashion similar toother thoracic surgical patients. Because of the risk of atrial fibrillation andsupraventricular tachycardia, patients are monitored while in the ICU or onthe ward. Myocardial ischemia or infarction should be suspected whenever a patient has hemodynamic instability that cannot be directly attributed toanother factor. Chest pain that is different from the patients ‘usual’ sternotomypain should be evaluated carefully any time in the postoperative period.
Gastrointestinal complications
Gastrointestinal (GI) complications occur in patients after LVRS with an incid-ence similar to that of other postoperative patients. Both minor and major GIcomplications have been documented. Bleeding, reflux, with or without aspira-tion, adynamic ileus, obstipation and perforation have all been documented in LVRS patients. As a group, GI complications probably are underreported in the published series because several of these conditions may not impactpatient outcome or hospitalization. In one report of over 100 patients, GI bleed-ing and perforation each occurred in five patients, giving a combined GI mor-bidity of 7% and were the only GI morbidities reported in that series [13]. Inthis same series, comparing LVRS by sternotomy with VATS LVRS, the five GIperforations all resulted in death and were responsible for five of the 11 deathsin the series. All of the GI perforations were in the sternotomy group. Thepatients in this group were significantly older than those undergoing VATSLVRS, but there was no significant difference in other measured parametersincluding non-steroidal anti-inflammatory drug use, narcotic use, steroids,duration of epidural, and duration of chest drainage. In several other series, GI perforation has been reported and may pose a particular problem in this
Complications of lung volume reduction procedures 125
patient population [5,8,12]. Postoperative pneumoperitoneum can be decept-ive, as it is not uncommon for patients with air leaks and anterior chest drainsto develop pneumoperitoneum from inadvertent placement of the tubethrough a small portion of peritoneum. When this is demonstrated on chestfilm, it is important to assess the patient clinically and document the absence ofsigns or symptoms of GI perforation as a source of the intraperitoneal air.
Like any postoperative thoracic surgery patient, GI bleeding can develop.When GI bleeding does occur, it should be managed in the usual fashionafluidresuscitation, transfusion, H2 blockers or proton-pump inhibitors, and endo-scopy for diagnosis and/or therapeutic interventionawith surgery reservedfor patients with bleeding refractory to medical therapy. Protection of the airway should be considered in any patient with significant bleeding and isparticularly important in these patients.
Wound complications
Sternal wound occurs after LVRS and can be particularly debilitating.Although the incidence of wound problems after LVRS does not appear to be any higher than after other operations utilizing median sternotomy, the perturbations in respiratory mechanics after sternal dehiscence can negate the benefits of the procedure. Appropriate perioperative antibiotics should beadministered to prevent sternal infection and operative technique should bemeticulous to prevent infection, dehiscence, or sternal non-union. Great careshould be taken to assure that the sternotomy is midline, and retraction shouldavoid sternal fractures. Secure closure is paramount to withstand aggressivepostoperative pulmonary toilet maneuvers. Should sternal instability occurpostoperatively as a result of such maneuvers, the patient should be takenback to the operating room for sternal fixation. If sternal wound infection is themechanism of dehiscence, early operative debridement and flap closureshould be performed in a fashion that maximizes stability.
Pulmonary embolus
The incidence of deep venous thrombosis (DVT) and pulmonary embolus inLVRS patients is unknown. Although this remains a theoretical and potentiallife-threatening complication, the lack of reports of pulmonary emboli as asignificant source of morbidity and mortality probably reflects the early andaggressive mobilization policy employed by most centres performing LVRS.This in combination with routine prophylaxis should keep the incidence ofDVT and pulmonary embolus low.
Psychiatric complications
Patients who have end-stage emphysema are prone to develop emotional andanxiety-related issues. Many patients see LVRS as a hope to return to a more

126 Chapter 6
normal lifestyle and proceed with preoperative screening and rehabilitationwith much expectation and enthusiasm. The operation itself, rather than therecovery, is often seen as the completion of the process. Combining the height-ened anticipation of surgery with benefits that are often not appreciated forweeks to months after the procedure predisposes these patients to anxiety anddepression that may alter outcome. Preoperative anxiety disorders or panicattacks have been associated with an increase in postoperative complicationsand mortality, and exacerbations in the postoperative period can complicatethe assessment of physiological abnormalities, such as hypoxemia or pneu-mothorax [25]. Depression is common after any major surgery and can resultin poor motivation and anorexia, easily leading to other complications, such aspneumonia and respiratory failure. These problems must be addressed andtreated aggressively as they occur after surgery, including pharmacologicalintervention if necessary.
Summary
A successful lung volume reduction program requires a multidisciplinaryteam approach that is committed to the significant amount of care that thesepatients require. If surgical options are to be available to patients with end-stage emphysema, it is imperative that LVRS centres focus on the min-imization of perioperative morbidity and mortality, beginning with patientevaluation and selection. Intraoperative considerations by both surgeon andanesthesiologist significantly affect length of stay and ultimate outcome.Meticulous postoperative care with focus on the prevention and aggressivetreatment of complications is the only way to achieve consistent success in thisgroup of fragile patients.
References
1 Cooper JD, Trulock EP, Triantafillou AN et al. Bilateral pneumectomy (volume reduction)for chronic obstructive pulmonary disease. J Thorac Cardiovasc Surg 1995; 109: 106–119.
2 Brantigan OC, Mueller E. Surgical treatment of pulmonary emphysema. Am Surg 1957; 23:789–804.
3 Brantigan OC, Mueller E, Kress MB. A surgical approach to pulmonary emphysema. AmRev Respir Dis 1959; 80: 194–202.
4 Brantigan OC, Kress MB, Mueller EA. The surgical approach to pulmonary emphysema.Dis Chest 1961; 39: 485–501.
5 Cooper JD, Patterson GA, Sundaresan RS et al. Results of 150 consecutive bilateral lungvolume reduction procedures in patients with severe emphysema. J Thorac Cardiovasc Surg1996; 112: 1319–1330.
6 Bingisser R, Zollinger A, Hauser M et al. Bilateral volume reduction surgery for diffusepulmonary emphysema by video-assisted thoracoscopy. J Thorac Cardiovasc Surg 1996;112: 875–882.
7 Daniel TM, Chan BB, Bhaskar V et al. Lung volume reduction surgery: case selection, oper-ative technique and clinical results. Ann Surg 1996; 223: 526–533.
Complications of lung volume reduction procedures 127
8 Naunheim KS, Keller CA, Krucylak PE et al. Unilateral video-assisted thoracic surgicallung reduction. Ann Thorac Surg 1996; 61: 1092–1098.
9 The National Emphysema Treatment Trial Research Group. Rationale and design of thenational emphysema treatment trial: a prospective randomized trial of lung volumereduction surgery. Personal communication, October 1998.
10 Cooper JD. The history of surgical procedures for emphysema. Ann Thorac Surg 1997; 63:312–319.
11 Travaline JM, Furakawa S, Kusma AM et al. Bilateral apical vs nonapical stapling resectionduring lung volume reduction surgery. Chest 1998; 114: 981–987.
12 Hazelrigg SR, Boley TM, Magee MJ et al. Comparison of staged thoracoscopy and mediansternotomy for lung volume reduction. Ann Thorac Surg 1998; 66: 1134–1139.
13 Roberts JR, Bavaria JE, Wahl P et al. Comparison of open and thoracoscopic bilateral vol-ume reduction surgery: complications analysis. Ann Thorac Surg 1998; 66: 1759–1765.
14 Mazolewski P, Turner JF, Baker M, Kurtz T, Little AG. The impact of nutritional status on the outcome of lung volume reduction surgery: a prospective study. Chest 1999; 116:693–696.
15 Hazelrigg SR, Boley TM, Naunheim KS et al. Effect of bovine pericardial strips on air leakafter stapled pulmonary resection. Ann Thorac Surg 1997; 63: 1573–1575.
16 Macchiarini P, Wain J, Almy S, Dartevelle P. Experimental and clinical evaluation of a newsynthetic, absorbable sealant to reduce air leaks in thoracic patients. J Thorac CardiovascSurg 1999; 117: 751–758.
17 Horsley SW, Miller JI. Management of the uncontrollable pulmonary air leak withcyanoacrylate glue. Ann Thorac Surg 1997; 63: 1492–1493.
18 Triantafillou AN. Anesthetic management for bilateral volume reduction surgery. SemThorac Cardiovasc Surg 1996; 1: 94–98.
19 Reynolds BR, Wood DE. A randomized prospective trial of suction versus water seal afterlung volume reduction surgery. Personal communication, 1997.
20 Szekely LA, Oelberg DA, Wright C et al. Preoperative predictors of operative morbidityand mortality in COPD patients undergoing bilateral lung volume reduction surgery.Chest 1997; 111: 550–558.
21 Wiser W, Klepetko W, Senbaklavaci O et al. Chronic hypercapnia should not excludepatients from lung volume reduction surgery. Eur J Cardiothorac Surg 1998; 14: 107–112.
22 Bach DS, Curtis JL, Christensen PJ et al. Preoperative echocardiographic evaluation ofpatients referred for lung volume reduction surgery. Chest 1998; 114: 972–980.
23 Hogue CW, Stamos T, Winters KJ et al. Acute myocardial infarction during lung volumereduction surgery. Anesth Analg 1999; 88: 332–334.
24 Thurnheer R, Muntwyler J, Stammberger U et al. Coronary artery disease in patientsundergoing lung volume reduction surgery for emphysema. Chest 1997; 112: 122–128.
25 Miller JI Jr, Lee RB, Mansour KA. Lung volume reduction surgery: lessons learned. AnnThor Surg 1996; 61: 1464–1468.
CHAPTER 7
Complications of lung transplantation
Paul F Waters
Complications of thoracic surgery
Lung transplantationThis chapter will discuss the complications directly related to lung transplanta-tion. The procedure may be performed through several standard thoracic inci-sions. Wound complications related to these will be discussed elsewhere in thisvolume. For purposes of discussion the complications will be divided into thosethat occur early and late in the postoperative period. Single lung transplantationis performed for patients with restrictive lung disease (e.g. pulmonary fibrosis),obstructive lung disease (e.g. emphysema) and pulmonary vascular diseasesuch as primary pulmonary hypertension or in patients with pulmonary vas-cular disease secondary to congenital heart abnormalities [1]. It is generallyperformed through a standard posterolateral thoracotomy, although a mediansternotomy has been used. Double lung transplant is generally performed forpatients with septic lung disease such as cystic fibrosis or bronchiectasis ofother etiologies. It is also sometimes done for pulmonary vascular disease oremphysema. The double sequential transplant procedure is usually carriedout through a bilateral anterior 4th interspace thoracotomy, either transverselydividing the sternum or leaving it intact [2]. Depending on the diagnosis, apatient may expect a 1-year actuarial survival in the 75% range as reported bythe International Society of Heart and Lung Transplantation Registry [3].
Early complicationsEarly complications are related to the anastomoses, to the graft or to recipientproblems. The standard implantation procedure involves a bronchial anastom-osis, and two vascular connections of the pulmonary artery and left atrium.The left atrial anastomosis includes both the inferior and superior pulmonaryveins. No reconstitution of the bronchial circulation is performed and con-sequently the implanted lung relies on the pulmonary circulation for both gasexchange and viability.
Air embolismMost single lung transplants are performed without cardiopulmonary bypass.Once the anastomoses are completed satisfactorily, the graft is reperfused and ventilated simultaneously. The pulmonary circulation of the transplanted
128
Complications of lung transplantation 129
lung contains residual preservation perfusate and air, both of which must beprevented from entering the left atrium. This is accomplished by severalmaneuvers. The patient is placed in the extreme Trendelenburg position soany inadvertent air in the left heart will avoid the cerebral circulation. Withboth the vascular anastomoses open, the atrial clamp is released, with the pulmonary artery (PA) clamp in place. This allows back bleeding through thelung and egress of unwanted material through the PA anastomosis. At thispoint the PA anastomosis is completed and the atrial clamp re-applied. The PAclamp is partially removed to allow anterograde flow, and venting through thestill open atrial anastomosis. Care must be taken to avoid full PA flow withoutthe open anastomosis. Once a suitable period has elapsed the atrial anastomo-sis is tied and the clamps removed simultaneously, and the lung re-ventilated.The anastomoses are examined for good flow, and hemostasis. The bronchial anastomosis is inspected for air leak, which if present is corrected with addi-tional sutures where necessary.
Reperfusion responseMost recipients will exhibit some degree of reperfusion response in the first 24–48 h after the transplant procedure. This may vary from being almostimperceptible to a fulminant reaction with serious and occasionally lethalresults. The precise etiology of the process is unknown but its pathophysiologysuggests a pulmonary capillary leak syndrome. It does not seem to be relatedto ischemic time, preservation technique or the precise method of reimplanta-tion. Studies have failed to determine immunological phenomena as a basis. Inthe most common scenario the patient will exhibit a modest but manageabledecline in oxygenation, a fluffy infiltrate of a varying degree with pleural effusion or some amount of increased chest tube fluid output. The problem isself-limiting and managed by judicious fluid balance, diuresis, ventilationwith PEEP, nitric oxide and continued appropriate hemodynamic support [4].The prophylactic use of inhaled nitric oxide appears to be a useful approach [5,6].Vascular anastomosis abnormality, particularly a partial venous obstruction,should be searched for and ruled out. In the fulminant situation the situationcan be more serious. The X-ray will demonstrate severe infiltrate or in somecases a complete ‘white-out’. Oxygenation may be difficult to maintain andhemodynamic instability is noted. In extreme cases extra-corporeal membraneoxygenator (ECMO) may be required to support the patient while the processruns its course [7,8]. The inflammatory response clearly produces vasoactivesubstances because hypotension, depressed myocardial function and peripheralprofound vasodilatation can be observed. The patient may appear as if theyare in septic shock. Many of these manifestations of ‘primary non-function’ canbe mimicked by a problem with the vascular supply to the graft, bacterialinfection and rejection eliminated as a cause. Most centres performing lungtransplantation will have ECMO available if oxygenation and gas exchangebecome impossible in the severe case. Prolonged use of ECMO has resulted inpoor results and high mortality but as a temporary strategy it has merit [9].

130 Chapter 7
Various techniques have been suggested for use prophylactically inattempts to prevent the development of reperfusion response. However, nonehas been predictably effective in its prevention [10–12].
Vascular anastomotic complicationsIf care is not taken with the configuration and positioning of the vascular con-nections poor flow and occasionally thrombosis can occur. This is a disastrouscomplication that must be recognized promptly and treated with a return to the operating room and correction of the problem. Several methods are available for the evaluation of these. A simple bedside bronchoscopy mayreveal a severely ischemic airway, suggesting a problem with its blood supply.Conversely, if the airway is obviously well vascularized it is unlikely that the PA has completely thrombosed. A portable quantitative perfusion scan can also be performed in the ICU setting. In general it should demonstratepreferential perfusion of the graft. If not, then usually rapid evaluation and re-exploration are necessary. Transesophageal echocardiography with an experi-enced operator can demonstrate pulmonary arterial flow, on the transplantedside. The venous flow may be more difficult to demonstrate, but obviously if there is good PA flow then venous outflow is satisfactory. Angiography isseldom used at this stage since prompt correction of a suspected problem is necessary to prevent irreversible damage to the graft. Once again, if there issufficient concern about the vascular anastomoses being patent then a promptre-exploration is indicated. Problems with the anastomoses discovered at thoracotomy are usually due to redundant vessel or impingement with localtissue such as pericardium. The anastomosis is revised and thombectomy performed.
Poor flow or lack of flow through the venous outflow tract can be a subtlediagnostic challenge. In the fulminant, thrombosed situation the patient willpresent with a pulmonary edema picture in the transplant and an abnormaltransesophageal echocardiography (TEE). Technical misadventure with theanastomosis is usually the cause.
In most cases where there is a complication with the anastomoses the dia-gnosis is readily apparent. However, on occasion because of the physiology and the residual native lung providing some support, it may not be obvious. I have personally seen a transplant patient, with emphysema, extubated andbreathing spontaneously, albeit with high oxygen requirements, with com-plete thrombosis of the PA anastomosis following single lung transplant. Forthis reason it is mandatory to examine the vascular supply of the graft as a routine in the immediate transplant period using the tools described [13–15].
Bronchial anastomotic complicationsComplications with the bronchus do not usually occur in the first few dayspost transplant. Before the patient is transferred from the operating room the anastomosis is examined both at thoracotomy and bronchoscopically toensure a satisfactory situation. Any problems should be diagnosed and corrected at that time. Later, problems with healing, usually on an ischemic

Complications of lung transplantation 131
basis, do not develop until necrosis of a portion of the donor bronchus occurs.This is frequently at the 10–14-day mark. Complete failure is decidedlyuncommon and usually speaks of many other complications and an unsal-vageable situation. The more common scenario will be the development ofnew mediastinal air or of a pneumothorax. A pneumothorax should be treatedwith the insertion of a chest tube. It does not always imply a bronchial ana-stomotic problem. In any case, a bedside fiberoptic bronchoscopy should be performed to examine and assess the status. A chest computed tomography(CT) scan is a very useful tool to determine the nature of the bronchus and thedegree of contamination. Appropriate drainage, often done percutaneouslyunder CT-guided control is necessary. With this and judicious antibiotics and pulmonary toilet the defect will heal satisfactorily. Sometimes such anoccurrence in the early postoperative period will lead to subsequent stenosisor bronchomalacia.
Acute rejectionAcute rejection in the early post-transplant period is a very common occur-rence. Standard immunosuppression is based on cyclosporine or FK506 incombination with steroids and usually with the addition of mycophenilatemofetil or imuran. Cytolytic therapy with anti-lymphocyte globulin (ALG),anti-thymocyte globulin (ATG) or monoclonal anti-bodies is infrequentlyrequired. Acute rejection usually presents at about day 5–7 but can occur atany time. The patient will demonstrate deterioration in oxygenation, some-times flu-like symptoms, a low-grade temperature and non-specific X-raychanges. These include a slight perihilar infiltrate or ‘flare’, a diffuse groundglass appearance or a small pleural effusion. There can also be no X-raychanges at all in the early stages. A moderate leukocytosis may also beobserved. Infectious causes of this constellation of signs and symptoms arerapidly ruled out and the diagnosis of acute rejection made. Frequently a diag-nostic and therapeutic dose of ‘pulse’ steroids will be given. If the problem isrejection, all of the abnormalities should subside within 8–12 h if the process isin its incipient stages. A more established process will take longer to reverse.Transbronchial biopsy at this point is appropriate but requires an experiencedpathologist because of the changes associated with the inflammatory responseto the ischemic period and reimplantation phenomena. Failure of the clinicaldiagnosis to respond promptly should trigger an immediate re-evaluationwith transbronchial biopsies and if necessary, open lung biopsy to establishthe diagnosis.
Late complicationsThe complications that occur later are related to infection, rejection and airwayproblems.
InfectionBecause the graft always and forever remains exposed to the environment it issusceptible to opportunistic infection. These may be viral, fungal or bacterial.
132 Chapter 7
Cytomegalovirus infection Pneumonitis and generalized cytomegalovirus (CMV) disease are an ongoingproblem in the long-term management of transplant patients. Logistically andpractically very few programs perform donor to recipient matching withrespect to CMV status. Donor CMV status at the time of organ retrieval is fre-quently unreliable. For this reason, many programs, including ours, have usedan aggressive prophylaxis program against CMV. This involves high-doseganciclovir, intravenously for the first 3 months post transplant when the level of immunosuppression is highest. CMV pneumonitis can mimic acuterejection, although it is often associated with a leukopenia. The diagnosis ismade with transbronchial biopsy demonstrating the characteristic histologicalappearance and with the appropriate profile on serological testing. Treatmentis with high-dose ganciclovir. Oral ganciclovir is available but is extremelypoorly absorbed. Its efficacy is such that if the diagnosis is firm, intravenoustherapy is required. Other viral infections seen include herpes and Epstein–Barr virus.
Bacterial infection is common and should prompt a rapid response from thecare giver. Appropriate antibiotics in appropriate doses should be begunpromptly and tailored according to culture and sensitivity data. Once more,because of the chronic immunosuppression these infections can be fulminant.
Infection with Pneumocystis carinii is uncommon, since all programs instituteprophylaxis post transplant with twice weekly Septra or the like.
Fungal infection or at least colonization is seen frequently. Aspergillus,Candida, and less commonly Nocardia and other pathogens are seen andshould be looked for in unclear infectious scenarios. Bronchoscopic examina-tion with cultures and biopsies, percutaneous needle biopsies or open lungbiopsy may be necessary to establish the diagnosis. Oral antifungals are appro-priate for colonization, whereas invasive infections are much more serious andoften fatal.
Late airway complicationsAirway complications are either stenosis or bronchomalacia in the late post-operative period. Stenosis can be seen after a known airway problem in theearlier post-transplant period, such as a partial dehiscence. At other times thelesion can develop with no previous suggestion of trouble. It usually manifestswith poor function and abnormal pulmonary function tests identifying airwayobstruction. Bronchoscopy will make the diagnosis and treatment will be rigidbronchoscopy with dilation. Continued narrowing or recurrent problems canbe managed with either silastic or expandable mesh wall stents. Both of thesetechniques have yielded satisfactory results for stenosis, although the disad-vantage of the wall stents is that they can not usually be removed. Both types ofstent can be problematic because of colonization with infectious organismsand because patients may have difficulty raising secretions through them. Themore difficult problem to manage is that of bronchomalacia. These ‘floppy’ air-ways will lead to respiratory insufficiency because of their tendency to close

Complications of lung transplantation 133
during the respiratory cycle. Stenting is less successful since there is not a narrowarea to grip the stent. Mesh stents seem to be the better choice in this situation.
Bronchiolitis obliterans and bronchiolitis obliterans syndromeAs experience with isolated lung transplantation developed it became appar-ent that a percentage (probably 30–50%) of long-term survivors expressed a decline in pulmonary function, which was not due to acute rejection. Thisfirst manifested in a decline in objectively measured pulmonary functionaspecifically a drop in forced expiratory volume in 1 s (FEV1). This decline canbe expressed as a percentage of the best FEV1 obtained by the recipient in the post-transplant period. Transbronchial biopsies in such patients may notreveal the abnormality since the changes generally occur in the small airways.Sensitivity of transbronchial biopsy has been reported in wide ranges from 20to 70%. Pathologically the lesion progresses from a lymphocytic bronchiolitiswith epithelial damage to evidence of scarring in the submucosa, which is pre-sumably permanent. It is this scarring which becomes obliterative to small air-ways, which leads to the decline in function measured both subjectively by thepatient and objectively by pulmonary function tests. The so-called bronchiol-itis obliterans syndrome (BOS) is now defined based on FEV1 determinations.This has been addressed in a working formulation to characterize and gradeBOS [16]. The syndrome may remain stable but frequently can show a rapiddownhill course and death by respiratory failure. Treatment strategies, noneof which is reliably efficacious, include manipulation of immunosuppressiveregimens, additional chemotherapeutic agents (e.g. methotrexate) and otherapproaches such as photopharesis. Multivariate analysis of large series of lungtransplant recipients suggest that CMV infection, acute rejection, and lympho-cytic bronchiolitis noted on lung biopsy are associated with an increased incid-ence of BOS. Therefore, management to avoid these, if possible, would makesense. If BOS patients do not stabilize, then consideration of retransplantationbecomes inevitable. A multi-institutional report suggests that reasonableresults of retransplantation can be expected in ambulatory, non-ventilatedpatients who are more than 2 years beyond their original transplant [17,18].Certainly the experience with other organs in retransplantation would suggestthat it is a reasonable tactic. In long-term follow-up this BOS accounts for mostdeaths and remains the Achilles’ heel of lung transplantation.
References
1 International guidelines for the selection of lung transplant candidates. The AmericanSociety for Transplant Physicians (ASTP)/American Thoracic Society (ATS)/EuropeanRespiratory Society (ERS)/International Society for Heart and Lung Transplantation(ISHLT). Am J Respir Crit Care Med 1998; 58: 335–339.
2 Meyers B, Sundaresan S, Cooper JD, Patterson GA. Bilateral sequential lung transplantwithout sternal division eliminates post transplant complications. J Thorac Cardiovasc Surg1999; 117: 358–364.
134 Chapter 7
3 Trulock EP, Edwards LB, Taylor DO et al. The Registry of the International Society forHeart und Lung Transplantation: Twentieth Official Adult Lung and Heart-lungTransplant Report – 2003. J Heart Lung Transplant 2003; 22: 625–635.
4 Haydock DA, Trulock EP, Kaiser LR et al. Management of dysfunction in the transplantedlung: experience with 7 clinical cases. Ann Thorac Surg 1992; 53: 635–641.
5 Date H, Triantafillou A, Trulock E et al. Inhaled nitric oxide reduces human lung allograftdysfunction. J Thorac Cardiovasc Surg 1996; 111: 913–919.
6 Ardehali A, Laks H, Levine M et al. A prospective trial of inhaled nitric oxide in clinicallung transplantation. Transplantation 2001; 72: 112–115.
7 Zanati M, Pham SM, Keenan RJ, Griffith BP. Extracorporeal memberan oxygenation forlung transplant recipients with primary severe donor lung dysfunction. Transpl Int 1996;9: 227–230.
8 Meyers BF, Sundt TM III, Henry S et al. Selective use of extracorporeal membrane oxy-genation is warranted after lung transplantation. J Thorac Cardiovasc Surg 2000; 120: 20–26.
9 Glassman LR, Keenan RJ, Fabrizio MC et al. Extracorporeal membrane oxygenation as anadjunct treatment for primary graft failure in adult lung transplant recipients. J ThoracCardiovasc Surg 1995; 110: 723–726.
10 Struber M, Hohlfeld JM, Fraund S, Kim P, Warnecke G, Haverich A. Low-potassium dex-tran solution ameliorates perfusion injury of the lung and protects surfactant function. J Thorac Cardiovasc Surg 2000; 120: 566–572.
11 Suda T, Mora BN, Cooper JA et al. In vivo adenoviral-mediated endothelial nitric oxidesynthase gene transfer ameliorates lung allograft ischemia reperfusion injury. J ThoracCardiovasc Surg 2000; 119: 297–304.
12 Fujino S, Nagahiro I, Yamashita M et al. Preharvest nitroprusside flush improves post-transplant lung function. Ann Thor Surg 1997; 63: 1383–1390.
13 Cooper JD, Patterson GA, Trulock EP. Results of single and bilateral transplantation in 131consecutive recipients. J Thorac Cardiovasc Surg 1994; 107: 460–471.
14 Waters PF. Lung transplant: postoperative management. In: Patterson GA, Courand L,eds. Current Topics in General Thoracic Surgery: an International Series, Vol. 3, LungTransplant. Amsterdam: Elsevier, 1995; 260–261.
15 Weill D, Zamora MR. Postoperative care in lung transplantation. Semin Resp Crit Care Med1996; 159–166.
16 Cooper JD, Billingham M, Egan TA. Working formulation for the standardiztion ofnomenclature and for clinical staging of chronic dysfunction in lung allografts. J HeartLung Transplant 1993; 12: 713–716.
17 Novick RJ, Andreassian B, Schafers H-J et al. Pulmonary retransplantation for obliterativebronchiolitis. J Thorac Cardiovasc Surg 1994; 107: 755–763.
18 Novick RJ, Stitt LW, Alkattan K et al. Pulmonary retransplantation: predictors of graftfunction and survival in 230 patients. Ann Thorac Surg 1998; 65: 227–234.

CHAPTER 8
Pleural space problems
Sudish Murthy, Thomas W Rice
Introduction
The pleura is a thin serous membrane that covers the lung and chest wall. It isdivided into two anatomic layers, a visceral layer, which envelops the pul-monary parenchyma and includes interlobar fissures, and a parietal layer,which covers the ribs, diaphragm and mediastinum. The pleura also consistsof two cellular layers: a mesothelial cell monolayer facing the pleural spaceand an underlying connective tissue matrix. The virtual cavity between vis-ceral and parietal pleura is referred to as the pleural space. Under normal cir-cumstances, the pleural surfaces are tightly coapted secondary to the negativepressure in the pleural space and the cavity contains only a small amount of fluid [1]. The pleura functions to mechanically couple the lung and chestwall, facilitating respiration [2]. Consequently, patients with disease processesaffecting the pleura can present with exertional dyspnea and respiratory compromise. The most common pathological processes affecting the pleurainclude inflammatory disease, infection, trauma, and neoplasm.
Diagnosis
Even though a complete physical examination and thorough medical historyoften suggest the nature of the disease, radiographic imaging is an importantadjunct in the initial evaluation of patients with suspected pleural disease [3].Conventional erect chest radiographs can demonstrate pneumothorax (Figure8.1a), pleural-based fluid collections (Figure 8.1b), and pleural thickening(Figure 8.1c). The high-resolution axial imaging provided by chest computedtomography (CT) scans allows for detailed assessment of pleural-based dis-ease (Figure 8.2) and is recommended for all patients with complex pleuralspace problems. Ultrasonography has a role in guiding percutaneous dia-gnostic maneuvers. Magnetic resonance imaging (MRI) is of use in the characterization of malignant mesothelioma to define resectability [4].
Blood tests are rarely useful in the diagnostic work-up of pleural disease.However, in the context of pleural-based pathology identified radiographic-ally, an elevated leukocyte count or positive blood culture suggest pleuralspace infection. Hypoglycemia alerts the clinician to the possibility of a solitaryfibrous tumor of the pleura.
135
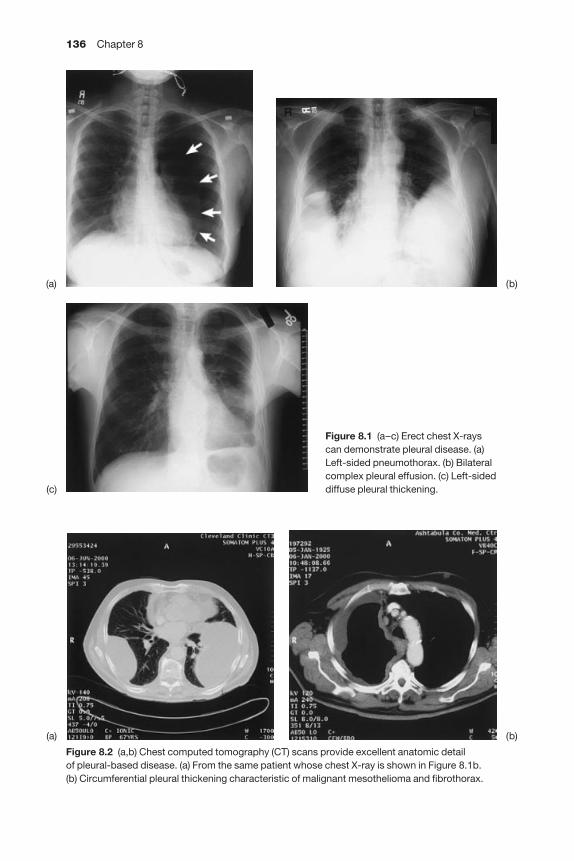
136 Chapter 8
Figure 8.1 (a–c) Erect chest X-rayscan demonstrate pleural disease. (a)Left-sided pneumothorax. (b) Bilateralcomplex pleural effusion. (c) Left-sideddiffuse pleural thickening.
(a) (b)
(c)
Figure 8.2 (a,b) Chest computed tomography (CT) scans provide excellent anatomic detail of pleural-based disease. (a) From the same patient whose chest X-ray is shown in Figure 8.1b. (b) Circumferential pleural thickening characteristic of malignant mesothelioma and fibrothorax.
(a) (b)
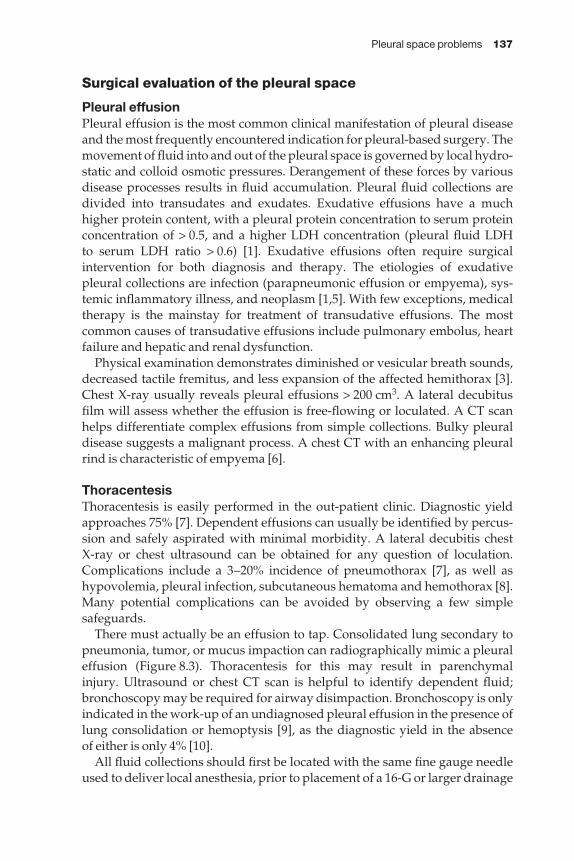
Pleural space problems 137
Surgical evaluation of the pleural space
Pleural effusionPleural effusion is the most common clinical manifestation of pleural diseaseand the most frequently encountered indication for pleural-based surgery. Themovement of fluid into and out of the pleural space is governed by local hydro-static and colloid osmotic pressures. Derangement of these forces by variousdisease processes results in fluid accumulation. Pleural fluid collections aredivided into transudates and exudates. Exudative effusions have a muchhigher protein content, with a pleural protein concentration to serum proteinconcentration of > 0.5, and a higher LDH concentration (pleural fluid LDH to serum LDH ratio > 0.6) [1]. Exudative effusions often require surgical intervention for both diagnosis and therapy. The etiologies of exudative pleural collections are infection (parapneumonic effusion or empyema), sys-temic inflammatory illness, and neoplasm [1,5]. With few exceptions, medicaltherapy is the mainstay for treatment of transudative effusions. The most common causes of transudative effusions include pulmonary embolus, heartfailure and hepatic and renal dysfunction.
Physical examination demonstrates diminished or vesicular breath sounds,decreased tactile fremitus, and less expansion of the affected hemithorax [3].Chest X-ray usually reveals pleural effusions > 200 cm3. A lateral decubitusfilm will assess whether the effusion is free-flowing or loculated. A CT scanhelps differentiate complex effusions from simple collections. Bulky pleuraldisease suggests a malignant process. A chest CT with an enhancing pleuralrind is characteristic of empyema [6].
ThoracentesisThoracentesis is easily performed in the out-patient clinic. Diagnostic yieldapproaches 75% [7]. Dependent effusions can usually be identified by percus-sion and safely aspirated with minimal morbidity. A lateral decubitis chest X-ray or chest ultrasound can be obtained for any question of loculation.Complications include a 3–20% incidence of pneumothorax [7], as well ashypovolemia, pleural infection, subcutaneous hematoma and hemothorax [8].Many potential complications can be avoided by observing a few simple safeguards.
There must actually be an effusion to tap. Consolidated lung secondary topneumonia, tumor, or mucus impaction can radiographically mimic a pleuraleffusion (Figure 8.3). Thoracentesis for this may result in parenchymal injury. Ultrasound or chest CT scan is helpful to identify dependent fluid;bronchoscopy may be required for airway disimpaction. Bronchoscopy is onlyindicated in the work-up of an undiagnosed pleural effusion in the presence oflung consolidation or hemoptysis [9], as the diagnostic yield in the absence of either is only 4% [10].
All fluid collections should first be located with the same fine gauge needleused to deliver local anesthesia, prior to placement of a 16-G or larger drainage
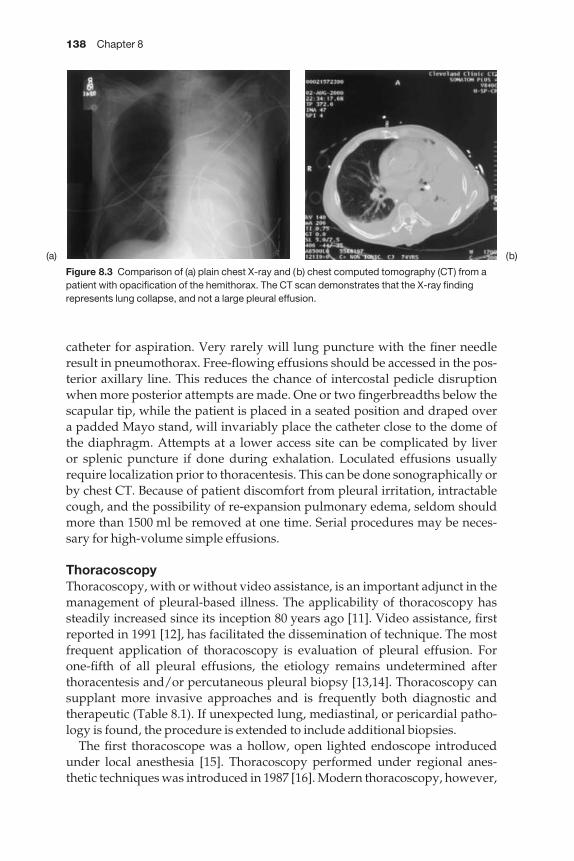
138 Chapter 8
catheter for aspiration. Very rarely will lung puncture with the finer needleresult in pneumothorax. Free-flowing effusions should be accessed in the pos-terior axillary line. This reduces the chance of intercostal pedicle disruptionwhen more posterior attempts are made. One or two fingerbreadths below thescapular tip, while the patient is placed in a seated position and draped over a padded Mayo stand, will invariably place the catheter close to the dome ofthe diaphragm. Attempts at a lower access site can be complicated by liver or splenic puncture if done during exhalation. Loculated effusions usuallyrequire localization prior to thoracentesis. This can be done sonographically orby chest CT. Because of patient discomfort from pleural irritation, intractablecough, and the possibility of re-expansion pulmonary edema, seldom shouldmore than 1500 ml be removed at one time. Serial procedures may be neces-sary for high-volume simple effusions.
ThoracoscopyThoracoscopy, with or without video assistance, is an important adjunct in themanagement of pleural-based illness. The applicability of thoracoscopy hassteadily increased since its inception 80 years ago [11]. Video assistance, firstreported in 1991 [12], has facilitated the dissemination of technique. The mostfrequent application of thoracoscopy is evaluation of pleural effusion. For one-fifth of all pleural effusions, the etiology remains undetermined after thoracentesis and/or percutaneous pleural biopsy [13,14]. Thoracoscopy cansupplant more invasive approaches and is frequently both diagnostic andtherapeutic (Table 8.1). If unexpected lung, mediastinal, or pericardial patho-logy is found, the procedure is extended to include additional biopsies.
The first thoracoscope was a hollow, open lighted endoscope introducedunder local anesthesia [15]. Thoracoscopy performed under regional anes-thetic techniques was introduced in 1987 [16]. Modern thoracoscopy, however,
Figure 8.3 Comparison of (a) plain chest X-ray and (b) chest computed tomography (CT) from apatient with opacification of the hemithorax. The CT scan demonstrates that the X-ray findingrepresents lung collapse, and not a large pleural effusion.
(a) (b)
Pleural space problems 139
is conducted under general anesthesia and facilitated by lung isolation. Basedon the complexity of the pleural disease, one of two surgical approaches isemployed.
Single-port thoracoscopySingle-port thoracoscopy is a simple thoracic surgical technique. The differ-ences between single-port thoracoscopy and thoracentesis are summarized inTable 8.2. For the former, a single incision (2 cm) is made in the mid or anterioraxillary line of interspace 6 or 7 (Figure 8.4). Preoperative marking (ultrasoundor CT) may be required for management of complex, loculated effusions. Ifpossible, the ipsilateral lung is deflated. The pleural space is entered judici-ously to prevent parenchymal, pericardial, or diaphragmatic injury. A medi-astinoscope is then gently inserted through the interspace. The pleural space isevaluated under direct vision (a videoscope or a rigid optical forceps may beinserted through the thoracoscope if necessary). When bulky pleural disease is encountered (e.g. mesothelioma), the leading edge of the Wolf scope can beused to dissect the pleura from the endothoracic fascia to allow for a greatervolume of tissue to be removed for diagnosis.
Table 8.1 Common indications for thoracoscopy in the diagnosis andtreatment of pleural disease.
Indication Goal of procedure
Pleural effusion of unclear etiology Diagnostic/therapeuticSuspicious pleural mass Diagnostic/therapeuticPleurectomy for spontaneous pneumothorax TherapeuticDrainage/decortication of empyema Diagnostic/therapeuticHemothorax Diagnostic/therapeuticChylothorax Diagnostic/therapeutic
Table 8.2 Differences between single-port thoracoscopy and percutaneous drainage in themanagement of pulmonary effusion of unclear etiology.
Factor Single-port thoracoscopy Percutaneous drainage
Cost > $4000* < $500†Diagnostic accuracy > 90% < 80%Hospital stay required Yes NoEvaluation of pleura Visual inspection of pleura Primarily cytological
Site-directed tissue biopsiesGoal of procedure Diagnostic and therapeutic DiagnosticMost frequent complication Pain Pneumothorax
*Estimate of Medicare reimbursement and co-payment for current procedural technology (CPT)32650.†Estimate of Medicare reimbursement and co-payment for CPT 32000.
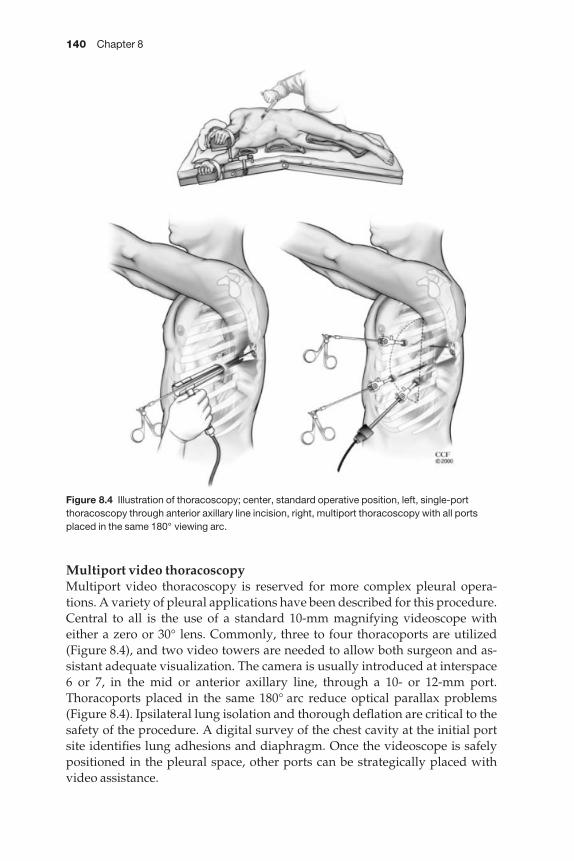
140 Chapter 8
Multiport video thoracoscopyMultiport video thoracoscopy is reserved for more complex pleural opera-tions. A variety of pleural applications have been described for this procedure.Central to all is the use of a standard 10-mm magnifying videoscope witheither a zero or 30° lens. Commonly, three to four thoracoports are utilized(Figure 8.4), and two video towers are needed to allow both surgeon and as-sistant adequate visualization. The camera is usually introduced at interspace 6 or 7, in the mid or anterior axillary line, through a 10- or 12-mm port.Thoracoports placed in the same 180° arc reduce optical parallax problems(Figure 8.4). Ipsilateral lung isolation and thorough deflation are critical to thesafety of the procedure. A digital survey of the chest cavity at the initial portsite identifies lung adhesions and diaphragm. Once the videoscope is safelypositioned in the pleural space, other ports can be strategically placed withvideo assistance.
Figure 8.4 Illustration of thoracoscopy; center, standard operative position, left, single-portthoracoscopy through anterior axillary line incision, right, multiport thoracoscopy with all portsplaced in the same 180° viewing arc.
Pleural space problems 141
Appreciation of the complications associated with thoracoscopy facilitatesthe safe performance of the procedure [15,17–20]. Avoidable complicationsinclude improper patient selection, unfamiliarity with the technique, inade-quate equipment, aberrant anatomy, and impatience.
Complications are classified as local or regional. Local complicationsinclude hematoma, superficial infection, rib fracture, neuralgia, and tumorseeding. Standard sterile surgical techniques and gentle handling of chest wall tissues reduce local complications. An interspace large enough to allowpassage of the scope or video port reduces soft tissue and rib trauma anddecreases postoperative pain syndromes. The operating table may be slightlyflexed and the patient buoyed off the table with pillows or a rigid beanbagplaced under the contralateral flank (Figure 8.4). Intercostal spaces are wideranteriorly and, unless the pathology mandates a posterior approach, anteriorinterspaces should be reserved for large trocar or scope placement. The latis-simus dorsi may be avoided by a more anterior port placement. The surgeonmust also be mindful of excessive torque applied on the ribs at the access site.In this setting, creation of a second port, with a more favorable viewing angle,may decrease neuralgia and reduce postoperative pain. Smaller operatingvideoscopes (5 mm vs. 10 mm) result in smaller and less painful incisions.Wound infection rates, though poorly documented in most reviews, should be< 3%. In addition to tissue trauma and hematoma, it is possible that soilage ofthe incision with talc during pleurodesis (for a malignant effusion) increasesthe risk of port site infection. We thoroughly irrigate the port site prior to clos-ure and occasionally tunnel the chest tube through a separate stab incision ifthe port site appears macerated.
Tumor seeding of the thoracoscopy tract presents a more formidable challenge. Port site recurrence rates as high as 4% have been observed withmesothelioma [18,21], although this problem has seldom been encountered in cases of metastatic cancers to the pleura [15]. Resection of the biopsy tract isrecommended if extra-pleura pneumonectomy is performed. Some surgeonsadvocate prophylactic radiotherapy (20 Gy) to each port following thoraco-scopy for malignant mesothelioma [18].
There are also regional and systemic complications of thoracoscopy. Hem-othorax and empyema complicate 1% of procedures [19]. Though consideredto be a risk for empyema, thoracoscopy with talc poudrage has been used totreat recalcitrant pleural space infections [22]. Prolonged air leak and subcuta-neous emphysema (2% incidence of each) are secondary to direct pulmonaryparenchymal injury. This often occurs during port placement when adherentlung is present at the entry site. Careful review of the preoperative CT scan isessential. Incomplete decortication done thoracoscopically may injure lung,while not allowing proper lung re-expansion and chest wall apposition to promote parenchymal healing. If any concerns regarding lung entrapment or incomplete expansion remain after a thoracoscopic decortication, a utilityincision should be made and the decortication finished. Esophageal, phrenicand recurrent nerve, diaphragmatic and cardiac injuries have been reported,
142 Chapter 8
and are attributable to the difficulty of appreciating anatomic boundaries in anoperative field shrouded with blood, pus, or tumor. If any question of safetyarises, it is advisable to convert to an open procedure.
Multiport thoracoscopy with video assistance has four times the complica-tion rate of conventional single-port thoracoscopy [17]. Most of the increasedrisk is secondary to the more complex nature of most video-assisted pro-cedures. The surgeon must remember, however, that in direct single-port thoracoscopy, there is no optical dissociation between the operator and operative field to confuse matters. Lung isolation, mandatory for video thora-coscopy, is often accompanied by extreme changes in arterial blood gas values[23]. The decision to employ multiport video thoracoscopy vs. single portdirect thoracoscopy must be tailored to the goals of the procedure, the fitnessof the patient, and skill of the operator.
Thoracoscopy for the malignant pleural effusion
Single-port thoracoscopy is ideally suited to management of malignant pleuraleffusion. Cost of the procedure is significantly greater than thoracentesis(Table 8.2); however, as a diagnostic and therapeutic intervention, it has no percutaneous equal. Talc poudrage through the thoracoscope is > 90%effective in controlling malignant effusions and appears to be 30–50% moreefficacious than either tetracycline or bleomycin instilled at the bedside [24,25].Over 50% of patients are febrile after talc pleurodesis [25]. Re-expansion pulmonary edema, acute respiratory distress syndrome, granulomatous pneu-monitis, and cerebral microembolism have been reported as rare complica-tions of talc insufflation [24,25]. We routinely instill 5 g of talc and often stagebilateral procedures to prevent such occurrences. If dense lung entrapment is noted at thoracoscopy, no attempt at talc insufflation is made, since lungexpansion is a prerequisite for successful pleurodesis. This situation should be anticipated if a preoperative thoracentesis (> 1000 ml) results in minimalimprovement in the patient’s respiratory status or if post-thoracentesis X-raydemonstrates incomplete lung expansion.
Thoracoscopy for empyema
Early empyema can also be treated thoracoscopically. The algorithm of man-aging patients with suspected empyema usually begins with tube thoraco-stomy. An exudative effusion with a pH < 7.3, low glucose concentration, andpreponderance of neutrophils is consistent with empyema. If evacuation of thepleural space is complete and the lung expands to fill the cavity, no furtherprocedures are necessary. The chest tube may be converted to open drainagewithin a week. If, however, the effusion is incompletely drained or loculated,or if the lung is entrapped, additional therapy is required. Fibrinolytic therapyhas been tried, but no randomized data support its efficacy and spontaneoushemothorax is an occasional complication of chemical fibrinolysis.
Pleural space problems 143
Single-port or multiport thoracoscopy is an excellent option in this situation,and may prevent thoracotomy [26]. An early empyema can frequently bedrained and the lung decorticated from its gelatinous peel through the thora-coscope. Large-bore chest tubes are then precisely placed under direct visionfor optimum drainage in the postoperative period.
If a more mature and complicated pleural space infection is found, videoassistance facilitates complete drainage. In addition to the video port, two or three operating ports are placed under video guidance. Sharp dissection isfrequently necessary to start the decortication, facilitated by endoscopic mono-polar scissors. Thoracoscopic ring forceps and 5-mm gauze-tipped dissectorscan then be used to develop the decortication plane. It is essential that the pleu-ral space be completely visualized and the entire lung mobilized to prevent aresidual undrained collection. The lung must completely fill the hemithorax atthe conclusion of the procedure. Preoperative bronchoscopic toilet decreasesthe likelihood that muco-purulent impaction will cause poor pulmonary re-expansion after the decortication. A 20% conversion rate to thoracotomy hasbeen reported [26].
It is not uncommon for patients to be septic after the operation. This is pre-sumably attributable to cytotoxins liberated from the pleural space duringsurgery. Supportive care includes broad-spectrum antibiotics, early enteralnutrition, mechanical ventilation, and vasoactive medications. Postoperativefevers are most commonly associated with the septic syndrome, atelectasis,lower extremity venous thrombosis, or recurrent pneumonia. A chest CT scanmay be needed to exclude an incompletely drained empyema. If a postoper-ative fluid collection is identified on the CT scan, percutaneous drainage isappropriate. Rarely should a repeat decortication be necessary if the initialprocedure was done properly.
Thoracoscopy for hemothorax
Though many of the same thoracoscopy principles apply in the operative management of hemothorax, a few additional guidelines should be followed.Thoracoscopic management of hemothorax should be considered only afterlarge-bore chest tubes have failed adequately to drain the chest. Any acutely developing hemothorax with hemodynamic compromise mandatesthoracotomy/sternotomy for control. Any coagulopathy must be correctedpreoperatively.
As with the management of empyema, drainage via single-port thoraco-scopy is often sufficient. Single-port thoracoscopy is perhaps most useful toevacuate clot after an open heart procedure in which the hemithorax has beenan innocent reservoir for mediastinal blood. In these instances, existing chesttubes may have become dysfunctional because of clot and they contaminatethe space. Early thoracoscopic drainage reduces the incidence of empyemaand fibrothorax. If an ongoing blood loss is suspected, this technique is likelyto be inadequate. At a minimum, video assistance would be required to survey
144 Chapter 8
the chest cavity in an attempt to identify and control the bleeding source.Finally, in a post-traumatic hemothorax, all efforts should be made to avoidplacing a port adjacent to a rib fracture as the injury may be worsened by scopetrauma. In the absence of an obvious bleeding source, intercostal pedicle ligation at the sites of fractures should be considered to prophylax against a rebleed postoperatively. The lung may need to be decorticated if the hemo-thorax is subacute.
Thoracotomy for pleural disease
With the advent of efficacious antituberculous therapy, a debilitating andpainful thoracoplasty is seldom necessary. On the rare occasion that the pleu-ral space needs to be reduced or collapsed, soft tissue transfer (e.g. rotationalmuscle flaps, omentum, etc.) is more effective, less painful and debilitating,and cosmetically more appealing. Thoracotomy for pleural disease is neces-sary for dense fibrothorax, mature empyema, and the primary neoplasm of thepleura, mesothelioma.
Thoracotomy for fibrothorax and mature empyema
Fibrothorax and mature empyema are two common indications for thoraco-tomy. The procedure of choice for both conditions is pleurectomy/decortica-tion. Since these are benign conditions, the durability of the surgery must be substantially longer than for malignant mesothelioma. Though many of thetechnical nuances are the same, a few points are worth noting.
Fibrothorax is most often a sequela of an incompletely drained hemothorax.Medications have rarely been implicated in the genesis of the disease. An idiopathic variant, akin to mediastinal or retroperitoneal fibrosis, also exists[27]. The differential diagnosis includes desmoplastic malignant mesothe-lioma. Since reversible acute pleural inflammation may accompany a varietyof conditions, surgery should be considered only if pleural disease persists for several weeks or months. Furthermore, the disease must be responsible for significant disability, and the patient must be a reasonable surgical candidate.
Fibrothorax predominates in the lower chest. Frequently, the diaphragm is entrapped in the process. Parietal pleurectomy is as important as the de-cortication, since chest wall and diaphragmatic compliance are restored withthe pleurectomy. When considering a patient for surgery, recognizing existingpulmonary hypertension alerts the surgeon to the risk of significant intra-operative blood loss.
Mature or chronic empyema is an insidious disease that manifests with constitutional, rather than local, symptoms. Recent history of respiratory tractinfection (2–6 months prior), low-grade fevers, night sweats, and fatigue characterize the disease. If accompanied by pleuritic chest pain and a complexfluid collection is found on chest X-ray, empyema becomes the most likely
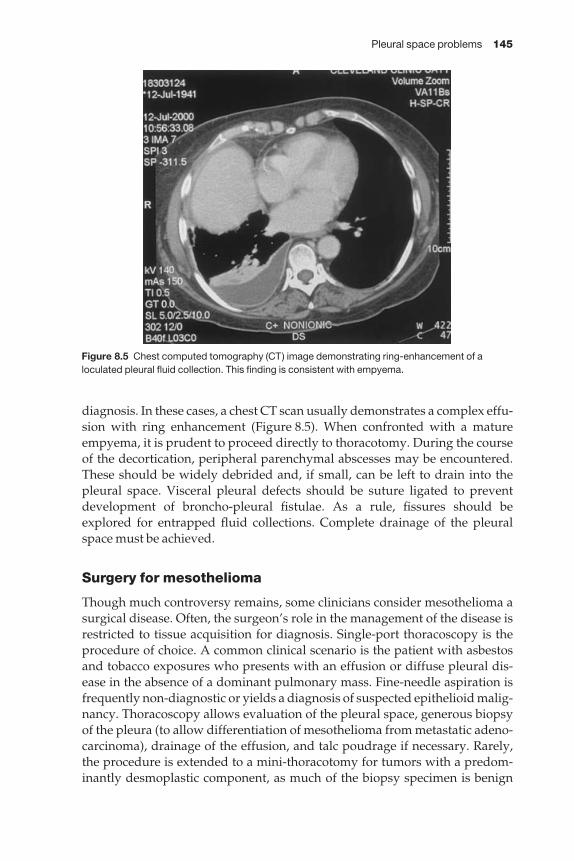
Pleural space problems 145
diagnosis. In these cases, a chest CT scan usually demonstrates a complex effu-sion with ring enhancement (Figure 8.5). When confronted with a matureempyema, it is prudent to proceed directly to thoracotomy. During the courseof the decortication, peripheral parenchymal abscesses may be encountered.These should be widely debrided and, if small, can be left to drain into thepleural space. Visceral pleural defects should be suture ligated to preventdevelopment of broncho-pleural fistulae. As a rule, fissures should beexplored for entrapped fluid collections. Complete drainage of the pleuralspace must be achieved.
Surgery for mesothelioma
Though much controversy remains, some clinicians consider mesothelioma asurgical disease. Often, the surgeon’s role in the management of the disease isrestricted to tissue acquisition for diagnosis. Single-port thoracoscopy is theprocedure of choice. A common clinical scenario is the patient with asbestosand tobacco exposures who presents with an effusion or diffuse pleural dis-ease in the absence of a dominant pulmonary mass. Fine-needle aspiration isfrequently non-diagnostic or yields a diagnosis of suspected epithelioid malig-nancy. Thoracoscopy allows evaluation of the pleural space, generous biopsyof the pleura (to allow differentiation of mesothelioma from metastatic adeno-carcinoma), drainage of the effusion, and talc poudrage if necessary. Rarely,the procedure is extended to a mini-thoracotomy for tumors with a predom-inantly desmoplastic component, as much of the biopsy specimen is benign
Figure 8.5 Chest computed tomography (CT) image demonstrating ring-enhancement of aloculated pleural fluid collection. This finding is consistent with empyema.

146 Chapter 8
fibrous tissue. In these cases, it is critical that a diagnosis be made on frozensection prior to concluding the procedure.
Benign localized mesotheliomaThe prognosis for benign localized mesothelioma (pleural fibroma, solitaryfibrous tumor of the pleura, fibrous mesothelioma) is favorable. Surgical therapy is generally straightforward. Preoperative chest CT scan usuallydemonstrates a well-circumscribed pleural-based mass with some degree ofpulmonary collapse. The differential includes primary lung cancer, solitarypleural metastasis, primary sarcoma of the chest wall, bronchogenic cyst, neurogenic tumor, rounded atelectasis/pneumonia, loculated empyema, and diaphragmatic hernia. This tumor has no documented link to asbestosexposure. If the pleura appears diffusely involved, a malignant process is most likely. Curiously, unique extrathoracic manifestations (pulmonaryosteoarthropathy, fever, hypoglycemia) are found in one-third of patients[3,28]. Unless resection is incomplete, surgery is curative. Surgical therapyincludes en bloc resection of the pleural-based mass, which usually arises fromthe visceral pleura. Resection should include a small wedge of lung to insurethat all involved visceral pleura is resected. If mediastinal or parietal pleura is the point of origin, generous margins of normal pleura should be included in the resection specimen. Bronchoscopy prior to extubation may be necessaryto alleviate mucous impaction from chronically compressed lung, dependingon the size of the tumor.
Malignant pleural mesotheliomaMalignant pleural mesothelioma a rare malignancy, arises from the mesothe-lium that lines the pleural cavities. Usually found in patients with a history of asbestos exposure, the time from exposure to its clinical presentation is > 20 years. The disease manifests as progressive dyspnea or chest pain; malig-nant effusion develops in most patients. Advanced disease can present withcachexia, ascites and/or chest wall deformitiy [29]. Microscopically, thesetumors exhibit epithelioid, sarcomatoid, or mixed differentiation patterns. Of the three, the more common epithelioid variants have the best prognosis;the least common, pure sarcomatoid tumors, have the poorest survival.Median survival of untreated malignant mesothelioma is approximately 1 year [30–33].
Three different surgical approaches should be considered for malignantmesothelioma: talc pleurodesis, pleurectomy/decortication, and extrapleuralpneumonectomy. Choice of treatment plan depends on the fitness of thepatient, histology type, stage of disease, and access to skilled radiation andmedical oncologists. Contraindications for aggressive therapy because of the increased risk of postoperative complications are age > 70 years, com-promised cardiac function (ejection fraction < 45% or ischemia), pulmonaryhypertension, hypercarbia (PCO2 < 45 mmHg), hypoxemia (PO2 < 65 mmHg),or a postresection predicted forced expiratory volume in 1 s < 1 l [29]. N2 or

Pleural space problems 147
T3–4 disease and mixed or sarcomatoid histology should relegate the patient to drainage and pleurodesis if a symptomatic effusion exists.
Pleurectomy/decortication for mesothelioma
Indications for pleurectomy/decortication in the management of malignantpleural mesothelioma are shrinking, as trimodality therapy with extrapleuralpneumonectomy gains acceptance for appropriate candidates. Initial optim-ism to incorporate pleurectomy/decortication into multimodality protocolsfor mesothelioma has subsided, after recent trials revealed a 60% local failurerate [34,35]. Yet, in an otherwise fit patient considered unsuitable for extra-pleural pneumonectomy, pleurectomy/decortication remains a reasonableoption for severe lung entrapment.
Incision is usually made through the 5th interspace. Though seldom neces-sary, resection of part of the 6th rib can be used to facilitate entrance into theendothoracic fascial plane. The parietal pleural is bluntly separated from thefascia and points of dense adherence usually connote reactive desmoplasia or periosteal and rib involvement. Cautery or sharp dissection can be used todisconnect the pleura in these regions. Intraoperative blood loss can be min-imized by serially packing the chest with laparotomy pads as the parietalpleura is mobilized from various regions. Gradually, the parietal pleura is sep-arated from the anterior, lateral and posterior chest wall. If intercostal pediclesare avulsed during the dissection, the plane is too deep. Sharp dissection isnecessary to regain the proper plane. Difficulty is most frequently encounteredin the apex, medially, and inferiorly. At the apex of the hemithorax, great care must be taken when detaching the pleura from the subclavian vessels.Antero-medially, careful dissection to avoid internal mammary artery injury isimportant as this is difficult to control if injured. Postero-medially, esophageal(right-side) or aortic (left-side) perforation is catastrophic. An injury to thephrenic pedicle anywhere along its course may negate the benefit of the pro-cedure, as will diaphragmatic evulsion. A small amount of gross tumor left in these regions may be warranted to prevent an intraoperative calamity orpostoperative disability. Some surgeons utilize ‘bunk-bed’ thoracotomies (asecond intercostal entry at the 7th interspace) to simplify the dissection on thediaphragm.
After the parietal pleura has been sufficiently mobilized, the tumor is incisedsharply at a convenient location and the visceral pleura decorticated. Rawparenchyma can be exposed when visceral pleura is peeled away along withthe tumor. As long as the lung injury remains superficial, this is of little concern. Bleeding from both parenchymal and chest wall sources is easily con-trolled with direct pressure, electrocautery, or argon beam coagulation. Caremust be taken when decorticating the fissures as they can be inadvertently followed into the distal pulmonary artery. After the tumor peel is removed, the air leak may be imposing; however, as long as the lung inflates to fill thehemithorax, resolution of the air leak is surprisingly quick. Large parenchymal
148 Chapter 8
rents should be plicated to reduce healing time and shorten hospital stay. Twoto three large-bore chest tubes are usually necessary to keep the hemithoraxdrained during the early recovery period. A preoperative epidural catheter isimportant for early ambulation and pulmonary toilet. Most patients are keptintubated and ventilated on the first postoperative night to promote lungexpansion. If the air leak is manageable, chest tubes are placed on high suctionto evacuate fluid from the pleural space. Positive end-expiratory pressure canbe applied to tamponade parenchymal and chest wall bleeding. Currently, wedo not advocate the routine use of adjuvant radiotherapy following pleurec-tomy/decortication. The amount of radiation that can be administered to thehemithorax is limited by the radiation intolerance of normal lung and, evenwhen the radiation planning has been meticulous, significant radiation pneu-monitis results [34]. Regardless, most patients recur within 1 year. Currently,no salvage therapy exists for recurrence.
Extrapleural pneumonectomy for mesothelioma
The technical challenge of this resection is matched equally by the diligenceand experience required to recover patients postoperatively. In 1976, the initialoperative mortality was reported at 30% [36]; today, a 30-day mortality of > 5% would be considered excessive [37]. This procedure is not restricted tomesothelioma. Pleural sarcoma and advanced, refractory tuberculous diseasemay also require extrapleural pneumonectomy as therapy. Comprehensivereviews of clinical indications [38] and technique of extrapleural pneumonec-tomy [29] have been written.
Since malignant mesothelioma is a locally aggressive disease, in theory themore complete the resection, the better the outcome should be expected. This may explain the markedly lower local recurrence rate after resection com-pared with pleurectomy/decortication [39]. Local control can be enhanced by aggressive adjuvant radiotherapy to the empty hemithorax. Patients who benefit most from resection have early-stage, node-negative, epithelioidtumors [38,40]. Extrapleural pneumonectomy for mesothelioma should bereserved for patients enrolled in a trimodality protocol.
Extrapleural pneumonectomy entails resection of the pleural envelope withlung, diaphragm, pericardium and a complete lymphadenectomy. Difficultiesencountered during the resection are identified in Figure 8.6. Resection of all gross disease is the goal, as benefit from the procedure has only beendemonstrated with negative resection margins [40]. Involvement of the ribs,mediastinum, esophagus, aorta, or subclavian vessels contraindicates re-section. This should be investigated preoperatively by MRI scanning [4]. If trans-pericardial or trans-diaphragmatic spread is found, the resectionshould be aborted. Limiting the number of intraoperative surprises facilitates asafe and beneficial outcome.
As with pleurectomy, much of the dissection is done bluntly. Hemostasis isobtained by direct pressure. If the proper extrapleural plane is developed, the

Pleural space problems 149
dissection proceeds smoothly. In the case of a frozen hemithorax, the 6th ribmay be sacrificed to allow access to the endothoracic fascial plane, although ribresection makes chest closure significantly more difficult. Using a sponge-stickand sharp dissection, it should be possible to mobilize the superior sulcus,leaving subclavian vessels, stellate ganglia, esophagus and vagus nerve intact.A nasogastric tube permits intraoperative identification of the esophagus. In very early-stage disease, with low tumor burden, dissection is frequentlymore tedious; the pleura is not thickened and the plane is difficult to develop.In these cases, islands of normal-appearing, thin, parietal pleura often separatefrom the specimen and remain attached to the chest wall. A piecemealapproach must be adopted to finish the resection.
Diaphragmatic and pericardial resections are undertaken only after it is cer-tain that the resection can be completed. The diaphragm is mobilized bluntly,beginning from the costovertebral sulcus. Much of this dissection is doneblindly, with fingers being interdigitated between slips of diaphragm muscle(a ‘bunk-bed’ thoracotomy may simplify this aspect). This sulcus is a difficultarea to visualize and a common site for gross disease to be left behind. It istherefore typical to spend more time during this part of the resection than formobilization of the rest of the pleura. Once the diaphragm has been partiallydisconnected, the specimen can be rolled into view, the lateral aspect of the diaphragm incised with cautery and bluntly separated from underlyingperitoneum.
As the diaphragm is resected, the peritoneum is frequently adherent to the underside of the central tendon and commonly avulsed. Any defects areoversewn to reduce the chance of ascites developing as the ipsilateral chest fills
Figure 8.6 Depending upon the side of the malignant mesothelioma, several anatomic structuresmust be protected during extrapleural pneumonectomy. (a) Subclavian vessels. (b) Esophagus. (c) Aazygous vein. (d) Vagus nerve. (e) Left recurrent nerve. (f ) Aorta. (g) IVC. Injury to any of thesestructures will result in intraoperative difficulty and postoperative morbidity.
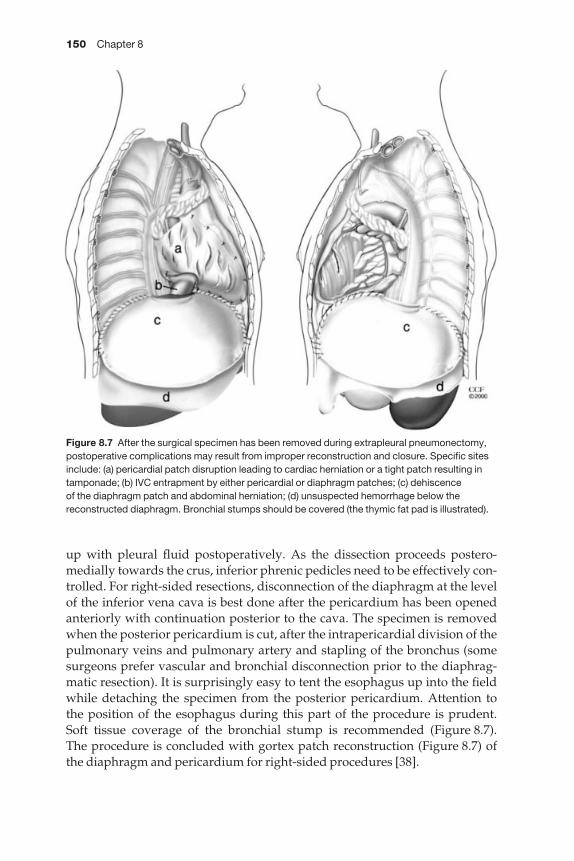
150 Chapter 8
up with pleural fluid postoperatively. As the dissection proceeds postero-medially towards the crus, inferior phrenic pedicles need to be effectively con-trolled. For right-sided resections, disconnection of the diaphragm at the levelof the inferior vena cava is best done after the pericardium has been openedanteriorly with continuation posterior to the cava. The specimen is removedwhen the posterior pericardium is cut, after the intrapericardial division of thepulmonary veins and pulmonary artery and stapling of the bronchus (somesurgeons prefer vascular and bronchial disconnection prior to the diaphrag-matic resection). It is surprisingly easy to tent the esophagus up into the fieldwhile detaching the specimen from the posterior pericardium. Attention to the position of the esophagus during this part of the procedure is prudent. Soft tissue coverage of the bronchial stump is recommended (Figure 8.7). The procedure is concluded with gortex patch reconstruction (Figure 8.7) ofthe diaphragm and pericardium for right-sided procedures [38].
Figure 8.7 After the surgical specimen has been removed during extrapleural pneumonectomy,postoperative complications may result from improper reconstruction and closure. Specific sitesinclude: (a) pericardial patch disruption leading to cardiac herniation or a tight patch resulting intamponade; (b) IVC entrapment by either pericardial or diaphragm patches; (c) dehiscence of the diaphragm patch and abdominal herniation; (d) unsuspected hemorrhage below thereconstructed diaphragm. Bronchial stumps should be covered (the thymic fat pad is illustrated).
Pleural space problems 151
In a procedure of this magnitude, even small technical complications can becatastrophic. Table 8.3 summarizes complications observed after extrapleuralpneumonectomy. Cognizance of the technical subtleties of the procedure promotes a more uneventful postoperative course.
During the recovery period, pulmonary edema, mediastinal shift, atrialarrhythmia, vocal cord palsy, and pain all contribute to respiratory insuffici-ency. In addition to effective pain management and early ambulation, aggress-ive diuresis, balancing of the mediastinum and vocal cord injection (to restorea functional cough) may be necessary. Most diaphragmatic patch problemsmanifest within the first week, if not the first day, and mandate an immediatereturn to the operating room. A postoperative chest X-ray demonstrates a left-sided diaphragm patch dehiscence as the gastric air bubble (and other abdom-inal organs) ascend into the left chest. A right-sided diaphragm patchdisruption may be more insidious. The liver is still partially fixed to the peri-toneal cavity laterally and posteriorly after resection, and may not swiftly fillthe cavity if the reconstruction fails. If the liver does herniate into the rightchest, the chest X-ray may not change appreciably. Often, an ultrasound orchest CT is required to diagnose the problem. Dehiscence of the right-sidedpericardial patch usually results in ventricular tachycardia followed promptlyby fibrillatory arrest. When the heart herniates into the pneumonectomy space,venous return is severely compromised as both inferior and superior venacavae become occluded. If this happens, the patient should be immediately
Table 8.3 Observed postoperative complications following extrapleural pneumonectomy.
Complication Possible cause
HypotensionFalling HCT Bleeding ± coagulopathyStable HCT Epidural analgesia ± ipsilateral sympathetic chain injury
Hypovolemia secondary to early fill-upMyocardial ischemiaAtrial arrhythmiaRight-sided Gortex patch compressing IVCSepsis from occult esophageal injury
Hoarseness/weak cough Left recurrent nerve injuryRespiratory insufficiency Post-pneumonectomy pulmonary edema
Mediastinal shift from rapid fill-upAspiration
Ventricular arrhythmia Myocardial ischemiaPericardial/diaphragm patch disruption and cardiac malrotation or entrapment
Dysphagia Submucosal esophageal hematomaVagal injury
Incisional seroma Improper chest closure and extravasation of fluid from chestContralateral pleural effusion Contralateral parietal pleura injury during the procedure

152 Chapter 8
placed in a left-lateral decubitus position, to drop the heart back into the peri-cardial cavity, and returned to the operating room. Cardiac compressions, if necessary, should be done open. If the pericardial patch is made too tight, a tamponade-like syndrome is created. It is important to reef or ‘pie-crust’ thepericardial patch to permit ample laxity (Figure 8.7).
Chest closure in these cases is also critical. Compared with a standard pneu-monectomy, the extrapleural dissection induces rapid filling of the hemitho-rax. Often, the fluid level is well above the carina on the first postoperative day,long before the thoracotomy has biologically sealed itself. Meticulous sutureclosure of the thoracotomy is important. If a rib was resected, serratus anteriormobilization and coverage may be required. The closure should be watertightto lessen the risk of a superficial seroma in free communication with theintrathoracic space. Should this occur, a compressive chest wrap can beemployed at the expense of pulmonary restriction. The skin incision must bekept intact to prevent seeding of the chest cavity by skin flora.
Regardless of mechanism, the development of empyema following extra-pleural pneumonectomy is a challenging problem. Infection is complicated bypatch material in the field and is not amenable to catheter-based, percuta-neous, antibiotic irrigation protocols (even in the absence of a broncho-pleuralfistula). As with a post-pneumonectomy empyema, patients are lethargic andfatigue easily. Low-grade fevers are common, but very little else localizes theinfection to the chest. A sterile thoracentesis is reassuring but does not rule out the diagnosis. Open drainage after debridement of the chest cavity andremoval of the patch material is recommended, particularly if a bronchialdehiscence is identified. The diaphragm can be reconstructed with vicryl meshand allowed to granulate. For empyema following a right-sided resection, the pericardial patch may be replaced by bovine pericardium, autologous fascia lata [41], or ipsilateral parietal pleura [42], and the cavity managed with dressing changes. A more conservative approach of closed antibiotic irrigation can be considered in the absence of a bronchial stump problem.Removal of infected tissue and the patch(es) at re-thoracotomy is a pre-requisite. Regardless, this postoperative complication usually prevents thepatient from receiving adjuvant therapy, severely compromising the benefitsof the surgery.
Conclusion
Long gone are the days when the most frequently performed pleural pro-cedure was the morbid and deforming thoracoplasty. The modern era of pleural surgery demands expertise in minimal access techniques as well as athorough understanding of surgical anatomy. There must be no reluctance to abort a video-assisted procedure in favor of the standard open approach if circumstances dictate. Thorough preoperative assessment, meticulous atten-tion to detail intraoperatively, and the recognition and treatment of postoper-ative complications facilitate the safe performance of pleural surgery.
Pleural space problems 153
References
1 Andrews CO, Gora ML. Pleural effusions. Pathophysiol Manage Ann Pharmacother 1994; 28:894–903.
2 LoCicero J. Benign and malignant disorders of the pleura. In: Baue AE, Geha AS,Hammond GL, Lak H, Naunheim KS, eds. Glenn’s Thoracic and Cardiovascular Surgery, 6th edn. Stanford, CT: Appleton and Glange, 1996; 537–555.
3 Deslauriers J, Carrier G, Beauchamp G. Diagnostic procedures. In: Pearson FG, Deslauriers J,Ginsberg RJ, Hiebert CA, McKneally MF, Urschel HC, Jr, eds. Thoracic Surgery. New York:Churchill Livingstone, 1995; 987–1001.
4 McLoud TC, Flower CDR. Imaging the pleura. Sonography, CT and MR imaging. AmJRoentgenol 1991; 156: 1145–1153.
5 Idell S. Evaluation of perplexing pleural effusions. Contemp Intern Med 1994; 6: 31–39.6 Im J-G. Imaging of the pleura. Opin Radiol 1991; 3: 387–393.7 Collins TR, Sahn SA. Thoracentesis: clinical value, complications, technical problems and
patient experience. Chest 1987; 91: 817–822.8 Kennedy L, Sahn SA. Non-invasive evaluation of the patient with a pleural effusion. Chest
Surg Clin N Am 1994; 4: 451–465.9 Tomlinson JR, Sahn SA. Invasive procedures in the diagnosis of pleural disease. Semin
Respir Med 1987; 9: 30–36.10 Feinsilver SH, Barrows AA, Braman SS. Fiberoptic bronchoscopy and pleural effusions of
unknown origin. Chest 1986; 90: 516–519.11 Jacobæus HC. The practical importance of thoracoscopy in surgery of the chest. Surg
Gynecol Obstet 1922; 34: 289–296.12 Krasna M, Flowers JL. Diagnostic thoracoscopy in a patient with a pleural mass. Surg
Laparosc Endosc Percutan Tech 1991; 1: 94–97.13 Kohmar LJ. Thoracoscopy for the evolution and treatment of pleural space disease. Chest
Surg Clin N Am 1994; 4: 467–478.14 Boutin C, Astoul P, Seitz B. The role of thoracoscopy in the evaluation and management of
pleural effusions. Lung 1990; 168 (Suppl.): 1113–1121.15 Kohman LJ. Thoracoscopy for the evaluation of treatment of pleural space disease. Chest
Surg Clin N Am 1994; 4: 467–479.16 Rusch VW, Mountain C. Thoracoscopy under regional anesthesia for the diagnosis and
management of pleural disease. Am J Surg 1987; 154: 274–278.17 Inderbitzi RGC, Grillet MP. Risk and hazards of video-thoracoscopic surgery: a collective
review. Eur J Cardiothorac Surg 1996; 10: 483–489.18 Chrétien J, Bignon J, Hirsch A, eds. The Pleura in Health and Disease. New York: Marcel
Dekker, 1985; 587–610. 19 Viskum A, Enk B. Complications of thoracoscopy. Poumon Coeur 1981; 37: 25–28.20 Viskum K. Contraindications and complications of thoracoscopy. Pneumologie 1989; 43:
55–57.21 Aelony Y, King R, Boutin C. Thoracoscopic talc poudrage pleurodesis for chronic recur-
rent pleural effusions. Ann Intern Med 1991; 115: 778–782.22 Weissberg D, Ben-Zeev I. Talc pleurodesis. J Thorac Cardiovasc Surg 1993; 106: 689–695.23 Zaugg M, Lucchinetti E, Zalunardo MP et al. Substantial changes in arterial blood gases
during thoracoscopic surgery can be missed by conventional intermittent laboratoryblood gas analysis. Anesth Analg 1998; 87: 647–653.
24 Yim APC, Liu H-P. Complications and failures of video-assisted thoracic surgery: experi-ence from two centers in Asia. Ann Thorac Surg 1996; 61: 538–541.
154 Chapter 8
25 Walker-Renard PB, Vaughan LM, Sahn SA. Chemical pleurodesis for malignant pleuraleffusions. Ann Intern Med 1994; 120: 56–64.
26 Scherer LA, Battistella FD, Owings JT, Aguilar MN. Video-assisted thoracic surgery in thetreatment of post-traumatic empyema. Arch Surg 1998; 133: 637–642.
27 Buchanan DR, Johnston ID, Kerr IH et al. Cryptogenic bilateral fibrosing pleuritis. Br J DisChest 1988; 82: 186–193.
28 Immerman SL, Sener SF, Khandekar JD. Causes and evaluation of tumor-induced hypo-glycemia. Arch Surg 1982; 117: 905–908.
29 Sugarbaker DJ, Richards WG, Garcia JP. Extrapleural pneumonectomy for malignantmesothelioma. Adv Surg 1998; 31: 253–271.
30 Antman K, Pass HI, Recht A. Benign and malignant mesothelioma. In: DeVita VT Jr,Hellman S, Rosenberg SA, eds. Cancer: Principles and Practice of Oncology, 3rd edn.Philadelphia: JB Lippincott, 1989; 1399–1414.
31 Chahinian AP, Ambinder RM, Mandel EM et al. Evaluation of 63 patients with diffusemalignant mesothelioma. Proc Am Soc Clin Oncol 1980; 21: 360A.
32 Law MR, Hodson ME, Turner-Warwick M. Malignant mesothelioma of the pleura: clinicalaspects and symptomatic treatment. Eur J Respir Dis 1984; 65: 162–168.
33 Ruffie P, Feld R, Minkin S et al. Diffuse malignant mesothelioma of the pleura in Ontarioand Quebec: a retrospective study of 332 patients. J Clin Oncol 1989; 7: 1157–1168.
34 Mychalczak BR, Nori D, Armstrong JG et al. Results of treatment of malignant pleuralmesothelioma with surgery, brachytherapy, and external beam irradiation. EndocurieHypertherm Oncol 1989; 5: 245.
35 Rusch VW, Saltz L, Venkatraman E et al. A phase II trial of pleurectomy/decortication fol-lowed by intrapleural and systemic chemotherapy for malignant pleural mesothelioma. J Clin Oncol 1994; 12: 1156–1163.
36 Butchart EG, Ashcroft T, Barnsley WC et al. Pleuropneumonectomy in the management ofdiffuse malignant mesothelioma of the pleura. Thorax 1976; 31: 15–24.
37 Sugarbaker DJ, Garcia JP, Richards WG et al. Extrapleural pneumonectomy in the multi-modality therapy of malignant pleural mesothelioma. Results in 120 consecutive patients.Ann Surg 1996; 224: 288–296.
38 Rusch VW. Indications for pneumonectomy: extrapleural pneumonectomy. Chest SurgClin N Am 1999; 9: 327–338.
39 Rusch VW, Piantadosi S, Holmes EC. The role of exptrapleural pneumonectomy in malig-nant mesothelioma. A Lung Cancer Group Trial. J Thorac Cardiovasc Surg 1991; 102: 1–9.
40 Sugarbaker DJ, Flores RM, Jaklitsch MT et al. Resection margins, extrapleural node status,and cell type determine postoperative long-term survival in trimodality therapy of malignant pleural mesothelioma: results in 183 patients. J Thorac Cardiovasc Surg 1999; 117:54–65.
41 Sollman M, Henze A, Peteffy A. Extended thoracic resection for lung cancer. Scand J ThoracCardiovasc Surg 1987; 21: 69–72.
42 Kageyama T, Suzuki K, Matsushita K et al. Pericardial closure using fascia lata in patientsundergoing pneumonectomy with pericardiectomy. Ann Thorac Surg 1998; 66: 586–587.

CHAPTER 9
Complications of chest wallreconstruction
M Bulent Tirnaksiz, Claude Deschamps
Prevention of complications is the key. Selection of the appropriate procedurefor a given patient, meticulous surgical technique and dedicated perioperativecare are paramount to prevent complications after chest wall (CW) resection.Complications can occur in the early postoperative period or late, as long-termsequelae (Table 9.1). Considerations for reconstruction of CW defects dependson factors such as the location and size of the defect, full or partial thicknessinvolvement, duration, conditions of the local tissue, general condition of thepatient, life style, type of work and the vital prognosis [1].
In small defects the skeletal component can be ignored as it will not affectchest wall function and the defect closed with only soft tissues. If structuralstability is required, however, either autogenous tissue, such as fascia lata orrib, or prosthetic material, such as the various meshes, metals, or soft tissuepatches, may be used. Defects of the CW almost always occur as a result ofsurgery for neoplasm (primary or recurrent), radiation injury, infection, ortrauma. CW defects produced by excision of most neoplasms results in loss of the skeleton and frequently the overlying soft tissues as well. Radiationinjury, infection, and trauma produce partial or full-thickness defects depend-ing upon their severity. Not uncommonly, various combinations of theseafflictions occur in the same patient, and management of these problems oftenbecomes problematic. The surgeon is anxious to obtain wide margins and ridthe patient of all possible malignant, contaminated, or irradiated tissue whileat the same time leaving a defect that can be closed in order to maintain life
155
Table 9.1 Type of complications after chest wall resection and reconstructions.
Early Late
Acute infection Recurrent/chronic infectionHemorrhage Instability/flailSeroma Arm weakness/wing scapulaFlail chest wall Chest contour irregularityIschemia/necrosis of a flap Local recurrence of malignancyInjury to vascular pedicle Chronic painRespiratory failure Ventral hernia

156 Chapter 9
itself. A thorough knowledge of reconstructive techniques with a clear operat-ive plan that includes a ‘secondary or fallback’ procedure, if possible, is mostdesirable. This dilemma is best managed by the combined efforts of both a thoracic and plastic surgeon [1–6].
Reconstruction of the bony CW is controversial. Differences of opinion existabout which patients should be reconstructed and what type of reconstructionshould be done [7–14]. In general, all full-thickness skeletal defects that havethe potential for allowing paradoxical chest wall motion should be re-constructed. The decision not to reconstruct the skeleton depends on the sizeand location of the defect. Defects < 5 cm in greatest diameter anywhere on the thorax are not usually reconstructed. Posterior defects < 10 cm, likewise,do not require reconstruction because the overlying scapula provides supportunless they are located at the tip of the scapula where entrapment of thescapula can occur during movement of the arm.
The choice of prosthetic material can be confusing. Numerous prosthesesexists and all work reasonably well [13,15]. For the most part, choice is basedon surgeon’s preference. We tend to use either Prolene® Mesh (PM) or Gore-Tex® Soft Tissue Patch (GT), although both materials are contraindicated incontaminated wounds unless the surgeon thinks that the patient cannot be extubated without this additional support. PM is more difficult than GT tostretch and suture without wrinkles and surface irregularities and does notachieve a watertight seal of the pleural space. GT, in contrast, is much easier tosuture, stretch and mold into the wound and provides a barrier that preventsfluid and air from moving between the pleural and subcutaneous space. Wesecure the patch with heavy interrupted non-absorbable sutures, which areplaced either through or around the ribs. GT, however, must be 2 mm thick asthe 1 mm thickness does not hold sutures well at the tension needed to stab-ilize the CW. For these reasons GT became our prosthesis of choice in the mid1980s. As experience was gained, we avoided placing a prosthesis in a contam-inated wound, but we became confident in leaving the prosthesis in situ in asubsequent wound infection if the prosthesis was incorporated by granulationtissue at the level of insertion to the chest wall. Combining this approach withintensive wound debridement and frequent dressing changes, the prosthesiscan be salvaged in most cases.
Suction drains are more often used in conjunction with muscle flaps whendead space and raw surface are significant. They are left in place usually untildaily drainage is < 25 cm3 per drain. Small seromas that do occur are best managed with observation as most eventually will resolve. When large orsymptomatic, aspiration under strict aseptic conditions offers the best treat-ment option. Surgical obliteration of the seroma cavity is rarely necessary inour experience.
Soft tissue reconstruction with local tissue, if possible, offers the simplestand most practical method of covering the prosthesis. If local tissue is notavailable, muscle transposition is the tissue of choice for coverage, with theomentum being reserved as back-up if muscle transposition has failed or if no
Complications of chest wall reconstruction 157
muscle is available [1–3]. Tension on a soft tissue flap should be avoided at alltimes, and on occasions a second and a third flap may be necessary to achieveproper closure of a defect. Ischemia of a flap can lead to varying degrees of tissue loss (including total necrosis of the flap) if not corrected immediately.Prevention of such circulatory embarrassment is one of the paramount goals ofany reconstruction [16]. Skin grafts are utilized where appropriate.
Several measures exist in addition to standard analgesia that may be used todecrease chest wall pain and respiratory complications in patients after CWreconstruction. These include liberal use of intercostal blocks and postoperat-ive epidural analgesia [16]. Most patients in our experience can be extubatedwithin 24 h of CW reconstruction.
Long-term sequelae following chest wall resection are uncommon. Theseinclude recurrent/chronic infection, instability/flail, arm weakness/wingscapula, chest contour irregularity, local recurrence of malignancy, chronicpain and ventral hernia [17]. Surgical removal of the sternum and manubriumin conjunction with muscle flap repair is usually well tolerated and will resultin minor changes in pulmonary function if any [18].
We recently reviewed our experience in patients undergoing prostheticbony reconstruction after CW resection with the specific goal of analysingearly and late morbidity and mortality [2]. From 1 January 1977 to 31December 1992, 197 patients underwent CW resection and reconstruction withprosthetic material at the Mayo Clinic in Rochester, Minnesota. This reviewcovers two time periods. Skeletal reconstruction was achieved with Prolene®
Mesh (PM) (Ethicon, Inc., Somerville, NJ, USA) in 64 patients (32.5%) duringthe period from 1977 to 1984. Subsequently, a 2 mm thick Gore-Tex® SoftTissue Patch (GT) (W.L. Gore and Associates, Inc., Flagstaff, AZ, USA) was util-ized in 133 (67.5%) in the second period from 1984 to 1992. Soft tissue coveragewas achieved with transposed muscle in 116 patients, local tissue only in 78,and omentum in three. Muscles transposed included latissimus dorsi in 45patients, pectoralis major in 44, serratus anterior in 15, external oblique in six,rectus abdominis in four, trapezius in one and internal oblique in one.
Postoperative complications occurred in 91 patients (46.2%) (Table 9.2).Wound seromas occurred in 10 patients with GT and in four with PM; nonedeveloped a wound infection. Twelve seromas were small and resolved, sixspontaneously and six after repeated aspirations. The remaining two patients(both with GT) required wound explorations and obliteration of the cavitywith eventual healing. Wound infections occurred in nine patients (five withPM and four with GT). The three patients who had a contaminated wound preoperatively developed a postoperative infection. All three patients hadtheir CW reconstructed with PM, and in each the PM was later removed, but atthat point (13–64 days) the underlying lung had adhered to the CW prevent-ing open pneumothorax. Thus, no further skeletal reconstruction was done. In addition, two other patients with wound infections had the PM removed. In contrast, the wounds in the four patients with GT were opened, debridedand packed with gauze. All four wounds were closed by secondary intent and
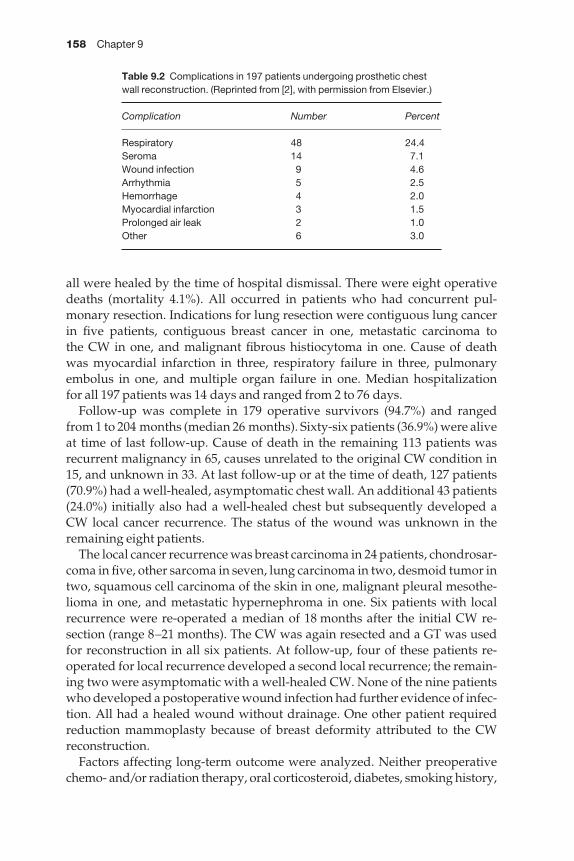
158 Chapter 9
all were healed by the time of hospital dismissal. There were eight operativedeaths (mortality 4.1%). All occurred in patients who had concurrent pul-monary resection. Indications for lung resection were contiguous lung cancerin five patients, contiguous breast cancer in one, metastatic carcinoma to the CW in one, and malignant fibrous histiocytoma in one. Cause of death was myocardial infarction in three, respiratory failure in three, pulmonary embolus in one, and multiple organ failure in one. Median hospitalization for all 197 patients was 14 days and ranged from 2 to 76 days.
Follow-up was complete in 179 operative survivors (94.7%) and rangedfrom 1 to 204 months (median 26 months). Sixty-six patients (36.9%) were aliveat time of last follow-up. Cause of death in the remaining 113 patients wasrecurrent malignancy in 65, causes unrelated to the original CW condition in15, and unknown in 33. At last follow-up or at the time of death, 127 patients(70.9%) had a well-healed, asymptomatic chest wall. An additional 43 patients(24.0%) initially also had a well-healed chest but subsequently developed aCW local cancer recurrence. The status of the wound was unknown in theremaining eight patients.
The local cancer recurrence was breast carcinoma in 24 patients, chondrosar-coma in five, other sarcoma in seven, lung carcinoma in two, desmoid tumor intwo, squamous cell carcinoma of the skin in one, malignant pleural mesothe-lioma in one, and metastatic hypernephroma in one. Six patients with localrecurrence were re-operated a median of 18 months after the initial CW re-section (range 8–21 months). The CW was again resected and a GT was usedfor reconstruction in all six patients. At follow-up, four of these patients re-operated for local recurrence developed a second local recurrence; the remain-ing two were asymptomatic with a well-healed CW. None of the nine patientswho developed a postoperative wound infection had further evidence of infec-tion. All had a healed wound without drainage. One other patient requiredreduction mammoplasty because of breast deformity attributed to the CWreconstruction.
Factors affecting long-term outcome were analyzed. Neither preoperativechemo- and/or radiation therapy, oral corticosteroid, diabetes, smoking history,
Table 9.2 Complications in 197 patients undergoing prosthetic chestwall reconstruction. (Reprinted from [2], with permission from Elsevier.)
Complication Number Percent
Respiratory 48 24.4Seroma 14 7.1Wound infection 9 4.6Arrhythmia 5 2.5Hemorrhage 4 2.0Myocardial infarction 3 1.5Prolonged air leak 2 1.0Other 6 3.0
Complications of chest wall reconstruction 159
presence of chronic obstructive pulmonary disease, histological type, nor typeof prosthesis significantly affected the incidence of seroma, wound infection,length of hospitalization, local cancer recurrence and other complications.Similarly, the extent of rib or sternal resection had no effect on postoperativemorbidity and mortality. However, associated pulmonary resection had anadverse effect on operative mortality (P = 0.0002).
This review demonstrated that CW resection and reconstruction with pros-thetic material will yield satisfactory results in most patients and that little difference exists between skeletal reconstruction with Prolene® Mesh andGore-Tex® Soft Tissue Patch. The decision of which prosthesis to use remainsthe surgeon’s choice. The goal of therapy after chest CW resection and re-construction remains a healthy patient with a healed and functional chest wall with no evidence of infection or recurrent malignancy.
References
1 Pairolero PC, Arnold PG. Thoracic wall defects: surgical management of 205 consecutivepatients. Mayo Clin Proc 1986; 61: 557–563.
2 Deschamps C, Tirnaksiz BM, Darbandi R et al. Early and long-term results of prostheticchest wall reconstruction. J Thorac Cardiovasc Surg 1999; 117: 588–591.
3 Arnold PG, Pairolero PC. Chest-wall reconstruction. An account of 500 consecutivepatients. Plast Reconst Surg 1996; 98: 804–810.
4 Arnold PG, Pairolero PC. Reconstruction of the radiated-damaged chest wall. Surg ClinNorth Am 1989; 69: 1081–1089.
5 Arnold PG, Pairolero PC. Surgical management of the radiated chest wall. Plast ReconstrSurg 1986; 77: 605–612.
6 Arnold PG, Pairolero PC. Chest wall reconstruction: experience with 100 consecutivepatients. Ann Surg 1984; 199: 725–732.
7 Soysal O, Walsh GL, Nesbitt JC et al. Resection of sternal tumors: extent, reconstructionand survival. Ann Thorac Surg 1995; 60: 1353–1359.
8 McCormack P, Bains MS, Beattie EJ Jr et al. New trends in skeletal reconstruction afterresection of chest wall tumors. Ann Thorac Surg 1981; 31: 45–52.
9 Ryan MB, McMurtrey MJ, Roth JA. Current management of chest-wall tumors. Surg ClinNorth Am 1989; 69: 1061–1080.
10 McKenna RJ, McMurtrey MJ, Larson D et al. A perspective on chest wall resection in breastcancer patients. Ann Thorac Surg 1984; 38: 482–486.
11 Kroll SS, Walsh G, Ryan B et al. Risks and benefits of using Marlex mesh in chest wallreconstruction. Ann Plast Surg 1993; 31: 303–306.
12 Economou SG, Southwick HW. The repair of thoracic wall defects with sliding rib grafts. J Thorac Surg 1958; 36: 112–116.
13 McCormack PM. Use of prosthetic materials in chest wall reconstruction: assets and liabil-ities. Surg Clin North Am 1989; 69: 965–976.
14 McKenna RJ Jr, Mountain CF, McMurtrey MJ et al. Current techniques for chest wallreconstruction: expanded possibilities for treatment. Ann Thorac Surg 1988; 46: 508–512.
15 Eschapasse H, Gaillard J, Henry E et al. Chest wall tumors: surgical management. In:Grillo HC, Eschapasse H, eds. International Trends in General Thoracic Surgery. MajorChallenges. Philadelphia: W.B. Saunders Co., 1987; 2: 292–307.

160 Chapter 9
16 Graeber GM, Seyfer AE. Complications of chest wall resection and the management of flail chest. In: Waldhausen JA, Orringer MB, eds. Complications in Cardiothoracic Surgery. St Louis: Mosby Year Book, 1991; 39: 413–421.
17 Yuen JC, Zhou AT, Serafin D et al. Long-term sequelae following median sternotomywound infection and flap reconstruction. Ann Plast Surg 1995; 35: 585–589.
18 Meadows JA III, Staats BA, Pairolero PC et al. Effect of resection of the sternum andmanubrium in conjunction with muscle transposition on pulmonary function. Mayo ClinProc 1985; 60: 604–609.
CHAPTER 10
Complications of esophageal resection
Richard J Battafarano, Nasser K Altorki
Esophageal surgery is now commonly performed for both benign and malignant disorders of the esophagus. Hospital mortality for esophagealresection has dramatically decreased over the past two decades and is cur-rently well below 10% in most esophageal centres. However, the procedure is still associated with substantial morbidity [1–3]. Because of the frequencyand severity of complications associated with esophagectomy, surgeons mustbecome familiar with each of the potential complications and take aggress-ive steps to anticipate and treat any problems that might arise in the post-operative period.
Hospital mortality
Underscoring the importance of appropriate management of postoperativecomplications, operative mortality has been shown to be inversely related tosurgeon experience [4,5]. In a retrospective review of esophagectomies per-formed for cancer, 42 patients were operated on by surgeons who performedsix or more esophagectomies per year and 32 patients were operated on by surgeons who performed five or fewer esophagectomies per year. In the 42patients operated on by frequent surgeons, there were three (7%) anastomoticleaks and no operative deaths. In 32 patients operated on by occasional sur-geons, there were seven (22%) anastomotic leaks and seven (22%) operativedeaths. The difference in anastomotic leak rates approached but did not quitereach statistical significance (7% vs. 22%, P < 0.07) and frequent surgeons had asignificantly lower operative mortality (0% vs. 7%, P < 0.001) [5].
A retrospective study attempted to determine if increased hospital volumeas well as surgeon frequency for selected surgical oncology procedures is associated with a decreased operative mortality. Over 5000 patients were iden-tified in the Surveillance, Epidemiology, and End Results (SEER)-Medicarelinked database who underwent esophagectomy, pneumonectomy, pancrea-tectomy, liver resection, or pelvic exenteration for cancers of the esophagus,lung, colon and rectum, and various genitourinary cancers diagnosed between1984 and 1993. Higher hospital volume was linked with lower operative mor-tality for esophagectomy (P < 0.001), pancreatectomy (P = 0.004), liver resec-tion (P = 0.04), or pelvic exenteration (P = 0.04), but not for pneumonectomy (P = 0.32). The most striking results were for esophagectomy in which the
161

162 Chapter 10
operative mortality was 17.3% in low-volume hospitals compared with 3.4% inhigh-volume hospitals [6].
Patient selection
Although individual surgical expertise and familiarity of all hospital person-nel with the management of patients after esophagectomy are important, theselection of patients who have adequate physiological reserves to withstandan extended operation and a potentially complicated postoperative courseremains an important responsibility of the surgeon. In an attempt to defineobjective criteria that might help to identify those patients unable to tolerateesophagectomy, a three-phase study was undertaken [7]. In phase I, therecords of 432 patients who underwent esophagectomy from 1982 to 1991were retrospectively reviewed. From this analysis, four parameters wereidentified that correlated with morbidity and mortality after esophagectomy:(i) Karnofsky index < 80%, (ii) aminopyrine breath test < 0.4, (iii) vital capacity< 90%, and (iv) PaO2 < 70 mmHg. Using this information, they devised a com-posite risk score incorporating a multiplier factor based on the relative riskassociated with each individual factor: general status × 4, cardiac function × 3,pulmonary function × 2, and hepatic function × 2 (Table 10.1). Summation ofthe results creates a single composite score ranging from 11 points in thosepatients without any risk factors to 33 points for a patient with the highest riskin all categories.
Table 10.1 Classification of individual organ dysfunction.
Objective data Score*
General statusNormal Karnofsky index > 80% and good cooperation 1Compromised Karnofsky index ≤ 80% or poor cooperation 2Severely impaired Karnofsky index ≤ 80% and poor cooperation 3
Cardiac functionNormal Normal risk for major surgical procedure 1Compromised Increased risk for major surgical procedure 2Severely impaired High risk for major surgical procedure 3
Pulmonary functionNormal VC > 90% and PaO2 > 70 mmHg 1Compromised VC < 90% or PaO2 < 70 mmHg 2Severely impaired VC < 90% and PaG2 < 70 mmHg 3
Hepatic functionNormal Aminopyrine breath test > 0.4 1Compromised Aminopyrine breath test < 0.4, no cirrhosis 2Severely impaired Cirrhosis 3
*A composite risk score was created by incorporating a multiplier factor based on the relative riskassociated with each individual factor: general status × 4, cardiac function × 3, pulmonary function× 2, and hepatic function × 2. Summation of the results creates a single composite score rangingfrom 11 points in those patients without any risk factors and 33 points for a patient with thehighest risk in all categories.
Complications of esophageal resection 163
In phase II, prospective evaluation of this composite scoring system in 121 consecutive patients undergoing esophagectomy for esophageal cancerconfirmed the ability of the scoring system in predicting postoperative course.Postoperative mortality was 2% in 46 patients classified as low risk (11–15points), 5% in 55 patients classified as moderate risk (16–21 points), and 25% in the 20 classified as high risk (22–33 points). Operative mortality wassignificantly higher in patients categorized as high risk compared with moder-ate risk (P < 0.05), and low risk (P < 0.01). Importantly, of the nine patients whodied postoperatively, five had a score of 22 points or greater.
In phase III of this study, the authors used the scoring system to determinehow to manage these patients with esophageal cancer. Use of the two-stageesophageal reconstruction (resection and delayed reconstruction 4 weekslater) in moderate and high-risk patients or complete exclusion of thesepatients from esophageal resection resulted in a marked reduction in the 30-day postoperative mortality rate from 7.4% to 1.6% in 252 patients whounderwent esophagectomy. Although rigid adherence to this system mayexclude some patients from esophagectomy who might otherwise surviveoperation, it does provide an objective means to identify those patients atgreatest risk of death after esophagectomy for whom palliative measures suchas stenting and/or radiation therapy might be more appropriate.
General complications
Cardiac complicationsThe most common cardiac complications after esophagectomy are supravent-ricular tachydysrhythmia (SVT) and myocardial infarction. After obtaining a careful history identifying a patient’s functional capacity and risk factors foratherosclerotic cardiovascular disease, the need for further cardiovascularinvestigation is individualized based on the patient’s risk of developing perioperative cardiac events [8,9]. Identification of cardiac ischemia on pre-operative stress electrocardiography or thallium studies mandates a completeevaluation prior to proceeding with esophagectomy.
In an effort to identify the incidence of cardiac complications after esopha-gectomy, 100 consecutive patients who underwent transhiatal esophagectomywithout a prior history of cardiac arrhythmias were prospectively studied. Thepostoperative incidence of SVT was 13% and the incidence of acute myocar-dial infarction was 1%. SVT was associated with hemodynamic compromise in nine (69%) of 13 patients and myocardial ischemia in four (31%) of 13. One patient required immediate cardioversion for a systolic arterial pressure < 70 mmHg. After controlling the ventricular rate with diltiazem, no patienthad evidence of ongoing myocardial ischemia or infarction. The one myocar-dial infarction in the study resulted in the patient’s death [10]. Two episodes of SVT developed late in the postoperative period (days 10 and 28) and wereassociated with sepsis. The median time to development of SVT was 72 h(range 16–576), suggesting that availability of cardiac telemetry in the first 3–5days of the postoperative period is advisable.
164 Chapter 10
Deep venous thrombosis/pulmonary embolusDeep venous thrombosis (DVT) and pulmonary embolism (PE) represent serious complications in surgical patients. Although the exact incidence isunknown in patients undergoing esophagectomy, the overall incidence ofDVT and PE in general surgical patients has been calculated by pooling datafrom control patients in published trials examining the effectiveness of pro-phylactic methods [11]. The overall incidence of DVT using fibrinogen uptaketests and phlebography confirmation was 19%. In surgical patients with malig-nant disease, the incidence of DVT was 29%. In this analysis, the incidence ofclinically recognized PE and fatal PE was 1.6% and 0.9%, respectively.
Because patients undergoing esophagectomy are considered at highest risk of developing a DVT or fatal PE (major surgery in patients > 40 years plusmalignant disease), all patients should receive preoperative prophylaxis.Successful preventive strategies include low-molecular-weight heparin, low-dose unfractionated heparin, intermittent pneumatic compression stock-ings, or oral anticoagulation. In a prospective randomized study of 2551patients who had cardiac surgery, the combination of low-dose unfractionatedheparin with intermittent pneumatic compression stockings resulted in alower incidence of PE compared with patients receiving low-dose unfraction-ated heparin alone (1.5% vs. 4%, P < 0.001) [12]. Based on this information, allpatients should have pneumatic compression stockings placed before theinduction of anesthesia and used throughout the postoperative period untilthe patient is ambulating on his own. In addition, subcutaneous low-doseunfractionated heparin is given every 12 h until the time of discharge from thehospital.
Complications associated with esophageal resection
Anastomotic leaksAnastomotic dehiscence is the most serious complication associated withesophageal resection. The rate of anastomotic leak and its associated morbidityand mortality vary depending on the location of the esophagogastric anastom-osis. In a meta-analysis of the literature of the surgical treatment of patientswith esophageal carcinoma by Muller [13], the anastomotic leak rate forintrathoracic anastomoses was significantly lower compared with cervicalanastomoses (11 ± 6% vs. 19 ± 15%). However, the mortality associated withan intrathoracic leak was three times higher (69 ± 16% vs. 20 ± 11%). In con-trast, a single group compared its experience with cervical anastomoses and thoracic anastomoses and found no statistical difference in anastomoticleak rate (4.3% vs. 3.7%) or mortality associated with anastomotic leak (40% vs. 36%) [14].
In a more recent review, Urschel categorized esophagogastric anastomoticleaks into four groups according to their clinical presentation and subsequentoutcome [15]. Group 1 constitutes early fulminant leaks that present within thefirst 48 h and are usually caused by gastric (or colonic) necrosis. These patients

Complications of esophageal resection 165
present with purulent chest tube drainage and septic shock and require imme-diate thoracotomy, resection of non-viable portions of the stomach, cervicalend esophagostomy, and abdominal gastrostomy. This complication occursinfrequently but is usually fatal even with prompt aggressive treatment.
Group 2 includes clinically apparent but less catastrophic thoracic leaks.These leaks are often identified by the development of a pneumothorax or pleural effusion associated with septic deterioration. The three critical prin-ciples in the management of this problem are: (i) complete drainage of thepleural space, (ii) adequate control of the esophagogastric fistula, and (iii) re-expansion of the lung. Small anastomotic leaks will often heal if the lung iscompletely expanded because the visceral pleura functions to buttress theleak. Chest tube drainage alone, thoracoscopic drainage and repair, and re-operative thoracotomy with direct repair and muscle flap reinforcement of the leak can all be successfully used to treat this complication as long asadherence to the above principles is followed. Because the mortality associatedwith intrathoracic anastomotic dehiscence approaches 60% [13,16,17], anaggressive approach to this problem is required.
The third group consists of clinically apparent cervical leaks. These patientsoften develop wound erythema and crepitus associated with fever and an elevated white blood cell count. Initial management requires reopening thewound at the bedside. In the majority of patients, the leak will be contained inthe neck by the surrounding tissues and frequent dressing changes are all thatis required. However, a small subset of patients with esophagogastric anastom-oses constructed via a cervical approach will leak into the mediastinum orpleural space and will require the aggressive approach described above forclinically apparent thoracic leaks. The overall mortality associated with theseclinically apparent leaks from cervical anastomoses has been reported to be20% [13], indicating the importance of managing these patients appropriately.
Clinically silent leaks are found incidentally during routine postoperativecontrast studies in patients with no systemic signs of infection. The leakidentified is contained by surrounding structures and often drains back intothe lumen through the anastomotic defect. Management of these leaks is dic-tated by their location and the patient’s clinical course. In the absence of signsof infection, the patient is simply maintained on intravenous fluids and/orjejunostomy tube feedings until repeat radiological studies document anastom-otic healing. Contained leaks close to the aorta and the trachea should bedrained because of the risk of developing fistulas to these vital structures[18–20]. In addition, radiographic progression of the leak or clinical deteriora-tion of the patient mandate immediate drainage of the leak.
Anastomotic strictureDysphagia following esophageal resection as a result of narrowing at the anastomosis occurs frequently in the postoperative period. The need for ana-stomotic dilation ranges from 5% to 44%, but the incidence of true anastomoticstricture is much lower [21–24].

166 Chapter 10
Stricture formation in the immediate postoperative period is probablyrelated to inflammatory changes associated with wound healing. In support of this hypothesis, the incidence of postoperative stricture has been shown toincrease if there is a postoperative anastomotic leak [24]. The treatment of earlystrictures consists of dilation with either the mercury-tipped Maloney dilators(46–50 Fr) or with the Savory dilators (12–60 Fr) over a guide-wire underfluoroscopic control. Most anastomoses require only a single dilation, but upto 10% will persist and require repeated dilations.
Delayed stricture formation most commonly is a result of either recurrentcarcinoma or reflux esophagitis. An aggressive search for anastomotic recur-rence including barium swallow, contrast-enhanced computed tomographyimaging of the chest, and esophagoscopy with biopsy is necessary prior to ini-tiating anastomotic dilation. In the absence of recurrent cancer, most stricturescan be easily dilated. Persistent strictures can be resected and new cervicogas-tric anastomoses can be constructed.
Dumping syndromeSweating, palpitations, tachycardia, nausea, and epigastric distension follow-ing meals in patients undergoing esophagogastrectomy represent symptomsof the dumping syndrome. These intestinal vasomotor symptoms are thoughtto occur because of the rapid transit of hyperosmolar gastric contents into thejejunum resulting in rapid hyperglycemia followed by reactive hypoglycemia.Although most patients will report some symptoms attributable to the dump-ing syndrome early in the postoperative period, dietary modifications includ-ing multiple small meals, avoidance of fluids during meals, avoidance of milkproducts and high carbohydrate meals and the occasional use of antidiarrhealmedications allow the patient to overcome these symptoms within the firstyear after esophageal resection.
Delayed gastric emptyingDelayed gastric emptying occurs in a minority of patients following esopha-gogastrectomy and has been attributed to any of a number of factors.Vagotomy, torsion of the stomach into the posterolateral gutter of the rightchest, the size of the gastric conduit, the pressure gradient between theintrathoracic stomach and the abdominal duodenum, compression of the dis-tal stomach at the level of the diaphragmatic hiatus, and the lack of a drainageprocedure have all been associated with this complication. Those patients withdelayed gastric emptying are at increased risk of aspiration pneumonia andultimately impaired oral alimentation.
Gastric outlet obstruction at the level of the pylorus should be addressed atthe time of the original operation. One prospective, randomized trial studyingthe effect of pyloroplasty vs. no drainage in a group of patients undergoingIvor-Lewis esophagogastrectomy found that pyloroplasty decreased theamount of nasogastric aspirate, the gastric emptying time by radioisotopestudy, and long-term symptoms of gastric outlet obstruction [25]. It would
Complications of esophageal resection 167
therefore seem reasonable to perform a pyloroplasty or a pyloromyotomy in all patients during reconstruction after esophagogastrectomy. In addition,the diaphragmatic hiatus should comfortably admit three or four fingersalongside the stomach at the completion of the operation to allow free flow ofgastric contents into the duodenum. This may necessitate an incision in one orboth pillars of the esophageal hiatus.
Delayed gastric emptying early in the postoperative period is often causedby mucosal edema at the level of the pyloromyotomy or pyloroplasty and generally resolves within 10–14 days. During this interval it is important tokeep the stomach decompressed to prevent aspiration and to decrease tensionon the esophagogastric anastomosis. In those patients with persistent delayedgastric emptying after 14 days, erythromycin has been shown to improve emptying [26,27].
Respiratory complicationsPulmonary complications including atelectasis, pneumonia, and respiratoryinsufficiency result in significant morbidity and mortality after esophagec-tomy regardless of technique used. The incidence of pulmonary complicationsranges from 25% to 47%, and these complications are responsible for many ofthe deaths that occur after esophagectomy [1,2].
Cessation of smoking combined with an exercise program including the useof incentive spirometry for at least 2 weeks is an important part of the patient’spreoperative preparation. Adequate perioperative and postoperative anal-gesia using epidural catheters and patient-controlled analgesia has been shownto decrease the incidence of pulmonary complications especially in patientswho underwent a transthoracic esophagectomy [28]. These should be rout-inely incorporated into the postoperative care of these patients so that they can cough and breath deeply, thus clearing secretions and maintaining bron-choalveolor expansion. The use of postoperative ventilatory assistance bykeeping the patient on a ventilator the night of operation was used previously.However, extubation can safely be performed postoperatively as soon as thepatient is awake, maintaining satisfactory ventilation and has a good gagreflex [29].
Prevention of aspiration and the control of pulmonary secretions are the two most important factors in decreasing the incidence of postoperative respiratory complications. Elevation of the head of the patient and decom-pression of the gastric tube or colon interposition graft using a nasogastric tube are required in the postoperative period until the return of gastro-intestinal function. Ambulation and chest physiotherapy are initiated on the first postoperative day and continued until the time of discharge. In those patients with significant bronchorrhea after esophagectomy, daily therapeutic bronchoscopy at the bedside is performed until the patient is independently able to mobilize his secretions on his own. This is especiallyimportant in those patients who have sustained a recurrent laryngeal nerveinjury.

168 Chapter 10
ChylothoraxChylothorax following esophagectomy has an incidence ranging from 0.4% to 2.7% [30,31]. However, this complication is poorly tolerated in nutritionaldepleted patients with esophageal cancer and mortality rates as high as 50%have been reported. Postoperative chylothorax presents as persistently elev-ated chest tube output that increases with the initiation of oral intake. As thepatient’s oral or feeding tube diet is advanced to include a higher fat content,the chest tube output becomes milky white. Definitive diagnosis can beconfirmed by determining the triglyceride content of the output, but this isoften unnecessary. In equivocal cases, a triglyceride level in the pleural fluid of > 110 mg/dl is associated with a 99% chance of a chylous leak, whereas a triglyceride level of < 50 mg/dl has less than a 5% chance of a chylous effusion [32].
Prevention of unrecognized thoracic duct injuries and subsequent chylotho-rax requires careful dissection along the course of the thoracic duct duringesophagectomy. The thoracic duct begins at the confluence of the cisterna chyli in the abdomen and enters the thorax through the aortic hiatus posteriorto the aorta and anterior to the vertebral bodies of T10–L2. It then ascends justto the right of the anterior surface of the vertebral bodies between the aorta andthe azygous vein in the right hemithorax. At the level of the T4 and T5 verteb-ral bodies, the duct crosses over to the left side of the spine and passes behindthe aortic arch and into the neck. In the neck, the duct passes posteriorly to thecarotid sheath and drains into the junction of the left jugular and subclavianveins. Any injury to the thoracic duct identified intraoperatively should bemanaged with ligation of all tissues lying between the azygous vein and thedescending aorta. Careful inspection of the thorax along the course of the ductshould be performed to identify chylous leaks prior to closure of the thorax.
The management of chylothorax after esophagectomy remains controver-sial, with advocates of both conservative therapy and immediate surgicalintervention. Conservative management usually includes total parenteralnutrition, alone, or in combination with medium-chain triglyceride enteral for-mulas. Surgical intervention is usually performed via a right thoracotomywith ligation of the thoracic duct as it enters the thorax. Early surgical ligationof the thoracic duct after recognition of a chylous leak effectively controls thiscomplication [33], but requires either an open right thoracotomy or a video-assisted approach and anterior retraction of the gastric or colonic conduit inthe early postoperative period. Conservative management of this complica-tion results in closure of the chylous fistula in approximately 80% of patientswithin 14–35 days, but has associated nutritional and septic complications[34,35].
In an effort to identify those patients who will spontaneously seal their chylous fistula without surgical intervention, Dugue et al. [31] retrospectivelyexamined their experience in 23 patients who developed chylothorax afterIvor-Lewis esophagectomy. Initial management included unilateral or bilat-eral chest drainage and total parenteral nutrition as soon as the diagnosis

Complications of esophageal resection 169
of chylothorax was established. Conservative treatment was continued for atleast 12 days, after which reoperation through the previous right thoracotomywas attempted if daily chest tube output was > 500 mL/day or the lung was not reexpanded. Just prior to reoperation, a cream-rich diet was administeredvia the nasogastric tube or feeding enterostomy to facilitate identification ofthe chylous leak.
Conservative management resulted in successful recovery in 14 (61%) of 23patients. In these patients, chest drainage was stopped after a mean of 9 days(range 3–17) and initiation of enteral nutrition within 12 days (range 7–21)without the recurrence of the chylous effusion. Conservative therapy wascomplicated in one patient who developed sepsis from his central venouscatheter.
In nine patients, conservative therapy did not result in closure of the chylousleak. These patients underwent reoperation after a mean of 18 days (range12–27). Reoperation with identification and ligation of the chylous fistula wassuccessful in all nine patients. However, two patients died from sepsis associ-ated with anastomotic dehiscence. Retrospective analysis of the data identifiedone variable that was reliable for differentiating those patients in whom con-servative therapy succeeded from those who required operation. Chylousdrainage from the chest tube on postoperative day 5 was < 10 ml/kg in 12 of 14 patients (mean 6.7 ± 5.5 ml/kg) who did not require reoperation and > 10 ml/kg in all patients (mean 23.5 ± 16.6 ml/kg) who underwent reoperation.
Using this information, any patient with a chylous output of > 10 ml/kg onpostoperative day 5 should be returned to the operating room for either an open or a video-assisted transthoracic ligation of the thoracic duct.Administration of heavy cream containing methylene blue via the feedingjejunostomy for 4 h prior to surgery facilitates identification of the leak andshould be utilized in all patients. In addition to identification and ligation ofthe leak, supradiaphragmatic ligation of all tissues between the azygous veinand the aorta is performed during reoperation.
Recurrent laryngeal nerve injuryInjury to the recurrent laryngeal nerve during esophagectomy results insignificant postoperative morbidity. The recurrent laryngeal nerve suppliesmotor function to the intrinsic muscles of the larynx (except for the cricothy-roid muscle which is supplied by the external laryngeal nerve) and suppliessensory fibers to the mucous membrane of the larynx below the vocal folds.Although hoarseness is often the initial presenting sign in patients with thisinjury, the risk of aspiration and the development of pneumonia represent itsmost serious consequences. Because recurrent laryngeal nerve injury results in inability to generate a vigorous cough, postoperative pulmonary toilet isseverely compromised and the risk of postoperative pneumonia is increased.In addition, cricopharyngeal motor dysfunction and its associated dysphagiacombined with an inability to completely appose the vocal cords markedlyincrease the risk of aspiration in these patients.

170 Chapter 10
The reported incidence of recurrent laryngeal nerve injury after esophagec-tomy ranges from 3% to 45% [1,24,36–38]. Higher vocal cord palsy rates havebeen reported in those series utilizing the extended radical esophagectomytechnique; however, this is not a universal finding. Baba et al. and Nishimaki et al. reported vocal cord palsy rates of 33% and 45%, respectively, whereasAltorki et al. had only a 6% incidence. Although the majority of patients sufferonly transient vocal cord paralysis, its impact on postoperative pulmonarycare is significant. The injury to the recurrent nerve most commonly occurs in the neck; therefore, care must be taken in that location. It is important tokeep the plane of dissection on the esophageal muscle when mobilizing theesophagus from the trachea to minimize the chances of injuring the nerve in the tracheo–esophageal groove. Additionally, avoiding the use of metalretractors against the medial cervical structures and the use of forceps in thearea of the tracheo–esophageal groove will diminish the odds of traumatizingthe nerve.
Vocal cord paralysis may not become apparent until the third postoperativeday or later when patients are noted to have difficulty generating a vigorouscough. This delay in presentation is thought to be caused by a gradual decreasein vocal cord edema in the postoperative period resulting in abduction of theparalyzed cord and an inability to generate pressure against a closed glottis.The diagnosis is often confirmed at the time of therapeutic bronchoscopy forretained secretions and bronchorrhea. Optimal management of these patientsincludes repeated therapeutic bronchoscopy and ultimately medialization ofthe paralyzed vocal cord prior to the initiation of oral intake.
References
1 Altorki NK, Girardi L, Skinner DB. En bloc esophagectomy improves survival for stage IIIesophageal cancer. J Thorac Cardiovasc Surg 1997; 114: 948–955.
2 Ferguson MK, Martin TR, Reeder LB et al. Mortality after esophagectomy: risk factor ana-lysis. World J Surg 1997; 21: 599–603.
3 Kelsen DP, Ginsberg R, Pajak TF et al. Chemotherapy followed by surgery compared withsurgery alone for localized esophageal cancer. N Engl J Med 1998; 339: 1979–1984.
4 Matthews HR, Powell DJ, McConkey CC. Effect of surgical experience on the results ofresection for oesophageal carcinoma. Br J Surg 1986; 73: 621–623.
5 Miller JD, Jain MK, de Gara CJ et al. Effect of surgical experience on results of esophagec-tomy for esophageal carcinoma. J Surg Oncol 1997; 65: 20–21.
6 Begg CB, Cramer LD, Hoskins WJ et al. Impact of hospital volume on operative mortalityfor major cancer surgery. JAMA 1998; 280: 1747–1751.
7 Bartels H, Stein HJ, Siewert JR. Preoperative risk analysis and postoperative mortality ofoesophagectomy for resectable oesophageal cancer. Br J Surg 1998; 85: 840–844.
8 Eagle KA, Brundage BH, Chaitman BR et al. Guidelines for perioperative cardiovascularevaluation for noncardiac surgery. Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Committee on Peri-operative Cardiovascular Evaluation for Noncardiac Surgery. J Am Coll Cardiol 1996; 27:910–948.
Complications of esophageal resection 171
9 Mangano DT, Goldman L. Preoperative assessment of patients with known or suspectedcoronary disease. N Engl J Med 1995; 333: 1750–1756.
10 Amar D, Burt ME, Bains MS et al. Symptomatic tachydysrhythmias after esophagectomy:incidence and outcome measures. Ann Thorac Surg 1996; 61: 1506–1509.
11 Clagett GP, Anderson FA Jr, Geerts W et al. Prevention of venous thromboembolism. Chest1998; 114: 531S–560S.
12 Ramos R, Salem BI, De Pawlikowski MP et al. The efficacy of pneumatic compressionstockings in the prevention of pulmonary embolism after cardiac surgery. Chest 1996; 109:82–85.
13 Muller JM, Erasmi H, Stelzner M et al. Surgical therapy of oesophageal carcinoma. Br JSurg 1990; 77: 845–857.
14 Lam TC, Fok M, Cheng SW et al. Anastomotic complications after esophagectomy for cancer. A comparison of neck and chest anastomoses. J Thorac Cardiovasc Surg 1992; 104:395–400.
15 Urschel JD. Esophagogastrostomy anastomotic leaks complicating esophagectomy: areview. Am J Surg 1995; 169: 634–640.
16 Patil PK, Patel SG, Mistry RC et al. Cancer of the esophagus: esophagogastric anastomoticleakaa retrospective study of predisposing factors. J Surg Oncol 1992; 49: 163–167.
17 Tam PC, Fok M, Wong J. Reexploration for complications after esophagectomy for cancer.J Thorac Cardiovasc Surg 1989; 98: 1122–1127.
18 Marty-Ane CH, Prudhome M, Fabre JM et al. Tracheoesophagogastric anastomosis fistula:a rare complication of esophagectomy. Ann Thorac Surg 1995; 60: 690–693.
19 Bartels HE, Stein HJ, Siewert JR. Tracheobronchial lesions following oesophagectomy:prevalence, predisposing factors and outcome. Br J Surg 1998; 85: 403–406.
20 Matory YL, Burt M. Esophagogastrectomy: reoperation for complications. J Surg Oncol1993; 54: 29–33.
21 Dewar L, Gelfand G, Finley RJ et al. Factors affecting cervical anastomotic leak and stric-ture formation following esophagogastrectomy and gastric tube interposition. Am J Surg1992; 163: 484–489.
22 Mathisen DJ, Grillo HC, Wilkins EW Jr et al. Transthoracic esophagectomy: a safeapproach to carcinoma of the esophagus. Ann Thorac Surg 1988; 45: 137–143.
23 Wong J, Cheung H, Lui R et al. Esophagogastric anastomosis performed with a stapler: theoccurrence of leakage and stricture. Surgery 1987; 101: 408–415.
24 Orringer MB, Marshall B, Stirling MC. Transhiatal esophagectomy for benign and malig-nant disease. J Thorac Cardiovasc Surg 1993; 105: 265–276.
25 Fok M, Cheng SW, Wong J. Pyloroplasty versus no drainage in gastric replacement of theesophagus. Am J Surg 1991; 162: 447–452.
26 Burt M, Scott A, Williard WC et al. Erythromycin stimulates gastric emptying afteresophagectomy with gastric replacement: a randomized clinical trial. J Thorac CardiovascSurg 1996; 111: 649–654.
27 Hill AD, Walsh TN, Hamilton D et al. Erythromycin improves emptying of the denervatedstomach after oesophagectomy. Br J Surg 1993; 80: 879–981.
28 Tsui SL, Law S, Fok M et al. Postoperative analgesia reduces mortality and morbidity afteresophagectomy. Am J Surg 1997; 173: 472–478.
29 Caldwell MT, Murphy PG, Page R et al. Timing of extubation after oesophagectomy. Br JSurg 1993; 80: 1537–1539.
30 Cerfolio RJ, Allen MS, Deschamps C et al. Postoperative chylothorax. J Thorac CardiovascSurg 1996; 112: 1361–1365.
172 Chapter 10
31 Dugue L, Sauvanet A, Farges O et al. Output of chyle as an indicator of treatment for chylothorax complicating oesophagectomy. Br J Surg 1998; 85: 1147–1149.
32 Staats BA, Ellefson RD, Budahn LL et al. The lipoprotein profile of chylous and non-chylous pleural effusions. Mayo Clin Proc 1980; 55: 700–704.
33 Orringer MB, Bluett M, Deeb GM. Aggressive treatment of chylothorax complicating tran-shiatal esophagectomy without thoracotomy. Surgery 1988; 104: 720–726.
34 Marts BC, Naunheim KS, Fiore AC et al. Conservative versus surgical management of chylothorax. Am J Surg 1992; 164: 532–534.
35 Bolger C, Walsh TN, Tanner WA et al. Chylothorax after oesophagectomy. Br J Surg 1991;78: 587–588.
36 Baba M, Aikou T, Natsugoe S et al. Quality of life following esophagectomy with three-field lymphadenectomy for carcinoma, focusing on its relationship to vocal cord palsy. DisEsoph 1998; 11: 28–34.
37 Gillinov AM, Heitmiller RF. Strategies to reduce pulmonary complications after transhi-atal esophagectomy. Dis Esoph 1998; 11: 43–47.
38 Nishimaki T, Suzuki T, Suzuki S et al. Outcomes of extended radical esophagectomy forthoracic esophageal cancer. J Am Coll Surg 1998; 186: 306–312.

CHAPTER 11
Complications of esophagealreconstruction
Alex G Little
Introduction
Esophageal reconstruction obviously follows upon an esophageal resection.Discussion of avoidance and treatment of complications of esophagectomy perse are reviewed in another chapter, while this chapter focuses on the recon-struction issues. The length of replacement organ required is dependent uponthe amount or length of the esophagus which is resected, which is in turndependent, among other factors, on whether or not the primary esophagealdisease is malignant or benign. Reconstruction can require replacement of theentire length of the thoracic esophagus with a proximal anastomosis in theneck or replacement of a shorter length of esophagus with a proximal anastom-osis in the chest. For reconstruction, either the stomach, colon, or jejunum are alternatives and any of them might be utilized. Finally, the location of thereconstruction can be either in the native bed of the esophagus in the posteriormediastinum, in a substernal location, or even above the sternum in a subcuta-neous location. It is also the case that reconstruction of the esophagus mustrestore both anatomic and functional continuity; failure or complications cantake place from either or both perspectives.
Anatomic complications
The principal anatomic issues related to complications of esophageal recon-struction are anastomotic leak, which is an early complication, and anastom-otic stricture formation, which is typically identified weeks or months after the operation. These are really two sides of the same coin and will be discussedtogether as some of the causes of either one of these two complications are also implicated in the etiology of the other [1]. Further, anastomoses that leakare more likely to stricture than those that do not. This is because the intenselocal inflammation and the ultimate wound-healing process, with collagendeposition and wound contraction, which follow exposure of the local tissuesto enteric contents and purulent material, inevitably result in constriction andnarrowing of the anastomosis.
173

174 Chapter 11
PreventionOrgan selectionThe choices for reconstruction are stomach, colon or jejunum. Each has advant-ages and disadvantages, but the stomach is usually preferred because of thereliability of the blood supply to the apex of the fundus [2]. In fact, regardlessof the organ which is utilized, the arterial flow to and venous drainage fromthe part of the interposed organ most distal from the origin of its blood supplyare probably the most important factors which influence the healing processand therefore the fate of the anastomosis.
StomachWhen stomach is used, the whole stomach can be utilized following division ofthe gastro–esophageal junction [2,3]. This division should be on the gastricside of the junction and not on the esophagus so that a remnant of squamousepithelium exposed to gastric contents is not retained. This can lead to irrita-tion and even erosion of the squamous island which is situated in a continuallyacidic environment. Alternatively, the lesser curve of the stomach, to includethe left gastric artery and its proximal branches with accompanying lymphnodes, can be resected so that a tubular configuration of the interposed stom-ach is achieved (Figure 11.1) [2,3]. Utilization of techniques which create so-called gastric tubes from either the lesser or greater curve, such as the Heimlichgastric tube, is not necessary and probably has less reliable vascularization ofthe distal end than either whole stomach or the tubularized stomach. Resectingthe lesser curve is also beneficial from an oncological perspective for cancerpatients, as it removes lymph nodes which frequently contain tumor meta-stases; however, the stomach is shortened by a few centimeters compared withthe whole stomach. Even so, the stomach tubularized in this fashion will stillroutinely reach the neck through both the posterior mediastinum and the sub-sternal route without an increase in either leak or stricture rates comparedwith the whole stomach.
Stomach preparation for esophageal replacement requires division of theleft gastric and short gastric arteries, leaving perfusion of the fundus depend-ent on flow from the right gastroepiploic and the right gastric arteries through the intramural vascular network. Gentle and minimal handling of thefundus during gastric mobilization is important for preservation of the smallvessels in this intramural plexus. If they are traumatized by rough handling ora clamp, the anastomosis of the esophagus will be to relatively ischemic tissue,increasing the likelihood of poor healing and therefore both leak and stricture.
ColonA variety of colon segments can be developed depending on which artery the segment is based upon. When choices are not restricted by intrinsic colondisease such as divertulosis or prior surgery, I prefer a colon segment based on the ascending branch of the left colic artery as shown in Figure 11.2 [4,5].The shorter the length of colon which is utilized, the more reliable is both
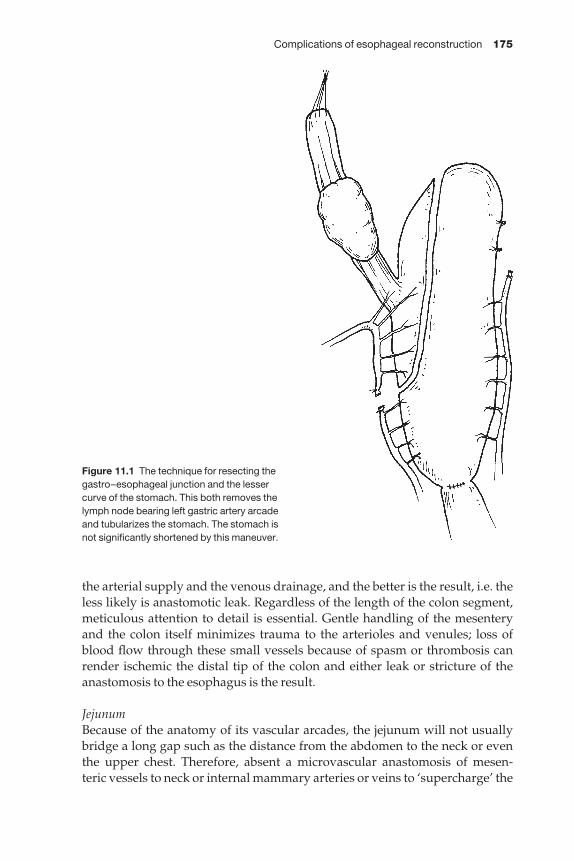
Complications of esophageal reconstruction 175
the arterial supply and the venous drainage, and the better is the result, i.e. theless likely is anastomotic leak. Regardless of the length of the colon segment,meticulous attention to detail is essential. Gentle handling of the mesenteryand the colon itself minimizes trauma to the arterioles and venules; loss ofblood flow through these small vessels because of spasm or thrombosis canrender ischemic the distal tip of the colon and either leak or stricture of theanastomosis to the esophagus is the result.
JejunumBecause of the anatomy of its vascular arcades, the jejunum will not usuallybridge a long gap such as the distance from the abdomen to the neck or eventhe upper chest. Therefore, absent a microvascular anastomosis of mesen-teric vessels to neck or internal mammary arteries or veins to ‘supercharge’ the
Figure 11.1 The technique for resecting thegastro–esophageal junction and the lessercurve of the stomach. This both removes thelymph node bearing left gastric artery arcadeand tubularizes the stomach. The stomach isnot significantly shortened by this maneuver.
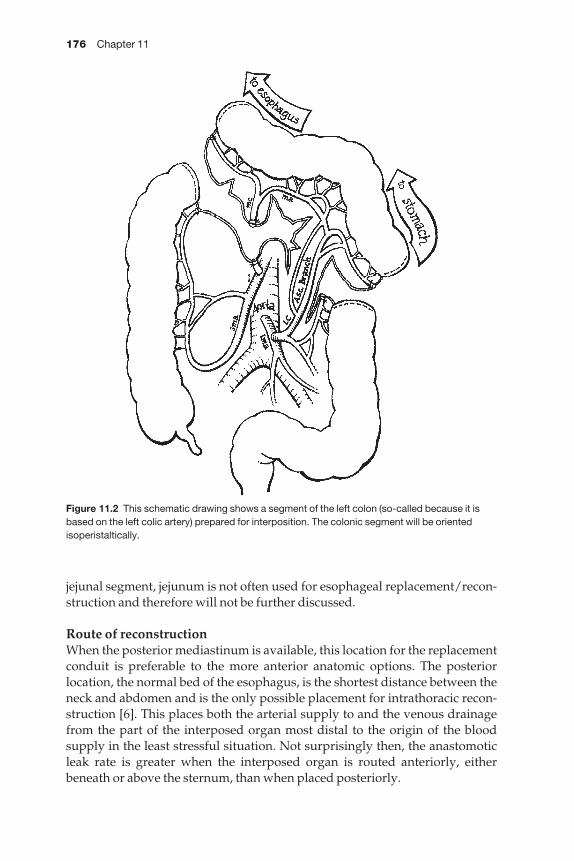
176 Chapter 11
jejunal segment, jejunum is not often used for esophageal replacement/recon-struction and therefore will not be further discussed.
Route of reconstructionWhen the posterior mediastinum is available, this location for the replacementconduit is preferable to the more anterior anatomic options. The posterior location, the normal bed of the esophagus, is the shortest distance between theneck and abdomen and is the only possible placement for intrathoracic recon-struction [6]. This places both the arterial supply to and the venous drainagefrom the part of the interposed organ most distal to the origin of the blood supply in the least stressful situation. Not surprisingly then, the anastomoticleak rate is greater when the interposed organ is routed anteriorly, eitherbeneath or above the sternum, than when placed posteriorly.
Figure 11.2 This schematic drawing shows a segment of the left colon (so-called because it isbased on the left colic artery) prepared for interposition. The colonic segment will be orientedisoperistaltically.
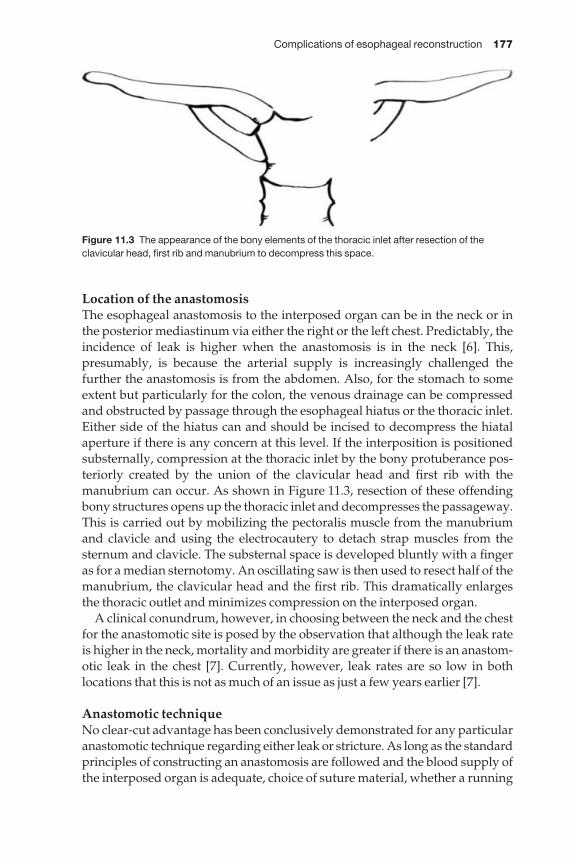
Complications of esophageal reconstruction 177
Location of the anastomosisThe esophageal anastomosis to the interposed organ can be in the neck or inthe posterior mediastinum via either the right or the left chest. Predictably, theincidence of leak is higher when the anastomosis is in the neck [6]. This, presumably, is because the arterial supply is increasingly challenged the further the anastomosis is from the abdomen. Also, for the stomach to someextent but particularly for the colon, the venous drainage can be compressedand obstructed by passage through the esophageal hiatus or the thoracic inlet.Either side of the hiatus can and should be incised to decompress the hiatalaperture if there is any concern at this level. If the interposition is positionedsubsternally, compression at the thoracic inlet by the bony protuberance pos-teriorly created by the union of the clavicular head and first rib with themanubrium can occur. As shown in Figure 11.3, resection of these offendingbony structures opens up the thoracic inlet and decompresses the passageway.This is carried out by mobilizing the pectoralis muscle from the manubriumand clavicle and using the electrocautery to detach strap muscles from the sternum and clavicle. The substernal space is developed bluntly with a fingeras for a median sternotomy. An oscillating saw is then used to resect half of themanubrium, the clavicular head and the first rib. This dramatically enlargesthe thoracic outlet and minimizes compression on the interposed organ.
A clinical conundrum, however, in choosing between the neck and the chestfor the anastomotic site is posed by the observation that although the leak rateis higher in the neck, mortality and morbidity are greater if there is an anastom-otic leak in the chest [7]. Currently, however, leak rates are so low in both locations that this is not as much of an issue as just a few years earlier [7].
Anastomotic techniqueNo clear-cut advantage has been conclusively demonstrated for any particularanastomotic technique regarding either leak or stricture. As long as the standardprinciples of constructing an anastomosis are followed and the blood supply ofthe interposed organ is adequate, choice of suture material, whether a running
Figure 11.3 The appearance of the bony elements of the thoracic inlet after resection of theclavicular head, first rib and manubrium to decompress this space.
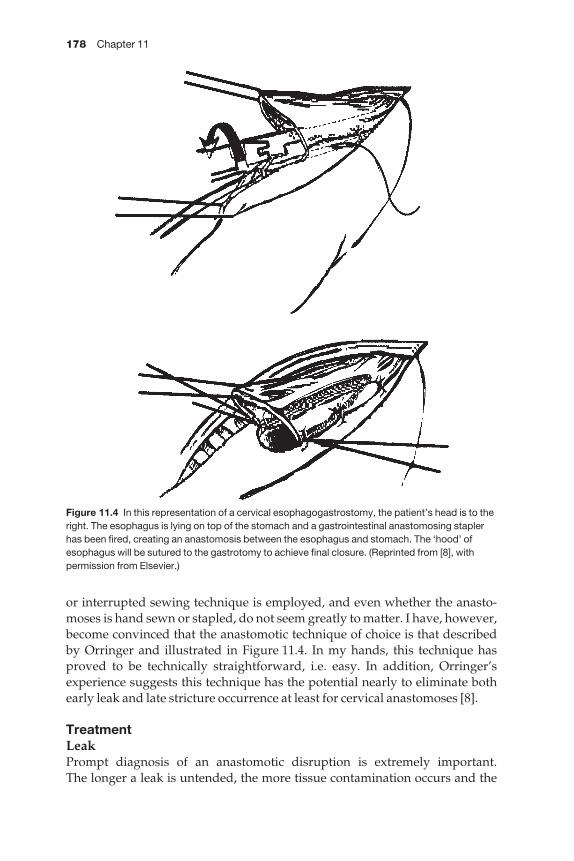
178 Chapter 11
or interrupted sewing technique is employed, and even whether the anasto-moses is hand sewn or stapled, do not seem greatly to matter. I have, however,become convinced that the anastomotic technique of choice is that describedby Orringer and illustrated in Figure 11.4. In my hands, this technique hasproved to be technically straightforward, i.e. easy. In addition, Orringer’sexperience suggests this technique has the potential nearly to eliminate bothearly leak and late stricture occurrence at least for cervical anastomoses [8].
TreatmentLeakPrompt diagnosis of an anastomotic disruption is extremely important. The longer a leak is untended, the more tissue contamination occurs and the
Figure 11.4 In this representation of a cervical esophagogastrostomy, the patient’s head is to theright. The esophagus is lying on top of the stomach and a gastrointestinal anastomosing staplerhas been fired, creating an anastomosis between the esophagus and stomach. The ‘hood’ ofesophagus will be sutured to the gastrotomy to achieve final closure. (Reprinted from [8], withpermission from Elsevier.)

Complications of esophageal reconstruction 179
greater the likelihood of septic complications. Therefore, a high level of suspi-cion is paramount. When an untoward, but non-specific event such as an unex-plained fever or tachycardia intrudes on a previously benign clinical course,anastomotic leak must be considered and a prompt barium swallow should beobtained. A normal radiological study causes no harm, while early detection ofa leak may permit salvage of the reconstruction and the patient.
If the leak is from a cervical anastomosis, initial treatment consists of fully opening all layers of the neck incision and providing local wound care with packing of the wound with saline-soaked gauze while supportingthe patient either with, preferably, enteral feeding via a jejunostomy, or par-enteral nutrition. Only if ischemic necrosis of the esophageal substitute is present is it necessary to intervene surgically. If this situation does occur, the nonviable portions of the interposed organ must be resected. If this pre-cludes immediate reanastomosis, stomach is returned to the abdomen and a feeding gastrostomy tube placed. After the patient has recovered, an altern-ative reconstruction can be attempted. If colon is involved, usually all of it is necrotic and must be removed. If only the distal tip is lost and there is asignificant viable portion which can be retained in the neck, after the patienthas recovered the gap between colon and esophagus can be bridged by a freeflap of jejunum.
StrictureWhen dysphagia is manifested in the very early postoperative period, withinthe first few weeks, the patient should be kept on a soft diet in the expectationof improvement as perianastomotic edema and inflammation subside. If reso-lution of the swallowing difficulty does not take place or if difficulty swallow-ing manifests after a few months have passed, anastomotic stricture formationis the likely cause. Intervention should be swift so that further nutritionaldepletion does not occur. Endoscopy should be performed to rule out the slimpossibility that recurrent carcinoma is present. In addition, I prefer to initiatedilation with Savary dilators passed over a wire placed during the endoscopy.Subsequent dilations can utilize either Savary or Maloney dilators. I believemultiple, gradual dilations are safer and more effective than abrupt, aggress-ive dilations. The use of balloon dilators has been reported, but I fear that anastomotic strictures might rupture and a gradual rather than an abruptstretching process seems preferable.
Functional complications
Even if anatomic continuity is restored following esophagectomy, there is nobenefit if the patient is not able to sustain a reasonable quality of life and eatand drink in a fashion approximating normal, i.e. the reconstruction mustfunction properly. Achieving this goal requires identification of and atten-tion to technical maneuvers during surgery that can reduce the incidence ofdysfunction.

180 Chapter 11
PreventionStomachThe ways in which gastric function can go awry are the occurrence of iatro-genic reflux, delayed gastric emptying and its opposite, rapid gastric emptyingwhich causes the dumping syndrome.
When stomach is used, the questions are whether to use the whole or thetubularized version and whether to perform a gastric emptying procedure.There is an enormous experience with the use of stomach as an esophagealsubstitute following esophagectomy for cancer and the functional results aregenerally satisfactory. Although the reported data are somewhat conflicting,the tubularized stomach seems to provide somewhat superior function thanthe whole stomach [3]. Peristalsis is not an important contributor to function of the transposed stomach but the tubularized configuration is less frequentlyassociated with delayed emptying, probably because the smaller tube resultsin a rapid increase in intragastric pressure as the stomach fills because of thelower compliance of the gastric wall. This rise in intragastric pressure is presumed to facilitate gastric emptying [9].
Although most patients have satisfactory gastric emptying following gastricinterposition, up to 20% of patients have dysphagia and regurgitation causedby trapping of gastric contents because of pylorospasm caused by vagotomy.For this reason, a judicious gastric emptying procedure is recommended[10–12]. An excessively aggressive pyloroplasty can allow rapid emptying ofsolids into the duodenum and dumping-type symptoms. I have found that a short Heinike–Mikulz pyloroplasty or a pyloromyotomy that divides allpyloric muscles but requires only three sutures to close achieves a reasonablebalance. Gastric emptying is expedited but does not occur with such rapiditythat dumping sequelae ensue.
ColonIn general, the shorter the length of the colon interposition, the better the func-tion and the greater the patient’s satisfaction with their ability to eat [4]. Whencolon is utilized, avoidance of redundancy is important, as if the segment sags it loops on itself and these loops can act as food traps, delaying emptyingcausing dysphagia and permitting aspiration. To prevent this complication the surgeon should use an appropriate, and not excessive, length of colon. Thisrequires that the surgeon take care intraoperatively to account for the tendencyof the harvested colon to develop spasm. If this is not done, when the colonrelaxes, the excess length will be redundant.
Although the colon contracts only infrequently, and does not immediatelyrespond to the arrival of a food bolus, it has a peristaltic orientation whichshould be respected, i.e. the interposed segment should be oriented peristaltic-ally [12]. Placing a colon segment antiperistaltically and hoping that food,salmon-like, will find its way upstream against the peristaltic gradient is foolishly hopeful.

Complications of esophageal reconstruction 181
TreatmentStomachWhen a gastric emptying procedure is not performed initially and/or gastricretention occurs postoperatively because of the failure of pyloric relaxation, a prokinetic agent such as metoclopramide or erythromycin can be tried. If this clinical trial does not succeed, endoscopic balloon dilation of the pylorus is safe and usually effective. Reoperation to perform a pyloroplasty can bedifficult, as the pylorus may be near or in the hiatus, but fortunately is rarelynecessary.
Most symptoms of dumping secondary to overly rapid gastric emptyingwill resolve without specific treatment. Encouraging water intake with meals and having the patient eat frequent small meals rather than large onesreduces the frequency and severity of the problem. Over time, symptoms typically relent and the patient can resume a more normal eating pattern.
ColonNormally, colonic transit occurs in an intermittent fashion, not continuously. It istherefore predictable that an interposed segment of colon is relatively ineffici-ent and empties by gravity assisted by intermittent mass peristalsis. Occasion-ally, however, a colon interposition simply does not function sufficiently and therefore retains food and empties mainly by gravity. Symptomatically,patients have dysphagia and frequent regurgitation and may aspirate. This is atrying situation both for the patient and the surgeon, but when it becomes clearthat the problem is functional and not anatomic (e.g. an anastomotic strictureis not the problem) then the alternative, if the stomach is available, is resectionof the colon segment and replacement with a gastric interposition.
References
1 Dewar L, Gelfand G, Finley R et al. Factors affecting cervical anastomotic leak and strictureformation following esophagogastrectomy and gastric tube interposition. Am J Surg 1992;163: 484–490.
2 Akiyama H, Miyazono H, Tsurumaru M et al. Use of the stomach as an esophageal sub-stitute. Ann Surg 1978; 188: 606–610.
3 Collard JM, Tinton N, Malaise J et al. Esophageal replacement: gastric tube or whole stomach? Ann Thorac Surg 1995; 60: 261–267.
4 Curet-Scott MJ, Ferguson MK, Little AG. Colon interposition for benign esophageal dis-ease. Surgery 1987; 102: 568–574.
5 Little AG, Skinner DB. Colon interposition for esophageal replacement. In: Cohn LH, ed.Modern Techniques in Cardiothoracic Surgery: Installment XII. Mount Kisco, NY: FuturaPublishing Co., 1985; 77-1–77-15.
6 Ngan SYK, Wong J. Lengths of different routes for esophageal replacement. J ThoracCardiovasc Surg 1986; 91: 790–792.
7 Hulscher JBF, Tijssen JGP, Obertop H, vanLanschot JJB. Transthoracic vs transhiatal resec-tion for carcinoma of the esophagus: a meta-analysis. Ann Thorac Surg 2001; 72: 306–313.
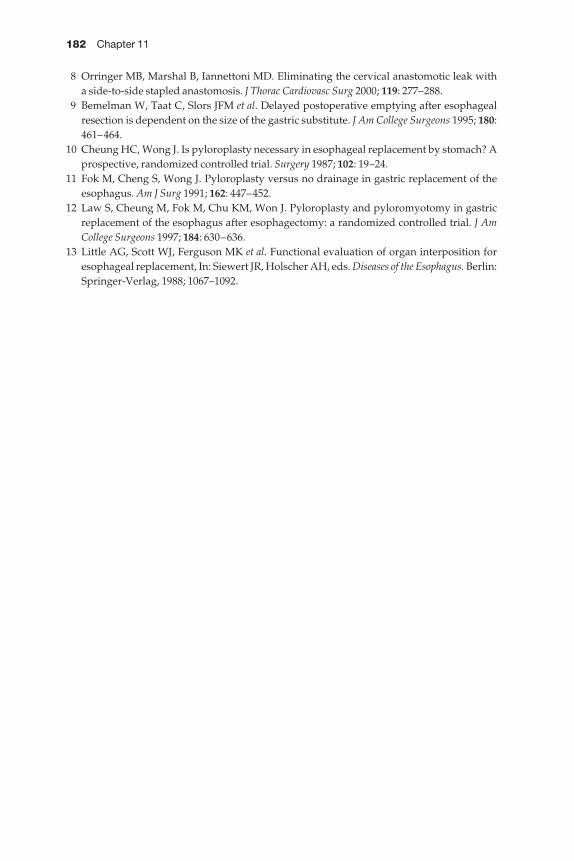
182 Chapter 11
8 Orringer MB, Marshal B, Iannettoni MD. Eliminating the cervical anastomotic leak with a side-to-side stapled anastomosis. J Thorac Cardiovasc Surg 2000; 119: 277–288.
9 Bemelman W, Taat C, Slors JFM et al. Delayed postoperative emptying after esophagealresection is dependent on the size of the gastric substitute. J Am College Surgeons 1995; 180:461–464.
10 Cheung HC, Wong J. Is pyloroplasty necessary in esophageal replacement by stomach? Aprospective, randomized controlled trial. Surgery 1987; 102: 19–24.
11 Fok M, Cheng S, Wong J. Pyloroplasty versus no drainage in gastric replacement of theesophagus. Am J Surg 1991; 162: 447–452.
12 Law S, Cheung M, Fok M, Chu KM, Won J. Pyloroplasty and pyloromyotomy in gastricreplacement of the esophagus after esophagectomy: a randomized controlled trial. J AmCollege Surgeons 1997; 184: 630–636.
13 Little AG, Scott WJ, Ferguson MK et al. Functional evaluation of organ interposition foresophageal replacement, In: Siewert JR, Holscher AH, eds. Diseases of the Esophagus. Berlin:Springer-Verlag, 1988; 1067–1092.

CHAPTER 12
Complications of antireflux surgery
Riivo Ilves, Mark R Dylewski
Introduction
There are multiple surgical approaches for the treatment of patients withsymptomatic gastroesophageal reflux disease (GERD). For many years surgeonsdebated the most appropriate route and technique by which an antirefluxoperation should be conducted, general surgeons advocating an abdominalapproach with thoracic surgeons supporting a transthoracic approach. Today,the laparoscopic approach has been established as the approach of choice for the great majority of patients. Several alternative procedures such as theposterior gastropexy described by Hill in 1959 can only be performed throughthe abdomen, whereas others, such as the modified Belsey Mark IV (1952), theNissen fundoplication (1955), and the Collis modifications (1957), can be con-structed from a thoracic or abdominal approach. The answer to which routeand technique is utilized is often dependent on the surgeon’s formal trainingas well as various physiological principles of GERD, which are beyond thescope of this chapter.
Independently of the approach utilized, opinions differ regarding the quality of the various antireflux procedures currently available to surgeons.Many criticisms have been reported for each technique, a number of which are the result of technical challenges involved in performing these operationsand the incidence of early and late surgical complications reported in the literature. The results of antireflux surgery published since the mid 1980sreveal that overall patient satisfaction is good to excellent in 86% (range73–97%) of patients, whereas a poor outcome was obtained in 14% (range3–33%) of patients [1,2]. The factors responsible for a poor outcome followingantireflux surgery are numerous and may result from erroneous preoperat-ive evaluation or patient selection, intraoperative technical misjudgement,iatrogenic complications, in addition to degradation or breakdown of the initial repair. The purpose of this chapter is to identify the pre-, intra-, andpostoperative pitfalls and perils of antireflux surgery that contribute to theacute and long-term unsatisfactory results, and outline methods to managethese complications.
183
184 Chapter 12
Preoperative pitfalls
Preoperative evaluationSurgical therapy for GERD was once reserved for patients who failed torespond to maximum medical therapy or for those who developed complica-tions of the disease. However, since the improvement in surgical results andthe advent of laparoscopic techniques, this is no longer the belief of manyphysicians. Current antireflux medical therapy is very effective in controllingsymptoms in most patients with reflux. When an individual presents withsymptomatic reflux completely refractory to medical therapy, one should besuspicious that reflux is not the cause of symptoms. Atypical respiratory andextra-esophageal symptoms secondary to GERD have been shown to respondto medical treatment [3]. Therefore, a high index of suspicion is required toconduct the proper preoperative evaluation and accurately identify and selectthe patients who will benefit from surgery.
The goals of preoperative evaluation are fivefold: (i) to diagnose GERD, (ii)to identify the anatomical and physiological defect predisposing the indi-vidual to reflux, (iii) to exclude other etiologies for the patient’s symptoms, (iv) to document objective measures of the severity of reflux, and (v) to definethe anatomy for surgical planning.
These objectives are accomplished by performing a history and physicalexamination. In addition, more objective data are obtained from upper gas-trointestinal series, esophagoscopy, manometry, and 24-h pH monitoring.
The performance of a thorough history and physical examination cannot beunderstated in this patient population. Particular attention should be paid toexcluding other etiologies that may be the underlying cause of the patient’ssymptom complex. The disease is generally idiopathic in origin, occurringmore commonly as the population grows older. Symptoms are often associ-ated with a variety of exogenous factors (i.e. alcohol, spicy food, smoking, obes-ity, etc.). These factors may exacerbate the disease, but are rarely the primarycause [4].
There are a variety of medical diseases, natural physiological states and surgical procedures that predispose patients to symptoms that mimic GERDand require an experienced clinician to differentiate them from classicalGERD. Such conditions are often resistant to standard medical therapy andresult in failure of surgical treatment when they go unrecognized [3]. The prototype condition is achalasia, in which there is insufficient relaxation of the lower esophageal sphincter and aperistalsis of the esophageal body pre-disposing the patients to retention esophagitis which can mimic heartburn.
In order to avoid erroneous diagnoses or a misadventure in patients beingconsidered for reflux surgery, the workup should follow a logical and system-atic algorithm. An upper gastrointestinal series should be the initial study performed in patients being evaluated for GERD. The benefit of this study isthat it defines the anatomy of the esophagus, the cardia and the relationship of the gastro–esophageal (GE) junction to the esophageal hiatus. The presence

Complications of antireflux surgery 185
of a foreshortened esophagus becomes an important detail in patients requir-ing antireflux surgery. Ferguson et al. documented a success rate for Nissenfundoplication of 75% in patients requiring surgical treatment of a distalesophageal stricture without shortening and an 85% success rate when aCollis-gastroplasty was added to a fundoplication in the presence of a fore-shortened esophagus [5,6]. Furthermore, a barium study may demonstratespontaneous and inducible reflux of barium in a retrograde fashion. Such afinding on barium swallow has a high correlation with abnormal gastroeso-phageal reflux. It excludes things such as gastric outlet obstruction, particu-larly in previously operated patients.
Endoscopy is an essential part of the preoperative evaluation for GERD. It isparticularly useful to exclude those less obvious lesions not well visualized on barium swallow. Contrast-enhanced radiography is relatively insensitivein diagnosing esophagitis and/or Barrett’s mucosa with dysplastic changes and even early in situ carcinoma. Barrett’s esophagus is suggested when thesquamocolumnar junction is very irregular, with tongues of columnar epithe-lium extending cephalad; however, the endoscopic diagnosis is not alwaysreliable. Therefore, if Barrett’s mucosa is suspected, it is imperative that oneobtains histological confirmation and excludes malignant disease prior to proceeding with antireflux surgery. Biopsies should be performed in all fourquadrants at the squamocolumnar junction and at multiple levels within theBarrett’s mucosa to determine histology. Brushings are also done for cytology.
The presence of an esophageal stricture should be suspected prior to endo-scopy. When present, the surgeon should attempt to determine the underly-ing etiology (benign peptic vs. malignant). This requires multiple biopsies. Onoccasion the length and diameter of the stricture may be significantly long andnarrow, making it difficult to advance the endoscope and obtain adequatebiopsies. Aggressive attempts at dilating the stricture using the endoscopeshould be condemned. If better visualization of the distal GE junction andstomach is needed in such circumstances a guide-wire should be advanced viathe endoscope through the stricture. Under fluoroscopy, serial dilatations ofthe stricture can be performed using Savory dilators. If the distal esophagealstricture is determined to be non-dilatable, primary antireflux surgery isunlikely to be successful.
Esophageal manometry provides essential information about the functionof the upper and lower esophageal sphincters as well as the body of the esoph-agus. A discussion of the diagnostic findings on manometry is beyond thescope of this chapter, but there are some important facts to remember whenconsidering whether to perform the study. The manometric studies are usuallyperformed following the clinical examination, barium and endoscopic studies.Although numerous authors have debated the utility of manometry, its prin-cipal value is to exclude motility disorders. Some authors argue that littlebenefit is received from additional studies beyond endoscopy when patientspresent with classical clinical finding of GERD. In such patients who havefailed medical management, these authors suggest that one can proceed with
186 Chapter 12
antireflux surgery with confidence that a motility disorder does not exist [7]. In our experience, we strongly recommend performing both manometry and24-h pH studies if the patient has symptoms that are not typical of GERD or if there is any significant dysphagia or abnormal findings on initial clinicalstudies.
Monitoring 24-h pH remains the gold standard for documenting GERD andquantifying the episodes of reflux. Much like manometry, patients who pre-sent with classical findings suggestive of reflux disease and are refractory to medical therapy may not require such documentation. Twenty-four-hourpH testing is particularly valuable in documenting gastroesophageal reflux in patients who present with atypical manifestations that do not respond tomedical treatment.
Other studies that have been utilized to evaluate GERD such as esophagealtransit and gastric emptying studies, endoscopic ultrasound, and computedtomography scan are reserved for specific indications to help establish thediagnosis or evaluate the surgical anatomy.
Misdiagnosis
AchalasiaThe complication that surgeons who perform antireflux surgery hope to avoidis performing an inappropriate fundoplication in patients with a primarymotility disorder. According to Jamieson, the reason for failure of antirefluxsurgery and need for reoperative surgery in 4–16% of patients is an undia-gnosed motility disorder [2,8]. The most common undiagnosed motility dis-order is achalasia. It is a rare condition with an incidence of one case per 100 000 population. Early achalasia may have symptoms similar to reflux disease, and without esophageal manometry is difficult to recognize. Thepatient who has erroneously undergone a fundoplication will represent withsevere postoperative dysphagia. It is imperative that a thorough preoperativeevaluation be conducted. The earliest symptom of achalasia is dysphagia,described in nearly all patients as a postprandial sticking sensation in the sub-sternal area. Occasionally the sensation is referred to the pharyngoesophagealregion. Regurgitation has been reported in more than 70% of patients withachalasia. In later stages it may be reported to occur at sleep and be associatedwith a nocturnal cough and perhaps aspiration in 10%. Odynophagia isrecorded in as many as 30% of patients. The pain is often described as radiatingfrom the substernal area to the mid-back or jaw [2]. Even to the most experi-enced surgeon all of these subjective clinical findings can be erroneouslylinked to GERD. If a definitive diagnosis of achalasia is made a total fund-oplication is not the appropriate treatment.
SclerodermaScleroderma is a progressive systemic sclerosis that is characterized by gener-alized inflammation, vasculitis, and fibrosis of multiple organ systems includ-ing: skin, gastrointestinal tract, heart, lungs, and kidneys. Esophageal disease,

Complications of antireflux surgery 187
namely gastroesophageal reflux, because of involvement and weakening ofthe muscle of the distal esophagus and lower esophageal sphincter (LES), hasbeen documented in 70–90% of patients diagnosed with scleroderma. Animportant associated finding present in nearly all patients with sclerodermainvolving the esophagus is the presence of Raynaud’s phenomenon [2].Therefore, patients with atypical symptoms who are refractory to medicaltherapy or those who present with recurrent disease following antirefluxsurgery should be questioned about episodes of Raynaud’s.
There is no specific therapy for systemic scleroderma. The treatment of gas-troesophageal reflux associated with scleroderma is primarily medical. Moreaggressive therapy is reserved for the development of complications of GERD.Peptic stricture should be treated with repeated dilatation. The indication for esophageal surgery in scleroderma patients includes refractory disease:peptic stricture causing dysphagia, intractable esophagitis, and documentedpulmonary complications. Orringer et al. argue that antireflux surgery is effective in scleroderma and the presence of such a systemic disease is not acontraindication to surgery and does not affect long-term results [3,9]. Becauseof decreased esophageal motility, others have advocated a loose total fundo-plication or partial (i.e. Belsey Mark IV) technique, combined with a Collis gastroplasty and stricture dilatation in patients with peptic stricture [10–12].However, it remains unclear how well scleroderma patients do in long-termfollow-up because of the rarity of this condition. In patients with refractorydisease, severe esophagitis or peptic stricture and significantly depressedesophageal motility, some authors have advocated total esophagectomy withgastric pull-up for primary treatment because of the high likelihood of dyspha-gia developing after a standard antireflux procedure [13]. Because of the multi-focal and progressive nature of scleroderma, which often leads to an earlymortality, a cavalier approach to surgical therapy should be avoided. In ourexperience early recognition and optimal medical treatment with close follow-up have been effective in reducing symptoms and avoiding the developmentof the severe complication of GERD.
MiscellaneousOther conditions or disease processes that are associated with gastroeso-phageal reflux and should be considered include: pregnancy, irritable bowelsyndrome, other upper GI surgery (partial gastrectomy, gastrojejunostomyaBillroth I or II, etc.) and states of hypersecretion of acid such as Zollinger–Ellison syndrome [3].
Selection of operation
Following the completion of the preoperative evaluation and the establish-ment of the diagnosis of GERD, the next step is to select the most appropriateantireflux procedure. The majority of patients that present for surgical evalu-ation have classic GERD secondary to poor LES tone and have essentially nor-mal esophageal motility. The most popular antireflux operationathe Nissen

188 Chapter 12
fundoplicationais appropriate in this patient population. The Nissen fundo-plication has many potential advantages. It is simple, reproducible, and easilyadaptable to laparoscopic techniques. Although both patient and surgeonhave embraced the laparoscopic Nissen fundoplication, it is important to real-ize that no single operative procedure is suitable for all patients with GERD.Surgeons who operate on the esophagus for GERD must have a thoroughunderstanding of esophageal pathophysiology and the expertise to recognizethose individuals with atypical symptoms that would be harmed by perform-ing a total fundoplication. Surgeons must have the ability to tailor an antirefluxprocedure to a particular patient who may have a foreshortened esophagusfrom a peptic stricture or abnormal esophageal motility. Surgeons in this fieldmust have within their armamentarium the ability to perform both partial and total fundoplications as well as Collis gastroplastic modifications and anesophageal myotomy in the appropriate setting. An algorithm for the selectionof an appropriate operation is difficult to devise, particularly for patients whoare atypical and have abnormal esophageal motility.
The selection of the operation is based on several factors, including: theanatomic or physiological defect, the training and experience of the surgeon,his/her comfort level with a transthoracic or transabdominal approach andthe various operative techniques. To the apprentice this decision tree mayappear complex. However, there are a few basic principles to remember.Patients with gastroesophageal reflux and abnormal motor function experi-ence a high incidence of dysphagia with a total fundoplication. Therefore, a partial fundoplication (Toupet, Belsey IV, Thal, Hill gastropexy, etc.) shouldbe performed in those patients. Patients with classical severe reflux diseasewill have greater success with a 360° Nissen fundoplication, which results in ahigher resting tone at the level of the LES. In patients with a foreshortenedesophagus, benefit has been demonstrated from increasing the distalesophageal length by performing a Collis gastroplasty [14]. This technique re-establishes the natural position of the GE junction. A laparoscopic abdominalapproach can be utilized for most patients with normal esophageal contractil-ity and length. For patients with a shortened esophagus or an associated hiatalhernia, extended mobilization of the intrathoracic esophagus may be required.Some authors prefer the thoracic approach in this circumstance. However, inour experience adequate mobilization can be achieved via the abdominalapproach and the complications associated with a thoracotomy can beavoided. The transthoracic or thoracoabdominal approach is reserved forpatients with a hostile abdomen from prior surgery, recurrent hiatal hernia, or recurrent GERD who may require extended esophageal mobilization andCollis gastroplasty.
Intraoperative pitfalls
Antireflux surgery is associated with a low operative mortality and morbidity,which differ only slightly depending on the technique utilized. Adherence to
Complications of antireflux surgery 189
basic principles of antireflux surgery and paying meticulous detail to operat-ive technique will minimize the frequency of complications. These principlesapply whether an open or minimally invasive approach is utilized. With the recent enthusiasm for laparoscopic techniques in antireflux surgery, performance of these operations by surgeons unfamiliar with the principles ofstandard fundoplication and who have not yet advanced beyond the laparo-scopic learning curve leads to an initial increase in technical errors accountingfor operative complications or failure of the antireflux operation.
Surgery for gastroesophageal reflux is associated with an acceptable incid-ence of morbidity and mortality when performed by experienced personnel.Complications are appropriately separated into acute perioperative eventsoccurring intraoperatively or in the immediate postoperative period, andthose occurring in a delayed manner. A number of the perioperative eventsthat can occur following major abdominal or thoracic gastrointestinal surgeryare not unique to antireflux surgery but are common to most surgical proced-ures. The primary focus of this section is to define the complications unique tothe surgical approach or type of antireflux operation. The following discussionwill center on detailing the potential operative pitfalls and perioperative complications for a variety of antireflux operationsaNissen fundoplication,Hill posterior gastropexy, Belsey Mark IV repair and the Collis gastroplastymodification.
Acute perioperative complications
Serious perioperative complications of antireflux surgery are uncommon, withstudies in the literature reporting morbidity ranging from 2% to 17% and mortality typically < 1% in properly selected candidates [15,16]. It is difficult to determine the exact incidence of acute perioperative complications becauseof the scarcity of reports with thorough documentation. However, a variety ofcomplications associated with antireflux surgery and their rate of occurrencehave been compiled from various sources (Table 12.1).
The majority of this comprehensive list of complications is not exclusive to antireflux surgery but may develop following any major abdominal or thoracic operation and is only mentioned for the sake of completeness. Thepurpose of this section is to discuss the perioperative complications that areunique to the various types of antireflux operations and the methods to avoidthese pitfalls.
Bleeding—splenic, hepatic and vascular injuriesThe spleen is particularly susceptible to unintentional injury during antirefluxsurgery. Small lacerations or capsular tears causing postoperative bleedinghave been reported to range from 1% to 7% in most series [15,17]. Splenicinjuries requiring total splenectomy occur in < 1% of all antireflux operations[6]. Most iatrogenic splenic lacerations occur during division of the short gastric arteries and mobilization of the gastric cardia. In general, splenic
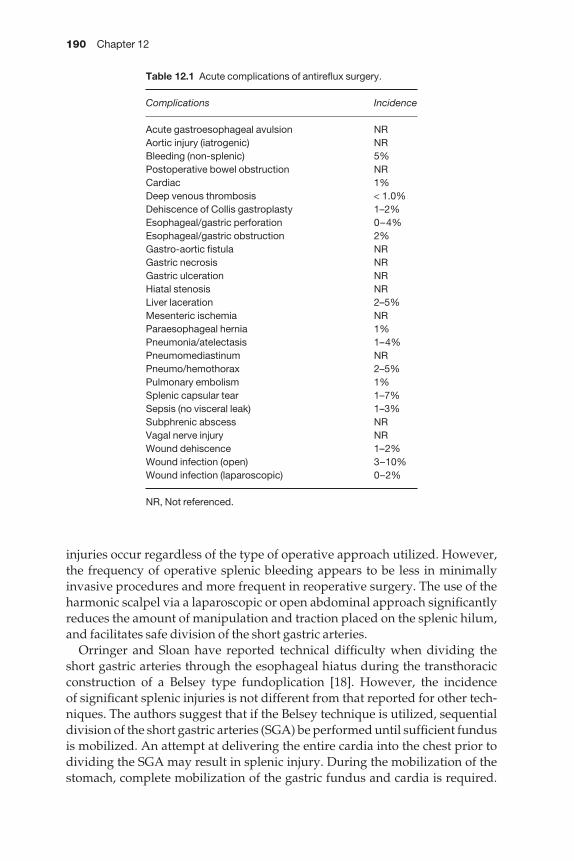
190 Chapter 12
injuries occur regardless of the type of operative approach utilized. However,the frequency of operative splenic bleeding appears to be less in minimallyinvasive procedures and more frequent in reoperative surgery. The use of theharmonic scalpel via a laparoscopic or open abdominal approach significantlyreduces the amount of manipulation and traction placed on the splenic hilum,and facilitates safe division of the short gastric arteries.
Orringer and Sloan have reported technical difficulty when dividing theshort gastric arteries through the esophageal hiatus during the transthoracicconstruction of a Belsey type fundoplication [18]. However, the incidence of significant splenic injuries is not different from that reported for other tech-niques. The authors suggest that if the Belsey technique is utilized, sequentialdivision of the short gastric arteries (SGA) be performed until sufficient fundusis mobilized. An attempt at delivering the entire cardia into the chest prior todividing the SGA may result in splenic injury. During the mobilization of thestomach, complete mobilization of the gastric fundus and cardia is required.
Table 12.1 Acute complications of antireflux surgery.
Complications Incidence
Acute gastroesophageal avulsion NRAortic injury (iatrogenic) NRBleeding (non-splenic) 5%Postoperative bowel obstruction NRCardiac 1%Deep venous thrombosis < 1.0%Dehiscence of Collis gastroplasty 1–2%Esophageal/gastric perforation 0–4%Esophageal/gastric obstruction 2%Gastro-aortic fistula NRGastric necrosis NRGastric ulceration NRHiatal stenosis NRLiver laceration 2–5%Mesenteric ischemia NRParaesophageal hernia 1%Pneumonia/atelectasis 1–4%Pneumomediastinum NRPneumo/hemothorax 2–5%Pulmonary embolism 1%Splenic capsular tear 1–7%Sepsis (no visceral leak) 1–3%Subphrenic abscess NRVagal nerve injury NRWound dehiscence 1–2%Wound infection (open) 3–10%Wound infection (laparoscopic) 0–2%
NR, Not referenced.
Complications of antireflux surgery 191
There is a well-known pitfall during this maneuver that all surgeons should befamiliar with, when performing either a Belsey repair or a Nissen fundoplica-tion through the chest. The upper end of the gastrohepatic and gastrocolicomentum requires division to deliver the proximal fundus and cardia into thechest cavity. An anastomotic vessel between the ascending branch of the leftgastric artery and the inferior phrenic artery referred to as ‘Belsey’s artery’requires careful division.
If splenic capsular injuries occur, most lesions can be repaired with standardsplenic salvage techniques without significantly increasing the perioperativemorbidity.
Subphrenic abscesses are uncommon following a splenic injury. However,the incidence increases when splenic bleeding is associated with iatrogenicinjury to the esophagus or stomach with contamination of the left sub-diaphragmatic space. In this situation drainage of the subdiaphragmatic spacehas proven to be ineffective but perioperative antibiotic coverage should beconsidered [19]. In case of reoperative antireflux surgery or a suspected hostileabdomen, a preoperative bowel preparation is prudent.
Mobilization of the left lobe of the liver can be difficult in one-third of patients and is associated with complications in up to 2–5% undergoingopen or laparoscopic antireflux surgery [6]. Bleeding, bile leaks and collateralinjuries to the diaphragm and heart can occur as a result of mobilization oraggressive retraction of the liver.
The incidence of vascular injuries to the aorta, mesenteric arteries and veins,diaphragmatic vessels, iliac vessels, inferior vena cava, and hepatic veins (left)has been reported and remain unusual. The celiac axis is at risk during medianarcuate ligament dissection for the Hill gastroplasty repair. These complica-tions are more commonly associated with port placement during laparoscopicprocedures, operations performed by inexperienced surgeons, aberrantanatomy and gross obesity.
Iatrogenic complications to the esophagus or stomachIntraoperative injuries to the esophagus and stomach are an infrequent occur-rence during antireflux surgery. The incidence of these iatrogenic complica-tions has been reported to be between 0 and 4% in various studies [6]. Theincidence of perforating injuries to the stomach or esophagus during antirefluxsurgery in experienced hands does not appear to be related to any particulartype of operation. However, the true percentage is difficult to determine due to insufficient data. Perforation of the esophagus and stomach in addition to other visceral organs is a particular risk in minimally invasive antirefluxsurgery. Most laparoscopic series of antireflux surgery report approximately a 1% incidence of perforation in experienced hands [20]. Perforation of the posterior aspect of the esophagus occurs when dissection of the posterior hiatus is performed. To avoid this, proper traction and counter traction dis-section techniques should be utilized. The backside of a blunt dissectinginstrument is used to lift the esophagus anteriorly while the other dissector

192 Chapter 12
is used to perform the posterior dissection. Once the esophagus is mobilizedcircumferentially, the esophagus should be encircled with a tape or Penrosedrain, stapled or sutured together anteriorly in order to utilize it for traction.This technique essentially avoids handling the esophagus directly. The ante-rior esophageal wall is at risk when a bougie is passed through the GE junction to calibrate the tightness of the fundoplication. This is avoided by carefulplacement of the bougie and continued observation during an open or laparo-scopic approach.
Improperly using instruments can cause gastric perforations from avulsioninjuries of the gastric wall due to aggressive traction. When recognized intraoperatively esophageal-gastric injuries generally can be repaired either laparoscopically or via an open technique without significant morbidity.When repairing a minor full-thickness esophageal injury, it is recommendedthat the mucosa and muscular layers be closed in two layers and buttressedwith the fundoplication wrap. Injuries to the stomach are closed in the stan-dard single or two-layer fashion. In the unusual situation that a perforationbecomes apparent in the postoperative period, and is contained, an attempt atconservative management with antibiotics, parenteral nutrition and no oralintake may be successful. Overt contamination of the abdominal or pleuralcavities requires an aggressive surgical approach. The mortality associatedwith unrecognized visceral perforation during antireflux surgery is reportedto range from 10% to 15% [21,22]. Injury to collateral viscera more commonlyoccurs in minimally invasive procedures and usually is a direct result of trocarplacement or careless introduction of the operating instruments into theabdominal cavity.
Perforation is less frequent with the open technique. Iatrogenic injuries aremore likely to occur in reoperative antireflux surgery as well as during Collisgastroplastic procedures when the esophagus is foreshortened and may have asurrounding inflammatory reaction. One particular complication that we havewitnessed is the complete avulsion of the GE junction secondary to aggress-ive traction on the stomach. Individuals that are elderly and reoperative candidates who may have poor tissue quality or those who have an inflamed,shortened esophagus are susceptible to an avulsion injury. Attention to detailand good communication with the surgical assistant will avoid this com-plication. Repair entails a neo-esophagogastric anastomosis.
Paraesophageal herniationParaesophageal hernia or herniation of the fundoplication wrap through thehiatus usually presents in the late follow-up period. However, the acute devel-opment of hiatal hernia in the early postoperative period has been reported inup to 1% of patients undergoing antireflux surgery [6,23,24]. The occurrence ofparaesophageal hernias is more common following laparoscopic fundoplica-tions and in patients who have GERD with an associated large hiatal hernia.Early postoperative disruption of the hiatal crura can occur secondary to sev-eral mechanisms. The most common is failure to approximate adequately the
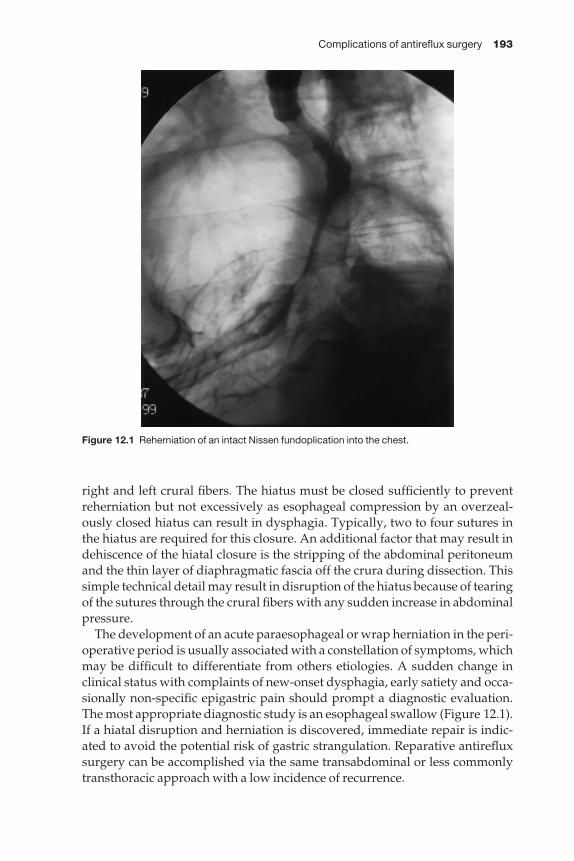
Complications of antireflux surgery 193
right and left crural fibers. The hiatus must be closed sufficiently to preventreherniation but not excessively as esophageal compression by an overzeal-ously closed hiatus can result in dysphagia. Typically, two to four sutures inthe hiatus are required for this closure. An additional factor that may result indehiscence of the hiatal closure is the stripping of the abdominal peritoneumand the thin layer of diaphragmatic fascia off the crura during dissection. Thissimple technical detail may result in disruption of the hiatus because of tearingof the sutures through the crural fibers with any sudden increase in abdominalpressure.
The development of an acute paraesophageal or wrap herniation in the peri-operative period is usually associated with a constellation of symptoms, whichmay be difficult to differentiate from others etiologies. A sudden change inclinical status with complaints of new-onset dysphagia, early satiety and occa-sionally non-specific epigastric pain should prompt a diagnostic evaluation.The most appropriate diagnostic study is an esophageal swallow (Figure 12.1).If a hiatal disruption and herniation is discovered, immediate repair is indic-ated to avoid the potential risk of gastric strangulation. Reparative antirefluxsurgery can be accomplished via the same transabdominal or less commonlytransthoracic approach with a low incidence of recurrence.
Figure 12.1 Reherniation of an intact Nissen fundoplication into the chest.

194 Chapter 12
Miscellaneous complicationsThe discussion of pitfalls associated with antireflux surgery is not completewithout mentioning a variety of rare complications that have been reported in the literature and others that have been witnessed during our experiencewith gastroesophageal reflux surgery. Cardiopulmonary complications suchas perioperative pneumonia, atelectasis or cardiac events are not unique to antireflux surgery. However, there have been a number of reports in the literature documenting specific complications associated with laparoscopicfundoplications [6,15,23,25]. The development of deep venous thrombosis and subsequent perioperative acute pulmonary embolism, pneumothorax,pneumomediastinum, extensive subcutaneous emphysema, in addition tomesenteric arterial and venous thrombosis has all been linked to the use ofintra-abdominal CO2 insufflation. The result of increased intraperitoneal pres-sure from the CO2 theoretically causes increased pressure on the pliable struc-tures within the abdominal cavity. The intra-abdominal venous pressurerarely exceeds 15 mmHg. With the standard use of intraperitoneal insufflationpressures of 15 mmHg the venous structures may collapse and contribute tostasis and thrombosis. Hypovolemia and increased ventilator pressures pre-dispose the patient to hypotension and low mesenteric arteriovenous flow thatmay aggravate the sequence of events. Presumably this mechanism may alsofunction in small arterial beds, thus contributing to the occasional rare devel-opment of mesenteric ischemia associated with laparoscopic surgery. To avoidthese complications we recommend the routine use of lower-limb com-pression devices, perioperative hydration, and limiting intraperitoneal CO2pressure to below 15 mmHg. The development of emphysema within the subcutaneous layer or mediastinum is also secondary to high insufflation pressures. This commonly occurs in three circumstances: when the initialintraperitoneal insufflation is delivered into the tissues of the abdominal wall,setting the insufflation pressure above 15 mmHg, or when the anesthesia isinadequate and the intra-abdominal pressure intermittently increases as thepatient begins to awaken. Pneumothorax occurs primarily as a result of excess-ively zealous mobilization of the esophagus resulting in penetration of theparietal pleura. The incidence of a pneumothorax occurring during laparo-scopic antireflux surgery varies between 2% and 5% [6,25].
Postoperative complications
The general postoperative complications of antireflux surgery are similar tothose of other major upper abdominal or thoracic operations in a populationwhich is typically middle aged or older, and often more obese than average.Thus, we will concentrate on problems specific to antireflux operations.
Gas bloatThis is one of the commonest postoperative problems [6,26,27,28]. It is morecommon with the Nissen total fundoplication than with the other types of

Complications of antireflux surgery 195
antireflux operations, although it occurs in all types. The causes are manifold.Many GERD patients are chronic air swallowers, having learned this habit tolessen symptoms. They continue this postoperatively, but the newly createdantireflux barrier makes belching more difficult, leading to gaseous distensionof the fundus and wrap. This produces symptoms of upper abdominal full-ness, discomfort, and distension. A temporary reduction in gastric motilityoften occurs after antireflux surgery due to vagal nerve dysfunction or gastricatony. This worsens the gas-bloat problem.
Management of gas bloat begins intraoperatively. Good surgical techniqueincludes gentle handling of tissues, especially the stomach and vagus nerves.The vagi should be maintained on the esophagus to avoid handling anddestruction of small perforating branches. In the Nissen fundoplication, thewrap should be made loose, or ‘floppy’ [6,27]. This requires the ligation anddivision of almost all of the short gastric vessels. It is my belief that the wrapshould be so loose that a bougie of any size is unnecessary. It is possible tostretch a wrap tightly around the largest bougie and still produce problems.Nonetheless, a large dilator should be in place as the wrap is constructed tocontribute to the likelihood of a loose fundoplication.
The length of wrap also may contribute to increased gas bloat. The tendencyover the years has been to shorten the wrap, with a few authors advocatingonly one stitch [28,29]. Our preference has been to use two horizontal mattresstype sutures, for an overall length of 2.5 cm.
Gas bloat syndrome improves with time. Gastro kinetic agents may helpwith the problem in the short term, and by 1 year only a few percent of patientsremain troubled by it.
FlatulenceThis problem is similar to gas bloat, with air swallowers being the mostaffected. Because of the antireflux nature of the operation, belching is moredifficult and most swallowed air ends up in the intestines. This creates distension, cramping and increased flatulence. Any vagal dysfunction maycontribute to this increased gaseousness, as may spastic colon that is often clinically associated with reflux disease. Avoidance of gaseous foods, intest-inal kinetics and time again are the therapy.
DysphagiaControl of reflux would be simple were it not necessary to preserve the abilityto swallow normally. Thus, there is a fine balance between these two require-ments in performing antireflux surgery. Early dysphagia can occur in up to50% of patients [6,30]. It can occur for many reasons. There may be post-operative inflammation or edema at the operative site, improving with time.Occasionally a hematoma may develop in the gastric wall of the wrap due tosuture injury of the submucosal vessels. Again, this improves spontaneously.As mentioned previously, the wrap may be too tight, or too long. There may be some spontaneous improvement from the former, as smooth muscle

196 Chapter 12
adaptively relaxes. There may also be distal esophageal dysfunction, due tovagal injury, usually improving with time.
A small percentage of patients have persistent dysphagia. This may be dueto too tight a wrap, or a wrap created below the GE junction on the stomachwall, or a true ‘slipped Nissen’ (Figure 12.2). It may be due to too narrow or too long a neo-esophageal tube after a Collis gastroplasty. It may also be secondary to a narrow esophageal hiatus from over-tight approximation of thecrurae. These problems can all be avoided in the operating room, and are muchmore difficult to manage postoperatively. It is worth attempting esophagealdilatation for some, but dilatation is unlikely to work for most and the need forreoperation to correct the underlying problem is likely.
Patients with a stricture preoperatively need to be dilatated to an adequatesize pre- and perioperatively. On occasion this may produce an esophagealrupture. This iatrogenic complication should be recognized promptly, and can be best dealt with by esophagectomy and cervical anastomosis, or short segment colon interposition. Patients with strictures successfully treated byantireflux surgery may require several dilatations until the inflammation andscarring settle down. The development of late dysphagia in patients with pre-vious strictures, or Barrett’s esophagus, should alert the surgeon to considerthe development of carcinoma, and lead to prompt endoscopy and biopsies.
Figure 12.2 Slipped Nissen fundoplicationaarrow shows wrap around stomach.
Complications of antireflux surgery 197
BleedingLate intra-abdominal or intrathoracic bleeding is exceedingly rare. However, it can occur from the late rupture of a subcapsular splenic hematoma. Also, one author while in training saw two late exsanguinating hemorrhages fromthe aorta at the hiatus several weeks after operation. Two possible etiologiesare periaortic infection and the most posterior crural closure stitch beingplaced too far posteriorly, and when tied was positioned similar to a ‘bow-string’ across the anterior aorta, eroding through the aortic wall over time.
Intraluminal late bleeding has been reported to occur from the gastric wrap.This is most often if the wrap has been left in the chest or more commonlywhen there is reherniation of an intact wrap into the chest through the hiatus[31]. This is due to venous stasis, or ulceration, and can be occult or massive. It is inadvisable to have a wrap in the chest because of the many potential complications. To avoid this, a lengthening procedure should be performed.Wrap herniation can be minimized by mobilizing sufficient esophagus, length-ening procedures if there is too much tension, and also fixing the wrap to the median arcuate ligament of Hill when feasible. Also crural repair should be part of every antireflux procedure.
Complete obstructionComplete occlusion of the GE junction has been infrequently reported [32]. It may occur with an extremely tight wrap, and has happened more in thelearning stages of laparoscopic fundoplication. It can also occur due to aslipped Nissen or a herniated wrap. Avoidance of too tight a wrap, particu-larly by mobilizing sufficient fundus, is important. The wrap should never be created on the stomach, and wrap stitches should incorporate sufficientesophageal wall to prevent wrap slippage. If this occurs, reoperation is almostalways necessary.
Internal fistulizationOn occasion, a fistula will develop from the wrap to the esophagus (Figure12.3). This is usually above the lower esophageal sphincter, and thus leads to intractable reflux symptoms. There may be several causes, depending on the operation. Stitches placed too deep in the gastric and esophageal wall, orsutures tied too tightly may cause strangulation and necrosis of tissue, leadingto a fistula site. Infection at the stitch site may also be a cause. It has beenreported that internal wrap to neo-esophagus fistulas have occurred in theuncut Collis–Nissen operation [33,34]. This occurs due to staple pull through.As always, avoidance by meticulous surgical detail is paramount. Fistulashave also been reported to pericardium and lung as well as other organs [35].When discovered, surgical intervention is usually necessary. The wrap is takendown and the fistula closed. A redo antireflux procedure is then performed. If the area is felt to be beyond repair, then local resection with replacement of the distal esophagus with a short segment of colon, or esophagectomy withesophagogastric anastomosis in the neck is warranted.

198 Chapter 12
External fistulizationAnecdotal and case reports exist of leaks from either the esophagus, the stom-ach or the wrap itself. These can be relatively early postoperatively fromunrecognized perforation at the time of surgery. However, they can occur at alater time. Delayed leaks can occur from a variety of causes. There may bedamage to the stomach or esophagus from diathermy. Ties or clips placed onblood vessels, particularly the short gastric arteries, may catch full-thicknessstomach wall leading to subsequent necrosis. I know of one Collis gastro-plasty, which necrosed because the left gastric artery had been previously lig-ated. External fistulas have also been reported due to an ulcer perforationwithin the fundic wrap. Again, this has been most common in fundoplicationsleft within the thoracic cavity, or those which have subsequently herniatedinto the chest. These situations, when found, usually involve a sick patient, onewho is septic. The management is often complicated and individualized,requiring drainage, resuscitation and reconstruction as appropriate to thepatient.
Bowel dysfunctionEarly postoperatively, this is a common complaint, as it is with any abdominal
Figure 12.3 Esophagogastric fistula following Belsey Mark IV fundoplication (arrow).
Complications of antireflux surgery 199
procedure. Long-term problems with diarrhea or dumping may occur withvagal nerve injury, or the use of pyloroplasty as is sometimes done with redoantireflux surgery.
Most of these problems are self-limited and lend themselves to the con-servative management of dumping syndrome.
Post-thoracotomy neuralgiaThe Belsey Mark IV procedure, as well as many of the combined Collis–Nissen,or Collis–Belsey operations, requires a thoracotomy or thoracoabdominal incision. Unique to this incision is the occasional development of long-termincisional pain. Thus, for benign disease, it is recommended that one avoidthese incisions if at all possible. If not, the use of epidural analgesia intra- andpostoperatively reduces the immediate postoperative pain and long-term neu-ralgia. Adequate intermediate pain control is also important. If pain persists,intercostal nerve block may be of short and even sometimes long-term benefit.Established post-thoracotomy neuralgia is difficult to treat, requiring analge-sia, anti-inflammatory drugs, antidepressants, transcutaneous electrical nervestimulation (TENS) apparatus, epidural steroids and even acupuncture in anycombination.
FailureThe commonest complication, particularly over time, is the failure of the operation to prevent gastroesophageal reflux. The incidence of this varies bytype of operation, author, and length of follow-up. In the open era, the recur-rence rate over the years has been reported between 5% and 20% [6,25,26]. In the laparoscopic era, the data are still in evolution. Much is made of thelearning curve and the complications and poor outcomes associated early withthe laparoscopic approach. Nonetheless, in series of sufficient numbers, therelatively early recurrence rates range from 1 to 10% [20]. It is hard to believethe long-term rates will be any better than for open procedures.
Thus, there are and will be a significant number of patients presenting with recurrent reflux symptoms at some time following previous antirefluxsurgery. This has and will always be a particular challenging group of patientsto manage. Their management will again involve the making of a precise dia-gnosis prior to any consideration of further surgical intervention. Treatmentshould once again be medical therapy at the onset. The indications for redosurgery must be even more stringent than for first-time operations. This isbecause the mortality and morbidity are higher, as is the likelihood of poorerlong-term results [36]. This in fact remains one of the most frustrating and challenging areas in surgery.
Summary
Complications of reflux surgery begin in the preoperative period, with erro-neous diagnoses or choice of operation for the patient. Many intraoperative
200 Chapter 12
pitfalls exist, leading to immediate or delayed problems. Many of these can be avoided by a thorough preoperative evaluation, appropriate selection ofpatient and procedure and proper surgical technique and attention to detail.
References
1 Little AG. Failed antireflux operations: pathophysiology and treatment. Chest Clin N Am1994; 4: 697–703.
2 Hinder RA, Klingler PJ, Perdikis G, Smith SL. Management of the failed antireflux opera-tion. Surg Clin N Am 1997; 77: 1083–1097.
3 Day JD, Richter JE. Medical and surgical conditions predisposing to gastroesophagealreflux disease. Gastroenterol Clin N Am 1990; 19: 587–603.
4 Donahue PE. Basic considerations in gastroesophageal reflux disease. Surg Clin N Am1997; 77: 1017–1040.
5 Ferguson MK. Medical and surgical management of peptic esophageal strictures. ChestSurg Clin N Am 1994; 4: 673.
6 Ferguson MK. Pitfalls and complications of antireflux surgeryaNissen techniques. ChestSurg Clin N Am 1997; 3: 489–511.
7 Jenkins AF, Cowan RJ, Richter JE. Gastroesophageal scintigraphy: is it a sensitive test forgastroesophageal reflux disease. J Clin Gastroenterol 1985; 7: 127–131.
8 Jamieson GG. The results of antireflux surgery and re-operative antireflux surgery. Gullet1993; 3: 41–45.
9 Orringer MB. Surgical management of scleroderma reflux esophagitis. Surg Clin N Am1983; 63: 859–867.
10 Henderson RD, Pearson FG. Surgical management of esophageal scleroderma. J ThoracCardiovasc Surg 1973; 66: 686–692.
11 Pearson FG, Henderson RD. Experimental and clinical studies of gastroplasty in the man-agement of acquired short esophagus. Surg Gynecol Obstet 1973; 136: 737–744.
12 Pearson FG, Langer B, Henderson RD. Gastroplasty and Belsey hiatal hernia repair: anoperation for the management of peptic stricture with acquired short esophagus. J ThoracCardiovasc Surg 1971; 61: 50–63.
13 Orringer MB, Orringer JS. Esophagectomy: definitive treatment for esophageal neuro-motor dysfunction. Ann Thorac Surg 1982; 34: 237–248.
14 Stirling MC, Orringer MB. The combined Collis–Nissen operation for esophageal refluxstrictures. Ann Thorac Surg 1988; 45: 148–157.
15 Urschel JD. Complications of antireflux surgery. Am J Surg 1993; 65: 68–70.16 Nicholson DA, Nohl-Oser HC. Hiatus hernia. A comparison between two methods of
fundoplication by evaluation of the long-term results. J Thorac Cardiovasc Surg 1976;72: 938.
17 Rossetti ME, Lieberman-Meffert D. Nissen antireflux operation. In: Nyhus LM, Baker RJ,eds. Mastery of Surgery. Boston: Little, Brown & Co., 1992; 505–515.
18 Orringer MP, Sloan H. Complications and failings of the combined Collis–Belsey opera-tion. J Thorac Cardiovasc Surg 1977; 74: 726–732.
19 Carmichael J, Thomas WO, Dillard D, Luterman A, Ferrara JJ. Indications for placement ofdrains in the splenic fossa. Am Surg 1990; 56: 313–318.
20 Collet D, Cadiere GB. Formation for the development of laparoscopic surgery for gastro-esophageal reflux disease group: conversions and complications of laparoscopic treatmentof gastroesophageal reflux disease. Am J Surg 1995; 169: 622.
Complications of antireflux surgery 201
21 Schauer PR, Meyers WC, Eubanks S, Norem RF, Franklin M, Pappas TN. Mechanisms ofgastric and esophageal perforations during laparoscopic Nissen fundoplication. Ann Surg1996; 223: 43.
22 Urschel FD. Gastroesophageal leaks after antireflux operations. Ann Thorac Surg 1994;57: 1229.
23 Johansson B, Glise H, Hallerback B. Thoracic herniation and intrathoracic gastric perfora-tion after laparoscopic fundoplication. Surg Endosc 1995; 9: 917.
24 Thayer JO Jr, Gibb SP, Ellis FH Jr. Gastroplasty and fundoplication for severe gastro-esophageal reflux with esophageal shortening. Dis Esoph 1988; 1: 153.
25 Bittner HB, Meyers WC, Brazer SR, Pappas TN. Laparoscopic Nissen fundoplication:operative results and short-term follow-up. Am J Surg 1994; 167: 193–200.
26 Maddern GJ, Jamieson GG, Chatterton BE, Collins PJ. Is there an association betweenfailed antireflux procedures and delayed gastric emptying? Ann Surg 1985; 202: 162–165.
27 Vassilakis JS, Xynos E, Kasapidis P et al. The effects of floppy Nissen fundoplication on esophageal and gastric motility in gastroesophageal reflux. Surg Gynecol Obstet 1993;177: 608.
28 Lundell LR. Gas bloat syndrome. An avoidance outcome of antireflux surgery? Dis Esoph1993; 6: 54.
29 Low DE, Mercer CD, James EC et al. Post-Nissen syndrome. Surg Gynecol Obstet 1988;167: 1.
30 Ferguson MK. Open Nissen fundoplication. Chest Clin N Am 1995; 5: 379.31 Buskin FL, Woodward ER, O’Leary JP. Occurrence of gastric ulcer after Nissen fundoplica-
tion. Am Surg 1967; 42: 821–826.32 Hill LD, Ilves R, Stevenson JK, Pearson JM. Reoperation for disruption and recurrence
after Nissen fundoplication. Arch Surg 1979; 114: 542–548.33 Pearson FG. Complications and pitfalls: Belsey and Collis-Belsey Anti-reflux repairs. Chest
Clin N Am 1997; 7: 513–531.34 Pearson FG, Cooper JD, Patterson GAP et al. Gastroplasty and fundoplication for complex
reflux problems. Ann Surg 1987; 206: 473–481.35 Hill LD. The Esophagus: Medical and Surgical Management. Philadelpia: Saunders, 1988;
167–179.36 Hinder RA, Klingler PJ, Perdikis G, Smith SL. Management of the failed antireflux opera-
tion. Surg Clin N Am 1997; 77: 1083–1099.
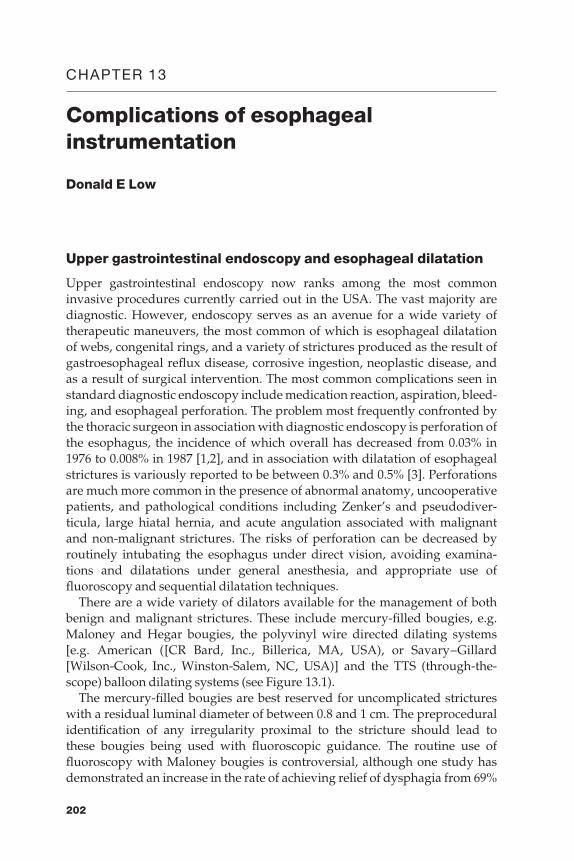
CHAPTER 13
Complications of esophagealinstrumentation
Donald E Low
Upper gastrointestinal endoscopy and esophageal dilatation
Upper gastrointestinal endoscopy now ranks among the most common invasive procedures currently carried out in the USA. The vast majority arediagnostic. However, endoscopy serves as an avenue for a wide variety oftherapeutic maneuvers, the most common of which is esophageal dilatation of webs, congenital rings, and a variety of strictures produced as the result ofgastroesophageal reflux disease, corrosive ingestion, neoplastic disease, andas a result of surgical intervention. The most common complications seen instandard diagnostic endoscopy include medication reaction, aspiration, bleed-ing, and esophageal perforation. The problem most frequently confronted bythe thoracic surgeon in association with diagnostic endoscopy is perforation ofthe esophagus, the incidence of which overall has decreased from 0.03% in1976 to 0.008% in 1987 [1,2], and in association with dilatation of esophagealstrictures is variously reported to be between 0.3% and 0.5% [3]. Perforationsare much more common in the presence of abnormal anatomy, uncooperativepatients, and pathological conditions including Zenker’s and pseudodiver-ticula, large hiatal hernia, and acute angulation associated with malignant and non-malignant strictures. The risks of perforation can be decreased byroutinely intubating the esophagus under direct vision, avoiding examina-tions and dilatations under general anesthesia, and appropriate use offluoroscopy and sequential dilatation techniques.
There are a wide variety of dilators available for the management of bothbenign and malignant strictures. These include mercury-filled bougies, e.g.Maloney and Hegar bougies, the polyvinyl wire directed dilating systems [e.g. American ([CR Bard, Inc., Billerica, MA, USA), or Savary–Gillard[Wilson-Cook, Inc., Winston-Salem, NC, USA)] and the TTS (through-the-scope) balloon dilating systems (see Figure 13.1).
The mercury-filled bougies are best reserved for uncomplicated strictureswith a residual luminal diameter of between 0.8 and 1 cm. The preproceduralidentification of any irregularity proximal to the stricture should lead to these bougies being used with fluoroscopic guidance. The routine use offluoroscopy with Maloney bougies is controversial, although one study hasdemonstrated an increase in the rate of achieving relief of dysphagia from 69%
202
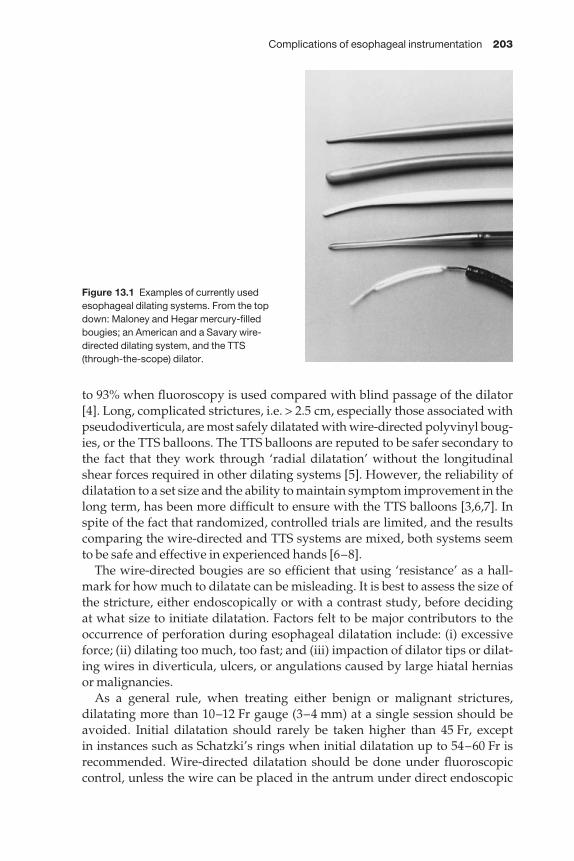
Complications of esophageal instrumentation 203
to 93% when fluoroscopy is used compared with blind passage of the dilator[4]. Long, complicated strictures, i.e. > 2.5 cm, especially those associated withpseudodiverticula, are most safely dilatated with wire-directed polyvinyl boug-ies, or the TTS balloons. The TTS balloons are reputed to be safer secondary tothe fact that they work through ‘radial dilatation’ without the longitudinalshear forces required in other dilating systems [5]. However, the reliability ofdilatation to a set size and the ability to maintain symptom improvement in thelong term, has been more difficult to ensure with the TTS balloons [3,6,7]. Inspite of the fact that randomized, controlled trials are limited, and the resultscomparing the wire-directed and TTS systems are mixed, both systems seem to be safe and effective in experienced hands [6–8].
The wire-directed bougies are so efficient that using ‘resistance’ as a hall-mark for how much to dilatate can be misleading. It is best to assess the size ofthe stricture, either endoscopically or with a contrast study, before deciding at what size to initiate dilatation. Factors felt to be major contributors to theoccurrence of perforation during esophageal dilatation include: (i) excessiveforce; (ii) dilating too much, too fast; and (iii) impaction of dilator tips or dilat-ing wires in diverticula, ulcers, or angulations caused by large hiatal hernias or malignancies.
As a general rule, when treating either benign or malignant strictures,dilatating more than 10–12 Fr gauge (3–4 mm) at a single session should beavoided. Initial dilatation should rarely be taken higher than 45 Fr, except in instances such as Schatzki’s rings when initial dilatation up to 54–60 Fr isrecommended. Wire-directed dilatation should be done under fluoroscopiccontrol, unless the wire can be placed in the antrum under direct endoscopic
Figure 13.1 Examples of currently usedesophageal dilating systems. From the topdown: Maloney and Hegar mercury-filledbougies; an American and a Savary wire-directed dilating system, and the TTS (through-the-scope) dilator.
204 Chapter 13
guidance [9]. Guide-wires should routinely be placed in the antrum, i.e. fur-ther than 60 cm from the incisors, and the wire position should be reconfirmedfollowing each sequential dilatation. Kinks in the wires can act as lead pointswhich have the potential for producing esophageal or gastric trauma. Theexperience of the operator is a major factor in the incidence of complications ingeneral, and the occurrence of perforations in particular. Two large series ofesophageal dilatations for a variety of pathological conditions demonstratedno major complications [10,11]. A major survey done by the American Societyof Gastrointestinal Endoscopy in 1974 suggests that perforation will occur in one out of every 500 endoscopies with dilatations when all techniques arecombined [12].
Whatever dilatation system is used, there should be no routine requirementfor postprocedural chest X-rays or barium studies. However, dilatation shouldnot be done with patients oversedated or under general anesthesia under normal circumstances, and patients should be closely monitored while main-taining a high level of suspicion for postprocedural symptoms of chest pain,dyspnea, voice changes, abdominal pain, or subcutaneous emphysema whichmay indicate the presence of a perforation. It should be noted, however, thattransient chest pain is common following dilatation of tight malignant stric-tures [13].
Diagnosis and treatment of perforation following upper endoscopyand esophageal dilatation proceduresSince the prompt diagnosis of perforations is essential to a good outcome, anysuspicion of perforation should lead to further studies. Cervical, mediastinal,or subdiaphragmatic air, pneumothorax or pneumopericardium, pleural effu-sion and persistent and/or severe chest or epigastric pain are all suggestive of perforation. Non-contrast studies are negative in up to 33% of cases ofesophageal perforation [14]. Contrast radiographic studies, with water-solublecontrast followed by thin barium when required, will demonstrate virtually all significant perforations. Water-soluble contrast should be used initially, but will miss some perforations [15]. When these initial studies are negative, a second examination with thin barium will identify more subtle perforations[15,16]. Water-soluble contrast examinations should not be done in patientswho are significant aspiration risks.
One of the most important aspects of these contrast studies in patients whomay have esophageal perforation is the need to provide clinical information to the radiologist and having the surgeon present for the examination whenpossible. We have had situations in which patients have been transferred toour institution with equivocal, unclear, or even frankly misleading, outsidestudies. This can lead to inappropriate operative decisions which significantlyimpact the outcome in these patients. As a result, any studies that are unclearor that do not match the clinical situation should be repeated, especially ifthere is any question regarding whether perforation is present or its exact location (see Figure 13.2a,b).
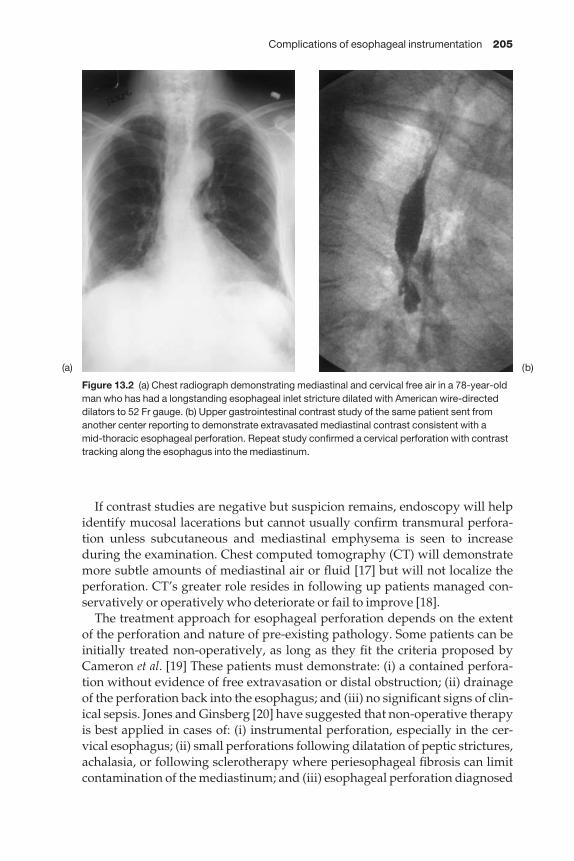
Complications of esophageal instrumentation 205
If contrast studies are negative but suspicion remains, endoscopy will helpidentify mucosal lacerations but cannot usually confirm transmural perfora-tion unless subcutaneous and mediastinal emphysema is seen to increase during the examination. Chest computed tomography (CT) will demonstratemore subtle amounts of mediastinal air or fluid [17] but will not localize theperforation. CT’s greater role resides in following up patients managed con-servatively or operatively who deteriorate or fail to improve [18].
The treatment approach for esophageal perforation depends on the extent of the perforation and nature of pre-existing pathology. Some patients can beinitially treated non-operatively, as long as they fit the criteria proposed byCameron et al. [19] These patients must demonstrate: (i) a contained perfora-tion without evidence of free extravasation or distal obstruction; (ii) drainageof the perforation back into the esophagus; and (iii) no significant signs of clin-ical sepsis. Jones and Ginsberg [20] have suggested that non-operative therapyis best applied in cases of: (i) instrumental perforation, especially in the cer-vical esophagus; (ii) small perforations following dilatation of peptic strictures,achalasia, or following sclerotherapy where periesophageal fibrosis can limitcontamination of the mediastinum; and (iii) esophageal perforation diagnosed
Figure 13.2 (a) Chest radiograph demonstrating mediastinal and cervical free air in a 78-year-oldman who has had a longstanding esophageal inlet stricture dilated with American wire-directeddilators to 52 Fr gauge. (b) Upper gastrointestinal contrast study of the same patient sent fromanother center reporting to demonstrate extravasated mediastinal contrast consistent with a mid-thoracic esophageal perforation. Repeat study confirmed a cervical perforation with contrasttracking along the esophagus into the mediastinum.
(a) (b)

206 Chapter 13
several days following injury with minimal symptoms. Careful patient selec-tion remains the hallmark for successful, non-operative therapy as mortalityrates remain in the range of 22% in collected series [20]. Conservative manage-ment of esophageal perforation includes appropriate fluid resuscitation,broad-spectrum antibiotics, enteral (preferably nasojejunal) or parenteralnutrition, proton pump inhibitors, and prokinetic agents, especially in patientswith pre-existing reflux disease. A baseline CT scan is used for comparisonpurposes in patients who deteriorate or fail to progress. This treatment strat-egy should always be associated with early surgical consultation. If initialstudies demonstrate esophageal perforation that extravasates freely, or if thereis evidence of systemic sepsis, then patients should always undergo immedi-ate surgical management.
In cases in which the esophagus is normal, surgical treatment will predomin-antly involve primary repair associated with chest and mediastinal drainage.Previous experience suggests that primary repair is less likely to succeed whena delay in diagnosis, i.e. > 24 h, has occurred [21]. This philosophy has beenincreasingly challenged recently [22–25]. I would agree that although earlyoperative management is always preferable, primary repair is often appro-priate even when a delay of several days has occurred prior to surgical inter-vention. I base the decision regarding the suitability of primary repair on endoscopic examination of the esophageal mucosa done either immediatelybefore or at the time of surgery. If the esophageal mucosa is healthy, I carry outa primary repair utilizing intraoperative endoscopy to minimize mediastinaland esophageal dissection by directing the surgeon precisely to the actual siteof perforation. Experience has shown that even when leaks occur followingappropriate primary closure, they are usually small and self-limited [22,24]. Ioften use a pedicled intercostal muscle bundle with attached pleura to buttressthe repair, especially when contamination is significant or the diagnosis hasbeen delayed. Grillo and Wilkins have demonstrated that buttressing withthickened pleura alone is another viable option [26].
Much has been written regarding debridement of tissue during primarytreatment of esophageal perforation. Devitalized tissue should be removed,although minimal dissection and debridement of the esophagus is preferable.The area of the perforation should be vigorously lavaged and thoroughlydrained and lung decortication should be carried out when required. Mucosaland muscular planes should be closed in separate layers, the mucosal repairbeing of particular importance. Endoscopic guidance can be used to minimizethe extent of esophageal muscular mobilization required to demonstrate themucosal defect in its entirety.
If esophageal perforation occurs in the presence of distal obstruction, mortal-ity rates are significantly higher when treatment is limited to primary closurealone [27]. Distal obstruction can often be managed with intraoperative dilata-tion of a distal stricture. In the presence of extremely fixed or malignantobstructions, I often carry out a primary repair of the perforation over a Celestintube which is fixed to the stomach with a chromic suture (see Figure 13.3). This
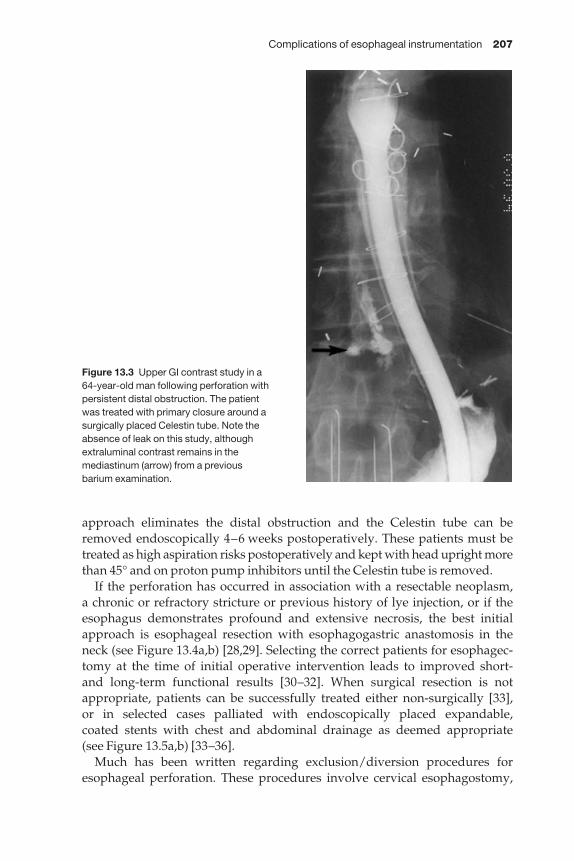
Complications of esophageal instrumentation 207
approach eliminates the distal obstruction and the Celestin tube can beremoved endoscopically 4–6 weeks postoperatively. These patients must betreated as high aspiration risks postoperatively and kept with head upright morethan 45° and on proton pump inhibitors until the Celestin tube is removed.
If the perforation has occurred in association with a resectable neoplasm, a chronic or refractory stricture or previous history of lye injection, or if theesophagus demonstrates profound and extensive necrosis, the best initialapproach is esophageal resection with esophagogastric anastomosis in theneck (see Figure 13.4a,b) [28,29]. Selecting the correct patients for esophagec-tomy at the time of initial operative intervention leads to improved short- and long-term functional results [30–32]. When surgical resection is not appropriate, patients can be successfully treated either non-surgically [33], or in selected cases palliated with endoscopically placed expandable, coated stents with chest and abdominal drainage as deemed appropriate (see Figure 13.5a,b) [33–36].
Much has been written regarding exclusion/diversion procedures foresophageal perforation. These procedures involve cervical esophagostomy,
Figure 13.3 Upper GI contrast study in a 64-year-old man following perforation withpersistent distal obstruction. The patient was treated with primary closure around asurgically placed Celestin tube. Note theabsence of leak on this study, althoughextraluminal contrast remains in themediastinum (arrow) from a previous barium examination.
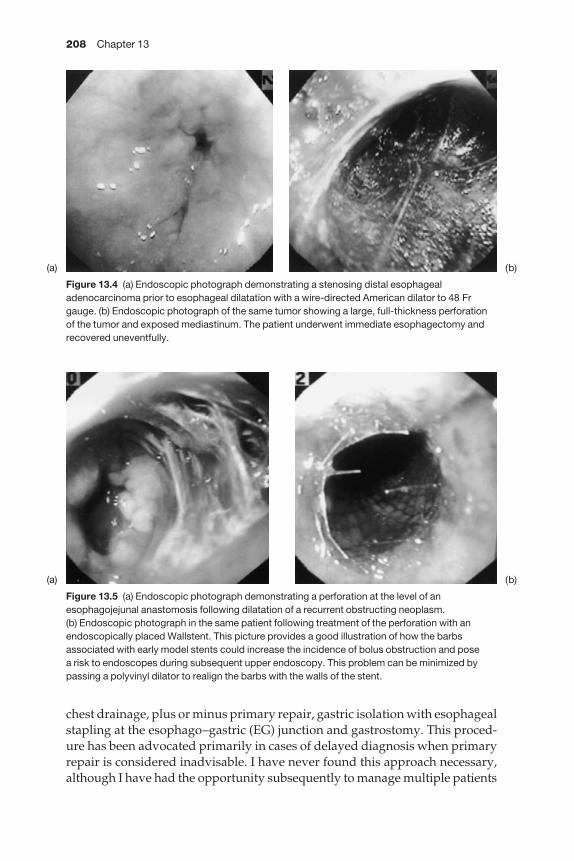
208 Chapter 13
chest drainage, plus or minus primary repair, gastric isolation with esophagealstapling at the esophago–gastric (EG) junction and gastrostomy. This proced-ure has been advocated primarily in cases of delayed diagnosis when primaryrepair is considered inadvisable. I have never found this approach necessary,although I have had the opportunity subsequently to manage multiple patients
Figure 13.4 (a) Endoscopic photograph demonstrating a stenosing distal esophagealadenocarcinoma prior to esophageal dilatation with a wire-directed American dilator to 48 Frgauge. (b) Endoscopic photograph of the same tumor showing a large, full-thickness perforationof the tumor and exposed mediastinum. The patient underwent immediate esophagectomy andrecovered uneventfully.
Figure 13.5 (a) Endoscopic photograph demonstrating a perforation at the level of anesophagojejunal anastomosis following dilatation of a recurrent obstructing neoplasm. (b) Endoscopic photograph in the same patient following treatment of the perforation with anendoscopically placed Wallstent. This picture provides a good illustration of how the barbsassociated with early model stents could increase the incidence of bolus obstruction and pose a risk to endoscopes during subsequent upper endoscopy. This problem can be minimized bypassing a polyvinyl dilator to realign the barbs with the walls of the stent.
(a)
(a)
(b)
(b)

Complications of esophageal instrumentation 209
sent to us following this procedure at other institutions. Patients with per-foration can virtually always be treated initially by either primary repair withintercostal muscle buttressing, creation of a controlled fistula (see section onsclerotherapy), or esophagectomy, even leaving reconstruction for a secondoperation if the patient is unstable.
All of the above approaches should be combined with placement of entericfeeding tubes, preferably a feeding jejunostomy which decreases the potentialfor esophageal reflux and leaves the stomach intact in case it is required as anesophageal replacement.
Pneumatic dilatation for achalasia
Successful dilatation therapy for achalasia requires forceful stretching and dis-ruption of the muscle layer of the EG junction to a diameter of ≥ 3 cm, therebyproducing marked reduction in the lower esophageal sphincter pressure. Themost commonly utilized device at the present time is the Rigiflex dilator(Microvasive, Inc., Natick, MA, USA), which consists of a double lumencatheter with a polyethylene low compliance 13.5 cm long radiolucent cylin-dric balloon. Radiopaque markers on the flexible shaft mark the two ends and the center of the balloon and the balloons come in three diameters of 30, 35,and 40 mm.
Prior to dilatation, a complete upper endoscopy is carried out and the esoph-agus emptied of food and fluid. A guide-wire is passed into the stomach andthe level of the EG junction noted fluoroscopically and measured from theincisors. The Rigiflex dilator is passed over the wire and positioned across theEG junction. Initial inflation is done with air to position the waist (area of narrowing in the balloon pertaining to the EG junction) in the center of the balloon. The balloon is fully inflated with air until waist obliteration occurs(usually between 48 and 103 kPa). This inflation is maintained for 60 s. Duringthis period, patients often complain of chest discomfiture. After the 60 s is complete, the balloon is deflated and then immediately reinflated until waistobliteration is again noted. Pressure required for obliteration during thisinflation is usually in the range of < 21 kPa. The balloon at this point isremoved. It is often found to be streaked with blood.
Chest pain usually does not persist for more than 15–20 min followingdilatations. Patients should be observed for 3–6 h following the procedure andduring this period of time an upper GI contrast study should be obtained.
Good or excellent results can be expected after a single treatment in 70% ofpatients undergoing pneumatic dilatation [37]. However, there is debate as to whether this level of success extends into the long-term. Eckardt and colleagues demonstrated only 25% good outcomes at 5 years’ follow-up [38].Treatments can be repeated with larger balloons, but success rate with sub-sequent treatments do not usually achieve the levels attained with primarydilatations [39]. There is no convincing evidence to date to suggest that largerballoons or longer inflations are more effective at relieving symptoms [40].

210 Chapter 13
Diagnosis and treatment of perforation following pneumatic dilatationThe most significant complication requiring surgical management is perfora-tion, the instance of which is reported between 0 and 22% of the time, with mostseries citing an incidence of 3–8% [37,41]. Patients historically thought to be atincreased risk of perforation include those with massively dilatated, tortuous‘sigmoid’ esophagus, epiphrenic diverticula, or those who have undergoneprevious myotomy. In fact, pneumatic dilatation can be carried out safely in any of these situations [40], although patients with massively dilatated tortuous esophagus should be considered for resection. The key to successfulmanagement of esophageal perforation requires maintaining a high level ofsuspicion and recognizing perforations when they occur. Any persistent painshould be considered highly suspicious and all contrast studies should utilizeinitially water-soluble contrast medium followed by dilute barium.
Perforations can be intramural, contained extramural, or freely extravasat-ing, and can involve the chest or abdominal cavities. Some carefully selectedpatients with perforation, especially those with non-transmural tears [42], canbe managed non-operatively (see guidelines and special recommendations for non-operative therapy of perforations listed earlier in this chapter). Thisapproach should always include early surgical consultation. All extramuralperforations should be treated surgically. This can involve either a transthor-acic or transabdominal approach. In the absence of significant chest involve-ment, I prefer the transabdominal approach to minimize contamination of thepleural space (see Figure 13.6).
Intraoperative endoscopic guidance minimizes the need for additional dis-section and esophageal muscle disruption. The mucosal and muscular layersare closed independently with monofilament absorbable suture. A myotomyis then carried out on the opposite side of the esophagus. I carry the myotomydown onto the surface of the stomach to completely disrupt the lower eso-phageal sphincter. This may necessitate the addition of a non-obstructive antire-flux procedure to avoid postoperative gastroesophageal reflux disease withoutcausing dysphagia. If the procedure is being done transabdominally, a Toupetprocedure, or if transthoracically, a Belsey Mark IV, are excellent alternatives.Prompt diagnosis and surgical treatment of perforation in achalasia patientsproduces long-term results comparable to primary surgical treatment [43].
If perforation occurs in achalasia patients with hugely dilatated, tortuousend-stage esophagus, primary treatment should be esophageal resection andreconstruction with either stomach or colon. This approach not only providesimmediate and effective treatment for the perforation, but also significantlyincreases the likelihood of good long-term results with respect to the ability toswallow and patient satisfaction [44].
Esophageal laser therapy
The most common application for esophageal laser treatment is palliation ofpatients with obstructing malignant strictures. The most commonly used laser
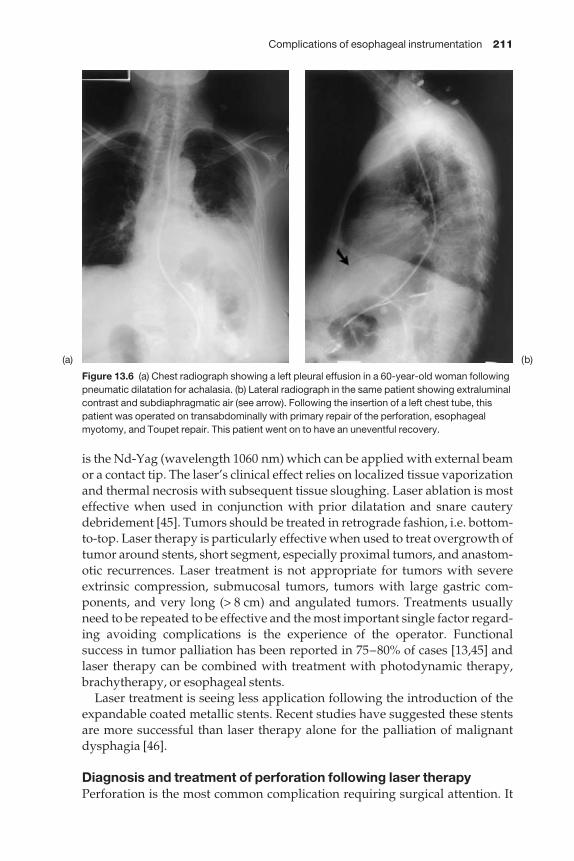
Complications of esophageal instrumentation 211
is the Nd-Yag (wavelength 1060 nm) which can be applied with external beamor a contact tip. The laser’s clinical effect relies on localized tissue vaporizationand thermal necrosis with subsequent tissue sloughing. Laser ablation is mosteffective when used in conjunction with prior dilatation and snare cauterydebridement [45]. Tumors should be treated in retrograde fashion, i.e. bottom-to-top. Laser therapy is particularly effective when used to treat overgrowth oftumor around stents, short segment, especially proximal tumors, and anastom-otic recurrences. Laser treatment is not appropriate for tumors with severeextrinsic compression, submucosal tumors, tumors with large gastric com-ponents, and very long (> 8 cm) and angulated tumors. Treatments usuallyneed to be repeated to be effective and the most important single factor regard-ing avoiding complications is the experience of the operator. Functional success in tumor palliation has been reported in 75–80% of cases [13,45] andlaser therapy can be combined with treatment with photodynamic therapy,brachytherapy, or esophageal stents.
Laser treatment is seeing less application following the introduction of theexpandable coated metallic stents. Recent studies have suggested these stentsare more successful than laser therapy alone for the palliation of malignantdysphagia [46].
Diagnosis and treatment of perforation following laser therapyPerforation is the most common complication requiring surgical attention. It
Figure 13.6 (a) Chest radiograph showing a left pleural effusion in a 60-year-old woman followingpneumatic dilatation for achalasia. (b) Lateral radiograph in the same patient showing extraluminalcontrast and subdiaphragmatic air (see arrow). Following the insertion of a left chest tube, thispatient was operated on transabdominally with primary repair of the perforation, esophagealmyotomy, and Toupet repair. This patient went on to have an uneventful recovery.
(a) (b)
212 Chapter 13
is reported to occur in between 4% and 6% of cases [47–49], and is the singlemost common cause of mortality associated with laser treatment [48]. Since the majority of these patients are not surgical candidates, most of the patientswho sustain perforations associated with laser therapy will be treated support-ively [33], or with expandable coated wire mesh stents [50,51]. These stents arehighly successful in providing the dual role of sealing the perforation andmaintaining luminal patency. Occasionally, multiple stents are required [34]and separate decisions must be made regarding the requirement of surgical orradiological mediastinal or pleural drainage.
Esophageal sclerotherapy
Sclerotherapy for esophageal varices secondary to portal hypertension hasimproved and simplified the treatment of these complex patients [52]. With theintroduction of endoscopic variceal ligation, and transjugular intrahepaticportal systemic shunting (TIPS), it has seen somewhat less application over the last 4–5 years. Sclerotherapy works by injecting a sclerosing agent (e.g.sodium tetradecyl sulfate, sodium morrhuate, or ethanolamine) into or aroundthe esophageal varices to promote an intense inflammatory reaction whichresults in variceal fibrosis and obliteration. Most injections are made in the distal one-third of the esophagus, more proximal varices being located belowthe muscularis mucosa, making injection more difficult and increasing thepotential for complications.
Sclerotherapy is usually not initiated prior to the onset of bleeding. Whentreatments are applied acutely at the time of hemorrhage, they are usuallyrepeated three to six times until variceal obliteration. Meta-analysis of com-bined, randomized, controlled trials show significant benefit of sclerotherapyover medical treatment in controlling initial bleeding, and reducing early re-bleeding rates, while suggesting the possibility of a decreased mortality [53].
Diagnosis and treatment of complications associated with variceal sclerotherapyComplication rates of 20–40% and procedure-related mortality rates of 1–5%following sclerotherapy are documented. These complications include eso-phageal ulceration, stenosis, intramural hematoma, and perforation. Perforationis the most devastating complication and the one most likely to come to theattention of thoracic surgeons. It is often associated with pre-existing eso-phageal ulceration and has been reported in up to 6.5% of patients undergoingsclerotherapy treatment. Some of the patients can be managed non-operatively;however, due to the fact that chest pain is often associated with sclerotherapyinjections, it is not uncommon for the diagnosis of esophageal perforation inthese patients to be delayed, resulting in the patients presenting with severemediastinitis, abscess, empyema, or even esophagorespiratory fistula.
Some of the most challenging perforations I have encountered have been in these otherwise medically compromised patients who present late with perforations following sclerotherapy. Many times, these patients are referred
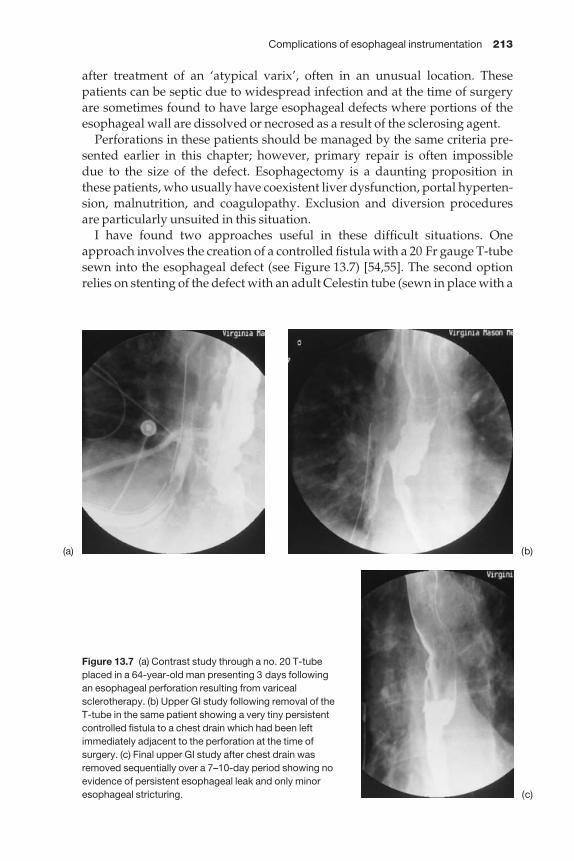
Complications of esophageal instrumentation 213
after treatment of an ‘atypical varix’, often in an unusual location. Thesepatients can be septic due to widespread infection and at the time of surgeryare sometimes found to have large esophageal defects where portions of theesophageal wall are dissolved or necrosed as a result of the sclerosing agent.
Perforations in these patients should be managed by the same criteria pre-sented earlier in this chapter; however, primary repair is often impossible due to the size of the defect. Esophagectomy is a daunting proposition in these patients, who usually have coexistent liver dysfunction, portal hyperten-sion, malnutrition, and coagulopathy. Exclusion and diversion procedures are particularly unsuited in this situation.
I have found two approaches useful in these difficult situations. Oneapproach involves the creation of a controlled fistula with a 20 Fr gauge T-tubesewn into the esophageal defect (see Figure 13.7) [54,55]. The second optionrelies on stenting of the defect with an adult Celestin tube (sewn in place with a
Figure 13.7 (a) Contrast study through a no. 20 T-tubeplaced in a 64-year-old man presenting 3 days following an esophageal perforation resulting from varicealsclerotherapy. (b) Upper GI study following removal of theT-tube in the same patient showing a very tiny persistentcontrolled fistula to a chest drain which had been leftimmediately adjacent to the perforation at the time ofsurgery. (c) Final upper GI study after chest drain wasremoved sequentially over a 7–10-day period showing noevidence of persistent esophageal leak and only minoresophageal stricturing.
(a) (b)
(c)
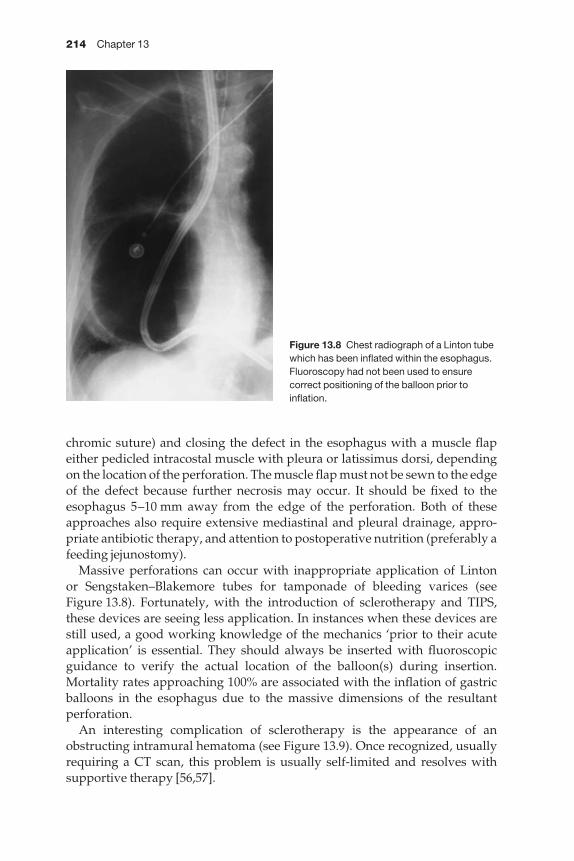
214 Chapter 13
chromic suture) and closing the defect in the esophagus with a muscle flapeither pedicled intracostal muscle with pleura or latissimus dorsi, dependingon the location of the perforation. The muscle flap must not be sewn to the edgeof the defect because further necrosis may occur. It should be fixed to theesophagus 5–10 mm away from the edge of the perforation. Both of theseapproaches also require extensive mediastinal and pleural drainage, appro-priate antibiotic therapy, and attention to postoperative nutrition (preferably afeeding jejunostomy).
Massive perforations can occur with inappropriate application of Linton or Sengstaken–Blakemore tubes for tamponade of bleeding varices (see Figure 13.8). Fortunately, with the introduction of sclerotherapy and TIPS,these devices are seeing less application. In instances when these devices are still used, a good working knowledge of the mechanics ‘prior to their acuteapplication’ is essential. They should always be inserted with fluoroscopicguidance to verify the actual location of the balloon(s) during insertion.Mortality rates approaching 100% are associated with the inflation of gastricballoons in the esophagus due to the massive dimensions of the resultant perforation.
An interesting complication of sclerotherapy is the appearance of anobstructing intramural hematoma (see Figure 13.9). Once recognized, usuallyrequiring a CT scan, this problem is usually self-limited and resolves with supportive therapy [56,57].
Figure 13.8 Chest radiograph of a Linton tubewhich has been inflated within the esophagus.Fluoroscopy had not been used to ensurecorrect positioning of the balloon prior toinflation.
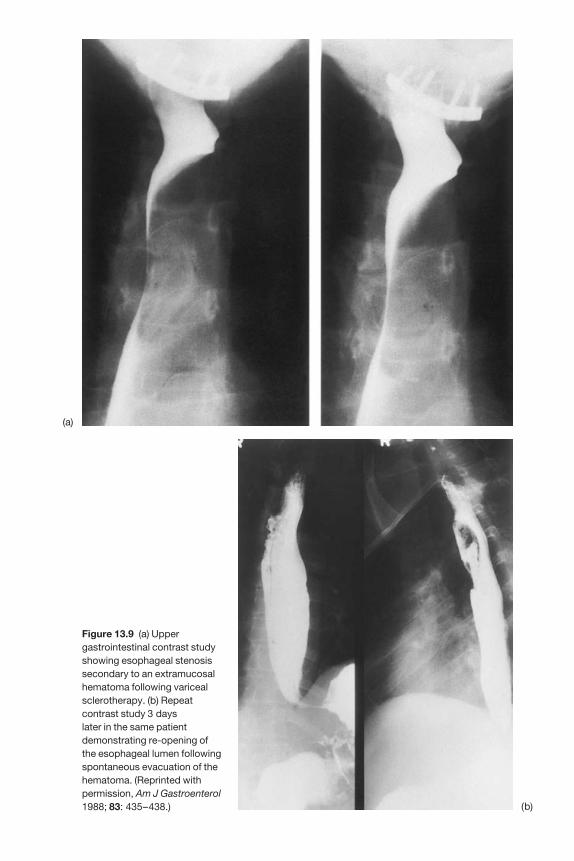
Figure 13.9 (a) Uppergastrointestinal contrast studyshowing esophageal stenosissecondary to an extramucosalhematoma following varicealsclerotherapy. (b) Repeatcontrast study 3 days later in the same patientdemonstrating re-opening ofthe esophageal lumen followingspontaneous evacuation of thehematoma. (Reprinted withpermission, Am J Gastroenterol1988; 83: 435–438.)
(a)
(b)

216 Chapter 13
Esophageal stents
Various types of endoscopic, radiological, or surgically placed esophagealprostheses have been utilized for the palliation of obstructing esophagealmalignancies, and more recently to treat malignant esophagorespiratory fistu-las [50]. Endoscopically placed stents originally were limited to conventionalplastic prostheses, such as the Wilson-Cook prosthesis (Wilson-Cook), theAtkinson tube (Key Med, Ltd, Southend, UK), or Celestin tube (Medoc, Ltd,Tetbury, UK) (see Figure 13.10). Recently, a new generation of expandablewire mesh stents, such as the Z-stent (Gianturco; Wilson-Cook, WinstonSalem, NC), Wallstent (Schneider, Inc., Minneapolis, MN, USA), Esophacoil(InStent; Eden Prairie, MN, USA), and Nitinol Ultraflex (Microvasive, Inc.,Natick, MA) has been introduced (see Figure 13.11). Most of the newer stentshave a silastic coating to help impede tumor ingrowth and facilitate fistulaocclusion. The exceptions are the Ultraflex I type stent, which is a tightlywoven mesh stent, and the Esophacoil, which is made from a single flattenedwire shaped into a tight coil.
These newer, expandable stents are reputed to be smaller and easier toinsert, and potentially more effective and safer to use. This statement may or may not be true and will be refuted or confirmed with more experience,additional comparative trials, and future technological advances.
Conventional plastic stents can be successfully placed in over 90% of cases[50,58]. These stents usually require initial dilatation up to a range of 45–54 Frgauge to facilitate insertion. Alternatively, the expandable stents are mountedon delivery systems as small as 18 Fr gauge, thereby requiring less preinser-tional dilatation. Although a review in our institution suggests that conven-tional and expandable prostheses are comparable with respect to dysphagiarelief, fistula occlusion, and instance of complications [50], two randomized,
Figure 13.10 Examples of conventional plastic prostheses: Atkinson tube (above), Wilson-Cookprosthesis (below).
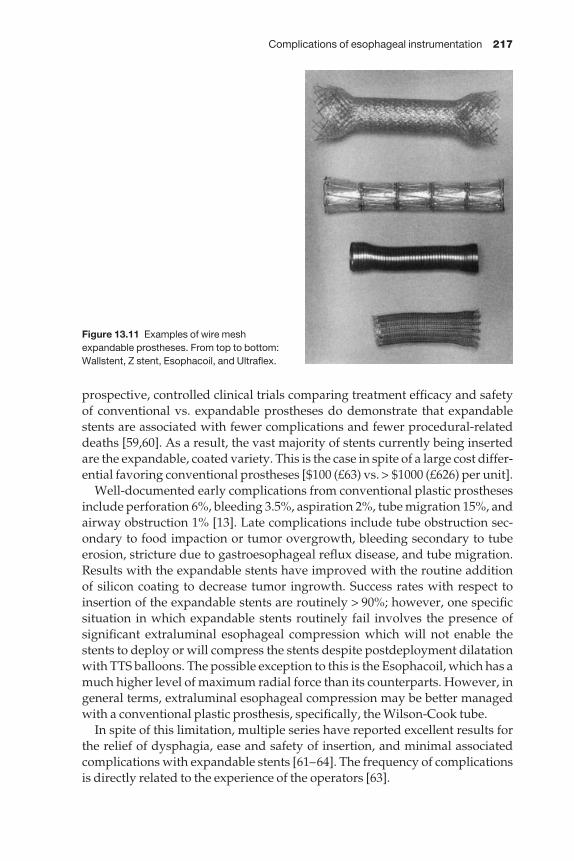
Complications of esophageal instrumentation 217
prospective, controlled clinical trials comparing treatment efficacy and safetyof conventional vs. expandable prostheses do demonstrate that expandablestents are associated with fewer complications and fewer procedural-relateddeaths [59,60]. As a result, the vast majority of stents currently being insertedare the expandable, coated variety. This is the case in spite of a large cost differ-ential favoring conventional prostheses [$100 (£63) vs. > $1000 (£626) per unit].
Well-documented early complications from conventional plastic prosthesesinclude perforation 6%, bleeding 3.5%, aspiration 2%, tube migration 15%, andairway obstruction 1% [13]. Late complications include tube obstruction sec-ondary to food impaction or tumor overgrowth, bleeding secondary to tubeerosion, stricture due to gastroesophageal reflux disease, and tube migration.Results with the expandable stents have improved with the routine addition of silicon coating to decrease tumor ingrowth. Success rates with respect toinsertion of the expandable stents are routinely > 90%; however, one specificsituation in which expandable stents routinely fail involves the presence ofsignificant extraluminal esophageal compression which will not enable thestents to deploy or will compress the stents despite postdeployment dilatationwith TTS balloons. The possible exception to this is the Esophacoil, which has amuch higher level of maximum radial force than its counterparts. However, ingeneral terms, extraluminal esophageal compression may be better managedwith a conventional plastic prosthesis, specifically, the Wilson-Cook tube.
In spite of this limitation, multiple series have reported excellent results forthe relief of dysphagia, ease and safety of insertion, and minimal associatedcomplications with expandable stents [61–64]. The frequency of complicationsis directly related to the experience of the operators [63].
Figure 13.11 Examples of wire meshexpandable prostheses. From top to bottom:Wallstent, Z stent, Esophacoil, and Ultraflex.
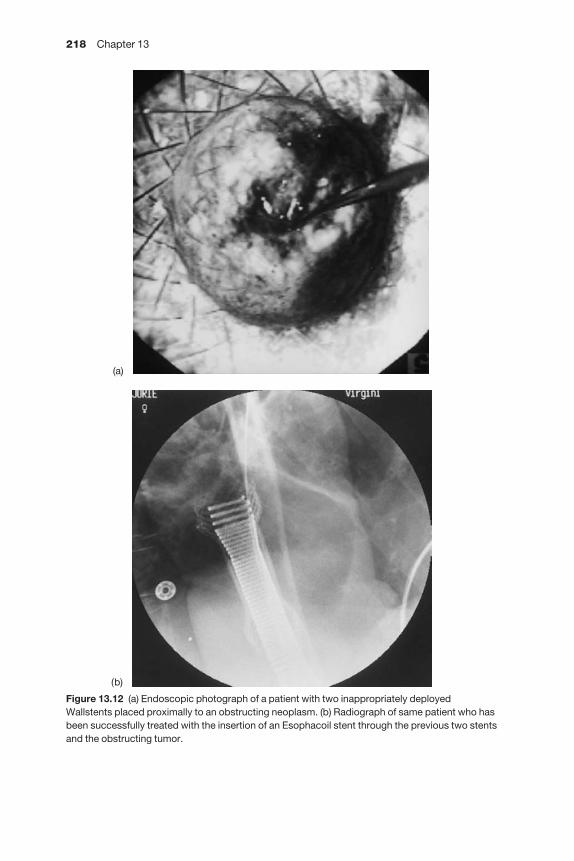
218 Chapter 13
Figure 13.12 (a) Endoscopic photograph of a patient with two inappropriately deployedWallstents placed proximally to an obstructing neoplasm. (b) Radiograph of same patient who hasbeen successfully treated with the insertion of an Esophacoil stent through the previous two stentsand the obstructing tumor.
(a)
(b)

Complications of esophageal instrumentation 219
Diagnosis and treatment of complications associated withexpandable, coated esophageal stentsPerforationThe mortality rates of perforation associated with stent insertion are reportedto be as high as 50% [61]. However, the incidence of perforation associatedwith these stents is reported to be as low as 0–2% [63–65]. This fairly low rate isattributed to the fact that expandable stents require significantly less preinser-tional dilatation than the rigid devices. Since these stents are usually insertedin patients who, for a variety of reasons, are not considered appropriate sur-gical candidates, surgical decision making following perforation is usuallylimited to whether additional stents will be required to seal the perforationand a decision regarding the placement of thoracic and abdominal drains.
Stent misplacementDue to the ease of insertion of the wire mesh, expandable stents, larger com-ponents of the radiological, GI, and surgical specialties are utilizing thesestents, in some cases with only limited experience of stent placement or patientselection. As a result, the incidence of inappropriate stent placement is vari-ously reported between 5% and 13% [63,65]. With the exception of the Z-typestents, the vast majority of expandable stents will shorten between 20% and 50% when deployed. This must be taken into account when placing theprosthesis and choosing the appropriate length. Placement of these stentsshould always be under fluoroscopic guidance after exact definition of theproximal and distal tumor margins with either mucosal contrast injection orexternally placed radiopaque markers. Once deployment has been initiated,only the Nitinol Ultraflex, Z stents, and the Wallstent can be repositioned.Most importantly, if inappropriately fully deployed or damaged, the majorityof these stents cannot be safely removed endoscopically. Paradoxically, the situation is usually salvaged by the insertion of additional stents (see Figure13.12) [34,66,67]. The Esophacoil stent has been presented as a design whichcan be removed when it is inappropriately placed or has migrated. We havehad the same experience reported by Segalin [68] where these devices haveproduced major esophageal injuries when the coiled stents are removed bypulling one end of the coiled wire out of the patient’s mouth (see Figure 13.13).When removed endoscopically, these stents should be removed as a wholeunit, preferably utilizing an overtube.
Stent migrationThe incidence of wire mesh, expandable stents migrating following insertion is in the range of 0–27% [19,50,63,65]. The incidence of this problem can bedecreased by ensuring full deployment, which often requires inflating TTS balloons within the stent at the time of insertion. Particular care must be ex-hibited with stents placed across the EG junction. The majority of these stentsmust be placed within the tumor and the esophagus to minimize the potentialfor distal displacement. Recently, reports have suggested that the Ultraflex

220 Chapter 13
stent has the greatest tendency for incomplete deployment and the need formore complex interventions [69,70].
While conventional plastic prostheses could be left in the stomach when distal migration occurs, this is clearly not the case with the new expandablestents. Small-bowel obstruction and perforation have been reported [71].These stents must be removed, either endoscopically or surgically. Safe endo-scopic removal can often be facilitated with the use of an overtube (see foreignbody extraction) (see Figure 13.14).
Tumor overgrowthOvergrowth of expandable stents with tumor was a much greater problemprior to the routine coating of many of these appliances with silicone.Although overgrowth is still noted in up to 36% of patients [70], it can usuallybe effectively managed with laser [13], snare electrocautery, photodynamictherapy (PDT) [72], or the insertion of additional stents (see Figure 13.15) [70].
Airway obstructionObstruction of the tracheal or proximal bronchial airway can occasionallyoccur with stent deployment, the risk being especially high in very proximaltumors. This problem can be identified prior to stent deployment by initial
Figure 13.13 Endoscopic photograph demonstrating an extensive mucosal tear involving theentire length of the esophagus following attempted removal of a misplaced Esophacoil stent.
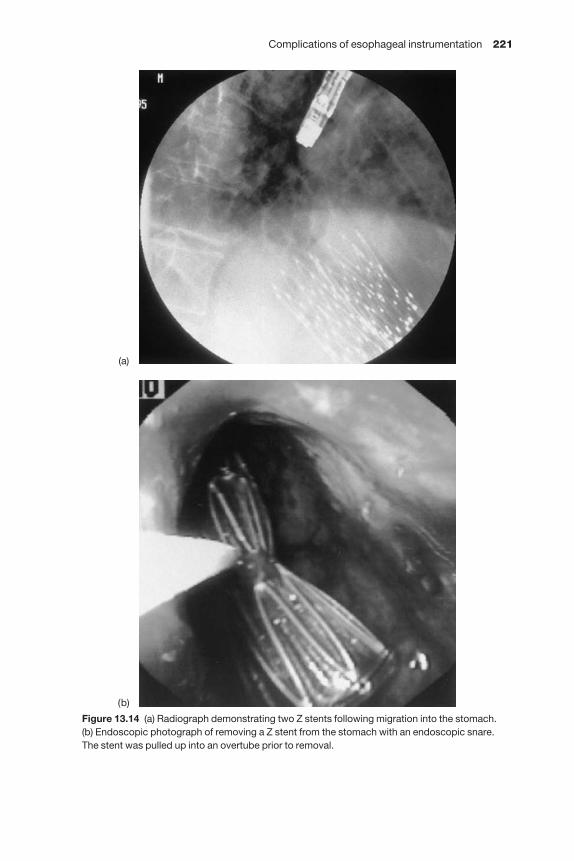
Complications of esophageal instrumentation 221
Figure 13.14 (a) Radiograph demonstrating two Z stents following migration into the stomach. (b) Endoscopic photograph of removing a Z stent from the stomach with an endoscopic snare.The stent was pulled up into an overtube prior to removal.
(b)
(a)

222 Chapter 13
prolonged dilatation with a polyvinyl dilatator or a TTS balloon prior to stentdeployment. If concern still exists, then one of the stents that can be sub-sequently removed, specifically the Ultraflex or Esophacoil, should be con-sidered in these patients. Particular care must be exhibited when deployingstents near the upper esophageal sphincter because life-threatening airwaycompromise has been documented [73].
Pressure necrosisPressure necrosis is a late complication of insertion of expandable stents and is often associated with acute angulation at the point of stenosis. The mostcommon manifestation of pressure necrosis is chest pain. Bleeding is a com-mon sequelae which can be massive, indicating erosion into a major vascularstructure [65,66,74–77]. The frequency of reports of major exsanguinatinghemorrhage with these new stents is worrisome. As a result, any indication ofminor upper GI bleeding should be investigated endoscopically and if majorulceration or erosion is identified, every effort should be made to remove or modify the offending stent. Expandable stents have also been seen to erodeinto other major mediastinal structures, such as pericardium [78], and the tracheal-bronchial tree [79,80].
Pressure necrosis and significant bleeding may increase when patientsundergo radiation or chemoradiation therapy following stent placement [81].However, the risk of complications does not seem to be higher when stents areplaced in patients who have completed radiation therapy or chemotherapyprior to stent placement [66,82].
Figure 13.15 Endoscopic photograph showing a Z stent being fully deployed with a through-the-scope (TTS) balloon inside an Ultraflex stent which had become obstructedsecondary to tumor ingrowth.
Complications of esophageal instrumentation 223
Expandable wire mesh stents in benign diseaseThe ease with which these stents can be inserted makes it tempting to applythis relatively new technology to patients with refractory dysphagia second-ary to benign disease. An increasing number of anecdotal reports is appearingin the literature citing experience with expandable stents in situations otherthan end-stage esophageal malignancy. As discussed, the incidence of majorcomplications with these stents is not insignificant. Major complications inpatients with benign disease such as perforation and death are reported [83],with some series noting complication rates of 100% [84]. Utilization of thesestents in patients with benign disease outside of an Institutional Review Board(IRB)-approved clinical trial is condemned.
Avoidance and treatment of complications associated withesophagogastric foreign body removal
Presence of foreign bodies in the upper gastrointestinal tract is a very commonproblem involving a wide and sometimes unbelievable variety of items. Upperendoscopy is the primary tool of investigation and treatment. The majority ofcomplications involve misadventure during attempted foreign body extrac-tion. The most important initial decision involves which foreign bodies requireremoval and which are too large and dangerous to be removed endoscopicallyand therefore require an initial surgical approach.
Approximately 70% of foreign bodies will pass through the GI tract spon-taneously and only 1% will result in perforation. Evidence of perforation at thetime of discovery of foreign bodies should be responded to with the decisionprofile outlined previously in this chapter. Patients who are prisoners, psy-chotic, or mentally retarded are at higher risk for having multiple foreign bodies.
The reasons to remove a foreign body from the upper GI tract can be sum-marized as: (i) esophageal impaction (small and smooth objects impacted inthe lower esophagus can undergo a short observation period of 12 h or less tosee if they will spontaneously pass; however, no foreign body should remainimpacted in the esophagus for greater than 24 h [85]); (ii) evidence of airwaycompromise; (iii) sharp or pointed objects (e.g. toothpicks, safety pins, andwires) even when they pass into the stomach; (iv) foreign bodies > 6 cm in children and 10 cm in adults [86,87]; (v) all button, disk, or regular batteries(disk batteries can result in esophageal perforation in a remarkably shortperiod of time when impacted in the esophagus); and (vi) packets of cocaine ineither condoms, balloons, or layers of tubular latex (these should be removedsurgically because endoscopic rupture during extraction can be fatal). Allpatients experiencing esophageal bolus obstruction require upper endoscopy,even when the bolus is seen to spontaneously pass. This is due to the high incidence (70%) of underlying disease, i.e. peptic stricture, rings, etc. [88,89]which should be identified and appropriately treated.
Up to 20–25 years ago, the routine approach to esophageal and gastric foreign bodies was removal with rigid esophagoscopy under general anesthesia.

224 Chapter 13
However, with the advent of flexible upper endoscopy which now providesbetter visibility, maneuverability, and safety, the requirement for rigid eso-phagoscopy has virtually disappeared. Success rates for endoscopic extrac-tion of foreign bodies are reported to range between 84% and 99% [88,89]. An initial surgical approach is usually reserved for very large foreign bodies,cocaine packets, and patients presenting with complications at the time of foreign body diagnosis.
The endoscopic approach to foreign body extraction usually involves a double lumen endoscope in association with an armamentarium of forceps,graspers, and snares. Some recent snares have even been fitted with a net to facilitate the removal of round or oval foreign bodies. The single mostimportant piece of equipment for the removal of sharp or irregular objects is the esophageal overtube (see Figure 13.16). This flexible plastic tube fits overthe endoscope and subsequently slides down the scope when it is in place inthe esophagus or stomach. Sharp foreign bodies can be pulled up into the tubeprior to removal. In addition, the tube can be left in place to facilitate the scopebeing passed repeatedly into the esophagus or stomach, thereby avoidingrepetitive instrumentation of the pharynx and hypopharynx for piecemealremoval of meat boluses or removal of multiple foreign bodies [90]. If the for-eign body is radiopaque, a plan for removal and the appropriate instrumenta-tion should be assembled prior to beginning the endoscopy. Intravenousglucagon will often aid removal by decreasing gastroduodenal motility.
Elongated foreign bodies should be removed by grasping one end and aligning the object with the long axis of the esophagus during removal. Sharpobjects should be removed with the point trailing, or as with irregular or spicu-lated foreign bodies, e.g. stents (see Figure 13.14) can be removed with the aid of an overtube. Special care must be used in passing overtubes through
Figure 13.16 Examples of long (esophageal) and short (gastric) esophageal overtubes.

Complications of esophageal instrumentation 225
the cervical esophagus, especially in elderly patients with osteophytes, due tothe increased risk of perforation.
Blind attempts at pushing a meat bolus through a distal obstruction ofunknown etiology carries an increased risk of perforation [88,91]. However, if the nature of the distal obstruction can be assessed endoscopically, meatboluses can often be broken up with snares and safely pushed into the stomach. Dissolving meat bolus obstruction with papain (meat tenderizer) hasbeen used with success; however, papain produces an enzymatic action on theesophageal wall and deaths have been reported with this approach [92,93].
The incidence of perforations associated with foreign bodies and theirextraction has been reported between 0 and 73% [88,89,94]. Extraction rates are lower and perforation rates higher (23%) in cases of deliberate ingestion[95]. Inability to extract a foreign body endoscopically will require a surgicalapproach. For objects that are sharp or irregular in configuration, and becomeimpacted or impaled in the lower esophagus, a transabdominal approach withtransgastric digital manipulation from below, gentle palpation from outsidethe esophagus, in conjunction with continued endoscopy will virtually alwaysbe successful. Careful subsequent inspection, both endoscopically and fromthe outside of the esophagus and stomach (often submerging the EG junc-tion in saline with endoscopic air insufflation) to identify any occult site of perforation is important following foreign body removal. If perforation is identified, it should be managed with the principles previously outlined.Primary repair will almost always be feasible, keeping in mind that the eti-ology of the esophageal obstruction may alter the approach used in repairingthe perforation.
References
1 Carey WD. Indications, contraindications and complications of upper gastrointestinalendoscopy. In: Sivak MV, ed. Gastroenterologic Endoscopy. Philadelphia: Saunders, 1987;296–306.
2 Mandelstam P, Sugawa C, Silvis SE et al. Complications associated with esophagogastricduodenoscopy and with esophageal dilation. Gastrointest Endosc 1976; 23: 16–19.
3 Nostrant TT, Nandi PS. Esophageal dilation. The Gastroenterologist 1998; 6: 5–15.4 McClave SA, Brady PG, Wright RA et al. Does fluoroscopic guidance for Maloney
esophageal dilation impact on the clinical endpoint of therapy: relief of dysphagia andachievement of luminal patency. Gastrointest Endosc 1996; 43: 93–97.
5 McLean GK, LeVeen RF. Shear stress in the performance of esophageal dilation: compar-ison of balloon dilation and bougienage. Radiology 1989; 172: 983–986.
6 Cox JG, Winter RK, Maslin SC et al. Balloon or bougie for dilation of benign oesophagealstricture? Gut 1988; 29: 1741–1747.
7 Clouse RE. Complications of endoscopic gastrointestinal dilation techniques. GastrointestEndosc Clin North Am 1996; 6: 323–341.
8 Saeed ZA, Winchester CB, Ferro PC et al. Prospective randomized comparison ofpolyvinyl bougies and through-the-scope balloons for dilation of peptic strictures of theesophagus. Gastrointest Endosc 1995; 41: 189–195.
226 Chapter 13
9 Mohandas KM, Santhi Swaroop V, Desai DC. Marked wire-guided esophageal dilationand the need for fluoroscopy (letter). Gastrointest Endosc 1992; 38: 634–635.
10 Marshall JB, Afridi SA, King PD et al. Esophageal dilation with polyvinyl (American) dilators over a marked guidewire: practice and safety at one center over a five-year period.Am G Gastroenterol 1996; 91: 1503–1506.
11 Kadakia SC, Parker A, Carrougher JB. Esophagal dilation with polyvinyl bougies using a marked guidewire without the aid of fluoroscopy: an update. Am J Gastroenterol 1996;88: 1381–1386.
12 Silvis SE, Nebel O, Rogers G. Endoscopic complications. Results of the 1974 AmericanSociety for Gastrointestinal Endoscopy Survey. JAMA 1976; 235: 928–930.
13 Reed CE. Pitfalls and complications of esophageal prosthesis, laser therapy and dilation.Chest Surg Clin North Am 1997; 7: 623–636.
14 Wychulis AR, Fontana RS, Payne WS. Instrumental perforation of the esophagus. Chest1969; 55: 184–189.
15 Foley MJ, Ghahremani GG, Rogers LF. Reappraisal of contrast media used to detect uppergastrointestinal perforation. Radiology 1982; 144: 231–237.
16 Phillips LG, Cumingham J. Esophageal perforation. Radiol Clin North Am 1984; 22:1607–1613.
17 Backer CL, LoCicero J 3rd, Hartz RS et al. Computed tomography in patients withesophageal perforation. Chest 1990; 98: 1078–1080.
18 Endicott JN, Molony TB, Campbell G et al. Esophageal perforations: the role of computer-ized tomography in diagnosis and management decisions. Laryngoscope 1986; 96: 751–757.
19 Cameron JL, Kieffer RF, Hendrix TR et al. Selective nonoperative management of con-tained intrathoracic esophageal disruptions. Ann Thorac Surg 1979; 27: 404–408.
20 Jones WG, Ginsberg RJ. Esophageal perforation: a continuing challenge. Ann Thorac Surg1992; 53: 534–543.
21 Nesbitt JC, Sawyers JL. Surgical management of esophageal perforation. Am Surg 1987; 53:183–191.
22 Whyte RI, Iannettoni MD, Orringer MB. Intrathoracic esophageal perforation. J ThoracCardiovasc Surg 1995; 109: 140–146.
23 Reeder LB, DeFilippi VJ, Ferguson MK. Current results of therapy for esophageal perfora-tion. Am J Surg 1995; 169: 615–617.
24 Wang N, Razzouk AJ, Safavi A et al. Delayed primary repair of intrathoracic esophagealperforation: is it safe? J Thorac Cardiovasc Surg 1996; 111: 114–122.
25 Gawrychowski J, Rokicki W, Dziedzic M. Observations related to causes and treatment ofiatrogenic esophageal injury. Wiadomosci Lekarskie 1997; 1: 254–258.
26 Grillo HC, Wilkins EW. Esophageal repair following late diagnosis of intrathoracic per-foration. Ann Thorac Surg 1975; 20: 387–399.
27 Moghissi K, Pender D. Instrumental perforations of the esophagus and their management.Thorax 1988; 43: 642–646.
28 Matthews HR, Mitchell IM, McGuigan JA. Emergency subtotal oesophagectomy. Br J Surg1989; 76: 918–920.
29 Yeo CJ, Lillemoe KD, Klein AS et al. Treatment of instrumental perforation of esophagealmalignancy by transhiatal esophagectomy. Arch Surg 1988; 123: 1016–1018.
30 Iannettoni MD, Vlessis AA, Whyte RI et al. Functional outcome after surgical treatment ofesophageal perforation. Ann Thorac Surg 1997; 64: 1606–1609.
31 Saabye J, Nielson HO, Anderson K. Long-term observation following perforation andrupture of the esophagus. Scand J Thorac Cardiovasc Surg 1988; 22: 79–80.
32 Salo JA, Isolauri JO, Heikkilä LJ et al. Management of delayed esophageal perforation withmediastinal sepsis. J Thorac Cardiovasc Surg 1993; 106: 1088–1091.
Complications of esophageal instrumentation 227
33 Bisgaard T, Wojdemann M, Heindorff H et al. Nonsurgical treatment of esophageal per-forations after endoscopic palliation in advanced esophageal cancer. Endoscopy 1997; 29:155–159.
34 Watkinson A, Ellul J, Entwisle K et al. Plastic-covered metallic endoprostheses in the man-agement of oesophageal perforation in patients with oesophageal carcinoma. Clin Radiol1995; 50: 304–309.
35 Bethge N, Kleist DV, Vakil N. Treatment of esophageal perforation with a coveredexpandable metal stent. Gastrointest Endosc 1996; 43: 161–163.
36 Nicholson AA, Royston CM, Wedgewood K et al. Palliation of malignant oesophageal per-foration and proximal oesophageal malignant dysphagia with covered metal stents. ClinRadiol 1995; 50: 11–14.
37 Reynolds JC, Parkman HP. Achalasia. Gastroenterol Clin North Am 1989; 18: 233–255.38 Eckardt VF, Aignherr C, Bernhard G. Predictors of outcome in patients with achalasia
treated with pneumostatic dilation. Gastroenterology 1992; 103: 1732–1738.39 Parkman HP, Reynolds JC, Ouyang A et al. Pneumatic dilation of esophagomyotomy
treatment for idiopathic achalasia: clinical outcomes and cost analysis. Dig Dis Sci 1993; 38:75–85.
40 Pasricha PJ, Huang RL, Rai R et al. Achalasia and other motor diseases. In: DiMarino AJ,Benjamin SB, eds. Gastrointestinal Disease: An Endoscopic Approach. Malden MA: Blackwell,1997; 219–240.
41 Abid S, Champion G, Richter JE et al. Treatment of achalasia: the best of both worlds. Am JGastroenterol 1994; 89: 979–985.
42 Molina EG, Stollman N, Grauer L et al. Conservative management of esophageal non-transmural tears after pneumatic dilation for achalasia. Am J Gastroenterol 1995; 91: 15–18.
43 Ferguson MK, Reeder LB, Olak J. Results of myotomy and partial fundoplication afterpneumatic dilation for achalasia. Ann Thorac Surg 1996; 62: 327–330.
44 Peters JH, Kauer WK, Crookes PF. Esophageal resection with colon interposition for end-stage achalasia. Arch Surg 1995; 130: 632–636.
45 Low DE, Pagliero MK. Palliative treatment of carcinoma of the esophagus. In: Bauer AE,ed. Glenn’s Thoracic and Cardiovascular Surgery, 6th edn. Stamford CT: Appleton & Lange,1996; 939–950.
46 Adam A, Ellul J, Watkinson AF et al. Palliation of inoperable esophageal carcinoma: aprospective randomized trial of laser therapy and stent placement. Radiology 1997; 202:344–348.
47 Tyrrell MR, Trotter GA, Adam A et al. Incidence and management of laser-associatedoesophageal perforation. Br J Surg 1995; 82: 1257–1258.
48 Ell C, Demling L. Laser therapy of tumor stenoses in the upper gastrointestinal tract: aninternational inquiry. Lasers Surg Med 1987; 7: 491–496.
49 Fleischer D. The Washington Symposium on Endoscopic Laser Therapy. GastrointestEndosc 1985; 31: 387–400.
50 Low DE, Kozarek RA. Comparison of conventional and wire mesh expandable prosthesesand surgical bypass in patients with malignant esophagorespiratory fistulas. Ann ThoracSurg 1998; 65: 919–923.
51 Weigert H, Neuhaus H, Rosch T et al. Treatment of esophagorespiratory fistulas with silicone-coated self-expanding metal stents. Gastrointest Endosc 1995; 41: 490–496.
52 Low DE, Kozarek RA, Ball TJ et al. Endoscopic vascular sclerotherapy as primary treat-ment for bleeding esophageal varices. J Clin Gastroenterol 1989; 11: 253–259.
53 Trudeau W, Kotrila W. Gastrointestinal manifestations of portal hypertension. In:Dimarino AJ, Benjamin SB, eds. Gastrointestinal Disease: An Endoscopic Approach. Malden,MA: Blackwell, 1997; 424–445.
228 Chapter 13
54 Andrade-Alegre R. T-tube intubation in the management of late traumatic esophagealperforations: case report. J Trauma 1994; 37: 131–132.
55 Naylor AR, Walker WS, Dark J. T tube intubation in the management of seriously illpatients with oesophagopleural fistulae. Br J Surg 1990; 77: 40–42.
56 Low DE, Patterson DJ. Complete esophageal obstruction secondary to dissecting intra-mural hematoma after endoscopic variceal sclerotherapy. Am J Gastroenterol 1988; 83:435–438.
57 Benoit R, Legoux JL, Serve MP et al. Obstructive intramural hematoma of the esophagusafter sclerotherapy. Presse Med 1996; 25: 1281–1284.
58 Spinelli P, Cerrai FG, Ciuffi M et al. Endoscopic stent placement for cancer of the loweresophagus and gastric cardia. Gastrointest Endosc 1994; 40: 455–457.
59 DePalma GD, DiMatteo E, Romano G et al. Plastic prostheses vs expandable metal stentsfor palliation of inoperable esophageal thoracic carcinoma. Gastrointest Endosc 1996; 43:478–482.
60 Knyrim K, Wagner HJ, Bethge N et al. A controlled trial of an expansile metal stent for palliation of esophageal obstruction due to inoperable cancer. N Engl J Med 1993; 329:1302–1307.
61 Fugger R, Niederle B, Jantsch H et al. Endoscopic tube implantation for the palliation ofmalignant esophageal stenosis. Endoscopy 1990; 22: 101–104.
62 Moores DW, Ilves R. Treatment of esophageal obstruction with covered, self-expandingesophageal Wallstents. Ann Thorac Surg 1996; 62: 963–967.
63 Ramirez FC, Dennert B, Zierer ST et al. Esophageal self-expandable metallic stentsaindica-tions, practice, techniques, and complications: results of a national survey. GastrointestEndosc 1997; 45: 360–364.
64 De Palma GD, Galloro G, Sivero L et al. Self-expanding metal stents for palliation of inop-erable carcinoma of the esophagus and gastroesophageal junction. Am J Gastroenterol 1995;90: 2140–2142.
65 Kozarek RA, Raltz S, Brugge WR et al. Prospective multicenter trial of esophageal Z-stentplacement for malignant dysphagia and tracheoesophageal fistula. Gastrointest Endosc1996; 44: 462–567.
66 Kozarek RA, Ball TJ, Brandabur JJ et al. Expandable versus conventional esophageal pros-theses: easier insertion may not preclude subsequent stent-related problems. GastrointestEndosc 1996; 43: 204–208.
67 Trowers EA, Dar S, Hodges D. Tandem expandable stent technique for a fractured nitinolstent. Gastrointest Endosc 1997; 45: 217–218.
68 Segalin A, Bonavina L, Siardi C et al. Can the expandable esophageal metal Endocoil stentbe safely removed? Endoscopy 1997; 29: 337–339.
69 Dorta G, Binek J, Blum AL et al. Comparison between esophageal Wallstent and Ultraflexstents in the treatment of malignant stenoses of the esophagus and cardia. Endoscopy 1997;29: 145–154.
70 Acunas B, Rozanes I, Akpinar S et al. Palliation of malignant esophageal strictures with self-expanding nitinol stents: drawbacks and complications. Radiology 1996; 199:648–652.
71 Henne TH, Schaeff B, Paolucci V. Small-bowel obstruction and perforation. A rare com-plication of an esophageal stent. Surg Endosc 1997; 11: 383–384.
72 Scheider DM, Siemens M, Cirocco M et al. Photodynamic therapy for the treatment oftumor ingrowth in expandable esophageal stents. Endoscopy 1997; 29: 271–274.
73 Shields SJ. Esophageal self-expandable metallic stents. Gastrointest Endosc 1997; 45:439–411.
Complications of esophageal instrumentation 229
74 Demarquay JF, Conio M, Dumas R et al. Fatal complications after placement of anesophageal self-expanding metal stent. Am J Gastroenterol 1996; 91: 178–179.
75 Grundy A, Glees JP. Aorto-oesophageal fistula: a complication of oesophageal stenting. BrJ Radiol 1997; 70: 846–849.
76 Allgaier HP, Schwacha H, Technau K et al. Fatal esophagoaortic fistula after placement ofa self-expanding metal stent in a patient with esophageal carcinoma. N Engl J Med 1997;337: 1778.
77 Siersema PD, Tan TG, Sutorius FF et al. Massive hemorrhage caused by a perforatingGianturco-Z stent resulting in an aortoesophageal fistula. Endoscopy 1997; 29: 416–420.
78 Dennert B, Ramirez FC, Sanowski RA. Pericardioesophageal fistula associated with metallic stent placement. Gastrointest Endosc 1997; 45: 82–84.
79 Hendra KP, Saukkonen JJ. Erosion of the right mainstem bronchus by an esophageal stent.Chest 1996; 110: 857–858.
80 Neustater BR, Goldberg RI. Tracheoesophageal fistula complicating placement of a self-expanding metallic tracheal stent. Am J Gastroenterol 1995; 90: 1360–1361.
81 Song HY, Do YS, Han YM et al. Covered, expandable esophageal metallic stent tubes:experience in 119 patients. Radiology 1994; 193: 689–695.
82 Raijman I, Siddique I, Lynch P. Does chemoradiation therapy increase the incidence ofcomplications with self-expanding coated stents in the management of malignantesophageal strictures? Am J Gastroenterol 1997; 92: 192–196.
83 Hramiec JE, O’Shea MA, Quinlan RM. Expandable metallic esophageal stents in benigndisease: a cause for concern. Surg Laparosc Endosc 1998; 8: 40–43.
84 Song HY, Park SI, Do YS et al. Expandable metallic stent placement in patients with benignesophageal strictures: results of long-term follow-up. Radiology 1997; 203: 131–136.
85 Ginsberg GG. Management of ingested foreign objects and food bolus impactions.Gastrointest Endosc 1995; 41: 33–38.
86 Pellerin D, Fortier-Beaulieu M, Gueguen J. The fate of swallowed foreign bodies: experi-ence of 1250 instances of subdiaphragmatic foreign bodies in children. Prog Pediatr Radiol1969; 1: 286–302.
87 Murat J, Vuillard P, Petua J et al. 108 cases of foreign bodies swallowed in the alimentarytract with the exception of the esophagus. Lyon Chirurg 1969; 65: 880–888.
88 Vizcarrondo FJ, Brady PG, Nord HJ. Foreign bodies of the upper gastrointestinal tract.Gastrointest Endosc 1983; 29: 208–210.
89 Webb WA. Management of foreign bodies of the upper gastrointestinal tract.Gastroenterology 1988; 94: 204–216.
90 Rogers BH, Kot C, Meiri S et al. An overtube for the flexible fiberoptic esophagogastroduo-denoscope. Gastrointest Endosc 1982; 28: 256–257.
91 Webb WA. Management of foreign bodies of the upper gastrointestinal tract: update.Gastrointest Endosc 1995; 41: 39–51.
92 Anderson HA, Bermatz PE, Grindley JH. Perforation of the esophagus after use of a digest-ive agent: report of a case and experimental study. Ann Otol Rhinol Laryngol 1959; 68:890–896.
93 Holsinger JW, Fuson RL, Seavy WC. Esophageal perforation following meat impactionand papain ingestion. JAMA 1968; 204: 188–189.
94 Classen M, Farthmann ER, Seifart E et al. Operative and therapeutic techniques inendoscopy. Clin Gastroenterol 1978; 7: 741–763.
95 Garcia C, Frey CR, Bodai BI. Diagnosis and management of ingested foreign bodies: a ten-year experience. Ann Emerg Med 1984; 13: 30–34.

CHAPTER 14
Complications of mediastinal surgery
Thomas A D’Amico
The mediastinum
The mediastinum is an anatomic region that is characterized by complex relationships involving components of the cardiovascular, gastrointestinal,respiratory, central nervous, and lymphatic systems. Both localized and sys-temic disorders can involve the mediastinum. A spectrum of diagnostic andtherapeutic procedures is employed in the management of patients with dis-eases that involve the mediastinum. The complex anatomic relationships ofthe mediastinum must be considered during the conduct of these proceduresand the management of the associated complications.
Mediastinal tumors and cysts occur in characteristic locations, therefore themediastinum has been subdivided for the convenience of localizing specifictypes of lesions. Some subdivide the mediastinum into four compartmentsasuperior, anterior, middle, and posterior; however, the frequency withwhich tumors occurring in the anterior or posterior mediastinum extend intothe superior mediastinum has prompted the recommendation of three sub-divisions: the anterior, middle, and posterior. The anterior compartment isdefined as the region posterior to sternum, anterior to heart and great vessels,and contains thymus, mediastinal lymph nodes, and fat. The middle medi-astinum contains the heart, pericardium, pulmonary artery and veins, ascend-ing and transverse aorta, brachiocephalic vessels, vena cava, trachea, bronchi,and lymph nodes. The posterior mediastinal compartment is posterior to heart and trachea, anterior vertebral bodies, and contains esophagus, descend-ing aorta, azygos veins, autonomic ganglia and nerves, thoracic duct, lymphnodes, and fat.
Mediastinal masses
The natural history of mediastinal masses varies: some are asymptomatic;some grow slowly and cause minimal symptoms; some are aggressive, invas-ive neoplasms that are often widely metastatic. Mediastinal masses are mostfrequently located in the anterior mediastinum (56%), with the posterior (25%)and middle mediastinum (19%) being less frequently involved [1]. Althoughdifferences in the relative incidence of neoplasms and cysts exist in someseries, the most common mediastinal masses are neurogenic tumors (20%),
230
Complications of mediastinal surgery 231
thymomas (19%), primary cysts (18%), lymphomas (13%), and germ celltumors (10%) [1].
Malignant neoplasms represent approximately 40% of mediastinal masses.Lymphomas, thymomas, germ cell tumors, primary carcinomas, and neuro-genic tumors are the most common. The relative frequency of malignancyvaries with the anatomic site. Superior mediastinal masses are more likelymalignant (59%), compared with middle mediastinal masses (29%) and pos-terior mediastinal masses (16%) [1]. Patients in the second through fourthdecades of life have a greater proportion of malignant mediastinal masses.This period corresponds to the peak incidence of lymphomas and germ cell tumors. In contrast, in the first decade of life, a mediastinal mass is mostprobably benign [1].
Clinical featuresThe clinical presentation varies from patients who are asymptomatic, to thosewith symptoms related to mechanical effects of invasion or compression, to those who have systemic symptoms. The most common symptoms are chest pain, fever, cough, and dyspnea. Symptoms related to compression orinvasion of mediastinal structures, such as the superior vena caval syndrome,Horner’s syndrome, hoarseness, and severe pain, are more indicative of amalignant histological diagnosis, although patients with a benign lesion maypresent in this manner.
Primary mediastinal masses may produce hormones or antibodies thatcause systemic symptoms, which may characterize a specific syndrome.Examples of these syndromes include Cushing’s syndrome, caused by ectopicproduction of adrenocorticotropic hormone, most frequently by carcinoidtumors; thyrotoxicosis, which is caused by a mediastinal goiter; hypertension,which may be caused by pheochromocytoma; and hypercalcemia, which maybe secondary to increased parathyroid hormone release from a mediastinalparathyroid adenoma.
DiagnosisThe goal of the diagnostic evaluation in a patient with a mediastinal mass is aprecise histological diagnosis so that optimal therapy can be performed. Thepreoperative evaluation of a patient with a mediastinal mass should achievethe following: differentiate a primary mediastinal mass from masses of othercauses that have a similar radiographic appearance; recognize associated systemic manifestations that may affect the patient’s perioperative course;evaluate for possible compression by the mass of the tracheobronchial tree,pulmonary artery, or superior vena cava; ascertain whether the mass extendsinto the spinal column; determine if the mass is a non-seminomatous germ celltumor; assess the likelihood of resectability; and identify significant factors ofmedical comorbidity and optimize overall medical condition.
The initial diagnostic intervention is a careful history and physical examina-tion. The recognition of associated systemic syndromes with many mediastinal

232 Chapter 14
neoplasms is necessary to avoid potentially serious intraoperative and post-operative complications. Although the majority of systemic syndromes are oflittle consequence regarding the planned surgical management, the associ-ation of myasthenia gravis, malignant hypertension, hypogammaglobulinemia,hypercalcemia, and thyrotoxicosis with mediastinal neoplasms may signific-antly affect the operative course and postoperative management.
The posteroanterior and lateral chest films provide important informationconcerning anatomic location and size of the tumor. Computed tomography(CT) scanning with contrast medium enhancement should be obtained rout-inely in patients with a mediastinal mass. Magnetic resonance imaging (MRI)may be more useful than CT in patients with posterior mediastinal masses, inevaluating involvement with the spinal canal, in patients with a contraindica-tion to the use of contrast dye, or in patients with surgical clips in the anatomicregion of interest. Additionally, MRI may provide information regardinginvolvement of major vascular structures and help identify a vascular abnormality.
Serologic evaluation is indicated in certain patients. Male patients with ananterior mediastinal mass in the second through fifth decades should havealpha-fetoprotein (α-FP) and beta-human chorionic gonadotropin (β-hCG)serologies obtained. A positive serology is indicative of a non-seminomatousgerm cell tumor. Patients with a mediastinal mass and a history of significanthypertension or hypermetabolism should have measurement of urinary excre-tion of vanillylmandelic acid and catecholamines. This enables the initiation ofappropriate perioperative adrenergic blockers in patients with hormonallyactive intrathoracic pheochromocytoma, paraganglioma, and neuroblastoma,limiting perioperative complications secondary to episodic catecholaminerelease. Nuclear scans using metaiodobenzylguanidine are useful in tumorlocation and in identifying sites of metastatic disease, particularly whenlocated in the middle mediastinum.
Percutaneous needle biopsy may be performed in order to obtain his-tological diagnosis, especially in patients with anterior mediastinal masses.However, poorly differentiated malignant tumors of the anterior medi-astinum, particularly thymomas, lymphomas, germ cell tumors, and primarycarcinomas, can have remarkably similar cytological and morphologicalappearances. In addition to light microscopy using special staining techniques,immunostaining techniques and electron microscopy of multiple sections ofthe tumor may be necessary to establish an accurate diagnosis. Monoclonalantibodies for surface antigens specific to a cell line of origin and for tumor-secretory products can be useful in establishing a precise diagnosis.
When needle biopsy techniques are contraindicated or do not producesufficient tissue for the histological diagnosis, more invasive procedures areoften required, such as mediastinoscopy, anterior mediastinotomy, thora-coscopy, thoracotomy, or median sternotomy. Mediastinoscopy is a usefultechnique to evaluate and biopsy lesions of the middle mediastinum. Lesions

Complications of mediastinal surgery 233
in the superior mediastinum, hilar, or paratracheal regions can be sampledusing thoracoscopy. Unresectable posterior mediastinal masses may be biopsied thoracoscopically or through a limited posterolateral thoracotomy. A representative section of the tissue obtained should be submitted for im-mediate frozen section to establish adequacy of the biopsy before closing.
Lesions that appear resectable should be completely excised. Median sternotomy and anterolateral thoracotomy provide optimal exposure forlesions in the anterior mediastinum. Middle and posterior mediastinal massesare usually excised through a posterolateral thoracotomy. Thoracoscopic pro-cedures have been used to sample and resect mediastinal lesions in carefullyselected patients [2].
Although most patients undergo surgical procedures safely, patients withlarge anterior or middle mediastinal masses, particularly children, have anincreased risk of developing severe cardiorespiratory complications duringgeneral anesthesia. Patients with posture-related dyspnea and superior venacaval syndrome are at increased risk. In patients with airway compression orsuperior vena caval obstruction, the risk of general anesthesia is markedlyincreased and attempts to obtain a histological diagnosis should be limited toneedle biopsies or open procedures done with local anesthesia. The majority ofthese lesions are malignant and unresectable.
Cervical mediastinoscopyCervical mediastinoscopy with biopsy is applicable in the evaluation of medi-astinal adenopathy associated with numerous malignant conditions, includ-ing lung cancer, lymphoma, esophageal cancer, head and neck cancer, breastcancer, melanoma, colorectal cancer, renal cell carcinoma, and mesothelioma.In addition, cervical mediastinoscopy may be used to characterize benignpathological conditions of the mediastinum, including sarcoidosis, histoplas-mosis, and tuberculosis. Mediastinoscopy may be used to biopsy primarymediastinal masses, such as thymomas, germ cell tumors, lymphomas, andmediastinal cysts.
General anesthesia is used in all patients. Because placement of the medi-astinoscope under the innominate artery may limit flow in the right carotidartery, a catheter is placed in the radial artery to monitor dampening of blood pressure, in order to avoid prolonged limitation of cerebral blood flow.Similarly, insertion of the scope over the aortic arch during extended cervicalmediastinoscopy may compress the left carotid and subclavian arteries, and apulse oximeter placed on the left upper extremity is a surrogate to monitor leftcarotid blood flow.
Sterile preparation and draping must allow for the possibility of an urgentmedian sternotomy or right anterolateral thoracotomy. A 2–3-cm incision ismade in the suprasternal notch, the platysma is incised, and the cervical strapmuscles are reflected bilaterally. There are two clearly defined mediastinal planesfor the assessment of mediastinal structures: the retrovascular pretracheal
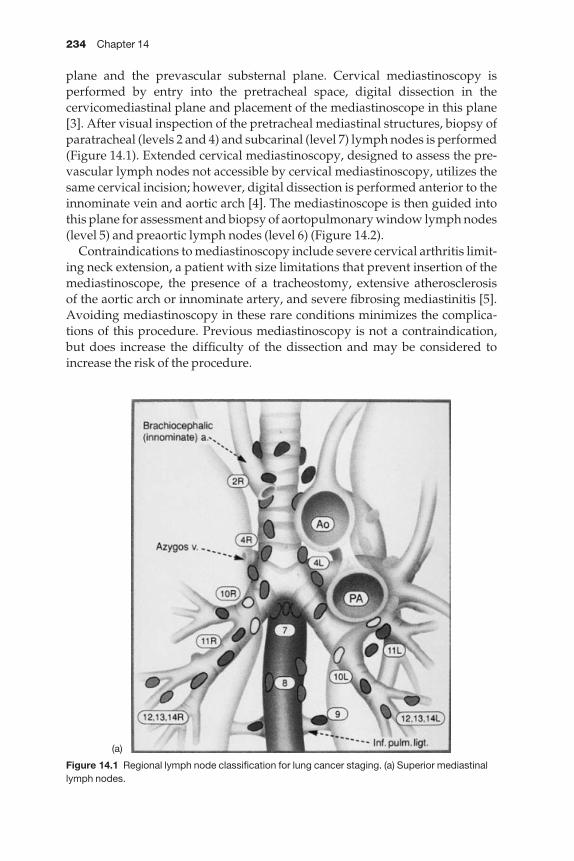
234 Chapter 14
plane and the prevascular substernal plane. Cervical mediastinoscopy is performed by entry into the pretracheal space, digital dissection in the cervicomediastinal plane and placement of the mediastinoscope in this plane[3]. After visual inspection of the pretracheal mediastinal structures, biopsy ofparatracheal (levels 2 and 4) and subcarinal (level 7) lymph nodes is performed(Figure 14.1). Extended cervical mediastinoscopy, designed to assess the pre-vascular lymph nodes not accessible by cervical mediastinoscopy, utilizes thesame cervical incision; however, digital dissection is performed anterior to theinnominate vein and aortic arch [4]. The mediastinoscope is then guided intothis plane for assessment and biopsy of aortopulmonary window lymph nodes(level 5) and preaortic lymph nodes (level 6) (Figure 14.2).
Contraindications to mediastinoscopy include severe cervical arthritis limit-ing neck extension, a patient with size limitations that prevent insertion of themediastinoscope, the presence of a tracheostomy, extensive atherosclerosis of the aortic arch or innominate artery, and severe fibrosing mediastinitis [5].Avoiding mediastinoscopy in these rare conditions minimizes the complica-tions of this procedure. Previous mediastinoscopy is not a contraindication,but does increase the difficulty of the dissection and may be considered toincrease the risk of the procedure.
Figure 14.1 Regional lymph node classification for lung cancer staging. (a) Superior mediastinallymph nodes.
(a)
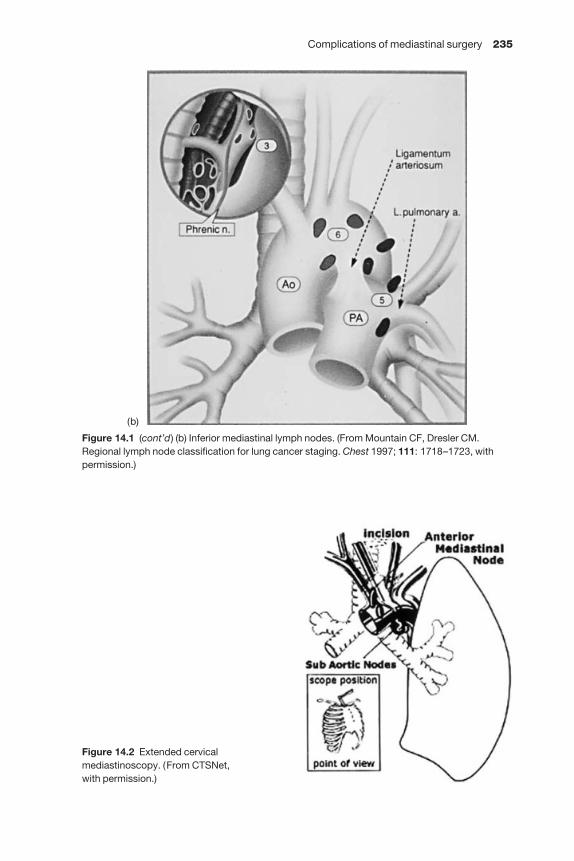
Complications of mediastinal surgery 235
Figure 14.2 Extended cervicalmediastinoscopy. (From CTSNet, with permission.)
Figure 14.1 (cont’d) (b) Inferior mediastinal lymph nodes. (From Mountain CF, Dresler CM.Regional lymph node classification for lung cancer staging. Chest 1997; 111: 1718–1723, withpermission.)
(b)

236 Chapter 14
Complications of mediastinoscopyThe morbidity and mortality associated with mediastinoscopy are low, withmost series reporting complications in approximately 0.5–4% of patients and amorality of < 0.5% [5–10]. In a series of 1000 cases at the University of Toronto,complications were reported in 2.3% of patients, with no deaths [7]. In thisseries, only three complications were considered major, including two cases of hemorrhage and one tracheal injury. In a series of 2137 patients fromWashington University, there were 12 complications (0.6%) and four deaths; ofthe four deaths, the authors attributed only one (0.05%) to mediastinoscopy[6]. The complication rate is higher in cases of repeat mediastinoscopy(approximately 7%) [11].
The most important common complication is hemorrhage. Minor bleedingis frequently encountered with routine dissection, especially in the subcarinalstation, which is supplied by bronchial arteries. Minor bleeding from smallvessels is usually controlled by direct pressure, applied with gauze packing, orprecise electrocoagulation, taking care to avoid cautery in the left paratrachealstation, which may endanger the left recurrent laryngeal nerve.
Major bleeding, defined as hemorrhage that obscures the vision through themediastinoscope, may originate from the azygos vein, innominate artery, aorta,pulmonary artery, or left atrium. The most common source is the azygos vein,which may be injured with vigorous dissection in the right paratracheal spaceor inadvertent biopsy. Biopsy-associated injury is preventable by ascertaininglymph node identity through either careful dissection or needle aspiration.
Small tears in the azygos vein may be controlled with gauze packing; moreextensive injuries must be addressed at thoracoscopy or thoracotomy. Rarely,an azygos vein injury may be controlled with a thoracoscopic clip applierthrough the mediastinoscope.
If the bleeding is temporarily controlled with packing, the cervical incision is closed and the patient turned to the left lateral decubitus position for rightthoracoscopy or thoracotomy. For patients with a resectable right-sided lungcancer, the pulmonary resection is completed at the same time. If the bleedingcan not be temporized through the mediastinoscopy incision, a right anterolat-eral thoracotomy is urgently performed for repair of the azygos vein; however,access to the azygos vein, a posterior mediastinal structure, is limited throughthis incision. Caudal retraction of the upper and middle lobes is required to visualize the site of hemorrhage; this maneuver may be facilitated by tem-porarily interrupting ventilation.
Injury to the innominate artery or aorta may occur when biopsy of firm,fibrous masses that encase the vessels is attempted. Such injuries should becompletely preventable by limiting the traction placed on the biopsy forcepswhen firm, fibrous masses are encountered. Torrential bleeding ensues withinjury to the innominate artery or aorta. Rather than attempting to pack suchinjuries, the surgeon should immediately remove the mediastinoscope andapply digital pressure to the injury while preparing for emergent median sternotomy [12]. It may be possible to repair injuries to the innominate artery
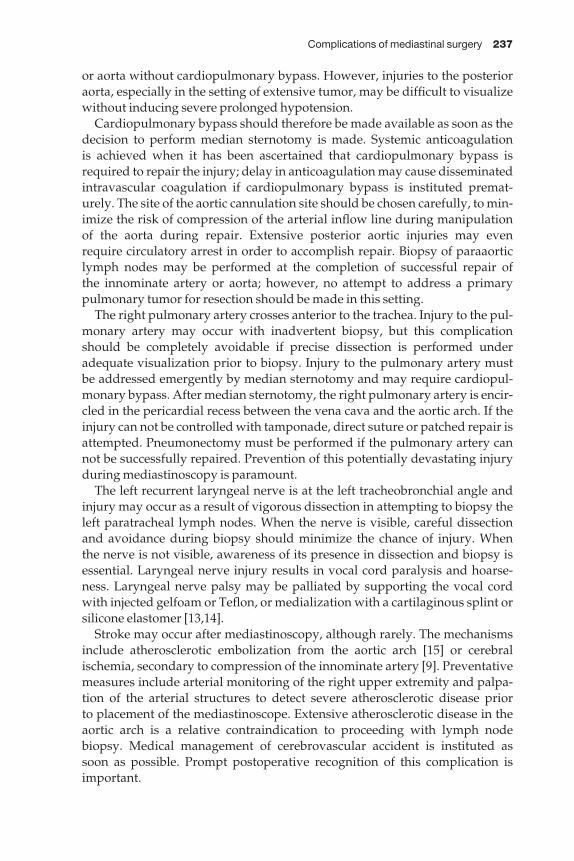
Complications of mediastinal surgery 237
or aorta without cardiopulmonary bypass. However, injuries to the posterioraorta, especially in the setting of extensive tumor, may be difficult to visualizewithout inducing severe prolonged hypotension.
Cardiopulmonary bypass should therefore be made available as soon as thedecision to perform median sternotomy is made. Systemic anticoagulation is achieved when it has been ascertained that cardiopulmonary bypass isrequired to repair the injury; delay in anticoagulation may cause disseminatedintravascular coagulation if cardiopulmonary bypass is instituted premat-urely. The site of the aortic cannulation site should be chosen carefully, to min-imize the risk of compression of the arterial inflow line during manipulation of the aorta during repair. Extensive posterior aortic injuries may even require circulatory arrest in order to accomplish repair. Biopsy of paraaorticlymph nodes may be performed at the completion of successful repair of the innominate artery or aorta; however, no attempt to address a primary pulmonary tumor for resection should be made in this setting.
The right pulmonary artery crosses anterior to the trachea. Injury to the pul-monary artery may occur with inadvertent biopsy, but this complicationshould be completely avoidable if precise dissection is performed under adequate visualization prior to biopsy. Injury to the pulmonary artery must be addressed emergently by median sternotomy and may require cardiopul-monary bypass. After median sternotomy, the right pulmonary artery is encir-cled in the pericardial recess between the vena cava and the aortic arch. If theinjury can not be controlled with tamponade, direct suture or patched repair isattempted. Pneumonectomy must be performed if the pulmonary artery cannot be successfully repaired. Prevention of this potentially devastating injuryduring mediastinoscopy is paramount.
The left recurrent laryngeal nerve is at the left tracheobronchial angle andinjury may occur as a result of vigorous dissection in attempting to biopsy theleft paratracheal lymph nodes. When the nerve is visible, careful dissectionand avoidance during biopsy should minimize the chance of injury. When the nerve is not visible, awareness of its presence in dissection and biopsy isessential. Laryngeal nerve injury results in vocal cord paralysis and hoarse-ness. Laryngeal nerve palsy may be palliated by supporting the vocal cordwith injected gelfoam or Teflon, or medialization with a cartilaginous splint or silicone elastomer [13,14].
Stroke may occur after mediastinoscopy, although rarely. The mechanismsinclude atherosclerotic embolization from the aortic arch [15] or cerebralischemia, secondary to compression of the innominate artery [9]. Preventativemeasures include arterial monitoring of the right upper extremity and palpa-tion of the arterial structures to detect severe atherosclerotic disease prior to placement of the mediastinoscope. Extensive atherosclerotic disease in theaortic arch is a relative contraindication to proceeding with lymph nodebiopsy. Medical management of cerebrovascular accident is instituted as soon as possible. Prompt postoperative recognition of this complication isimportant.
238 Chapter 14
Esophageal perforation may occur during vigorous dissection of the subcarinal lymph nodes. Unlike other complications of mediastinoscopy,esophageal injury may not be apparent at surgery or in the immediate post-operative period. Dissection of the subcarinal space may be associated withbleeding that obscures visibility. It is inadvisable to continue to attempt tobiopsy lymph nodes under these circumstances. Occult esophageal injuryshould be suspected in any patient with fever, leukocytosis, pleural effusion,or cardiac arrhythmia after mediastinoscopy. Perforation of the esophagus is confirmed by barium esophagogram, and immediate repair performedthrough right thoracotomy. Primary repair is achieved by identifying the complete extent of the mucosal injury and closing the mucosa precisely withinterrupted absorbable suture [16]. The muscular layers should then be re-approximated as well. Reinforcement of the repair with an intercostal musclepedicle is advisable, but optional. Gastrostomy or feeding jejunostomy shouldbe considered after repair of the esophageal injury, depending on the extent ofthe injury.
When extensive tumor fibrosis is present, especially after induction ther-apy or in repeated mediastinoscopy, dissection and biopsy may lacerate thetrachea or bronchus. This injury is manifested immediately by a large air leak,easily recognized at mediastinoscopy.
Repair is accomplished through a cervical incision, if the injury is proximal,or right thoracotomy, if the injury is more distal. If pulmonary resection is performed at the time of thoracotomy, the injury may be repaired by itsincorporation in the bronchial stump suture line [17]. Prevention of this injury, in the setting of fibrosis, may be accomplished by using a thoracos-copic approach for paratracheal lymph node biopsy, rather than cervical mediastinoscopy.
Pneumothorax may occur after mediastinoscopy, usually secondary to pleural entry. If recognized at surgery, the pleural space may be evacuatedprior to closure using the mediastinoscope and the suction-dissector. If a smallpneumothorax is present postoperatively, observation is appropriate. If thelung was biopsied or traumatized, tube thoracostomy may be required.
The development of incisional metastases after mediastinoscopy has beenreported [18]. Direct implantation of malignant cells in the surgical field during may be a plausible mechanism; however, it does not necessarilyexplain the appearance of incisional metastases arising after negative medi-astinoscopy. Other possible explanations include lymphatic disseminationand hematogenous spread followed by implantation in the hyperemic woundin the early stages of healing [18]. In the absence of metastatic disease, thetumor implant may be locally excised and radiation therapy employed.
Thymectomy for myasthenia gravis
Resection of anterior mediastinal masses is routinely performed using med-ian sternotomy; however, thymectomy for myasthenia gravis can also be
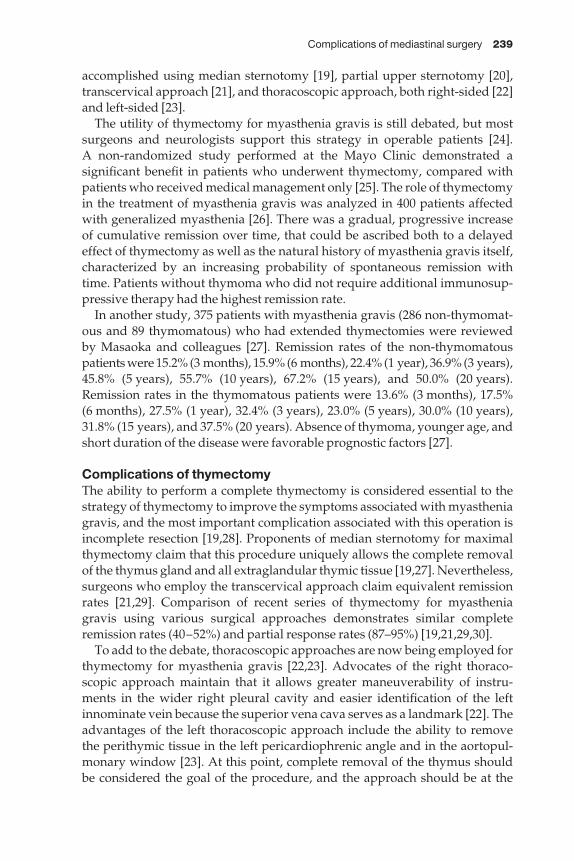
Complications of mediastinal surgery 239
accomplished using median sternotomy [19], partial upper sternotomy [20],transcervical approach [21], and thoracoscopic approach, both right-sided [22]and left-sided [23].
The utility of thymectomy for myasthenia gravis is still debated, but mostsurgeons and neurologists support this strategy in operable patients [24]. A non-randomized study performed at the Mayo Clinic demonstrated asignificant benefit in patients who underwent thymectomy, compared withpatients who received medical management only [25]. The role of thymectomyin the treatment of myasthenia gravis was analyzed in 400 patients affectedwith generalized myasthenia [26]. There was a gradual, progressive increaseof cumulative remission over time, that could be ascribed both to a delayedeffect of thymectomy as well as the natural history of myasthenia gravis itself,characterized by an increasing probability of spontaneous remission withtime. Patients without thymoma who did not require additional immunosup-pressive therapy had the highest remission rate.
In another study, 375 patients with myasthenia gravis (286 non-thymomat-ous and 89 thymomatous) who had extended thymectomies were reviewed by Masaoka and colleagues [27]. Remission rates of the non-thymomatouspatients were 15.2% (3 months), 15.9% (6 months), 22.4% (1 year), 36.9% (3 years),45.8% (5 years), 55.7% (10 years), 67.2% (15 years), and 50.0% (20 years).Remission rates in the thymomatous patients were 13.6% (3 months), 17.5% (6 months), 27.5% (1 year), 32.4% (3 years), 23.0% (5 years), 30.0% (10 years),31.8% (15 years), and 37.5% (20 years). Absence of thymoma, younger age, andshort duration of the disease were favorable prognostic factors [27].
Complications of thymectomyThe ability to perform a complete thymectomy is considered essential to thestrategy of thymectomy to improve the symptoms associated with myastheniagravis, and the most important complication associated with this operation isincomplete resection [19,28]. Proponents of median sternotomy for maximalthymectomy claim that this procedure uniquely allows the complete removalof the thymus gland and all extraglandular thymic tissue [19,27]. Nevertheless,surgeons who employ the transcervical approach claim equivalent remissionrates [21,29]. Comparison of recent series of thymectomy for myastheniagravis using various surgical approaches demonstrates similar completeremission rates (40–52%) and partial response rates (87–95%) [19,21,29,30].
To add to the debate, thoracoscopic approaches are now being employed forthymectomy for myasthenia gravis [22,23]. Advocates of the right thoraco-scopic approach maintain that it allows greater maneuverability of instru-ments in the wider right pleural cavity and easier identification of the leftinnominate vein because the superior vena cava serves as a landmark [22]. Theadvantages of the left thoracoscopic approach include the ability to remove the perithymic tissue in the left pericardiophrenic angle and in the aortopul-monary window [23]. At this point, complete removal of the thymus should be considered the goal of the procedure, and the approach should be at the

240 Chapter 14
discretion of the surgeon, provided equivalent remission rates have been documented.
In the perioperative period following thymectomy for myasthenia gravis,the most important significant complication is considered to be respiratoryfailure, which occurs in 0–4% of patients [19,23,27,31,32]. Pulmonary functionhas been found to be significantly better after thoracoscopic thymectomy com-pared with sternotomy [33]. Adequate preoperative medical management,including plasmapheresis when appropriate, avoiding paralytic agents intra-operatively, and aggressive postoperative pulmonary physiotherapy con-tribute to minimizing the potential for postoperative respiratory therapy.Plasmapheresis involves filtering the plasma of specific proteins, including theacetylcholinesterase antibody. Plasmapheresis produces a rapid, transientclinical improvement in patients with myasthenia gravis and should be con-sidered in every patient preoperatively. Plasmapheresis may be performedevery other day for four to six cycles, up to 48 h prior to surgery. The clinicalimprovement associated with plasmapheresis minimizes the risk of postoper-ative weakness and respiratory failure and avoids the use of anticholinesteraseagents perioperatively.
The choice of agents to induce anesthesia is dependent on the degree ofweakness that the patient demonstrates at the time of surgery. A patient withgood muscle strength may be induced with an agent of choice (propofol, a barbiturate, or etomidate) followed by a fractional dose of a neuromuscularblockade agent. A weaker patient will require a more careful induction with asmaller dose of an induction agent and no neuromuscular blockade agent.Maintenance of anesthesia may be accomplished with propofol infusion orinhalational agent; muscle relaxation is not necessary after successful intuba-tion. With minimization of anesthetic agents, such as narcotics and barbituratesand avoidance of benzodiazepines, the majority of patients can be successfullyextubated in the operating room.
Postoperative recovery in an intensive care unit is considered routine, butwith excellent analgesia (including placement of an epidural catheter), mostpatients may be observed overnight on a step-down unit. The patient must beobserved closely throughout the recovery period for signs of weakness, whichmay occur several days after thymectomy. In addition to monitoring for signsof weakness, attention must be given to aggressive pulmonary physiotherapy,in order to minimize the risk of postoperative atelectasis and pneumonia.Prolonged ventilator dependence may be treated with additional anti-cholinesterase agents, reversal of narcosis, intravenous immunoglobulin, orplasmapheresis to clear circulating antiacetylcholine receptor antibodies [24].Tracheostomy is occasionally beneficial to facilitate pulmonary performance.
Technical complications related to the conduct of thymectomy for myas-thenia gravis should be rare in the absence of thymoma. Complications such as vascular or nerve injury, which are important considerations during theresection of anterior mediastinal masses, are completely avoidable. Injury to the recurrent laryngeal nerve or the phrenic nerve after thymectomy for
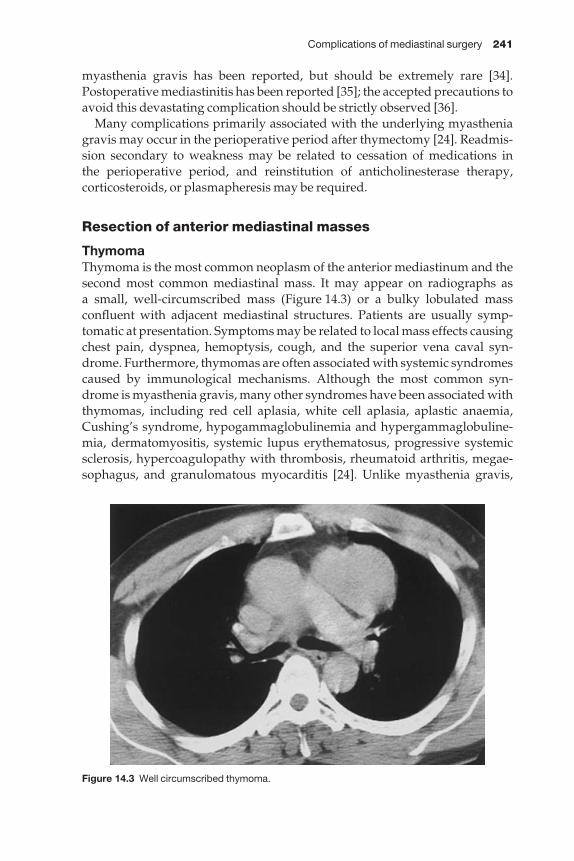
Complications of mediastinal surgery 241
myasthenia gravis has been reported, but should be extremely rare [34].Postoperative mediastinitis has been reported [35]; the accepted precautions toavoid this devastating complication should be strictly observed [36].
Many complications primarily associated with the underlying myastheniagravis may occur in the perioperative period after thymectomy [24]. Readmis-sion secondary to weakness may be related to cessation of medications in the perioperative period, and reinstitution of anticholinesterase therapy, corticosteroids, or plasmapheresis may be required.
Resection of anterior mediastinal masses
ThymomaThymoma is the most common neoplasm of the anterior mediastinum and thesecond most common mediastinal mass. It may appear on radiographs as a small, well-circumscribed mass (Figure 14.3) or a bulky lobulated massconfluent with adjacent mediastinal structures. Patients are usually symp-tomatic at presentation. Symptoms may be related to local mass effects causingchest pain, dyspnea, hemoptysis, cough, and the superior vena caval syn-drome. Furthermore, thymomas are often associated with systemic syndromescaused by immunological mechanisms. Although the most common syn-drome is myasthenia gravis, many other syndromes have been associated withthymomas, including red cell aplasia, white cell aplasia, aplastic anaemia,Cushing’s syndrome, hypogammaglobulinemia and hypergammaglobuline-mia, dermatomyositis, systemic lupus erythematosus, progressive systemicsclerosis, hypercoagulopathy with thrombosis, rheumatoid arthritis, megae-sophagus, and granulomatous myocarditis [24]. Unlike myasthenia gravis,
Figure 14.3 Well circumscribed thymoma.
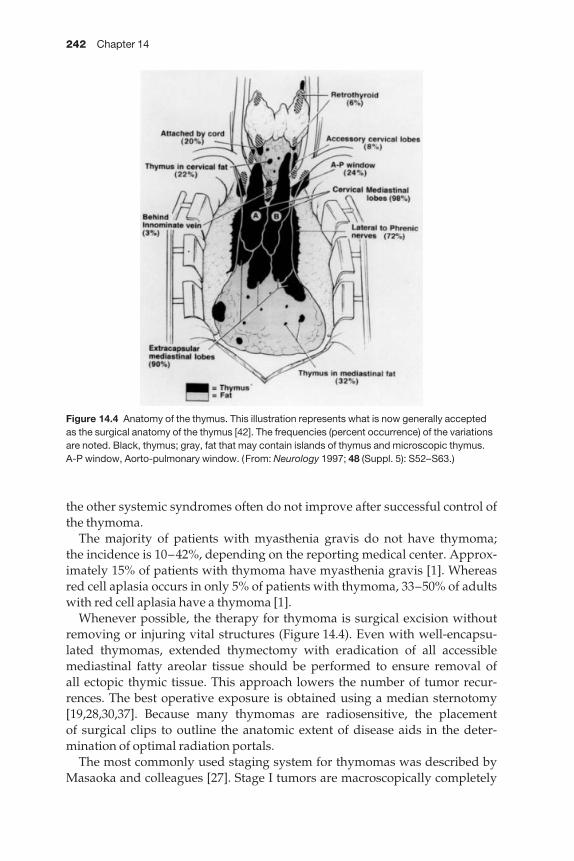
242 Chapter 14
the other systemic syndromes often do not improve after successful control ofthe thymoma.
The majority of patients with myasthenia gravis do not have thymoma; the incidence is 10–42%, depending on the reporting medical center. Approx-imately 15% of patients with thymoma have myasthenia gravis [1]. Whereasred cell aplasia occurs in only 5% of patients with thymoma, 33–50% of adultswith red cell aplasia have a thymoma [1].
Whenever possible, the therapy for thymoma is surgical excision withoutremoving or injuring vital structures (Figure 14.4). Even with well-encapsu-lated thymomas, extended thymectomy with eradication of all accessiblemediastinal fatty areolar tissue should be performed to ensure removal of all ectopic thymic tissue. This approach lowers the number of tumor recur-rences. The best operative exposure is obtained using a median sternotomy[19,28,30,37]. Because many thymomas are radiosensitive, the placement of surgical clips to outline the anatomic extent of disease aids in the deter-mination of optimal radiation portals.
The most commonly used staging system for thymomas was described byMasaoka and colleagues [27]. Stage I tumors are macroscopically completely
Figure 14.4 Anatomy of the thymus. This illustration represents what is now generally acceptedas the surgical anatomy of the thymus [42]. The frequencies (percent occurrence) of the variationsare noted. Black, thymus; gray, fat that may contain islands of thymus and microscopic thymus.A-P window, Aorto-pulmonary window. (From: Neurology 1997; 48 (Suppl. 5): S52–S63.)

Complications of mediastinal surgery 243
encapsulated, with no microscopical capsular invasion; stage II tumorsdemonstrate microscopic invasion into surrounding fatty tissue, mediastinalpleura or capsule; stage III tumors have macroscopic invasion into adjacentmediastinal structures; stage IVa disease is characterized by pleural or pericardial dissemination; and IVb disease is defined by lymphogenous orhematogenous metastasis.
Complete surgical resection for stage I thymoma is sufficient treatment. Theadjunctive use of radiation therapy is the recommended treatment for stage II and III disease [37]. Tumors > 5 cm, locally invasive tumors, unresectabletumors, and metastatic tumors should be treated by protocols that includechemotherapy, followed by surgical exploration with the goal of completeresection and postoperative radiation. The best results are seen with cisplatin-based regimens with overall response rates of 70–100% [38].
An aggressive surgical approach is recommended for invasive thymomasincluding radical resection and vascular reconstruction of the superior venacava or its branches when invaded. Utilizing this aggressive approach toobtain complete resections a significant difference in 5-year survival is seen inpatients with stage III thymomas (94%) compared with those with incompleteresections (35%) [37]. Thymomas frequently show recurrence and reoperationfor recurrent disease has been recommended. Since thymomas have beenreported to have late recurrence, cure rates should be based on 10-year follow-up data.
Germ cell tumorsGerm cell tumors are benign and malignant neoplasms thought to originatefrom primordial germ cells that fail to complete the migration from the urogenital ridge. These lesions are identical histologically to germ cell tumorsoriginating in the gonads, but are not metastatic. The current recommenda-tions for evaluating the testes of a patient with mediastinal germ cell tumor are careful physical examination and ultrasonography. Biopsy is reserved forpositive findings.
Teratomas are neoplasms composed of multiple tissue elements derivedfrom the three primitive embryonic layers foreign to the area in which theyoccur. These tumors are located most commonly in the anterior mediastinum,although they are sometimes found in the posterior mediastinum (Figure14.5). Symptoms are related to mechanical effects and include chest pain,cough, dyspnea, or symptoms related to recurrent pneumonitis. CT findings of a predominantly fatty mass with a denser dependent portion containingglobular calcifications, bone, or teeth and a solid protuberance into a cysticcavity are considered specific. Malignant tumors are identified by the presenceof embryonic tissue or by the presence of malignant components.
Diagnosis and therapy rely on surgical excision. For those benign tumors of such large size or with involvement of adjacent mediastinal structures such that complete resection is impossible, partial resection has led to resolu-tion of symptoms, frequently without relapse. For malignant teratomas,
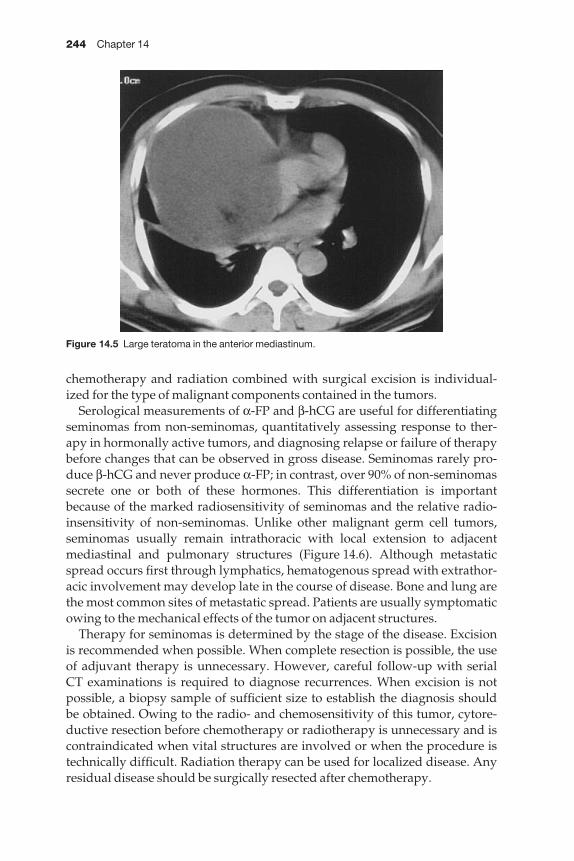
244 Chapter 14
chemotherapy and radiation combined with surgical excision is individual-ized for the type of malignant components contained in the tumors.
Serological measurements of α-FP and β-hCG are useful for differentiatingseminomas from non-seminomas, quantitatively assessing response to ther-apy in hormonally active tumors, and diagnosing relapse or failure of therapybefore changes that can be observed in gross disease. Seminomas rarely pro-duce β-hCG and never produce α-FP; in contrast, over 90% of non-seminomassecrete one or both of these hormones. This differentiation is importantbecause of the marked radiosensitivity of seminomas and the relative radio-insensitivity of non-seminomas. Unlike other malignant germ cell tumors, seminomas usually remain intrathoracic with local extension to adjacent mediastinal and pulmonary structures (Figure 14.6). Although metastaticspread occurs first through lymphatics, hematogenous spread with extrathor-acic involvement may develop late in the course of disease. Bone and lung arethe most common sites of metastatic spread. Patients are usually symptomaticowing to the mechanical effects of the tumor on adjacent structures.
Therapy for seminomas is determined by the stage of the disease. Excision is recommended when possible. When complete resection is possible, the useof adjuvant therapy is unnecessary. However, careful follow-up with serial CT examinations is required to diagnose recurrences. When excision is notpossible, a biopsy sample of sufficient size to establish the diagnosis should be obtained. Owing to the radio- and chemosensitivity of this tumor, cytore-ductive resection before chemotherapy or radiotherapy is unnecessary and iscontraindicated when vital structures are involved or when the procedure istechnically difficult. Radiation therapy can be used for localized disease. Anyresidual disease should be surgically resected after chemotherapy.
Figure 14.5 Large teratoma in the anterior mediastinum.
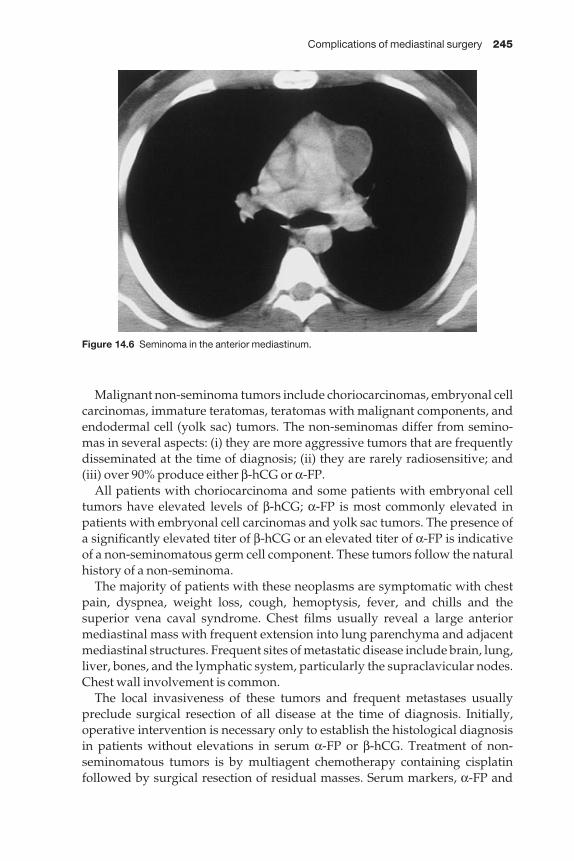
Complications of mediastinal surgery 245
Malignant non-seminoma tumors include choriocarcinomas, embryonal cellcarcinomas, immature teratomas, teratomas with malignant components, andendodermal cell (yolk sac) tumors. The non-seminomas differ from semino-mas in several aspects: (i) they are more aggressive tumors that are frequentlydisseminated at the time of diagnosis; (ii) they are rarely radiosensitive; and(iii) over 90% produce either β-hCG or α-FP.
All patients with choriocarcinoma and some patients with embryonal celltumors have elevated levels of β-hCG; α-FP is most commonly elevated inpatients with embryonal cell carcinomas and yolk sac tumors. The presence ofa significantly elevated titer of β-hCG or an elevated titer of α-FP is indicativeof a non-seminomatous germ cell component. These tumors follow the naturalhistory of a non-seminoma.
The majority of patients with these neoplasms are symptomatic with chestpain, dyspnea, weight loss, cough, hemoptysis, fever, and chills and the superior vena caval syndrome. Chest films usually reveal a large anteriormediastinal mass with frequent extension into lung parenchyma and adjacentmediastinal structures. Frequent sites of metastatic disease include brain, lung,liver, bones, and the lymphatic system, particularly the supraclavicular nodes.Chest wall involvement is common.
The local invasiveness of these tumors and frequent metastases usually preclude surgical resection of all disease at the time of diagnosis. Initially,operative intervention is necessary only to establish the histological diagnosisin patients without elevations in serum α-FP or β-hCG. Treatment of non-seminomatous tumors is by multiagent chemotherapy containing cisplatin followed by surgical resection of residual masses. Serum markers, α-FP and
Figure 14.6 Seminoma in the anterior mediastinum.
246 Chapter 14
β-hCG are followed to assess response to treatment, and when these markersnormalize the patient is taken to the operating room and removal of as much of the remaining tumors as possible is performed. The presence of residual disease after chemotherapy portends a poor prognosis and the need for additional chemotherapy. If the tumor markers do not normalize, a secondcourse of chemotherapy is begun with new agents.
Resection of tumors of the anterior mediastinum is usually performedthrough median sternotomy. Dissection of thymic malignancies and germ celltumors requires the development of planes between the tumor and the phrenicnerves, the recurrent laryngeal nerve, the thoracic duct, the great vessels, the trachea, the pericardium, the sternum, and the lungs. Resection of locallyadvanced malignancies may require resection of involved structures; vascularreconstruction may be required in some circumstances.
Complications related to resection of anterior mediastinal massesInjury to one or both phrenic nerves may occur during resection. Prior to surgery, the function of the phrenic nerves may be assessed by evaluatingthe position of the diaphragms on the preoperative chest radiograph or byfluoroscopy. The phrenic nerves should be assessed intraoperatively in termsof their relationship to the tumor. If one phrenic nerve is non-functional due totumor involvement, it is resected with the tumor, and every effort is made topreserve the contralateral nerve. The left phrenic nerve lies in a more anteriorposition than the right phrenic nerve in relation to the pulmonary hilum and ismore likely to be in jeopardy during dissection.
Unilateral phrenic nerve injury is tolerated by most patients, and no specifictherapy is required. Plication of the diaphragm may be performed sub-sequently in patients who develop prominent diaphragmatic eventration orparadoxical motion. Bilateral phrenic nerve injury is poorly tolerated; patientswith bilateral diaphragmatic dysfunction may require bilateral plication ortracheostomy and mechanical ventilation [39].
Tumors of the anterior mediastinum near the aortopulmonary window mayinvolve the left recurrent laryngeal nerve. Complete resection of the tumor is the primary goal, and resection of the recurrent nerve is required if it isinvolved. Postoperatively, the resulting vocal cord palsy may be treated withTeflon or gelfoam injection or with vocal cord medialization [13,14].
Chylothorax may result after resection of mediastinal masses, although it ismore commonly associated with esophagectomy or pneumonectomy. Injuryto the thoracic duct during dissection of anterior mediastinal masses occurs at the level of the aortic arch, where the thoracic duct passes behind the leftcarotid artery, or at the insertion into the left subclavian vein. If the thoracicduct is involved with the tumor or is in jeopardy from the dissection, it shouldbe intentionally ligated, rather than risk postoperative leak.
If the injury is not recognized at surgery, the development of an early post-operative effusion or persistent pleural drainage, especially if the fluid is milky

Complications of mediastinal surgery 247
in appearance, suggests trauma to the thoracic duct. The diagnosis of chylo-thorax is confirmed if triglyceride level in the pleural fluid is > 110 mg/dl [40].
Prolonged drainage of chyle causes malnutrition if not recognized and managed aggressively. Non-operative management includes pleural drainageand enteral or parenteral nutritional support. Enteral support, using a formulabased on medium chain triglycerides, is infrequently successful. Pleural sclerosis may be used to expedite closure of the injured thoracic duct [41].
The most successful approach is early reoperation and surgical closure of the thoracic duct [42]. Preoperative lymphoscintigraphy to identify the siteof injury is unnecessary. Ligation of the thoracic duct in the right chest at thelevel of the diaphragm (using thoracotomy or thoracoscopy) is successful in a majority of cases. For patients who have undergone extensive mediastinaldissection for anterior mediastinal masses, direct ligation at the site of injurymay be preferred. Intraoperative localization of the injury is improved if a substantial amount of lipid (such as cream or vegetable oil) is administeredprior to surgery via nasogastric tube.
Cerfolio and colleagues reported the Mayo Clinic experience with post-operative chylothorax [41]. Of the 47 patients in this series with postoperative chylothorax, six had undergone resection of mediastinal mass. In this series,conservative management was associated with failure, and the authors re-commend early operative intervention.
Resection of complex anterior mediastinal masses, especially stage III thy-momas after induction chemotherapy, requires careful dissection of vascularstructures, in order to avoid intraoperative hemorrhage and sacrifice of essential vessels. Most anterior mediastinal masses have a close relationship to the brachiocephalic vein; if the tumor is directly invasive or if the vessel isobliterated, the brachiocephalic vein may be resected en bloc with the tumor.Reconstruction is optional if the superior vena cava is patent; if both the brachiocephalic vein and the superior vena cava are involved, reconstitutionof at least one cavoatrial connection is recommended to avoid severe cerebraledema [43].
Bacha and colleagues reported their results after extended radical resectionin 89 patients with primary mediastinal tumors invading adjacent structures[43]. In this series, there were 35 invasive thymomas, 12 thymic carcinomas, 17 germ cell tumors, 16 lymphomas, three neurogenic tumors, three thyroidcarcinomas, two radiation-induced sarcomas, and one mediastinal mesothe-lioma. Adjacent resected structures included 38 phrenic nerves, 21 superiorvenae cavae, 16 upper lobes, and 13 innominate veins, and in five patients a pneumonectomy was required. The complication rate was 17% and the mortality rate 6% [43].
A heterogeneous group of tumors, both benign and malignant, involve the thoracic inlet and adjacent structures, including superior sulcus tumors,primary neurogenic tumors arising in autonomic and somatic nerves aroundthe spine or brachial plexus, soft-tissue neoplasms, and metastases from a variety of primary sites. Complete resection requires careful dissection, and
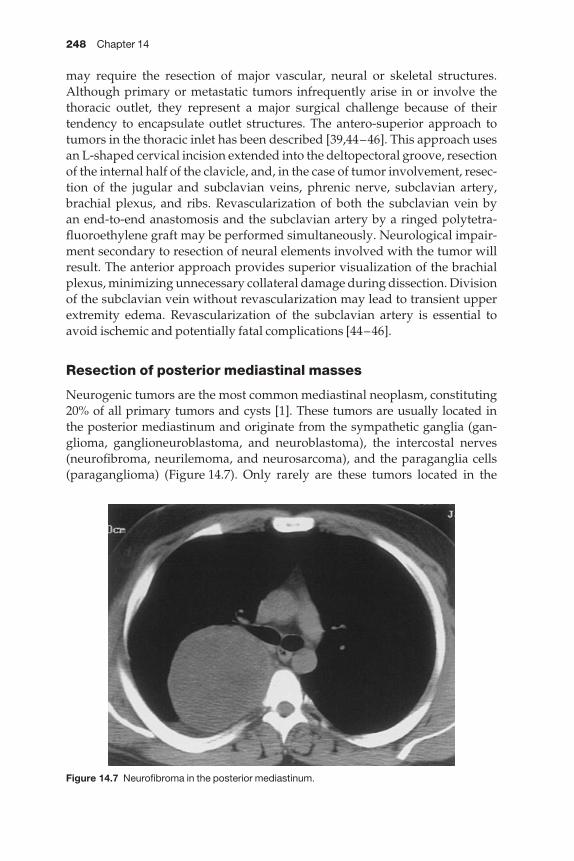
248 Chapter 14
may require the resection of major vascular, neural or skeletal structures.Although primary or metastatic tumors infrequently arise in or involve thethoracic outlet, they represent a major surgical challenge because of their tendency to encapsulate outlet structures. The antero-superior approach totumors in the thoracic inlet has been described [39,44–46]. This approach usesan L-shaped cervical incision extended into the deltopectoral groove, resectionof the internal half of the clavicle, and, in the case of tumor involvement, resec-tion of the jugular and subclavian veins, phrenic nerve, subclavian artery,brachial plexus, and ribs. Revascularization of both the subclavian vein by an end-to-end anastomosis and the subclavian artery by a ringed polytetra-fluoroethylene graft may be performed simultaneously. Neurological impair-ment secondary to resection of neural elements involved with the tumor willresult. The anterior approach provides superior visualization of the brachialplexus, minimizing unnecessary collateral damage during dissection. Divisionof the subclavian vein without revascularization may lead to transient upperextremity edema. Revascularization of the subclavian artery is essential toavoid ischemic and potentially fatal complications [44–46].
Resection of posterior mediastinal masses
Neurogenic tumors are the most common mediastinal neoplasm, constituting20% of all primary tumors and cysts [1]. These tumors are usually located in the posterior mediastinum and originate from the sympathetic ganglia (gan-glioma, ganglioneuroblastoma, and neuroblastoma), the intercostal nerves(neurofibroma, neurilemoma, and neurosarcoma), and the paraganglia cells(paraganglioma) (Figure 14.7). Only rarely are these tumors located in the
Figure 14.7 Neurofibroma in the posterior mediastinum.
Complications of mediastinal surgery 249
anterosuperior mediastinum. Although the peak incidence occurs in adults,neurogenic tumors comprise a proportionally greater percentage of mediastinalmasses in children. Whereas the majority of neurogenic tumors in adults arebenign, a greater percentage of neurogenic tumors are malignant in children.
Many of these tumors are found in asymptomatic patients on routine chest films. When present, symptoms are usually caused by mechanical factorssuch as chest and back pain due to compression or invasion of intercostalnerve, bone, and chest wall; cough and dyspnea due to compression of the tracheobronchial tree; Pancoast’s syndrome; and Horner’s syndrome due toinvolvement of the brachial and the cervical sympathetic chain. Symptomsmay be systemic and related to production of neurohormonal agents.
Thoracoscopy has played an increasing role both in diagnosis and treatmentof neurogenic tumors. Benign neurogenic tumors are particularly amenable to thoracoscopic removal, and more rapid postoperative recovery is seen with thoracoscopic removal compared with open excision [2]. For malignanttumors, the standard of care remains thoracotomy.
The complications associated with resection of posterior mediastinal massesare similar to those following resection of anterior mediastinal masses.However, posterior masses uniquely may involve the vertebral bodies orspinal cord. Approximately 10% of neurogenic tumors have extensions intothe spinal column [1]. These are termed dumbbell tumors because of theircharacteristic shape with relatively large paraspinal and intraspinal portionsconnected by a narrow isthmus of tissue traversing the intervertebral foramen.Although the majority of patients with a dumbbell tumor have neurologicalsymptoms related to spinal cord compression, the significant proportion ofpatients without symptoms underscores the importance of evaluating allpatients with a posterior mediastinal mass for possible intraspinal extensionwith a MRI. The recommended surgical approach to dumbbell tumors is a one-stage excision of the intraspinal component before resecting the thoraciccomponent to minimize any spinal column hematoma. The incision used for the posterior laminectomy is extended into the appropriate interspace to allow resection of the mediastinal component. Anterior video-assisted thoracoscopy for removal of the intrathoracic component of the tumor is combined with a posterior laminectomy for microneurosurgical removal ofthe spinal component [47].
Thoracoscopic sympathectomy
The thoracoscopic approach is the most commonly used approach for surgicalsympathectomy of the upper extremities. Thoracoscopic sympathectomy isused in the treatment of palmar and axillary hyperhidrosis [48], reflex sym-pathetic dystrophy [49], atherosclerotic peripheral vascular disease [50], andRaynaud’s disease [51]. Usually, the sympathetic ganglia are removed fromT2–T4, although some surgeons prefer a more limited dissection, at T2 only[48].
250 Chapter 14
Death after thoracoscopic sympathectomy has been reported, secondary to cerebral edema, when CO2 insufflation has been employed [52]. Anotherpatient in this series sustained severe neurological dysfunction, secondary to cerebral edema. The development of cerebral edema after thoracoscopicsympathectomy is attributable to gas insufflation, which is not required andshould be avoided. Major vascular injury during thoracoscopic sympathec-tomy has also been reported, and this complication should be completelyavoidable [52]. Chylothorax after sympathectomy has also been described and is related to division of accessory ducts rather than injury to the thoracicduct [53,54]. In these cases, treatment with chest tube drainage was successfuland reoperation was not required.
The most common complications of sympathectomy are related to mani-pulation of the autonomic nervous system [55]. Injury to the brachial plexus has been described [56]. Inadvertent injury of the stellate ganglion will pro-duce ipsilateral Horner’s syndrome, either total or partial (without meiosis).Injury to the stellate ganglion is caused by mechanical or thermal damage to T1 during dissection. In order to prevent this injury, precise identification ofribs 1–4 is required prior to dissection of the sympathetic ganglion at T2; nodissection is performed above this level. Furthermore, excessive nerve tractionis avoided during dissection. Finally, the use of bipolar cautery or ultrasonicdissection will prevent current diffusion to the stellate ganglion.
Neuralgia along the ulnar aspect of the upper limb may occur after sympathectomy, which usually resolves within 6 weeks [55]. Compensatorysweating may occur after upper extremity sympathectomy, in various areas,including the axillary, inguinal, and truncal regions. This complication isunpredictable and there are no techniques to avoid its occurrence. Gustatorysweating (facial perspiration provoked by the taste of food) can also occur [57].
Medical complications of mediastinal surgery
In patients undergoing thoracic surgery, the incidence of atrial arrhythmias is 15–40% [58]. In addition to extent of resection, the risk factors for the development of atrial fibrillation include age, presence of coronary artery disease, history of congestive heart failure, and the use of theophylline.Proposed mechanisms for the development of atrial fibrillation include rightventricular dilatation, elevated catecholamine levels, and atrial conductiondelay resulting in reentrant circuits, secondary to pulmonary vein manipula-tion and surgical dissection. Atrial arrhythmias most commonly present on postoperative days 2–4, related to the increased adrenergic activity in thepostsurgical state.
A treatment algorithm for postoperative atrial fibrillation includes the following:1 Correction of hypoxia.2 Correction of acid/base abnormalities.3 Correction of hypokalemia, hypomagnesemia.
Complications of mediastinal surgery 251
4 Limitation of β-adrenergic agents and theophylline.5 Rate control with diltiazem, if hemodynamically stable; β-adrenergicblockade may be used in patients with low risk of congestive heart failure andbronchospasm [58]..6 Medical cardioversion with amiodarone, sotalol, propafenone, or pro-caineamide may be attempted in patients who do not spontaneously return tosinus rhythm.7 Synchronized electrical cardioversion may be used in selective patients,including those who are hemodynamically unstable.8 Anticoagulation may be required in patients who remain in atrial fibrillation.
In patients with no history of cardiac disease, the incidence of myocardialinfarction (MI) after thoracic surgery is < 0.5%. In patients with a previous MI,the incidence of postoperative MI is 3–15%, with an associated mortality of25–50% [59]. If MI is suspected in the postoperative period, the diagnosis is confirmed with electrocardiography and serum isoenzymes, including tro-ponin. If the patient is hemodynamically stable, optimal medical managementshould be instituted, including continuous electrocardiographic surveillancemonitoring for at least 48 h, supplemental oxygen, heparin (unless contrain-dicated by surgical issues), β-blockade, control of hypertension, and close attention to acid/base and fluid/electrolyte balance. Thrombolytic adminis-tration and interventional procedures are usually not indicated in the stablepostoperative patient.
For patients who deteriorate despite medical management, more intensivetherapy must be considered. If ventricular failure is a component of the pre-sentation, pulmonary artery catheterization is performed for measurement of right and left heart pressures, more accurate assessment of volume status,and monitoring for the administration of inotropic and vasodilatory agents.Transesophageal echocardiography may be required for patients to determinethe degree of mitral valvular insufficiency. Cardiac catheterization for angio-plasty and stenting must be considered in the presence of ongoing ischemia.Intraaortic balloon pumping may also be used in patients with refractoryischemia, particularly in those with malignant ischemic arrhythmias.
Atelectasis is a common postoperative complication, with several manifesta-tions, including the creation of a pulmonary shunt and resulting hypoxia,decreased immune response and associated pneumonia, and potential perman-ent functional loss. Pathogenic factors that predispose to atelectasis includepostoperative pain, general anesthesia, diaphragmatic dysfunction, chest wall alteration, partial pneumothorax, pleural effusion, abdominal distension,chronic obstructive pulmonary disease, and active smoking. The diagnosis ofatelectasis is both radiographic and clinical. It may be difficult to distinguishfrom active pneumonia in the early postoperative period. The treatment ofatelectasis includes adequate analgesia, chest physiotherapy, patient educa-tion regarding coughing, deep breathing, and incentive spirometry (prefer-ably performed preoperatively), mucolytics, bronchoscopy, and tracheostomy(rarely).

252 Chapter 14
Analgesic regimen
A comprehensive analgesic strategy should be made for every patient prior to thoracic surgery. Epidural analgesia, paravertebral blocks, extrapleuralcatheters, and intercostal blocks are all effective means of optimizing pain control that are superior to the practice of supplying analgesia in the postoper-ative period exclusively. Adequate pain control is essential to optimizing pain control and pulmonary toilet, to prevent pulmonary complications, and mayhelp to limit catecholamine flux and the associated cardiac complications.
References
1 Davis RD, Oldham HN, Sabiston DC. Primary cysts and neoplasms of the mediastinum:recent changes in clinical presentation, methods of diagnosis, management, and results.Ann Thorac Surg 1987; 44: 229–237.
2 Demmy TL, Krasna MJ, Detterbeck FC et al. Multicenter VATS experience with medias-tinal tumors. Ann Thorac Surg 1998; 66: 187–192.
3 Pearson FG. Mediastinoscopy. A method of biopsy in the superior mediastinum. J ThoracCardiovasc Surg 1965; 49: 11–15.
4 Ginsberg RJ, Rice TW, Goldberg M et al. Extended cervical mediastinoscopy. A singlestaging procedure for bronchogenic carcinoma of the left upper lobe. J Thorac CardiovascSurg 1987; 94: 673–678.
5 Foster ED, Munro DD, Dobell AR. Mediastinoscopy. A review of anatomical relationshipsand complications. Ann Thorac Surg 1972; 13: 273–286.
6 Hammoud ZT, Anderson RC, Meyers BF et al. The current role of mediastinoscopy in theevaluation of thoracic disease. J Thorac Cardiovasc Surg 1999; 118: 894–899.
7 Luke WP, Pearson FG, Todd TR et al. Prospective evaluation of mediastinoscopy forassessment of carcinoma of the lung. J Thorac Cardiovasc Surg 1986; 91: 53–56.
8 Puhakka H. Complications of mediastinoscopy. J Laryngol Otol 1989; 103: 312.9 Trinkle JK, Bryant LR, Hiller AJ et al. Mediastinoscopyaexperience with 300 consecutive
cases. J Thorac Cardiovasc Surg 1970; 60: 297–300.10 Vallieres E, Page A, Verdant A. Ambulatory mediastinoscopy and anterior mediastino-
tomy. Ann Thorac Surg 1991; 52: 1122–1126.11 Meersschaut D, Vermassen F, Brutel de la Riviere A et al. Repeat mediastinoscopy in the
assessment of new and recurrent lung neoplasm. Ann Throrac Surg 1992; 53: 120–122.12 Kirschner PA. Cervical mediastinoscopy. Surg Clin North Am 1996; 6: 1–19.13 Kraus DH, Ali MK, Ginsberg RJ et al. Vocal cord medialization for unilateral paralysis
associated with intrathoracic malignancies. J Thorac Cardiovasc Surg 1996; 111: 334–341.14 Mom T, Filaire M, Advenier D et al. Concomitant type I thyroplasty and thoracic opera-
tions for lung cancer: preventing respiratory complications associated with vagus orrecurrent laryngeal nerve injury. J Thorac Cardiovasc Surg 2001; 121: 642–648.
15 Urschel JD, Vretenar DF, Dickout WJ et al. Cerebrovascular accident complicating cervicalmediastinoscopy. Ann Thorac Surg 1994; 57: 740–741.
16 Whyte RI, Iannettoni MD, Orringer MB. Intrathoracic esophageal perforation. The meritof primary repair. J Thorac Cardiovasc Surg 1995; 109: 140–146.
17 Schubach SL, Landreneau RJ. Mediastinoscopic injury to the bronchus: use of in-continuity bronchial flap repair. Ann Thorac Surg 1992; 53: 1100–1103.
18 Al-Sofyani M, Maziak DE, Shamji FM. Cervical mediastinoscopy incisional metastasis.Ann Thorac Surg 2000; 69: 1255–1257.
Complications of mediastinal surgery 253
19 Jaretzki A, Penn AS, Younger DS et al. ‘Maximal’ thymectomy for myasthenia gravis.Results. J Thorac Cardiovasc Surg 1988; 95: 747–757.
20 Wilkins EW, Grillo HC, Scannell JG et al. Role of staging in prognosis and management ofthymoma. Ann Thorac Surg 1991; 51: 888–892.
21 Cooper JD, Al-Jilaihawa AN, Pearson FG et al. An improved technique to facilitate tran-scervical thymectomy for myasthenia gravis. Ann Thorac Surg 1988; 45: 242–247.
22 Yim APC, Kay RLC, Ho JKS. Video-assisted thoracoscopic thymectomy for myastheniagravis. Chest 1995; 108: 1440–1443.
23 Mineo TC, Pompeo E, Lerut TE et al. Thoracoscopic thymectomy in autoimmune myas-thenia: results of left-sided approach. Ann Thorac Surg 2000; 69: 1537–1541.
24 Drachman DB. Myasthenia gravis. N Engl J Med 1994; 330: 1797–1810.25 Buckingham JM, Howard FM, Bernatz PE et al. The value of thymectomy in myasthenia
gravis: a computer-assisted matched study. Ann Surg 1976; 184: 453–456.26 Durelli L, Maggi G, Casadio C et al. Actuarial analysis of the occurrence of remission
following thymectomy for myasthenia gravis in 400 patients. J Neurol Neurosurg Psychiatry1991; 54: 406–411.
27 Masaoka A, Yamakawa Y, Niwa H et al. Extended thymectomy for myasthenia gravispatients: a 20-year review. Ann Thorac Surg 1996; 62: 853–859.
28 Jaretzki A, Barohn RJ, Ernstoff RM et al. Myasthenia gravis: recommendations for clinicalresearch standards. Ann Thorac Surg 2000; 70: 327–334.
29 Bril V, Kojic J, Ilse WK et al. Long-term clinical outcome after transcervical thymectomy formyasthenia gravis. Ann Thorac Surg 1998; 65: 1520–1522.
30 Mulder DG, Graves M, Hermann C. Thymectomy for myasthenia gravis: recent observa-tions and comparisons with past experience. Ann Thorac Surg 1989; 48: 551–555.
31 Detterbeck FC, Scott WW, Howard JF Jr et al. One hundred consecutive thymectomies formyasthenia gravis. Ann Thorac Surg 1996; 62: 242–245.
32 Mack MJ, Landreneau RJ, Yim AP et al. Results of video-assisted thymectomy in patientswith myasthenia gravis. J Thorac Cardiovasc Surg 1996; 112: 1352–1360.
33 Bulkley GB, Bass KN, Stephenson GR et al. Extended cervicomediastinal thymectomy inthe integrated management of myasthenia gravis. Ann Surg 1997; 226: 3243–34.
34 Goldman L, Caldera D, Nussbaum S et al. Multifactorial index of cardiac risk in noncar-diac surgical procedures. N Engl J Med 1977; 297: 845–850.
35 Rückert JC, Walter M, Müller JM. Pulmonary function after thoracoscopic thymectomyversus median sternotomy for myasthenia gravis. Ann Thorac Surg 2000; 70: 1656–1661.
36 Nieto IP, Robledo JPP, Pajuelo MC et al. Prognostic factors for myasthenia gravis treatedby thymectomy: review of 61 cases. Ann Thorac Surg 1999; 67: 1568–1571.
37 Baskett RJF, MacDougall CE, Ross DB. Is mediastinitis a preventable complication? A 10-year review. Ann Thorac Surg 1999; 67: 462–465.
38 Masaoka A, Monden Y, Nakahara K, Tanioka T. Follow-up study of thymomas with special reference to their clinical stages. Cancer 1981; 48: 2485–2492.
39 Thomas CR, Wright CD, Loehrer PJ. Thymoma. State of the art. J Clin Oncol 1999; 17:
2280–2289.40 de Leeuw M, Williams JM, Freedom RM et al. Impact of diaphragmatic paralysis after
cardiothoracic surgery in children. J Thorac Cardiovasc Surg 1999; 118: 510–517.41 Staats RA, Ellefson RD, Budahn LL et al. The lipoprotein profile of chylous and unchylous
pleural effusions. Mayo Clinic Proc 1980; 55: 700–704.42 Cerfolio RJ, Allen MS, Deschamps C et al. Postoperative chylothorax. J Thorac Cardiovasc
Surg 1996; 112: 1361–1366.43 Fahimi H, Casselman FP, Mariani MA et al. Current management of postoperative chy-
lothorax. Ann Thorac Surg 2001; 71: 448–450.
254 Chapter 14
44 Bacha EA, Chapelier AR, Macchiarini P et al. Surgery for invasive primary mediastinaltumors. Ann Thorac Surg 1998; 66: 234–239.
45 Dartevelle P, Chapelier A, Macchiarini P et al. Anterior transcervical-thoracic approachfor radical resection of lung tumors invading the thoracic inlet. J Thorac Cardiovasc Surg1993; 105: 1025–1034.
46 Macchiarini P, Dartevelle P, Chapelier A et al. Technique for resecting primary andmetastatic nonbronchogenic tumors of the thoracic outlet. Ann Thorac Surg 1993; 55:
611–618.47 Vanakesa T, Goldstraw P. Antero-superior approaches in the practice of thoracic surgery.
Eur J Cardiothorac Surg 1999; 15: 774–780.48 Heltzer JM, Krasna MJ, Aldrich F et al. Thoracoscopic excision of a posterior mediastinal
‘dumbbell’ tumor using a combined approach. Ann Thorac Surg 1995; 60: 431–433.49 Hsu C, Chen C, Lin C et al. Video-assisted thoracoscopic T2 sympathectomy for hyper-
hydrosis palmaris. J Am Coll Surg 1994; 179: 59–61.50 Hazelrigg SR, Mack MJ. Surgery for autonomic disorders. In: Kaiser LR, Daniel TM, eds.
Thoracoscopic Surgery. Boston: Little Brown, 1993; 89.51 Daniel TM. Thoracoscopic sympathectomy. Chest Surg Clin North Am 1996; 6: 69–83.52 Nicholson ML, Hopkinson DR, Dennis MJ. Endoscopic transthoracic sympathectomy:
successful in hyperhidrosis but can the indications be extended? Ann R Coll Surg Engl1994; 76: 311–314.
53 Cameron AE. Complications of endoscopic sympathectomy. Eur J Surg 1998; 164: 33–35.54 Cheng W, Chang C, Lin T. Chylothorax after endoscopic sympathectomy: case report.
Neurosurgery 1994; 35: 330–331.55 Gossot D. Chylothorax after thoracoscopic sympathectomy. Surg Endosc 1996; 10: 949.56 Gossot D, Kabiri H, Caliandro R et al. Early complications of thoracic endoscopic sym-
pathectomy: a prospective study of 940 procedures. Ann Thorac Surg 2001; 71: 1116–1119.57 Lange JF. Inferior brachial plexus injury during thoracoscopic sympathectomy. Surg
Endosc 1995; 68: 1177–1181.58 Nesathurai S, Harvey DT, Schatz SW. Gustatory facial sweating subsequent to upper
thoracic sympathectomy. Arch Phys Med Rehabil 1995; 76: 104–107.59 Amar D. Cardiac arrhythmias. Chest Surg Clin North Am 1998; 8: 479–493.
PART I I I
Cardiac surgery


CHAPTER 15
Complications of coronary artery bypass surgery
Nader Moazami, Hendrick Barner
Improvements in surgical technique, anesthesia, and postoperative care havehad a significant positive impact on results obtained with coronary arterybypass grafting (CABG) in the last two decades. Increasing and aggressive per-cutaneous interventions, use of new stents and potent platelet inhibitors havecreated a group of patients with an increasingly complicated risk profile thatpose a challenge to all cardiac surgeons. Despite these factors, operative mor-tality from isolated CABG has steadily declined in the last decade to under 3%(STS Database 2000 results) with postoperative length of stay of about 6 days.
Preoperative assessment clearly plays an important role in selecting patientsfor operative intervention. Risk factors associated with all cardiac surgicalinterventions include advancing age, obesity (wt > 1.5 × ideal), diabetes,chronic obstructive pulmonary disease, New York Heart Association (NYHA)functional class, peripheral vascular disease, previous history of cerebrovascu-lar accidents, and renal failure. Furthermore emergency operations, presenceof cardiogenic shock, recent myocardial infarction (MI), and reoperations are all factors that incrementally increase risk of morbidity and mortality aftercardiac operations. The majority of these topics have been discussed in detailelsewhere and in major textbooks [1]. In this chapter, we will focus on deci-sion-making and technical factors that effect the short-term outcome of CABG.Specifically, we will discuss how to avoid complications and how to correctmistakes during the operation. A short description of early postoperative complications is also given.
Preoperative assessment
A complete history, physical, and review of available tests are important inassessing any patient prior to cardiac surgery. Several important elements arecentral in this evaluation.
Predisposition to bleedingPreoperative blood dyscrasias that may predispose to bleeding are infrequentbut a key element in the history. Renal insufficiency can predispose to bleeding[2] but more commonly, bleeding problems arise from preoperative treatment
257

258 Chapter 15
with thrombolytic therapy or long-acting antiplatelet agents. Aspirin takenwithin 1 week may increase bleeding time but infrequently causes postoperat-ive blood loss [3]. On the other hand, platelet inhibitors given during percuta-neous interventions can have a profound effect on clotting. Urgent CABG canbe safely performed on these patients and the effect can be reversed withplatelet transfusion. Operative plan should include platelet transfusion forCABG after discontinuation of cardiopulmonary bypass only if persistent non-surgical bleeding is present [4].
Central neurological complicationsStroke following CABG has been estimated to occur in 6% of operations with permanent neurological deficits occurring in about 3% [5]. Although theliterature suggests that carotid stenosis is not a risk factor for patients withouthistory of neurological symptoms [6], we are very aggressive in performingscreening for carotid disease with color flow duplex ultrasound. We prefercarotid endarterectomy in all asymptomatic patients with critical stenosis (> 75%). In patients with symptomatic carotid stenosis carotid endarterectomyis performed before CABG or concomitantly.
Although stroke after cardiac surgery is multifactorial, one of the most probable causes is atheroembolization from the ascending aorta or arch.Calcified aorta on chest X-ray is a particularly ominous sign. A non-contrastcomputed tomography scan can more accurately determine the extent ofcalcification. If cannulation of the ascending aorta is not possible and an on-pump operation is planned, axillary artery cannulation for antegrade flow during cardiopulmonary bypass (CPB) offers an excellent option [7].Intraoperative epiaortic ultrasound is another option to ascertain the degree ofdisease prior to manipulation of the aorta [8].
Coronary angiogramCareful preoperative review of the coronary angiogram is of critical import-ance in developing a strategy for revascularization. Critical to this evaluationis selection of appropriate targets, size of the recipient vessel, and degree ofproximal stenosis. We typically aim for complete revascularization in all cases,and if appropriate, an all arterial grafting strategy. The recipient vessel shouldbe at least 1.5 mm in size and extend out from the A-V groove with a good runoff. In cases where the degree of proximal stenosis is judged to be 70% we hesit-ate to use an all-arterial grafting practice because of concern for detrimentaleffect of competitive flow to overall graft patency, particularly when the radialartery is used. It should be noted that although the coronary angiogram is currently the best modality available for assessing anatomy, it frequentlyunderestimates the degree of atherosclerotic involvement of the coronaries,and extent of calcification. This is of particular concern in diabetics and renalfailure patients. In selecting an appropriate target it is important to view thevessel from different projections to ensure that the segment is suitable forgrafting. Calcification is often best appreciated on the frames immediatelyprior to injection of dye.
Complications of coronary artery bypass surgery 259
Selection of conduitsWe prefer an all-arterial revascularization strategy when feasible [8]. Recentdata on patency support strategies to maximize the number of arterial ana-stomoses by T-grafting or Y-grafting techniques [9–11]. The radial artery or theright internal mammary artery (IMA) is taken off the left IMA for completerevascularization, using multiple sequential grafting. Early patency for theseconstructs has been excellent with freedom from reintervention of > 90% at 5 years.
We emphasize that for low-grade stenoses of 70%, because of concernsregarding competitive flow and graft failure, we have moved away from usingthe radial artery (RA) as a conduit. Despite a resurgence of interest in the radialartery, use of vein grafts is always an excellent strategy. Saphenous vein graftsare free of atherosclerotic disease, have rarely been damaged by indwellinglines (as is the case with radial arteries), can be harvested quickly, and mostimportantly are reliable because they are not prone to spasm.
Harvesting techniquesRadial arteryPrior to harvesting, collateral circulation to the hand must be assessed. Wehave used only the Allen test, which requires occlusion of the radial and ulnararteries at the wrist, closing of the hand totally for 20 s, followed by release ofthe ulnar artery. Capillary refilling of the palm and digits requires 2–10 s; if ittakes longer than 10 s, the test is considered positive and the RA is not har-vested. If the palmar skin is heavily pigmented so that capillary filling cannotbe visualized, a digital pulse oximeter can be used to assess return of capillaryflow. In 528 patients studied, 4.4% had a bilaterally positive test and 11.9% hada unilaterally positive test. The RA from the non-dominant arm is usually har-vested. Hypoperfusion of the hand or claudication has not been noted in thecurrent era of RA use. Sensory disturbance related to the lateral antebrachialcutaneous nerve or superficial branch of the radial nerve has occurred in5–10%, but has not been a debilitating or persistent problem. Others have recommended that a more sophisticated and objective evaluation of collateralcirculation to the hand be used. Non-invasive assessment has included pulsevolume recording, oximetric plethysmography with calculation of a perfusionindex, and pulsed Doppler scanning [12]. Measurement of flow velocity in the ulnar artery, in the palmar branch of the radial artery, and in the artery ofthe thumb is performed with and without radial artery occlusion at the wrist.With the latter technique, 5.9% (11/185) of non-dominant RAs were excludedfrom use. When the former methodology was used in 224 patients (448 extrem-ities), 17 patients had bilaterally positive tests (7.6%) and 16 had unilaterallypositive tests (7.1%) [12].
Harvesting techniqueThe incision is made over the course of the RA with a central medial curvealong the border of the brachioradialis muscle, which will reflect the ante-brachial cutaneous nerve lying in the deep subcutaneous tissue in the lateral
260 Chapter 15
flap. Electrocautery is used to divide the subcutaneous tissue, but is limited tothe deep fascia in the proximal half of the incision because distally the RA isclose to the fascia. The brachioradialis muscle is reflected laterally to exposethe RA beneath its medial edge. The RA is dissected as a pedicle, with its venaecomitantes and associated fatty areolar tissue, beginning in its midportion andusing blunt and sharp technique. A tape or vessel loop can be placed aroundthe pedicle to facilitate exposure of the dorsally placed branches, which aredivided between small clips. The dissection continues proximally to the originof the artery, which is confirmed by identifying the ulnar artery. Division ofthe radial recurrent artery may add more length to the RA, depending on thelevel of origin of this branch. Division of the radial veins will expose the originof the RA. Distal dissection continues to the major wrist crease, and the lengthof the artery is measured in situ as this information may be helpful in planningthe operation. The superficial radial nerve runs lateral and parallel to the radial artery as far as the distal forearm, where it passes dorsally to the distal forearm. It is usually not seen in dissection of the RA unless dissection strayson the lateral side of the artery. The artery is ligated or clipped at both ends and removed. Some like to observe the distal pulse (with proximal occlusion)as evidence of adequate collateral flow before dividing the artery. We have notused this maneuver but have relied on the results of the Allen test. The incisionis closed in layers with absorbable suture after achieving hemostasis, and thearm can be left on the arm board or tucked at the patient’s side. Drains are not used.
Internal thoracic arteryWe continue to harvest the left internal thoracic artery (ITA) as a pedicle graftwith approximately 0.5 cm fascia on either side of the artery along with theaccompanying mammary veins. Harvesting is performed with the hemister-num elevated and under direct vision with good lighting and magnification.Removal of the peri-pleural fat pad from underneath the sternum will aid invisualization of the course of the artery. A plane can be developed medial andparallel to the artery by dividing the endothoracic fascia and sternocostalismuscle which is then used as a handle for gentle traction. Excessive downwardtraction anywhere along the artery can lead to avulsion injury of the small perforating branches that may lead either to dissection of the vessel or persist-ent bleeding. If bleeding from one of the torn branches occurs, we prefer tomobilize the vessel off the chest wall to allow adequate access and visualiza-tion of the vessel. Blind repairs lead to unacceptable narrowing of the ITA.Harvesting is done with the cautery on a low setting. The cautery tip should be protected with a rubber-covered or insulated blade bent at 45–60°. Cauteryshould be used at short bursts at the branching sites with most of the dissectioncarried out bluntly with gentle strokes. Electrocautery injuries can lead to early graft failure or induce vasospasm. Branch arteries are generally con-trolled with small clips. It is important that the clip applier not ‘scissor’ duringapplication, otherwise avulsion may occur leading to possible dissection.
Complications of coronary artery bypass surgery 261
Mobilization of the ITA pedicle is carried from the level of the innominate veinto its bifurcation into the two subdivisions of this vessel (the musculophrenicand superior epigastric arteries). During the proximal dissection, care must be taken to identify clearly the phrenic nerve and avoid injury. Bleedingencountered in this area must be controlled under direct vision. By holdingventilation, the left lung will be out of the field allowing coagulation or clipping of the culprit vessel.
The distal extent of the dissection should also be limited to immediately pastthe bifurcation. After this point the caliber of the vessel is small. In addition,preservation of collateral flow to the lower aspect of the incision may be important to avoid wound infection and necrosis of the lower sternum andsubxiphoid area [13]. If additional length is needed and the superior epigastricartery is of good quality then it may be used, although some believe this segment to be associated with lower patency rates [14].
Skeletonization of the ITASome prefer to harvest the ITA without associated tissue and without thevenae comitantes. The ITA is exposed by incising the overlying endothoracicfascia and sternocostalis muscle with scissors, or the dissection can be initiatedmedially with cautery. Blunt dissection with the cold cautery tip is used to ease the artery from its bed. Electrocautery can injure the skeletonized ITA;branches must be divided between small clips. With magnification it is possible to see the anatomy of arterial branches and place clips to maximallypreserve collateral sternal blood flow by dividing sternal/perforating andsternal/intercostal branches upstream to their division without injuring theITA. Those who utilize the skeletonized ITA believe that there is less reductionin sternal blood flow, less mediastinal wound infection, longer length of theITA, easier construction of sequential anastomoses, and easier recognition ofpersistent spasm or harvesting-related ITA injury [15]. Although preservationof collateral sternal blood flow is theoretically possible based on anatomicstudies, this benefit has not been proved. Sequential grafting is facilitated by askeletonized ITA because pedicle tissue may interfere with construction of aside-to-side anastomosis. Spasm and injury are recognized more easily, but theharvest technique is more difficult, and the potential for damage is greater.Skeletonization also requires twice the time needed for pedicle mobilization.
Ultrasonic dissection can also be used for skeletonization. Division of thefascia, muscle and branches can be achieved with division of branches 2 mmfrom the ITA without injury to the ITA and preservation of distal branching toprovide collateral flow [16]. Patency at 1 year is excellent [17].
Vein harvestingSuperficial wound complications arising from the vein harvest site are com-mon, especially in diabetic patients. In one study, impaired wound healingdefined as mild inflammation, drainage, or erythema occurred in 24% ofpatients undergoing CABG [18]. Recent advances in endoscopic vein harvesting

262 Chapter 15
suggest that atraumatic dissection can be performed with a limited number ofskin incisions. Because most of the dissection is done in a subcutaneous tunnel,risk of infection may be diminished [19]. Although endoscopic vein harvestingyields suitable conduits, and the incisions are more cosmetically appealing,large prospective studies are needed to show a reduced rate of infection. Atour institution, we still use standard techniques for harvesting the vein andminimize skin incisions by creating ‘bridges’ of skin. A key factor in perform-ing vein harvest, using any technique available, is to avoid excessive tractionon the vein. Disruption of the endothelium can lead to early graft thrombosis.A suitable vein is 3–5 mm in diameter. Varicosed and aneurysmal vein graftshould never be used unless they are focal and can be fixed. We refrain fromusing the lesser saphenous graft unless absolutely no conduits are available,usually in re-do operations.
Sternotomy
We generally perform the incision down to the level of the sternum with the knife to avoid excessive damage caused by electrocautery. Extensivecautery application to the skin edges or the avascular subcutaneous fat leads tonecrosis and postoperative infection. Closing the vessel shut using forceps andbriefly applying cautery can control focal areas of bleeding without the need toapply cautery indiscriminately. We generally avoid marking the sternum inthe middle with electrocautery to define the line of sternotomy. This devascu-larizes the sternum by burning the periosteum. If during sternotomy the line is not exactly followed, then areas of avascularized bone will remain and mayact as a nidus for infection. Once the sternum is open, we try to avoid use of foreign bodies on the marrow, particularly bone wax. If bleeding is low grade,tamponade with pads will suffice. If bleeding is more brisk, then we generallyrub Gelfoam (± thrombin) on the marrow (Pharmacia, Kalamazoo, MI, USA).This has excellent hemostatic properties.
After harvesting the ITA, heparin is administered, clamped and the ITA issharply divided. We measure flow visually and as long as the stream of bloodprojects 7.5–10 cm beyond the distal end, we consider it adequate. Green hassuggested that the flow should be measured with the minimal acceptable flowbeing 50 ml/min [20]. Once satisfied with the conduit, papaverine (2 mg/ml)is sprayed on the pedicle, which is then wrapped in a Papaverine-soakedsponge and placed in the left chest. Alternatively, heparinized blood contain-ing papaverine solution (2 mg/ml) can be injected directly into the lumen witha 1–2-mm blunt plastic or metallic olive-tip cannula. The ITA should not beoccluded proximally during injection. We routinely combine papaverine withblood to utilize the buffering capacity of blood for the normally acidic pH ofpapaverine (pH 2–3). This preparation has a more physiological pH (7.3) andmay cause less perturbation of the endothelial milieu. The cannula for injectionmust be inserted gently with adequate visualization of the lumen, otherwisethe vessel may dissect. If a short dissection flap is created, then the vessel canbe cut back to the point where normal lumen is present. We absolutely refrain
Complications of coronary artery bypass surgery 263
from directly instrumenting the ITA with probes or dilators to avoid potentialdamage, which will jeopardize overall patency.
T-grafting with the RA or right ITA
In cases where we have decided on complete revascularization with the radialartery or the right skeletonized ITA, we perform the proximal anastomosisfirst utilizing a T graft or Y configuration. Overall patency is reported as > 90%[9–11, 21,22].
In this configuration, the free right ITA is anastomosed to the dorsal (smoothor pleural surface) side of the left ITA pedicle at the level of the left atrialappendage (or where the left ITA crosses the edge of the incised pericardium),which has been cut across the pulmonic valve into the ‘bare area’ of the peri-cardium to the phrenic nerve and then parallel to the phrenic nerve 1–2 cm. Itis helpful to harvest the left ITA with a pedicle to facilitate the T anastomosis.Two stay sutures are placed in the ITA pedicle at the site of the intended ana-stomosis to elevate the pedicle from the superior mediastinum and avoidmotion transmitted from the heart and lungs (it may be necessary to pack theleft upper lobe away from the operative area with a single laparotomy pad).After systemic heparinization (300 U/kg), the left ITA is bled distally to fill itwith heparinized blood, and a vascular bulldog clamp (soft/Fibra, 6 mm;Applied Medical Resources, Laguna Hills, CA, USA) is applied proximally. A4- to 5-mm incision is made in the left ITA, and the right ITA or RA is spatu-lated 2–3 mm. A Y-shaped anastomosis is performed with continuous 7–0 or 8–0 polypropylene suture which may lie at a right angle depending on the ultimate position of the anastomosis and its limbs. The pedicles of the two conduits are attached with two sutures of 6–0 polypropylene to relieve anastomotic stress. The bulldog clamp is released, and each conduit is thenfilled with heparinized blood containing papaverine (2 mg/ml), via 1- or 2-mm olive-tipped cannula. The conduits are allowed to dilatate while can-nulation for cardiopulmonary bypass is completed. The conduits are thenchecked visually and by palpation for satisfactory dilatation. It not suitable,they are refilled with papaverine, and bypass is not initiated until the surgeonis satisfied with the conduits.
The T and Y configuration grafts are technically complex and demanding for the surgeon. The elements involved in this procedure are best learned in a step-wise fashion, with mastery and confidence gained with each step beforeproceeding to another. Because all inflow is from a single source, there is the potential for hypoperfusion, which is greater than that from use of indi-vidual arterial conduits for each coronary artery. A faulty T anastomosis canjeopardize the entire arterial reconstruction.
Cannulation
The pericardium is opened to the level of the pericardial reflection on the aorta.Complete exposure and visualization of the innominate vein is not necessary
264 Chapter 15
and may make future reoperation easier. The thymic fat pad can be ligated to avoid problems with bleeding. If a large amount of fatty tissue remains after ligation it should be resected as a devascularized segment can act as a nidus for infection. Inferiorly the pericardium is T’ed off to the right and left pleural reflections with approximately 1 cm of pericardial edge remainingon the diaphragm, again to avoid bleeding problems from diaphragmatic vessels.
Initial palpation of the aorta will give a general sense of suitability of theaorta for cannulation. Palpation is a very gross assessment with a false-negative rate of 55–60%. In patients with severe vasculopathy, age > 65 years,previous history of stroke or significant atherosclerotic disease in the de-scending aorta as assessed by transesophageal echocardiography (TEE), weroutinely perform an epiaortic echocardiogram. This technique allows a betterappreciation of the severity of intraluminal, non-palpable disease and forselection of proximal anastomotic sites [23]. If the aorta is judged not suitablefor cannulation then an alternate site (femoral or subclavian artery) can be chosen, an off-pump procedure may be elected or hypothermic fibrillatoryarrest with left ventricular venting is appropriate.
Cardioplegia deliveryWe acknowledge that there are many strategies for cardioplegia delivery andmyocardial protection. We routinely use both antegrade and retrograde bloodcardioplegia. We use a retrograde cannula with a soft tip self-inflating balloonthat is inserted after arterial and venous cannulation. If during maneuvers forproper placement the patient becomes hypotensive, we generally go on bypassand position the cannula with the heart full, gently lifting the heart to visualizethe coronary sinus. Excessive force for placing cannula can lead to rupture ofthe coronary sinus. If this happens the sinus can be repaired preferably with apericardial patch. If repair is not possible then it can be ligated with pledgetedsuture. The antegrade needle is generally placed while on bypass to avoid therisk of aortic dissection as the needle is introduced.
Distal anastomosis
Selection of target siteWith the heart in its normal beating state, the distal targets can be visualizedand palpated to select an area for anastomosis. Ideally the anastomosis is madeto an area that is minimally diseased and has a diameter of 1.5–2 mm. Vesselsthat are 1 mm have very poor patency rates and should not be bypassed. On the right, the coronary artery in the A-V groove is frequently severely diseased, but not always, and may be used for distal anastomosis when theposterior descending artery or the posterior ventricular branch are not suitablefor bypass.
After application of the aortic cross clamp and cardiac arrest with combinedantegrade and retrograde cardioplegia, the heart should be positioned to

Complications of coronary artery bypass surgery 265
achieve easy access and visualization of the anastomotic site. The epicardiumis then gently dissected with a rounded blade exposing the artery. Arteriotomycan be performed by multiple gentle strokes with a sharp Beaver blade or witha single upward movement of the blade after partially inserting the tip in thecoronary artery at a 45° angle. Running retrograde cardioplegia during thismaneuver will distend the vessel and help prevent damaging the posteriorwall of the artery. If the posterior wall is damaged through the adventitia itmust be repaired from the inside with fine 7–0 or 8–0 Prolene suture placed as a mattress suture and tied on the outside. Bleeding into the myocardium can cause significant myocardial dysfunction. The arteriotomy is extended in either direction. Care is taken to remain in the middle of the artery. Obliquearteriotomy incisions will distort the toe or heel of the anastomosis.Attempting to correct an oblique arteriotomy may lead to creation of a bivid-shaped arteriotomy that is difficult to sew to.
The size of the arteriotomy incision should be approximately twice thediameter of the coronary or about 3–5 mm in length. Vein grafts can typicallybe transected at right angles to the long axis. If the vein is small it can either be beveled or ‘fish-mouthed’. The compliance of the vein allows it to stretchover the arteriotomy site. Arterial grafts are generally spatulated to create a hood about 1–2 mm longer than the arteriotomy because these grafts do not safely stretch over an arteriotomy that is longer than the graft opening. Amismatch can put the fragile coronary under tension and cause a tear.
Occasionally after the arteriotomy is created a tight lesion is encountered atthe toe of the anastomosis. This will lead to early graft failure unless the arteri-otomy is extended further distally across the plaque as a patch angioplasty.This will create a longer anastomosis but reduce the likelihood of graft closure.If the area involved with stenosis is too long then a second separate distal anastomosis should be created. We frequently even consider a sequential anastomosis to the same artery with one graft to maximize the revasculariza-tion of the coronary artery bed in terms of proximal and distal perfusion.
Occasionally, the diseased coronary vessel has an intramyocardial courseand is difficult to identify. The course of the other coronary arteries, if visible,provide a road map to the general location of the target vessel. If branches are visible, they can be traced back to their origin to identify the main trunk. Alternatively, the distal end can be identified and traced back with electrocautery set at a very low level to divide muscle bridges. If none of thesemaneuvers allows identification of the vessel, the side branch can be chosen as the site of anastomosis provided that it is of sufficient caliber and has noproximal stenosis. This is especially useful when the left anterior descendingartery can not be identified. In this case, the diagonal artery can be used ifappropriate.
When dissecting the submuscular left anterior descending (LAD), the rightventricle is occasionally entered, particularly if the LAD has a course justunder the endocardium of the right ventricle. Historically, this has beenrepaired by placing sutures from the epicardium under the LAD and through

266 Chapter 15
the opposite epicardium. These are large, gross bites and can compromise septal branches. A preferable technique is that of closing the right ventricleendocardium with 6–0 polypropylene and then closing the epicardium overthis repair. The anastomosis is done away from this area.
Anastomotic techniquesEnd-to-side anastomosisThe most critical parts of the anastomosis are the heel and the toe; narrowing ateither location will comprise blood flow. We start most of our anastomoses at the heel taking bites that are approximately 1 mm from the edge and 1 mmapart from each other. Care should be taken to minimize handling of the graftfor exposure. Gentle traction of the adventitia should provide adequate ex-posure. Instrumentation of the lumen should be avoided. Usually five suturesare placed around the heel before parachuting the graft onto the coronaryartery as the suture line is tightened. The anastomosis is then continued on theside wall until the toe. At the toe, again small close bites are taken. If the biteson the coronary side are too deep a dimpling effect will occur at the distal site.In addition, this ensures that a purse-string effect would not narrow the lumenwhen the suture is tied. Minimizing leeks at the heel or toe is importantbecause a repair at these locations can compromise the lumen.
Once the toe sutures are placed, the suture is placed under tension and thelumen is gently probed with an undersized 1-mm probe to ensure proximaland distal patency. Excessive force or blindly passing the probe without notic-ing the course of the coronary artery can lead to intimal dissection or full thick-ness tear. This maneuver should be avoided if a large posterior plaque ispresent or the artery is severely diseased. Once patency is assured, the ana-stomosis is completed. Prior to tying the suture, the graft is flushed to de-air.Gentle pressure is maintained to minimize purse stringing as the suture is tieddown. In case of the ITA graft, blood flow is re-established to accomplish this.The ITA graft is tacked down to the epicardium with 6–0 prolene near theanastomosis site. This prevents the pedicle from twisting or angulating alongits axis.
Order of distalsThe order of performing distals depends on the conduits used, degree of disease in the native vessels, and planned strategy for cardiac protection. Asdescribed before, we routinely employ antegrade and retrograde cardioplegiafor myocardial protection during CABG surgery. If vein grafts are used, cardioplegia is delivered down the grafts as each anastomosis is completed.Concerns for protection of the right heart with retrograde cardioplegia mayprompt us to construct the distal right bypass first. On the other hand, if the circumflex territory has a very critical stenosis, we may proceed with branchesof the circumflex system first. We almost routinely perform LAD anastomosislast because traction on the heart during access to the posterior vessels maydamage the anastomosis.
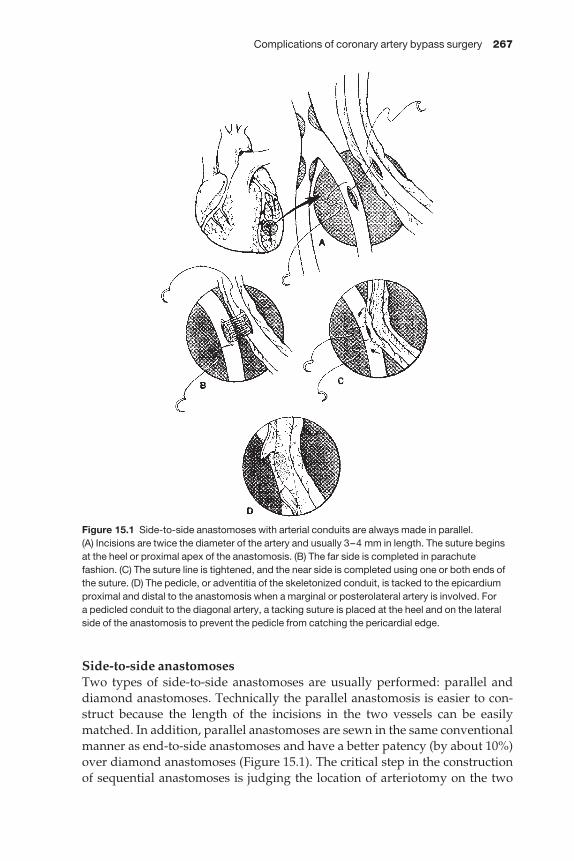
Complications of coronary artery bypass surgery 267
Side-to-side anastomosesTwo types of side-to-side anastomoses are usually performed: parallel anddiamond anastomoses. Technically the parallel anastomosis is easier to con-struct because the length of the incisions in the two vessels can be easilymatched. In addition, parallel anastomoses are sewn in the same conventionalmanner as end-to-side anastomoses and have a better patency (by about 10%)over diamond anastomoses (Figure 15.1). The critical step in the constructionof sequential anastomoses is judging the location of arteriotomy on the two
Figure 15.1 Side-to-side anastomoses with arterial conduits are always made in parallel. (A) Incisions are twice the diameter of the artery and usually 3–4 mm in length. The suture beginsat the heel or proximal apex of the anastomosis. (B) The far side is completed in parachutefashion. (C) The suture line is tightened, and the near side is completed using one or both ends ofthe suture. (D) The pedicle, or adventitia of the skeletonized conduit, is tacked to the epicardiumproximal and distal to the anastomosis when a marginal or posterolateral artery is involved. For a pedicled conduit to the diagonal artery, a tacking suture is placed at the heel and on the lateralside of the anastomosis to prevent the pedicle from catching the pericardial edge.

268 Chapter 15
Figure 15.2 Techniques of side-to-side vein-to-coronary artery anastomoses are illustrated. (A) Incisions are at least twice the diameter of the coronary artery, and the suture line begins at the heel or proximal part of the anastomosis and continues distally on the far side in parachutefashion. (B) After suture bites are placed around the toe, the suture line is pulled tight. (C) The nearside is completed usually with the suture from the heel. (D) When the anastomosis crosses, thecoronary incision is the same as in A, but the vein must be large enough for a similar incision.Again, the suture line starts at the heel and continues on the far side in parachute fashion until the toe is completed. The suture line is pulled tight, and the anastomosis is completed. (E) If thediameter of the vein is adequate, the anastomosis will be satisfactory. (F) If the vein is small, thevein will be flattened at the anastomotic site (seagull deformity). A better anastomosis for thissituation is illustrated in G. The incision is made parallel to the long axis of the vein rather thantransversely. (H) The completed anastomosis is shown. (I) No seagull deformity develops because the longitudinal incision in the vein adds tissue to the anastomosis.
Complications of coronary artery bypass surgery 269
coronaries and the exact length between the two areas on the conduit. Longlengths can cause kinking, short lengths will cause excessive tension. For veinconduits it is important gently to distend the vein to judge the proper distance.Arterial grafts should also be distended by providing inflow. The graft shouldlay on the epicardium to allow the distal anastomoses to be created on goodtarget areas without torsion or angulation. Either the proximal or distal ana-stomosis can be done first. Having one end of the conduit free allows for bettervisualization of the anastomosis since the free end can be moved back andforth. For vein grafts we typically construct the distal anastomosis first. Forarterial grafts if the proximal is taken as a Y- or T-graft, we construct the moreproximal coronary anastomosis first. If the arterial graft is taken off the aorta,we perform the distal sequential anastomosis first.
The diamond side-to-side anastomosis is more difficult to construct (Fig-ure 15.2). The incisions on the vein and artery should be the same length. We use the ‘parachute’ technique for full visualization and start taking one bitefrom the proximal apex of the coronary and one bite from the middle of the conduit. The suture line is continued using the parachute technique to thenear arterial apex, at which point the suture line is tightened. Precise sutureplacement is important to avoid jeopardizing a graft that may supply morethan one critical territory.
EndarterectomyIndicationsCoronary endarterectomy was used early in the history of direct myocardialrevascularization, but enthusiasm for it has varied through the intervening 30 years. Some surgeons commonly utilize this technique, while others rarelydo so.
Endarterectomy is usually undertaken when there is diffuse, severe diseasewithin a coronary artery so that no suitable site to anastomose is availablewithout endarterectomy. Some surgeons undertake endarterectomy only iftotal occlusion is present to minimize the small risk of perioperative occlusiondue to an intimal flap and/or acute thrombosis of the endarterectomized seg-ment. This philosophy assumes that reocclusion will not cause infarction, butthis is not entirely true, since extensive thrombosis can produce infarctiondespite good collateral flow.
We prefer to avoid endarterectomy and achieve revascularization by one ofseveral alternatives. Anastomoses can be placed distally, where disease is lessor absent, if the lumen is 1.5 mm in diameter. Frequently a diffusely diseasedvessel has small areas where the anterior wall is normal or relatively so with areasonable lumen. One, two, or three anastomoses may be placed to a singlecoronary artery to provide flow into segments separated by severe stenosesalternating with intervening healthier areas. Finally, relatively healthybranches of adequate size (1.5 mm), such as diagonal arteries, can be grafted.These anastomoses provide retrograde perfusion of the primary trunk and secondary branches and distal perfusion of the grafted artery. Thus use of
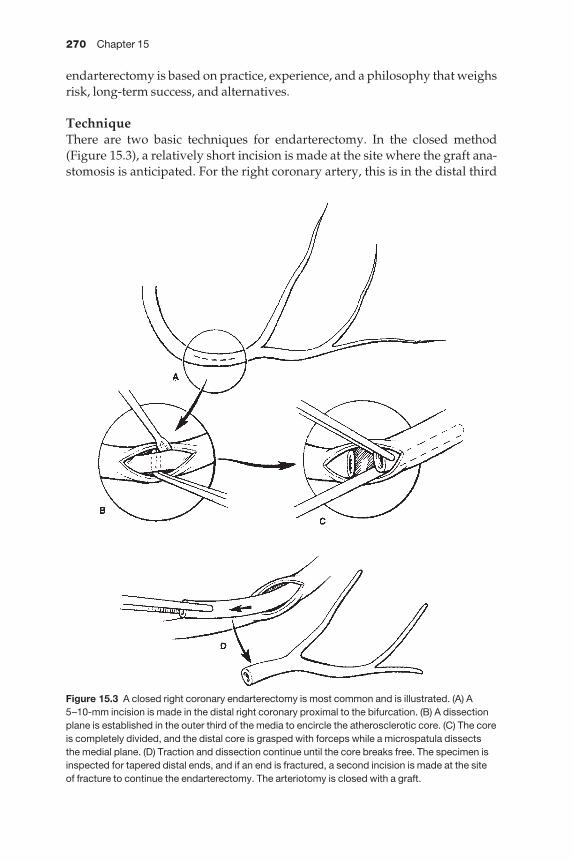
270 Chapter 15
endarterectomy is based on practice, experience, and a philosophy that weighsrisk, long-term success, and alternatives.
TechniqueThere are two basic techniques for endarterectomy. In the closed method(Figure 15.3), a relatively short incision is made at the site where the graft ana-stomosis is anticipated. For the right coronary artery, this is in the distal third
Figure 15.3 A closed right coronary endarterectomy is most common and is illustrated. (A) A5–10-mm incision is made in the distal right coronary proximal to the bifurcation. (B) A dissectionplane is established in the outer third of the media to encircle the atherosclerotic core. (C) The coreis completely divided, and the distal core is grasped with forceps while a microspatula dissectsthe medial plane. (D) Traction and dissection continue until the core breaks free. The specimen isinspected for tapered distal ends, and if an end is fractured, a second incision is made at the siteof fracture to continue the endarterectomy. The arteriotomy is closed with a graft.

Complications of coronary artery bypass surgery 271
just proximal to the bifurcation. After making a 5–10-mm incision, a dissectionplane is developed in the outer third of the media and carried around the ves-sel. The core is elevated and divided. Using a variety of instruments includingwire loop, microspatula, or a tonsil spatula, the endarterectomy plane is devel-oped in both directions by placing gentle traction on the plaque as the dis-section proceeds. At some point the plaque is fully dissected and is extractedfrom the coronary artery. Occasionally, firm traction must be applied to thecore while countertraction is applied to the heart in the distribution of theinvolved artery to separate the plaque. The tip of the plaque is inspected todetermine whether or not the plaque is tapered and has separated cleanly. Ifthe plaque has fractured, a ledge is left that may produce an intimal flap. If thecore is fractured, the vessel should be opened (unless too small, i.e. < 1.5 mm)at the site of fracture to extend the endarterectomy or to tack the intimal flapdown with fine polypropylene. This can be difficult in a vessel less than 2.5 mm in diameter. The distal arteriotomy also can be used for graft anastom-osis with closure of the proximal arteriotomy or use for a second anastomosis.A proximal (to the coronary arteriotomy) endarterectomy is safe in the rightcoronary system if the right coronary artery is occluded to its origin. However,if flow is antegrade to right ventricular branches, proximal endarterectomyshould not be undertaken because it could disrupt flow into important rightventricular or collateral branches to the left ventricle. Proximal endarterec-tomy is not recommended for the left coronary arterial system.
The bypass graft can be vein or artery and is anastomosed in standard fash-ion. The anastomosis may be longer than for a non-endarterectomized vesselbecause of the longer incision for the endarterectomy.
Open endarterectomy is applied most commonly to the left anteriordescending coronary artery, but can be applied to any coronary artery. Theincision extends the length of the segment to be endarterectomized, but if the distal vessel becomes small (< 1.5 mm) and the disease extends beyond, aclosed distal endarterectomy is performed. The dissection plane is developedcircumferentially in the proximal or middle segment, and the plaque isdivided. With gentle traction, the plaque is dissected in the outer third of themedia, and large branches are identified. Care is taken to carry the dissectionplane into branches so that the entire plaque is removed to achieve taperedendings if possible. Proximal dissection ends at the end of the arteriotomywhere the plaque is sharply transected. Blind proximal endarterectomy, par-ticularly on the left side, may disrupt flow into major proximal branches,including the circumflex artery, a ramus artery, or septal branches.
It is possible to close the artery directly if the coronary artery is large, butusually a patch of vein or artery is used. Patch closure can be a free vein patchwith subsequent incision of the patch for anastomosis of the bypass graft.Alternatively, the bypass graft, whether artery or vein, can be spatulated thelength of the arteriotomy to create an end-to-side anastomosis with a longtongue. A third technique has been described for saphenous vein in which twocircumferentially equidistant longitudinal incisions one-half the length of the
272 Chapter 15
arteriotomy are made in the vein to create two venous flaps with the body ofthe vein placed in the center to create a T anastomosis.
Anastomotic bleedingAfter each anastomosis is created it is important to check for bleeding and fixthe leak on the non-beating heart. We run antegrade cardioplegia at 30–40 mmHg down the graft spraying saline on the site to assess bleeding. If a major leak is identified, a 7–0 prolene suture on a small needle is used forrepair as the vessel is gently distended. Blind suture placement in a collapsedvessel jeopardizes the integrity of the anastomosis. Large repair bites can distort the anastomosis.
Construction of the proximal anastomosisWe use a single clamp technique to perform proximal anastomoses on theaorta. We avoid partial cross clamping because of the risk of embolization withrepeated manipulation of the aorta. The disadvantage of this technique is thatcross clamp time is prolonged. However, with current cardioplegia antegradeand retrograde protection seem to support this strategy. Recent increase in theuse of Y-grafting has eliminated the need for this as the proximals have beenalready constructed prior to application of the cross clamp.
For constructing proximals on the aorta it is important to create a visual estimate of where these grafts should lie while the heart is beating prior toapplication of the cross clamp. With the heart arrested one can then estimatethe location of the proximals that would allow the grafts to lie well. It is import-ant to orient the grafts along the longitudinal axis to avoid a twist which cansometimes be difficult to recognize. If the anastomosis is completed before atwist is recognized, the proximal should either be re-done or the vein can bedivided and a venovenotomy created. We recommend the former.
In order to measure the length of the graft the heart must be filled, all peri-cardial tacking sutures that elevate the heart should be released, and the con-duit should be gently distended. These maneuvers help avoid the problemwith having a short or long graft. The conduit is then cut obliquely at an angleleaving approximately 0.5 cm of extra length from the point of desired ana-stomosis to the aorta. The vein is spatulated for 5–7 mm to allow the creation ofa ‘cobra-hood’ anastomosis. Using an 11-blade, 3–4-mm incisions are made inthe aorta and a 4- or 5-mm aortic punch is used to remove circular segments ofthe aortic wall. A parachute technique is used to sew the graft with the needletraversing the aorta from inside to outside. Full intimal bites are important to avoid the dreadful possibility of aortic dissection once the heart resumesejection. If a soft accessible plaque is encountered it should be removed. Ifremoval is not technically possible then suturing must be done in such a wayas to ensure the plaque is tacked to the aortic wall. Sometime the aortic wallmay be diseased with only a limited area for proximal anastomosis. In this case a second vein graft can be taken off from the hood of the first vein graft by making a 5-mm incision on the hood. For free arterial grafts, we prefer this
Complications of coronary artery bypass surgery 273
technique as opposed to taking them directly off the aorta. Occasionally afterthe initial punch it is apparent that the aortic wall is too diseased for a satisfact-ory anastomosis. One solution is to enlarge the aortotomy and cover the defect with a pericardial patch. The proximal anastomosis can then be made tothe patch. If the aorta is extensively diseased, then ascending aortic replace-ment with a Dacron graft may be necessary. The conduits can be placed to theDacron graft.
Flow capacityIn contrast to the saphenous vein, ITA flow capacity is limited and relates tothe diameter (2 vs. 5 mm) or cross-sectional area of the conduit. This obviousdifference raises concern as to whether or not the ITA can supply adequateflow, particularly at times of increased need (i.e. after cross-clamp release orduring exercise). Intraoperative measurements with an electromagneticflowmeter or more recently with a transit-time flowmeter demonstrate thatbasal flows are comparable for the ITA and saphenous vein but that reactivehyperemic flows or those induced by intracoronary papaverine are signi-ficantly greater for saphenous vein [24]. In other reports, ITA flow is less thanfor saphenous vein, probably because of competitive flow in the native coron-ary artery [25].
Clinical studies [26] and earlier observations that ITA grafts enlarge overtime in accordance with flow demand indicate that ITA grafts have the capac-ity to grow to meet physiological demands of the myocardium. Nevertheless,there may be perioperative situations or times of stress in the postoperativeinterval when myocardial flow requirements are not met by an ITA graft. Awell-documented instance occurs during reoperative coronary bypass. If a dis-eased but patent vein graft to an occluded left anterior descending coronaryartery is ligated and replaced with an ITA graft, the new graft may not imme-diately provide adequate perfusion of affected myocardium [27].
Solutions to problems during CABG
Aortic tearAortic tears may result from application of non-padded clamps to the ascend-ing aorta. Tears vary from a limited transmural lesion to aortic dissection.Local tears are usually repaired with a 4–0 polypropylene running horizontalmattress suture without additional supporting tissue. If the aorta is fragile,two strips of pericardium are added. Alternatively, interrupted horizontalmattress sutures of 4–0 polypropylene with felt pledgets or with strips of feltare used to close the tear. Pericardium is easier to work with than Dacron for suturing to the aorta or vein graft. However, because long-term data onpericardial patches apply only to small patches, and because of concern aboutaneurysm formation, Dacron is used for large aortic patch repairs.
If the injury is related to the aortic cannula, the cannula may have to bemoved to the femoral artery to allow satisfactory repair of a tear or localized
274 Chapter 15
dissection. The aorta should not be repaired under arterial pressure as the tearwill extend and the aorta will rupture. If a partial exclusion clamp or crossclamp does not give clear access to the injury, profound hypothermia with circulatory arrest may be necessary to repair the aorta. In this setting, directsuture may be inadequate, and a pericardial or Dacron patch or tube graft maybe needed. Similarly, if the dissection has propagated beyond the local area,hypothermic circulatory arrest is necessary for inspection of the tear, evalu-ation of the arch and aortic replacement with a tube graft.
Root dissectionWhen aortic root dissection occurs, the ascending aorta must be resected. Thisrequires cardiopulmonary bypass with femoral artery cannulation and provi-sion for profound hypothermia (18 °C or less) and an open distal anastomosis.Usually the aortic valve can be resuspended. Vein grafts are attached to theDacron graft after it has been placed. If vein grafts were anastomosed to theaorta before the dissection occurred and are not involved in the dissection, anisland patch can be placed in the anterior wall of the Dacron tube graft.
De-airing of aortic rootOnce the anastomoses are near completion, the heart is filled to allow for passive de-airing of the aortic root before the last suture is placed and tied.Administration of warm retrograde blood, with gentle suction on the aorticroot vent, would allow for active de-airing of the root. If visible air remains inthe vein grafts, a soft clamp can be placed on the vein and air removed with asmall stab using a 27-G needle. The goal of all these maneuvers is to prevent airembolization to the coronaries, a frequent cause of myocardial dysfunctionand arrhythmias, particularly ventricular fibrillation. If air appears to haveembolized or wide QRS complexes are seen, increasing the mean arterial pressure to 90–100 mmHg may help in ‘washing out’ the air. Defibrillation of the heart should be attempted with the heart empty and non-ejecting.Lidocaine, calcium, and magnesium administration will help in cardioversion.If it appears that the ventricular fibrillation is refractory, amiodarone bolus at adose of 150 mg followed by electrical cardioversion is usually successful.Restoration of a rhythm and contractility are important elements to preventthe non-beating perfused heart from becoming edematous. Myocardial edemaleads to postoperative ventricular dysfunction and the need for inotropic sup-port, which can further deplete the cardiac energy stores and also predisposeto postoperative arrhythmias.
Reperfusion of the heartDuring the period of reperfusion and myocardial recovery all anastomosesshould be checked for bleeding. Small needle stick bleeders should not befixed. There are now many topical hemostatic agents available that can be usedif bleeding continues after heparin reversal with protamine. Epicardial pace-maker wires are also placed in all cases to facilitate separation from CPB. The
Complications of coronary artery bypass surgery 275
ability to control heart rate in the postoperative period can assist in manag-ing blood pressure and cardiac output without the need to add pharmacolo-gical support. The wires should be positioned on the ventricle and atria in afashion that the bare wires would not contact each other and short out. Finally,careful attention to the placement of the wires with respect to the position ofthe grafts is essential. If the wires are placed crossing under the grafts, at thetime of wire removal a graft may be inadvertently avulsed or a side branchmay be torn.
During the reperfusion period we also study the flow through the conduitswith a Doppler flow probe.
Failure to separate from cardiopulmonary bypassSeparation from cardiopulmonary bypass may be directed by the anesthesiolo-gist or the surgeon, but even if the former, the surgeon must have an intimateknowledge of the process and its physiology. During and after separation fromCPB we routinely evaluate the heart by transesophageal endocardiography.Presence of new functional abnormalities in the coronary territory revascular-ized or new mitral regurgitation should raise suspicion regarding the ade-quacy of the target and patency of the graft. Vascular spasm, specifically inarterial conduits, can manifest as such. The ITA has less spasm than other arter-ial conduits, presumably because it contains less smooth muscle in the media.Spasm can be treated with a variety of drugs applied topically or systemically.We generally apply papaverine (2 mg/ml) mixed with heparinized blood topically on the conduits. Systemic nitroglycerin, nitroprusside, or one of thecalcium channel blockers can also be administered. In addition, axial orienta-tion of the conduits should be checked again. If a graft is too long and kinks,then a gentle curve should be given to the graft to remove kinking. The conduitcan be tucked in that position by epicardial to adventitial suturing.
Failure to separate from CPB with reasonable hemodynamics, low cardiacindex (CI), poor ventricular function (specifically if regional and associatedwith poor graft flow) should prompt revascularization of that territory with avein graft. If the surgeon is familiar with off-pump techniques then repeatcross clamping is not necessary and this is ideal. Currently available stabilizersare excellent in providing a stable platform for beating heart coronary bypasssurgery.
If the surgeon is not familiar with techniques of off-pump CABG then it isnecessary to reclamp, arrest the heart and perform the distal anastomosis. Theaortic clamp can then be removed and the proximal taken off from a previ-ously vein graft to minimize the period of arrest. If after the new graft is placed,CI remains low or regional abnormalities persist, consideration should begiven to placement of intra-aortic balloon pump (IABP). The mortality associ-ated with postcardiotomy shock following CABG is high. If after inotropicsupport and IABP the CI still remains low, immediate consideration should be given to biventricular mechanical support. In these situations the problemmay be secondary to poor myocardial preservation with global myocardial
276 Chapter 15
stunning or MI. Isolated left ventricular support is rarely the solution and consideration should be given to biventricular support and decompression ofthe heart to ‘rest’ the myocardium. Low flows should be maintained throughthe heart to prevent thrombosis. Patients should then be transferred to centreswith transplant and device expertise.
Postoperative complications
Early conduit failureThe incidence of perioperative MI is between 3 and 7% in most series [28,29],but with better cardioplegia techniques these numbers are probably lower.Early graft failure may manifest in the ICU with arrhythmias, low output state,increase in pulmonary artery pressure, or ECG changes.
Some conduits fail because of unrecognized harvest injury or injury sus-tained during graft preparation (instrumentation, excessive dilatation).Technical errors include large bites, deep bites, back walling, trauma to ITAduring handling, and stenosis caused by linear tension or pursestring effect ona small anastomosis.
Perioperative MI increases the risk of additional mortality and morbidity 2.5times compared with patients who do not have infarction [29]. An aggressiveapproach in this setting is warranted. Immediate echocardiography can definewall motion abnormalities. Emergency angiography can identify conduitspasm which can be treated with direct intravascular injection of nitrates orcalcium channel blockers. In addition, percutaneous interventions or surgicalinterventions could be promptly instituted depending on the findings onangiography [28]. We generally continue nitroglycerin in the perioperativeperiod because of concerns with spasm, particularly with the radial artery.Aspirin is given soon after arrival to the ICU either via nasogastric tube or as asuppository. In patients who have had endarterectomy, Plavix 75 mg is givenas soon as it is ascertained that there is no bleeding.
Pericardial tamponadeEarly pericardial tamponade typically occurs as a result of ongoing mediast-inal bleeding. Increase in central venous pressure (CVP), or pulmonary arterypressure in the setting of low cardiac output is generally indicative of cardiactamponade. Although the classical teaching is that the CVP and pulmonaryartery pressures ‘equalize’, this clinical scenario may not necessarily be pre-sent after an open procedure. Localized clot may cause compression in onearea sufficiently to compromise venous return but not cause pressure equal-ization [30]. The typical scenario is a patient who bleeds postoperativelyreceives blood products and has a sudden decrease in chest tube drainage withassociated decreased cardiac output. Chest X-ray may or may not demonstratea widened madisterium. Echocardiography is helpful but often delays inter-vention and does not provide adequate windows for evaluation. If the clinicaldiagnosis of tamponade is even a remote possibility, emergent return to theoperating room and re-exploration is mandatory. This is particularly true with

Complications of coronary artery bypass surgery 277
primary CABG patients who have excessive bleeding. In this case our thresh-old for re-exploration is even lower. Delay in treatment can be fatal. In theoperating room the surgeon should be scrubbed and ready to open chest withthe prep being carried out by others. It is very common that upon induction ofanesthesia, with removal of the sympathetic tone, the blood pressure wouldprecipitously fall resulting in cardiac arrest. If the patient remains stable, drap-ing is done as to only expose the skin incision with wires and chest tubes out ofthe area to minimize contamination.
Upon entering the chest all clots should be carefully removed without jeop-ardizing the grafts that may be buried under. Warm saline irrigation can helpin cleaning the mediastinum. We typically pack the chest and initiate a searchfor the bleeder by removing the packs sequentially and looking in a systematicway in each area. Aortic, venous, and cardioplegia cannulation sites should beinspected. The conduits should be checked for branch site bleeding. The medi-astinum, thymic remnant, ITA harvest site and sternal wire areas should all beinspected. Once the patient is hemodynamically stable, the distal anastomosescan be checked. Gently placing packs behind the heart, traction sutures on the pericardium to lift the heart, and rotation of the operating table can aid in visualization without hemodynamic instability. Placing the patient inTrendelenburg can also assist with higher blood pressure as the heart is lifted.Most bleeding should be controllable with gentle compression using topicalhemostatic agents. Once bleeding is controlled the chest must be irrigated withcopious amounts of warm saline. The chest tubes must be cleared and the sternum closed primarily.
Delayed cardiac tamponade generally occurs after 1 week. The etiology isunclear but may be related to anticoagulation, persistent postperioperativemediastinal drainage, or post-pericardiotomy syndrome. Diagnosis is usuallyestablished by echocardiography and the treatment is drainage by surgicalsubxiphoid pericardial window. Percutaneous techniques in this setting areusually unsuccessful because the effusion is thick and loculated.
ArrhythmiasPostoperative supraventricular arrhythmias are common after heart opera-tions. The arrhythmia chapter deals with this matter in detail. In general, wefavor an aggressive approach to treatment of postoperative atrial fibrillationwhich includes pharmacological treatment and electric cardioversion prior toconsidering anticoagulation.
Of particular interest is a history of non-sustained ventricular tachycardia orperioperative ventricular tachycardia. In patients with low ejection fraction orprevious MI, an electrophysiological study is indicated to search for inducibleventricular tachycardia. If found, placement of an automatic internal car-dioverter defibrillator should be considered.
Wound complicationsSternal wound complications are of particular concern in diabetics andpatients with bilateral ITA harvest. The incidence of deep wound infections
278 Chapter 15
ranges from 0.4 to 5% [31]. Risk factors include re-exploration, obesity, pro-longed ventilatory support, immunosuppression and renal insufficiency.
Early aggressive drainage and debridement of the infected sternum are necessary. Areas of bone necrosis must be resected and necrotic tissue must be debrided and the mediastinum irrigated with antibiotic-containing solu-tion. If the bone appears viable, primary closure can be attempted with chesttubes and Jackson–Pratt tubes left in the mediastinum for irrigation anddrainage as needed. If the bone is not viable a complete sternectomy followedby omental or muscular flap coverage is necessary.
Conclusion
The high-risk profile of patients requiring CABG continues to challenge surgeons daily. Meticulous attention to the preoperative selection and intra-operative technical details should minimize the morbidity and mortality ofCABG. Every step can lead to a poor outcome unless care is taken to avoidcomplications and be prepared to fix problems as they arise.
Acknowledgments
We thank Beverly Wolff for her assistance in preparing this manuscript.
References
1 Utley JR, Leyland SA, Edmunds HL. Preoperative evaluation. In: Edmunds, ed. CardiacSurgery in the Adult. New York: McGraw-Hill, 1997.
2 Rawitcher RE, Jones JW, McCoy TA et al. A prospective study of aspirin’s effect on redblood cell loss in cardiac surgery. J Cardiovasc Surg 1991; 32: 1.
3 Anderson RJ, O’Brien M, MaWhinney S et al. Renal failure predisposes patients to adverseoutcome after coronary artery bypass surgery. VA cooperative study #5. Kidney Int 1999;55: 1057–1062.
4 Lemmer JH Jr. Clinical experience in coronary bypass surgery for abciximab-treatedpatients. Ann Thorac Surg 2000; 1986; 70 (2 Suppl.): 533–537.
5 Roach GW, Kanchuger M, Mora-Mangano C et al. Adverse cerebral outcomes after cor-onary bypass surgery. N Engl J Med 1996; 335: 1857–1863.
6 Smith PL, Treasure T, Newman SP et al. Cerebral consequences of cardiopulmonarybypass. Lancet 1986; 1: 823–825.
7 Gillinov AM, Sabik JF, Lytle BW, Cosgrove DM. Axillary artery cannulation. J ThoracCardiovasc Surg 1999; 118: 1153.
8 Lytle BW, Blackstone EH, Loop FD et al. Two internal thoracic artery grafts are better thanone. J Thoracic Cardiovasc Surg 1999; 117: 855–872.
9 Tector AJ, McDonald ML, Kress DC et al. Purely internal thoracic artery grafts: outcomes.Ann Thorac Surg 2001; 72: 450–455.
10 Sundt TM, Barner HB, Camillo CJ, Gay WA, Jr. Total arterial revascularization with aninternal thoracic artery and radial artery T graft. Ann Thorac Surg 1999; 68: 399–404.
11 Calafiore AM, Teodori G, DiGiammarco G et al. Multiple arterial conduits without cardiopulmonary bypass: early angiographic results. Ann Thorac Surg 1999; 67: 450–456.
Complications of coronary artery bypass surgery 279
12 Broadman RF, Frame R, Camacho M et al. Routine use of unilateral and bilateral radialarteries for coronary artery bypass graft surgery. J Am Coll Cardiol 1996; 28: 959–963.
13 Francel TJ, DuFresne CR, Baumgartner WA. Anatomic and clinical consideration of aninternal mammary artery harvest. Arch Surg 1992; 127: 1107.
14 Morin JE, Hedderich G, Poirier NL et al. Coronary artery bypass using internal mammaryartery branches. Ann Thorac Surg 1992; 54: 911.
15 Cunningham JM, Gharavi MA, Fardin R. Consideration in the skeletonization techniqueof internal thoracic artery dissection. Ann Thorac Surg 1992; 54: 947.
16 Higami T, Mauro A, Yareashita T et al. Histologic and physiologic evaluation of skele-tonized internal thoracic artery harvesting with an ultrasonic scalpel. J Thorac CardiovascSurg 2000; 120: 1142–1147.
17 Higami T, Yamashita T, Nohara H et al. Early results of coronary grafting using ultrasonic-ally skeletonized internal thoracic arteries. Ann Thorac Surg 2001; 71: 1224–1228.
18 Utley JR, Thomason ME, Wallace DJ et al. Preoperative correlates of impaired wound heal-ing after saphenous vein excision. J Thorac Cariovasc Surg 1989; 98: 147–149.
19 Isgro F, Weisse U, Voss B et al. Minimally invasive vein harvesting: is there an improve-ment of the results with the endoscopic approach? Eur J Cardiothorac Surg 1999; 16 (Suppl.2): S58–60.
20 Green GE. Internal mammary artery-to-coronary anastomosis: three year experience with165 patients. Ann Thorac Surg 1972; 42: 260.
21 Iaco AL, Teodori G, DiGiammarco G et al. Radial artery for myocardial revascularization:long-term clinical and angiographic results. Ann Thorac Surg 2001; 70: 1378–1383.
22 Calafiore AM, DiMauro M, D’Alessandro S et al. Revascularization of the lateral wall:long-term angiographic and clinical results of radial artery versus right internal thoracicartery grafting. J Thorac Cardiovasc Surg 2002; 123: 225–231.
23 Davila-Roman VG, Barzilai B, Wereing TH et al. Intra-operative ultrasonographic evalu-ation of the ascending aorta in 100 consecutive patients undergoing cardiac surgery.Circulation 1991; 84 (Suppl. 5): 47–53.
24 Barner HB. Blood flow in the internal mammary artery. Am Heart J 1973; 86: 575.25 Navia D, Cosgrove DM, Lytle BW et al. Is the internal thoracic artery the conduit of choice
to replace a stenotic vein graft? Ann Thorac Surg 1994; 57: 40.26 Gurne O, Chenu P, Polidori C et al. Functional evaluation of internal mammary artery
bypass grafts in the early and late postoperative periods. J Am Coll Cardiol 1995; 25: 1120.27 Louagie YAG, Hayhe J-P, Buche M et al. Intraoperative electromagnetic flow meter meas-
urements in coronary artery bypass grafts. Ann Thorac Surg 1994; 57: 357.28 Baur HR, Peterson TA, Arnar O et al. Predictors of perioperative myocardial infarction in
coronary artery operation. Ann Thorac Surg 1981; 31: 36.29 Force T, Hibberd P, Weeks G et al. Perioperative myocardial infarction after coronary
bypass surgery. Clinical significance and approach to risk stratification. Circulation 1990;82: 903.
30 D’Cruz IA, Overton DH, Pai GM. Pericardial complications of cardiac surgery: Emphasison the diagnostic role of echocardiography. J Card Surg 1992; 7: 257.
31 Blanchard A, Hurni M, Ruchat P et al. Incidence of deep and superficial sternal infectionafter open heart surgery: a ten years retrospective study from 1981 to 1991. Eur J Car-diothoracic Surg 1995; 9: 153.
CHAPTER 16
Complications of cardiopulmonarybypass and cardioplegia
Lawrence L Creswell
Introduction
Although cardiopulmonary bypass (CPB) and the use of cardioplegia formyocardial protection are used routinely today in the practice of cardiovascu-lar surgery, these are both relatively new techniques. The potential utility ofextracorporeal circulation was recognized in 1813, when Le Gallois wrote:
‘But if the place of the heart could be supplied by injecting and if, with a regular continuance of this injection, there could be furnished a quantity ofarterial blood, whether naturally or artificially formed, supposing such afunction possible, then life might be indefinitely maintained in any portion.’[1]
Bruchonenko was the first to suggest that extracorporeal circulation might beuseful clinically. Using a circuit with a roller pump and excised canine lungsfor oxygenation, he was able to support the arrested canine heart for severalhours. A pump circuit of this design was later used for successful valvularheart surgery in animal models in the 1930s and early 1940s.
Credit for the first successful clinical use of a pump-oxygenator, the fore-runner of today’s modern CPB machine, goes to John H. Gibbon Jr, MD. Hisvision for this device dates to 1930 when he was caring for a patient who diedof massive pulmonary embolism. At that time, he wrote:
‘During the 17 h by this patient’s side, the thought constantly recurred thatthe patient’s hazardous condition could be improved if some of the blueblood in the patient’s distended veins could be continuously withdrawninto an apparatus where the blood could pick up oxygen and discharge car-bon dioxide and then pump this blood back into the patient’s arteries.’ [1]
Gibbon also recognized the importance of heparin, which became availablein sufficient quantities only in the late 1930s. Development of his pump oxy-genator continued during the 1940s in laboratory animals. Even at this earlystage, the potential complications associated with CPB were recognized byGibbon and he made refinements related to the problems of hemolysis, airembolism, and the unwanted effects of a blood–surface boundary. The first
280
Complications of cardiopulmonary bypass and cardioplegia 281
clinical use of his pump oxygenator took place in 1952 in an infant with sus-pected atrial septal defect. The attempted use of the pump oxygenator in thispatient and two other early patients was unsuccessful. The first successfuloperation using the pump oxygenator took place on 6 May 1953, when anatrial septal defect was repaired using a 26-min period of extracorporeal sup-port [2].
As more complex cardiac operations became possible with the use of thepump oxygenator, it became apparent that there were still limitations imposedby the beating heart and the return of bronchial blood into the operating field. The technique of intentional cardiac arrest imposed by the injection ofpotassium chloride solution dates to animal studies from the early 1900s [1].Melrose was the first to report in 1955 the technique of induced cardioplegicarrest of the heart during heart surgery, using injection of potassium citratesolution, or cardioplegia, directly into the aortic root after cross-clamping of the aorta [3]. The alternative technique of retrograde, or coronary sinus cardioplegia was introduced by Lillihei who reported its use during an aorticvalve replacement in 1956 [4]. Both of these techniques have come intowidespread clinical usage.
The development and clinical application of CPB and modern techniques of myocardial protection have allowed a wide array of cardiopulmonary operations that would not otherwise be possible. These techniques, however, are associated with a variety of complications and pathophysiological con-sequences that affect nearly every patient in whom they are applied. Thischapter focuses on the complications associated with the clinical use of CPB and myocardial protection, which are presented in five sections: (i) themechanics of CPB and related complications; (ii) monitoring for CPB andrelated complications; (iii) anticoagulation for CPB and related complications;(iv) the pathophysiological consequences of CPB; and (v) the complications of cardioplegia. Many of these complications may also be covered in otherchapters of this book that focus on specific organ systems (e.g. pulmonary,renal, neurological) or the complications related to specific cardiac operations(e.g. coronary artery bypass surgery, aortic surgery, valvular heart surgery).This discussion is necessarily a summary of the most important aspects of CPB and the related complications. The reader is referred to other, excellent texts on cardiac surgery in adults [5], the techniques of cardiopulmonary bypass[6–8], and cardiothoracic anesthesia [9,10] for additional information.
Mechanics of cardiopulmonary bypass and relatedcomplications
Components of the cardiopulmonary bypass circuit and related complicationsCPB is used to facilitate many cardiac operations today. Although the featuresof the cardiopulmonary bypass circuit and the conduct of CPB will vary frominstitution to institution, and may vary with the special requirements dictated
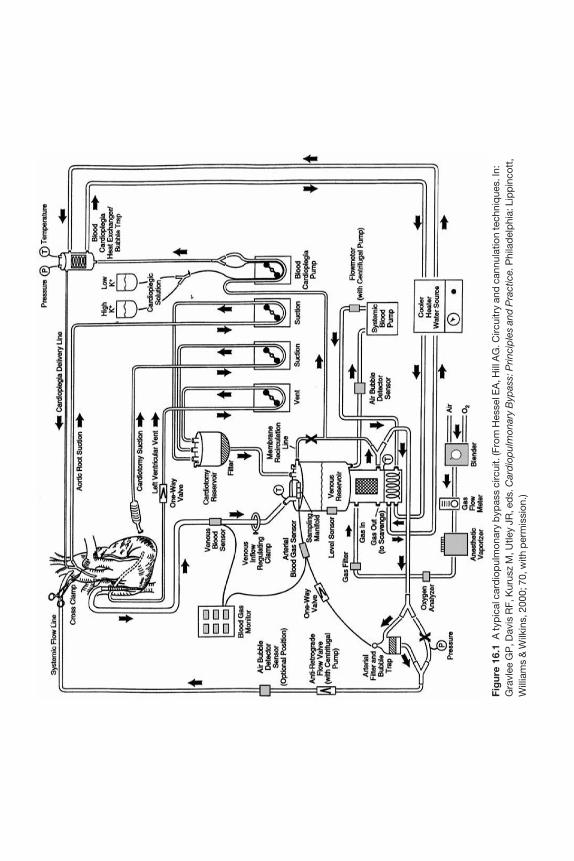
Fig
ure
16.1
A ty
pic
al c
ard
iop
ulm
onar
y b
ypas
s ci
rcui
t. (F
rom
Hes
sel E
A, H
ill A
G. C
ircui
try
and
can
nula
tion
tech
niq
ues.
In:
Gra
vlee
GP
, Dav
is R
F, K
urus
z M
, Utle
y JR
, ed
s. C
ard
iop
ulm
onar
y B
ypas
s: P
rinci
ple
s an
d P
ract
ice.
Phi
lad
elp
hia:
Lip
pin
cott
,W
illia
ms
& W
ilkin
s, 2
000;
70,
with
per
mis
sion
.)

Complications of cardiopulmonary bypass and cardioplegia 283
by a particular operative procedure, many features are common to all ap-plications [11]. A typical cardiopulmonary bypass circuit is presented inFigure 16.1. Many of the mechanical complications associated with the use of cardiopulmonary bypass are related to the individual components of the circuit.
Venous cannulasVenous cannulas are available in a variety of designs, materials, and sizes and are often categorized as either 1-stage (atrial) or 2-stage (cavo-atrial). Thevenous cannulas may be wire-wound or made from hard synthetic materialsto prevent kinking. Thin metal, rather than thicker plastic, tips may increasethe effective size of a given cannula. The simplest method for atrial can-nulation is with a single venous cannula (either 1-stage or 2-stage). For mostoperations in which the right side of the heart is entered, however, bi-cavalcannulation is required. With bi-caval cannulation, caval occlusion, often withumbilical tape secured around the cannulas, provides a clear operative fieldfor operations on or through the right side of the heart.
Venous cannulationDuring venous cannulation, atrial arrhythmias or untoward hemodynamiceffects may be caused by manipulation of the heart. This is particularly true if the heart must be retracted leftward and superiorly for placement of inferiorvena cava (IVC) cannulation sutures. These hemodynamic effects are usuallytransient, but electrical cardioversion for atrial arrhythmias may be necessaryand the appropriate equipment should be available during cannulation. Thepotential for arrhythmias may be increased if the systemic temperature isallowed to drift too low during opening and cannulation. In situations inwhich bi-caval cannulation will be used, IVC purse-string sutures can beplaced and cannulation can be performed after CPB is initiated (i.e. with onlysuperior vena cava (SVC) cannulation) to help avoid hemodynamic difficul-ties. Incisions in the atrium or vena cavae should be made carefully to preventinadvertent extension of these incisions and unwanted bleeding. The fingersshould be used to confirm the correct position of the venous cannulas duringinsertion. Without proper care, venous cannulas may be placed inadvertentlyin a variety of locations, including the innominate vein, the hepatic veins, thecoronary sinus, or even through a septal defect to the left side of the heart.Caval tapes should be used carefully because they may tear or lacerate theatrium or vena cavae, particularly with retraction (i.e. as for mitral valve operations). After the termination of CPB, cannulation incisions in the SVCshould be closed carefully to prevent narrowing of the SVC [12]. This problemcan be avoided in many situations by inserting the SVC cannula through apurse-string in the right atrial appendage. Inadvertent narrowing of the cannulation incision is usually not a problem for incisions in the right atrium.
Pre-existing central venous or pulmonary artery catheters may be dis-placed or dislodged during cannulation. The surgeon must be aware of this
284 Chapter 16
possibility and the anesthesiologist must monitor for this type of complication.On rare occasions, purse-string sutures may entrap or injure one of thesecatheters and may necessitate reoperation for removal of the affected catheter[13,14]. Transesophageal echocardiography (TEE) may sometimes be useful to identify these problems [14]. With the use of caval occlusion tapes, monitor-ing lines caught between the tape and the venous cannula may be rendereduseless temporarily or even damaged permanently. In practice, it may be helpful to ‘pull back’ the pulmonary artery catheter before caval tapes aretightened and then advance the catheter once again when the caval tapes arereleased.
During venous cannulation, it is important for the surgeon to be aware of thepossibility of a persistent left superior vena cava (LSVC). This anomaly is pre-sent in approximately 0.5% of the general population, but it is more common inpatients undergoing cardiac surgical procedures, and particularly those withcongenital heart disease. When a 2-stage venous cannula is used, the presenceof a persistent LSVC is not usually a problem. When the right heart must beentered and bi-caval cannulation is used, the extra return of blood through the coronary sinus may pose difficulties, however. If the innominate vein isnormal in size, the persistent LSVC may simply be occluded during CPB. If theinnominate vein is small or absent, occlusion of the persistent LSVC duringCPB may produce venous hypertension and possibly neurological injury.Alternative approaches in this situation include the use of a cardiotomy suc-tion device placed in the orifice of the coronary sinus through the open rightatrium or direct (retrograde) cannulation of the persistent LSVC and the use ofan occlusion tape around this vessel.
Venous air embolism may occur during insertion of venous cannulas [15]. If an intracardiac shunt is present, this situation may potentially result in systemic air embolism.
Before CPB is initiated, the presence of venous cannulas in the right atriummay obstruct the ordinary venous return to the heart and interfere with properhemodynamics. This unwanted side-effect is most pronounced with bi-cavalcannulation. If obstruction to proper venous flow produces persistent hemo-dynamic instability, CPB should be initiated immediately.
Peripheral venous cannulation (rather than direct atrial cannulation) may beuseful in circumstances such as cardiopulmonary arrest outside of the operat-ing room, during redo operations before the repeat sternotomy, and in certainaortic surgery procedures. In these circumstances, the use of as large a venouscannula as possible will help to facilitate adequate CPB. When possible, aperipheral venous cannula should be advanced into the right atrium, usingeither palpation, measurement of the length of the cannula, or TEE to guideproper placement. A variety of commercially available thin-walled cannulas,often with guide-wire or other introducer systems, are available for use in thissituation. When peripheral vessels are cannulated under direct vision using acutdown approach, special care should be used after decannulation to closethe venotomy without narrowing the vessel.
Complications of cardiopulmonary bypass and cardioplegia 285
Venous reservoir and drainageWhen a membrane oxygenator is used, the venous reservoir is placed in thecircuit immediately before the pump. This device also serves as a gross bubbletrap for all blood that returns to the perfusion circuit from the venous line and from cardiotomy suction lines. The venous reservoir may be constructedof heavy plastic or a collapsible plastic bag. Advantages of the heavy plasticvariety include: ease of measuring blood volume in the reservoir, ease of prim-ing, and the ability to attach a vacuum suction for assisted venous drainage, ifdesired. The collapsible type may be advantageous because it eliminates someof the blood–air interface and may help to prevent inadvertent air embolism.The collapsible type is more susceptible to damage (i.e. tearing), however.Regardless of the type of venous reservoir, this device provides the perfusion-ist with a ready source for volume infusion into the patient and also a safetymargin if the venous return is interrupted during CPB.
In most applications of CPB, the venous drainage is accomplished simply bysiphon effect (due to gravity) to the venous reservoir which is placed below thelevel of the patient. The amount of venous drainage is affected by: (i) the heightof the patient above the venous reservoir, (ii) the central venous pressure, and (iii) the resistance of the venous cannulas and circuitry. The relationshipbetween the central venous pressure and these factors is given by: Pvsys = f [(Q,viscosity)/(cannula size, venous line size, venous line suction)], where Pvsys isthe mean systemic venous pressure and Q is the systemic blood flow [16]. Thegoal during CPB is to maintain the systemic venous pressure as low as pos-sible. Inadequate venous drainage will limit the ability of the perfusionist tomaintain an adequate flow rate and can be due to one or more related factors.The venous drainage can be improved by: (i) elevating the patient in relation to the venous reservoir; (ii) increasing the venous cannula size (the sum of the cross-sectional areas of all venous cannulas in use); (iii) increasing thediameter of the venous line; or (iv) the use of venous line suction (augmentedvenous drainage).
Augmented venous drainageThe technique of augmented venous drainage may be useful in a variety of clinical situations, but is particularly useful when long, relatively narrowvenous cannulas are needed (e.g. for minimal access procedures). Two generaltechniques are available. In the first technique, either a roller or a centrifugalpump is placed in the venous line between the patient and the venous re-servoir. When a roller pump is used, the perfusionist must be careful to mon-itor the pump speed continuously to prevent the build-up of excessive negativepressure that may cause the right atrium or great veins to collapse around thecannula. The use of a centrifugal pump may decrease this risk. In either case, a‘shunt’ placed around the pump may reduce the risk of excessive negativepressure. The venous line pressure should be measured near the pump andkept < – 60 to – 100 mmHg [17]. The second general technique involves theapplication of a vacuum directly to the venous reservoir. This approach is

286 Chapter 16
simpler and avoids the use of a second pump. Application of 20–60 mmHgvacuum to the venous reservoir is usually adequate and safe.
Although augmented venous drainage may facilitate operative proceduresthat would otherwise be more difficult, there are several potential risks. Themost obvious problem relates to the increased risk of air entry into the venouscircuit from holes in the heart or around the venous cannulas. Air may alsoenter the heart through central venous catheters or introducer sheaths thatmay be in place [18]. In most circumstances a small amount of air in the venousside of the circuit will be well tolerated, but large amounts of air that accumu-late at the venous reservoir may predispose to systemic air embolization. In addition, if a second pump is used in the venous circuit, the perfusionistmust be vigilant to keep the venous drainage and systemic flow balanced. If not, dramatic changes in the patient’s intravascular volume may occur veryquickly. Lastly, hemolysis may result from excessive negative pressures in thevenous line [19,20].
Arterial cannulasA wide variety of arterial cannulas are available for clinical use. Differences in their materials and design facilitate their use in different arteries, both central and peripheral, during cannulation. The arterial cannula is typicallythe narrowest portion of the perfusion circuit. As a result, the arterial cannulais subject to relatively large pressure gradients across the cannula. As a generalrule, the shorter the narrow segment of the arterial cannula, the lower the pressure gradient will be. As an example, a long, uniformly narrow cannulawill be highly resistant to flow and there are few examples of this type ofdesign. Ordinarily, arterial cannulas narrow only at or near their tip to min-imize this problem. At the tip, the use of hard plastic or metal may be used toincrease the inside diameter (ID) to outside diameter (OD) ratio and minimizethe pressure gradient. Hemolysis and protein denaturation may occur with pressure gradients of > 100 mmHg [21]. Regardless of the design of thearterial cannula, high-velocity jets of blood exiting the cannula and enter-ing the cannulated artery may produce localized damage such as tearing, dislodgement of calcific plaque (producing circulating emboli), or arterial dissection. Devices such as the EMBOL-X Intraaortic Filtration System(EMBOL-X Inc., Mountain View, CA, USA) have shown promise in the ex-traction of particulate debris at the arterial cannula tip, but the clinical utility of these devices is yet to be proved [22]. These devices are promising sincecerebral macroembolism is thought to be a major determinant of neurologicalinjury after CPB [23–25].
Arterial cannulationArterial cannulation for cardiac surgery can be accomplished through a variety of arteries. In adult cardiac surgical procedures, the aorta is the mostcommon site for arterial cannulation, but other arteries such as the femoralartery or axillary artery may also be used.
Complications of cardiopulmonary bypass and cardioplegia 287
Aortic cannulation The aorta is easily exposed through the standard mediansternotomy incision and is a relatively safe site for cannulation. Dislodgementand circulation of emboli from calcific plaque from the aorta is thought to beresponsible for many of the neurological complications associated with car-diac surgery [23–25]. Embolization can be due to either direct manipulation of the aorta during cannulation or due to the effects of a high-velocity jet ofblood striking the inner surface of the diseased aorta. Embolism of very smallparticles may produce no symptoms at all in many patients, but these smallparticles may be responsible for some of the neurocognitive changes encoun-tered postoperatively in some patients [26–31]. Aortic cannulas with sideholes, instead of end holes, near the tip may help to disperse blood as it entersthe aorta and help to limit embolic injury [32].
Several techniques are available to help prevent inadvertent embolization.The surgeon should use manual palpation of the ascending aorta and exposedportion of the aortic arch and proximal great vessels to evaluate for the presence of calcific plaque. It is important to be sure that the planned sites for arterial cannulation, cardioplegia cannulation, aortic cross-clamping, andproximal anastomoses are free from significant disease. Unfortunately, man-ual palpation alone can underestimate the extent of atherosclerotic disease inthese vessels [33–37]. With the introduction and increasingly widespread useof TEE during cardiac surgical procedures, this is another technique that canbe used to assess the extent of atherosclerosis in the ascending aorta. AlthoughTEE may not be able to image the mid-portion of the aortic arch completely,this technique can be used to assess the ascending and descending portions ofthe aorta [36–38]. More recently, epiaortic ultrasound has become the mostsensitive method for the detection of significant atherosclerotic disease in theascending aorta before cannulation [36,37]. With this technique, an ultrasoundprobe in a sterile sheath is passed into the operative field. The pericardium isfilled with saline and the probe is placed directly on the aorta to create cross-sectional or longitudinal images. When significant disease is discovered, theoperative plan can be changed in response to the findings: (i) an alternative site for arterial cannulation such as the axillary artery or femoral artery may beselected; (ii) sites that are free of disease can be selected for cannulation, aorticcross-clamping, and siting of proximal anastomoses; (iii) for patients requiringonly CABG, an off-pump approach might be selected; and (iv) a decision canbe made in certain cases to replace the ascending aorta in addition to the originally planned procedure.
When aortic cannulation is performed, most surgeons place a single or twoconcentric purse-string sutures directly in the anterior surface of the ascendingaorta. Often, the adventitia is cleared within the purse-string suture(s) beforecannulation. The systemic blood pressure should be kept in the low normalrange during aortic cannulation to help prevent the complications of aortic tear or dissection. Intraluminal placement of the cannula is suggested by back-bleeding into the cannula and the presence of a pulsatile blood pressure in the arterial line. Back-bleeding into the cannula may also facilitate removal of

288 Chapter 16
small particulate debris dislodged at the cannulation site as well as smallamounts of entrained air. The tip of the aortic cannula should be directedtoward the central portion of the aortic arch.
A variety of complications are possible during or due to aortic cannulation.First, it may not be possible to introduce the cannula properly. This may be dueto too small an opening, to fibrosis of the aortic wall, or to calcific plaque at thesite of cannulation. It may be possible to insert the cannula tip into an intramu-ral location; in this case, an improper cannulation may not be noticed untilthere is obstruction to blood flow and a high perfusion pressure is noted by theperfusionist when CPB is initiated. Too vigorous an introduction of the can-nula may result in tearing at the cannulation site or to injury to the back wall ofthe aorta. Poor positioning of the tip of the cannula may result in ‘retrograde’cannulation, with the tip pointing toward (or even through) the aortic valve.Other undesirable locations for the cannula tip include the head vessels or in aposition firmly against the aortic wall itself; these positions may be suggestedby high line pressures when CPB is initiated. Intramural hematoma may occurat the site of cannulation and is treated by prompt incision of the adventitia.Antegrade aortic dissection during cannulation occurs in < 0.1% of cases and is suggested by a sudden enlargement and bluish discoloration of the aorta,sudden bleeding from cannulation sites, and difficulties with venous returnand arterial inflow [38–41]. Although this complication can be treated occa-sionally by suture plication of the ascending aorta, more often CPB must be re-established via an alternative route (e.g. femoral artery) to facilitate repair orreplacement of the ascending aorta.
Immediately after decannulation, any bleeding at the aortic cannulation site can usually be controlled by placement of additional sutures. Late com-plications after aortic cannulation may include recurrent hemorrhage or thedevelopment of a pseudoaneurysm [42].
Femoral artery cannulation Femoral artery cannulation is used when theascending aorta is not available for arterial cannulation (e.g. aneurysm or dissection of the ascending aorta, minimal access surgery with poor exposureof the ascending aorta). Although femoral cannulation can be accomplishedpercutaneously, more often the femoral artery is exposed surgically, neces-sitating an additional surgical incision. Complications related to femoral cannulation include: direct injury to the femoral vessel, bleeding, dissection,formation of a pseudoaneurysm, formation of a lymphocele, nerve injury, retrograde dissection of the aorta [43,44], and embolism (either air or calcificdebris) to the distal extremity.
During CPB with femoral cannulation, the distal extremity may becomeischemic. With prolonged ischemia, tissue necrosis and the development of compartment syndrome in either the calf or thigh may occur [45]. As analternative to direct cannulation, a graft (e.g. PTFE, Dacron) can be suturedend-to-side to the femoral artery to allow introduction of the arterial cannulawhile maintaining distal perfusion. Alternatively, a second, smaller caliber
Complications of cardiopulmonary bypass and cardioplegia 289
perfusion cannula can be placed in the femoral artery distal to the site of cannulation to provide distal perfusion to the extremity.
Femoral cannulation and subsequent ‘retrograde’ perfusion may result in ‘retrograde’ embolism if any calcific debris is dislodged from the femoral,iliac, or descending aortic vessels. TEE can be used to screen for the presence of atherosclerosis in the descending aorta and if there is severe disease (andespecially, for cases in which there is loose or ‘hanging’ debris), an alternativesite for cannulation (e.g. axillary artery) should be selected.
Axillary artery cannulation The axillary artery has recently been advocatedfor situations in which cannulation of the aorta or the femoral artery is not possible or desired [46,47]. The right axillary artery is typically favored overthe left. The axillary artery is less likely than either the aorta or femoral arteryto be heavily involved with atherosclerosis. In addition, there is good collater-alization around this artery, and if a separate incision is used for cannulation,wound healing is often better than for a groin incision. The axillary artery canbe cannulated directly or through a small caliber graft that is attached to theaxillary artery in end-to-side fashion.
Pump oxygenatorThe two basic types of oxygenators in use today are the membrane oxygenatorand the bubble oxygenator [48]. The membrane oxygenator is used almost universally worldwide, however. The ‘oxygenator’ is responsible for both oxygenation and ventilation (e.g. CO2 removal). For the typical microporousmembranes (usually hollow fiber), there is direct contact between the bloodand the membrane only at the outset of CPB. A thin protein coating then formson the membrane quickly after the initiation of CPB and prevents direct contact between the blood and the membrane thereafter. Ventilation is con-trolled by the rate of gas flow and oxygenation is controlled by adjusting the oxygen fraction in the gas supplied to the oxygenator. There is a relativelyhigh resistance to flow across the membrane, so blood must be pumped acrossthe membrane before returning to the patient via the arterial line.
Compared with bubble oxygenators, the use of a membrane oxygenator is associated with less hemolysis [49]. Studies have shown that, regardless ofthe type of oxygenator, there is reduced red blood cell survival after CPB [50].The membrane oxygenator may also be associated with reduced complementactivation, granulocyte activation, and platelet activation [49,51–53]. Some,but not all, studies have also shown less cerebral microembolism with mem-brane than with bubble oxygenators [54,55]. When an arterial filter is used,these differences are less pronounced, however. Recently, heparin-coated oxy-genators have become available and have been advocated because of potentialreductions in the subsequent systemic inflammatory response [56,57].
Bypass pumpA pump is placed in the perfusion circuit to provide forward flow of blood

290 Chapter 16
through the circuit and back to the patient. Two general types are available:roller pumps and centrifugal pumps [58]. Each has relative advantages anddisadvantages as well as its own set of potential complications. Even if a centrifugal pump is used as the primary pump, roller pumps are typicallyused for delivery of cardioplegia and the operation of any cardiotomy or ventsuction lines.
With the roller pump, a length of tubing is placed in a curved ‘raceway’which is adjacent to a set of rollers. Forward flow is generated as the rollersspin, compressing the tubing in the raceway. For a given pump and tubingtype, the flow rate that is generated is proportional to the pump speed (in rev/min). The degree of occlusiveness of the rollers against the tubing is important. Too much compression may promote hemolysis and too littlecompression may reduce the effective forward flow rate. The ideal degree of compression may occur when the rollers are adjusted to be just barely non-occlusive [19]. Other complications that are specific to the use of roller pumpsinclude miscalibration [59] and the potential for fracture of the pump tubing.The roller pump is particularly susceptible to pumping large amounts of air into the arterial line if the venous reservoir is not monitored carefully and empties inadvertently. Spallation, the fragmentation and detachment of tubing particles, may also occur and an arterial line filter will limit subsequentembolization [60–62]. If there is inadvertent obstruction to outflow in the arterial line (e.g. from a clamp), pressure will build up in the arterial line untilthe tubing separates at a connector or the tubing ruptures.
The centrifugal pump has an impeller design and is totally non-occlusive.The resulting flow rate with a centrifugal pump is not only determined by therotational rate of the pump, but is affected by the afterload in both the circuitand the patient. When the pump is not rotating, blood can flow backward (e.g. from the patient) and exsanguination may occur if the arterial line is notclamped [63]. By the same mechanism, it is possible to draw air into the arterialside of the perfusion circuit at the cannulation site. In the event that the arterialline becomes occluded the centrifugal pump, unlike the roller pump, will notgenerate high pressures and it is unlikely that the tubing would rupture. Onepurported benefit of the centrifugal pump over the roller pump is a reducedlikelihood of air embolism. Although it is true that a large amount of air will‘de-prime’ the centrifugal pump (stopping it), smaller amounts of air may easily be pumped into the arterial line.
Heat exchangerOne or more heat exchangers may be placed in the perfusion circuit to warm orcool the patient’s blood. The main heat exchanger is generally placed beforethe oxygenator to prevent any release of microbubbles because of warmingblood that has just been oxygenated. The hot or cold water source may comefrom the hospital’s supply line or be part of a stand-alone unit. Malfunction of the heater-cooler during CPB will result in an inability to control the tem-perature of the patient’s blood properly [64].
Complications of cardiopulmonary bypass and cardioplegia 291
Cardiotomy suctionThe use of cardiotomy suction during cardiac surgical procedures allows foreven large amounts of blood to be evacuated from the operative field duringthe procedure [65]. This blood is typically returned to the perfusion circuit atthe cardiotomy or venous reservoir by way of a defoaming chamber and amicrofilter. These suction lines are typically regulated by a roller pump. Theperfusionist must constantly monitor the speed of the roller pump because if the line or suction tip becomes occluded, high negative pressures may buildup and promote hemolysis.
The use of cardiotomy and vent suction lines may result in hemolysis,gaseous or fat or other particulate microemboli, activation of coagulation andfibrinolysis, cellular aggregation, and platelet dysfunction [66–76]. Room aircan be entrained into these suction lines and contribute to the formation ofgaseous emboli and can produce additional shear stress that is detrimental to the blood elements. The detrimental effect of cardiotomy suction on theplatelets is proportional to the amount of cardiotomy suction and the amountof entrained air [75,76]. Hemolysis is due to negative pressure at the car-diotomy suction tip and the entrainment of air and is minimized if the largestpossible cardiotomy suction tip is used with the minimum necessary suction,and then, only when needed [77,78].
Cell saverThe cell saver can be used in addition, or instead of, cardiotomy suction toscavenge blood from the operative field. With this technique, the scavengedcells are washed with saline and separated from the plasma by centrifugation.The cells can then be returned to the patient either intravenously or into the pump. In contrast to cardiotomy suction, the cell saver can be used, then, to filter out any particulates such as fat, air, and tissue before the blood isreturned to the patient. The relative disadvantage is that there is loss of coagu-lation factors, platelets, and other plasma proteins that are lost during the centrifugation process. From a practical standpoint, the cell saver can be usedinstead of cardiotomy suction in operations in which there is little blood loss tothe operative field (e.g. CABG). For operations in which larger volumes ofbleeding are expected (e.g. redo operations, aortic surgery) and when ventingis required, cell saver suction alone may not be practical. The cell saver can alsobe used at the conclusion of CPB to process any remaining blood in the venousreservoir before returning it to the patient.
Venting of the left heartSuction lines, or ‘vents’, can be used to decompress the left side of the heartduring cardiac surgical procedures [65,79]. Even during cardioplegic arrest,there will be return of bronchial, Thebesian vein, and coronary sinus bloodflow to the right side of the heart that will, unless vented, make its way to theleft side of the heart. In addition, aortic insufficiency may lead to filling of theleft ventricle (through an incompetent aortic valve) during administration of
292 Chapter 16
antegrade cardioplegia. On the basis of experimental as well as clinical studies,venting this blood prevents distension of the ventricle that might increasemyocardial oxygen demand and reduce subendocardial perfusion [80–82]. Inaddition, venting of the left side of the heart may help to prevent unwantedrewarming of the heart during cardioplegic arrest and facilitate the operativeexposure. Nonetheless, there remains considerable variation in clinical prac-tice and debate about the true benefits of routine venting of the left heart[83,84].
Distension of the left side of the heart can be recognized visually, but thepresence of cold saline or slush in the pericardium as well as the posterior loca-tion of the left ventricle may make recognition of left ventricular distensiondifficult. TEE can be used to monitor for distension of the left atrium and vent-ricle. An increase in the left atrial or pulmonary artery pressure (monitored by the pulmonary artery catheter) can also be an indication of left ventriculardistension.
Several methods are available for left heart venting. An antegrade car-dioplegia cannula inserted into the ascending aorta provides an opportunityfor aortic root venting. Venting is not possible during administration of car-dioplegia, however. In addition, if aortic insufficiency is present it may be necessary to administer the antegrade cardioplegia intermittently to preventleft ventricular distension. Complications associated with the use of aortic root venting include potential injury to the aorta at the cannulation site (andeven early or late aortic dissection) and introduction of air into the aorta ifover-zealous suction is applied to the root vent. A second option for left heartventing is direct venting of the left ventricle, with insertion of a vent catheterdirectly through the apex into the left ventricle. This technique is seldom usedtoday because of the risk of bleeding, myocardial injury, and even late pseu-doaneurysm formation. Insertion of vent catheters directly into the left atrium or into the pulmonary artery may have applications [80], but these methodsmay not be completely effective for venting the left ventricle (LV). The mostcommon method for LV venting is indirect, with insertion of a vent catheterthrough a pulmonary vein (usually the right superior) into the left atrium, andthrough the mitral valve into the LV.
Several complications have been associated with left heart venting [85]. Air can be introduced into the left side of the heart, either during insertion or removal of the vent catheter. The likelihood of this complication can bereduced if the heart is allowed to fill, at least partially, during insertion andremoval of the LV vent catheter. It may also be useful to remove the LV ventcatheter while the pericardium is filled with saline (or blood) and the lungs are inflated to prevent aspiration of air into the left atrium. Excessive suctionon the LV vent may cause introduction of air into the left heart around thepurse-string suture or through open coronary arteries during the operativeprocedure [86]. It is important for the perfusionist to be vigilant for entrapmentof the vent catheter tip and to prevent excessive suction. Mishaps with the LV vent line, in which positive pressure was applied to this line, have been
Complications of cardiopulmonary bypass and cardioplegia 293
reported. A 1-way valve in the LV vent line will prevent the introduction of air. Whenever LV venting is used, there should be meticulous efforts for de-airing to avoid subsequent embolization of air that is entrapped in the pulmonary veins, left atrium, or left ventricle. TEE can be used to evaluate the effectiveness of de-airing maneuvers [87]. More recently, many surgeonshave adopted the practice of ‘flooding’ the field with CO2, particularly duringportions of an operation when the left side of the heart is open. When this technique is used, excessive CO2 absorption may lead to hypercarbia andmetabolic acidosis in rare cases [88]. Because it is more soluble, residual CO2 inthe heart is much less likely to cause difficulties with embolization.
Mechanical complications during cardiopulmonary bypassElectrical failureA variety of electrical mishaps may occur during CPB, but these problemsrarely cause significant harm to the patient [89]. A total power failure willaffect the CPB pump as well as its monitors. All perfusion pumps should havea hand crank available so that manual operation of the CPB pump can continuedespite an electrical power failure. Many hospitals in the USA are equippedwith emergency power generators in the event of a power failure, but it maytake several minutes for a back-up generator to come on line. More recently,operating rooms have been equipped with isolated electrical systems with alocal back-up power supply in the event that the main hospital power fails.Newer perfusion machines are often equipped with battery back-up powerunits as a component. With all of these systems and safeguards, however, it isimportant to have regular safety checks and periodic review of emergencyprocedures.
Massive air embolismMassive air embolism is a rare complication, occurring in < 0.2% of cases, butthe impact of this complication can be devastating [89]. Nearly 50% of affectedpatients die or suffer permanent neurological damage [90]. In general, thisterm refers to embolism to the systemic, rather than the pulmonary circulation.Because of the ‘open’ nature of the perfusion circuit, there are many potentialsites for introduction of air, including the operative field, the perfusion circuititself, or introduction of air inadvertently or iatrogenically through intra-venous lines [91].
At the operative field, air can be introduced during the surgical procedure at a variety of stages. Before an aortic cross clamp is applied, small amounts ofair may be introduced inadvertently during aortic cannulation or insertion ofantegrade cardioplegia delivery cannulas. Back-bleeding into the cannulasduring these cannulations may help to prevent the introduction of air. If theleft side of the heart is opened during the procedure, there is an obvious op-portunity for air to be introduced and entrapped. The left atrium, left ventricle,and pulmonary veins are all sites where air can become entrapped. Rigorousde-airing maneuvers at the conclusion of the operative procedure are

294 Chapter 16
warranted and TEE can be used to evaluate the success of these maneuvers.Even when the left side of the heart is not opened (e.g. during CABG opera-tions), air can be drawn in through openings in the coronary arteries if there isexcessive venting at the aortic root or through a superior pulmonary vein.
There are many opportunities for introduction of air in the perfusion circuit[92]. Inadvertent emptying of the venous reservoir and pumping of air into thearterial side of the circuit may be the most common cause of massive airembolism [93,94]. Modern perfusion set-ups typically include monitors andalarms to indicate a low level in the venous reservoir, but attention to thispotential situation on the part of the perfusionist is probably the most import-ant safeguard. When a roller pump is used as the primary pump, fracture of the tubing at the roller head may cause the introduction of air. In addition,any break in the arterial side of the circuit (e.g. fracture, open stopcock) maypredispose to the introduction of air. Another potential source for introductionof air is cavitation that can occur at sites of high-velocity flow throughrestricted diameter tubing (e.g. at kinks, at sites of clamping).
Air embolism can be recognized at several stages during operation. Perhapsthe most common stage where air embolism is suspected is during weaningfrom CPB. Introduction of air antegrade into the coronary arteries can producetemporary myocardial dysfunction that is recognized by regional ECGchanges or regional changes in myocardial function by TEE. Raising the aorticroot pressure, either pharmacologically or by partial manual occlusion of thedistal aorta, may help to force air through the coronary arteries into the venouscirculation. As an alternative, with the cross clamp still applied, a large syringecan be used to inject blood under pressure directly into the aortic root to help pass intracoronary air into the venous circulation [95]. In addition, the administration of retrograde cardioplegia may help to force air from thecoronary arteries into the aortic root, where it can be removed with an aorticroot vent catheter [96]. The patient can be supported by continued CPB andthis problem should resolve in several minutes.
If massive air embolism is recognized during operation, the source of the airmust be determined quickly. CPB should be stopped immediately if the sourceof air is from the arterial side of the perfusion circuit. In this situation, the venous line should be clamped to prevent exsanguination. Air in the arter-ial line should be removed either by aspiration or by filling before CPB is re-initiated. A variety of techniques are available to remove unwanted air fromthe other components of the perfusion circuit, such as the oxygenator, cen-trifugal pump, and arterial filter [89]. Some authorities have recommendedplacing the patient in Trendelenberg position to allow air to flow back into theascending aorta (for possible aspiration), but recent animal experiments havecalled this practice into question [97,98]. If a large volume of air is suspected to have entered the arterial circulation, the use of a period of retrograde cerebral perfusion and profound systemic hypothermia may limit permanentneurological injury [99–103]. Pharmacological therapy may be useful duringan episode of massive air embolism, but there are few clinical data to guide

Complications of cardiopulmonary bypass and cardioplegia 295
the surgeon. Corticosteroids, anticonvulsants, barbiturates, and diuretics maybe used to help limit neurological injury or the symptoms of that injury. Oneuseful algorithm for the postoperative treatment of patients with massive airembolism is presented in Figure 16.2. When the operation is completed andthe patient is sufficiently stable for transfer to a suitable facility, considerationshould be given to additional treatment in a hyperbaric chamber [104–106].
Monitoring for cardiopulmonary bypass and related complications
The level of monitoring for an individual patient undergoing a cardiac surgical procedure will depend not only on the patient’s characteristics (e.g. cardiac function, type of operation, other medical conditions), but also oninstitutional factors (e.g. availability of resources, technical expertise, programobjectives, etc.). Typical monitoring may include arterial catheters, centralvenous catheters, pulmonary artery catheters, and TEE. Each of these monitor-ing techniques carries a small risk of complications.
Arterial cathetersPlacement of an arterial catheter allows for continuous blood pressure mon-itoring and facilitates blood sampling for arterial blood gas determinationsboth during and after CPB. The radial artery is the most common site of cannulation, but the femoral and other arteries may also be used [107].
Before sterile insertion of the radial artery catheter, the overlying skinshould be cleansed thoroughly. Injury to the artery can be avoided by a gentleinsertion technique; the catheter should not be advanced forcefully. Selectionof the contralateral radial artery for cannulation may be preferable to repeatedcannulation attempts at the same site. The use of a topical antibiotic at theinsertion site is controversial, but a sterile dressing should be applied. If a stopcock and extension tubing set are used, care should be taken to ensure thatexcess pressure is not placed on the stopcock against the patient’s arm or handbecause this may cause discomfort and skin necrosis.
Complications of radial artery cannulation may include infection, emboliza-tion, ischemia, and hematoma formation [108–110]. Cellulitis at the site of cannulation may occur in as many as 10% of patients, but documented bac-teremia is rare [111]. Ischemic complications are also uncommon. The Allen’stest is often used to evaluate the integrity of the ulnar artery and palmar archbefore radial artery cannulation, but this test is not completely reliable for pre-dicting ischemic complications. Distal embolization may produce evidence of ischemia at the fingertips and thrombosis of the radial artery may occur in1–2% of patients. Serious sequelae are uncommon because of collateral bloodsupply [111,112]. Patients with poor peripheral blood flow, particularly in thesetting of high-dose vasopressor therapy, are more prone to this complication.Removing the catheter is the treatment and the catheter should be removed assoon as an ischemic complication is suspected. Hematoma formation usually
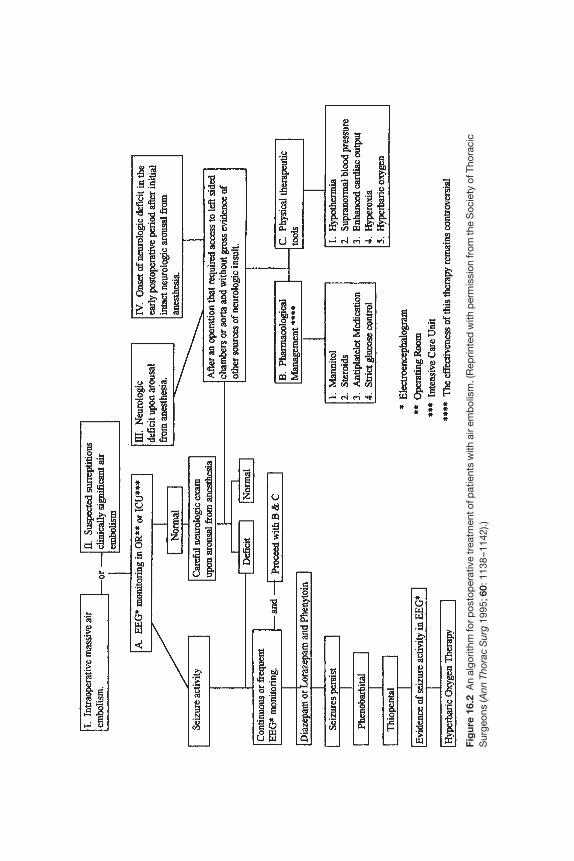
Fig
ure
16.2
An
algo
rithm
for p
osto
per
ativ
e tr
eatm
ent o
f pat
ient
s w
ith a
ir em
bol
ism
. (R
eprin
ted
with
per
mis
sion
from
the
Soc
iety
of T
hora
cic
Sur
geon
s (A
nn T
hora
c S
urg
1995
;60:
1138
–114
2).)

Complications of cardiopulmonary bypass and cardioplegia 297
occurs with inadequate compression after a failed cannulation attempt orremoval of a radial artery catheter, particularly in the setting of systemic anticoagulation. Other uncommon complications include necrosis of the skinoverlying the insertion site, formation of an arteriovenous fistula or pseudoa-neurysm, and median nerve neuropathy.
Femoral arterial cannulation is often used when the radial arteries are notavailable (e.g. used for bypass conduits) [113]. Sterile technique should beused and a longer catheter may help to prevent inadvertent dislodgement. Thefemoral arterial catheter should be sutured to the skin and a sterile dressingshould be applied. Potential complications include infection at the cannulationsite, bacteremia, distal embolization, pseudoaneurysm, the formation of an arteriovenous fistula, and injury to the femoral nerve. Femoral arterialcatheters or introducer sheaths (often placed at the time of cardiac catheter-ization) should be removed as early as possible to prevent complications andpromote early mobilization of the patient [114,115].
Central venous cathetersCentral venous catheterization can be used for: (i) intravenous access for theadministration of medications, fluids, or blood products, (ii) monitoring thecentral venous pressure, and (iii) subsequent cannulation of the pulmonaryartery with a Swan–Ganz catheter. The internal (or external jugular) and sub-clavian veins are used most commonly, but the femoral vein may also be used.The most common immediate complications of central venous catheterizationinclude: (i) inadvertent injury to the nearby artery, (ii) misplacement of thecatheter, and (iii) pneumothorax [116–122].
Arterial puncture can often be recognized by the return of pulsatile bloodwhen the syringe is removed from the large-bore introducer needle. If thisoccurs, the needle should be removed immediately. In the case of jugularinsertion, the frequency of carotid arterial puncture is approximately 4%. If thejugular or femoral route is being used, pressure should be held at the cannula-tion site to help prevent hematoma formation. The usefulness of manual pres-sure to the subclavian artery and vein is controversial. Occasionally, arterialcannulation will not be recognized until after the catheter has been inserted.Arterial catheterization may be indicated by i.v. fluids that do not flow freelyinto the catheter, an arterial pressure tracing, or an ‘arterial’ course of thecatheter on a subsequent chest radiograph (CXR). Once arterial catheterizationhas been discovered, the catheter should be removed and pressure should be held over the cannulation site. Unexplained blood loss or hemodynamicinstability during a cardiac operation should prompt consideration of vascularinjury from central venous catheterization and the ipsilateral pleural spaceshould be inspected.
For catheters placed by the jugular or subclavian routes, the catheter tipshould lie at the junction between the superior vena cava and the right atrium.A CXR immediately after operation should be used to document the correctposition of the catheter tip and to evaluate for any unexpected hematoma or

298 Chapter 16
pleural effusion [123]. A variety of incorrect positions are possible: ‘doubledback’ into the contralateral neck, distally in the subclavian vein, in the internalmammary vein, looped or coiled in the right atrium, in the IVC, across thechest into the contralateral subclavian vein, or abutting the SVC wall [124]. A mispositioned catheter may not necessarily be harmful to the patient, but we recommend removal and replacement of all mispositioned catheters. If theguide-wire is inadvertently ‘lost’ into the central circulation, urgent retrieval isindicated. In many cases, these guide-wires can be retrieved by an interven-tional radiologist using an intravascular snare.
Depending on the route of central venous catheterization, pneumothoraxoccurs in approximately 1–4% of cases [116–118,125]. Tension pneumothoraxmay be manifested by cardiopulmonary compromise or increasing airwaypressures and can be treated by introduction of a large-bore needle or catheterthrough the 2nd intercostal space, anteriorly. Pneumothorax is occasionallyrecognized after opening the chest and visualizing the air in the pleural space;an opening in the pleura serves to decompress the pneumothorax.
Late complications of central venous catheterization may not manifest untilafter the operation and, sometimes, not for hours to days. Venous thrombosismay occur, particularly in patients with large-bore, multilumen catheters thatare left in place for long periods of time. This condition may manifest with uni-lateral upper extremity or neck swelling and discomfort. The diagnosis can beconfirmed by ultrasound or venography. The catheter should be removed andconsideration should be given to systemic anticoagulation. Catheter-relatedinfection may be suggested by erythema or drainage at the insertion site, fever, leukocytosis, and documented bacteremia. When infection is suggested, the catheter should be removed and replaced at another site, if needed. Some authorities have recommended routine replacement of central venouscatheters after several days to help prevent catheter-related infection, but thereis no consensus [116,126]. Air embolism may occur if a port or stopcock is left open or if a catheter is removed with the patient in the upright position[127]. As little as 5–10 cm3 of air may cause cardiac arrest. If air embolismoccurs, the patient should be placed on the left side and the catheter should be aspirated to remove any air. Thoracotomy is occasionally indicated forremoval of air directly from the pulmonary artery.
In some centres, multiple central venous catheters are used for monitoringin patients undergoing cardiac surgical procedures. By report, this practice isassociated with little additional risk of complication compared with singlevenous catheterization [128].
Pulmonary artery cathetersA pulmonary artery (e.g. Swan–Ganz) catheter is used to provide informationabout the central venous, pulmonary artery, and pulmonary artery wedgepressures and to allow continuous or ‘on-demand’ measurement of the cardiacoutput and mixed venous oxygen saturation. Postoperatively, the pulmonaryartery catheter can be used to provide information about the patient’s intra-vascular volume status, aid in the treatment of heart failure, and facilitate

Complications of cardiopulmonary bypass and cardioplegia 299
temporary pacemaking (through a pacing port). Because the pulmonary arterycatheter is typically placed through an introducer sheath in a central vein, pulmonary artery catheterization is associated with many of the same com-plications as central venous catheterization (see above).
Serious complications related to the use of a pulmonary artery catheter for cardiac surgery are uncommon [129]. During insertion of the pulmonaryartery catheter, transient or sustained arrhythmias may occur and should betreated by prompt advancement or withdrawal of the catheter. During anywithdrawal of the catheter, the balloon should be deflated to prevent injury to the pulmonary or tricuspid valves. Persistent arrhythmias should promptconsideration of the administration of an antiarrhythmic medication such aslidocaine, but arrhythmias due to mechanical irritation of the catheter may beresistant to these medications [130]. Heart block may develop or may worsen,especially for patients with pre-existing fascicular block. Perforation or injuryto the tricuspid valve [131], pulmonary valve [132], or ventricle during inser-tion is rare. A pulmonary artery catheter that becomes knotted can usually beremoved non-surgically, often by the interventional radiologist [133].
Rupture of the pulmonary artery is the most serious complication of pulmonary artery catheterization and carries a substantial mortality rate[129,134–142]. Proper care of the pulmonary catheter aimed at preventing thiscomplication requires frequent checking to make certain that the catheter tip does not remain in the ‘wedged’ position. Movement during the cardiacsurgical procedure is common and the anesthesiologist should be vigilant for this possibility. Pulmonary artery rupture is a potentially life-threateningcomplication that may produce localized or uncontrolled hemorrhage andquick deterioration of the hemodynamic and respiratory status. If hemoptysissuggests pulmonary artery rupture before the cardiac surgical procedure hasbegun, several measures may help temporize the situation. First, medicationsthat affect clotting (e.g. heparin, Coumadin, aspirin) should be stopped, if pos-sible, and alterations in the patient’s clotting profile should be corrected withadministration of vitamin K or fresh frozen plasma. Intubation and mechanicalventilation may be required. A thoracostomy tube should be inserted to drainany blood from the affected pleural space. Bronchoscopy may be helpful to determine an exact site of bleeding and can be used to insert a balloon-tipped catheter to isolate the affected pulmonary segment. Persistent bleed-ing should prompt exploration, either through a thoracotomy or median sternotomy approach. A segmentectomy or lobectomy is used to control thebleeding. In this circumstance, cardiac operation is deferred, if possible.
Pulmonary rupture may manifest during the cardiac operation, usually atthe conclusion of CPB, or later in the ICU. The principles of treatment outlinedabove apply in these situations as well.
Transesophageal echocardiography (TEE)Transesophageal echocardiography is a common diagnostic procedure out-side of the operating room and is thought to carry little risk to the patient. In large series of TEE in the general cardiology population, the frequency of
300 Chapter 16
serious complications is < 0.2% [143,144]. The ultrasound probe and unitshould be well maintained to prevent thermal or electrical injury to the patientand the probe should be cleaned properly to prevent disease transmissionbetween patients.
Intraoperative TEE is used commonly today as a monitoring tool in cardiacsurgery, particularly in those patients undergoing valve procedures, aorticprocedures, and correction of congenital defects. Intraoperative TEE pro-vides information about the cardiac anatomy and function that can help to determine the most appropriate surgical procedure (e.g. valve repair vs.replacement), facilitate weaning from CPB, and assess the immediate results of operation. In a large series of intraoperative TEE, the morbidity rate was0.2% and the reported mortality rate attributable to TEE was 0% [145].
The most frequent complication of intraoperative TEE is transientodynophagia [145]. Swallowing dysfunction has been reported in up to 4% ofpatients after operations in which intraoperative TEE was used [146]. Propercare should be exercised during insertion of the TEE probe to prevent dentalinjury or dislodgement of the endotracheal tube [145]. Upper gastrointestinalbleeding may occur after intraoperative TEE, but this may be due not only tomechanical irritation by the TEE probe but also to pre-existing conditions ofthe esophagus or stomach [145]. The most serious complication associatedwith intraoperative TEE is gastrointestinal perforation. This may occur in theoropharynx [147], hypopharynx [148], esophagus [145,149,150], or stomach.Some authorities have suggested that a preoperative history of dysphagia is arisk factor for perforation [148]. The treatment of patients with gastrointestinalperforation should focus on localization of the site of perforation, administra-tion of antibiotics, and, in many cases, operative repair. This complication is associated with substantial morbidity and mortality risk for the patient[145,149,150].
Anticoagulation for cardiopulmonary bypass and related complications
Anticoagulation for cardiopulmonary bypassSome degree of anticoagulation is required during CPB to prevent coagulationwithin the pump circuit and its components. Although heparin is the mostcommon agent used for anticoagulation in conjunction with CPB, other anti-coagulants may be useful in special circumstances. The surgeon, perfusionist,and anesthesiologist should be aware of the potentially adverse effects that areassociated with each of these anticoagulants.
Heparin is the most common anticoagulant used for CPB because this agentis effective, reversible, well tolerated, and inexpensive [151]. Unfractionatedheparin is a mixture of mast cell polysaccharides (1000–50 000 d) that producesits anticoagulant effect by potentiating the activity of antithrombin III (ATIII)and inhibiting thrombin directly by binding to cofactor II. There is substantialinterpatient variability in the clinical effects of a fixed dose of heparin, how-
Complications of cardiopulmonary bypass and cardioplegia 301
ever. In addition, acute reactions such as anaphylaxis, pulmonary edema, and disseminated intravascular coagulation (DIC) may occur rarely afteradministration of heparin.
For clinical applications other than anticoagulation for CPB, the most common complication following heparin administration is bleeding. In thesetting of CPB, however, anticoagulation is essential regardless of the risk of any potential excess bleeding. During cardiac surgery, bleeding into theoperative field does not usually pose a problem because of the availability ofcell saver or cardiotomy suction. Excess administration of heparin, however,may produce fibrinolysis and unwanted platelet activation. Insufficient anti-coagulation during CPB may result in consumption of coagulation factors.
Historically, heparin administration in preparation for CPB was guidedempirically. Today, the appropriate dose of heparin can be monitored beforeand during CPB. The initial dosage is usually 200–400 U/kg, with main-tenance doses (administered intermittently during CPB) of 50–100 U/kg. Inaddition, 10 000–20 000 U are typically placed in the bypass pump before theinstitution of CPB.
Heparin resistanceHeparin resistance refers to the circumstance in which a patient receives thestandard dose of heparin before CPB but does not become fully anticoagu-lated. Several etiologies are possible, including: congenital ATIII deficiency,acquired ATIII deficiency, thrombocytosis, pregnancy, sepsis, hypercoagu-lable states, and coagulopathic processes [152–156]. A deficiency of ATIII is themost common cause and can be treated with administration of fresh frozenplasma or recombinant ATIII [155].
Heparin-induced thrombocytopeniaHeparin-induced thrombocytopenia (HIT) occurs in up to 10% of patientstreated with heparin [157–161] and has been documented in 1–5% of surgicalpatients [157]. This condition may manifest after exposure to either unfrac-tionated or low-molecular-weight heparin preparations. The relatively highincidence of HIT in surgical patients has been attributed, in part, to thewidespread use of heparin for a variety of indications and a high prevalence ofheparin-associated antibodies in patients who are referred for cardiac surgery[157].
Two forms of HIT have been described [158]. Type I HIT is due to plateletaggregation and is associated with mild thrombocytopenia (never less than100 × 109/l) [158]. For patients with type I HIT, the thrombocytopenia devel-ops within a few days of heparin exposure but resolves without specific treatment. Patients are often asymptomatic and the risk of serious associatedmorbidity is low. Type II HIT is immunologically mediated, with develop-ment of heparin-associated antiplatelet antibodies that promote platelet activation [158,159]. The IgG, IgA, or IgM antibodies are directed against thecomplex of heparin and platelet factor 4 (H–PF4) [159]. For patients with type

302 Chapter 16
II HIT, the thrombocytopenia often develops 5–14 days after heparin exposureand the platelet count is often well below 100 × 109/l [158].
The more serious condition of heparin-induced thrombocytopenia andthrombosis (HITT) occurs in a subset of patients with HIT, and in 10% of theseindividuals there is significant end-organ injury due to thrombosis [157]. Avariety of vascular complications may occur, including cerebral infarction,mesenteric infarction, myocardial infarction, bypass graft occlusion, and limbischemia. Amputation may be needed in as many as 25% of patients withaffected limbs. The mortality rate approaches 30% [157].
There should be a high index of suspicion for the diagnoses of HIT andHITT. The diagnosis of HIT is suggested by a fall in the platelet count of > 50%or an absolute platelet count < 100 × 109/l [157]. When this diagnosis is suspected, heparin should be withheld in all of its forms, the platelet countshould be measured daily, and the patient should be monitored closely for thedevelopment of thrombotic complications. A variety of laboratory tests areavailable to establish the diagnosis of HIT, including platelet aggregometry,the serotonin release assay (SRA), flow cytometric assays, and enzyme-linkedimmunosorbent assay (ELISA) to measure anti-H–PF4 antibody titres [159].Each of these tests has relative advantages and disadvantages and may not beavailable in all institutions. Because of slow turnaround time for these tests,treatment should be instituted promptly while awaiting the results of the laboratory test(s).
The primary treatment for patients with HIT is withdrawal of heparin andanticoagulation with another agent that reduces thrombin generation [160].Agents that may be useful in this situation include danaparoid, ancrod, recom-binant hirudin, and argatroban. Arterial thrombotic complications should betreated expeditiously.
Alternatives to heparinAlternatives to heparin for anticoagulation may be useful for patients with aknown heparin allergy, protamine allergy, or history of HIT [161]. For patientswith a history of HIT, a delay in surgery may allow time for antiplatelet antibodies to fall to an unmeasurable level. Unfortunately, this does not neces-sarily preclude the development of recurrent HIT [161]. Another useful strat-egy may be preoperative plasmapheresis to remove circulating antiplatelet antibodies [162]. A variety of anticoagulants may be useful alternatives to heparin in certain circumstances: warfarin, low-molecular-weight dextran,low-molecular-weight heparin, heparanoids (e.g. orgaran), ancrod, antithrom-bin agents (e.g. hirudin, argatroban), and prostacyclins [161,163–165].
Monitoring of anticoagulation for cardiopulmonary bypassHistorically, heparin dosing was accomplished empirically, with a fixeddosage based on the patient’s weight. In most centers today, however, an initial dose of heparin is administered and then the activated clotting time(ACT) or heparin levels are monitored periodically to: (i) ensure adequate

Complications of cardiopulmonary bypass and cardioplegia 303
anticoagulation before the institution of CPB, (ii) assess for the need for addi-tional doses of heparin during CPB, and (iii) assess the effectiveness of reversalof heparinization after CPB.
Reversal of anticoagulationAt the conclusion of CPB, the effects of heparin are typically reversed withadministration of protamine. Calculation of an appropriate dose of protamineis important because incomplete reversal of the heparin results from too little protamine and excessive protamine administration may lead to increasedplatelet dysfunction, increased postoperative bleeding, and increased trans-fusion requirements [151]. Individual patient factors (e.g. sensitivity to pro-tamine, metabolism of heparin) as well as operation-related factors (e.g.degree and duration of hypothermia) will influence the appropriate dose of protamine for a given patient [166].
Several techniques are available to calculate the appropriate dose of pro-tamine. In the simplest technique, a fixed dose of protamine can be admin-istered per amount of heparin that is administered. This calculation can bebased either on the initial heparin dose or on the total amount of heparinadministered during the operation [167]. A variety of approaches have beendescribed, with administration of as little as 1 mg to as much as 5 mg of pro-tamine for every 1 mg of heparin administered. A second method of calculat-ing the appropriate protamine dose is by use of heparin dose–response curvesthat are based on the ACT before and during CPB [168]. This curve can be used at the conclusion of CPB to estimate an appropriate dose of protamine.This approach has been reported to reduce the amount of protamine usedcompared with the fixed-dose approach [167,169]. There are potential dis-advantages to the heparin dose–response method, however. In particular, the heparin dose–response curve is actually non-linear and this results in inac-curacies at either very low or very high levels of anticoagulation [167,170–172].The last method for calculation of the appropriate protamine dose is based onmeasurement of heparin concentrations directly [166,173–175]. Protaminetitration using measured heparin concentrations may reduce the amount ofprotamine used by as much as 30–40% compared with the heparin dose–response curve method [151,170].
Serious adverse reactions may occur with protamine administration[176,177]. Risk factors include pulmonary hypertension, previous exposure toprotamine or protamine-containing insulin preparations, previous vasectomy,and fish allergies [178]. Some authorities have advocated administration ofprotamine on the left side of the circulation (e.g. into the aorta) to prevent pul-monary exposure to heparin–protamine complexes and to reduce the chanceof pulmonary histamine release, but the results from clinical studies have beenconflicting [179,180].
Protamine reactions are usually described in three categories: type I, withtransient hypotension; type II, with anaphylaxis; and type III, with pulmonaryvasoconstriction [181,182]. The type I protamine reaction is mediated by
304 Chapter 16
release of histamine from mast cells and basophils. This effect is more pro-nounced with rapid injection, so it is recommended that protamine be admin-istered over 5–10 min, or longer [178,183,184]. Pretreatment with histaminereceptor antagonists may reduce the effect but not eliminate the possibility of atype I reaction [185]. Histamine release produces reductions in the systemicarterial pressure and the central venous pressures. There will often be a reduc-tion in the cardiac output, but this may be due simply to decreased preload[186,187]. Animal studies have suggested a direct negative effect of protamineon myocardial contractility, but the evidence is not convincing in humans[187–189].
The classic type II protamine reaction is mediated by IgE on the surface of mast cells which interacts with protamine and causes degranulation. Thesymptoms may include rash, bronchospasm, edema, stridor, hypotension, and cardiovascular collapse. Patients at increased risk of this type of reactioninclude those with previous exposure to protamine or protamine-containinginsulin preparations (e.g. NPH or protamine-zinc insulin), previous vasec-tomy, or fish allergies. Several tests are available to evaluate the patient forpotential protamine allergy, including: intradermal skin testing [178,190]; in vitro whole blood leukocyte histamine release [180,191]; and radioaller-gosorbent testing for serum antiprotamine IgE [178,191,192]. For most patientsundergoing cardiac surgical procedures, however, these tests are not prac-tical. Less commonly, type II anaphylactoid reactions are mediated by the classic complement pathway, in which protamine–heparin complexes causerelease of C3a, C5a, and other vasoactive mediators, producing anaphylaxis[193,194].
In the type III protamine reaction, patients develop acute pulmonary hyper-tension, decreased left atrial pressure, right ventricular failure, and systemichypotension [177,178]. It is not clear whether the rate of protamine admin-istration affects the likelihood of a type III reaction [181,195]. The reaction may be transient or prolonged and may necessitate re-institution of CPB. Re-administration of protamine in a given patient may or may not result in the same reaction again. Although the mechanism of the type III reaction is not completely understood, it is probably mediated by complement when protamine–heparin complexes result in release of vasoactive substances (e.g. oxygen free radicals, thromboxane A2) [196–200].
There are several alternatives to protamine for the reversal of the effects of heparin, but none enjoys much clinical use. Hexadimethrine neutralizesheparin with the same mechanism as protamine and with less effect on the sys-temic hemodynamics [201,202]. Unfortunately, this agent also produces directlung injury and can cause a clinical syndrome of non-cardiogenic pulmonaryedema [203]. Moreover, this agent may produce platelet aggregation and renalfailure [204,205]. Because of these side-effects, this agent is not currently clinic-ally available. A second alternative is the use of a cellulose filter that containsimmobilized protamine [206–208]. This filter can be placed in the arterial linejust before the termination of CPB. Several passes of blood through the circuit
Complications of cardiopulmonary bypass and cardioplegia 305
may be needed for effective neutralization of heparin, however, and this mayresult in fibrin-clot deposition at the filter. A third alternative to protamine is heparinase [209,210]. In animal studies, a heparinase-bonded filter has been shown to neutralize heparin effectively with two to three passes of theblood through the filter. A fourth alternative to protamine is platelet factor 4, aprotein released from platelets with a highly specific heparin-neutralizingproperty [211–215]. In animal models, platelet factor 4 has been shown to neut-ralize heparin effectively, with no effect on the platelet count, leukocyte count,or complement levels.
Residual circulating heparin may be present even after protamine adminis-tration if an insufficient amount of protamine is used or if there is subsequentrelease of heparin from heparin–protamine complexes, heparin-binding pro-teins, or from other sites [151]. The term ‘heparin rebound’ is used to describethe situation in which there is recurrent heparin activity after complete neut-ralization of heparin. Persistent circulating heparin, regardless of the cause,may lead to an increase in bleeding after CPB [151].
CPB and bleedingCardiac surgical patients are particularly susceptible to postoperative medi-astinal bleeding. The incidence of severe bleeding after CPB depends on thedefinition, but as many as 5–7% of patients may experience bleeding of > 2 lduring the first 24 h after operation [216]. In recently reported large series of adult cardiac surgery patients, as many as 3–5% of patients require re-exploration of the chest because of excessive postoperative bleeding [217,218].The need for re-exploration of the chest after a cardiac surgical procedure isassociated with substantial morbidity and mortality [219]. In one large series,re-exploration was associated with a twofold increase in operative mortality aswell as a significantly increased incidence of renal failure, adult respiratorydistress syndrome (ARDS), prolonged mechanical ventilation, sepsis, andatrial arrhythmias [217]. In addition, the transfusion of blood products becauseof excessive bleeding is associated with a variety of potentially adverse events,including blood-borne disease transmission (e.g. hepatitis, HIV), increasedincidence of wound infection, and transfusion reactions [219].
Aprotinin and AmicarFibrinolysis ordinarily prevents or limits propagation of intravascular throm-bosis. Although the mechanism is not entirely clear, there is typically increasedfibrinolytic activity during cardiac surgery [220]. Three antifibrinolytic agentsare currently available to help limit fibrinolytic activity during CPB and to help reduce postoperative bleeding: tranexamic acid, epsilon-aminocaproicacid (EACA, Amicar), and aprotinin (Trasylol) [221]. Of these agents, epsilon-aminocaproic acid and aprotinin have both been shown to reduceantifibrinolytic activity during CPB and to reduce postoperative bleeding and transfusion requirements, particularly among patients undergoing ‘redo’operations [220].
306 Chapter 16
A variety of complications have been described in association withantifibrinolytic therapy, particularly with the administration of aprotinin. In particular, there were early concerns that antifibrinolytic therapy mightincrease the possibility of a thrombotic complication. Although the data havebeen conflicting, the majority of reports have not found an increase in periop-erative myocardial infarction or early bypass graft occlusion [220]. Manyauthorities have suggested that intraoperative thrombosis associated withaprotinin may be due to inadequate anticoagulation and have suggested aminimum (celite) ACT of 750 s [220]. Another potential complication is thedevelopment of renal failure after aprotinin therapy, particularly when used in conjunction with hypothermic circulatory arrest [222]. Prospective trialshave failed to demonstrate an association between aprotinin therapy and postoperative renal insufficiency, however, [223]. Lastly, the overall incidenceof anaphylactoid reaction to aprotinin is reported by the manufacturer to beapproximately 0.5%, but this risk may increase to as much as 6–9% followingre-exposure [220,224].
Blood conservation techniquesAlthough blood product transfusion is generally safe, transfusion can be asso-ciated with viral or bacterial transmission [225] (Table 16.1), isoimmunization,potentially increased incidence of postoperative wound infection [226–228],and increased cost. Because of these potential risks as well as a limited supplyof banked blood products, there is considerable impetus to avoid transfusionwhenever possible, and today transfusion can be avoided in many cardiacsurgery patients. A variety of techniques that can be applied before, during,and after operation can be used to help avoid blood product transfusion inpatients undergoing cardiac surgery procedures (Table 16.2).
Preoperative techniquesAlthough the technique may be available to only a minority of cardiac surgerypatients, autologous red blood cell predonation can be used to limit the need for allogeneic transfusion during and after operations of many types[229–231]. Factors that may limit the use of this technique in cardiac surgerypatients include: (i) insufficient lead time, (ii) preoperative anaemia, and (iii)cardiac instability. In addition, autologous predonation is more expensivethan allogeneic transfusion [232]. When 2 U of red blood cells are harvestedover a 2–3-week period, the preoperative hemoglobin typically falls byapproximately 2 g/dl. Even for patients who are anticipating cardiac surgery,however, this practice is generally safe and well tolerated [233,234]. Erythro-poietin has been shown to be useful, alone or in combination with iron, toimprove the hematocrit in anaemic patients before cardiac surgery and mayimprove the yield of autologous predonation in some patients [235–237].
Intraoperative techniquesA variety of intraoperative techniques are available to help reduce the need for
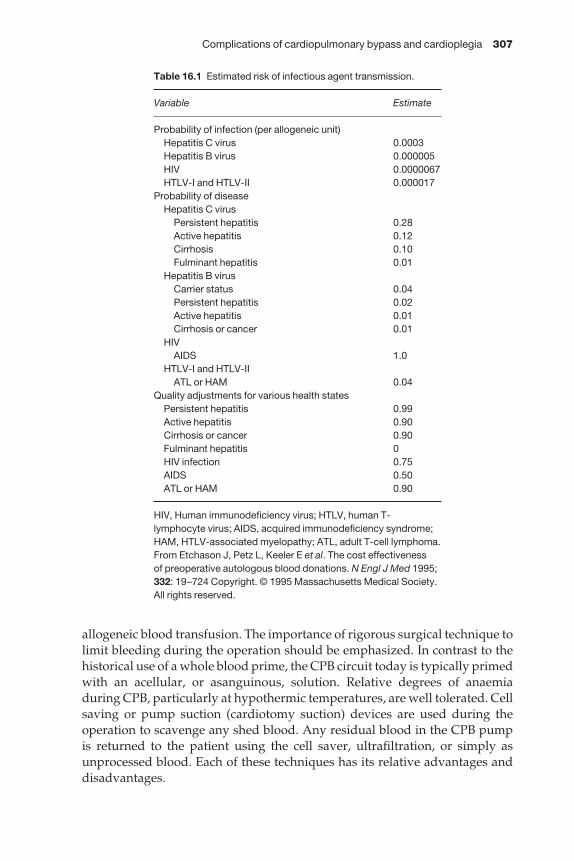
Complications of cardiopulmonary bypass and cardioplegia 307
allogeneic blood transfusion. The importance of rigorous surgical technique tolimit bleeding during the operation should be emphasized. In contrast to thehistorical use of a whole blood prime, the CPB circuit today is typically primedwith an acellular, or asanguinous, solution. Relative degrees of anaemia during CPB, particularly at hypothermic temperatures, are well tolerated. Cellsaving or pump suction (cardiotomy suction) devices are used during theoperation to scavenge any shed blood. Any residual blood in the CPB pump is returned to the patient using the cell saver, ultrafiltration, or simply asunprocessed blood. Each of these techniques has its relative advantages anddisadvantages.
Table 16.1 Estimated risk of infectious agent transmission.
Variable Estimate
Probability of infection (per allogeneic unit)Hepatitis C virus 0.0003Hepatitis B virus 0.000005HIV 0.0000067HTLV-I and HTLV-II 0.000017
Probability of diseaseHepatitis C virus
Persistent hepatitis 0.28Active hepatitis 0.12Cirrhosis 0.10Fulminant hepatitis 0.01
Hepatitis B virusCarrier status 0.04Persistent hepatitis 0.02Active hepatitis 0.01Cirrhosis or cancer 0.01
HIVAIDS 1.0
HTLV-I and HTLV-IIATL or HAM 0.04
Quality adjustments for various health statesPersistent hepatitis 0.99Active hepatitis 0.90Cirrhosis or cancer 0.90Fulminant hepatitis 0HIV infection 0.75AIDS 0.50ATL or HAM 0.90
HIV, Human immunodeficiency virus; HTLV, human T-lymphocyte virus; AIDS, acquired immunodeficiency syndrome;HAM, HTLV-associated myelopathy; ATL, adult T-cell lymphoma.From Etchason J, Petz L, Keeler E et al. The cost effectiveness of preoperative autologous blood donations. N Engl J Med 1995;332: 19–724 Copyright. © 1995 Massachusetts Medical Society. All rights reserved.

308 Chapter 16
Preoperative harvesting of platelet-rich plasma (PRP) can be used to limitthe exposure of platelets to CPB and is usually performed in the operatingroom before the initiation of CPB. Whole blood is collected, spun in a cen-trifuge to separate the PRP from the cells, and the blood is re-administered to the patient. This process is repeated until a sufficient volume of PRP hasbeen obtained. Using this technique, approximately 9–30% of the circulatingplatelets can be harvested and stored safely for 2–3 h. The inability to harvestan adequate volume of platelets may currently limit the utility of this technique,but improvements in equipment and techniques may increase the yield of theharvest. Studies of intraoperative transfusion of PRP to reduce the need forpostoperative allogeneic transfusion have produced mixed results [238–241].
Acute normovolemic hemodilution refers to the withdrawal of whole bloodfrom the patient and replacement with crystalloid or colloid, usually before the initiation of CPB. Like harvesting of PRP, this technique protects blood elements from the deleterious effects of CPB. The withdrawal of blood can beaccomplished either through a central venous catheter before heparinization(using citrate storage bags) or through the venous line of the CPB pump afterheparinization. The volume of blood that can be withdrawn safely depends on the patient’s body size and preoperative hemoglobin level, but in a typicalpatient approximately 1000 ml of blood can be withdrawn. This techniqueappears to be safe and well tolerated in many patients and its efficacy in terms of reduction in allogeneic transfusion has been documented in several
Table 16.2 Techniques for reducing blood product transfusion in cardiac surgery patients.
PreoperativeAutologous predonation of whole blood, red blood cells, FFP, platelets, erythropoietin
IntraoperativeInstitutional program of guidelines for blood product transfusionRigorous surgical techniquePre-CPB isovolemic hemodilutionPre-CPB pheresis of platelets and FFPPheresis of FFP and plateletsNon-sanguinous primeWhole blood collection at CPB onsetRetransfusion of pump bloodCell saver or ultrafiltration of pump bloodDrug therapy
Antifibrinolytic agentsDDAVP
PostoperativeInstitutional program of guidelines for allogeneic blood product administration.Shed mediastinal blood transfusion
CPB, cardiopulmonary bypass; FFP, fresh frozen plasma.From Brody SC, Morse DS. Coagulation, transfusion, and cardiac surgery. In: Spiess BD, CountisRB, Gould SA, eds. Perioperative Transfusion Medicine. Baltimore: Lippincott Williams & Wilkins,1998; 443, with permission.
Complications of cardiopulmonary bypass and cardioplegia 309
studies [242,243]. Proponents point to a higher platelet count after CPB as themechanism for reduced bleeding and transfusion requirement [244,245].
Postoperative techniquesInstitutional guidelines or ‘triggers’ for blood product transfusion may limitunnecessary transfusion postoperatively. As an example, a ‘trigger’ pointhematocrit of 24% in the early postoperative period might prompt automatictransfusion of 2 U of red blood cells. This practice carries the advantage that transfusion happens automatically at predetermined ‘trigger’ points.Unfortunately, though, automatic transfusion may not always be indicated foran individual patient.
Autotransfusion of shed mediastinal blood in the early postoperative periodhas been advocated as another technique to reduce the need for postoperativetransfusion. Most [246–248] but not all studies [249–251] have shown this tech-nique to be effective, but despite years of clinical use there is still controversyregarding the safety of this technique. Potential complications with autotrans-fusion of shed mediastinal blood include altered coagulation [252], systemicfibrinolysis [253], and bacterial contamination [254].
Pathophysiological consequences of cardiopulmonary bypass
The use of CPB produces pathophysiological effects in nearly all of the body’sorgan systems. Although these effects might not be considered complicationsin the classic sense, they are a necessary byproduct of CPB and lead to much ofthe morbidity associated with its use. A complete discussion of these patho-physiological effects is beyond the scope of this chapter; the reader is referredto other sources for additional information [255,256]. For the purpose of thischapter, we confine our discussion to: the effects of CPB generated at theblood–surface interface; the consequences of hypothermia, which is often usedin conjunction with CPB; the metabolic consequences of CPB; the effects ofCPB on the lungs; the effects of CPB on the kidneys; and the neurologicaleffects of CPB.
Consequences of the blood–surface interfaceOrdinarily, the blood and plasma come into contact only with endothelial linedvessels. During cardiac surgical procedures with the use of CPB, however, theblood and plasma are exposed to a variety of foreign surfaces, including notonly the components of the perfusion circuit but also the exposed tissues in theopen surgical wound. As a result of this contact at the blood–surface interface,a host of specific reactions are initiated that result in a systemic response toCPB [257].
Almost immediately after contact with a non-endothelial surface, plasmaproteins are adsorbed onto that surface, producing a monolayer of many different proteins [258,259]. Fibrinogen is among the most important of theplasma proteins that is adsorbed [260,261]. The type and relative mix of pro-teins will be determined by the particular non-endothelial surface involved.
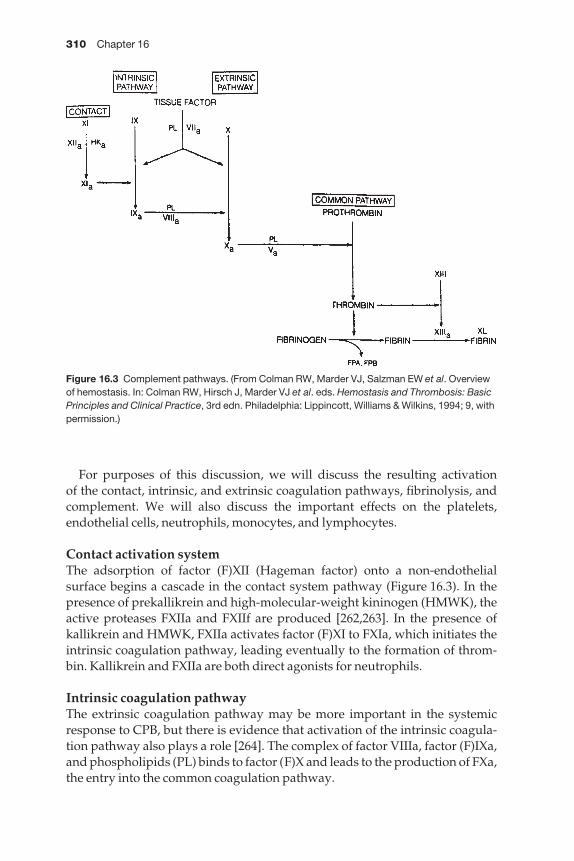
310 Chapter 16
For purposes of this discussion, we will discuss the resulting activation of the contact, intrinsic, and extrinsic coagulation pathways, fibrinolysis, andcomplement. We will also discuss the important effects on the platelets,endothelial cells, neutrophils, monocytes, and lymphocytes.
Contact activation systemThe adsorption of factor (F)XII (Hageman factor) onto a non-endothelial surface begins a cascade in the contact system pathway (Figure 16.3). In thepresence of prekallikrein and high-molecular-weight kininogen (HMWK), theactive proteases FXIIa and FXIIf are produced [262,263]. In the presence ofkallikrein and HMWK, FXIIa activates factor (F)XI to FXIa, which initiates theintrinsic coagulation pathway, leading eventually to the formation of throm-bin. Kallikrein and FXIIa are both direct agonists for neutrophils.
Intrinsic coagulation pathwayThe extrinsic coagulation pathway may be more important in the systemicresponse to CPB, but there is evidence that activation of the intrinsic coagula-tion pathway also plays a role [264]. The complex of factor VIIIa, factor (F)IXa,and phospholipids (PL) binds to factor (F)X and leads to the production of FXa,the entry into the common coagulation pathway.
Figure 16.3 Complement pathways. (From Colman RW, Marder VJ, Salzman EW et al. Overviewof hemostasis. In: Colman RW, Hirsch J, Marder VJ et al. eds. Hemostasis and Thrombosis: BasicPrinciples and Clinical Practice, 3rd edn. Philadelphia: Lippincott, Williams & Wilkins, 1994; 9, withpermission.)
Complications of cardiopulmonary bypass and cardioplegia 311
Extrinsic coagulation pathwayUnder ordinary circumstances, tissue factor is a membrane-bound protein thatis not exposed to the blood. Activated monocytes and endothelial cells alsoexpress tissue factor [265,266]. During CPB, tissue factor acts with activatedfactor VIIa and phospholipid (PL) to promote activation of both FIX to FIXaand FX to FXa, the entry into the common coagulation pathway. As such, FXa is produced by both the intrinsic and extrinsic coagulation pathways. Theintrinsic coagulation pathway is activated primarily in the perfusion circuitand the extrinsic coagulation pathway is activated primarily in the surgicalwound. The result of both coagulation pathways is the production of the cir-culating protease, thrombin.
FibrinolysisOne of the effects of circulating thrombin is the activation of endothelial cells, leading to the release of tissue plasminogen activator (t-PA), which thenbinds to fibrin. The combination of t-PA, fibrin, and plasminogen cleaves plasminogen to plasmin. Plasmin then cleaves fibrin.
ComplementBoth the classic and alternative complement pathways are activated duringCPB (Figure 16.3). In the perfusion circuit, the blood–surface contact leads to activation of the classic pathway via C1, C2, and C4 to form C3 convertasewhich cleaves C3 into C3a and C3b. The alternate pathway, through factors B and D, also leads to production of C3b and may be the more important path-way during CPB [193]. The classic pathway is also activated at the terminationof CPB when protamine is administered and heparin–protamine complexesare formed [267].
C3b then cleaves C5 into C5a and C5b. C5b leads to production of the terminal complement complex (TCC) by binding with C6, C7, C8, and C9. TCCinteracts with cell membranes, leading to lysis of cells. In addition, TCC alsoleads to increased thrombin formation [268]. The released factors C3a, C4a,and C5a are vasoactive. C5a is a major neutrophil agonist [269,270].
PlateletsThe circulating platelets are subject to a variety of adverse influences duringCPB. Perhaps the first noticeable effect on the platelets is a reduction in their circulating numbers because of dilution with the pump prime volume.Heparin inhibits platelet binding to von Willebrand factor and increases thebleeding time [271,272]. Heparin leads to increased sensitivity of the platelet tocirculating agonists, including thrombin [273], C5b [268], plasmin [274,275],cathepsin G, serotonin, and epinephrine, among others. All of these influencescontribute to platelet loss and dysfunction.
The numbers of circulating platelets are also reduced by platelet–plateletadhesion and aggregation. Activated platelets express a variety of cell-surfaceglycoproteins and receptors that promote aggregation [276–278]. In addition

312 Chapter 16
to platelet–platelet aggregation, activated platelets also form aggregates withmonocytes and neutrophils [276,279].
A subset of the activated platelets will produce and release a variety of sub-stances, including thromboxane A2 [280], platelet factor 4, α-thromboglobulin[281], P-selectin [276], serotonin, adenosine diphosphate (ADP), adenosinetriphosphate (ATP), calcium, mitogens, acid hydrolases [282], and neutral proteases.
Although the effect will depend on many factors, both with respect to thepatient and the surgical procedure, the circulating platelet count typically falls by 30–50% during CPB [283,284]. In addition to intact platelets, there areoften platelet fragments in the circulation after the termination of CPB [285].The overall platelet function is reduced and there is typically a prolongation ofthe measured bleeding time after CPB [283].
Endothelial cellsDuring CPB, endothelial cells are activated by thrombin, C5a, and a variety ofcytokines [e.g. interleukin-1 (IL-1), tumor necrosis factor (TNF)] [286–288].
NeutrophilsThe neutrophils are responsible for much of the systemic inflammatoryresponse after CPB. These cells are strongly activated during CPB by kallikreinand C5a, but other agonists such as FXIIa, heparin, leukotriene B4, IL-1α, IL-8,and TNF also activate neutrophils [263,270,289,290]. Activated neutrophilsrelease a variety of detrimental substances, including elastase, cathepsin G,lysozyme, myeloperoxidase, defensins, acid hydrolases, bacterial permeab-ility agent, lactoferrin, collagenase, hydrogen peroxide, hydroxyl radicals,hypobromous acid, and hypochlorous acid [291].
MonocytesMonocytes are activated by monocyte chemotactic protein-1 (MCP-1), C5a,immune complexes, endotoxin, and IL-1 [292,293]. Activated monocytesexpress tissue factor, both in the perfusion circuit and in the surgical wound[294]. In addition, these monocytes produce a variety of cytokines (e.g. IL-1, IL-6, and TNF-α) that peak in concentration several hours after CPB [295,296].The number of circulating monocytes is not changed during CPB, but thisnumber increases for several hours after CPB [297,298].
LymphocytesThe numbers and function of both B and T cells are decreased in the first fewdays after CPB [299–301].
Consequences of hypothermiaMild to moderate hypothermia (25–34 °C) is used in conjunction with CPB toprovide some degree of organ protection from ischemic injury during theoperation. This safety margin with respect to organ ischemia is provided by

Complications of cardiopulmonary bypass and cardioplegia 313
a temperature-related reduction in the organs’ oxygen demand and con-sumption [302]. In neural tissues, there is also a direct beneficial effect ofhypothermia in terms of preservation of high-energy stores and a reduction in excitatory neurotransmitter release [303–306]. Because of a reduction in thebody’s oxygen consumption during hypothermia, CPB can be maintainedwith lower flow rates. The use of lower flow rates produces several importantbenefits for the patient and surgeon, including less blood trauma and bettervisualization in the operative field [307,308].
Hypothermia produces a variety of effects in the body’s organs [309]. Innearly all tissues, hypothermia decreases the organ blood flow, but this effectis pronounced for the skeletal muscle, kidneys, splanchnic bed, heart, andbrain. In the heart, hypothermia is associated with heart block and both atrialand ventricular arrhythmias. It is important that the patient’s temperature notbe allowed to fall precipitously during opening and cannulation because anyresulting arrhythmias may be difficult to control before the initiation of CPB. In the lung, hypothermia leads to decreased ventilation. In the kidneys,hypothermia leads to increased renal vascular resistance. There is a decrease in tubular reabsorption, the urine output may increase, and there is oftenspilling of glucose into the urine. The adjunctive technique of hemodilutionduring CPB may improve renal blood flow during CPB and limit renal injury.Hypothermia leads to decreased metabolic and excretory function in the liver,but clinically significant liver injury during hypothermic CPB is rare.
Hypothermic CPB often leads to hyperglycemia. Gluconeogenesis andglycogenolysis are increased and endogenous insulin production is decreased.Moreover, hypothermia results in a relative insensitivity to exogenous insulinadministration. The surgical team should monitor the serum glucose levelclosely and administer exogenous insulin, as needed. There is ample evidencethat avoiding even modest degrees of hyperglycemia may reduce the incid-ence of postoperative wound infection [310].
Water and electrolyte changes also accompany hypothermia. Hypothermialeads to a decrease in the free water clearance and serum potassium concentra-tion and to increases in serum osmolality.
Hypothermia produces both systemic and pulmonary vasoconstriction attemperatures < 26 °C [193]. Arteriovenous shunts may appear at low tem-peratures and have a deleterious effect on tissue oxygen delivery. There is an increase in blood viscosity and red blood cell aggregation and rouleaux formation may further reduce tissue oxygen delivery. Attention to properanesthesia, hemodilution, and administration of vasodilators may help to limitthese unwanted effects.
Profound hypothermia and circulatory arrestFor certain cardiovascular operations (e.g. aortic surgery), a period of circulat-ory arrest is helpful or necessary [302]. During periods of circulatory arrest, the use of profound hypothermia (16–20 °C) may help to limit ischemic centralnervous system (CNS) neurological injury. Data regarding a ‘safe’ period of
314 Chapter 16
circulatory arrest have been conflicting, but periods as long as 30–45 min arerelatively well tolerated at deep hypothermia. Neurological injury after pro-found hypothermia and circulatory arrest may manifest as choreoathetosis,seizures, transient metabolic encephalopathy, stroke, and neurocognitive disorders.
Every effort should be made to make these techniques as safe as possible for the patient. Circulatory arrest should not be initiated until there has beensufficiency time for uniform cerebral cooling. Topical cooling of the head (i.e. packed in ice) may be a useful adjunct. The use of barbiturates and cor-ticosteroids is advocated by many authorities as useful adjuncts as well.
Metabolic consequences of CPBThe use of CPB produces a variety of changes in the endocrine, humoral, andmetabolic functions of the body.
Pituitary hormonesThe serum concentration of vasopressin [antidiuretic hormone (ADH)] isincreased significantly with the use of CPB and persists for several hours postoperatively [311–313]. This exaggerated ADH response may be due to avariety of causes, including: transient hypotension at the initiation of CPB, a decrease in the circulating blood volume with the initiation of CPB, and adecrease in left atrial pressure with the initiation of CPB. ADH produces anincrease in the peripheral vascular resistance, a decrease in cardiac contractil-ity, a decrease in coronary blood flow, an increase in renal vascular resistance,and an increase in the release of von Willebrand factor [314,315]. The use ofpulsatile perfusion or adjunctive regional anesthetic techniques (e.g. thoracicepidural anesthesia) may blunt, but not eliminate the exaggerated ADHresponse during CPB [313,316–318].
Adrenal hormonesDuring hypothermic CPB, the plasma epinephrine concentration is typicallyincreased 10-fold and the plasma norepinephrine level is typically increasedfourfold [319–322]. The increased concentrations of these catecholamines leadsto increased peripheral vasoconstriction and changes in intraorgan blood flow[320–324]. The use of deeper anesthesia, regardless of the type of anesthesia,may reduce the catecholamine response to CPB [325–328]. The effect of pul-satile perfusion on the catecholamine response is not clear [320,329].
Cortisol is released in response to the stress of any major operation, usuallywith a quick rise in concentration and then a slow fall to baseline within 24 h[330]. With CPB, cortisol rises to a high concentration during CPB and remainsmarkedly elevated for > 48 h postoperatively [331–333]. Some studies haveshown a blunted cortisol response with greater degrees of hypothermia [334]and with the adjunctive use of thoracic epidural anesthesia [327,328]. There is also an increase in adrenocorticotropic hormone (ACTH) in response to CPB [335].
Complications of cardiopulmonary bypass and cardioplegia 315
Atrial natriuretic factorAlthough there is some conflicting evidence, most studies have shownreduced levels of atrial natriuretic factor during CPB, especially in thosepatients with high preoperative levels (e.g. those with valvular heart disease)[336–338]. For most patients, there is a relative increase in atrial natriuretic factor that starts during rewarming and persists for up to several days afterCPB [336,338–340]. Outside the setting of CPB, atrial natriuretic factor isreleased in response to atrial distension and acts to increase glomerular filtration, inhibit renin release, reduce the serum aldosterone concentra-tion, and reduce the arterial blood pressure. In patients undergoing CPB, thenormal regulatory mechanisms are lost during CPB and are diminished for thefirst 24 h postoperatively [341,342].
Renin–angiotensin–aldosterone axisThe role of the renin–angiotensin–aldosterone axis during CPB is unclear[343]. For patients undergoing non-pulsatile hypothermic CPB, renin,angiotensin II, and aldosterone concentrations are elevated during and shortlyafter CPB [344–346]. Angiotensin-converting enzyme concentrations, cor-rected for the degree of hemodilution, are probably not affected by CPB but are typically lower than normal during rewarming and for some period post-operatively [322,347]. Most evidence suggests that postoperative hypertensionis not related to abnormal concentrations of renin, angiotensin II, or aldos-terone [348,349].
Thyroid hormonesSeveral studies have documented the presence of sick euthyroid syndrome in patients during and after CPB [350]. This syndrome is characterized bydecreased T3 concentrations, normal or reduced T4 concentrations, decreasedfree thyroxine, and normal thyrotropin concentrations. Administration of heparin before CPB causes a slight increase in the free serum T3 and T4 con-centrations because heparin displaces these hormones from various bind-ing proteins [351,352]. Adjusted for the level of hemodilution, however, T3 concentrations are not altered by CPB [322]. During normothermic CPB,thyrotropin concentrations are normal, but during hypothermic CPB, thyro-tropin levels fall with the initiation of CPB and then rise steadily during theperiod of CPB [351,353].
Based on the fact that T3 regulates the heart rate, contractility, and oxygenconsumption, some authorities have advocated the administration of T3 peri-operatively to improve cardiac function. In experimental models, T3 adminis-tration has been shown to improve myocardial contractility after CPB [354,355].In human studies, however, the evidence has been conflicting [356,357].
Other serum changesWith the initiation of CPB, there is a fall in the serum total and ionized calciumlevels [358–362]. With crystalloid priming solutions, the fall in the calcium
316 Chapter 16
concentration is due to hemodilution. Historically, many surgeons and anes-thesiologists have favored the administration of calcium empirically at theconclusion of CPB to help with weaning from CPB. The effectiveness of this approach is not certain, however. Excessive calcium administration (i.e.without a decrease in the ionized calcium concentration) may contribute to perioperative pancreatitis and reduce the effectiveness of α-adrenergicreceptor agonists [362,363].
Similar to calcium, the serum concentrations of total and ultrafiltratablemagnesium also fall with the initiation of CPB [362,364]. After CPB, serummagnesium levels return to normal only very slowly [361]. In the postoperat-ive period, hypomagnesemia may predispose the patient to the developmentof both atrial and ventricular arrhythmias, so many authorities recommendempiric replacement or supplementation with magnesium during and earlyafter CPB [364–366].
The serum potassium level can vary considerably during CPB. In theabsence of cardioplegia, the serum potassium concentration typically fallsduring hypothermic CPB. In most patients, however, the use of hyperkalemiccardioplegia solutions will promote a tendency for a rise in the serum potas-sium concentration during CPB [367]. The serum potassium concentrationshould be monitored closely during CPB, but a normal concentration is notneeded until after CPB and a normal electrical rhythm is needed [368]. Afterthe termination of CPB, there is typically an exaggerated loss of potassium inthe urine and the clinician should be alert to this possibility [369].
Effects of CPB on the lungThe lungs are affected by CPB in several ways [370–375]. First, collapse of thelungs during CPB produces atelectasis that may persist postoperatively.Second, the lung is a target organ for the systemic inflammatory response toCPB. And lastly, pulmonary metabolic activity is affected by CPB.
AtelectasisAtelectasis is the most common pulmonary complication after cardiac surgery[371]. Many patients undergoing cardiac surgical procedures will be predis-posed to the development of atelectasis on the basis of a smoking history,chronic bronchitis, obesity, or the presence of pulmonary edema. Even beforethe initiation of CPB, passive ventilation with a paralyzed diaphragm and amonotonous ventilatory pattern will predispose the patient to the develop-ment of atelectasis.
During a typical cardiac surgical procedure, many technical aspects of theoperation itself may contribute to atelectasis. If the left internal mammaryartery (IMA) is used for revascularization, the left pleural space is typicallyentered. Once the left pleural cavity is exposed, blood and irrigation fluid may collect in the pleural space and cause compression of the lung. Because ofthis problem, some surgeons advocate an extrapleural dissection of the IMA. Once CPB is initiated, the heart rests on the left lower lobe and this may be one
Complications of cardiopulmonary bypass and cardioplegia 317
explanation for the high frequency of left lower lobe atelectasis after CPB.Endotracheal suctioning during the procedure may produce mucosal injuryand lead to atelectasis. Surfactant may be inhibited during CPB and this, combined with increased lung water due to complement activation, may alsopredispose the patient to atelectasis.
The degree of atelectasis will vary from patient to patient, but the functionalresidual capacity (FRC) will decrease by approximately 20% [372]. Because of atelectasis, the arterial-alveolar (A–a) oxygen gradient is elevated after CPB and remains elevated for at least 7 days postoperatively. Intrapulmonaryshunting is also increased during CPB. Other mechanical changes that havebeen observed during or after CPB include a decrease in lung compliance andan increase in airway resistance, but it is difficult to determine the relative con-tribution of CPB (rather than other aspects of the operation) to these changes.Nonetheless, these changes lead to a situation in which there is increased workof breathing postoperatively.
Efforts to prevent atelectasis during CPB have produced only mixed results.There is some evidence to suggest that avoiding entry into the pleural space(s)may lead to better lung compliance postoperatively. A variety of ventilatormanagement strategies during CPB, including intermittent or low-pressurestatic inflation of the lungs, have produced conflicting results with regard topostoperative lung function [373]. At the conclusion of CPB, it may be helpfulto administer a series of sighs, with airway pressures of approximately 30 cmH2O to help reverse any atelectasis that has developed during CPB. After operation, the most effective treatment for atelectasis is positive-pressure ventilation which is provided for most patients as routine care. The clinicianshould be aware that levels of positive end-expiratory pressure (PEEP) > 6 cmH2O may impair the cardiac output. As an alternative, relatively large tidalvolumes (i.e. 12–15 ml/kg) may be helpful. A high A–a gradient postoperat-ively may also be due to underlying chronic lung disease or to the presence ofpulmonary edema.
Acute lung injurySoon after the introduction of CPB in the 1950s, a syndrome of acute re-spiratory failure termed ‘pump lung’ was noted to carry a high mortality rate.This acute lung injury was originally thought to be due to microemboli, but the use of appropriate filters in the perfusion circuit did not eliminate this complication. Today, most acute lung injury is thought to be mediated by com-plement activation [374].
There is a significant relationship between the duration of CPB, the degree ofelevation of the circulating levels of C3a, and the degree of lung dysfunctionafter CPB. In animal studies, complement produces pulmonary leukocytesequestration and intrapulmonary release of thromboxane A2 that producespulmonary vasoconstriction and hypertension. There is also an accompanyingincrease in pulmonary vascular permeability that leads to an increase in lungwater.
318 Chapter 16
The incorporation of filters in the perfusion circuit is used to limit microembolization and its contribution to acute lung injury. Leukocyte filters have been used for leukocyte depletion during CPB, with varying effectiveness in preventing postoperative lung dysfunction [375]. Leukocytedepletion of the residual volume of blood in the pump at the conclusion of CPBcan also be used to help improve postoperative lung function. Hemodilutionand avoidance of pulmonary vascular distension (i.e. with appropriate leftheart venting) may also help to improve postoperative lung function.
Renal effects of cardiopulmonary bypassSeveral factors associated with cardiac surgery, including not only CPB but also hypothermia and hemodilution, may produce an adverse effect on renal function postoperatively. The relative contributions of each of thesefactors remain uncertain. Although the frequency of postoperative renal failure has decreased in recent years, this complication still carries a poor prognosis [376–379]. Not only is there a high associated short- (approxim-ately 50%) and long-term mortality rate, but this complication typically is associated with other early postoperative complications, prolongs the hospitalstay, and is associated with a substantial increase in the cost of medical care[380].
The incidence of postoperative renal failure after cardiac surgery that neces-sitates dialysis is approximately 1% [377,381]. Postoperative renal failure has been associated with a variety of preoperative patient-related factors,including: impaired renal function, impaired preoperative cardiac function,diabetes, peripheral vascular disease, history of acute rheumatic fever, olderpatient age, more complex operations (i.e. valvular surgery rather than first-time CABG), previous myocardial infarction, and the presence of congestiveheart failure [378,380,382–386].
The contribution of CPB per se to postoperative renal dysfunction is notentirely clear. Hemodilution is thought to increase tissue microcirculatoryblood flow and oxygen delivery because of a reduction in the blood viscosity,but this effect has not been demonstrated in the human kidney [387]. Moststudies that have examined the effect of varying levels of hypothermia on post-operative renal function have failed to show a relationship [388]. Both animaland clinical studies of pulsatile vs. non-pulsatile perfusion have failed to showa relationship between perfusion technique and postoperative renal function[389–393]. With the use of membrane oxygenators and arterial line filters, thereis a reduction in embolism during CPB and this, theoretically, should help to prevent embolic damage to the kidneys during CPB. The most importantperioperative factors related to postoperative renal dysfunction are thought to be renal hypoperfusion due to either low perfusion pressures during CPB orto the use of vasoconstrictor agents.
Dopamine administered intravenously at low dose (1–3 μg/kg per min) has been shown to increase renal blood flow. Although the practice of admin-istering dopamine at low dose in the perioperative period is common, there is
Complications of cardiopulmonary bypass and cardioplegia 319
no conclusive evidence that dopamine can ameliorate postoperative renal dysfunction, whether the agent is administered before or after the renal dysfunction becomes apparent [394,395]. Recent studies of the selectivedopamine-2 receptor agonist, fenoldopam, have shown that this agent, whenadministered prophylactically to patients undergoing intravenous dye tests,confers a degree of protection from postprocedure renal dysfunction [396].This benefit has not yet been confirmed in cardiac surgical patients, however.Other agents such as clonidine [397], calcium channel blockers [398,399], andatrial natriuretic peptide analogs [400,401] have not shown a convincingbenefit in preventing or treating postoperative renal failure.
Neurological effects of CPBNeurological complications after cardiac surgery can be categorized into three general types: encephalopathy, stroke, and neurocognitive disorders[402–405]. The incidence of major neurological complications after cardiacsurgery is reported to be approximately 1–6%, but this figure does not include those with neurocognitive disorders [406–409]. In an alternative, andincreasingly popular, classification, these complications have been categ-orized as type I [cerebral death, non-fatal stroke, new transient ischemic attack(TIA)] or type II (new intellectual deterioration or new seizures) [406]. Thedevelopment of a major neurological complication is associated with a sub-stantial higher perioperative mortality rate, a prolonged hospital stay, andmarkedly increased in- and out-of-hospital medical costs [406,407,410].
Identified risk factors for the development of a type I neurological complica-tion include: proximal aortic atherosclerosis, a history of previous neurolog-ical event (e.g. TIA, stroke), use of an intraaortic balloon pump (IABP) duringthe surgical procedure, diabetes mellitus, hypertension, pulmonary disease,unstable angina, increasing patient age, perioperative hypotension, and theuse of LV venting during the operation [406]. Increasing patient age may be the most important risk factor, with an approximately 2% risk of a type I neurological complication at age 40–49 years but an approximately 8% risk atage 70–79 years [406]. Although there is some overlap, the risk factors for thedevelopment of a type II neurological complication are somewhat different:increasing patient age, pulmonary disease, hypertension, history of excessivealcohol consumption, history of previous CABG, arrhythmias, history ofperipheral vascular disease (PVD), and congestive heart failure (CHF) on theday of operation.
In recent years, it has become apparent that neurocognitive (type II) compli-cations are probably much more common than type I complications. At thetime of discharge from the hospital, the prevalence of neurocognitive declinemay be as high as 60%, depending on the testing methods used to documentthis complication [411–413]. In the early postoperative period, the results of testing may be influenced by poor patient cooperation due to pain, sleepdeprivation, and the effects of medications. Deficits have been documented in psychomotor speed, attention and concentration, new learning ability, and
320 Chapter 16
short-term memory. These neurocognitive changes may persist for monthsafter operation and have an immeasurable effect on the individual patient’squality of life.
Considerable efforts have been made to understand the relative con-tributions of many perioperative factors on the development of neurologicalcomplications after CPB. Nonetheless, it has been difficult to dissect out theindividual contributions of potentially detrimental factors such as emboliza-tion, hypoperfusion, hypoxia, hypotension, arrhythmias, disorders in coagula-tion, dehydration, and inflammation. All patients undergoing CPB probablyexperience some degree of embolization, despite the presence of filters in the perfusion circuit [410,414–416]. Transcranial Doppler has been used to document the significant relationship between the rate of cerebral emboliza-tion during CPB and the risk of a subsequent neurological complication [414].There is no convincing evidence that the mean perfusion pressure during CPBis related to the risk of neurological complications [417,418], but there can be no doubt that hypoperfusion regionally or in the microvasculature can contribute to neurological injury. Recently, there has been increased attentionto the systemic inflammatory response and its effect on the brain [419]. Several potential neuroprotective agents, including thiopental, propofol, andnimodipine, have been suggested, but there is little evidence for their effective-ness [419]. In early trials, aprotinin has shown promise as a neuroprotectiveagent during CPB [419]. It may be the case that inflammatory mechanisms may be as important as embolism in the etiology of neurological complicationsafter CPB.
Several aspects of the conduct of CPB have a bearing on neurological func-tion and the development of neurological complications after CPB. In the non-CPB setting, the brain is able to autoregulate cerebral blood flow with a meanarterial pressure of as low as 50–55 mmHg. Given the lack of reliable evidencelinking mean perfusion pressure and neurological outcomes, it is prudent to target the arterial perfusion pressure to be at least in this autoregulatoryrange. It is probably prudent to maintain the mean perfusion pressure higherfor patients at increased risk of cerebral hypoperfusion (e.g. known cerebralvascular disease, previous stroke). Although there have been some conflictingdata, most reports suggest that the systemic temperature during CPB probablyhas little independent effect on the frequency of postoperative neurologicalcomplications, at least for degrees of moderate hypothermia (28 °C) throughnormothermia (37 °C) [413,420–422]. Systemic rewarming at the end of CPBshould be conducted to avoid even small degrees (i.e. 39 °C) of systemic hyper-thermia. Although higher glucose concentrations in experimental modelshave been associated with worse neurological outcome, studies have failed to document this association in the clinical setting of CPB [413,423,424]. It isprudent to maintain the glucose concentration in the physiological range of150–250 mg/dl. There are conflicting reports on the effect of pH managementduring CPB in adult patients and the risk of neurological complications
Complications of cardiopulmonary bypass and cardioplegia 321
[425–428]. For adult patients at high risk of embolic events undergoing CPB at moderate hypothermia, alpha-stat pH management may be beneficial inreducing the embolic risk.
Despite the considerable morbidity that accompanies neurological injuriesafter CPB, it is not a common practice to monitor for the development of thesecomplications during CPB. Although the technical details are beyond thescope of this chapter, the methods that are available for this purpose include:measurement of jugular bulb oxyhemoglobin saturation [429]; near-infraredspectroscopy (NIRS) [430]; transcranial Doppler [431]; and electrophysiolo-gical monitors such as EEG and evoked potentials [432].
Complications of cardioplegia
Pathophysiological aspects of myocardial ischemic injuryIn the beating heart, the myocardial oxygen consumption (MvO2) is a functionof the heart rate, the stroke work, and the inotropic state [433,434]. During a typical cardiac surgical procedure, the MvO2 varies significantly. The MvO2 islowest when the heart is arrested and is greatest just after release of the aorticcross clamp, when an oxygen debt must be repaid. The MvO2 is also influencedby temperature, with markedly decreased MvO2 at lower temperatures.Myocardial ischemia occurs when there is an imbalance between myocardialoxygen delivery and myocardial oxygen consumption. Anaerobic metabolismresults in acidosis, mitochondrial dysfunction, and, eventually, myocardialnecrosis. ATP stores are reduced almost immediately, there is impaired con-tractility after a few minutes, and there is irreversible myocardial injury after30–40 min of warm (37 °C) ischemia. In its severe forms, this myocardialinjury can be apparent visually in the operating room, with discoloration of anaffected region of the heart. TEE may document regional wall motion abnorm-alities that are due to regional myocardial ischemia. Postoperatively, thisinjury can be documented by a rise in the serum creatinine kinase (CPK), itsmyocardial (MB) isoform, lactate dehydrogenase (LDH), and troponin [435].The peak of the CPK curve is usually at 24 h after injury, but the LDH peakmay occur 4–5 days after injury. The incidence of perioperative myocardialinfarction, documented by elevation of the cardiac enzymes, is approximately1–2%.
There is a spectrum of myocardial dysfunction after cardiac surgery, and some myocardial injury may be reversible. Myocardial ‘stunning’ refers tothe situation in which initially dysfunctional ischemic myocardium regainsnormal function after some period of time. For some patients, this situationmay be a manifestation of poor myocardial protection during the operation.For patients with substantial amounts of stunned myocardium, it may takehours or days for this recovery to occur. This condition can be manifested by alow cardiac output syndrome that may require inotropic or intraaortic balloon(IABP) support until the myocardium has recovered.

322 Chapter 16
Myocardial protectionThe earliest cardiac operations were performed on the beating heart. It was theintroduction, however, of CPB and controlled arrest of the heart that enabledcomplex coronary and intracardiac operations to be performed routinely. Theuse of a hyperkalemic ‘cardioplegia’ solution was first described in 1955. Atthat time, very high concentrations of potassium resulted in severe cardiacinjury and these solutions were abandoned [436]. For operations that requireda ‘still’ heart, fibrillatory arrest induced by hypothermia was widely used. It was not until the 1970s that cardioplegia solutions with lower potassiumconcentration were shown to avoid direct cardiac injury during use [437,438].These solutions have enjoyed widespread use because asystolic arrest sig-nificantly reduces the myocardial oxygen consumption. Despite years of study, there are still clinical challenges in the area of myocardial protection[439]. In most applications, intermittent doses of cardioplegia are delivered to satisfy the low-level oxygen and substrate demands of the myocardium during cardioplegic arrest.
Historically, hyperkalemic crystalloid solutions were used to achieve andmaintain cardioplegic arrest of the heart. More recently, blood cardioplegicsolutions in which oxygenated blood is mixed (1 : 1–8 : 1) with a hyperkalemiccrystalloid solution have become the standard. In animal studies, blood cardioplegia has been shown to reduce irreversible myocardial injury, reduceanaerobic metabolism, preserve high-energy phosphate stores, and result in better postischemic ventricular function compared with crystalloid car-dioplegia solutions [440,441]. Moreover, clinical studies of blood vs. crystal-loid cardioplegia have shown better outcomes (e.g. reduced perioperativemyocardial infarction, less postoperative low cardiac output syndrome, andimproved operative mortality rates) for blood cardioplegia [442].
Historically, cold cardioplegia solutions were used most commonly because of the added benefit of reduced oxygen consumption in the coldermyocardium. Often, cardioplegia solutions were supplemented with topicalcold saline or slush to help ensure cooling of the myocardium. If cold saline orslush is used, however, the surgeon must be aware of the small risk of phrenicnerve injury due to cold injury [443–445]. If phrenic nerve paralysis occurs, thepatient may require prolonged mechanical ventilation and other respiratorycomplications are more likely. More recently, it has been recognized that lowering the temperature of the myocardium provides only a small additivebenefit in terms of oxygen consumption on top of cardioplegic arrest at nor-mothermia [446]. This feature, combined with the finding that myocardialcooling results in slower recovery of postischemic ventricular function, hasprompted many surgeons to move toward the use of normothermic (37 °C) ortepid (approximately 34 °C) cardioplegia solutions.
Antegrade cardioplegiaAntegrade cardioplegia is administered directly into the aortic root. A purse-string suture is typically placed in the ascending aorta and a cardioplegia
Complications of cardiopulmonary bypass and cardioplegia 323
cannula or needle is introduced to deliver the cardioplegia. Cardioplegia is typically administered in an initial dose (to cause arrest of the heart) followed by maintenance doses every 15–30 min afterwards. In practice, themaintenance doses are usually given between anastomoses for CABG operations and at convenient points during valve or other procedures. Theperfusion pressure is monitored by the perfusionist and should be maintainedat approximately 70 mmHg. An inability to maintain an adequate perfusionpressure during administration of the cardioplegia solution during the initialdose may indicate aortic insufficiency. The perfusionist should be alert to this possibility and the surgeon should be vigilant for dilatation of the left ventricle that results in this situation. If this occurs, intermittent dosing (withperiods of aortic root venting), manual closure of the aortic valve (by pinch-ing), or the use of retrograde cardioplegia may be necessary. Before each maintenance dose of antegrade cardioplegia, the aortic root should be de-airedto prevent air entry into the coronary arteries.
Cardioplegia achieves its desirable effects (e.g. cardiac arrest, cardiac cooling) by distribution throughout the myocardium. The distribution of thecardioplegia solution in the myocardium will be most complete in territories of unobstructed coronary arteries. To help ensure better distribution of the cardioplegia solution, the use of retrograde cardioplegia should be consideredin patients with high-grade coronary stenoses or occluded coronary arteries.
Complications related to aortic root delivery of antegrade cardioplegia arerelatively uncommon, but include tearing of the aorta, local hematoma forma-tion, dissection of the aorta, and dislodgement of intraluminal plaque withsubsequent embolization. During cannulation, a site free of atherosclerotic disease should be selected; manual palpation, TEE, or epiaortic ultrasoundshould be used to help guide the surgeon. At the conclusion of the procedure,the cardioplegia cannula should be removed and the site should be securedwith a suture. Late aortic dissection or pseudoaneurysm formation at this siteare possible.
For most CABG operations performed with the use of CPB, administrationof continuous antegrade cardioplegia is not practical. During CABG proced-ures, continuous antegrade cardioplegia will flow through any unoccludedcoronary arteries and will obscure the operative field at the coronary arterio-tomy. As with beating heart surgery, a misted blower can be used to ‘sprayaway’ cardioplegia solution from the operative site if antegrade cardioplegia is administered at a low rate during creation of the anastomoses. During elevation of the heart for construction of bypass anastomoses on the lateralwall of the heart, kinking of the proximal coronary arteries may limit the ability to administer antegrade cardioplegia.
During operations for aortic valve replacement (AVR), an initial dose of cardioplegia can be administered by cannula in the aortic root as de-scribed above. Once the aorta is opened to expose the aortic valve, however,another cardioplegic technique must be selected for subsequent administra-tions of the cardioplegia solution. Retrograde cardioplegia is used commonly
324 Chapter 16
in this situation [447], but ostial perfusion cannulas can be inserted into the coronary ostia to deliver antegrade cardioplegia either continuously orintermittently. If continuous cardioplegia delivery is desired, small, flexible,soft-tipped cannulas can be placed in each of the coronary ostia and sutured inplace with fine silk or Prolene suture. These cannulas can be held out of theway with additional sutures. If intermittent cardioplegia delivery is satisfac-tory, the left and right coronary ostia can be cannulated successively withhand-held ostial perfusion cannulas. Whenever ostial perfusion cannulas areused, the perfusionist must be vigilant to the pressure of delivery and the sur-geon must be vigilant for dislodgement of the cannulas. With either continu-ous or intermittent delivery, direct injury to the coronary ostia may occur andlead to early or late coronary occlusion.
During operations for mitral valve repair (MVR) or replacement, eitherhand-held or self-retaining retractors used for left atrial exposure have the additional effect of rendering the aortic valve incompetent. As a result,maintenance doses of antegrade cardioplegia can be administered only if theretraction is released and the aortic root is vented of any air. This obviouslydisrupts the flow of the operative procedure. Most surgeons choose to use retrograde cardioplegia in this situation.
Retrograde cardioplegiaThe use of retrograde cardioplegia has come into widespread use, largelybecause of the problems with distribution of antegrade cardioplegia in situ-ations with occlusion or high-grade stenoses of the coronary arteries [448,449].Typically, the retrograde cardioplegia cannula is inserted through a purse-string suture in the right atrium and correct placement of the cannula in the coronary sinus is confirmed by palpation and/or TEE. If a balloon-tippedcannula and pressure monitoring line are used, inflation of the balloon shouldresult in ‘ventricularization’ of the pressure waveform. The cannula should be placed in the most proximal position in the coronary sinus that allowsproper fixation. Unlike antegrade cardioplegia, one particular advantage of retrograde cardioplegia is that repeated de-airing of the aortic root is notnecessary.
Because of the position of the posterior interventricular vein in the proximalportion of the coronary sinus, this vein will not receive cardioplegia solution ifthe tip (and balloon) of the retrograde cardioplegia cannula is passed beyondthis vein. This may be the most important drawback of retrograde cardiople-gia. If the cannula is advanced too far into the coronary sinus, the right side ofthe heart will not be perfused adequately [450–453]. Some authorities havesuggested carefully ‘backing out’ the retrograde cardioplegia cannula whilecardioplegia solution is administered at a low rate until the posterior intervent-ricular vein is seen to fill. Alternatively, a suture snare can be placed aroundthe coronary sinus, just proximal to the posterior interventricular vein, to pre-vent migration of the cannula into the right atrium.
Complications of cardiopulmonary bypass and cardioplegia 325
During administration of retrograde cardioplegia, the pressure in the cor-onary sinus should be measured continuously. Effective distribution of the cardioplegia solution requires coronary sinus pressures in the 25–40 mmHgrange. Excessive pressure in the coronary sinus may cause localized disruptionof this vessel and lead to hemorrhage [454]. When elevating or retracting theheart with a retrograde cardioplegia cannula in place, care should be taken toavoid direct injury of the coronary sinus with the cannula tip. Visible injuriesto the coronary sinus should be repaired with fine suture. Occasionally, coronary sinus injuries remain occult until excessive blood is noticed in thepericardial sac at the conclusion of the operative procedure. Another unusualcomplication of retrograde cardioplegia that has been reported is inadvertentpuncture of the inner wall of the right atrium [455].
Neurological protectionProfound hypothermia and circulatory arrest are helpful for a variety of car-diovascular operations (see Chapter 17, Complications of Aortic Surgery). Avariety of adjuncts are available to help prevent neurological injury duringthese operations and will be discussed elsewhere. Two adjuncts that relate tocardiopulmonary bypass are profound hypothermia and the use of retrogradecerebral perfusion.
Profound hypothermiaDuring many routine cardiac surgical procedures (e.g. CABG, valve replace-ment/repair), the systemic temperature can be maintained at normothermia(37 °C) or at mild hypothermia (32–36 °C) to avoid the unwanted effects of sys-temic hypothermia. For operations on the aortic arch or thoracoabdominal aorta,however, an ‘open’ approach is often necessary and profound degrees ofhypothermia (16–20 °C) with circulatory arrest can be used to reduce the cereb-ral or spinal cord oxygen requirements and help to limit neurological injuryduring the operation. The ‘safe’ period of circulatory arrest at profound degreesof hypothermia is probably 30–45 min [456–459]. Longer periods of circulat-ory arrest have been associated with increased risk of neurological injury.
Some operations are only possible with the use of profound hypothermiaand circulatory arrest. Nonetheless, profound hypothermia has a detrimentaleffect on platelet function and myocardial recovery postoperatively.
Retrograde cerebral perfusionAnother adjunct that may be useful during periods of profound hypothermiaand circulatory arrest is retrograde cerebral perfusion [460–466]. There is con-siderable debate about the practical details, however. In its typical application,a venous cannula or a cardioplegia-type cannula is inserted into the superiorvena cava. A tape or snare is secured around the cannula and retrograde per-fusion can be established. The perfusion should be measured and maintainedin the range of 25–30 mmHg [467].

326 Chapter 16
References
1 Westaby S, Bosher C. Landmarks in Cardiac Surgery. Oxford: ISIS Medical Media, 1997;49–89.
2 Gibbon JH. Application of mechanical heart and lung apparatus to cardiac surgery. MinnMed 1954; March: 171–185.
3 Melrose DG, Dreyer B, Bentall HH et al. Elective cardiac arrest. Lancet 1955; July 2: 21–22.4 Lillihei CW, DeWall RA, Gott VL et al. The direct vision correction of calcified aortic
stenosis by means of pump-oxygenator and retrograde coronary sinus perfusion. DisChest 1956; 30: 123–132.
5 Edmunds LH Jr, ed. Cardiac Surgery in the Adult. New York: McGraw-Hill, 1997.6 Gravlee GP, Davis RF, Kurusz Utley JR, eds. Cardiopulmonary Bypass. Principles and
Practice, 2nd edn. Philadelphia: Lippincott, Williams & Wilkins, 2000.7 Taylor KM, ed. Cardiopulmonary Bypass. Principles and Management. Baltimore: Williams
& Wilkins, 1986.8 Casthely PA, Bregman D. Cardiopulmonary bypass. Physiology, related complications,
and pharmacology. Mount Kisco, NY: Futura, 1991.9 Estafanous FG, Barash PG, Reves JG, eds. Cardiac Anesthesia. Principles and Clinical
Practice, 2nd edn. Philadelphia: Lippincott, Williams & Wilkins, 2001.10 DiNardo JA, ed. Anesthesia for Cardiac Surgery, 2nd edn. Stanford, CT: Appleton & Lange,
1998.11 Hessell EA II, Hill AG. Circuitry and cannulation techniques. In: Gravlee GP, Davis
RF, Kurusz M, Utley JR, eds. Cardiopulmonary Bypass: Principles and Practice, 2nd edn.Philadelphia: Lippincott, Williams & Wilkins, 2000; 69–97.
12 Ambesh SP, Singh SK, Dubey DK et al. Inadvertent closure of the superior vena cava afterdecannulation: a potentially catastrophic complication after termination of bypass. JCardiothorac Vasc Anesth 1998; 12: 723 [Letter].
13 Ratnaraj J, Manohar G. Pulmonary artery catheter displacement during cannulation forCPB. J Cardiothorac Vasc Anesth 1991; 5: 648 [Letter].
14 Troianos CA. Transesophageal echocardiographic diagnosis of pulmonary arterycatheter entrapment and coiling. Anesthesiology 1993; 79: 602–604.
15 Horrow JC, Laucks SO. Coronary air embolism during venous cannulation. Anesthesio-logy 1982; 56: 212–214.
16 McGiffin DC, Kirklin JK. Cardiopulmonary bypass for cardiac surgery. In: Sabiston DC Jr, Spencer FC, eds. Surgery of the Chest, 6th edn. Philadelphia: W.B. Saunders, 1995;1256–1271.
17 Toomasian JM, McCarthy JP. Total extrathoracic cardiopulmonary support with kineticassisted venous drainage: experience in 50 patients. Perfusion 1998; 13: 137–143.
18 Davila RM, Rawles T, Mack MJ. Venoarterial air embolus: a complication of vacuum-assisted venous drainage. Ann Thorac Surg 2001; 71: 1369–1371.
19 Bernstein EF, Gleason LR. Factors influencing hemolysis with roller pumps. Surgery1967; 61: 432–442.
20 Indeglia RA, Shea MA, Forstrom R et al. Influence of mechanical factors on erythrocytesublethal damage. Trans Am Soc Artif Intern Organs 1968; 14: 264–271.
21 Galletti PM, Brecher GA. Heart-Lung Bypass, Principle and Techniques of ExtracorporealCirculation. New York: Grune & Stratton, 1962; 184–188.
22 Harringer W. Capture of particulate emboli during cardiac procedures in which aorticcross-clamp is used. Ann Thorac Surg 2000; 70: 1119–1123.
23 Borger MA, Ivanov J, Weisel RD et al. Stroke during coronary bypass surgery: principalrole of cerebral macroemboli. Eur J Cardiothorac Surg 2001; 19: 627–632.
Complications of cardiopulmonary bypass and cardioplegia 327
24 Barbut D, Grassineau D, Lis E et al. Posterior distribution of infarcts in strokes related tocardiac operations. Ann Thorac Surg 1998; 65: 1656–1659.
25 Béïque FA, Joffe D, Tousignant G et al. Echocardiographic-based assessment and man-agement of atherosclerotic disease of the thoracic aorta. J Cardiothoracic Vasc Anesth 1998;12: 206–220.
26 Wong BI, McLean RF, Naylor CD et al. Central-nervous-system dysfunction after warmor hypothermic cardiopulmonary bypass. Lancet 1992; 339: 1383–1384.
27 Hammeke TA, Hastings JE. Neuropsychologic alterations after cardiac operation. JThorac Cardiovasc Surg 1998; 96: 326–331.
28 Shaw PJ, Bates D, Cartlidge NEF et al. Early neurological complications of coronaryartery bypass surgery. Br Med J 1985; 291: 1384–1387.
29 Newman MF, Kirchner JL, Phillips-Bute B et al. Longitudinal assessment of neurocog-nitive function after coronary-artery bypass surgery. N Engl J Med 2001; 344: 395–402.
30 Henriksen L. Evidence suggestive of diffuse brain damage following cardiac operations.Lancet 1984; 331: 816–820.
31 Åberg T, Ronquist G, Tydén H et al. Adverse effects on the brain in cardiac operations asassessed by biochemical, psychometric, and radiologic methods. J Thorac Cardiovasc Surg1984; 87: 99–105.
32 Weinstein GS. Left hemispheric strokes in coronary surgery: implications for end-holeaortic cannulas. Ann Thorac Surg 2001; 71: 128–132.
33 Bar-El Y, Goor DA. Clamping of the atherosclerotic ascending aorta during coronaryartery bypass operations: its cost in strokes. J Thorac Cardiovasc Surg 1992; 104: 469–474.
34 Ohteki H, Itoh T, Natsuaki M et al. Intraoperative ultrasonic imaging of the ascendingaorta in ischemic heart disease. Ann Thorac Surg 1990; 50: 539–542.
35 Wareing TH, Davilla-Roman VG, Barzilai B et al. Management of the severely atheroscle-rotic ascending aorta during cardiac operations: a strategy for detection and treatment. J Thoracic Cardiovasc Surg 1992; 103: 453–462.
36 Sylivris S, Calafiore P, Matalanis G et al. The intraoperative assessment of ascending aor-tic atheroma: epiaortic imaging is superior to both transesophageal echocardiographyand direct palpation. J Cardiothorac Vasc Anesth 1997; 11: 704–707.
37 Dávilla-Román VG, Phillips KJ, Daily BB et al. Intraoperative transesophageal echocar-diography and epiaortic ultrasound for assessment of atherosclerosis of the thoracicaorta. J Am Coll Cardiol 1996; 28: 942–947.
38 Still RJ, Hilgenberg AD, Atkins CW et al. Intraoperative aortic dissection. Ann ThoracSurg 1992; 53: 374–380.
39 Gott JP, Cohen CL, Jones EL. Management of ascending aortic dissections andaneurysms early and late following cardiac operations. J Card Surg 1990; 5: 2–13.
40 Aoyagi S, Tayama E, Nishimi M et al. Aortic dissections complicating open cardiacsurgery: report of three cases. Surg Today 2000; 30: 1022–1025.
41 Ishino K, Murakami T, Teramoto S. Cannulation-induced coronary artery dissection:successful management with circulatory assist devices and coronary bypass grafting.Surg Today 1998; 28: 563–566.
42 Salama FD, Blesovsky A. Complications of cannulation of the ascending aorta for openheart surgery. Thorax 1970; 25: 604–607.
43 Benedict JS, Buhl TL, Henney RP. Acute aortic dissection during cardiopulmonarybypass. Arch Surg 1974; 108: 810–813.
44 Carey JS, Skow JR, Scott C. Retrograde aortic dissection during cardiopulmonary bypass:“nonoperative” management. Ann Thorac Surg 1977; 24: 44–48.
45 Gates JD, Bichell DP, Rizzo RJ et al. Thigh ischemia complicating femoral vessel cannula-tion for cardiopulmonary bypass. Ann Thorac Surg 1996; 61: 730–733.
328 Chapter 16
46 Sabik JF, Lytle BW, McCarthy PM et al. Axillary artery: an alternative site of arterial cannulation for patients with extensive aortic and peripheral vascular disease. J ThoracCardiovasc Surg 1995; 109: 885–891.
47 Baribeau YR, Westbrook BM, Charlesworth DC et al. Arterial inflow via an axillary arterygraft for the severely atherosclerotic aorta. Ann Thorac Surg 1998; 66: 33–37.
48 High KM, Bashein G, Kurusz M. Principles of oxygenator function. Gas exchange, heattransfer, and operation. In: Gravlee GP, Davis RF, Kurusz M, Utley JR, eds. Cardio-pulmonary Bypass: Principles and Practice, 2nd edn. Philadelphia: Lippincott Williams &Wilkins, 2000; 49–68.
49 Nilsson L, Bagge L, Nyström S-O. Blood cell trauma and postoperative bleeding: com-parison of bubble and membrane oxygenators and observations on coronary suction.Scand J Thorac Cardiovasc Surg 1990; 24: 65–69.
50 Tabak C, Eugene J, Stemmer EA. Erythrocyte survival following extracorporeal cir-culation: a question of membrane versus bubble oxygenator. J Thorac Cardiovasc Surg1981; 81: 30–33.
51 Pearson DT. Gas exchange: bubble and membrane oxygenators. Semin Thorac CardiovascSurg 1990; 2: 313–319.
52 Peterson KA, Dewanjee MK, Kaye MP. Fate of indium 111-labeled platelets during cardiopulmonary bypass performed with membrane and bubble oxygenators. J ThoracCardiovasc Surg 1982; 84: 39–43.
53 Edmunds LH Jr, Ellison N, Colman RW et al. Platelet function during cardiac operation:comparison of membrane and buddle oxygenators. J Thorac Cardiovasc Surg 1982; 83:805–812.
54 Padayachee TS, Parsons S, Theobold R et al. The detection of microemboli in the middlecerebral artery during cardiopulmonary bypass: a transcranial Doppler ultrasound invest-igation using membrane and bubble oxygenators. Ann Thorac Surg 1987; 44: 298–302.
55 Pedersen TH, Karlsen HM, Semb G et al. Comparison of bubble release from varioustypes of oxygenators: an in vivo investigation. Scand J Thorac Cardiovasc Surg 1987; 21:73–80.
56 Hatori N, Yoshizu H, Haga Y et al. Biocompatibility of heparin-coated membrane oxygenator during cardiopulmonary bypass. Artif Organs 1994; 18: 904–910.
57 Shigemitsu O, Hadama T, Takasaki H et al. Biocompatibility of heparin-bonded mem-brane oxygenator (Carmeda MAXIMA) during the first 90 minutes of cardiopulmonarybypass: clinical comparison with the conventional system. Artif Organs 1994; 18: 936–941.
58 Tayama E, Raskin SA, Nose Y. Blood pumps. In: Gravlee GP, Davis RF, Kurusz M, UtleyJR, eds. Cardiopulmonary Bypass: Principles and Practice, 2nd edn. Philadelphia: Lippincott,Williams & Wilkins, 2000; 37–48.
59 Tempe DK, Khanna SK. Accidental hyperperfusion during cardiopulmonary bypass:suggested safety features. Ann Thorac Surg 1998; 65: 306 [Letter].
60 Briceño JC, Runge TM. Tubing spallation in extracorporeal circuits. An in vitro studyusing an electronic particle counter. Int J Artif Organs 1992; 15: 222–228.
61 Noon GP, Harrell JE Jr, Feldman L et al. Development and evaluation of pulsatile rollerpump and tubing for cardiac assistance. Artif Organs 1983; 7: 49–54.
62 Peek GJ, Thompson A, Killer HM et al. Spallation performance of extracorporeal oxy-genation tubing. Perfusion 2000; 15: 457–466.
63 Kolff J, McClurken JB, Alpern JB. Beware centrifugal pumps: not a one-way street, but a potentially dangerous “siphon”. Ann Thorac Surg 1990; 50: 512 [Letter].
64 Jenkins OF, Morris R, Simpson JM. Australasian perfusion incident survey. Perfusion1997; 12: 279–288.
Complications of cardiopulmonary bypass and cardioplegia 329
65 Hessel EAII, Hill AG. Cardiotomy suction and venting. In: Gravlee GP, Davis RF, KuruszM, Utley JR, eds. Cardiopulmonary Bypass: Principles and Practice, 2nd edn. Philadelphia:Lippincott, Williams & Wilkins, 2000; 98–104.
66 Edmunds LH Jr, Saxena NC, Hillyer P et al. Relationship between platelet count and cardiotomy suction return. Ann Thorac Surg 1978; 25: 306–310.
67 Pearson DT. Microemboli: gaseous and particulate. In: Taylor KM, ed. CardiopulmonaryBypass: Principles and Management. Baltimore: Williams & Wilkins, 1986; 313–354.
68 Wright G, Sanderson JM. Cellular aggregation and trauma in cardiotomy suction systems. Thorax 1979; 34: 621–628.
69 Solis RT, Noon GP, Beall AC Jr et al. Particulate microembolism during cardiac operation.Ann Thorac Surg 1974; 17: 332–344.
70 Liu JT-F, Su Z-K, Ding W-X. Quantitation of particulate microemboli during cardiopul-monary bypass: experimental and clinical studies. Ann Thorac Surg 1992; 54: 1196–1202.
71 Brooker RF, Brown WR, Moody DM et al. Cardiotomy suction: a major source of brainlipid emboli during cardiopulmonary bypass. Ann Thorac Surg 1998; 65: 1651–1655.
72 Tabuchi N, de Haan J, Boonstra PW et al. Activation of fibrinolysis in the pericardial cavity during cardiopulmonary bypass. J Thorac Cardiovasc Surg 1993; 106: 828–833.
73 Siderys H. Pericardial fluid and hemolysis. Ann Thorac Surg 1993; 56: 595 [Letter].74 Orenstein JM, Sato N, Aaron B et al. Microemboli observed in deaths following car-
diopulmonary bypass surgery: silicone antifoam agents and polyvinyl chloride tubing assources of emboli. Hum Pathol 1982; 13: 1082–1090.
75 de Jong JCF, ten Duis HJ, Sibinga CTS. Hematologic aspects of cardiotomy suction in cardiac operations. J Thorac Cardiovasc Surg 1980; 79: 227–236.
76 Boonstra PW, van Imhoff GW, Eysman L et al. Reduced platelet activation and improvedhemostasis after controlled cardiotomy suction during clinical membrane oxygenatorperfusions. J Thorac Cardiovasc Surg 1985; 89: 900–906.
77 Wielogorske JW, Cross DE, Nwadike EVO. The effects of subatmospheric pressure onthe hemolysis of blood. J Biomechan 1975; 8: 321–325.
78 Hirose T, Burman SO, O’Connor RA. Reduction of perfusion hemolysis by use of atraum-atic low-pressure suction. J Thorac Cardiovasc Surg 1964; 47: 242–247.
79 Arom KV, Vinas JF, Fewel JE et al. Is a left ventricular vent necessary during cardiopul-monary bypass? Ann Thorac Surg 1977; 24: 566–573.
80 Burton NA, Graeber GM, Zajtchuk R. An alternate method of ventricular ventingathepulmonary artery sump. Chest 1984; 85: 814–815.
81 Breyer RH, Meredity JW, Mills SA et al. Is a left ventricular vent necessary for coronaryartery bypass operations performed with cardioplegic arrest? J Thorac Cardiovasc Surg1983; 86: 338–349.
82 Olinger GN, Bonchek LI. Ventricular venting during coronary revascularization: assess-ment of benefit by intraoperative ventricular function curves. Ann Thorac Surg 1978; 26:525–534.
83 Najafi H, Javid H, Goldin MD et al. Aortic valve replacement without left heart decom-pression. Ann Thorac Surg 1976; 21: 131–133.
84 Salerno TA, Charrette EJP. Elimination of venting in coronary artery surgery. Ann ThoracSurg 1979; 27: 340–343.
85 Utley JR, Stephens DB. Venting during cardiopulmonary bypass. In: Utley JR, ed.Pathophysiology and Techniques of Cardiopulmonary Bypass, Vol. II. Baltimore: Williams &Wilkins, 1983; 115–127.
86 Robicsek F, Duncan GD. Retrograde air embolization in coronary operations. J ThoracCardiovasc Surg 1987; 94: 110–114.
330 Chapter 16
87 Tingleff J, Joyce FS, Pettersson G. Intraoperative echocardiographic study of airembolism during cardiac operations. Ann Thorac Surg 1995; 60: 673–677.
88 O’Connor BR, Kussman BD, Park KW. Severe hypercarbia during cardiopulmonarybypass: a complication of CO2 flooding of the surgical field. Anesth Analg 1998; 86:264–266.
89 Kurusz M, Mills NL. Management of unusual problems encountered in initiating andmaintaining cardiopulmonary bypass. In: Gravlee GP, Davis RF, Kurusz M, Utley JR,eds. Cardiopulmonary Bypass: Principles and Practice, 2nd edn. Philadelphia: LippincottWilliams and Wilkins, 2000; 578–612.
90 Stoney WS, Alford WC, Burrus GR et al. Air embolism and other accidents using pumpoxygenators. Ann Thorac Surg 1980; 29: 336–340.
91 Kurusz M, Butler B, Katz J et al. Air embolism during cardiopulmonary bypass. Perfusion1995; 10: 361–391.
92 Mitchell S, Gorman D. The pathophysiology of cerebral arterial gas embolism. J ExtraCorpor Technol 2002; 34: 18–23.
93 Kurusz M, Wheeldon DR. Risk containment during cardiopulmonary bypass. SeminThorac Cardiovasc Surg 1990; 2: 400–409.
94 Dennis C. Perspective in press: one group’s struggle with development of a pump-oxygenator. Trans Am Soc Artif Intern Organ 1985; 31: 1–11.
95 Chaudhuri N, Hickey MS. A simple method of treating coronary air embolism after cardiopulmonary bypass. Ann Thorac Surg 1999; 68: 1867–1868.
96 Sandhu AA, Spotnitz HM, Dickstein ML et al. Retrograde cardioplegia preservesmyocardial function after induced coronary air embolism. J Thorac Cardiovasc Surg 1997;113: 917–922.
97 Butler BD, Laine GA, Leiman BC et al. Effect of the Trendelenberg position on the distribution of arterial air emboli in dogs. Ann Thorac Surg 1988; 45: 198–202.
98 Mehlhorn U, Burke EJ, Butler BD et al. Body position does not affect the hemodynamicresponse to venous air embolism in dogs. Anesth Analg 1994; 79: 734–739.
99 Watanabe T, Shimasaki T, Kuraoka S et al. Retrograde cerebral perfusion against massiveair embolism during cardiopulmonary bypass. J Thorac Cardiovasc Surg 1992; 104:532–533 [Letter].
100 Rozanski J, Szufladowicz M. Successful treatment of massive air embolism. J Card Surg1994; 9: 430–432.
101 Stark J, Hough J. Air in the aorta: treatment by reversed perfusion. Ann Thorac Surg 1986;41: 337–338.
102 Hendricks FFA, Bogers AJJC, de la Riviere AB et al. The effectiveness of venoarterial per-fusion in treatment of arterial air embolism during cardiopulmonary bypass. Ann ThoracSurg 1983; 36: 433–436.
103 Kern JA, Arnold S. Massive cerebral embolization: successful treatment with retrogradeperfusion. Ann Thorac Surg 2000; 69: 1266–1268.
104 Lar LW, Lai LC, Ren LW. Massive arterial air embolism during cardiac operation: successful treatment in a hyperbaric chamber under 3 ATA. J Thorac Cardiovasc Surg 1990;100: 928–930 [Letter].
105 Armon C, Deschamps C, Adkinison C et al. Hyperbaric treatment of cerebral airembolism sustained during an open-heart surgical procedure. Mayo Clin Proc 1991; 66:565–571.
106 Bitterman H, Melamed Y. Delayed hyperbaric treatment of cerebral air embolism. Israel JMed Sci 1993; 29: 22–26.
Complications of cardiopulmonary bypass and cardioplegia 331
107 Franklin C. The technique of radial artery cannulation. Tips for maximizing results whileminimizing the risk of complications. J Crit Ill 1995; 10: 424–432.
108 Slogoff S, Keats AS, Arlund C. On the safety of radial artery cannulation. Anesthesiology1983; 59: 42–47.
109 Wilkins RG, Lane N. Radial artery cannulation and ischaemic damage: a review.Anesthesia 1985; 40: 896–899.
110 Rose SH. Ischemic complications of radial artery cannulation: an association with a cal-cinosis, Raynaud’s phenomenon, esophageal dysmotility, sclerodactyly, and telangiec-tasia variant of scleroderma. Anesthesiology 1993; 78: 587–589.
111 Gronbeck C, Miller EL. Nonphysician placement of arterial catheters: experience with500 insertions. Chest 1993; 104: 1716–1717.
112 Mangar D, Laborde RS, Vu DN. Delayed ischaemia of the hand necessitating amputationafter radial artery cannulation. Can J Anesth 1993; 40: 247–250.
113 Grier D, Hartnell G. Percutaneous femoral artery puncture. Prac Anat Br J Radiol 1990;63: 602–604.
114 Resar JR, Brinker JA. Peripheral arterial access. The large and small of it. Cathet CardiovascDiagn 1994; 33: 212–213.
115 Smith SMV, Galland RB. Late presentation of femoral artery complications followingpercutaneous cannulation for cardiac angiography or angioplasty. J Cardiovasc Surg1992; 33: 437–439.
116 Polderman KH, Girbes ARJ. Central venous catheter use. Part 2: Infectious complica-tions. Intens Care Med 2002; 28: 18–28.
117 Polderman KH, Girbes ARJ. Central venous catheter use. Part 1: Mechanical complica-tions. Intens Care Med 2002; 28: 1–17.
118 Bambauer R, Inniger R, Pirrung KJ et al. Complications and side-effects associated withlarge-bore catheters in the subclavian and internal jugular veins. Artif Org 1994; 18:318–321.
119 Herbst CA Jr. Indications, management, and complications of percutaneous subclaviancatheters. Arch Surg 1978; 113: 1421–1425.
120 Conces DJ, Holden RW. Aberrant locations and complications in initial placement ofsubclavian vein catheters. Arch Surg 1984; 119: 293–295.
121 Smith BE, Model JH, Gaub ML et al. Complications of subclavian vein catheterization.Arch Surg 1965; 90: 228–229.
122 Robinson JF, Robinson WA, Cohn A et al. Perforation of the great vessels during centralvenous line placement. Arch Intern Med 1995; 155: 1225–1228.
123 Gray P, Sullivan G, Ostryzniuk P et al. Value of postprocedural chest radiographs in theadult intensive care unit. Crit Care Med 1992; 20: 1513–1518.
124 Duntley P, Siever J, Korwes ML. Vascular erosion by central venous catheters. Chest 1992;101: 1633–1638.
125 Whitman ED. Complications associated with the use of central venous access devices.Curr Probl Surg 1996; 33: 309–378.
126 Snyder RH, Archer FJ, Endy T et al. Catheter infection: a comparison of two cathetermaintenance techniques. Ann Surg 1988; 208: 651–653.
127 Flanagan JP, Gradisar IA, Gross RJ et al. Air embolus: a lethal complication of subclavianvenipuncture. New Engl J Med 1969; 281: 488–489.
128 Reeves ST, Roy RC, Dorman BH. The incidence of complications after the double-cathetertechnique for cannulation of the right internal jugular vein in a university teaching hospital. Anesth Analg 1995; 81: 1073–1076.
332 Chapter 16
129 Shah KB, Rao TLK, Laughlin S et al. A review of pulmonary artery catheterization in6,245 patients. Anesthesiology 1984; 61: 271–275.
130 Salmenpera M, Peltola K, Rosenberg P. Does prophylactic lidocaine control cardiacarrhythmias associated with pulmonary artery catheterization? Anesthesiology 1982; 56:210–212.
131 Boscoe MJ, de Lange S. Damage to the tricuspid valve with a Swan-Ganz catheter. Br MedJ 1981; 283: 346–347.
132 O’Toole JD, Wurtzbacher JJ, Wearner NE et al. Pulmonary-valve injury and insufficiencyduring pulmonary-artery catheterization. N Engl J Med 1979; 301: 1167–1168.
133 Bottiger BW, Schmidt H, Bohrer H. Nonsurgical removal of a knotted pulmonary arterycatheter. J Cardiothorac Vasc Anesth 1991; 5: 647 [Letter].
134 Feng WC, Singh AK, Drew T. Swan-Ganz catheter-induced massive hemoptysis and pulmonary artery false aneurysm. Ann Thorac Surg 1990; 50: 644–646.
135 Cervenko FW, Shelley SE, Spence DG et al. Massive endobronchial hemorrhage duringcardiopulmonary bypass: treatable complication of balloon-tipped catheter damage tothe pulmonary artery. Ann Thorac Surg 1983; 35: 326–328.
136 Kron IL, Piepgrass W, Carabello B et al. False aneurysm of the pulmonary artery: a com-plication of pulmonary artery catheterization. Ann Thorac Surg 1982; 33: 629–630.
137 Urschel JD, Myerowitz PD. Catheter-induced pulmonary artery rupture in the setting ofcardiopulmonary bypass. Ann Thorac Surg 1993; 56: 585–589.
138 Stone JG, Faltas AN, Khambatta HJ et al. Temporary unilateral pulmonary artery occlu-sion: a method for controlling Swan-Ganz catheter-induced hemoptysis. Ann Thorac Surg1984; 37: 508–510.
139 McDaniel DD, Stone JG, Faltas AN et al. Catheter-induced pulmonary artery hemor-rhage: diagnosis and management in cardiac operations. J Thorac Cardiovasc Surg 1981;82: 1–4.
140 Pellegrini RV, Marcelli G, Di Marco RF et al. Swan-Ganz catheter induced pulmonaryhemorrhage. J Cardiovasc Surg 1987; 28: 646–649.
141 Lemen R, Jones JG, Cowan G. A mechanism of pulmonary-artery perforation by Swan-Ganz catheters. N Engl J Med 1975; 292: 211–212.
142 Johnston WE, Royster R, Vinten-Johansen J et al. Influence of balloon inflation anddeflation on location of pulmonary artery catheter tip. Anesthesiology 1987; 67: 110–115.
143 Daniel WG, Erbel R, Kasper W et al. Safety of transesophageal echocardiography: a multi-center survey of 10,419 examinations. Circulation 1991; 83: 817–821.
144 Seward JB, Khandheria BK, Oh JK. Critical appraisal of transesophageal echocardio-graphy: limitations, pitfalls, and complications. J Am Soc Echocardiogr 1992; 5: 288–305.
145 Kallmeyer IJ, Collard CD, Fox JA et al. The safety of intraoperative transesophagealechocardiography: a case series of 7200 cardiac surgical patients. Anesth Analg 2001; 92:1126–1130.
146 Hogue CW, Lappas GD, Creswell LL et al. Swallowing dysfunction after cardiac operations: associated adverse outcomes and risk factors including intraoperative transesophageal echocardiography. J Thorac Cardiovasc Surg 1995; 110: 517–522.
147 Savino JS, Hanson CW III, Bigelow DC. Oropharyngeal injury after transesophagealechocardiography. J Cardiothorac Vasc Anesth 1994; 8: 76–78.
148 Spahn DR, Schmid S, Carrel T et al. Hypopharynx perforation by a transesophagealechocardiography probe. Anesthesiology 1995; 82: 581–583.
149 Brinkman WT, Schanewise JS, Clements SD et al. Transesophageal echocardiography:not an innocuous procedure. Ann Thorac Surg 2001; 72: 1725–1726.
Complications of cardiopulmonary bypass and cardioplegia 333
150 Dewhirst WE, Stragand JJ, Fleming BM. Mallory-Weiss tear complicating intraoperativetransesophageal echocardiography in a patient undergoing aortic valve replacement.Anesthesiology 1990; 73: 777–778.
151 Despotis GJ, Gravlee G, Filos K et al. Anticoagulation monitoring during cardiac surgery:a review of current and emerging techniques. Anesthesiology 1999; 91: 1122–1151.
152 Conrad J, LeCompte T, Horellou M et al. Antithrombin III in patients treated with sub-cutaneous or intravenous heparin. Thromb Res 1981; 22: 507–511.
153 Miciniak E, Gockerman J. Heparin induced decrease in circulating AT III. Lancet 1980; 2:581–584.
154 Jordan RE, Oosta GM, Gardner WT et al. The kinetics of the hemostatic enzyme–antithrombin interactions in the presence of low molecular weight heparin. J Biol Chem1980; 255: 10081–10090.
155 Sabbagh AH, Chung GKT, Shuttleworth P et al. Fresh frozen plasma: a solution to hep-arin resistance during cardiopulmonary bypass. Ann Thorac Surg 1984; 37: 466–468.
156 Anderson EF. Heparin resistance prior to cardiopulmonary bypass. Anesthesiology 1986;64: 504–507.
157 Blakeman B. Management of heparin-induced thrombocytopenia: a cardiovascular surgeon’s perspective. Semin Hematol 1999; 36 (Suppl. 1): 37–41.
158 Cohen M. Heparin-induced thrombocytopenia and the clinical use of low molecularweight heparins in acute coronary syndromes. Semin Hematol 1999; 36 (Suppl. 1): 33–36.
159 Walenga JM, Jeske WP, Wood JJ et al. Laboratory tests for heparin-induced thrombocy-topenia: a multicenter study. Semin Hematol 1999; 36 (Suppl. 1): 22–28.
160 Kelton JG. The clinical management of heparin-induced thrombocytopenia. SeminHematol 1999; 36 (Suppl. 1): 17–21.
161 Body SC, Morse DS. Coagulation, transfusion, and cardiac surgery. In: Spiess BD, CountsRB, Gould SA, eds. Perioperative Transfusion Medicine. Baltimore: Williams & Wilkins,1998; 419–460.
162 Vender J, Matthew E, Silverman I et al. Heparin-associated thrombocytopenia: altern-ative managements. Anesth Analg 1986; 65: 520–522.
163 Fareed J, Callas D, Hoppensteadt DA et al. Antithrombin agents as anticoagulants andantithrombotics: implications in drug development. Semin Hematol 1999; 36 (Suppl. 1):42–56.
164 Sodian R, Loebe M, Gorman KF et al. Heparin induced thrombocytopenia: experiences in 12 heart surgery patients. ASAIO J 1997; 43: M430–M433.
165 Smith RE, Townsend GE, Berry BR. Enoxaparin for unstable angina and ancrod for cardiac surgery following heparin allergy. Ann Pharmacother 1996; 30: 476–480.
166 Arén C. Heparin and protamine therapy. Semin Thorac Cardiovasc Surg 1990; 2: 364–372.167 Bull BS, Korpman RA, Huse WM et al. Heparin therapy during extracorporeal circula-
tion. I. Problems inherent in existing heparin protocols. J Thorac Cardiovasc Surg 1975; 69:674–684.
168 Bull BS, Huse WM, Brauer FS et al. Heparin therapy during extracorporeal circulation. II. The use of a dose–response curve to individualize heparin and protamine dosage. JThorac Cardiovasc Surg 1975; 69: 685–689.
169 Akl B, Vargas G, Neal J, Robillard J, Kellp P. Clinical experience with the activated clot-ting time for the control of heparin and protamine therapy during cardiopulmonarybypass. Thorac Cardiovasc Surg 1980; 79: 98–102.
170 Culliford A, Gitel SN, Starr N et al. Lack of correlation between activated clotting timeand plasma heparin during cardiopulmonary bypass. Ann Surg 1981; 193: 105–111.
334 Chapter 16
171 O’Neill AI, McAllister C, Corke CF et al. A comparison of five devices for the bedsidemonitoring of heparin therapy. Anesth Intens Care 1991; 19: 592–601.
172 Esposito RA, Culliford AT, Colvin SB et al. The role of the activated clotting time in hep-arin administration and neutralization for cardiopulmonary bypass. J Thorac CardiovascSurg 1983; 85: 174–185.
173 Hurt R, Perkins HA, Osborn JJ et al. The neutralization of heparin by protamine in extra-corporeal circulation. J Thorac Surg 1956; 32: 612–619.
174 Bull MH, Huse WM, Bull BS. Evaluation of tests used to monitor heparin therapy duringextracorporeal circulation. Anesthesiology 1975; 43: 346–353.
175 Anido G, Freeman DJ. Heparin assay and protamine titration. Am J Clin Pathol 1981; 76:410–415.
176 Jaques L. A study of the toxicity of the protamine, salmine. Br J Pharmacol 1949; 4: 135.177 Lowenstein E, Johnston WE, Lappas DG et al. Catastrophic pulmonary vasoconstriction
associated with protamine reversal of heparin. Anesthesiology 1983; 59: 470–473.178 Horrow JC. Protamine allergy. J Cardiothorac Anesth 1988; 2: 225–242.179 Frater RWM, Oka Y, Hong Y et al. Protamine-induced circulatory changes. J Thorac
Cardiovasc Surg 1984; 87: 687–692.180 Levy JH, Schwieger IM, Zaidan JR et al. Evaluation of patients at risk for protamine
reactions. J Thorac Cardiovasc Surg 1989; 98: 200–204.181 Morel DR, Mo Costabella PM, Pittet J-F. Adverse cardiopulmonary effects and in-
creased plasma thromboxane concentrations following the neutralization of heparin withprotamine in awake sheep are infusion rate-dependent. Anesthesiology 1990; 73: 415–424.
182 Horrow J. Management of coagulation and bleeding disorders. In: Kaplan JA, ed. CardiacAnesthesia. Philadelphia: W.B. Saunders, 1983; 951–994.
183 Keller R. Interrelations between different types of cells. II. Histamine-release from themast cells of various species by cationic polypeptides of polymorphonuclear leukocytelysosomes and other cationic compounds. Int Arch Allergy Appl Immunol 1968; 34:139–144.
184 Stoelting RK, Henry DP, Verburg KM et al. Haemodynamic changes and circulating histamine concentrations following protamine administration to patients and dogs. CanAnesth Soc J 1984; 31: 534–540.
185 Parsons RS, Mohandas K. The effect of histamine-receptor blockade on the hemody-namic responses to protamine. J Cardiothorac Anesth 1989; 3: 37–43.
186 Sethna D, Gray R, Bussell J et al. Further studies on the myocardial metabolic effect ofprotamine sulfate following cardiopulmonary bypass. Anesth Analg 1982; 61: 476–477.
187 Michaels IAL, Barash PG. Hemodynamic changes during protamine administration.Anesth Analg 1983; 62: 831–835.
188 Iwatsuki N, Matsukawa S, Iwatsuki K. A weak negative inotropic effect of protaminesulfate upon the isolated canine heart muscle. Anesth Analg 1980; 59: 100–102.
189 Hird RB, Wakefield TW, Mukherjee R et al. Direct effects of protamine sulfate on myocytecontractile processes: cellular and molecular mechanisms. Circulation 1995; 92 (Suppl. II):II-443–II-446.
190 Doolan L, McKenzie I, Krafchek J et al. Protamine sulfate hypersensitivity. Anesth IntensCare 1981; 9: 147–149.
191 Levy JH, Zaidan JR, Faraj B. Prospective evaluation of risk protamine reactions inpatients with NPH insulin-dependent diabetes. Anesth Analg 1986; 65: 739–742.
192 Samuel T, Kolk AHJ, Rümke P et al. Autoimmunity to sperm antigens in vasectomizedmen. Clin Exp Immunol 1975; 21: 65–74.
Complications of cardiopulmonary bypass and cardioplegia 335
193 Kirklin JK, Chenoweth DE, Naftel DC et al. Effects of protamine administration after cardiopulmonary bypass on complement, blood elements, and the hemodynamic state.Ann Thorac Surg 1986; 41: 193–199.
194 Lakin JD, Blocker TJ, Strong DM et al. Anaphylaxis to protamine sulfate mediated by acomplement-dependent IgG antibody. J Allergy Clin Immunol 1978; 61: 102–107.
195 Lowenstein E, Zapol WM. Protamine reactions, explosive mediator release, and pul-monary vasoconstriction. Anesthesiology 1990; 73: 373–374 [Editorial].
196 Hobbhahn J, Conzen PF, Zenker B et al. Beneficial effect of cyclooxygenase inhibition onadverse hemodynamic responses after protamine. Anesth Analg 1988; 67: 253–260.
197 Morel DR, Lowenstein E, Nguyenduy T et al. Acute pulmonary vasoconstriction andthromboxane release during protamine reversal of heparin anticoagulation in awakesheep: evidence for the role of reactive oxygen metabolites following nonimmunologicalcomplement activation. Circ Res 1988; 62: 905–915.
198 Nuttall GA, Murray MJ, Bowie EJW. Protamine-heparin-induced pulmonary hyperten-sion in pigs: effects of treatment with a thromboxane receptor antagonist on hemody-namics and coagulation. Anesthesiology 1991; 74: 138–145.
199 Schumacher W, Heran C, Ogletree M. Effect of thromboxane receptor antagonism onpulmonary hypertension caused by protamine–heparin interaction in pigs. Circulation1988; 78: 207.
200 Colman RW. Humoral mediators of catastrophic reactions associated with protamineneutralization. Anesthesiology 1987; 66: 595–596 [Editorial].
201 Godal H. A comparison of two heparin-neutralizing agents: protamine and polybrene.Scand J Clin Lab Invest 1960; 12: 446–457.
202 Weiss W, Gilman J, Catenacci A, Osterberg A. Heparin neutralization with polybreneadministered intravenously. JAMA 1958; 166: 630–637.
203 Toyofuku T, Koyama S, Kobayashi T et al. Effects of polycations on pulmonary vascularpermeability in conscious sheep. J Clin Invest 1989; 83: 2063–2069.
204 Egerton W, Robinson C. The antiheparin, anticoagulant and hypotensive properties ofhexadimethrine and protamine. Lab Invest 1987; 56: 170–179.
205 Ransdell HT Jr, Haller JA Jr, Stowens D et al. Renal toxicity of polybrene (hexadimethrinebromide). J Surg Res 1965; 5: 195–199.
206 Yang VC, Port FK, Kim J-S et al. The use of immobilized protamine in removing heparinand preventing protamine-induced complications during extracorporeal blood circula-tion. Anesthesiology 1991; 75: 288–297.
207 Teng C-LC, Kim J-S, Port FK et al. A protamine filter for extracorporeal blood heparinremoval. ASAIO Trans 1988; 34: 743–746.
208 Kim J-S, Vincent C, Teng C-LC et al. A novel approach to anticoagulation control. ASAIOTrans 1989; 35: 644–646.
209 Despotis GJ, Summerfield AL, Joist JH et al. In vitro reversal of heparin effect with heparinase: evaluation with whole blood prothrombin time and activated partial throm-boplastin time in cardiac surgical patients. Anesth Analg 1994; 79: 670–674.
210 Langer R, Linhardt RJ, Hoffberg S et al. An enzymatic system for removing heparin inextracorporeal therapy. Science 1982; 217: 261–263.
211 Cook JJ, Niewiarowski S, Yan Z et al. Platelet factor 4 efficiently reverses heparin anti-coagulation in the rat without adverse effects of heparin–protamine complexes. Circulation1992; 85: 1102–1109.
212 Levy JH, Cormack JG, Morales A. Heparin neutralization by recombinant platelet factor4 and protamine. Anesth Analg 1995; 81: 35–37.
336 Chapter 16
213 Bernabei A, Gikakis N, Maione TE et al. Reversal of heparin anticoagulation by recombi-nant platelet factor 4 and protamine sulfate in baboons during cardiopulmonary bypass.J Thorac Cardiovasc Surg 1995; 109: 765–771.
214 Williams RD, D’Ambra MN, Maione TE et al. Recombinant platelet factor 4 reversal ofheparin in human cardiopulmonary bypass blood. J Thorac Cardiovasc Surg 1994; 108:975–983.
215 Dehmer GJ, Fisher M, Tate DA et al. Reversal of heparin anticoagulation by recombinantplatelet factor 4 in humans. Circulation 1995; 91: 2188–2194.
216 Despotis GJ, Filos KS, Zoys TN et al. Factors associated with excessive postoperativeblood loss and hemostatic transfusion requirements: a multivariate analysis in cardiacsurgical patients. Anesth Analg 1996; 82: 13–21.
217 Moulton MJ, Creswell LL, Mackey ME et al. Reexploration for bleeding is a risk factor foradverse outcomes after cardiac operations. J Thorac Cardiovasc Surg 1996; 111: 1037–1046.
218 Dacey LJ, Munoz JJ, Baribeau YR et al. Reexploration for hemorrhage following coronarybypass grafting: incidence and risk factors. Northern New England CardiovascularDisease Study Group. Arch Surg 1998; 133: 442–447.
219 Despotis GJ, Skubas NJ, Goodnough LT. Optimal management of bleeding and trans-fusion in patients undergoing cardiac surgery. Semin Thorac Cardiovasc Surg 1999; 11:84–104.
220 Slaughter TF, Greenberg CS. Antifibrinolytic drugs and perioperative hemostasis. Am JHematol 1997; 56: 32–36.
221 Peters DC, Noble S. Aprotinin: an update of its pharmacology and therapeutic use inopen heart surgery and coronary artery bypass surgery. Drugs 1999; 57: 233–260.
222 Sundt TM III, Kouchoukos MD, Saffitz JE et al. Renal dysfunction and intravascular coagulation with aprotinin and hypothermic circulatory arrest. Ann Thorac Surg 1993; 55:1418–1424.
223 Cosgrove DM III, Heric B, Lytle BW et al. Aprotinin therapy for reoperative myocardialrevascularization: a placebo-controlled study. Ann Thorac Surg 1992; 54: 1031–1036.
224 Schulze K, Graeter T, Schaps D et al. Severe anaphylactic shock due to repeated applica-tion of aprotinin in patients following intrathoracic aortic replacement. Eur J CardiothoracSurg 1993; 7: 495–496.
225 Etchason J, Petz L, Keeler E et al. The cost effectiveness of preoperative autologous blooddonations. N Engl J Med 1995; 332: 719–724.
226 Tartter PI, Quintero S, Barron DM. Perioperative blood transfusion associated with infec-tious complications after colorectal cancer operations. Am J Surg 1986; 152: 479–482.
227 Dawes LG, Aprahamian C, Condon RE et al. The risk of infection after colon injury.Surgery 1986; 100: 796–803.
228 Murphy P, Heal JM, Blumberg N. Infection or suspected infection after hip replacementsurgery with autologous or homologous blood transfusions. Transfusion 1991; 31: 212–217.
229 Love TR, Hendren WG, O’Keefe DD et al. Transfusion of predonated autologous blood inelective cardiac surgery. Ann Thorac Surg 1987; 43: 508–512.
230 Gluck D, Kubanek B, Ahnefeld F. Autologous transfusion. Objectives and benefits, limitsand risks shown in a practical clinical concept. Anesthesia 1988; 37: 565–571.
231 Anderson BV, Tomasulo PA. Current autologous transfusion practices. Implications forthe future. Transfusion 1988; 28: 394–396.
232 Forbes J, Anderson M, Anderson G, Bleecher G, Rossi E, Moss G. Blood transfusion costs:a multicenter study. Transfusion 1991; 31: 318–323.
233 Britton L, Eastlund T, Dziuban S et al. Predonated autologous blood use in elective car-diac surgery. Ann Thorac Surg 1989; 47: 529–532.
Complications of cardiopulmonary bypass and cardioplegia 337
234 Owings DV, Kruskall MS, Thurer RL et al. Autologous blood donations prior to electivecardiac surgery. JAMA 1989; 262: 1963–1968.
235 Konishi T, Ohbayashi T, Kaneko T et al. Preoperative use of erythropoietin for cardiovas-cular operations in anemia. Ann Thorac Surg 1993; 56: 101–103.
236 Schmoekel M, Nollert G, Mempel M et al. Effects of recombinant human erythropoietinon autologous blood donation before open heart surgery. Thorac Cardiovasc Surg 1993;41: 364–368.
237 Kyo S, Omoto R, Hirashima K, Eguchi S, Fujita T. Effect of human recombinant erythro-poietin on reduction of homologous blood transfusion in open-heart surgery. A Japanesemulticenter study. Circulation 1992; 86: 413–418.
238 Wong CA, Franklin ML, Wade LD. Coagulation tests, blood loss, and transfusionrequirements in platelet rich plasmapheresed versus nonpheresed cardiac surgerypatients. Anesth Analg 1994; 78: 29–36.
239 Jones JW, McCoy TA, Rawitscher RE et al. Effects of intraoperative plasmapheresis onblood loss in cardiac surgery. Ann Thorac Surg 1990; 49: 585–590.
240 Giordano GF, Rivers SL, Chung GKT et al. Autologous platelet-rich plasma in cardiacsurgery: effect on intraoperative and postoperative transfusion requirements. AnnThorac Surg 1988; 46: 416–419.
241 Del Rossi AJ, Cernaianu AC, Vertrees RA et al. Platelet-rich plasma reduces post-operative blood loss after cardiopulmonary bypass. J Thorac Cardiovasc Surg 1990; 100:281–286.
242 Petry AF, Jost J, Sievers H. Reduction of homologous blood requirements by blood-pooling at the onset of cardiopulmonary bypass. J Thorac Cardiovasc Surg 1994; 107:1210–1214.
243 Schönberger JPAM, Bredée JJ, Tjian D et al. Intraoperative predonation contributes toblood saving. Ann Thorac Surg 1993; 56: 893–898.
244 Lawson L, Ochsner J, Mills N, Leonard G. The use of hemodilution and fresh autologousblood in open heart surgery. Anesth Analg 1974; 53: 672–683.
245 Robblee JA. Pro: blood should be harvested immediately before cardiopulmonarybypass and infused after protamine reversal to decrease blood loss following cardiopul-monary bypass. J Cardiothorac Anesth 1990; 4: 519–521.
246 Schaff HV, Hauer J, Gardner TJ et al. Routine use of autotransfusion following cardiacsurgery: experience in 700 patients. Ann Thorac Surg 1979; 27: 493–499.
247 Breyer RH, Engelman RM, Rousou JA et al. Blood conservation for myocardial revascu-larization: is it cost effective? J Thorac Cardiovasc Surg 1987; 93: 512–522.
248 Eng J, Kay PH, Murday AJ et al. Postoperative autologous transfusion in cardiac surgery.A prospective, randomised study. Eur J Cardiothorac Surg 1990; 4: 595–600.
249 Adan A, de la Rivière AB, Haas F et al. Autotransfusion of drained mediastinal bloodafter cardiac surgery: a reappraisal. Thorac Cardiovasc Surg 1988; 36: 10–14.
250 Axford TC, Dearani JA, Ragno G et al. Safety and therapeutic effectiveness of reinfusedshed blood after open heart surgery. Ann Thorac Surg 1994; 57: 615–622.
251 Bouboulis N, Kardara M, Kesteven PJ et al. Autotransfusion after coronary artery bypasssurgery: is there any benefit? J Card Surg 1994; 9: 314–321.
252 de Haan J, Schönberger J, Haan J et al. Tissue-type plasminogen activator and fibrinmonomers synergistically cause platelet dysfunction during retransfusion of shed bloodafter cardiopulmonary bypass. J Thorac Cardiovasc Surg 1993; 106: 1017–1023.
253 Griffith LD, Billman GF, Daily PO et al. Apparent coagulopathy caused by infusion ofshed mediastinal blood and its prevention by washing of the infusate. Ann Thorac Surg1989; 47: 400–406.
338 Chapter 16
254 Bland LA, Villarino ME, Ardunino MJ et al. Bacteriologic and endotoxin analysis of salvaged blood used in autologous transfusions during cardiac operations. J ThoracCardiovasc Surg 1992; 103: 582–588.
255 Gravlee GP, Davis RE, Kurusz M, Utley JR, eds. Cardiopulmonary Bypass. Principles andPractice, 2nd edn. Philadelphia: Lippincott, Williams & Wilkins, 2000.
256 Edmunds LH Jr. Extracorporeal perfusion. In: Edmunds LH Jr, ed. Cardiac Surgery in theAdult. New York: McGraw-Hill, 1997; 255–294.
257 Blackstone EH, Kirklin JW, Stewart RW et al. The damaging effects of cardiopulmonarybypass. In: Wu KK, Roxy EC, eds. Prostaglandins in Clinical Medicine: Cardiovascular andThrombotic Disorders. Chicago: Year Book, 1982; 355.
258 Uniyal S, Brash JL. Patterns of adsorption of proteins from human plasma onto foreignsurfaces. Thromb Haemost 1993; 70: 253.
259 Ziats NP, Pankowsky DA, Tierney BP et al. Adsorption of Hageman factor (factor XII)and other human plasma proteins to biomedical polymers. J Lab Clin Med 1990; 116:687–696.
260 Horbett TA. Principles underlying the role of adsorbed plasma proteins in blood inter-actions with foreign materials. Cardiovasc Pathol 1993; 2: 137S–148S.
261 Horbett TA. Proteins: structure, properties, and adsorption to surfaces. In: Ratner BD,Hoffman AS, Schoen FJ et al., eds. Biomaterials Science. An Introduction to Materials inMedicine. San Diego: Academic Press, 1996; 133–141.
262 Volanakis JE, Frank MM, eds. The Human Complement System in Health and Disease. NewYork: Marcel Dekker, 1998.
263 Colman RW. Surface-mediated defense reactions: the plasma contact activation system. JClin Invest 1984; 73: 1249–1253.
264 Gikakis N, Khan MMH, Hiramatsu Y et al. Effect of factor Xa inhibitors on thrombin formation and complement and neutrophil activation during in vitro extracorporeal circulation. Circulation 1996; 94 (Suppl. II): II-341–II-346.
265 Drake TA, Ruf W, Morrissey JH et al. Functional tissue factor is entirely cell surfaceexpressed on lipopolysaccharide-stimulated human blood monocytes and a constitut-ively tissue factor-producing neoplastic cell line. J Cell Biol 1989; 109: 389–395.
266 Grabowski EF, Rodriguez M, Nemerson Y et al. Flow limits factor Xa production bymonolayers of fibroblasts and endothelial cells. Blood 1990; 76 (Suppl. I): 422 [Abstract].
267 Wachtfogel YT, Harpel PC, Edmunds LH Jr. et al. Formation of Cîs-C1–inhibitor,kallikrien-Cî-inhibitor and plasmin-α2-plasmin-inhibitor complexes during cardiopul-monary bypass. Blood 1989; 73: 468–471.
268 Wiedmer T, Esmon CT, Sims PJ. Complement proteins C5b-9 stimulate procoagulantactivity through platelet prothrombinase. Blood 1986; 68: 875–880.
269 Berger M. Complement-mediated phagocytosis. In: Volanakis JE, Frank MM, eds. TheHuman Complement System in Health and Disease. New York: Marcel Dekker, 1998; 9–32.
270 Chenowith DE, Hugli TE. Demonstration of specific C5a receptor on intact human polymorphonuclear leukocytes. Proc Natl Acad Sci USA 1978; 75: 3943.
271 Ellison N, Edmunds LH Jr, Colman RW. Platelet aggregation following heparin and protamine administration. Anesthesiology 1978; 48: 65–68.
272 Sobel M, McNeill PM, Carlson PL et al. Heparin inhibition of von Willebrand factor-dependent platelet function in vitro and in vivo. J Clin Invest 1991; 87: 1787–1793.
273 Coughlin SR, Vu T-KH, Hung DT et al. Characterization of a functional thrombin receptor: issues and opportunities. J Clin Invest 1992; 89: 351–355.
274 Niewiarowski S, Senyi AF, Gillies P. Plasmin-induced platelet aggregation and plateletrelease reaction. J Clin Invest 1973; 52: 1647–1659.
Complications of cardiopulmonary bypass and cardioplegia 339
275 Lu H, Soria C, Cramer EM et al. Temperature dependence of plasmin-induced activationor inhibition of human platelets. Blood 1991; 77: 894.
276 Rinder CS, Bonner J, Rinder HM et al. Platelet activation and aggregation during car-diopulmonary bypass. Anesthesiology 1991; 74: 388–393.
277 Abrams CS, Ellison N, Budzynski AZ et al. Direct detection of activated platelets andplatelet-derived microparticles in humans. Blood 1990; 75: 128–138.
278 Lefkovits J, Plow EF, Topol EJ. Platelet glycoprotein IIb/IIIa receptors in cardiovascularmedicine. N Engl J Med 1995; 332: 1553–1559.
279 Rinder HM, Bonan JL, Rinder CS et al. Activated and unactivated platelet adhesion tomonocytes and neutrophils. Blood 1991; 78: 1760–1769.
280 Addonizio VP Jr, Smith JB, Strauss JF III et al. Thromboxane synthesis and platelet secre-tion during cardiopulmonary bypass with bubble oxygenator. J Thorac Cardiovasc Surg1980; 79: 91–96.
281 Hennessy VL Jr, Hicks RE, Niewiarowski S et al. Function of human platelets duringextracorporeal circulation. Am J Physiol 1977; 232: H622–H628.
282 Addonizio VP Jr, Strauss JF III, Chang L-F et al. Release of lysosomal hydrolases duringextracorporeal circulation. J Thorac Cardiovasc Surg 1982; 84: 28–34.
283 Edmunds LH Jr, Ellison N, Colman RW et al. Platelet function during cardiac operation:comparison of membrane and bubble oxygenators. J Thorac Cardiovasc Surg 1982; 83:805–812.
284 Zilla P, Fasol R, Groscurth P et al. Blood platelets in cardiopulmonary bypass operations:recovery occurs after initial stimulation, rather than continual activation. J ThoracCardiovasc Surg 1989; 97: 379–388.
285 Wenger RK, Lukasiewicz H, Mikuta BS et al. Loss of platelet fibrinogen receptors duringclinical cardiopulmonary bypass. J Thorac Cardiovasc Surg 1989; 97: 235–239.
286 Saadi S, Plait JL. Endothelial cell responses to complement activation. In: Volanakis JE,Frank MM, eds. The Human Complement System in Health and Disease. New York: MarcelDekker, 1998; 335–353.
287 Francis CW, Marder VJ. Physiologic regulation and pathologic disorders of fibrinolysis.In: Colman RW, Hirsch J, Marder VJ et al. Hemostasis and Thrombosis: Basic Principles andClinical Practice, 3rd edn. Philadelphia: JB Lippincott, 1994; 1076–1103.
288 Asimakopoulos G, Taylor KM. Effects of cardiopulmonary bypass on leukocyte andendothelial adhesion molecules. Ann Thorac Surg 1998; 66: 2135–2144.
289 Ember JA, Jagels MA, Hugli TE. Characterization of complement anaphylatoxins andtheir biological responses. In: Volanakis JE, Frank MM, eds. The Human ComplementSystem in Health and Disease. New York: Marcel Dekker, 1998; 241–244.
290 Insel PA. Analgesic-antipyretic and anti-inflammatory agents and drugs employed in the treatment of gout. In: Hardman IG, Limbird LE, eds. Goodman and Gillman’sPharmacological Basis of Therapeutics. New York: McGraw-Hill, 1996; 618–619.
291 Wachtfogel YT, Kucich U, Greenplate J et al. Human neutrophil degranulation duringextracorporeal circulation. Blood 1987; 69: 324–330.
292 Enofsson M, Thelin S, Siegbahn A. Monocyte tissue factor expression, cell activation, andthrombin formation during cardiopulmonary bypass: a clinical study. J Thorac CardiovascSurg 1997; 113: 576–584.
293 Ernofsson M, Siegbahn A. Platelet-derived growth factor-BB and monocyte chemotacticprotein-1 induce human peripheral blood monocytes to express tissue factor. Thromb Res1996; 83: 307–320.
294 Chung JH, Gikakis N, Rao AK et al. Pericardial blood activates the extrinsic coagulationpathway during clinical cardiopulmonary bypass. Circulation 1996; 93: 2014–2018.
340 Chapter 16
295 Frering B, Philip I, Dehoux M et al. Circulating cytokines in patients undergoing nor-mothermic cardiopulmonary bypass. J Thorac Cardiovasc Surg 1994; 108: 636–641.
296 Kawahito K, Kawakami M, Fujiwara T et al. Interleukin-8 and monocyte chemotacticactivating factor responses to cardiopulmonary bypass. J Thorac Cardiovasc Surg 1995;110: 99–102.
297 Fingerle-Rowson G, Auers J, Kreuzer E et al. Down-regulation of surface monocytelipopolysaccharide-receptor CD14 in patients on cardiopulmonary bypass undergoingaorta-coronary bypass operation. J Thorac Cardiovasc Surg 1998; 115: 1172–1178.
298 Haeffner-Cavaillon N, Roussellier N, Ponzio O et al. Induction of interleukin-1 produc-tion in patients undergoing cardiopulmonary bypass. J Thorac Cardiovasc Surg 1989; 98:1100–1106.
299 Roth JA, Golub SH, Cukingnan RA et al. Cell-mediated immunity is depressed followingcardiopulmonary bypass. Ann Thorac Surg 1981; 31: 350–356.
300 Ide H, Kakiuchi T, Furuta N et al. The effect of cardiopulmonary bypass on T cells andtheir subpopulations. Ann Thorac Surg 1987; 44: 277–282.
301 Nguyen DM, Mulder DS, Shennib H. Effect of cardiopulmonary bypass on circulatinglymphocyte function. Ann Thorac Surg 1992; 53: 611–616.
302 Kirklin JW, Barratt-Boyes BG. Hypothermia, circulatory arrest, and cardiopulmonarybypass. In: Cardiac Surgery, 2nd edn. New York: Churchill Livingstone, 1993; 61–127.
303 Swain JA, McDonald TJ Jr, Griffith PK et al. Low-flow hypothermic cardiopulmonarybypass protects the brain. J Thorac Cardiovasc Surg 1991; 102: 76–84.
304 Michenfelder JD. The hypothermic brain. In: Michenfelder JD, ed. Anesthesia and theBrain. New York: Churchill Livingstone, 1998; 23–34.
305 Rothman SM, Olney JW. Glutamate and the pathophysiology of hypoxic-ischemic braindamage. Ann Neurol 1986; 19: 105–111.
306 Busto R, Globus MY-T, Dietrich WD et al. Effect of mild hypothermia on ischemia-inducedrelease of neurotransmitters and free fatty acids in rat brain. Stroke 1989; 20: 904–910.
307 Hickey RF, Hoar PF. Whole-body oxygen consumption during low-flow hypothermiccardiopulmonary bypass. J Thorac Cardiovasc Surg 1983; 86: 903–906.
308 Nussmeier NA, Arlund C, Slogoff S. Neuropsychiatric complications after cardiopul-monary bypass: cerebral protection by a barbiturate. Anesthesiology 1986; 64: 165–170.
309 Davies LK. Hypothermia: physiology and clinical use. In: Gravlee GP, Davis RF, KuruszM, Utley JR, eds. Cardiopulmonary Bypass: Principles and Practice, 2nd edn. Philadelphia:Lippincott, Williams & Wilkins, 2000; 197–213.
310 Furnary AP, Zerr KJ, Grunkemeier GL et al. Continuous intravenous insulin infusionreduces the incidence of deep sternal wound infection in diabetic patients after cardiacsurgical procedures. Ann Thorac Surg 1999; 67: 352–360.
311 Knight A, Forsling M, Treasure T et al. Changes in plasma vasopressin concentration inassociation with coronary artery surgery or thymectomy. Br J Anesth 1986; 58: 1273–1277.
312 Wu W-h, Zbuzek VK, Bellevue C. Vasopressin release during cardiac operation. J ThoracCardiovasc Surg 1980; 79: 83–90.
313 Kaul TK, Swaminathan R, Chatrath RR et al. Vasoactive pressure hormones during andafter cardiopulmonary bypass. Int J Artif Organs 1990; 13: 293–299.
314 Baylis PH. Vasopressin, diabetes insipidus, and syndrome of inappropriate antidiuresis.In: DeGroot LJ, Jameson JL, eds. Endocrinology, 4th edn, Vol. 1. Philadelphia: W.B.Saunders, 2001; 363–376.
315 Heyndrickx GR, Boettcher DH, Vatner SF. Effects of angiotensin, vasopressin, andmethoxamine on cardiac function and blood flow distribution in conscious dogs. Am JPhysiol 1976; 231: 1579–1587.
Complications of cardiopulmonary bypass and cardioplegia 341
316 Philbin DM, Levine FH, Emerson CW et al. Plasma vasopressin levels and urinary flowduring cardiopulmonary bypass in patients with valvular heart disease: effect of pul-satile flow. J Thorac Cardiovasc Surg 1979; 78: 779–783.
317 Kuitunen A, Hynynen M, Salmenperä M et al. Anesthesia affects plasma concentrationsof vasopressin, von Willebrand factor and coagulation factor VIII in cardiac surgicalpatients. Br J Anesth 1993; 70: 173–180.
318 Kehlet H. Surgical stress. The role of pain and analgesia. Br J Anesth 1989; 63: 189–195.319 Anand KJS, Hickey PR. Halothane-morphine compared with high-dose sufentanil for
anesthesia and postoperative analgesia in neonatal cardiac surgery. N Engl J Med 1992;326: 1–9.
320 Landymore RW, Murphy DA, Kinley CE et al. Does pulsatile flow influence the incid-ence of postoperative hypertension? Ann Thorac Surg 1979; 28: 261–268.
321 Hirvonen J, Huttunen P, Nuutinen L et al. Catecholamines and free fatty acids in plasmaof patients undergoing cardiac operations with hypothermia and bypass. J Clin Pathol1978; 31: 949–955.
322 Reed HL, Chernow B, Lake CR et al. Alterations in sympathetic nervous system activitywith intraoperative hypothermia during coronary artery bypass surgery. Chest 1989; 95:616–622.
323 Balasaraswathi K, Glisson SN, El-Etr AA et al. Effect of priming volume on serum cate-cholamines during cardiopulmonary bypass. Can Anesth Soc J 1980; 27: 135–139.
324 Reves JG, Karp RB, Buttner EE et al. Neuronal and adrenomedullary catecholaminerelease in response to cardiopulmonary bypass in man. Circulation 1982; 66: 49–55.
325 Samuelson PN, Reves JG, Kirklin JK et al. Comparison of sufentanil and enflurane-nitrous oxide anesthesia for myocardial revascularization. Anesth Analg 1986; 65: 217–226.
326 Ng A, Tan SSW, Lee HS et al. Effect of propofol infusion on the endocrine response to cardiac surgery. Anesth Intens Care 1995; 23: 543–547.
327 Stenseth R, Bjella L, Berg EM et al. Thoracic epidural anesthesia in aortocoronary bypasssurgery II. Effects on the endocrine metabolic response. Acta Anesthesiol Scand 1994;38: 834–839.
328 Moore CM, Cross MH, Desborough JP et al. Hormonal effects of thoracic extradural analgesia for cardiac surgery. Br J Anesth 1995; 75: 387–393.
329 Minami K, Körner MM, Vyska K et al. Effects of pulsatile perfusion on plasma cate-cholamine levels and hemodynamics during and after cardiac operations with car-diopulmonary bypass. J Thorac Cardiovasc Surg 1990; 99: 82–91.
330 Hume DM, Bell CC, Bartter F. Direct measurement of adrenal secretion during operativetrauma and convalescence. Surgery 1962; 52: 174–186.
331 Flezzani P, Croughwell ND, McIntyre RW et al. Isoflurane decreases the cortisol responseto cardiopulmonary bypass. Anesth Analg 1986; 65: 1117–1122.
332 Lacoumenta S, Yeo TH, Paterson JL et al. Hormonal and metabolic responses to cardiacsurgery with sufentanil-oxygen anesthesia. Acta Anesthesiol Scand 1987; 31: 258–263.
333 Uozumi T, Manabe H, Kawashima Y et al. Plasma cortisol, corticosterone, and nonprotein-bound cortisol in extra-corporeal circulation. Acta Endocrinol 1972; 69: 517–525.
334 Taggart DP, Fraser WD, Borland WW et al. Hypothermia and the stress response to cardiopulmonary bypass. Eur J Cardiothorac Surg 1989; 3: 359–364.
335 Taylor KM, Walker MS, Rao LGS et al. Plasma levels of cortisol, free cortisol and corticotrophin during cardio-pulmonary by-pass. J Endocrinol 1975; 67: 29P–30P.
336 Terán N, Rodríguez-Iturbe B, Parra G et al. Atrial natriuretic peptide levels in brainvenous outflow during cardiopulmonary bypass in humans: evidence for extracardiachormonal production. J Cardiothorac Vasc Anesth 1991; 5: 343–347.
342 Chapter 16
337 Kharasch ED, Yeo K-T, Kenny MA et al. Influence of hypothermic cardiopulmonarybypass on atrial natriuretic factor levels. Can J Anesth 1989; 36: 545–553.
338 Curello S, Ceconi C, De Giuli F et al. Time course of human atrial natriuretic factor releaseduring cardiopulmonary bypass in mitral valve and coronary artery diseased patients.Eur J Cardiothorac Surg 1991; 5: 205–210.
339 Northridge DB, Jamieson MP, Jardine AG et al. Pulmonary extraction and left atrialsecretion of atrial natriuretic factor during cardiopulmonary bypass surgery. Am Heart J1992; 123: 698–703.
340 Pasaoglu I, Erbas B, Varoglu E et al. Changes in the circulating endothelin and atrial natriuretic peptide levels during coronary artery bypass surgery. Jpn Heart J 1993; 34:693–706.
341 Amano J, Suzuki A, Sunamori M et al. Attenuation of atrial natriuretic peptide response to sodium loading after cardiac operation. J Thorac Cardiovasc Surg 1995; 110:75–80.
342 Hynynen M, Palojoki R, Heinonen J et al. Renal and vascular effects of atrial natriureticfactor during cardiopulmonary bypass. Chest 1991; 100: 1203–1209.
343 Feddersen K, Aurell M, Delin K et al. Effects of cardiopulmonary bypass and prostacyclinon plasma catecholamines, angiotensin II and arginine-vasopressin. Acta AnesthesiolScand 1985; 29: 224–230.
344 Hedner J, Towle A, Saltzman L et al. Changes in plasma atrial natriuretic peptide-immunoreactivity in patients undergoing coronary artery bypass graft placements.Regulatory Peptides 1987; 17: 151–157.
345 Diedericks BJS, Roelofse JA, Shipton EA et al. The renin–angiotensin–aldosterone systemduring and after cardiopulmonary bypass. S Afr Med J 1983; 64: 946–949.
346 Canivet JL, Larbuisson R, Damas P et al. Plasma renin activity and during α2-microglobu-lin during and after cardiopulmonary bypass: pulsatile vs nonpulsatile perfusion. EurHeart J 1990; 11: 1079–1082.
347 Smallridge RC, Chernow B, Snyder R et al. Angiotensin-converting enzyme activity: apotential marker of tissue hypothyroidism in critical illness. Arch Intern Med 1985; 145:1829–1832.
348 Weinstein GS, Zabetakis PM, Clavel A et al. The renin–angiotensin system is not re-sponsible for hypertension following coronary artery bypass grafting. Ann Thorac Surg1987; 43: 74–77.
349 Taylor KM, Morton IJ, Brown JJ et al. Hypertension and the renin–angiotensin system fol-lowing open-heart surgery. J Thorac Cardiovasc Surg 1977; 74: 840–845.
350 Thrush DN, Austin D, Burdash N. Cardiopulmonary bypass temperature does not affectpostoperative euthyroid sick syndrome? Chest 1995; 108: 1541–1545.
351 Bremner WF, Taylor KM, Baird S et al. Hypothalamo–pituitary–thyroid axis functionduring cardiopulmonary bypass. J Thorac Cardiovasc Surg 1978; 75: 392–399.
352 Schwartz HL, Schadlow AR, Faierman D et al. Heparin administration appears todecrease cellular binding of thyroxine. J Clin Endocrinol Metab 1973; 36: 598–600.
353 Holland FWII, Brown PS Jr, Weintraub BD et al. Cardiopulmonary bypass and thyroidfunction: a “euthyroid sick syndrome”. Ann Thorac Surg 1991; 52: 46–50.
354 Novitzky D, Human PA, Cooper DKC. Inotropic effect of triiodothyronine followingmyocardial ischemia and cardiopulmonary bypass: an experimental study in pigs. AnnThorac Surg 1988; 45: 50–55.
355 Novitzky D, Human PA, Cooper DKC. Effects of triiodothyronine (T3) on myocardialhigh energy phosphates and lactate after ischemia and cardiopulmonary bypass: anexperimental study in baboons. J Thorac Cardiovasc Surg 1988; 96: 600–607.
Complications of cardiopulmonary bypass and cardioplegia 343
356 Novitzky D, Cooper DKC, Barton CI et al. Triiodothyronine as an inotropic agent afteropen heart surgery. J Thorac Cardiovasc Surg 1989; 98: 972–978.
357 Klemperer JD, Klein I, Gomez M et al. Thyroid hormone treatment after coronary-arterybypass surgery. N Engl J Med 1995; 333: 1522–1527.
358 Das JB, Eraklis AJ, Adams JG Jr et al. Changes in serum ionic calcium during cardiopul-monary bypass with hemodilution. J Thorac Cardiovasc Surg 1971; 62: 449–453.
359 Yoshioka K, Tsuchioka H, Abe T et al. Changes in ionized and total calcium concentra-tions in serum and urine during open heart surgery. Biochem Med 1978; 20: 135–143.
360 Gray R, Braunstein G, Krutzik S et al. Calcium homeostasis during coronary bypasssurgery. Circulation 1980; 62 (Suppl. I): I-57–I61.
361 Robertie PG, Butterworth JFIV, Prielipp RC et al. Parathyroid hormone responses tomarked hypocalcemia in infants and young children undergoing repair of congenitalheart disease. J Am Coll Cardiol 1992; 20: 672–677.
362 Robertie PG, Butterworth JFIV, Royster RL et al. Normal parathyroid hormone responsesto hyocalcemia during cardiopulmonary bypass. Anesthesiology 1991; 75: 43–48.
363 Butterworth JFIV, Royster RL, Prielipp RC et al. Should calcium be administered prior toseparation from cardiopulmonary bypass? Anesthesiology 1991; 75: 1121–1122.
364 Aglio LS, Stanford GG, Maddi R et al. Hypomagnesemia is common following cardiacsurgery. J Cardiothorac Vasc Anesth 1991; 5: 201–208.
365 Harris MNE, Crowther A, Jupp RA et al. Magnesium and coronary revascularization. Br JAnesth 1988; 60: 779–783.
366 Abraham AS, Rosenmann D, Kramer M et al. Magnesium in the prevention of lethalarrhythmias in acute myocardial infarction. Arch Intern Med 1987; 147: 753–755.
367 Munday KA, Blane GF, Chin EF et al. Plasma electrolyte changes in hypothermia. Thorax1958; 13: 334–342.
368 Manning SH, Angaran DM, Arom KV et al. Intermittent intravenous potassium therapyin cardiopulmonary bypass patients. Clin Pharmacol 1982; 1: 234–238.
369 Cohn LH, Angell WW, Shumway NE. Body fluid shifts after cardiopulmonary bypass. I.Effects of congestive heart failure and hemodilution. J Thorac Cardiovasc Surg 1971; 62:423–430.
370 Oster JB, Sladen RN, Berkowitz DE. Cardiopulmonary bypass and the lung. In: GravleeGP, Davis RF, Kurusz M, Utley JR, eds. Cardiopulmonary Bypass: Principles and Practice,2nd edn. Philadelphia: Lippincott, Williams & Wilkins, 2000; 367–390.
371 Sladen R, Jenkins L. Intermittent mandatory ventilation and controlled mechanical ven-tilation without positive end-expiratory pressure following cardiopulmonary bypass.Can Anesth Soc J 1978; 25: 166–172.
372 Dobbinson T, Miller J. Respiratory and cardiovascular responses to PEEP in artificiallyventilated patients after cardiopulmonary bypass surgery. Anesth Intens Care 1981; 9:307–313.
373 Berry CB, Butler PJ, Myles PS. Lung management during cardiopulmonary bypass: iscontinuous positive airways pressure beneficial? Br J Anesth 1993; 71: 864–868.
374 Chenowith DE, Cooper SW, Hugli TE et al. Complement activation during cardiopul-monary bypass: evidence for generation of C3a and C5a anaphylotoxins. N Engl J Med1981; 304: 497–502.
375 Morioka K, Muraoka R, Chiba Y et al. Leukocyte and platelet depletion with a blood cellseparator: effects on lung injury after cardiac surgery with cardiopulmonary bypass. JThorac Cardiovasc Surg 1996; 111: 45–54.
376 Werner HA, Wensley DF, Lirenman DS et al. Peritoneal dialysis in children after car-diopulmonary bypass. J Thorac Cardiovasc Surg 1997; 113: 64–70.
344 Chapter 16
377 Fleming F, Bohn D, Edwards H et al. Renal replacement therapy after repair of congenitalheart disease in children. J Thorac Cardiovasc Surg 1995; 109: 322–331.
378 Mangos GJ, Brown MA, Chan WYL et al. Acute renal failure following cardiac surgery:incidence, outcomes and risk factors. Aust NZ J Med 1995; 25: 284–289.
379 McCullough PA, Wolyn R, Rocher LL et al. Acute renal failure after coronary interven-tion: incidence, risk factors and relationship to mortality. Am J Med 1997; 103: 368–375.
380 Mangano CM, Diamondstone LS, Ramsay JG et al. Renal dysfunction after myocardialrevascularization: risk factors, adverse outcomes, and hospital resource utilization. Themulticenter study of perioperative ischemia research group. Ann Intern Med 1998; 128:194–203.
381 Zanardo G, Michielon P, Paccagnella A et al. Acute renal failure in the patient under-going cardiac operation: prevalence, mortality rate, and main risk factors. J ThoracCardiovasc Surg 1994; 107: 1489–1495.
382 Butterworth JF, Legault C, Royster RL et al. Factors that predict the use of positiveinotropic drug support after cardiac valve surgery. Anesth Analg 1998; 86: 461–467.
383 Cohen Y, Raz I, Merin G et al. Comparison of factors associated with 30-day mortalityafter coronary artery bypass grafting in patients with versus without diabetes mellitus.Am J Cardiol 1998; 81: 7–11.
384 Lema G, Meneses G, Urzua J et al. Effects of extracorporeal circulation on renal functionin coronary surgical patients. Anesth Analg 1995; 81: 446–451.
385 Chertow GM, Lazarus JM, Christiansen CL et al. Preoperative renal risk stratification.Circulation 1997; 95: 878–884.
386 Picca S, Principato F, Mazzera E et al. Risks of acute renal failure after cardiopulmonarybypass surgery in children: a retrospective 10-year case–control study. Nephrol DialTransplant 1995; 10: 630–636.
387 Crystal GJ, Salem MR. Myocardial and systemic hemodynamics during isovolemichemodilution alone and combined with nitroprusside-induced controlled hypotension.Anesth Analg 1991; 72: 227–237.
388 Regragui IA, Izzat MB, Birdi I et al. Cardiopulmonary bypass perfusion temperaturedoes not influence perioperative renal function. Ann Thorac Surg 1995; 60: 160–164.
389 Taylor KM, Bain WH, Maxted KJ et al. Comparative studies of pulsatile and nonpulsatileflow during cardiopulmonary bypass. I. Pulsatile system employed and its hematologiceffects. J Thorac Cardiovasc Surg 1978; 75: 569–573.
390 Dapper F, Neppl H, Wozniak G et al. Effects of pulsatile and nonpulsatile perfusionmode during extracorporeal circulationaa comparative clinical study. Thorac CardiovascSurg 1992; 40: 345–351.
391 Gaer JAR, Shaw ADS, Wild R et al. Effect of cardiopulmonary bypass on gastrointestinalperfusion and function. Ann Thorac Surg 1994; 57: 371–375.
392 Taylor KM. Pulsatile cardiopulmonary bypass: a review. J Cardiovasc Surg 1981; 22:561–568.
393 Hickey PR, Buckley MJ, Philbin DM. Pulsatile and nonpulsatile cardiopulmonarybypass: review of a counterproductive controversy. Ann Thorac Surg 1983; 36: 720–737.
394 Myles PS, Buckland MR, Schenk NJ et al. Effect of “renal-dose” dopamine on renal func-tion following cardiac surgery. Anesth Intens Care 1993; 21: 56–61.
395 Perdue PW, Balser JR, Lipsett PA et al. “Renal dose” dopamine in surgical patients:dogma or science? Ann Surg 1998; 227: 470–473.
396 Tumlin JA, Wang A, Murray PT et al. Fenoldopam mesylate blocks reductions in renalplasma flow after radiocontrast dye infusion: a pilot trial in the prevention of contrastnephropathy. Am Heart J 2002; 143: 894–903.
Complications of cardiopulmonary bypass and cardioplegia 345
397 Kulka PJ, Tryba M, Zenz M. Preoperative α2-adrenergic receptor agonists prevent thedeterioration of renal function after cardiac surgery: results of a randomized, controlledtrial. Crit Care Med 1996; 24: 947–952.
398 Bertolissi M, Antonucci F, De Monte A et al. Effects on renal function of a continuousinfusion of nifedipine during cardiopulmonary bypass. J Cardiothorac Vasc Anesth 1996;10: 238–242.
399 Amano J, Suzuki A, Sunamori M et al. Effect of calcium antagonist diltiazem on renalfunction in open heart surgery. Chest 1995; 107: 1260–1265.
400 Allgren RL, Marbury TC, Rahman SN et al. Anaritide in acute tubular necrosis. N Engl JMed 1997; 336: 828–834.
401 Rahman SN, Kim GE, Mathew AS et al. Effects of atrial natriuretic peptide in clinicalacute renal failure. Kidney Int 1994; 45: 1731–1738.
402 Hogue CW Jr, Sundt TM III, Goldberg M et al. Neurological complications of cardiacsurgery: the need for new paradigms in prevention and treatment. Semin ThoracCardiovasc Surg 1999; 11: 105–115.
403 Puskas JD, Winston AD, Wright CE et al. Stroke after coronary artery operation: incid-ence, correlates, outcome and cost. Ann Thorac Surg 2000; 69: 1053–1056.
404 Salazar JD, Wityk RJ, Grega MA et al. Stroke after cardiac surgery: short- and long-termoutcomes. Ann Thorac Surg 2001; 72: 1195–1202.
405 Ahlgren E, Arén C. Cerebral complications after coronary artery bypass and heart valve surgery. Risk factors and onset of symptoms. J Cardiothorac Vasc Anesth 1998; 12:270–273.
406 Roach GW, Kanchuger M, Mangano CM et al. Adverse cerebral outcomes after coronarybypass surgery. N Engl J Med 1996; 335: 1857–1863.
407 Wolman RL, Nussmeier NA, Aggarwal A et al. Cerebral injury after cardiac surgery:identification of a group at extraordinary risk. The multicenter study of perioperativeischemia (McSPI) research group and the ischemia research and education foundation(IREF) investigators. Stroke 1999; 30: 514–522.
408 van Dijk D, Keizer AMA, Diephuis JC et al. Neurocognitive dysfunction after coronaryartery bypass surgery: a systematic review. J Thorac Cardiovasc Surg 2000; 120: 632–639.
409 Borger MA, Peniston CM, Weisel RD et al. Neuropsychologic impairment after coronarybypass surgery: effect of gaseous microemboli during perfusionist interventions. J ThoracCardiovasc Surg 2001; 121: 743–749.
410 Barbut D, Lo Y-W, Gold JP et al. Impact of embolization during coronary artery bypassgrafting on outcome and length of stay. Ann Thorac Surg 1997; 63: 998–1002.
411 McKhann GM, Goldsborough MA, Borowicz LM Jr et al. Cognitive outcome after coron-ary artery bypass: a one-year prospective study. Ann Thorac Surg 1997; 63: 510–515.
412 Vingerhoets G, Van Nooten G, Vermassen F et al. Short-term and long-term neuro-psychological consequences of cardiac surgery with extracorporeal circulation. Eur JCardiothorac Surg 1997; 11: 424–431.
413 Mora CT, Henson MB, Weintraub WS et al. The effect of temperature management dur-ing cardiopulmonary bypass on neurologic and neuropsychologic outcomes in patientsundergoing coronary revascularization. J Thorac Cardiovasc Surg 1996; 112: 514–522.
414 Pugsley W, Klinger L, Paschalis C et al. The impact of microemboli during cardiopul-monary bypass on neuropsychological functioning. Stroke 1994; 25: 1393–1399.
415 Barbut D, Yao F-SF, Lo Y-W et al. Determination of size of aortic emboli and embolic loadduring coronary artery bypass grafting. Ann Thorac Surg 1997; 63: 1262–1267.
416 Stump DA, Rogers AT, Hammon JW et al. Cerebral emboli and cognitive outcome aftercardiac surgery. J Cardiothorac Vasc Anesth 1996; 10: 113–119.
346 Chapter 16
417 Savageau JA, Stanton B-A, Jenkins CD et al. Neuropsychological dysfunction followingelective cardiac operation. I. Early assessment. J Thorac Cardiovasc Surg 1982; 84: 585–594.
418 Kolkka R, Hilberman M. Neurologic dysfunction following cardiac operation with low-flow, low-pressure cardiopulmonary bypass. J Thorac Cardiovasc Surg 1980; 79: 432–437.
419 Murkin JM. Attenuation of neurologic injury during cardiac surgery. Ann Thorac Surg2001; 72: S1838–S1844.
420 Martin TD, Craver JM, Gott JP et al. The Warm Heart Investigators. Randomized trial ofnormothermic versus hypothermic coronary bypass. Prospective, randomized trial ofretrograde warm blood cardioplegia: myocardial benefit and neurologic threat. AnnThorac Surg 1994; 57: 298–304.
421 Martin TD, Craver JM, Gott JP et al. Prospective, randomized trial of retrograde warmblood cardioplegia: myocardial benefit and neurologic threat. Ann Thorac Surg 1994; 57:298–304.
422 Plourde G, Leduc AS, Morin JE et al. Temperature during cardiopulmonary bypass forcoronary artery operations does not influence postoperative cognitive function: aprospective, randomized trial. J Thorac Cardiovasc Surg 1997; 114: 123–128.
423 Dietrich WD, Alonso O, Busto R. Moderate hyperglycemia worsens acute blood–brainbarrier injury after forebrain ischemia in rats. Stroke 1993; 24: 111–116.
424 Metz S, Keats AS. Benefits of a glucose-containing priming solution for cardiopulmonarybypass. Anesth Analg 1991; 72: 428–434.
425 Murkin JM, Martzke JS, Buchan AM et al. A randomized study of the influence of perfu-sion technique and pH management strategy in 316 patients undergoing coronary arterybypass surgery. II. Neurologic and cognitive outcomes. J Thorac Cardiovasc Surg 1995;110: 349–362.
426 Patel RL, Turtle MR, Chambers DJ et al. Alpha-stat acid-base regulation during car-diopulmonary bypass improves neuropsychologic outcome in patients undergoingcoronary artery bypass grafting. J Thorac Cardiovasc Surg 1996; 111: 1267–1279.
427 Stephan H, Weyland A, Kazmaier S et al. Acid-base management during hypothermiccardiopulmonary bypass does not affect cerebral metabolism but does affect blood flowand neurological outcome. Br J Anesth 1992; 69: 51–7.
428 Bashien G, Townes BD, Nessly ML et al. A randomized study of carbon dioxide manage-ment during hypothermic cardiopulmonary bypass. Anesthesiology 1990; 72: 7–15.
429 Clauss RH, Hass WK, Ransohoff J. Simplified method for monitoring adequacy of brainoxygenation during carotid artery surgery. N Engl J Med 1965; 273: 1127–1131.
430 Brown R, Wright G, Royston D. A comparison of two systems for assessing cerebralvenous oxyhaemoglobin saturation during cardiopulmonary bypass in humans. Anes-thesia 1993; 48: 697–700.
431 Spencer MP, Thomas GI, Moehring MA. Relation between middle cerebral artery blood flow velocity and stump pressure during carotid endarterectomy. Stroke 1992; 23:1439–1445.
432 Edmunds HL Jr, Griffiths LK, van der Laken J et al. Quantitative electroencephalographicmonitoring during myocardial revascularization predicts postoperative disorientationand improves outcome. J Thorac Cardiovasc Surg 1992; 103: 555–563.
433 Silverman NA. Myocardial oxygen consumption after reversible ischemia. J Cardiac Surg1994; 9 (Suppl.): 465–468.
434 Krukenkamp IB, Silverman NA, Sorlie D et al. Characterization of postischemic myocar-dial oxygen utilization. Circulation 1986; 74 (Suppl. III): III-125–III-129.
435 Etievent J-P, Chocron S, Toubin G et al. Use of cardiac troponin I as a marker of perioper-ative myocardial ischemia. Ann Thorac Surg 1995; 59: 1192–1194.
Complications of cardiopulmonary bypass and cardioplegia 347
436 Melrose DG, Dreyer B, Bentall HH et al. Elective cardiac arrest. Lancet 1955; 2: 21–22.437 Weisel RD, Lipton IH, Lyall RN et al. Cardiac metabolism and performance following
cold potassium cardioplegia. Circulation 1978; 58 (Suppl. I): I-217–I-226.438 Gay WA. Potassium-induced cardioplegia. Ann Thorac Surg 1975; 20: 95–100.439 Cohen G, Borger MA, Weisel RD et al. Intraoperative myocardial protection: current
trends and future perspectives. Ann Thorac Surg 1999; 68: 1995–2001.440 Feindel CM, Tait GA, Wilson GJ et al. Multidose blood versus crystalloid cardioplegia. J
Thorac Cardiovasc Surg 1984; 87: 585–595.441 Fremes SE, Christakis GT, Weisel RD et al. A clinical trial of blood and crystalloid car-
dioplegia. J Thorac Cardiovasc Surg 1984; 88: 726–741.442 Christakis GT, Fremes SE, Weisel RD et al. Reducing the risk of urgent revascularization
for unstable angina: a randomized clinical trial. J Vasc Surg 1986; 3: 764–772.443 Allen BS, Buckberg GD, Rosenkranz ER et al. Topical cardiac hypothermia in patients
with coronary disease: an unnecessary adjunct to cardioplegic protection and cause ofpulmonary morbidity. J Thorac Cardiovasc Surg 1992; 104: 626–631.
444 Efthimiou J, Butler J, Woodham C et al. Diaphragm paralysis following cardiac surgery:role of phrenic nerve cold injury. Ann Thorac Surg 1991; 52: 1005–1008.
445 Tripp HF, Bolton JWR. Phrenic nerve injury following cardiac surgery: a review. J CardSurg 1998; 13: 218–223.
446 Buckberg GD, Brazier JR, Nelson RL et al. Studies of the effects of hypothermia on regionalmyocardial flow and metabolism during cardiopulmonary bypass. I. The adequatelyperfused beating, fibrillating, and arrested heart. J Thorac Cardiovasc Surg 1977; 73: 87–94.
447 Menasché P, Kural S, Fauchet M et al. Retrograde coronary sinus perfusion: a safe altern-ative for ensuring cardioplegic delivery in aortic valve surgery. Ann Thorac Surg 1982;34: 647–658.
448 Gott VL, Gonzalez JL, Zuhdi MN et al. Retrograde perfusion of the coronary sinus fordirect vision aortic surgery. Surg Gynecol Obstet 1957; 104: 319–328.
449 Salerno TA, Houck JP, Barrozo CAM et al. Retrograde continuous warm blood cardio-plegia: a new concept in myocardial protection. Ann Thorac Surg 1991; 51: 245–247.
450 Partington MT, Acar C, Buckberg GD et al. Studies of retrograde cardioplegia. I.Capillary blood flow distribution to myocardium supplied by open and occluded arter-ies. J Thorac Cardiovasc Surg 1989; 97: 605–612.
451 Menasché P, Subayi J-B, Veyssié L et al. Efficacy of coronary sinus cardioplegia inpatients with complete coronary artery occlusions. Ann Thorac Surg 1991; 51: 418–423.
452 Crooke GA, Harris LJ, Grossi EA et al. Biventricular distribution of cold blood cardio-plegic solution administered by different retrograde techniques. J Thorac Cardiovasc Surg1991; 102: 631–638.
453 Stirling MC, McClanahan TB, Schott RJ et al. Distribution of cardioplegic solution infusedantegradely and retrogradely in normal canine hearts. J Thorac Cardiovasc Surg 1989; 98:1066–1076.
454 Panos AL, Ali IS, Birnbaum PL et al. Coronary sinus injuries during retrograde continu-ous, normothermic blood cardioplegia. Ann Thorac Surg 1992; 54: 1137–1138.
455 He G-W. Rare complication of retrograde cardioplegia: inner wall perforation of theright atrium. Ann Thorac Surg 1997; 63: 539–541.
456 Griepp RB, Stinson EB, Hollingsworth JF et al. Prosthetic replacement of the aortic arch. J Thorac Cardiovasc Surg 1975; 70: 1051–1063.
457 Svennson LG, Crawford ES, Hess KR et al. Deep hypothermia with circulatory arrest:determinants of stroke and early mortality in 656 patients. J Thorac Cardiovasc Surg 1993;106: 19–31.
348 Chapter 16
458 Kimura T, Muraoka R, Chiba Y et al. Effect of intermittent deep hypothermic circulatoryarrest on brain metabolism. J Thorac Cardiovasc Surg 1994; 108: 658–663.
459 Newburger JW, Jonas RA, Wernovsky G et al. A comparison of the perioperative neuro-logic effects of hypothermic circulatory arrest versus low-flow cardiopulmonary bypassin infant heart surgery. N Engl J Med 1993; 329: 1057–1064.
460 Mills NL, Ochsner JL. Massive air embolism during cardiopulmonary bypass. J ThoracCardiovasc Surg 1980; 80: 708–717.
461 Lytle BW, McCarthy PM, Meaney KM et al. Systemic hypothermia and circulatory arrestcombined with arterial perfusion of the superior vena cava: effective intraoperative cereb-ral protection. J Thorac Cardiovasc Surg 1995; 109: 738–743.
462 Safi HJ, Brien HW, Winter JN et al. Brain protection via cerebral retrograde perfusionduring aortic arch aneurysm repair. Ann Thorac Surg 1993; 56: 270–276.
463 Deeb GM, Jenkins E, Bolling SF et al. Retrograde cerebral perfusion during hypothermiccirculatory arrest reduces neurologic morbidity. J Thorac Cardiovasc Surg 1995; 109:259–268.
464 Yamashita C, Nakamura H, Nishikawa Y et al. Retrograde cerebral perfusion with circulatory arrest in aortic arch aneurysms. Ann Thorac Surg 1992; 54: 566–568.
465 Miyamoto K, Kawashima Y, Matsuda H et al. Optimal perfusion flow rate for the brainduring deep hypothermic cardiopulmonary bypass at 20°C. J Thorac Cardiovasc Surg1986; 92: 1065–1070.
466 Reich DL, Uysal S, Ergin A et al. Retrograde cerebral perfusion as a method of neuro-protection during thoracic aortic surgery. Ann Thorac Surg 2001; 72: 1774–1782.
467 Usui A, Oohara K, Liu T-L et al. Determination of optimum retrograde cerebral perfusionconditions. J Thorac Cardiovasc Surg 1994; 107: 300–308.

CHAPTER 17
Complications of aortic surgery
Thoralf M Sundt III, Whitney M Burrows
Background
Cardiovascular surgeons may be called on to treat aneurysmal disease involv-ing the ascending aorta and aortic root, the aortic arch, or the descending thoracic and thoracoabdominal aorta. Surgery may be indicated for the management of degenerative disease, dissection, or the prevention of com-plications of connective tissue disorders. Although these procedures representa relatively small proportion of the practice of most surgeons, they may beindicated emergently, behooving all surgeons to become familiar with theirconduct. Operations on the aorta are often complex, and patients requiringthem often have significant comorbidities. Complications are therefore notuncommon.
Despite a wide spectrum of underlying conditions and pathological anatom-ical characteristics, most aortic surgical procedures present common challenges.These operations generally involve interrupting or redirecting the circulationto some or all of the organ beds for a period, with end-organ ischemia being anobvious concern. The procedures may be lengthy, most often requiring extra-corporeal support, which predisposes patients to hemorrhagic complications.Furthermore, many patients who have a surgical procedure for complex aorticproblems have underlying pulmonary disease or renal dysfunction.
Therefore, we have organized our comments by organ system rather than by type of procedure, with a focus on the recognition, treatment, and, mostimportantly, prevention of the common complications. Although we subscribeto the concept of evidence-based practice, complex aortic procedures remainrelatively uncommon and sufficiently heterogeneous so that few centers per-form enough aortic procedures to permit rigorous analysis of risk factors andprevention. Therefore, many of our recommendations are based on anecdotalexperience.
Vascular complications
Patients undergoing aortic procedures often have a systemic vasculopathy, sothat the site of cannulation for perfusion assistance is an abnormal vessel, asare the vessels at the limits of any repair. Vascular complications are the mostimmediate and prominent technical challenges in aortic surgery.
349

350 Chapter 17
Vascular accessMost aortic reconstructions in the adult require temporary circulatory supportas either full cardiopulmonary bypass or partial left heart bypass. Tradi-tionally, arterial inflow has usually been achieved through femoral arterialcannulation; however, these vessels are often diseased with either localatherosclerosis or dissection. Therefore, attention must be paid to the potentialfor significant local vessel trauma with the disruption of atherosclerotic debristhat may embolize proximally during perfusion or move anterograde throughthe limb after decannulation. Local thrombosis may also occur as a con-sequence of endothelial damage or elevation of local plaque. Malperfusion dueto cannulation of the false lumen in dissections that have propagated beyondthe common femoral artery, or as a result of an iatrogenic retrograde dis-section, may also occur. In addition, pathological features of the abdominalaorta pose potential problems whenever retrograde perfusion is institutedwith dislodgement of thrombotic or atheroembolic material that may be propelled cephalad to the kidneys or brain.
Early recognition of the local complications of thrombosis or iatrogenicstenosis of the femoral artery permits the most expeditious management,which is in the operating room at the termination of the procedure. A satisfact-ory femoral pulse should always be verified manually or by Doppler analysis.Similarly, pedal pulses, which must be accurately documented preoperatively,must be identified. Reexploration of the arteriotomy can then be readily per-formed with local endarterectomy or patch arterioplasty as indicated. Whenthere is significant concern that plaque has been disrupted, we approach local endarterectomy and reconstruction aggressively, with a small patch ofsynthetic material.
Evidence of distal embolization should also be investigated before thedrapes are removed entirely. Intact popliteal pulses with loss of a pedal pulseor mottling of the distal lower extremity may be addressed by passing anembolectomy catheter distally from the femoral arteriotomy. Occasionally,popliteal exploration is requiredain either case, prompt recognition of theproblem minimizes limb ischemia and the risk of tissue loss. As dishearteningas such problems may be in the operating theater after a long procedure, the news comes much harder several hours later, after the patient is in theintensive care unit, with the prospect of remobilizing the operating room staff.
Malperfusion syndromes may be more difficult to recognize. Unfortunately,their consequences, which are obvious, may be more grave. One must considerthe possibility of malperfusion whenever peripheral perfusion is initiated. It may be evidenced by a decrease in urine output when the renal vessels areinvolved or by acidosis when the viscera are ischemic. These are non-specificsigns, and they may not become apparent until later during the procedure.Some surgeons advocate the use of bilateral radial artery lines, particularlywith acute dissection, when the risk of malperfusion is probably the greatest.The onset of a significant gradient between radial artery pressures may then betaken as evidence of malperfusion. If this occurs at the initiation of perfusion,

Complications of aortic surgery 351
its discontinuance and an attempt at alternative cannulation are indicated. Ifmalperfusion becomes evident when an aortic cross clamp is placed for acutedissection, removal of the cross clamp and cooling to hypothermic circulatoryarrest are indicated.
Perhaps most vexing is retrograde embolization of local debris from the can-nulation site or from thoracoabdominal disease. The consequences are usuallyappreciated only postoperatively when stroke or visceral infarction becomesapparent. Preoperatively and intraoperatively, the surgeon must be attentiveto the potential for retrograde embolization and should consider all possibleperfusion strategies.
The risk of retrograde embolization may be minimized by a preference forcentral cannulation, an approach that has gained popularity recently and withwhich we agree. Ascending aortic aneurysms are rarely lined with thrombusas are abdominal aneurysms. Preoperative computed tomography (CT) canhelp to exclude thrombus. Furthermore, although atherosclerotic disease may be present, most often it consists of medial calcification. Intraoperativetransesophageal echocardiography or intraoperative aortic surface echocar-diography can help to rule out shaggy intraluminal disease that is more likelyto embolize.
When forced to cannulate in the groin, either because of central disease orwhen using left heart bypass, we have preferred the time-honored approach ofsewing a ‘chimney’ of 8–10 mm of Dacron (DuPont, Wilmington, DE, USA) tothe common femoral artery before heparinization [1]. A 22-Fr or 24-Fr arterialcannula easily fits into such a chimney, essentially eliminating all concerns ofthe perfusionist about arterial line pressure. It also permits a careful, atrau-matic entry into the arterial system, minimizing the risk of retrograde dis-section or elevating a proximal plaque with the tip of our inflow cannula. Localvessel trauma is also minimized, and perfusion of the extremity throughoutthe procedure is permitted. At the termination of bypass, the chimney can beoversewn, leaving a small Dacron patch arterioplasty. Often the chimney canbe sewn to the femoral artery simultaneously with intubation and placementof the pulmonary artery catheter. When the patient must be repositioned (e.g., for thoracoabdominal aneurysm repair), the chimney graft may betucked inside the groin wound and the skin closed with staples to be reopenedafter the patient is rolled into a right lateral decubitus position.
An alternative site of arterial cannulation is the subclavian artery [2]. Thisapproach avoids retrograde perfusion of a diseased thoracoabdominal aortaand facilitates early antegrade reperfusion of the brachiocephalic vessels during arch reconstruction. It is accomplished most easily with a chimneygraft and is gaining popularity rapidly.
Femoral venous cannulation for partial femorofemoral bypass or full cardiopulmonary bypass may be complicated by disruption of the vessel proximally during placement of the cannula. This complication is most oftenrecognized by acute and sometimes nearly catastrophic volume loss. Whenthis occurs, rapid extension of the femoral incision and retroperitoneal

352 Chapter 17
exploration can be lifesaving. To avoid this complication we prefer to use anover-the-wire system, of which several are available.
The most common late complication of femoral venous access is deep veinthrombosis. To minimize local trauma, we have abandoned circumferentialdissection and control of the vessel in favor of exposure of the ventral surfaceonly and placement of a narrow, longitudinally orientated purse-string sutureon the top of the vessel. The vein can then be accessed and the purse-stringsuture secured, disrupting only a limited portion of the vessel and permittingvenous return from the distal extremity around the cannula. This avoidsplethora of the limb. On decannulation, the purse-string suture can be securedwithout narrowing the vessel.
Anastomotic complicationsAnastomotic complications may occur early or late after major aortic re-construction. Early problems include dislodgement of atheroembolic diseaseand tissue failure with anastomotic disruption and hemorrhage. Late post-operative pseudoaneurysms are most likely an underdiagnosed complication.
The site of distal anastomosis is often diseased, particularly in arch and thoracoabdominal aneurysms. If the material is calcific, local endarterectomymay be necessary to make distal anastomosis possible. The prophylactic valueof local endarterectomy on distal embolization is unclear, however, becausethere is usually no discrete border to the lesion and a shaggy ledge oftenremains. More frequently, the material is soft, like silt on the bottom of a slow-moving stream. Therefore, we usually try to minimize disruption of thematerial rather than attempt to remove it. Occasionally, we have created a ‘sandwich’ of Teflon felt (DuPont), first basting two strips of the material atthe site of anastomosis with 4–0 suture in a continuous horizontal mattresspattern and then sewing the graft to the sandwich itself.
Late pseudoaneurysms may be diagnosed when their sequelae of rupture or mass effect occur. Preferably, they should be identified by routine non-invasive imaging studies, such as CT or magnetic resonance imaging. Althoughthere are no evidence-based guidelines for the appropriate frequency of post-operative imaging studies, it is clear from articles about abdominal aorticgrafts that the frequency of diagnosis of postoperative pseudoaneurysms ismuch greater in series including routine surveillance studies [3]. Therefore,our view is that long-term surveillance, perhaps on an annual or biannualbasis, should be undertaken of all patients who have undergone major aorticreconstructions. This practice also provides surveillance for the formation of sub-sequent aneurysms in other locations, because multiple aneurysms may occur.
The risk of late pseudoaneurysm formation may be minimized by meticuloussurgical technique. Kouchoukos et al. [4] have demonstrated that, for com-posite aortic root replacement, fewer late pseudoaneurysms result from an ‘open’ technique that consists of creation of separate coronary artery but-tons for reimplantation, complete transection of the distal aorta to ensure
Complications of aortic surgery 353
full-thickness sutures, and avoidance of wrapping the remaining aneurysmalaorta around the repair. This approach permits repair of any imperfections inthe anastomoses during the initial operative procedure and prevents inadvert-ent covering of potential problems. Of course, this technique is only possiblebecause low-porosity grafts and excellent suture material are available.
Another potential contributor to late pseudoaneurysm formation is infec-tion. Placement of a graft in an infected field is uncommon, but it must be recognized. Therefore, when the suspected cause of an aneurysm is mycotic,either grossly or on CT, or when a patient with a known aneurysm exhibitsbacteremia, the use of antibiotic impregnated grafts and lifelong antibiotictherapy should be considered. The value of aortic homografts in this setting isnot yet widely accepted [5].
Finally, the surgeon should recognize the existence of collagen vascular disease, such as the Marfan syndrome, that may predispose to late aneurysmformation. It is now well recognized, for example, that complete root replace-ment rather than separate valve and graft repair is necessary to address adequately pathological lesions of the aortic root or dissection in Marfan syndrome, because sinus tissue left behind will dilatate with time. Therefore,one is well advised to consider the existence of connective tissue disease whenoperating for aneurysmal disease, particularly in young patients, because thisfinding may influence a surgeon’s intraoperative decisions.
Myocardial complications
Complications related to myocardial ischemia and infarction are among the most common causes of death after aortic surgery. The cornerstone of dealing with these complications is prevention, and the most important step isadequate preoperative evaluation.
Our practice is to perform coronary arteriography on all patients who areundergoing work on the ascending aorta or aortic arch for which the surgicalapproach will be a median sternotomy and for which cardioplegic arrest willbe required. Occasionally concerns are raised about the risk of embolization of material from the aneurysm by the angiography catheter; however, from a practical standpoint this is quite rare and the information gathered is ofsufficient value to warrant the risk. The notable exception to this policy is acuteaortic dissection. Although some surgeons have defended the value of pre-operative angiography in this setting, the majority now think that the yield ofuseful information obtained from angiography is not worth the required timeand the accompanying risk imposed by the delay in surgery. We do, however,prepare the legs of all patients who have aortic dissection and manually per-form intraoperative inspection of the coronary arteries. We are liberal with the placement of saphenous vein grafts to vessels with palpable disease andfor patients with preoperative evidence of myocardial ischemia or significantinvolvement of the coronary ostia by the dissection flap.
354 Chapter 17
For operations on the thoracic or thoracoabdominal aorta, we prefer cardiaccatheterization whenever circulatory arrest is planned. In our experience, theuse of thallium or dobutamine echocardiographic non-invasive studies mayresult in underestimating the extent of disease in a substantial number of cases,and we are concerned about the stress imposed on the myocardium duringventricular fibrillation as the patient cools. We prefer coronary angiography ininstances of circulatory arrest because we think the magnitude of myocardialinsult is greater in these situations. We have seen the extent of disease dramat-icallyaand fatallyaunderestimated by the reliance on non-invasive studies.When left heart partial bypass is planned, we are more willing to accept theresults of non-invasive imaging.
The principles of intraoperative management to minimize ischemia arefamiliar to cardiothoracic surgeons. The debate over cardioplegia compositionand routes of its delivery need not be repeated here. However, with the use ofventricular fibrillation, either when an ascending aorta cannot be clamped orwhen the thoracic or thoracoabdominal aorta is approached through the leftside of the chest, the mean perfusion pressure must be maintained > 75 mmHgto maintain adequate myocardial perfusion. In order to prevent left ventriculardistension, we are liberal with placement of a left ventricular vent through thecardiac apex when we operate in the left side of the chest. Ventricular fibrilla-tion is contraindicated for patients with severe left ventricular hypertrophy orwith significant aortic regurgitation. The existence of these conditions shouldbe evaluated by preoperative echocardiography.
Pulmonary complications
Respiratory failure is a common complication of aortic surgery, probablybecause of the high incidence of concomitant emphysema in these patients.Tobacco use is rampant among those with degenerative aneurysmal diseaseand may lead to destructive airway disease and aneurysmal disease by thecommon pathophysiological mechanism. Recognition of respiratory failure isnot difficult, and its management is supportive, but its impact on survival is profound (Figure 17.1) [6].
Prevention of pulmonary complications begins with the patient. Tobaccouse should be discontinued before aneurysm repair, but that is often imprac-tical. Intraoperatively the surgeon should minimize lung manipulation througha collaborative approach with the anesthesiologists. During deflation of theleft lung, the right lung must not be hyperinflated. Full cardiopulmonarybypass averts problems with intraoperative oxygenation but probably exacer-bates postoperative lung dysfunction. When operating on patients who haveextensive pulmonary disease preoperatively, we use heparin-bonded circuitsin the hope that we will minimize cytokine activation. In addition, we useaprotinin as a pulmonary protective agent. However, we avoid performingfull bypass whenever possible in patients with the worst lung disease, and wehave occasionally used an oxygenator spliced into the left heart circuit to
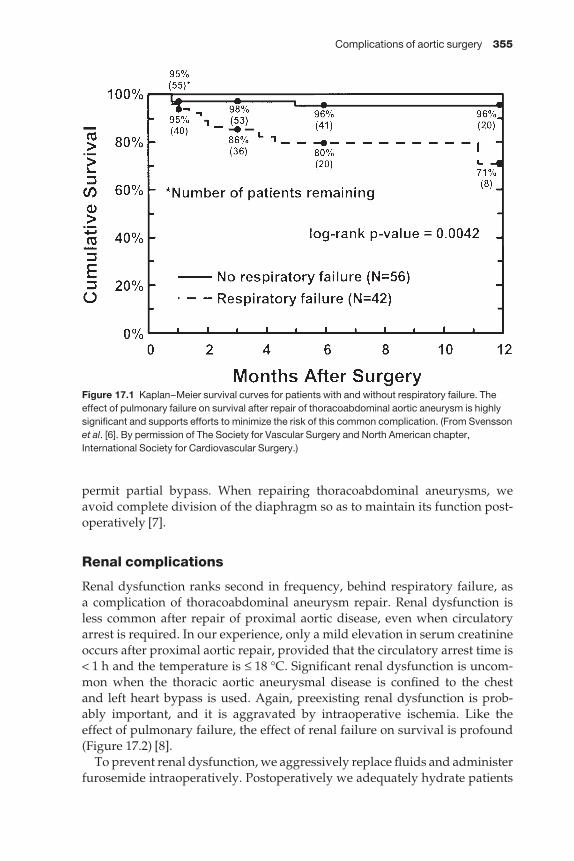
Complications of aortic surgery 355
permit partial bypass. When repairing thoracoabdominal aneurysms, weavoid complete division of the diaphragm so as to maintain its function post-operatively [7].
Renal complications
Renal dysfunction ranks second in frequency, behind respiratory failure, as a complication of thoracoabdominal aneurysm repair. Renal dysfunction isless common after repair of proximal aortic disease, even when circulatoryarrest is required. In our experience, only a mild elevation in serum creatinineoccurs after proximal aortic repair, provided that the circulatory arrest time is< 1 h and the temperature is ≤ 18 °C. Significant renal dysfunction is uncom-mon when the thoracic aortic aneurysmal disease is confined to the chest and left heart bypass is used. Again, preexisting renal dysfunction is prob-ably important, and it is aggravated by intraoperative ischemia. Like the effect of pulmonary failure, the effect of renal failure on survival is profound(Figure 17.2) [8].
To prevent renal dysfunction, we aggressively replace fluids and administerfurosemide intraoperatively. Postoperatively we adequately hydrate patients
Figure 17.1 Kaplan–Meier survival curves for patients with and without respiratory failure. Theeffect of pulmonary failure on survival after repair of thoracoabdominal aortic aneurysm is highlysignificant and supports efforts to minimize the risk of this common complication. (From Svenssonet al. [6]. By permission of The Society for Vascular Surgery and North American chapter,International Society for Cardiovascular Surgery.)
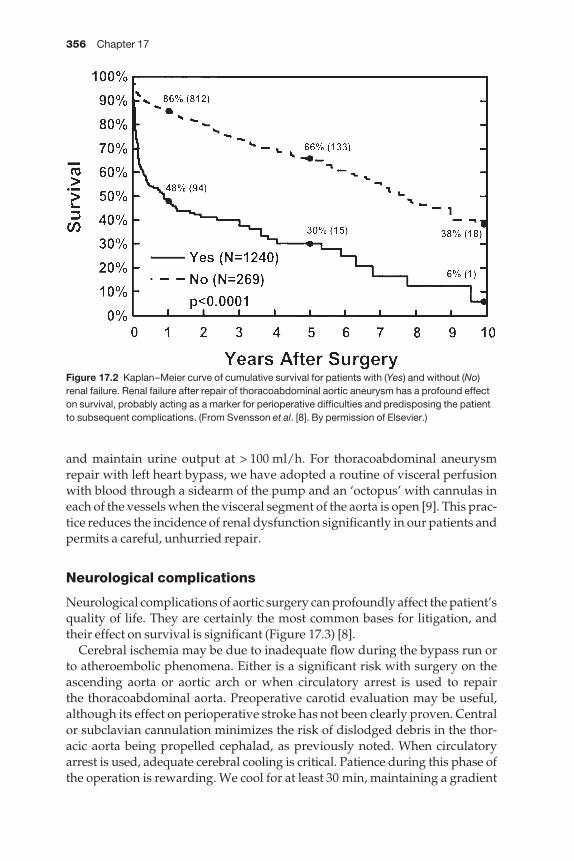
356 Chapter 17
and maintain urine output at > 100 ml/h. For thoracoabdominal aneurysmrepair with left heart bypass, we have adopted a routine of visceral perfusionwith blood through a sidearm of the pump and an ‘octopus’ with cannulas ineach of the vessels when the visceral segment of the aorta is open [9]. This prac-tice reduces the incidence of renal dysfunction significantly in our patients andpermits a careful, unhurried repair.
Neurological complications
Neurological complications of aortic surgery can profoundly affect the patient’squality of life. They are certainly the most common bases for litigation, andtheir effect on survival is significant (Figure 17.3) [8].
Cerebral ischemia may be due to inadequate flow during the bypass run orto atheroembolic phenomena. Either is a significant risk with surgery on theascending aorta or aortic arch or when circulatory arrest is used to repair the thoracoabdominal aorta. Preoperative carotid evaluation may be useful,although its effect on perioperative stroke has not been clearly proven. Centralor subclavian cannulation minimizes the risk of dislodged debris in the thor-acic aorta being propelled cephalad, as previously noted. When circulatoryarrest is used, adequate cerebral cooling is critical. Patience during this phase ofthe operation is rewarding. We cool for at least 30 min, maintaining a gradient
Figure 17.2 Kaplan–Meier curve of cumulative survival for patients with (Yes) and without (No)renal failure. Renal failure after repair of thoracoabdominal aortic aneurysm has a profound effecton survival, probably acting as a marker for perioperative difficulties and predisposing the patientto subsequent complications. (From Svensson et al. [8]. By permission of Elsevier.)
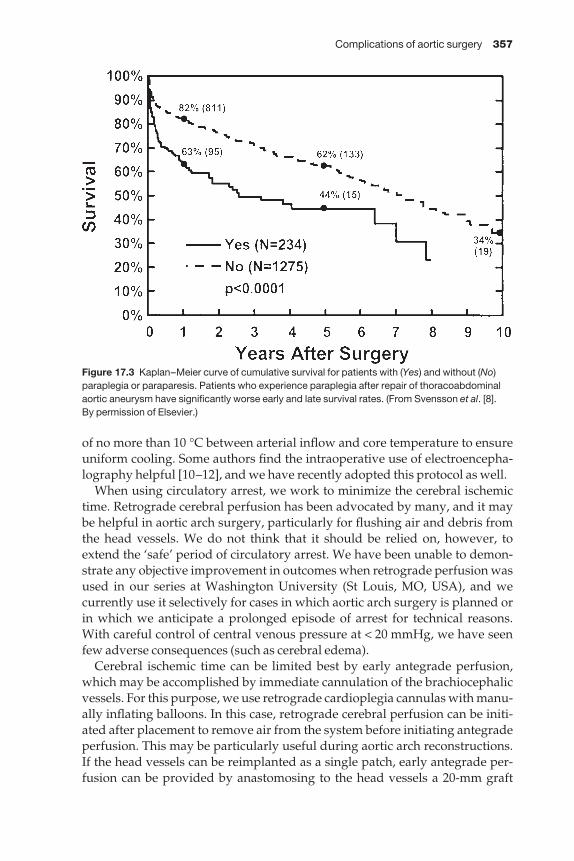
Complications of aortic surgery 357
of no more than 10 °C between arterial inflow and core temperature to ensureuniform cooling. Some authors find the intraoperative use of electroencepha-lography helpful [10–12], and we have recently adopted this protocol as well.
When using circulatory arrest, we work to minimize the cerebral ischemictime. Retrograde cerebral perfusion has been advocated by many, and it maybe helpful in aortic arch surgery, particularly for flushing air and debris fromthe head vessels. We do not think that it should be relied on, however, toextend the ‘safe’ period of circulatory arrest. We have been unable to demon-strate any objective improvement in outcomes when retrograde perfusion wasused in our series at Washington University (St Louis, MO, USA), and we currently use it selectively for cases in which aortic arch surgery is planned orin which we anticipate a prolonged episode of arrest for technical reasons.With careful control of central venous pressure at < 20 mmHg, we have seenfew adverse consequences (such as cerebral edema).
Cerebral ischemic time can be limited best by early antegrade perfusion,which may be accomplished by immediate cannulation of the brachiocephalicvessels. For this purpose, we use retrograde cardioplegia cannulas with manu-ally inflating balloons. In this case, retrograde cerebral perfusion can be initi-ated after placement to remove air from the system before initiating antegradeperfusion. This may be particularly useful during aortic arch reconstructions.If the head vessels can be reimplanted as a single patch, early antegrade per-fusion can be provided by anastomosing to the head vessels a 20-mm graft
Figure 17.3 Kaplan–Meier curve of cumulative survival for patients with (Yes) and without (No)paraplegia or paraparesis. Patients who experience paraplegia after repair of thoracoabdominalaortic aneurysm have significantly worse early and late survival rates. (From Svensson et al. [8]. By permission of Elsevier.)
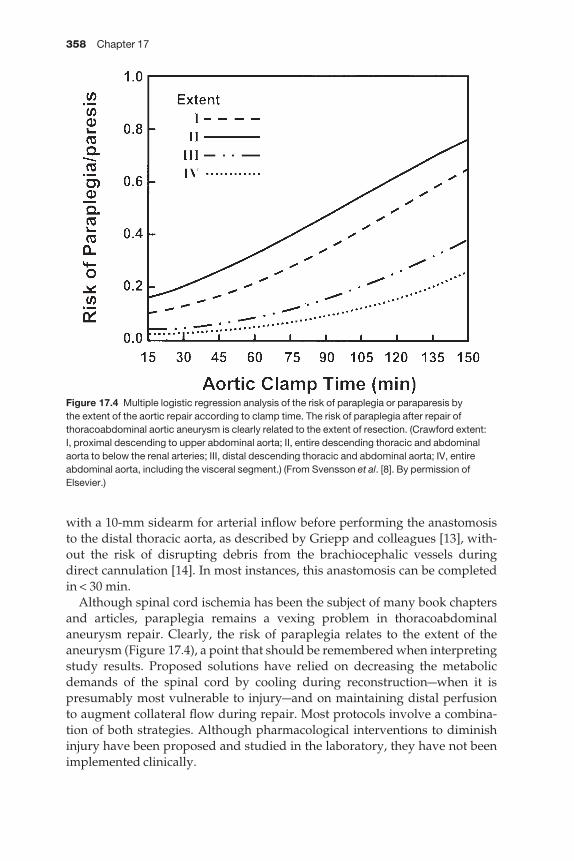
358 Chapter 17
with a 10-mm sidearm for arterial inflow before performing the anastomosis to the distal thoracic aorta, as described by Griepp and colleagues [13], with-out the risk of disrupting debris from the brachiocephalic vessels during direct cannulation [14]. In most instances, this anastomosis can be completedin < 30 min.
Although spinal cord ischemia has been the subject of many book chaptersand articles, paraplegia remains a vexing problem in thoracoabdominalaneurysm repair. Clearly, the risk of paraplegia relates to the extent of theaneurysm (Figure 17.4), a point that should be remembered when interpretingstudy results. Proposed solutions have relied on decreasing the metabolicdemands of the spinal cord by cooling during reconstructionawhen it is presumably most vulnerable to injuryaand on maintaining distal perfusion to augment collateral flow during repair. Most protocols involve a combina-tion of both strategies. Although pharmacological interventions to diminishinjury have been proposed and studied in the laboratory, they have not beenimplemented clinically.
Figure 17.4 Multiple logistic regression analysis of the risk of paraplegia or paraparesis by the extent of the aortic repair according to clamp time. The risk of paraplegia after repair ofthoracoabdominal aortic aneurysm is clearly related to the extent of resection. (Crawford extent: I, proximal descending to upper abdominal aorta; II, entire descending thoracic and abdominalaorta to below the renal arteries; III, distal descending thoracic and abdominal aorta; IV, entireabdominal aorta, including the visceral segment.) (From Svensson et al. [8]. By permission ofElsevier.)

Complications of aortic surgery 359
Routine use of femorofemoral bypass to achieve profound hypothermia forcirculatory arrest during repair has been advocated by Kouchoukos andRokkas [15] and has gained a loyal following. Good results with low rates ofparaplegia have been reported with this technique. Other authors, however,have expressed concern that the physiological insult imposed by this strategyis too great, essentially trading death for paraplegia. An alternative means of cooling the spinal cord, proposed by Cambria and Davison [16], entails cold epidural perfusion to accomplish topical cooling. This process is typicallyperformed without distal perfusion.
Distal perfusion during thoracic aortic occlusion may be accomplished byvarious means, including partial femorofemoral bypass, which demands complete heparinization, and left-atrial-to-femoral partial bypass, which canbe accomplished with minimal anticoagulation. Additional measures toimprove spinal cord perfusion during the vulnerable period include drainageof cerebrospinal fluid and vigorous support of blood pressure to maintainmean pressures > 75–80 mmHg above and below the clamp. The value ofreimplantation of intercostal vessels is questioned by some authors, but thetrend is certainly in favor of this approach [17]. Some authors use intraoperat-ive motor evoked potentials as well to help guide this process.
We think that a thoughtful, integrated approach to the prevention of spinal cord ischemia is appropriate. We prefer to use partial left heart bypasswhenever possible with strict adherence to segmental occlusion techniques.This practice permits an unhurried operation. Drainage of cerebrospinal fluidis routine [18]. We take advantage of the benefits of mild hypothermia and permit the systemic temperature to decrease to 34 °C during aortic reconstruc-tion. The temperature is returned to normal with an in-line heat exchangerbefore discontinuing bypass. We routinely reimplant sizable intercostal ves-sels between T8 and the visceral segment and have recently begun using motorevoked potentials. We are compulsive about maintaining adequate blood pres-sure postoperatively, and we emphasize to the house staff and nursing staffthat hypotension is far more dangerous than hypertension in these patients.
When left heart bypass is not possible because atherosclerotic disease at the left subclavian artery prevents placement of a cross clamp, we use cir-culatory arrest. In this instance, we do not use a spinal drain because we areconcerned about a subdural hematoma developing and compressing the cord.We reserve circulatory arrest for special instances because we are concernedabout the pulmonary insult and hematological abnormalities imposed by thisapproach.
Hematological complications
Although less often fatal, hematological derangements are common with aortic surgeryamuch to the consternation of surgeons and anesthesiologists.Coagulopathy is often a problem after extensive aortic procedures involving
360 Chapter 17
circulatory arrest. A lengthy pump run and hypothermia lead to platelet dysfunction, and extensive suture lines as well as large surface areas of Dacronconsume platelets and clotting factors. This is particularly true for the elephanttrunk procedure, possibly because of sequestration of clotting factors outsidethe distal trunk. Prompt and aggressive replacement of clotting factors is usu-ally satisfactory, but it is critical that all clotting factors arrive in the operatingroom simultaneously. When using left heart bypass, ongoing follow-up of the replacement of clotting factors during the period of partial bypass is critical. A strategy of waiting to give clotting factors until after partial bypass is completed can be disastrous.
Therapy with adjunctive medication such as aprotinin or otherantifibrinolytics may be helpful. Our early experience with aprotinin raisedconcerns about its safety during circulatory arrest, and we prefer to administerthe drug only after the arrest episode is complete [19]. Also, adequate concen-trations of heparin must be maintained. Although there is much enthusiasmfor using various glues and sealants, we find meticulous attention to surgicaltechnique, care in handling tissues, and smooth passage of suture needles to beof far greater importance.
Conclusion
Complications after major aortic surgery are common, in part because thepatients undergoing the procedures have underlying multisystem disease.The procedures themselves are often complex, with unique challenges. A coordinated team approach with meticulous attention to detail is critical toachieving the best possible results. With such an approach, excellent resultscan be achieved even when replacing extensive portions of the aorta. There-fore, it is likely that optimal results will be achieved by concentrating the experience among surgical teams with a special interest in this area.
References
1 Vander Salm TJ. Prevention of lower extremity ischemia during cardiopulmonary bypassvia femoral cannulation. Ann Thorac Surg 1997; 63: 251–252.
2 Gillinov AM, Sabik JF, Lytle BW et al. Axillary artery cannulation. J Thorac Cardiovasc Surg1999; 118: 1153.
3 Edwards JM, Teefey SA, Zierler RE et al. Intraabdominal paraanastomotic aneurysmsafter aortic bypass grafting. J Vasc Surg 1992; 15: 344–350.
4 Kouchoukos NT, Wareing TH, Murphy SF et al. Sixteen-year experience with aortic rootreplacement. Results of 172 operations. Ann Surg 1991; 214: 308–318.
5 Vogt P, Pasic M, von Segesser L et al. Cryopreserved aortic homograft for mycoticaneurysm. J Thorac Cardiovasc Surg 1995; 109: 589–591.
6 Svensson LG, Hess KR, Coselli JS et al. A prospective study of respiratory failure afterhigh-risk surgery on the thoracoabdominal aorta. J Vasc Surg 1991; 14: 271–282.
7 Engle J, Safi HJ, Miller CC III et al. The impact of diaphragm management on prolongedventilator support after thoracoabdominal aortic repair. J Vasc Surg 1999; 29: 150–156.
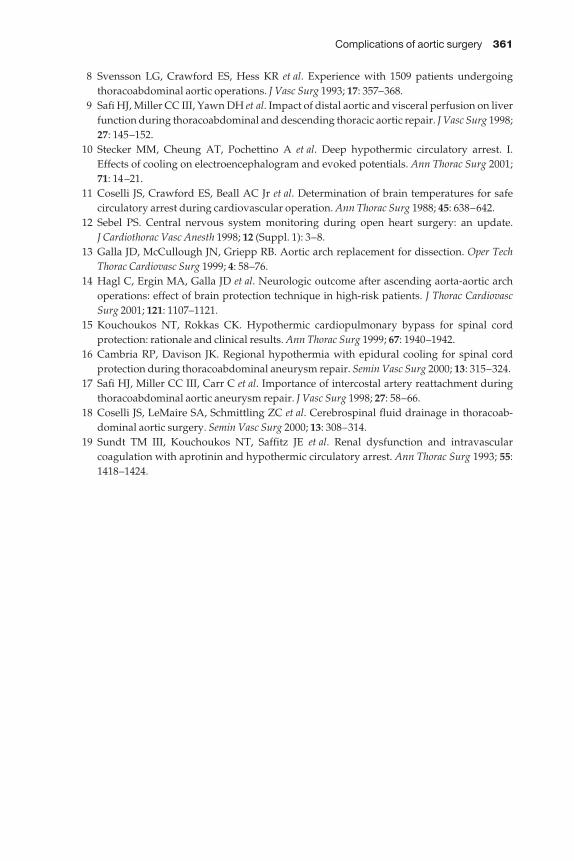
Complications of aortic surgery 361
8 Svensson LG, Crawford ES, Hess KR et al. Experience with 1509 patients undergoing thoracoabdominal aortic operations. J Vasc Surg 1993; 17: 357–368.
9 Safi HJ, Miller CC III, Yawn DH et al. Impact of distal aortic and visceral perfusion on liverfunction during thoracoabdominal and descending thoracic aortic repair. J Vasc Surg 1998;27: 145–152.
10 Stecker MM, Cheung AT, Pochettino A et al. Deep hypothermic circulatory arrest. I.Effects of cooling on electroencephalogram and evoked potentials. Ann Thorac Surg 2001;71: 14–21.
11 Coselli JS, Crawford ES, Beall AC Jr et al. Determination of brain temperatures for safe circulatory arrest during cardiovascular operation. Ann Thorac Surg 1988; 45: 638–642.
12 Sebel PS. Central nervous system monitoring during open heart surgery: an update. J Cardiothorac Vasc Anesth 1998; 12 (Suppl. 1): 3–8.
13 Galla JD, McCullough JN, Griepp RB. Aortic arch replacement for dissection. Oper TechThorac Cardiovasc Surg 1999; 4: 58–76.
14 Hagl C, Ergin MA, Galla JD et al. Neurologic outcome after ascending aorta-aortic archoperations: effect of brain protection technique in high-risk patients. J Thorac CardiovascSurg 2001; 121: 1107–1121.
15 Kouchoukos NT, Rokkas CK. Hypothermic cardiopulmonary bypass for spinal cord protection: rationale and clinical results. Ann Thorac Surg 1999; 67: 1940–1942.
16 Cambria RP, Davison JK. Regional hypothermia with epidural cooling for spinal cord protection during thoracoabdominal aneurysm repair. Semin Vasc Surg 2000; 13: 315–324.
17 Safi HJ, Miller CC III, Carr C et al. Importance of intercostal artery reattachment duringthoracoabdominal aortic aneurysm repair. J Vasc Surg 1998; 27: 58–66.
18 Coselli JS, LeMaire SA, Schmittling ZC et al. Cerebrospinal fluid drainage in thoracoab-dominal aortic surgery. Semin Vasc Surg 2000; 13: 308–314.
19 Sundt TM III, Kouchoukos NT, Saffitz JE et al. Renal dysfunction and intravascular coagulation with aprotinin and hypothermic circulatory arrest. Ann Thorac Surg 1993; 55:1418–1424.

CHAPTER 18
Complications of valvular surgery
Jeffrey T Sugimoto, Anthony D Bruno, Karen A Gersch
Aortic valve surgery
AnatomyThe aortic valve is a tri-leaflet structure which separates the left ventricularoutflow tract and the aorta or Sinuses of Valsalva. There are three leaflets orcusps, the left, the right and non-coronary, which are attached in a semicircularpath to the base of the aorta at the fibrous annulus. For each leaflet the annularattachment does not lie in a single plane, being half moon in shape with thenadir at the mid-point of the leaflets and the peak at the commissural posts.There is a slight dilatation of the aorta above the valve associated with each ofthe leaflets, the Sinuses of Valsalva. This dilatation creates a vortex of bloodflow important in valve closure. The sinuses end at the sino–tubular junctionwhich is the narrowest portion of the ascending aorta. Below and in continuitywith the left and non-coronary cusps is the anterior leaflet of the mitral valve.The ventricular septum lies below the right coronary cusp and within it a portion of the conduction system, most importantly the left bundle, and bundle of His. The left main coronary artery arises from the left Sinus ofValsalva. Its ostium lies directly posterior near the level of the sino–tubularjunction. The left main coronary artery runs to the left under the pulmonaryartery before dividing into the left anterior descending and circumflex arteries.Anatomic variants have been described and it is important to identify andavoid injury to the ostium as well as the artery as it courses behind the aortanear the annulus. The left main coronary artery can run perilously close to thecommissure between the left and right coronary cusps. The right coronaryostium is an anterior structure located above the right coronary cusp. Its posi-tion tends to be more variable and is often displaced with aneurysmal changesin the aorta. Awareness of these anatomic relationships is critical to the safeconduct of aortic valve surgery (see Figure 18.1).
Incisions and cardiopulmonary bypassRecently ‘less invasive’ incisions or approaches to the aortic valve have beendescribed; transverse sternotomy, partial sternotomy, right para-sternotomy,manubrial inverted ‘T’, reversed Z sternotomy, ‘J/j ’ incision and upper rightanterior thoracotomy have all been utilized successfully [1–4]. Each can beuseful and generally do provide adequate exposure of the valve. However, if
362
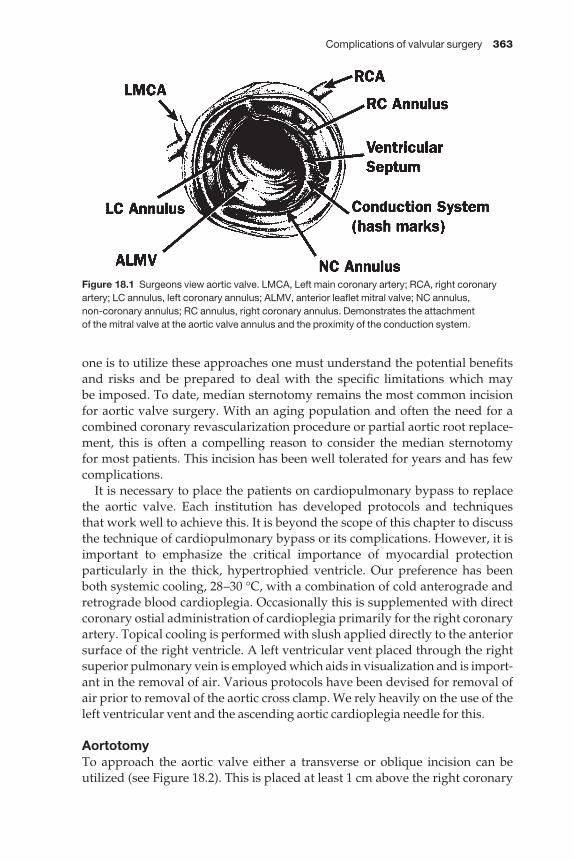
Complications of valvular surgery 363
one is to utilize these approaches one must understand the potential benefitsand risks and be prepared to deal with the specific limitations which may be imposed. To date, median sternotomy remains the most common incisionfor aortic valve surgery. With an aging population and often the need for acombined coronary revascularization procedure or partial aortic root replace-ment, this is often a compelling reason to consider the median sternotomy for most patients. This incision has been well tolerated for years and has fewcomplications.
It is necessary to place the patients on cardiopulmonary bypass to replacethe aortic valve. Each institution has developed protocols and techniques that work well to achieve this. It is beyond the scope of this chapter to discussthe technique of cardiopulmonary bypass or its complications. However, it isimportant to emphasize the critical importance of myocardial protection particularly in the thick, hypertrophied ventricle. Our preference has beenboth systemic cooling, 28–30 °C, with a combination of cold anterograde andretrograde blood cardioplegia. Occasionally this is supplemented with directcoronary ostial administration of cardioplegia primarily for the right coronaryartery. Topical cooling is performed with slush applied directly to the anteriorsurface of the right ventricle. A left ventricular vent placed through the rightsuperior pulmonary vein is employed which aids in visualization and is import-ant in the removal of air. Various protocols have been devised for removal ofair prior to removal of the aortic cross clamp. We rely heavily on the use of theleft ventricular vent and the ascending aortic cardioplegia needle for this.
AortotomyTo approach the aortic valve either a transverse or oblique incision can be utilized (see Figure 18.2). This is placed at least 1 cm above the right coronary
Figure 18.1 Surgeons view aortic valve. LMCA, Left main coronary artery; RCA, right coronaryartery; LC annulus, left coronary annulus; ALMV, anterior leaflet mitral valve; NC annulus, non-coronary annulus; RC annulus, right coronary annulus. Demonstrates the attachment of the mitral valve at the aortic valve annulus and the proximity of the conduction system.

364 Chapter 18
ostium to avoid compromise on closure which can result in right ventricular orinferior infarction. With an aging population calcifications of the aortic rootinvolving the Sinuses of Valsalva, sino–tubular junction and ascending aortaare common. Attempts to avoid these areas when feasible are recommended.Otherwise limited endarterectomy and debridement, or aortic reconstructionmay be necessary to allow for successful closure. If the ascending aorta is heav-ily calcified, consideration of femoral artery cannulation, deep hypothermiaand circulatory arrest without aortic cross clamping must be made to avoidembolization, stroke, as well as to allow for the successful completion of theoperation. Epi-aortic and transesophageal echo may be a useful adjuncts [5]. In most cases it will be possible to place the aortic cannula, the aortic crossclamp and aortotomy in the ascending aorta, avoiding calcified areas.
Post-stenotic dilatation or pure aneurysmal disease will cause thinning and enlargement of the aorta with the potential catastrophic complication ofaortic dissection. Great care in controlling blood pressure and flow while oncardiopulmonary bypass, with particular attention to detail with the bloodpressure at cannulation, cross clamp placement and removal as well as whenweaning the patient from cardiopulmonary bypass, is critical to avoid thiscomplication. Aggressive anesthetic management and communication withthe anesthesiologist are particularly important to avoid wide fluctuations inblood pressure.
The transverse aortotomy is made above the sino–tubular junction, avoid-ing the right coronary ostium with the oblique incision directed towards themid portion of the non-coronary leaflet through the sino–tubular junction.Rarely is the aorta completely transected except with the implant of somestentless valves. A longitudinal T-shape aortotomy can also be used [6].Uncontrolled tearing of the aortotomy must be avoided. More room for inser-tion of the prosthesis is achieved by utilizing the oblique incision which opensthe narrow sino–tubular junction. Closure of the aorta often depends on thestrength and thickness of the aorta. A secure closure in select cases can beachieved with a single running mono-filament suture line (4–0 Prolene RB-1®).
Figure 18.2 Surgeons viewaaortotomy.Oblique incision in aorta carried down throughthe sino–tubular junction in the non-coronarysinus of valsalva.

Complications of valvular surgery 365
In a thin or diseased aorta, a two-layer closure is recommended with an initialhorizontal mattress everting suture line followed by a single running over anover suture line. This suture line can also be performed buttressing the initialhorizontal mattress suture with strips of Teflon felt or strips of a Hemashield®
Dacron graft or pericardium. At the completion of the closure there is rarelybleeding, though, with the force of left ventricular contraction as the patient is weaned from cardiopulmonary bypass, bleeding may occur. It is best to control all bleeding while on cardiopulmonary bypass, controlling flow andblood pressure. Early removal of cannulas should be avoided. Resumption of 364a brief period of cardiopulmonary bypass is preferable to tearing of thesuture line which may then require major revision. Strict control of the bloodpressure and anesthetic management is critical at this phase. With the avail-ability of Bioglue®, it is often best to consider aortic repair of the friable-debrided areas prior to suturing. One can apply the Bioglue® protectingadequately the prosthesis prior to suturing of the aortotomy.
Aortic valve removalRemoval of the aortic valve for insufficiency is usually straight forward. It isbest to leave a thin rim of valve tissue and not to excise the annulus completely.Any excess valve tissue can be trimmed leaving a solid annulus. In calcific disease it is often possible to achieve the same result, though invariably theannulus, subannular region, mitral valve can be involved with calcifications.Careful debridement is required to avoid detaching the aorta from the left vent-ricle below. A pituitary rongeur can be used to crush the calcium into smallerparticles and then remove the calcium, leaving the aorta, aortic annulus as wellas left ventricle intact. Crushing horizontally along the axis of the annulus issafer than vertically. Tears in the aorta, annulus and mitral valve can occurwith over-aggressive force trying to remove the calcium. If tears occur, repairis achieved with pledgeted horizontal mattress sutures brought from below.These can be later used to secure the valve. Extensive calcification below theright coronary annulus may require debridement with the potential hazard of heart block. Calcium often extends into the anterior leaflet of the mitralvalve from the non-coronary annulus. Superficial debridement to allow forplacement of sutures and valve seating can be performed without perforatingthe valve. One should avoid debriding calcium from the walls of the Sinuses of Valsalva unless it is protruding significantly or will not allow for properseating of the prosthesis. If the calcifications of the annulus extend directly into and up the wall of the sinuses, very limited debridement may be appliedavoiding the coronary ostia. This should avoid the need for extensive re-construction or root replacement. Rarely should this be necessary even whenextensive calcification is identified, and should be avoided when possible.
All debris must be accounted for, with the potential for losing calcium intothe left ventricle and coronary ostia, particularly the left. Sponges, tampons,and balloons have been utilized to prevent the loss of calcium into the left vent-ricular cavity [7]. Small pieces of gauze (nu-gauze®) or cotton-tip applicators
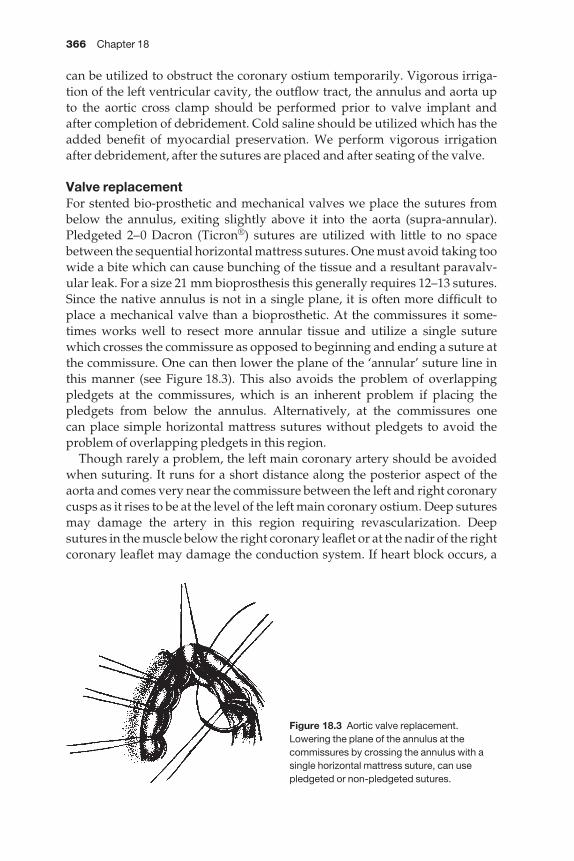
366 Chapter 18
can be utilized to obstruct the coronary ostium temporarily. Vigorous irriga-tion of the left ventricular cavity, the outflow tract, the annulus and aorta up to the aortic cross clamp should be performed prior to valve implant and after completion of debridement. Cold saline should be utilized which has theadded benefit of myocardial preservation. We perform vigorous irrigationafter debridement, after the sutures are placed and after seating of the valve.
Valve replacementFor stented bio-prosthetic and mechanical valves we place the sutures frombelow the annulus, exiting slightly above it into the aorta (supra-annular).Pledgeted 2–0 Dacron (Ticron®) sutures are utilized with little to no spacebetween the sequential horizontal mattress sutures. One must avoid taking toowide a bite which can cause bunching of the tissue and a resultant paravalv-ular leak. For a size 21 mm bioprosthesis this generally requires 12–13 sutures.Since the native annulus is not in a single plane, it is often more difficult toplace a mechanical valve than a bioprosthetic. At the commissures it some-times works well to resect more annular tissue and utilize a single suturewhich crosses the commissure as opposed to beginning and ending a suture atthe commissure. One can then lower the plane of the ‘annular’ suture line inthis manner (see Figure 18.3). This also avoids the problem of overlappingpledgets at the commissures, which is an inherent problem if placing the pledgets from below the annulus. Alternatively, at the commissures one can place simple horizontal mattress sutures without pledgets to avoid theproblem of overlapping pledgets in this region.
Though rarely a problem, the left main coronary artery should be avoidedwhen suturing. It runs for a short distance along the posterior aspect of theaorta and comes very near the commissure between the left and right coronarycusps as it rises to be at the level of the left main coronary ostium. Deep suturesmay damage the artery in this region requiring revascularization. Deepsutures in the muscle below the right coronary leaflet or at the nadir of the rightcoronary leaflet may damage the conduction system. If heart block occurs, a
Figure 18.3 Aortic valve replacement.Lowering the plane of the annulus at thecommissures by crossing the annulus with asingle horizontal mattress suture, can usepledgeted or non-pledgeted sutures.

Complications of valvular surgery 367
permanent transvenous pacemaker can be placed postoperatively. Removaland replacement of the sutures should not be attempted. Damage to the rightcoronary artery or ostium can also lead to stenosis or acute right ventricularfailure intraoperatively [8]. After removal of the aortic valve below the non-coronary and left coronary leaflet, the anterior leaflet of the mitral valve is obvious. Small defects can be repaired with monofilament suture. Thoughdiscussions about what to do with the small aortic root will follow, it is oftenhelpful in a small annulus to place the sutures along the non-coronary annulusfrom outside the aorta and bring it directly through or above the non-coronaryannulus, leaving the pledgets outside the aorta. This often avoids the need for placing the valve obliquely above either the non-coronary annulus or theaortic root enlargement. If the aorta in the region appears thin, these suturesshould exit the aorta directly through the annulus. The pledgets lay on the outside of the aorta.
Seating the valve at the lowest point of each annular leaflet is critical. In general, it is best to tie one suture at the point lowest in each cusp before tyingall others. This ensures proper seating of the valve and confidence that the valve will fit before having to remove multiple sutures for an oversizedprosthesis or before deciding that an aortic root enlargement procedure maybe necessary. The coronary ostia must always be identified and reconfirmedwhile seating the valve. At times this does require the use of a small dental mir-ror to re-identify the right coronary ostium. When tying the sutures one shouldavoid contact of the suture with the leaflets, particularly for a bioprostheticvalve. Though it is often difficult to tie the sutures along the axis of the valvering, it is generally best to avoid tying the sutures across the valve in a per-pendicular manner. The bioprosthetic valve should be moistened regularly toprevent drying. Once the valve is seated and tied into position, one shouldcarefully inspect the suture line using a small suction tip (Frazier) for possibleparavalvular leaks. Additionally, one can take a final look for any potentialdebris which might have been dislodged from the Sinuses of Valsalva in tyingdown the valve. Mechanical prostheses should be tested for unrestrictedleaflet motion. It is generally good practice to irrigate the left ventricularoutflow tract, suture line and aorta at this point prior to aortic closure.
The small aortic root, aortic valve replacementCritical to the success of operations for aortic stenosis is the placement of aprosthesis that does not leave the patient with significant residual aortic sten-osis (patient–prosthetic mismatch). In general, for the stented bioprosthesis, this would mean the use of at least a size 21 mm valve and for a mechanicalvalve a size 19 mm. It is also important to consider the fragility and size of the patient when making the decision for aortic root enlargement. Each of the various prosthetic devices utilizes a different set of sizers and it is not recommended to interchange them. The sizer should fit comfortably into theannulus, particularly when the aortic root is stiff, thickened or calcified. Oncethe appropriate sized valve is chosen, it is generally good practice to check to
368 Chapter 18
be sure that the prosthesis will fit into the orifice before placing the sutures intothe sewing ring.
If there is concern about placement of the valve, one simple option that doesnot prolong the operation is to ‘tilt’ the valve placing the suture line in the non-coronary cusp above the true annulus in the wall of the aorta (see Figure 18.4).This will often increase the size of the prosthesis by one and avoid the need to enlarge the aortic root. This can be done with any of the stented biopros-theses. However, care must be taken when considering this for a mechanicalvalve, given the potential for leaflet impingement by the non-coronary annulartissue below. If a single-leaflet mechanical prosthesis is utilized, the majororifice should be directed towards the patient’s right side to allow for unre-stricted maximal opening.
If aortic root enlargement is still desired, multiple procedures have beendescribed. The simplest is extension of the aortotomy to the mid point of the non-coronary annulus [9]. One does not necessarily need to transect theannulus. An elliptical piece of Dacron graft (Hemashield®) is then suturedwhich allows for aortic root enlargement just above the aortic annulus in thenon-coronary cusp. One does not necessarily need to enter the roof of the leftatrium or cut into the mitral valve to perform this procedure. The prosthesiscan then be sutured in a tilted position again a few millimeters above the trueannulus incorporating the patch as part of the valve suture line (see Figure18.5). We perform this procedure with a small patch of a Hemashield® Dacrongraft and utilize a running 4.0 Prolene® suture. The graft is sutured in place to apoint a few millimeters above where we believe the valve will be sutured to thepatch. After placement of the valve we complete this suture line. This sutureline below the prosthesis must be placed carefully and securely. It is virtuallyinaccessible once the prosthesis is placed. Troublesome bleeding generallycannot be controlled with simple sutures. We have found this procedure to
Figure 18.4 Aortic valve replacement. ‘Tilting’ the aortic valve prosthesis by placing suturesslightly above the annulus in the non-coronary cusp. This often eliminates the need to enlarge the annulus.
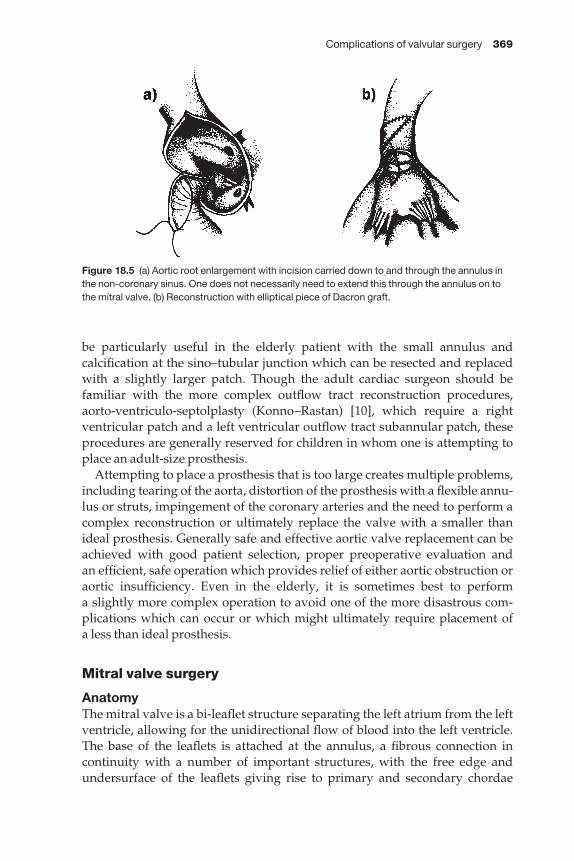
Complications of valvular surgery 369
be particularly useful in the elderly patient with the small annulus andcalcification at the sino–tubular junction which can be resected and replacedwith a slightly larger patch. Though the adult cardiac surgeon should be familiar with the more complex outflow tract reconstruction procedures,aorto-ventriculo-septolplasty (Konno–Rastan) [10], which require a right ventricular patch and a left ventricular outflow tract subannular patch, theseprocedures are generally reserved for children in whom one is attempting toplace an adult-size prosthesis.
Attempting to place a prosthesis that is too large creates multiple problems,including tearing of the aorta, distortion of the prosthesis with a flexible annu-lus or struts, impingement of the coronary arteries and the need to perform acomplex reconstruction or ultimately replace the valve with a smaller thanideal prosthesis. Generally safe and effective aortic valve replacement can beachieved with good patient selection, proper preoperative evaluation and an efficient, safe operation which provides relief of either aortic obstruction oraortic insufficiency. Even in the elderly, it is sometimes best to perform a slightly more complex operation to avoid one of the more disastrous com-plications which can occur or which might ultimately require placement of a less than ideal prosthesis.
Mitral valve surgery
AnatomyThe mitral valve is a bi-leaflet structure separating the left atrium from the leftventricle, allowing for the unidirectional flow of blood into the left ventricle.The base of the leaflets is attached at the annulus, a fibrous connection in continuity with a number of important structures, with the free edge andundersurface of the leaflets giving rise to primary and secondary chordae
Figure 18.5 (a) Aortic root enlargement with incision carried down to and through the annulus inthe non-coronary sinus. One does not necessarily need to extend this through the annulus on tothe mitral valve. (b) Reconstruction with elliptical piece of Dacron graft.
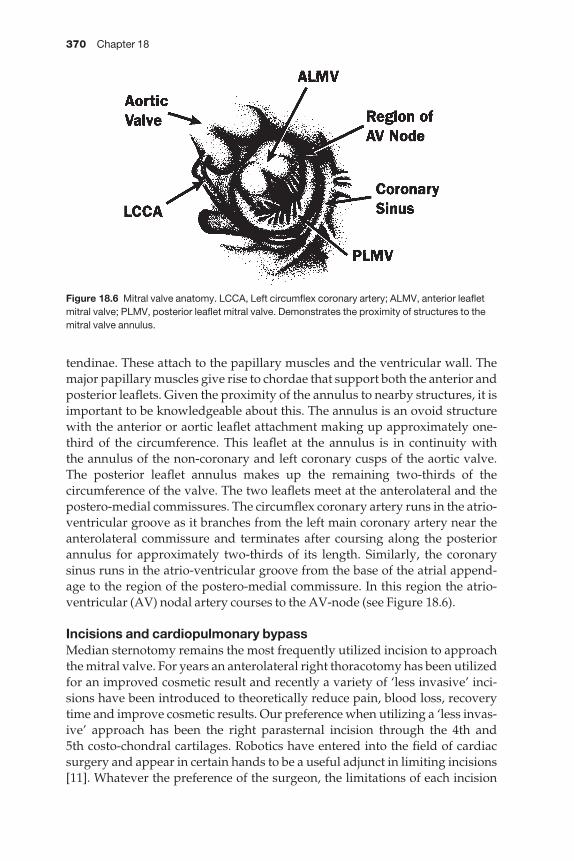
370 Chapter 18
tendinae. These attach to the papillary muscles and the ventricular wall. Themajor papillary muscles give rise to chordae that support both the anterior andposterior leaflets. Given the proximity of the annulus to nearby structures, it isimportant to be knowledgeable about this. The annulus is an ovoid structurewith the anterior or aortic leaflet attachment making up approximately one-third of the circumference. This leaflet at the annulus is in continuity with the annulus of the non-coronary and left coronary cusps of the aortic valve.The posterior leaflet annulus makes up the remaining two-thirds of the circumference of the valve. The two leaflets meet at the anterolateral and thepostero-medial commissures. The circumflex coronary artery runs in the atrio-ventricular groove as it branches from the left main coronary artery near theanterolateral commissure and terminates after coursing along the posteriorannulus for approximately two-thirds of its length. Similarly, the coronarysinus runs in the atrio-ventricular groove from the base of the atrial append-age to the region of the postero-medial commissure. In this region the atrio-ventricular (AV) nodal artery courses to the AV-node (see Figure 18.6).
Incisions and cardiopulmonary bypassMedian sternotomy remains the most frequently utilized incision to approachthe mitral valve. For years an anterolateral right thoracotomy has been utilizedfor an improved cosmetic result and recently a variety of ‘less invasive’ inci-sions have been introduced to theoretically reduce pain, blood loss, recoverytime and improve cosmetic results. Our preference when utilizing a ‘less invas-ive’ approach has been the right parasternal incision through the 4th and 5th costo-chondral cartilages. Robotics have entered into the field of cardiacsurgery and appear in certain hands to be a useful adjunct in limiting incisions[11]. Whatever the preference of the surgeon, the limitations of each incision
Figure 18.6 Mitral valve anatomy. LCCA, Left circumflex coronary artery; ALMV, anterior leafletmitral valve; PLMV, posterior leaflet mitral valve. Demonstrates the proximity of structures to themitral valve annulus.

Complications of valvular surgery 371
must be carefully weighed in preparation for anticipated surgery. Often multi-valve corrective procedures and concomitant coronary artery disease precludethe use of incisions other than a median sternotomy.
Exposure of the mitral valve dictates the type of venous cannulation for car-diopulmonary bypass. With a large left atrium, venous cannulation throughthe right atrial appendage with a two-stage single venous cannula and direct incision at the interatrial groove into the left atrium achieved (verticalleft atriotomy). This incision runs in front of the right pulmonary veins and can be extended safely under the inferior vena cava (IVC). It can also beextended under the superior vena cava (SVC), though it is more difficult to close this region safely. Incising the lateral pericardial attachments of thesuperior and inferior vena cavae, being careful to avoid the right phrenic nerveas it courses in a postero-lateral relation to the superior and inferior venacavae, is generally performed to assist in elevation of the heart. Careful dis-section to avoid thinning of the cavae is critical to avoid tears caused by retrac-tion. Occasionally exposure remains inadequate without vigorous retraction.Uncontrolled tearing of the atria or cavae should be avoided. One can place aright angle cannula in the SVC with a caval tourniquet, replace the two-stagesingle venous cannula with an IVC cannula and caval tourniquet and thentransect the SVC about 1 cm above the SVC and right atrial junction. Whenplacing the SVC tourniquet one should dissect in the plane between the anter-ior surface of the right pulmonary artery and SVC to avoid damage to the azygous vein. This gives excellent exposure to the mitral valve. Alternatively,the valve can be approached through the dome of the left atrium utilizing atwo-stage single venous cannula, though this does require more mobilizationof the aorta as one enters the left atrium between the aorta and SVC and right atrium (superior approach). Calcification of the ascending aorta is a contraindication to this approach given the need for retraction of the aorta andaortic valve, and there is some increased risk of damage to the sinus nodeartery with atrial dysrhythmias.
Bi-caval cannulation with caval tourniquets is employed for patients withnormal or small atria. Cannulation of the SVC is direct to give more roomwithin the right atrium to work with cannulation of the IVC low in the rightatrium. Exposure of the valve is through the right atrium, the fossa ovalis andthe atrial septum (trans-septal approach). The incision in the septum is verticaland extended to the lower edge of the fossa, avoiding the coronary sinus andsuperiorly into the septum. The roof of the left atrium under the aorta can beavoided. Most repairs and replacements can be performed without extendingthe incision outside of the confines of the septum (see Figure 18.7). Use of two small retractors works well to avoid tearing of the septal incision. Closure of the septum and right atrium as separate incisions with a runningmonofilament suture is straightforward. Cardioplegia can be administereddirectly into the coronary sinus. A vent is generally placed through the rightsuperior pulmonary vein down into the left atrium. The right atrial closure canbe achieved while rewarming after cross clamp removal and after removal of
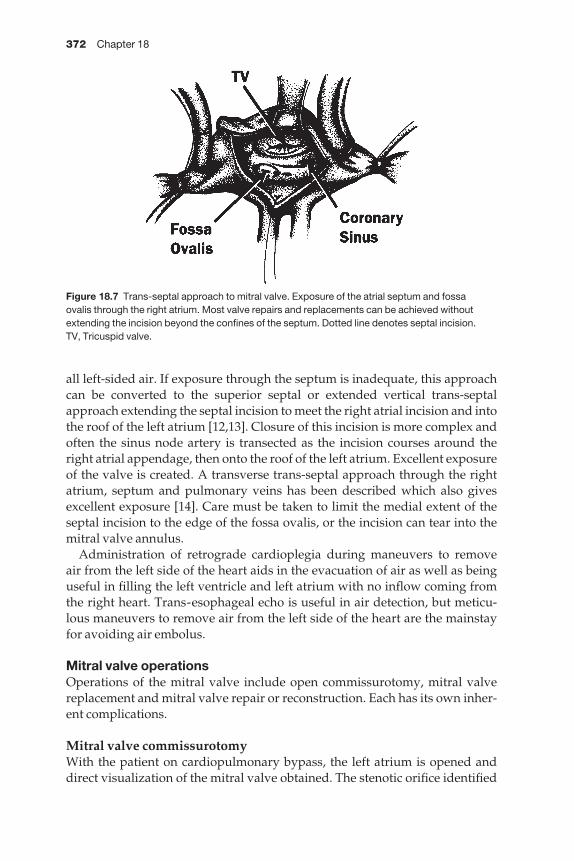
372 Chapter 18
all left-sided air. If exposure through the septum is inadequate, this approachcan be converted to the superior septal or extended vertical trans-septalapproach extending the septal incision to meet the right atrial incision and intothe roof of the left atrium [12,13]. Closure of this incision is more complex andoften the sinus node artery is transected as the incision courses around theright atrial appendage, then onto the roof of the left atrium. Excellent exposureof the valve is created. A transverse trans-septal approach through the rightatrium, septum and pulmonary veins has been described which also givesexcellent exposure [14]. Care must be taken to limit the medial extent of theseptal incision to the edge of the fossa ovalis, or the incision can tear into themitral valve annulus.
Administration of retrograde cardioplegia during maneuvers to remove air from the left side of the heart aids in the evacuation of air as well as beinguseful in filling the left ventricle and left atrium with no inflow coming fromthe right heart. Trans-esophageal echo is useful in air detection, but meticu-lous maneuvers to remove air from the left side of the heart are the mainstayfor avoiding air embolus.
Mitral valve operationsOperations of the mitral valve include open commissurotomy, mitral valvereplacement and mitral valve repair or reconstruction. Each has its own inher-ent complications.
Mitral valve commissurotomyWith the patient on cardiopulmonary bypass, the left atrium is opened anddirect visualization of the mitral valve obtained. The stenotic orifice identified
Figure 18.7 Trans-septal approach to mitral valve. Exposure of the atrial septum and fossa ovalis through the right atrium. Most valve repairs and replacements can be achieved withoutextending the incision beyond the confines of the septum. Dotted line denotes septal incision. TV, Tricuspid valve.
Complications of valvular surgery 373
as well as the fused commissures. The fusion point is incised with a #15 scalpelprotecting the underlying chordae and papillary muscles which may be fusedand foreshortened below with a right angle clamp. One must avoid extendingthe commissurotomy through the annulus and serial testing of the valve mustbe performed to avoid creating severe insufficiency. To gain increased mobil-ity of the valve leaflets one often has to split chordae which are fused. This attimes also involves splitting partially the papillary muscle. If significant mitralinsufficiency is created, early valve replacement should be considered, thoughif the leaflets are pliable, a mitral valve reparative procedure may be possible.Generally, if extensive debridement of calcium from the leaflets and annulus isrequired to achieve a commissurotomy, the patient is best served by replace-ment of the valve with chordal preservation.
Mitral valve replacementRemoval of the mitral valve for replacement begins with downward tractionon the mid portion of the anterior leaflet with either a stay suture or an Allisclamp. The valve is incised 2–3 mm from the true annulus. Utilizing theremaining leaflet as traction, the anterior annulus is exposed well and valvesutures can be placed serially as one removes the remainder of the leaflet. If theentire leaflet is removed prior to placement of valve sutures it is sometimesdifficult to visualize well the anterior annulus without undue upward traction.Our practice has been to place the sutures from the ventricular side up throughthe annulus utilizing pledgeted horizontal mattress sutures of 2–0 Dacron(Ticron®) suture. These sutures are placed a few millimeters apart. Once thecommissures are reached, a decision can be made whether or not to attemptchordal preservation. In most cases, the posterior leaflet tissue can be left inplace, except in valves that are heavily calcified or severely scarred and fore-shortened. One must remove or reposition most of the anterior leaflet tissueprior to suturing in the valve, otherwise it is likely that systolic anterior motion(SAM) of the anterior leaflet and left ventricular outflow tract obstruction candevelop, particularly with the use of a bioprosthetic valve. Anterior chordalpreservation must be performed precisely to avoid interference with propervalve function. This is particularly important when utilizing a mono-leafletmechanical prosthesis. Care must be taken to avoid bunching of tissue at theannulus which may protrude below the annulus of the prosthetic valve. If oneelects not to preserve the anterior chordae, they should be transected flushwith the papillary muscle tip to avoid interference with proper valve function.Over-zealous traction on the valve leaflets still attached to papillary musclescan tear the posterior ventricular wall, creating a muscular defect which is often difficult to close but must be recognized immediately. This requiresdeep ventricular sutures of pledgeted 2–0 Dacron avoiding the nearby coron-ary arteries, particularly the posterior descending artery for a postero-medialpapillary muscle tear.
To achieve adequate valve seating it is often necessary to remove annularcalcium. In general this calcification involves the posterior leaflet more heavily

374 Chapter 18
than the anterior leaflet, and sometimes spreads into the posterior ventricularwall. Great care must be taken to avoid losing debris as one removes thecalcifications into either the left atrium, pulmonary veins, or left ventricle.Again vigorous irrigation and immediately accounting for any debris are the mainstay of avoiding calcific emboli. Over-aggressive debridement of theannulus and calcifications may result in a significant defect separating the left ventricle from the left atrium (atrio-ventricular discontinuity), ventricularrupture or atrial dissection. Resultant atrio-ventricular groove hematoma,pseudoaneurysm and posterior rupture have been described [15–18]. This isrepaired with pledgeted sutures brought from below beginning in the ventri-cular muscle up through the atrial wall at the level of the annulus. The suturesultimately can be utilized to anchor the valve (see Figure 18.8). Preservation ofboth the valvular and subvalvular apparatus reduces the risk of ventricularrupture [19]. Both the circumflex coronary artery and coronary sinus are atsome risk if a large defect has been created. Great care most be taken to avoiddamaging these structures during reconstruction, which may require revascu-larization of the circumflex system. At times it is more prudent to leave cal-cium in place, utilizing large needles to go around the calcific deposits, or onecan place the valve inside the calcified annulus taking smaller bites of primar-ily valvular tissue and using a smaller prosthesis. To circumvent the problemof an uneven surface on which the valve must sit, a strip of Teflon felt can be fashioned and sandwiched between the prosthetic valve ring and annulartissue. This allows one to seat the valve on a very irregular surface without the need for extensive debridement. When placing sutures in or around the annulus the anatomic structures in close proximity must always be kept inmind (see Anatomy). Creating aortic insufficiency because of anterior annularsutures placed too deeply or myocardial infarction secondary to circumflexartery damage should not occur.
With bioprostheses, the valve should be orientated to avoid positioning astrut directly posterior. Leaving posterior leaflet tissue in place has reduced
Figure 18.8 Mitral valve replacement. Atrio-ventricular discontinuity caused byremoval of calcium from the posterior annulusof the mitral valve. This can be repaired with pledgeted sutures brought up throughventricular muscle, annular and left atrialtissue. Sutures can be used to anchor theprosthesis or annuloplasty ring.

Complications of valvular surgery 375
the rare complication of posterior ventricular rupture secondary to strut pro-trusion. It is still recommended to orientate the valve with one of the struts at the 4 : 00 position and the second at the 8 : 00 with the third strut directlyanterior at the 12 : 00 position. This also avoids the complication of strutobstruction anteriorly of the left ventricular outflow tract. Bi-leaflet mechan-ical valves are orientated with the hinges at the 12 : 00 and 6 : 00 positions.Mono-leaflet valves are orientated with the major orifice opening anteriorly.Most mechanical valves can now be rotated within the sewing ring and unre-stricted leaflet motion tested in virtually any position. Chordal preservationmust be precise to avoid interference with mechanical valve function. Excesstissue sutured at the annulus may prevent proper leaflet excursion.
Hemorrhage or hematoma in the atrio-ventricular groove on the posterioraspect of the heart represents posterior ventricular rupture and must be dealt with immediately by removal of the prosthesis, repair of the defect withsutures buttressed with Teflon, and then re-replacement of the valve. The incidence of ventricular rupture with mitral valve replacement is 0.5%. Izzat[20] described three influences together which are necessary to produce a vent-ricular rupture: a predisposition by an underlying weakened myocardium, i.e. inferior infarction, factors that may initiate this primary tear which includedebridement of calcium, and dynamic forces which include immediate periop-erative hypertension and left ventricular strain. Clearly all of these increase therisk of this complication, which in various series has carried a 75% mortalityrate. Most survivors of this complication were recognized in the operatingroom at the time of the initial valve replacement.
Prior to tying down the bioprosthetic valve but after seating of the valve, oneshould inspect the valve struts to be sure that none of the sutures has becomeentangled on the struts. If the struts cannot be well visualized, often a smalldental mirror will expedite the process. A suture entangled in a strut will resultin both central valve insufficiency and a paravalvular leak.
If a vent is utilized and after tying the valve, the vent is moved from its posi-tion in the left atrium across the valve prosthesis. For a bi-leaflet mechanicalprosthesis, it should be placed across the central orifice. For a mono-leafletmechanical valve it should be placed across the minor orifice to avoid the complication of closure of the valve on the vent and forces that will not allowthe vent to be removed. Internal closure of the left atrial appendage is re-commended with either a purse-string suture or a double running over andover suture, being careful not to take a deep bite which could compromise thecircumflex coronary artery. As the left atrium is being closed, meticulousmaneuvers to remove air from the left side of the heart must be performedprior to aortic cross clamp removal. Simultaneously aspirating from the leftventricular vent and the ascending aorta, one should be able to evacuate all ofthe air. Once the cross clamp is removed, one should avoid over-distension ofthe left ventricle by controlling the vent volume until the heart begins to beat.
For combined aortic and mitral valve surgery one should always repair or replace the mitral valve first to avoid retraction and damage to the aorta or

376 Chapter 18
the aortic valve prosthesis caused by retraction to expose the mitral valve.Similarly, if coronary bypasses are to be performed, particularly those to the circumflex system, these should be performed prior to either mitral valverepair or replacement or aortic valve replacement. One should avoid lifting the heart once the prosthesis is in place, which can cause posterior ventricularrupture.
Mitral valve reparative procedureValve repair or valvuloplasty for mitral insufficiency vs. valve replacementunder appropriate circumstances is the operation of choice, with a decrease inboth long-term thromboembolic complications and mortality when properlyreconstructed [21]. The experience of the surgeon dictates valve replace-ment vs. valve repair because of the potential for leaving significant mitralinsufficiency or creating mitral stenosis when not performed adequately.Though reconstructive procedures can be done through any of the previouslydescribed approaches, adequate visualization is critical for successful recon-struction. It is also best to visualize the valve without excessive retraction,which may distort the valve. Preoperative and intraoperative assessment of the pathology with trans-esophageal echocardiography is often helpful in dictating the type of repair, and necessary after completion to assess forresidual mitral insufficiency, mitral stenosis or systolic anterior motion of the mitral valve with left ventricular outflow tract obstruction, all of whichconditions require correction prior to leaving the operating room.
Numerous techniques have been described to reduce the length of the poster-ior annulus, which is almost always increased relative to the anterior leafletwhen mitral insufficiency is encountered. Figure-of-eight sutures placedevenly on each side of the posterior annulus just below the commissures oftensuffice to eliminate mitral regurgitation. A ‘Kay-Reed’ measured annuloplastyplicating the posterior leaflets at the commissures has been used for years and is a simple, safe and effective technique when posterior annular dilatationis the pathology [22,23]. Though acutely quite effective since the entire posterior annulus is not supported by the repair, there is the potential for pro-gressive posterior annular dilatation and recurrence of mitral insufficiencyover time. Additionally, because of the height of the posterior leaflet tissue,there is the potential for causing systolic anterior motion of the anterior leaflet of the mitral valve and left ventricular outflow tract obstruction. If the height of the posterior leaflet with any of the reconstructive procedures is > 1 cm, one must consider plication of the posterior leaflet to prevent thiscomplication.
One of the commonest indications for mitral valve repair is mitralinsufficiency secondary to a myxomatous valve plus or minus ruptured chordae to the posterior leaflet. The anatomy can be well delineated withechocardiography preoperatively, and although patients with severe mitralinsufficiency may initially tolerate it well, their long-term prognosis is poorand a mitral valve reconstructive procedure is generally indicated [24].
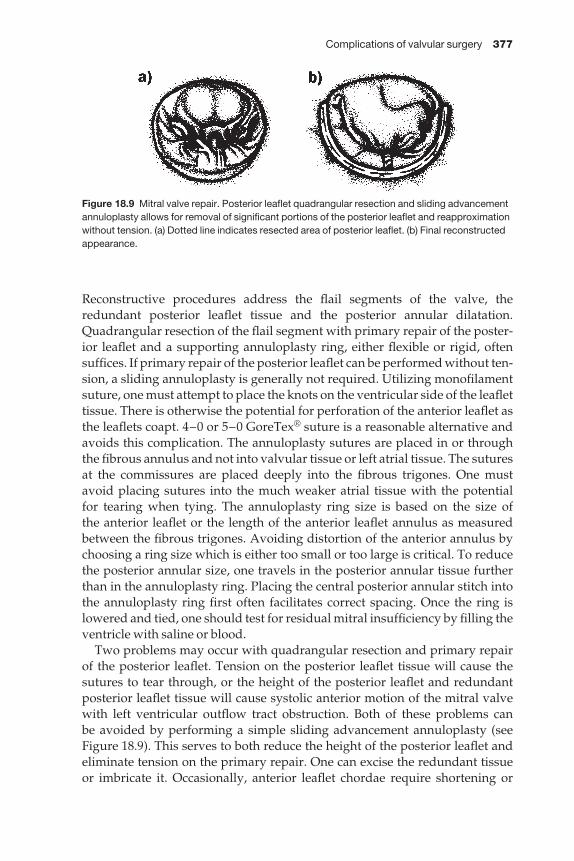
Complications of valvular surgery 377
Reconstructive procedures address the flail segments of the valve, the redundant posterior leaflet tissue and the posterior annular dilatation.Quadrangular resection of the flail segment with primary repair of the poster-ior leaflet and a supporting annuloplasty ring, either flexible or rigid, oftensuffices. If primary repair of the posterior leaflet can be performed without ten-sion, a sliding annuloplasty is generally not required. Utilizing monofilamentsuture, one must attempt to place the knots on the ventricular side of the leaflettissue. There is otherwise the potential for perforation of the anterior leaflet asthe leaflets coapt. 4–0 or 5–0 GoreTex® suture is a reasonable alternative andavoids this complication. The annuloplasty sutures are placed in or throughthe fibrous annulus and not into valvular tissue or left atrial tissue. The suturesat the commissures are placed deeply into the fibrous trigones. One mustavoid placing sutures into the much weaker atrial tissue with the potential for tearing when tying. The annuloplasty ring size is based on the size of the anterior leaflet or the length of the anterior leaflet annulus as measuredbetween the fibrous trigones. Avoiding distortion of the anterior annulus bychoosing a ring size which is either too small or too large is critical. To reducethe posterior annular size, one travels in the posterior annular tissue furtherthan in the annuloplasty ring. Placing the central posterior annular stitch intothe annuloplasty ring first often facilitates correct spacing. Once the ring islowered and tied, one should test for residual mitral insufficiency by filling theventricle with saline or blood.
Two problems may occur with quadrangular resection and primary repairof the posterior leaflet. Tension on the posterior leaflet tissue will cause thesutures to tear through, or the height of the posterior leaflet and redundantposterior leaflet tissue will cause systolic anterior motion of the mitral valvewith left ventricular outflow tract obstruction. Both of these problems can be avoided by performing a simple sliding advancement annuloplasty (seeFigure 18.9). This serves to both reduce the height of the posterior leaflet andeliminate tension on the primary repair. One can excise the redundant tissue or imbricate it. Occasionally, anterior leaflet chordae require shortening or
Figure 18.9 Mitral valve repair. Posterior leaflet quadrangular resection and sliding advancementannuloplasty allows for removal of significant portions of the posterior leaflet and reapproximationwithout tension. (a) Dotted line indicates resected area of posterior leaflet. (b) Final reconstructedappearance.

378 Chapter 18
even replacement. Excellent visualization is a prerequisite. Fine sutures placedthrough the chordae at about 1/2 of the distance required for shortening areplaced. The papillary muscle is carefully split and the chordae imbricated.Small pledgets avoid cutting of suture into muscular tissue. Too deep a bite inthe papillary muscle and tying the suture too tightly may cause necrosis of themuscle with resultant tip necrosis, detachment and severe mitral insufficiency.If there are multiple anterior leaflet chordae which are elongated, thoughrepair may be possible, resection and primary repair of the anterior leaflet isgenerally not advocated. Since the anterior leaflet is responsible for most of thecompetency of the valve, one must be extremely careful when considering this.Replacement is generally indicated, though occasionally small segments of theanterior leaflet can be repaired utilizing posterior leaflet chordae (the flip-overtechnique) [25].
Mitral stenosis can be created in the repair of mitral insufficiency by choos-ing an annuloplasty ring which is too small or by failing to recognize that the leaflet tissue is thickened or stiff secondary to rheumatic heart disease.Intraoperative trans-esophageal echocardiography at the end of the reparativeprocedure is mandatory, and though often fixated on the small residual jet of mitral insufficiency, one must be alert for mitral stenosis and check appro-priate velocities. If mitral stenosis is created, reinstituting cardiopulmonarybypass and correction are performed, which require removal of the annulo-plasty ring, resizing and occasionally replacement of the valve.
Systolic anterior motion of the mitral valve causing left ventricular outflowtract obstruction has been described with rigid and flexible annuloplasty rings,though more commonly with rigid rings [26]. Redundant anterior and poster-ior leaflet tissue as well as a large annulus, a bulging septum, a narrow mitral-aortic angle, a non-dilatated hyperdynamic LV and anteriorly displaced mitralcoaptation line are predispositions. One can often avoid this by replacing arigid ring with a flexible ring, shortening the anterior leaflet chordae, reduc-ing the height of the posterior leaflet, or by some combination of these. Ourpractice has been to eliminate posterior leaflet height as a cause by always performing a height-reducing sliding advancement annuloplasty when theheight of the posterior leaflet is > 1 cm, as well as by always utilizing a flexibleannuloplasty ring.
With any of the mitral valve replacement or reparative procedures, low cardiac output can occur. A variety of factors may be causative, includinglong-standing disease with impaired left ventricular function, marginalmyocardial protection, coronary insufficiency with previous infarction, as wellas the importance of maintaining both left and right ventricular geometry bypreservation of the chordal-papillary muscle continuity [19]. Clearly posteriorleaflet preservation can be achieved in most cases. Numerous techniques to preserve anterior continuity have been described [27–29]. Understandingthe complex physiology, anatomy, and techniques, and awareness of the pre-ventable complications, will allow for the safe conduct of mitral valve surgeryand improvement in both the quality and quantity of life for patients.
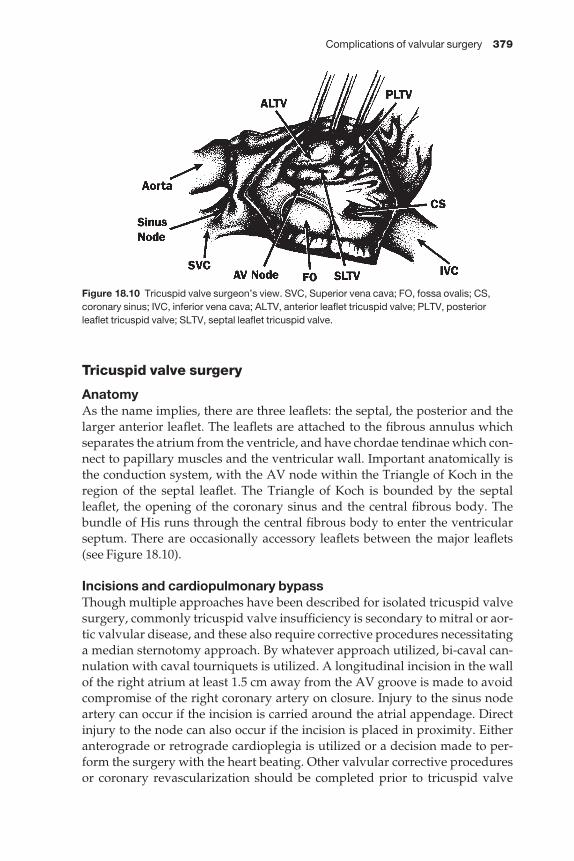
Complications of valvular surgery 379
Tricuspid valve surgery
AnatomyAs the name implies, there are three leaflets: the septal, the posterior and thelarger anterior leaflet. The leaflets are attached to the fibrous annulus whichseparates the atrium from the ventricle, and have chordae tendinae which con-nect to papillary muscles and the ventricular wall. Important anatomically isthe conduction system, with the AV node within the Triangle of Koch in theregion of the septal leaflet. The Triangle of Koch is bounded by the septalleaflet, the opening of the coronary sinus and the central fibrous body. Thebundle of His runs through the central fibrous body to enter the ventricularseptum. There are occasionally accessory leaflets between the major leaflets(see Figure 18.10).
Incisions and cardiopulmonary bypassThough multiple approaches have been described for isolated tricuspid valvesurgery, commonly tricuspid valve insufficiency is secondary to mitral or aor-tic valvular disease, and these also require corrective procedures necessitatinga median sternotomy approach. By whatever approach utilized, bi-caval can-nulation with caval tourniquets is utilized. A longitudinal incision in the wallof the right atrium at least 1.5 cm away from the AV groove is made to avoidcompromise of the right coronary artery on closure. Injury to the sinus nodeartery can occur if the incision is carried around the atrial appendage. Directinjury to the node can also occur if the incision is placed in proximity. Eitheranterograde or retrograde cardioplegia is utilized or a decision made to per-form the surgery with the heart beating. Other valvular corrective proceduresor coronary revascularization should be completed prior to tricuspid valve
Figure 18.10 Tricuspid valve surgeon’s view. SVC, Superior vena cava; FO, fossa ovalis; CS,coronary sinus; IVC, inferior vena cava; ALTV, anterior leaflet tricuspid valve; PLTV, posteriorleaflet tricuspid valve; SLTV, septal leaflet tricuspid valve.

380 Chapter 18
reconstruction. Often the surgeon elects to repair the tricuspid valve whilerewarming and after the aortic cross clamp has been removed. The atrial inci-sion is closed with a single layer of a 4–0 monofilament suture utilizing aninverting horizontal mattress suture technique which avoids troublesomebleeding from a thin atrial wall.
Tricuspid valve repairGenerally tricuspid valve insufficiency results from secondary enlargement of the right ventricle and annulus, with correction primarily restoring theannular dimensions. A reparative procedure should be entertained when-ever moderate insufficiency is documented or if there is significant right vent-ricular enlargement without severe right ventricular dysfunction or severeirreversible pulmonary hypertension given the likelihood of progressiveinsufficiency.
DeVega annuloplastyWith the valve exposed a pledgeted double armed 2–0 monofilament suture is begun in the annulus at the posterior-septal leaflet commissure, with bites taken in the annulus every 5 mm to encircle the valve to the region of theanterior-septal commissure. Tension on the valve with a nerve hook oftenhelps to identify the annular tissue. The other end of the suture is placed sim-ilarly, resulting in a double row of sutures encircling the annulus but avoidingthe septal leaflet. The suture is then tied over pledgets plicating the annulus. Aprosthetic valve sizer can be placed when tying to prevent over-tightening ofthe annuloplasty repair. It is important to incorporate the fibrous annulus intothe suture line, otherwise the suture will tear out of the thin valve tissue andweak atrial tissue. This repair avoids placing sutures along the septal leafletand the potential damage to the AV node and conduction system. There havebeen variable reports of both excellent and at times only moderate long-termsuccess with this procedure [30].
Bicuspidization (Kay)Another technique is plication of the posterior leaflet with either figure-of-eight sutures or pledgeted mattress sutures placed at the posterior-septalleaflet commissure and the posterior-anterior leaflet commissure to essentiallyeliminate the posterior leaflet [31]. Results with this technique are variable.However, it has the advantage of avoiding the septal leaflet and the potentialfor conduction disturbances, and is a simple technique which can be added to acomplex multivalve procedure without significantly increasing morbidity.
Carpentier–Edwards annuloplastyThis repair is designed to plicate the posterior leaflet and commissures with a semirigid ring which is open along a portion of the septal leaflet to avoidplacing sutures near the conduction system (see Figure 18.11). With the valveexposed the ring is sized by either measuring the septal annulus or by using
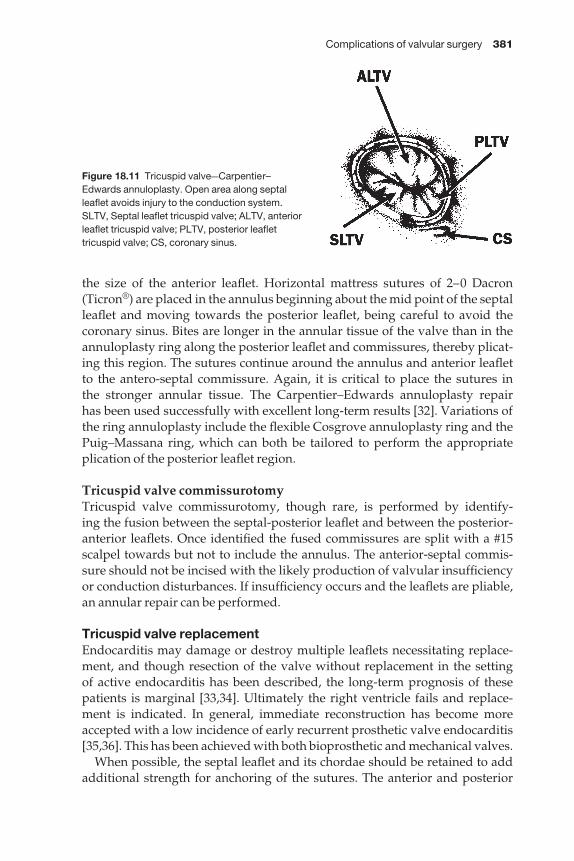
Complications of valvular surgery 381
the size of the anterior leaflet. Horizontal mattress sutures of 2–0 Dacron(Ticron®) are placed in the annulus beginning about the mid point of the septalleaflet and moving towards the posterior leaflet, being careful to avoid thecoronary sinus. Bites are longer in the annular tissue of the valve than in theannuloplasty ring along the posterior leaflet and commissures, thereby plicat-ing this region. The sutures continue around the annulus and anterior leaflet to the antero-septal commissure. Again, it is critical to place the sutures in the stronger annular tissue. The Carpentier–Edwards annuloplasty repair has been used successfully with excellent long-term results [32]. Variations ofthe ring annuloplasty include the flexible Cosgrove annuloplasty ring and thePuig–Massana ring, which can both be tailored to perform the appropriate plication of the posterior leaflet region.
Tricuspid valve commissurotomyTricuspid valve commissurotomy, though rare, is performed by identify-ing the fusion between the septal-posterior leaflet and between the posterior-anterior leaflets. Once identified the fused commissures are split with a #15scalpel towards but not to include the annulus. The anterior-septal commis-sure should not be incised with the likely production of valvular insufficiencyor conduction disturbances. If insufficiency occurs and the leaflets are pliable,an annular repair can be performed.
Tricuspid valve replacementEndocarditis may damage or destroy multiple leaflets necessitating replace-ment, and though resection of the valve without replacement in the setting of active endocarditis has been described, the long-term prognosis of thesepatients is marginal [33,34]. Ultimately the right ventricle fails and replace-ment is indicated. In general, immediate reconstruction has become moreaccepted with a low incidence of early recurrent prosthetic valve endocarditis[35,36]. This has been achieved with both bioprosthetic and mechanical valves.
When possible, the septal leaflet and its chordae should be retained to addadditional strength for anchoring of the sutures. The anterior and posterior
Figure 18.11 Tricuspid valveaCarpentier–Edwards annuloplasty. Open area along septalleaflet avoids injury to the conduction system.SLTV, Septal leaflet tricuspid valve; ALTV, anteriorleaflet tricuspid valve; PLTV, posterior leaflettricuspid valve; CS, coronary sinus.

382 Chapter 18
leaflets and chordae are then resected to the papillary muscles. Placement of aprosthesis generally requires annular plication which is performed primarilyalong the anterior and posterior leaflets. Sutures can be placed from eitherabove or below the annulus. We have utilized pledgeted 2–0 Dacron suturesplacing the pledgets below the annulus on the ventricular side. This is particu-larly useful when portions of the septal leaflet can be left in place to buttress theannulus and avoid placing sutures too deeply, potentially damaging the AVnode and conduction system. Given the large size of the ventricle, it is unlikelythat the struts of a bioprosthesis will impinge on the ventricular muscle or that mechanical valve leaflet excursion will be affected. Suturing at the antero-septal commissure must be precise to avoid a paravalvular leak and damage tothe conduction system. There have been numerous reports of mechanicalvalve thrombosis, particularly involving tilting disc valves [37–39]. For thatreason, except in the very young patient, bioprosthetic valves have become the valve of choice, with a lower propensity to thrombosis and the theoreticaladvantage of increased longevity in a low-pressure system.
Prognosis with tricuspid valve repair or replacement is often dictated by the left-sided lesion and the potential for pulmonary hypertension reversal. At times, however, with a corrected left-sided lesion, tricuspid valve insuffici-ency and right ventricular failure persist and progress despite a reduction in pulmonary hypertension. There are, unfortunately, no reliable tests to determine if right ventricular failure will improve with valve repair or replace-ment in patients with progressive symptoms of right heart failure and tricuspid insufficiency. Echocardiographic improvement of right ventricularfunction with intensive medical therapy as well as clinical improvement withintensive medical therapy may be our best guide. Obviously, it is critical for the cardiac surgeon to understand the anatomy, physiology and potentialcorrective procedures of the tricuspid valve so that he may employ them under appropriate circumstances in the management of complex heart surgerypatients.
References
1 Gundry SR, Shattuck OH, Razzouk AJ et al. Facile minimally invasive cardiac surgery viaministernotomy. Ann Thorac Surg 1998; 65: 1100–1104.
2 Nair RU, Sharpe DA. Minimally invasive reversed Z sternotomy for aortic valve replace-ment. Ann Thorac Surg 1998; 65: 1165–1166.
3 Svensson LG, D’Agostino RS. Minimal-access aortic and valvular operations, includingthe ‘J/j’ incision. Ann Thorac Surg 1998; 66: 431–435.
4 Olin CL, Peterffy A. Minimal access aortic valve surgery. Eu J Cardiothorac Surg 1999; 15(Suppl.): S32–S38.
5 Byrne JG, Aranki SF, Cohn LH. Aortic valve operations under deep hypothermic cir-culatory arrest for the porcelain aorta: ‘no-touch’ technique. Ann Thorac Surg 1998; 65:1313–1315.
6 Angell WW, Pupello DF, Bessone LN. Universal method for insertion of unstented aorticautografts, homografts, and xenografts. J Thorac Cardiovasc Surg 1992; 103: 642–648.
Complications of valvular surgery 383
7 Khonsari S. Cardiac Surgery Safeguards and Pitfalls in Operative Technique. Rockville, MD:Aspen Publishers, Inc., 1988.
8 Tomasco B, Di Natale M, Minale C. Coronary ostial stenosis after aortic valve replace-ment. Ital Heart J 2002; 3: 133–136.
9 Nicks R, Cartmill T, Bernstein L. Hypoplasia of the aortic root: the problem of aortic valvereplacement. Thorax 1970; 25: 339–346.
10 Roughneen PT, Deleon SY, Cetta F et al. Modified Konno-Rastan procedure for subaorticstenosis: indications, operative techniques, and results. Ann Thorac Surg 1998; 65:1368–1375.
11 Jacobs S, Falk V. Pearls and pitfalls: lessons learned in endoscopic robotic surgeryathe daVinci experience. Heart Surg Forum 2001; 4: 3007–3110.
12 Masiello P, Triumbari F, Leone R et al. Extended vertical transseptal approach vs. conven-tional left atriotomy for mitral valve surgery. J Heart Valve Dis 1999; 8: 440–444.
13 Guiraudon GM, Ofiesh JG, Kaushk R. Extended verticle transatrial septal approach to themitral valve. Ann Thorac Surg 1991; 52: 1058–1060.
14 Brawley RK. Improved exposure of the mitral valve in patients with a small left atrium.Ann Thorac Surg 1980; 29: 179–181.
15 Cheng LC, Chiu CS, Lee JW. Left ventricular rupture after mitral valve replacement. J Cardiovasc Surg 1999; 40: 339–342.
16 El Asmar B, Acker M, Couetil JP et al. Mitral valve repair in the extensively calcified mitralvalve annulus. Ann Thorac Surg 1991; 52: 66–69.
17 Craver JM, Jones EL, Guyton RA et al. Avoidance of transverse midventricular disruptionfollowing mitral valve replacement. Ann Thorac Surg 1985; 40: 163–171.
18 Giovanni R, Speziale G, Voci P et al. ‘Patch-Glue’ annular reconstruction for mitral valvereplacement in severely calcified mitral annulus. Ann Thorac Surg 1997; 63: 570–571.
19 Le Tourneau T, Grandmougin D, Foucher C et al. Anterior chordal transection impairs notonly regional left ventricular function but also impairs right ventricular function in mitralregurgitation. Circulation 2001; 104 (Suppl. I): 41–46.
20 Izzat MB, Smith GH. Rupture of the left ventricle after mitral valve repair: case report andnew technique of repair. Br Heart J 1993; 69: 366–367.
21 Onnasch JF, Scheider F, Mierzwa M. Mitral valve repair vs. mitral valve replacement. ZKardiol 2001; 90: 75–80.
22 Kay GL, Kay JH, Zubiate P et al. Mitral valve repair for mitral regurgitation secondary tocoronary artery disease. Circulation 1996; 74: I–88.
23 Reed GE, Tice DA, Clauss RH. Asymmetric exaggerated mitral annuloplasty: repair ofmitral insufficiency with hemodynamic predictability. J Thor Cardiovasc Surg 1965; 49: 752.
24 Reul RM, Cohn LH. Mitral valve reconstruction for mitral insufficiency. Prog CardiovascDis 1997; 39: 567–599.
25 El-Khoury G, Noirhomme P, Verhelst R et al. Surgical repair of the prolapsing anteriorleaflet in degenerative mitral valve disease. J Heart Valve Dis 2000; 9: 75–80.
26 Shah PM, Raney AA. Echocardiographic correlates of ventricular outflow obstruction andsystolic anterior motion following mitral valve repair. J Heart Valve Dis 2001; 10: 302–306.
27 Smedira NG, Selman R, Cosgrove DM et al. Repair of anterior leaflet prolapse: chordaltransfer is superior to chordal shortening. J Thorac Carciovasc Surg 1996; 112: 287–292.
28 Timek TA, Nielsen SL, Green GR et al. Influence of anterior mitral leaflet second orderchordae on leaflet dynamics and valve competence. Ann Thorac Surg 2001; 72: 535–541.
29 Moon MR, DeAnda A, Daughters GT et al. Experimental evaluation of different chordalpreservation methods during mitral valve replacement. Ann Thorac Surg 1994; 58:931–944.
384 Chapter 18
30 Chidamgaram M, Abdulai SA, Baliga BG. Long-term results of DeVega tricuspid annulo-plasty. Ann Thorac Surg 1987; 43: 185–188.
31 Kay JH, Mendez AM, Zubiate P. A further look at tricuspid annuloplasty. Ann Thor Surg1976; 22: 498.
32 Cohn LH. Tricuspid regurgitation secondary to mitral valve disease: when and how torepair. J Card Surg 1994; 9 (Suppl. 2): 37–41.
33 Nihoyannopoulos P. Tricuspid valvectomy following tricuspid valve endocarditis in anintravenous drug addict. Heart 2001; 86: 144.
34 Couie EK, Lin SS, Reynetson SI et al. Pressure and volume loading of the right ventriclehave opposite effects on left ventricular ejection fraction. Circulation 1995; 92: 819–824.
35 Katsumata T, Westaby S. Mitral homograft replacement of the tricuspid valve for endo-carditis. Ann Thorac Surg 1997; 63: 1480–1482.
36 Tanaka M, Abe T, Hosokawa S et al. Tricuspid valve candida endocarditis cured by valvesparing debridement. Ann Thorac Surg 1989; 48: 857–858.
37 Thorburn CW, Morgan JJ, Shanahan MX. Long-term results of tricuspid valve replace-ment and the problem of prosthetic valve thrombosis. Am J Cardiol 1983; 51: 1128–1132.
38 Boskovic D, Elezovic J, Boskovic D. Late thrombosis of the Bjork-Shiley tilting disc valve inthe tricuspid position: thrombolytic treatment with streptokinase. J Thorac Cardiovasc Surg1986; 91: 1–8.
39 Shapira Y, Nili M, Hirsch R et al. Mid term clinical and echocardiographic follow up ofpatients with CarboMedics valves in the tricuspid position. J Heart Valve Dis 2000; 9:396–402.

CHAPTER 19
Postpericardiotomy syndrome
William A. Gay Jr
Postpericardiotomy syndrome (PPS) is an illness, which occurs after anintrapericardial intervention, and is characterized by fever, malaise andpleuro-pericardial pain. The condition usually has its onset in the second orthird week after surgery, and is often accompanied by a pericardial and/orpleural friction rub. The incidence of PPS has been reported between 10 and60% following intrapericardial surgery [1–7], but the condition is uncommonin children less than 2 years of age [8]. An identical illness has been reported tooccur in some patients following acute myocardial infarction [9]. Some authorsnow refer to the condition as post cardiac injury syndrome [5].
PPS was first described in association with closed mitral valvotomy, occur-ring in 30% of patients [10]. Initially, clinicians felt that the symptom complexrepresented a recurrence of acute rheumatic fever in the postoperative period[11]. These observers noted that the syndrome typically had its onset duringthe second week after surgery, and described the pain as pleuropericardial, inthat it was aggravated by ‘swallowing and change of position’. They alsonoted that about 5% of the afflicted patients developed a small pleural effu-sion. Today, PPS is most commonly seen following cardiac surgery using car-diopulmonary bypass, but it has also been reported after epicardial pacemakerlead placement [12,13], percutaneous transluminal coronary angioplasty [14],RF ablation of accessory conduction pathways [15] and following insertion oftransvenous pacemaker leads [16,17].
When PPS was described in patients without prior rheumatic fever [18], andwhen no evidence of rheumatic activity could be found in these patients[19–21] the theory of a rheumatic etiology was discarded. Similarly, although a relationship was seen between PPS and viral illness [8], there has been no evidence of an infectious etiology [22]. The thinking in this regard is that theviral illness may condition the immune system so that the trauma associatedwith cardiac surgery results in the development of antibodies against themyocardium. The presence of these heart-reactive antibodies correlates wellwith other manifestations of the syndrome [23,24]. These antibodies aredirected against both the sarcolemma (IgG) and the myofibrils (IgM) [24]. Thisantigen–antibody activity, along with the circulating immune complexes, produces both local and systemic symptoms.
The diagnosis of PPS requires a high index of suspicion by the clinician.Fever is common in cardiac surgery patients during the early postoperative
385

386 Chapter 19
period. The usual causes include complement activation by cardiopulmonarybypass, early stasis atelectasis and sensitivity reactions (drugs, transfusions,etc.). Fevers due to wound infection usually have onset after 1–2 weeks, andare obvious on close examination of the patient. Urinary tract infections mostoften present with specific symptoms and are easy to detect by urinalysis andblood counts. When postoperative fever persists, and/or is not due to one ofthe conditions mentioned above, the clinician should consider PPS as a pos-sible cause. The fever is usually in the range of 38–39 °C, but may be higher, par-ticularly in children. While fever is virtually always present, other symptomsoften vary. These may include malaise, irritability (particularly in children),decreased appetite, arthralgias and pleuro-pericardial pain (i.e. sharp painintensified by deep breaths, lying down, swallowing or other movements).
A pericardial friction rub may or may not be present early to assist in makingthe diagnosis, but such a rub is almost always audible at some time during the course of the illness. A tachycardia, out of proportion to the fever, is oftenpresent. Pleural effusions, when present, are usually left-sided and small, andmay be difficult to detect clinically. Although pericardial effusions are usuallypresent to some extent, tamponade is rare, but can be a devastating com-plication when it occurs. The finding of a weak, thready pulse, narrow pulsepressure, distended neck veins, shortness of breath of hepatomegaly shouldalert the clinician to this possibility. If there is difficulty with cardiac fillingother signs may be present, such as ankle edema or ascites.
A leukocytosis in the range of 10 000–15 000/mm3 with neutrophilic prepon-derance is usually present, as is elevation of the sedimentation rate and C-reactive protein. ECG findings of elevation of the ST segments in the limband lateral precordial leads are helpful when present, but may be obscured by post-surgical changes. The most specific blood test for PPS remains thefinding of anti-heart antibodies in the serum using immunoflourescence,recently enhanced by employing monoclonal antibodies directed againsthuman IgG [25].
Conventional X-ray of the chest usually reveals moderate cardiomegaly,and may show evidence of pericardial effusion, but these changes are notspecific for PPS. Indeed, modest cardiac enlargement is a common finding onearly postoperative films, and pericardial effusion may be difficult to appreci-ate in patients with open communication between the pericardial and pleuralspaces. Large pericardial and/or pleural effusions are more easily detectedand, in the presence of cardiac restriction, may be accompanied by radio-graphic evidence of pulmonary congestion. The presence of a pericardial effu-sion is not diagnostic of PPS, since many, if not most, patients undergoingcardiac surgery develop a small effusion postoperatively [26]. The extensiveuse of echocardiography in the postoperative cardiac surgery patient hasmade the finding of pericardinal effusions common. Small effusions are usu-ally posterior, and may sometimes be recognizable only during ventricularsystole, whereas larger effusions may extend all around the heart and be visible throughout the cardiac cycle. Collapse or indentation of the atria, and
Postpericardiotomy syndrome 387
sometimes the right ventricle, during diastole indicate interference with car-diac filling suggestive of tamponade.
Despite the fact that PPS and echocardiographic evidence of pericardialeffusions are common following cardiac surgery, tamponade is rare [27,28].Late cardiac tamponade has been reported to have an incidence of 0.1–6%,usually occurring in patients taking anticoagulants and probably unrelated to PPS [29,30]. Additionally, although constrictive pericarditis can occur lateafter cardiac surgery, there appears to be no relation to PPS [31].
Remembering that PPS is largely a diagnosis of exclusion, other causes offever, malaise and chest pain should be considered and ruled out before start-ing treatment for PPS. This treatment consists of various anti-inflammatoryagents, starting with the most benign and proceeding from there. Salicylates inanti-inflammatory doses (30–75 mg/kg per day) are usually effective in allevi-ating the symptoms in adults. Children may require lower doses. From per-sonal experience, indomethacin has proved quite effective, although somepatients experience GI upset with this drug. Ibuprofen has also been useful.More severe cases, and those with large pericardial effusions, may require theadministration of steroids. Indeed, patients given steroids will respond morerapidly than those treated with salicylates [32]. However, the prophylactic useof steroids pre-operatively has not been effective in preventing the subsequentdevelopment of PPS [33]. Those patients who develop large effusions resultingin tamponade will require more invasive treatment. An initial pericardiocen-tesis to relieve the tamponade can be life-saving and definitive. However, inthe most severe cases the effusion may return, necessitating surgical drainage(pericardial window) or, more rarely, pericardiectomy [34].
PPS is usually a benign, self-limited condition which responds to rest andanti-inflammatory agents. The necessity for more aggressive therapy is rare.The long-term prognosis is good.
References
1 Clapp SK. Postoperative inflammatory syndromes. In: Garson A, Bricker JT, Fisher DJ,Neish SR, eds. The Science and Practice of Pediatric Cardiology, 2nd edn. Baltimore: Williamsand Wilkins, 1998; 1817–1821.
2 Livelli FD Jr, Johnson RA, McEnany MT et al. Unexplained in-hospital fever following car-diac surgery. Natural history, relation to postpericardiotomy syndrome, and a prospect-ive study of therapy with indomethacin versus placebo. Circulation 1978; 57: 968–975.
3 McCabe JC, Ebert PA, Engle MA et al. Circulating heart-reactive antibodies in the post-pericardiotomy syndrome. J Surg Res 1973; 14: 158–163.
4 McClendon CE, Leff RD, Clark EB. Postpericardiotomy syndrome. Drug Intell ClinPharmacol 1986; 20: 20–23.
5 Kahn AH. The postcardiac injury syndromes. Clin Cardiol 1992; 15: 67–74.6 Engelman RM, Spencer FC, Reed GE et al. Cardiac tamponade following cardiac surgery.
Circulation 1970; 41(Suppl): 1165–1171.7 Kirsh MM, McIntosh K, Kahn DR et al. Postpericardiotomy syndromes. Ann Thor Surg
1970; 9: 158–179.
388 Chapter 19
8 Engle MA, Zabriskie JB, Senterfit LB et al. Viral illness and the postpericardiotomy syn-drome. A prospective study in children. Circulation 1980; 62: 1151–1158.
9 Dressler W. A post-myocardial infarction syndrome: preliminary report of complicationresembling idiopathic, recurrent, benign pericarditis. JAMA 1956; 160: 1379–1384.
10 Janton OH, Glover RP, O’Neill JE et al. Results of the surgical treatment of mitral stenosis.Circulation 1952; 6: 321–333.
11 Soloff LA, Zatuchui J, Janton DH et al. Reactivation of rheumatic fever following mitralcommissurotomy. Circulation 1953; 8: 481–493.
12 Gillette PC, Shannon C. Cardiac pacing in children. In: Dreifus LS, ed. Pacemaker Therapy.Philadelphis: FA Davis, 1983; 209–221.
13 Wang RYC, Mok CK. Erosion of an epicardial pacemaker secondary to postpericar-diotomy syndrome. Pace 1983; 6: 33–36.
14 Velander M, Grip L, Mogenson L et al. The postcardiac injury syndrome following per-cutaneous transluminal coronary angioplasty. Clin Cardiol 1993; 16: 353–354.
15 Rouang KS, Hee TT, Pogano TV et al. Dressler syndrome complicating radiofrequency abla-tion of an accessory atrioventricular pathway. Pacing Clin Electrophysiol 1993; 16: 251–253.
16 Hargreaves M, Bashir Y. Postcardiotomy syndrome following transvenous pacemakerinsertion. Eur Heart J 1994; 15: 1005–1008.
17 Lau CP, Fong PC, Tai YT et al. Postpericardiotomy syndrome complicating transvenousdual chamber, rate-adaptive pacing: diagnosis aided by transesophageal echocardio-graphy. Am Heart J 1992; 123: 1388–1393.
18 Ito T, Engle MA, Goldberg HP. Postpericardiotomy syndrome following surgery for non-rheumatic heart disease. Circulation 1958; 17: 549–555.
19 Elster SK, Wood HF, Seely RD. Clinical and laboratory manifestations of the postpericar-diotomy syndrome. Am J Med 1954; 17: 826–831.
20 Epstein S. Is the postcommissurotomy syndrome of rheumatic origin? Arch Int Med 1957;99: 253–257.
21 Larson DL. Relation of postcommissurotomy syndrome to the rheumatic state. Circulation1957; 15: 203–208.
22 Harthorne JW, Williams C, Bland EF. Postpericardiotomy and related syndromes. In:Andrus EC, ed. The Heart and Circulation: second national conference on cardiovasculardiseases. Washington, DC, 1964. Fed Am Soc Exper Biol 1965; 1: 513–521.
23 DeScheerder I, Wulfrank D, Van Renterghem L et al. Association of anti-heart antibodiesand circulating immune complexes in the postpericardiotomy syndrome. Clin ExpImmunol 1984; 57: 423–428.
24 Maisch B, Berg PA, Kochesiek K. Clinical significance of immunopathological findings inpatients with postpericardiotomy syndrome. 1. Relevance of antibody pattern. Clin ExpImmunol 1979; 38: 189–196.
25 Kocazeybek B, Erenturk S, Calyk MK et al. An immunological approach to postpericar-diotomy syndrome occurrence and its relation with autoimmunity. Acta Chirurgica Belgica1998; 98: 203–206.
26 Stevenson LW, Child JS, Laks H et al. Incidence and significance of early pericardial effu-sions after cardiac surgery. Am J Cardiol 1984; 54: 848–854.
27 Clapp SK, Garson A Jr, Gutgesell HP et al. Postoperative pericardial effusion and its rela-tion to postpericardiotomy syndrome. Pediatrics 1980; 66: 585–588.
28 Weitzman LB, Tinker WP, Kronzon J et al. The incidence and natural history of pericardialeffusion after cardiac surgery: an echocardiographic study. Circulation 1984; 69: 506–517.
29 Merrill W, Donahoo JS, Brawley RK et al. Late cardiac tamponade: a potentially lethal com-plication of open-heart surgery. J Thorac Cardiovasc Surg 1976; 72: 929–932.

Postpericardiotomy syndrome 389
30 Hochberg MS, Merrill WH, Gruber M et al. Delayed cardiac tamponade associated withprophylactic anticoagulation in patients undergoing bypass grafting: early diagnosis withtwo-dimensional echocardiography. J Thorac Cardiovasc Surg 1978; 75: 777–781.
31 Ng ASH, Dorosti K, Sheldon WC. Constrictive pericarditis following cardiac surgery-theCleveland Clinic experience. Cleve Clin Quart 1984; 50: 39–44.
32 Engle MA, Zabriskie JB, Senterfit LB. Heart-reactive antibody, viral illness and the post-pericardiotomy syndrome: correlates of a triple-blind, prospective study. In: Transactionsof the American Clinical and Climatological Association, 87th annual meeting. Baltimore:Waverly, 1975; 147–160.
33 Mott AR, Fraser CD Jr, Kusnoor AV et al. The effect of short-term prophylactic methly-prednisolone on the incidence and severity of postpericardiotomy syndrome in childrenundergoing cardiac surgery with cardiopulmonary bypass. J Am Coll Cardial 2001; 37:1700–1706.
34 McCabe JC, Engle MA, Ebert PA. Chronic pericardial effusion requiring pericardiectomyin the postpericardiotomy syndrome, J Thor Cardiovasc Surg 1974; 67: 814–820.
CHAPTER 20
Pulmonary and pleural complicationsafter cardiac surgery
Jeffrey E Everett
Pulmonary complications are one of the leading causes of morbidity and mortality after cardiac surgery. They are associated with prolonged intensivecare unit stay, ventilatory times, and increased hospital costs. The reportedincidence ranges from 25 to 90% [1,2]. Included are atelectasis, pneumonia,pulmonary embolus, pulmonary edema, diaphragmatic weakness or para-lysis, and disorders of the pleura. The following will attempt to identify preop-erative risk factors, techniques to prevent their occurrence, keys to early diag-nosis, and treatment planning for each of these postoperative complicationsfollowing cardiac surgery.
Respiratory failure
Postoperative respiratory failure, as defined by prolonged mechanical ventila-tion or abnormal gas exchange that adversely limits one’s physical endurance,is a significant concern in any patient undergoing a cardiothoracic procedure.Indeed, mortality approaches 30% in postoperative cardiac surgery patientsrequiring mechanical ventilatory support for > 3 days. Patients become sus-ceptible to nosocomial pneumonia, stress ulceration, airway injury, and debil-itation. It is known that postoperative pulmonary dysfunction is associatedwith prolonged operative time, the surgical site, advanced age, obesity, intrin-sic lung disease, preoperative level of function, and tobacco abuse. Of these,advanced age, obesity, and tobacco abuse are also known risk factors for cor-onary artery disease, making a large percentage of cardiac surgery patients atpotential risk of postoperative respiratory failure. The process begins with theinduction of a general anesthetic. The supine position reduces functionalreserve capacity (FRC) by 0.5–1 l, probably secondary to upward pressure ofthe abdominal contents and laxity of the diaphragm from the anesthetic. Thisthen corresponds to the development of postoperative lower lobe atelectasis.With regard to surgical site, proximity to the diaphragm affords the greatestrisk. There is up to a 40% decrease in vital capacity, total lung capacity, FRC, and inspiratory reserve capacity following a sternotomy incision alone.These values slowly return to normal but remain significantly lower until 4–7months postoperatively [3]. The impact is even greater with a thoracotomy.
390
Pulmonary and pleural complications after cardiac surgery 391
Postoperative pain with resultant splinting, hypoventilation, atelectasis andventilation–perfusion (VQ) mismatch is primarily responsible.
Identifying at-risk patients, however, is complicated by the fact that no single test predicts poor outcome and clinical reviews report conflicting results[4]. The goal is to identify the high-risk patient in order to optimize their pre-operative status or perhaps even exclude the highest risk patient in which riskexceeds the benefit. Screening begins with careful history specifically address-ing exercise tolerance, extent of dyspnea, sputum production, cough andsmoking habits. Physical examination looks for signs of intrinsic lung disease,specifically chest contour, clubbing, cyanosis, rales, rhonchi, wheezing, qualityof breath sounds, respiratory rate and pattern, and use of accessory muscles[5]. A young, non-smoking patient with no discernable symptoms warrants noadditional testing. The more risk factors identified the more helpful laboratorytesting including chest X-ray, arterial blood gas, pulmonary function test, andsputum culture will be. Unfortunately, there has been no reported study thatdefines a lower limit of preoperative spirometry volume or capacity [6]. Thereare, however, some findings consistently identified throughout reported seriesthat assign risk. An elevated blood pCO2 > 45 mmHg is associated with ahigher mortality [2,7]. A diffusing capacity of CO2 (DLCO), a forced expiratoryvolume in 1 s (FEV1) or a forced vital capacity (FVC) < 50% have been shown topredict a higher incidence of postoperative pulmonary failure. Though none isprohibitive, they do serve as indicator of risk and alert to the need for pul-monary optimization and appropriate discussion with the patient and family.
Having identified at-risk patients, preoperative maneuvers may serve tolower the incidence of postoperative pulmonary complications. When the lux-ury of time permits, patients will benefit from 2–4 weeks of chest physiother-apy [1,2,5]. First and foremost is cessation of smoking. It may take severalweeks for sputum production and bronchorrhea to decrease in heavy smokers.Postural drainage and percussion for 10 min four times daily will facilitateclearance of secretions. Purulent sputum should be cultured and antibiotictherapy initiated as indicated. Diaphragm exercises are performed by deeplyinspiring and then exhaling with pursed lips. An incentive spirometer isissued to give objective feedback and to familiarize one with proper techniqueprior to its postoperative use. Specialized pulmonary rehabilitation centersutilize graded inspiratory resistance as another technique to condition re-spiratory muscles. Bronchodilators are prescribed to relieve bronchospasm [1].Anemia should be corrected to restore oxygen-carrying capacity and the fluid balance returned to euvolemia. Though no study has demonstrated a reduction in postoperative pulmonary failure or pneumonia, preoperativeconditioning has been shown to reduce atelectasis significantly, lead to earlierextubation times, improve gas exchange, and reduce impairment of respirat-ory muscle function compared with controls [1,2]. Once ventilator depend-ence occurs, a multidisciplinary approach is necessary to achieve recovery.Proper nutritional support is initiated, preferably using the enteral route.Respiratory quotient analysis is performed to prevent overfeeding that

392 Chapter 20
produces excess CO2 and may impair the ability to wean. Physical and re-spiratory therapists are utilized to institute aggressive chest physiotherapy.Prophylaxis for both stress gastritis and deep venous thrombosis (DVT) is routinely administered.
Ventilatory support must be tailored to the individual patient. Those withchronic obstructive pulmonary disease (COPD) have a significantly higherwork of breathing. Auto-positive end pressure (PEEP) is responsible, aspatients must overcome intrinsic elastic recoil. Adding external PEEP withoutcausing hyperinflation reduces the work of breathing and may facilitate weaning. Bronchodilators and corticosteroids are used to decrease airwayresistance. A short course of corticosteroids administered after postoperativeday 2 does not adversely effect wound healing. In those patients with acutelung injury, intrapulmonary shunting occurs from increased lung water andloss of effective alveolar units. PEEP is optimized with a pulmonary arterycatheter to monitor changes in cardiac output. This is a means to recruit alveoliand improve tissue oxygenation. Inverting the inspiratory to expiratory ratioimproves oxygenation by increasing lung volume, recruiting alveoli, andenhancing collateral ventilation. Inhaled nitric oxide (NO) decreases right-to-left shunting and improves oxygenation. Allowing the CO2 to rise, permissivehypercapnea, allows lower tidal volumes which reduces barotraumas. Bene-ficial results, however, have been conflicting when compared with standardventilation. Once stabilized, slow pressure support weaning is attempted. This gradually increases the work of breathing to allow for conditioning.High-volume, low-pressure endotracheal tube cuffs have proven safe, butafter 2 weeks tracheostomy should be considered to facilitate weaning andpulmonary hygiene.
Atelectasis
Atelectasis may be present in up to 90% of patients following cardiac surgery.The etiology is multifactorial, including decreased FRC, splinting from post-operative pain, phrenic nerve dysfunction, impaired cough, mucous plugging,and surfactant deficiency [8]. Atelectasis may be classified as major, thatinvolving a segment, lobe, or lung, or minor when it affects a smaller distribu-tion. The pathophysiology of atelectasis includes several mechanisms (Figure20.1). Absorption atelectasis occurs distal to an obstruction where there is noaeration. Compressive atelectasis occurs secondary to such disorders ashemothorax, pleural effusion, and abdominal distension. Passive atelectasisarises from pneumothorax, hypoventilation or diaphragmatic dysfunction.Preoperative intrinsic lung disease and smoking are predisposing factors, butare more probably markers for patients with limited pulmonary reserves whowill be compromised by loss of functioning alveolar units. Known swallowingdisorders such as those occurring with neurological disease or previous headand neck surgery are also predisposing factors. Atalectatic changes are presenteven at 8 weeks’ follow-up.
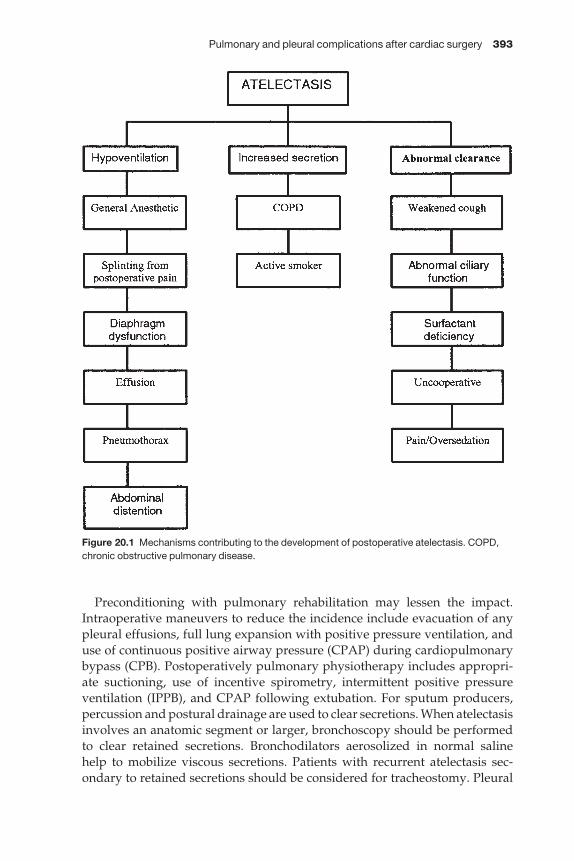
Pulmonary and pleural complications after cardiac surgery 393
Preconditioning with pulmonary rehabilitation may lessen the impact.Intraoperative maneuvers to reduce the incidence include evacuation of anypleural effusions, full lung expansion with positive pressure ventilation, anduse of continuous positive airway pressure (CPAP) during cardiopulmonarybypass (CPB). Postoperatively pulmonary physiotherapy includes appropri-ate suctioning, use of incentive spirometry, intermittent positive pressure ventilation (IPPB), and CPAP following extubation. For sputum producers,percussion and postural drainage are used to clear secretions. When atelectasisinvolves an anatomic segment or larger, bronchoscopy should be performed to clear retained secretions. Bronchodilators aerosolized in normal saline help to mobilize viscous secretions. Patients with recurrent atelectasis sec-ondary to retained secretions should be considered for tracheostomy. Pleural
Figure 20.1 Mechanisms contributing to the development of postoperative atelectasis. COPD,chronic obstructive pulmonary disease.
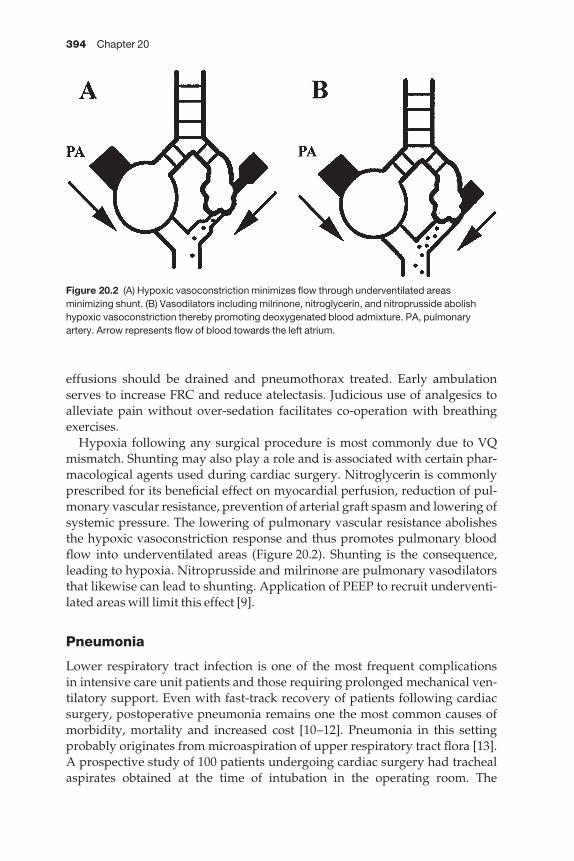
394 Chapter 20
effusions should be drained and pneumothorax treated. Early ambulationserves to increase FRC and reduce atelectasis. Judicious use of analgesics toalleviate pain without over-sedation facilitates co-operation with breathingexercises.
Hypoxia following any surgical procedure is most commonly due to VQmismatch. Shunting may also play a role and is associated with certain phar-macological agents used during cardiac surgery. Nitroglycerin is commonlyprescribed for its beneficial effect on myocardial perfusion, reduction of pul-monary vascular resistance, prevention of arterial graft spasm and lowering ofsystemic pressure. The lowering of pulmonary vascular resistance abolishesthe hypoxic vasoconstriction response and thus promotes pulmonary bloodflow into underventilated areas (Figure 20.2). Shunting is the consequence,leading to hypoxia. Nitroprusside and milrinone are pulmonary vasodilatorsthat likewise can lead to shunting. Application of PEEP to recruit underventi-lated areas will limit this effect [9].
Pneumonia
Lower respiratory tract infection is one of the most frequent complications in intensive care unit patients and those requiring prolonged mechanical ven-tilatory support. Even with fast-track recovery of patients following cardiacsurgery, postoperative pneumonia remains one the most common causes ofmorbidity, mortality and increased cost [10–12]. Pneumonia in this settingprobably originates from microaspiration of upper respiratory tract flora [13].A prospective study of 100 patients undergoing cardiac surgery had trachealaspirates obtained at the time of intubation in the operating room. The
Figure 20.2 (A) Hypoxic vasoconstriction minimizes flow through underventilated areasminimizing shunt. (B) Vasodilators including milrinone, nitroglycerin, and nitroprusside abolishhypoxic vasoconstriction thereby promoting deoxygenated blood admixture. PA, pulmonaryartery. Arrow represents flow of blood towards the left atrium.
Pulmonary and pleural complications after cardiac surgery 395
incidence of lower respiratory tract infection was 31% (8/26) with positive bacteriology compared with 1.4% (1/72) in those with negative aspirates [11].Patients with a prolonged preoperative in-hospital stay are likely to haveoropharyngeal colonization by more virulent and resistant organisms that predispose to postoperative pneumonia. Tobacco use is also a known risk fac-tor for pneumonia. In addition, host defenses are weakened following generalanesthesia and cardiopulmonary bypass. Decreased levels of complement,gamma globulin, and fibronectin are noted postoperatively. There is alsoreduced mucociliary clearance and impaired cough reflex. Prolonged op-erative times and multiple blood transfusions have also been established riskfactors. Postoperative risk factors include impaired cough reflex, impaired muco-ciliary clearance, and microaspiration. Prolonged endotracheal intubationincreases the risk of developing pneumonia by 1–3% per day [14].
Postoperative pneumonia is defined as new radiographic infiltrate withthree of the following: purulent sputum [> 25 white blood cells (WBC)], posit-ive culture, leukocytosis (> 10 000 WBC), and fever > 38 °C. Sputum samplesin the acute setting may be misleading, for they are more a reflection of upperairway and oropharyngeal colonization than the true distal airway infection.Pneumonia is therefore often over-diagnosed, but acceptably so in light of thepotential mortality if not aggressively treated. If diagnosis is in doubt, fiberopticbronchoscopy with lavage can have a negative predictive value (< 50% poly-morphonuclear cells) approaching 100% [15]. Protected brush catheter sam-ples from the distal airway also have improved yield with sensitivity andspecificity of 95% [16]. The offending organisms vary amongst institutions,with Klebsiella pneumoniae, Pseudomonas aeruginosa, Staphylococcus aureus,Haemophilus influenzae, Streptococcus pneumoniae, and Gram-negative aerobesand anaerobes being most common. Sterilization of the upper respiratory tractwould appear to be a preemptive strike. Colonization, however, does notalways correlate with infection. This is perhaps more likely an indicator ofunderlying lung disease, specifically COPD. Inappropriate preoperativeantimicrobials may lead to resistant strains, and secondary bacterial and fun-gal overgrowth. A more prudent approach would be cessation of smoking,optimized clearance of secretion with chest physiotherapy, and treatment ofsubclinical infection. Preoperative instruction on the use of an incentivespirometer and bronchodilators has been advocated as a way to lower post-operative pulmonary complications. Perioperative antimicrobials, usuallyadministered for wound infection prophylaxis, may be of benefit if appropri-ate antibiotics for nosocomial pneumonia are selected [17]. Previous concernon pneumonia secondary to Gram-negative overgrowth with stomach acidneutralization has not been consistently reproduced in the prospective setting[18]. Intraoperative maneuvers include shorter bypass run and time undergeneral anesthesia. Postoperative early extubation, ambulation, chest physio-therapy and perhaps intermittent positive pressure breaths will help to reducethe incidence. Early recognition and empiric antibiotics based on clinical set-ting and Gram stain are the first step in treatment. Hospital antibiograms help
396 Chapter 20
to tailor therapy. Antimicrobials together with aggressive chest physiotherapyshould minimize the morbidity and mortality of postoperative pneumonia.
Adult respiratory distress syndrome
Adult respiratory distress syndrome (ARDS) is a clinical entity characterizedby radiographic infiltrates, impaired gas exchange and decreased lung com-pliance. It is associated with aspiration, sepsis, shock and trauma. It is inessence the lung injury resulting from the systemic inflammatory response.Reported mortality rates range from 40 to 70% when the lungs are the sole sys-tem affected [19]. This condition has also been linked to cardiac surgery andthe use of cardiopulmonary bypass. The pathophysiology probably originateswith complement activation with the onset of bypass and subsequent elabora-tion of C3a and C5a [20]. Neutrophils become activated and are sequestered in the lung where they release elastase and myeloperoxidase leading to tissueinjury. A second insult may be induced by visceral hypoperfusion during CPB,especially with frequent use of neosynephrine to maintain mean arterial pres-sure. Endotoxins are released as bacterial translocation occurs [21]. Anotherpredisposing factor in this patient population is complement activation byprotamine via the classic pathway. The net result is pulmonary dysfunctionsecondary to injury at the capillary–alveolar interface. At onset this is an exuda-tive process, yet in some it will progress to fibrosis and irreversible damage[19]. Increased capillary permeability results in alveolar flooding with pro-teinaceous fluid. Lung compliance is reduced and hypoxic respiratory failureensues. Inflammatory cellular infiltrate follows with thickening of alveolar wallsand further reduction in compliance. The late phase is characterized by a reduc-tion in cellular infiltrate and progression of collagen deposition in the interstitium.
Though rare, with an incidence of only 0.4–3% of cardiac cases, the mortalityremains high. Cardiopulmonary bypass elicits the inflammatory cascade in allpatients. Most, however, have only subtle alterations in pulmonary function.There have been retrospective reviews that attempt to identify the predispos-ing factors for ARDS. Age > 60 years, reoperative surgery, duration of CPB,smoking history, shock, emergent surgery, low cardiac output, preoperativeamiodarone, and multiple transfusions have been identified. Attempts havebeen made to limit the inflammatory response with the use of pre-CPB corti-costeroids, but conflicting results have been obtained [19]. Most would agreethat there is little benefit. Leukocyte filters likewise have shown variableresults. Though laboratory models suggest benefit, this has not proven usefulin the clinical setting. This limits therapy to early detection and supportivemeasures. The diagnosis is established by the presence of tachypnea, bilateralpulmonary infiltrates, hypoxia, requirement of PEEP > 5, and absence of leftheart failure with pulmonary capillary wedge (PCW) < 18. Management beginswith eliminating any further mediators such as hypoperfusion, bacterialtranslocation, or tissue ischemia. Ventilator management includes avoidanceof barotraumas, optimal PEEP levels, use of prone position to improve VQ
Pulmonary and pleural complications after cardiac surgery 397
mismatch, limit FiO2 < 0.6, paralysis or sedation to reduce oxygen consumptionand facilitate mechanical ventilation, permissive hypercapnea, and inverse I/Eraito [22,23]. Fluid management should be guided by pulmonary arterycatheter monitoring. The goal is to reduce lung water without compromisingend-organ perfusion. Low-dose NO may reduce shunting and improve oxy-genation. The mortality from ARDS is usually secondary to multisystem organfailure. These supportive measures and preventing further complicationsremain the mainstay of therapy.
Pulmonary edema
Postoperative pulmonary edema results from several conditions. First, there iscapillary leak secondary to the inflammatory response elicited during CPB.This occurs even with normal left atrial pressure. The majority of patients willnot have a significant clinical manifestation other than decreased pulmonarycompliance and increased alveolar–arterial gradient [24]. This lung edema willresolve over the first few postoperative days and may be hastened by the use ofdiuretics. The next form of pulmonary edema develops after 3–5 days. It isassociated with the mobilization of extravascular fluid retained during bypass.The left atrial pressures if measured may be elevated. Though usually self-limited, diuretics may speed recovery. Congestive heart failure is the last formof pulmonary edema. It is the most serious and difficult to manage. The eti-ology is systolic or diastolic dysfunction of the left ventricle. Left atrial pressuresrise with resultant pulmonary congestion. In the immediate postoperativeperiod, preload and afterload are optimized first with inotropic agents addedas needed. Should the desired response not be obtained, intra-aortic ballooncounterpulsation or a left ventricular assist device may be considered. In thelater postoperative period, management includes afterload reducing agents,typically ACE inhibitors, diuretics (loop or spironolactone), and perhaps digi-talis. For patients with marginal pulmonary status preoperatively, considera-tion should be given for off-pump strategies to avoid at least the inflammatorycascade. For those requiring the use of CPB, ultrafiltration during the run will reduce free water load and perhaps lower cytokine levels. Modifiedultrafiltration popularized in pediatric cases has been shown to improve postoperative oxygenation compared with controls [25].
Pulmonary embolus
Pulmonary embolus (PE) is an infrequent complication following cardiacsurgery, with reported incidence ranging from 0.5 to 3.5% [26]. Even thoughresultant mortality may approach 40%, the net perioperative risk adjusts to only 0.3–1.7%, which is significantly lower than other surgical serviceswhich typically report PE mortality of 1–6% [27]. This difference is probablysecondary to high-dose heparin intraoperatively, antiplatelet therapy post-operatively, platelet dysfunction resulting from CPB, and hemodilution.
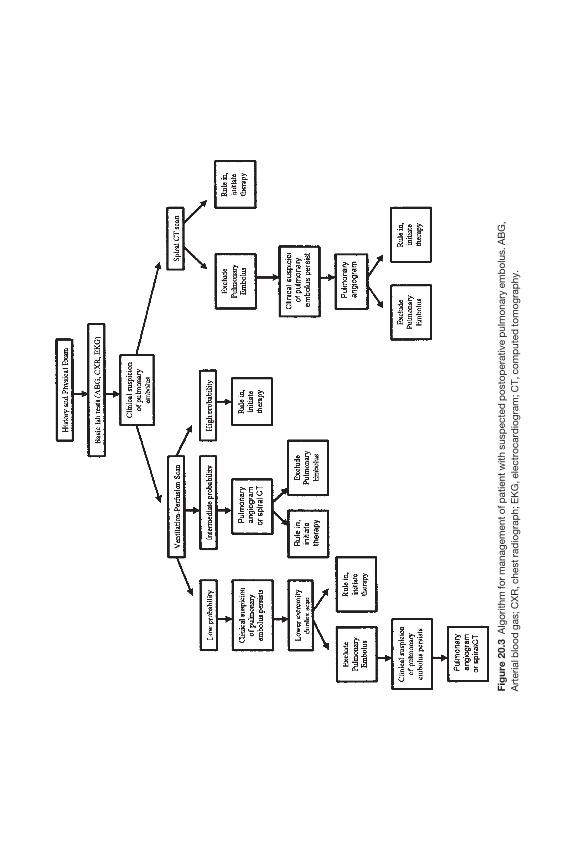
Fig
ure
20.3
Alg
orith
m fo
r man
agem
ent o
f pat
ient
with
sus
pec
ted
pos
top
erat
ive
pul
mon
ary
emb
olus
. AB
G,
Art
eria
l blo
od g
as; C
XR
, che
st ra
dio
grap
h; E
KG
, ele
ctro
card
iogr
am; C
T, c
omp
uted
tom
ogra
phy
.
Pulmonary and pleural complications after cardiac surgery 399
The vast majority of PE arise from deep vein thrombosis (DVT) from the lowerextremities or pelvic veins. Screening duplex imaging of postoperative cardiacpatients yields a DVT incidence of 20–40%. Interestingly, the side distributionof DVT is equal, and therefore does not appear influenced by saphenous veinharvesting. Most are limited to the calf veins and have low rate of propagationand resultant PE. Indeed, routine duplex scanning has been shown not to becost effective in prospective testing [27]. A high index of suspicion must bemaintained and diagnostic testing obtained judiciously. Though symptoms ofleg tenderness and swelling commonly occur in this patient population fromsurgical trauma and fluid overload, the onset of unilateral symptoms shouldbe further investigated. Sound clinical judgement together with appropriatetesting should allow for accurate and effective diagnosis (Figure 20.3).
The diagnosis of PE is equally challenging. As mentioned, DVT, the pre-cursor of PE, is accurately diagnosed by clinical criteria in < 5% of cases [27].The clinical signs and symptoms of PE are often marked by postsurgicalchanges. Chest pain, tachycardia, tachypnea are attributed to the surgicaltrauma including the recent sternotomy, presence of pleural drainage tubes,and internal thoracic artery (ITA) harvesting. Routine narcotic administrationfurther masks the clinical picture. Hypoxia, distended neck veins, and wheez-ing are just as likely from atelectasis, pleural effusion, fluid overload, or car-diac dysfunction which occur with higher frequency.
Preventative measures begin by identifying high-risk groups. The classictriad of stasis, hypercoagulable state, and endothelial injury is relevant to mostsurgical patients. Specific patient groups are at even higher risk. Several series have shown that preoperative or postoperative bed rest for > 3 dayssignificantly increases the incidence of PE. Congestive heart likewise is a riskfactor consistently identified in separate reports. A variety of other factorshave been reported and should be considered, but have not proven statisticallysignificant in multivariate analysis. These include hyperlipidemia, obesity,history of DVT or PE, heparin-induced thrombocytopenia, and recent myocar-dial infarction. Other variables such as gender, race, age, tobacco use, varicoseveins, diabetes mellitus and use of an intra-aortic balloon pump have not been associated with an increased risk of PE after cardiac surgery. In addition,patients undergoing valve operation have a significantly lower incidence of PEthan other cardiac procedures such as coronary bypass. This difference isbelieved secondary to the use of anticoagulants in this patient group [26].
Prophylactic maneuvers begin with the avoidance of indwelling catheters inthe lower extremities, and early ambulation, preferably on postoperative day1. Antiplatelet therapy, which is standard practice, should be instituted andmay decrease the incidence of DVT. The role of graded compression stockings(GCS) and sequential compression devices (SCD) is controversial. Studiesfrom other surgical services have shown a significant reduction in DVT withthe use of SCD. A prospective study of cardiac surgery patients, however, hasshown no such benefit. The use of subcutaneous heparin has not undergonesafety or efficacy study in this patient population. Concern over bleeding

400 Chapter 20
complication, the development of thrombocytopenia, and overall low incidenceof PE in cardiac surgery patients explain the avoidance. It must be kept inmind, however, that reported series are taken from the general population ofcardiac surgery patients, most of which ambulate early and may not havesignificant risk factors. A more aggressive approach should be applied topatients targeted at high risk. The use of SCD and even subcutaneous heparinshould be considered for patients with delayed recovery, congestive heart failure or combination of previously mentioned risk factors.
Diagnostic workup begins with clinical examination, chest X-ray, and arterial blood gas analysis. Ventilation–perfusion scanning has been the tradi-tional screening examination. Although a high-probability scan may be usedto confirm the diagnosis accurately, an intermediate or low-probability testcannot be used as confirmation of diagnostic exclusion. In fact, up to 54% ofpost-cardiac surgery patients with a low–intermediate VQ scan have beenshown to have PE by pulmonary angiography or autopsy [28]. To improvediagnostic accuracy, Duplex evaluation of the lower extremities may beobtained. If both Duplex examination for DVT and VQ scanning together are negative, the incidence of PE falls to < 9%. Spiral computed tomography isnow emerging as a rapid non-invasive screening tool to diagnose PE. In ex-perienced centers diagnostic yield approaches angiography with sensitivity of94% and specificity of 94% [29]. No large series have reported its use in cardiacsurgery patients. The postoperative patient with unexplained dyspnea andhypoxia should have an aggressive workup. If VQ scanning is other than highprobability, pulmonary angiogram should be obtained. Early detection willlead to therapy which decrease the likelihood of recurrent emboli as well asprevent propagation.
Pulmonary embolism, once diagnosed, is classified based upon the patient’shemodynamic status, oxygenation and percent pulmonary artery occlusion(Table 20.1). Classification schemes have been derived to guide therapy andprognosis. Patients with class I or II embolism are managed with anticoagula-tion alone. Heparin is administered to achieve a partial thromboplastin
Table 20.1 Classification of pulmonary embolism.
Class Symptoms PaO2 % PA occlusion Hemodynamics
I None Normal < 20 NormalII Anxiety, hyperventilation < 80 20–30 TachycardiaIII Dyspnea < 65 30–50 CVP elevated, PA > 20 mmHgIV Shock, dyspnea < 50 > 50 CVP elevated, PA > 25 mmHg,
BP < 100V Syncope < 50 > 50 CVP elevated, PA > 40 mmHg,
shock
PA, Pulmonary artery; CVP, central venous pressure; BP, blood pressure. (Adapted fromGreenfield L. Complications in Surgery and Trauma. Philadelphia: JB Lippincott Co., 1984.)

Pulmonary and pleural complications after cardiac surgery 401
level two times control. Oral therapy with coumadin is initiated and the twooverlapped until the INR reaches the therapeutic range. Patients with com-plications of anticoagulation therapy, recurrence despite therapeutic anti-coagulation, hemodynamically compromising PE, or inability to comply with medical therapy are evaluated for placement of a caval filter. Class IV–V PE are managed with emergent emobolectomy via suction catheter or open technique.
Pleural disease
Pleural effusions are evident in 50% of post-cardiac surgery cases. The major-ity are left sided and will resolve with no specific therapy. The onset may beimmediately postoperative or delayed anywhere from days to weeks later. In the largest reported series of post-cardiac surgery patients, < 1% developeda large effusion, one which occupies > 25% of the hemithorax [30]. Congestiveheart failure, pericardial inflammation, and pulmonary embolus are the mostcommonly identified causes. The majority, at least two-thirds, are idiopathic.Pleural effusions are characterized as bloody or serous. Bloody effusions occursooner postoperatively, contain high lactate dehydrogenase, and typicallyresolve with 1–2 thoracenteses. They originate from postsurgical bleeding into the thoracic cavity. These effusions reach their maximal size on average 12 days postoperatively. Hemorrhage into the pleural space elaborates inter-leukin-5 by CD4 cells and may explain the presence of eosinophilia in fluidsamples. Untreated bloody effusions may incite pleural fibrosis and lungentrapment [31]. Early drainage and lung expansion prevents this unusual but serious complication. Pleurectomy and decortication are necessary onceentrapment has occurred. Non-bloody effusions are less likely to have anidentifiable source, contain low LDH, reach their maximal size on average 1 month postoperatively and are lymphocytic. These effusions may be a formof hypersensitivity reaction. There is a direct correlation with pericardial effusions when screened using echocardiography, suggesting a potential relationship to the postcardiotomy syndrome. Indeed, mammals are known to have small fenestrations that provide direct communication between thepleural and pericardial spaces. In addition, harvesting of the internal thoracicartery (ITA) interrupts pleural lymphatics, impeding resorption of pleuralfluid. There is also a higher incidence in cases in which topical hypothermia is used. Serous effusions are more likely to recur and require repeated inter-ventions. Consideration may be given to the administration of non-steroidalanti-inflammatory agents or prednisone for recurrent cases. Treatment failuresmay be managed with mechanical or chemical pleurodesis.
Pneumothorax
Pneumothorax is an uncommon complication following cardiac surgery,occurring in 0–1.4% of cases. The etiology is direct lung injury, usually ITA

402 Chapter 20
harvesting, spontaneous rupture of bullae or blebs from barotraumas, or from air drawn into the thoracic cavity from thoracostomy tube sites.Identifiable risk factors include intrinsic pulmonary disease such as emphy-sema and bronchitis, mainstem intubation with barotraumas, iatrogenic injury during placement of central venous catheters, and tobacco abuse.Presentation ranges from asymptomatic incidental chest X-ray finding to cardiopulmonary arrest. In the sedated and intubated patient an index of sus-picion must be maintained. Restlessness, hypoxia, dysrrhythmia or increasedairway pressure are suggestive in the intubated patient. Spontaneouslybreathing patient complaints may be vague, including chest pain, dyspnea oranxiety. Early diagnosis begins with physical examination. Obvious findingsinclude unilateral absence of breath sounds and hyperresonace to percussion.Most, however, will not have such clear findings and if the clinical conditionpermits the diagnosis should be confirmed with chest X-ray. Observation may be all that is necessary for the small incidental pneumothorax. Others will require aspiration or thoracostomy tube drainage. Persistent air leak over72 h may be managed by thoracoscopic stapling, pleural abrasion or pleurec-tomy, or chemical pleurodesis.
Phrenic nerve injury
Diaphragmatic elevation or paralysis occurs in 7–11% of patients after cardiacsurgery. Topical hypothermia has been shown both clinically and experi-mentally to cause phrenic nerve dysfunction with resultant hemidiaphragmelevation and lobar atelectasis. Phrenic nerve conduction velocity measuringalso identifies prolonged cardiopulmonary bypass as a statistically significantrisk factor. Slow resolution is the typical clinical course. By 6 months 44% norm-alize and by 1 year 90%. Diagnosis is suspected in patients with diminishedbreath sounds and poor diaphragmatic excursion during percussion and an elevated hemidiaphragm on chest X-ray. The diagnosis can be confirmedwith videofluoroscopy or ultrasound of the diaphragm. Phrenic nerve con-duction velocities are available in some centers. Observation is the mainstay of therapy, as most will resolve. Diaphragmatic plication is unusually appliedto adult patients.
References
1 Castillo R, Haas A. Chest physical therapy: comparative efficacy of preoperative and postoperative in the elderly. Arch Phys Med Rehabil 1985; 66: 376–379.
2 Weiner P, Zeidan F, Zamir D et al. Prophylactic inspiratory muscle training in patientsundergoing coronary artery bypass graft. World J Surg 1998; 22: 427–431.
3 Ingwersen UM, Larsen KR, Bertelsen MT et al. Three different mask physiotherapy regimens for prevention of postoperative pulmonary complications after heart and pulmonary surgery. Intens Care Med 1993; 19: 294–298.
4 Ingersoll GL, Grippi MA. Preoperative pulmonary status and postoperative extubationoutcome of patients undergoing elective cardiac surgery. Heart Lung 1991; 20: 137–143.
Pulmonary and pleural complications after cardiac surgery 403
5 Nealon TF Jr, McNeil AG. Management of operations in the pulmonary cripple. Surg ClinNorth Am 1967; 47: 1223–1234.
6 Gass GD, Olsen GN. Preoperative pulmonary function testing to predict postoperativemorbidity and mortality. Chest 1986; 89: 127–135.
7 Celli BR. What is the value of preoperative pulmonary function testing? Med Clin NorthAm 1993; 77: 309–325.
8 Johnson D, Thomson D, Mycyk T et al. Respiratory outcomes with early extubation aftercoronary artery bypass surgery. J Cardiothorac Vasc Anesth 1997; 11: 474–480.
9 Berthelsen P, St Haxholdt O, Husum B et al. PEEP reverses nitroglycerin-induced hypox-emia following coronary artery bypass surgery. Acta Anesthesiologica Scand 1986; 30:243–246.
10 Carrel TP, Eisinger E, Vogt M et al. Pneumonia after cardiac surgery is predictable by tracheal aspirates but cannot be prevented by prolonged antibiotic prophylaxis. AnnThoracic Surg 2001; 72: 143–148.
11 Carrel T, Schmid ER, von Segesser L et al. Preoperative assessment of the likelihood ofinfection of the lower respiratory tract after cardiac surgery. Thorac Cardiovasc Surg 1991;39: 85–88.
12 Gould FK, Freeman R, Brown MA. Respiratory complications following cardiac surgery.The role of microbiology in its evaluation. Anesthesia 1985; 40: 1061–1064.
13 Harrington OB, Duckworth JK, Starnes CL et al. Silent aspiration after coronary arterybypass grafting. Ann Thoracic Surg 1998; 65: 1599–1603.
14 Fagon J, Chastre J, Domart Y et al. Nosocomial pneumonia in patients receiving continu-ous mechanical ventilation. Am Rev Resp Dis 1989; 139: 877.
15 Kirtland S, Corley D, Winterbauer R et al. The diagnosis of ventilator-associated pneumo-nia: a comparison of histologic, microbiologic, and clinical criteria. Chest 1997; 112: 445.
16 Wimberly N, Bass J, Boyd B et al. Use of a bronchoscopic protected catheter brush for thediagnosis of pulmonary infections. Chest 1982; 81: 556.
17 Bernard A, Pillet M, Goudet P et al. Antibiotic prophylaxis in pulmonary surgery. J ThorcCardiovasc Surg 1994; 107: 896.
18 Poullis M. Chronic H2 receptor antagonist treatment and pulmonary complications postcardiac surgery. Ann Roy Coll Surg Engl 1999; 81: 239–241.
19 Milot J, Perron J, Lacasse Y et al. Incidence and predictors of ARDS after cardiac surgery.Chest 2001; 119: 884–888.
20 Kutsal A, Ersoy U, Ersoy F et al. Complement activation during cardiopulmonary bypass.J Cardiovasc Surg 1989; 30: 359–363.
21 Berger D, Bolke E, Huegel H et al. New aspects concerning the regulation of the postoperat-ive acute phase reaction during cardiac surgery. Clinica Chimica Acta 1995; 239: 121–130.
22 Brussel T, Hachenberg T, Roos N et al. Mechanical ventilation in the prone position foracute respiratory failure after cardiac surgery. J Cardiothorac Vasc Anesth 1993; 7: 541–546.
23 Matthay MA, Wiener-Kronish JP. Respiratory management after cardiac surgery. Chest1989; 95: 424–434.
24 Thorsen MK, Goodman LR. Extracardiac complications of cardiac surgery. SeminRoentgenol 1988; 23: 32–48 [Review].
25 Kiziltepe U, Uysalel A, Corapcioglu T et al. Effects of combined conventional andmodified ultrafiltration in adult patients. Ann Thorac Surg 2001; 71: 684–693.
26 Josa M, Siouffi SY, Silverman AB et al. Pulmonary embolism after cardiac surgery. J AmColl Cardiol 1993; 21: 990–996.
27 Shammas N. Pulmonary embolus after coronary artery bypass surgery: a review of the lit-erature. Clin Cardiol 2000; 23: 637–644.
404 Chapter 20
28 Ramos R, Salem BI, Haikal M et al. Critical role of pulmonary angiography in the diagnosisof pulmonary emboli following cardiac surgery. Catheter Cardiovasc Diagn 1995; 36:112–117.
29 Ost D, Rozenshtein A, Saffran L et al. The negative predictive value of spiral computedtomography for the diagnosis of pulmonary embolism in patients with nondiagnosticventilation-perfusion scans. Am J Med 2001; 110: 16–21.
30 Light RW, Rogers JT, Cheng D et al. Large pleural effusions occurring after coronary arterybypass grafting. Cardiovascular Surgery Associates, PC. Ann Intern Med 1999; 130:891–896.
31 Lee YC, Vaz MA, Ely KA et al. Symptomatic persistent postcoronary artery bypass graftpleural effusions requiring operative treatment: clinical and histologic features. Chest2001; 119: 795–800.
CHAPTER 21
Neurological complications in cardiac surgery
George J Koullias, John A Elefteriades
Introduction
The close correlation between the heartathat gives lifeaand the brainathatprovides quality of lifeais such that on many occasions, neurological complica-tions following cardiac surgical procedures severely minimize the beneficialeffects of the operation.
In the 1960s, severe neurological complications during cardiac surgery wereappearing in 20% of patients [1,2]. In the 1970s and 1980s, with improvementsin surgical technique, anesthesia and monitoring, the incidence fell to therange of 5% [3,4]. Recently, with the increased average age of the cardiac sur-gical patient, studies have shown that stroke rate is once again in the range of5%. Prolonged encephalopathy occurs in about 10% of patients [5]. From apathophysiological standpoint, three major mechanisms cause neurologicalinjury during cardiac surgery: macroembolism, microembolism and reducedcerebral blood flow.
Systemic inflammatory response syndrome (SIRS) in cardiac surgery
Cardiac surgery with cardiopulmonary bypass (CPB) is known to induce systemic inflammatory response syndrome (SIRS). SIRS is associated withincreased morbidity and mortality, mainly due to organ and resultant hemo-dynamic failure. SIRS is diagnosed based on specific clinical criteria, but as asyndrome incorporates a conglomeration of pathophysiological alterationssuch as:1 Reduction of circulating immunoglobulins (especially antibodies againstendotoxin).2 Leukocyte and complement system activation.3 Immunological suppression.4 Interleukin and inflammatory mediator release.5 Diffuse endothelial damagealeaking.6 Resultant hemodynamic failure and collapse.
SIRS has long been described after cardiac surgery with the use of CPB.Intensive research efforts have focused on identifying patients at increased
405
406 Chapter 21
preoperative risk of SIRS, increased risk of SIRS during the first few postoperat-ive hours, and finally on diminishing the morbid effects of SIRS or its resultantMODS (multiple organ dysfunction syndrome). The APACHE III immediatepostoperative scoring system is a reliable predictor of postoperative SIRS.Cardiac surgical patients that have lower preoperative anti-endotoxin anti-body levels release more anti- and proinflammatory cytokines during CPB.This increase in cytokines [IL-6, IL-8, IL-1β, C-reactive protein (CRP)] is higherin patients with longer CPB times [6,7]. Several aspects of the cell-mediatedimmune response are either severely depressed or greatly increased duringCPB [8]. These actions are usually mediated by proinflammatory cytokines.Some of these proinflammatory molecules (specifically IL-8 and CRP) havebeen studied as impending SIRS markers in the immediate postoperative set-ting in cardiac surgical patients [9,10]. SIRS seems to be equal in conventionaland minimally invasive cardiac surgery [11], but lower in ‘off-pump’ proce-dures [12]. Preoperative risk factors for SIRSabesides low anti-endotoxin anti-body levelsainclude chronic use of ACE inhibitors, high preoperative CRPlevels and preoperative respiratory infection [13,14].
One thing needs to be remembered: the single most important intra-operative risk factor for SIRS appears to be CPB duration [15].
The effects of SIRS on the brain have been studied in the contest of traumaand systemic infections, but not during the cardiac surgery postoperativestate. In the event of SIRS, the central nervous system seems to react in a manner that mimics both protective adaptation and self-induced injury. Themain SIRS-induced CNS adaptations are the following, and should always be considered in cases of neurological injury during cardiac surgery:1 Cerebral vasodilatation followed by vasoconstriction.2 Increase of the blood–brain barrier permeability.3 Reduced neuronal metabolic rate.4 Increased CSF pressure.5 Neuronal membrane damage of various degrees.6 Enhanced expression of leukocyte adhesion molecules.7 Synthesis and release of nitric oxide, glutamate and aspartate, all of whichact as neurotransmitters and later as potent neurotoxins.
Types of neurological injury in coronary and valve surgery
Two main types of neurological injury during and after surgery have beendescribed.
Type I neurological injuriesType I neurological injuries encompass all major and moderate focal neuro-logical injuries, including shock and coma resulting from a major cerebralinfarct.
Major cerebral infarction incorporating a large portion of the cerebrumand/or the cerebellum occurs in 0.3–2% of all cardiac operations, depending

Neurological complications in cardiac surgery 407
on the study. Its incidence follows the general trend of decrease over the last 30 years, with an increase in the last decade. The overwhelming majority of these are of embolic origin. Detailed pathological studies have shown thatthe primary sites of damage reside in the posterior cortex, basal ganglia andcerebellum. Characteristically, the brain stem is pathologically spared in casesof major neurological injuries [6]. Aggregates of fibrin, fat particles, atheromat-ous particles and platelets are usually discovered in embolized small-caliberarteries and higher size atheromatous debris coated with platelets are dis-covered in occluded major arteries [16].
Focal cerebrovascular accidents incorporating smaller portions of the CNSappearing for a period of > 24 h are also classified as type I injuries and are usually seen after valve replacement procedures (10%), after coronary revas-cularization procedures (< 2%) and even after percutaneous transluminalcoronary angioplasty (0.2%). Macroembolism (in contrast to microembolismshowering) is identified as the major etiological factor in the appearance ofcerebrovascular accidents during and after valve surgery. Clinically, in themajority of these cases, the patient has a left hemiparesis caused by embolismof a major branch of the right middle-cerebral artery.
Although there is no solid explanation, the predilection for cardiogenicembolism of right cerebral vessels has been documented repeatedly in the literature. Decreased tolerance of the right cerebral hemisphere to micro- andmacroembolism has also been hypothesized [7]. The remaining 20–30% ofcerebrovascular accidents involve the sensory mechanisms and cerebellum,producing sensory deficits and postoperative balance disorders.
Major epileptic seizures, another form of type I injury, are found in an aver-age of 0.3–0.8% of cases. They are usually a consequence of cerebral infarctionand have been described as early as immediately after the patient has beenweaned from bypass. Usually seizures appear in the first postoperative week.Twenty percent to 30% of the cases are seen as late as 1 year after surgery.Unfavorable outcome correlates with seizures difficult to control initially andwith seizures that appear as myoclonic crises [17,18].
Coma is an extreme form of decreased level of consciousness and its incidence is fortunately low. Approximately 50% of major cerebral functionsmanifest clinically as immediate postoperative coma. Bilateral preexistentcarotid and cerebrovascular disease and postoperative acidosis are associatedwith poor outcome. Brain stem dysfunction, signs of decerebration or decor-tication and persistent absence of response to painful stimuli predict poor out-come. In comas of < 1 week duration, a 90–93% functional recovery has beenobserved. If the coma lasts 3.5–4 weeks, there is practically no chance of anyfunctional recovery [19].
Spinal cord injury in non-aortic cardiac surgery is a rare complication and isevidenced by the appearance of postoperative hemiparesis or paraparesis.This complication is seen when an intra-aortic balloon pump is used andattributed to embolization and ischemia of the spinal cord vessels caused byatheromas dislodged locally from the aorta during balloon counterpulsation.
408 Chapter 21
Type II neurological injuriesThe collective category of type II injuries encompasses a wide variety of neuro-logical injuries of either lesser magnitude or lesser duration. Ophthalmologicalcomplications, minor seizure disorders, focal deficits that last < 24 h, diffusemild encephalopathy, disorders of attention, recent or remote memory, andaffect, immediate or later psychiatric disorders, as well as dysfunction of components of the peripheral nervous system are included in this category. Ingeneral, the more immediate and more detailed the neurological assessment,the higher the discovered incidence of type II neurological injury.
Ophthalmological disorders are encountered in 17–25% of cardiac surgicalpatients. Because of their short duration in the immediate postoperative set-ting of the cardiac surgical patient, ophthalmological disorders are frequentlyoverlooked. They are caused by single, or more frequently, multiple fibrin andplatelet microemboli to the retinal vessels [20]. Usually the patient complainsof temporary partial loss of vision, hemianopic defects or intermittent ‘flash-ing lights’ vision. Relatively frequently, the patient also experiences corticalblindness (Anton syndrome) due to bilateral occipital lobe microembolism.The vast majority of the above ophthalmological disorders do not last morethan 6 weeks [10] and permanent blindness after cardiac surgery is very rare.
Minor seizure disorders and diffuse mild encephalopathyMinor seizure disorders usually accompany clinically non-significant embolicischemic lesions. Their overall incidence is 1–4% and they are easily controlledwith short-term antiseizure medication regimens. Mild diffuse encephalo-pathy has been discovered in > 40% of patients after cardiac surgery [21,22].This is associated with the appearance of abnormal (bilateral Babinski reflexes,corticomodullar reflexes) or primitive reflexes (grasping or sucking reflex).These reflexes are of minor clinical importance and are attributed to diffusemild ischemic dysfunction of the frontal lobes during cardiopulmonarybypass [21,22].
Mental and cognitive dysfunctionThe incidence of diagnosed mental disorders after coronary and vascularsurgery ranges from 30 to 80% [22–24]. This wide range is due to the use of dif-ferent diagnostic criteria and cognitive tests in the literature. The sooner andmore complete the neurocognitive testing, the higher the reported incidence of diagnosed dysfunction. These disorders usually manifest as disorders ofrecent and remote memory, judgement, affect and behavior. Initially in cardiacsurgery, these disorders were attributed to stress after a major operation.Today all indications point to discrete diffuse hypoperfusion-related cerebraldamage with or without additional microembolic phenomena. In comparativeneurocognitive studies [25] of patients who underwent major surgery andpatients who had cardiac surgery with cardiopulmonary bypass, it wasproven that postoperative neurocognitive deficits were more pronounced inthe cardiac surgery patient group.
Neurological complications in cardiac surgery 409
Nevertheless, two points need to be emphasized. First, in the vast majorityof cardiac surgical patients, the observed neurocognitive deficits are not debil-itating. Second, almost complete resolution of those deficits is observed clinic-ally and during cognitive testing in 98–99% of these patients, 4–8 weeks aftersurgery [26,27].
Psychiatric complicationsPsychiatric complications after cardiac surgery are reported in 1–5% of thepatients, and usually manifest as confusion, psychokinetic instability, para-noid ideation and irritability. They last between 1 and 3 weeks and their etiology (organic or psychiatric) is still debated. As in the case of postoperat-ive cognitive dysfunction, the wide variation in the reported incidence is attributed to the variety of diagnostic criteria and timing [22,28–31]. Clinic-ally, a differential diagnosis between the so-called ‘ICU psychosis’ and a psychiatric complication after cardiac surgery should be made. ICU psychosisusually starts after the third to fifth ICU stay day as opposed to psychiatricdysfunction after cardiac surgery that starts the first or second postoperativeday.
Peripheral nervous system complications are generally considered innocentand are not discovered unless the patient develops specific complaints. Theiroverall incidences ranges from 2.6 to 13%. Most such complications are relatedto brachial plexus injuries. Specifically the lower trunk of the plexus is injuredmore frequently, with resultant digit weakness or hypersthesia, especially inthe ulnar distribution.
The majority of these complaints significantly subside 4–8 weeks aftersurgery [31]. More infrequent complications are phrenic nerve damage, recur-rent laryngeal nerve injury and peroneal nerve injury during saphenous veinharvesting [32].
Risk factors for neurological injury in coronary and valve surgery
Several well-designed multicentre prospective randomized trials have iden-tified risk factors for type I and type II neurological injuries in patients after cardiac surgery. Risk factors for type I injury after coronary artery bypass were proximal aortic atherosclerosis, prior neurological event, use ofintra-aortic balloon pump (IABP), diabetes mellitus, hypertension, pulmonarydisease, angina and age [33].
Risk factors for type II injury in coronary artery bypass grafting (CABG)were: history of pulmonary disease, age, the use of preoperative antihypertens-ives, systolic blood pressure > 180 mmHg on admission, excessive alcohol consumption, prior CABG, and dysrythmias on the day of surgery [5,33,34].
Several risk factors were also identified for the patient who underwentCABG plus an intracardiac procedure. Type I injury risk factors in thesepatients included the presence of atrial and ventricular thrombus, proximal
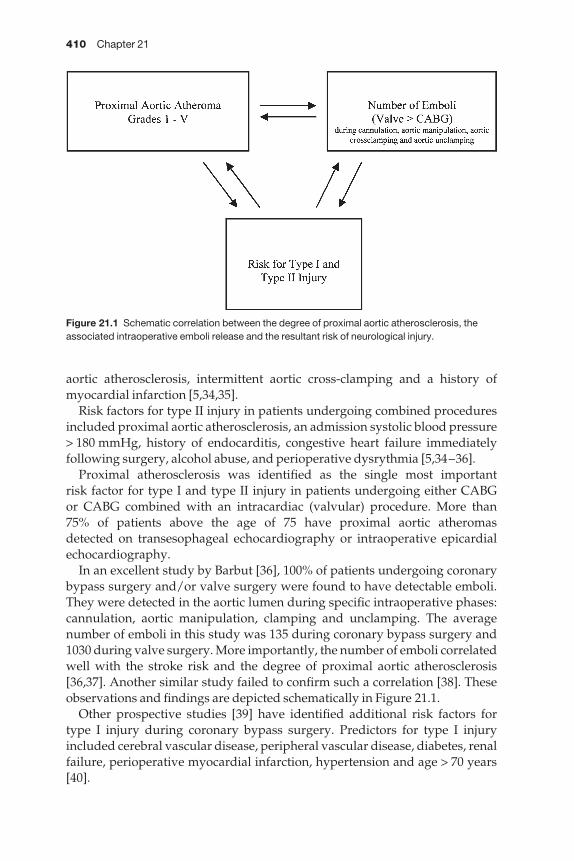
410 Chapter 21
aortic atherosclerosis, intermittent aortic cross-clamping and a history ofmyocardial infarction [5,34,35].
Risk factors for type II injury in patients undergoing combined proceduresincluded proximal aortic atherosclerosis, an admission systolic blood pressure> 180 mmHg, history of endocarditis, congestive heart failure immediately following surgery, alcohol abuse, and perioperative dysrythmia [5,34–36].
Proximal atherosclerosis was identified as the single most important risk factor for type I and type II injury in patients undergoing either CABG or CABG combined with an intracardiac (valvular) procedure. More than 75% of patients above the age of 75 have proximal aortic atheromas detected on transesophageal echocardiography or intraoperative epicardialechocardiography.
In an excellent study by Barbut [36], 100% of patients undergoing coronarybypass surgery and/or valve surgery were found to have detectable emboli.They were detected in the aortic lumen during specific intraoperative phases:cannulation, aortic manipulation, clamping and unclamping. The averagenumber of emboli in this study was 135 during coronary bypass surgery and1030 during valve surgery. More importantly, the number of emboli correlatedwell with the stroke risk and the degree of proximal aortic atherosclerosis[36,37]. Another similar study failed to confirm such a correlation [38]. Theseobservations and findings are depicted schematically in Figure 21.1.
Other prospective studies [39] have identified additional risk factors for type I injury during coronary bypass surgery. Predictors for type I injuryincluded cerebral vascular disease, peripheral vascular disease, diabetes, renalfailure, perioperative myocardial infarction, hypertension and age > 70 years[40].
Figure 21.1 Schematic correlation between the degree of proximal aortic atherosclerosis, theassociated intraoperative emboli release and the resultant risk of neurological injury.
Neurological complications in cardiac surgery 411
Prevention of neurological injury in coronary artery and valve surgery
Preoperative prevention—the role of carotid endarterectomyThe presence of carotid disease is consistently identified as a predictor of neurological injury in cardiac surgery and is one factor that can be easilyidentified and treated preoperatively. Initial efforts to correlate carotid diseasewith the risk of type I neurological injury during cardiac surgery were focusedon the preoperative detection of carotid bruits. Reed and coworkers reportedthat the risk of type I injury during cardiac surgery was 3.9 times higher when a carotid bruit was present preoperatively [41]. Two years later, Faggliolishowed that the incidence of type I neurological injury after cardiac surgeryincreased by 9.9-fold if carotid stenoses > 75% were not addressed pre- orintraoperatively [42]. The advantages of carotid endarterectomy in the gen-eral population are well documented. Two randomized trials defined theadvantages of carotid endarterectomy compared with medical therapy forsymptomatic carotid stenosis (> 70%). In the NASCET study [43], the risk of ipsilateral stroke in 2 years was 9% for the surgical arm as opposed to 26%for the non-surgical arm. In the European Carotid Surgery Trial [44], the strokerate for the surgical arm was 10.3% compared with 16.8% for the non-surgicalarm. Two additional randomized trials also defend the advantages of carotidendarterectomy for asymptomatic patients with ≥ 60% carotid stenosis. The1993 VA Cooperative study [45] and the 1995 ACAS study showed signific-ant stroke and survival advantages in asymptomatic patients (with carotidstenosis > 70%) who had elective carotid endarterectomy [46].
How does this demonstrated efficacy of carotid endarterectomy translate tothe patient about to undergo cardiac surgery? In the only randomized study ofcombined coronary artery surgery and carotid endarterectomy in patientswith unstable angina and high-grade asymptomatic carotid stenosis, Hetzerand coworkers [47] showed that the stroke rate in combined procedures was2.8%, compared with a 14.4% for a staged approach (6.9% during initial CABGand 7.5% during the subsequent performed carotid endarterectomy).
Combined cardiac and carotid procedures were also demonstrated by Akins[48] and Daily [49] to be cost effective, with very low associated morbidity andstroke rates. A factually based paradigm emerged from the presentation anddiscussion of Dr Akins’ paper at the adult postgraduate course of the 70thAmerican Medical Association for Thoracic Surgery Meeting (New Orleans,April 16, 1999). Based on these comments and our own practice, we recom-mend [50]:1 In making our decision on a patient with coronary artery and carotid disease, we should address operatively first the more compelling lesion, heartor carotid. Poorly compensated carotid lesions (in patients with transientischemic attack (TIA), or with critically tight lesions) should be correctedbefore elective cardiac surgery. Critical cardiac disease should be correctedbefore non-compelling carotid disease.

412 Chapter 21
2 If the patient has a tight carotid lesion and unstable angina then he shouldundergo a combined operation.3 If the patient has a tight carotid lesion and a contralateral but not tightly dis-eased carotid and unstable angina, he should undergo a combined correction,followed by an endarterectomy of the less diseased side in the near future.4 In patients with unstable angina and asymptomatic high-grade carotidlesions, we proceed with CABG with systematic hypothermia (and IABP if theleft main disease present) for cerebral protection.
Intraoperative prevention of neurological injuryAortic atheromaWith the increasing use of transesophageal echocardiology (TEE), intra-operative epiaortic echocardiography (IEE) and transcranial doppler echocar-diography (TCD), it has become feasible to estimate qualitatively and quanti-tatively the presence and degree of aortic atheroma as well as the amount ofembolizing atherosclerotic debris. The presence and degree of aortic atheromahas emerged as the single most important risk factor for type I and type II neu-rological injury during cardiac injury [5,34].
Embolic neurological injury occurs mainly via embolization of atheroscler-otic debris. To a lesser degree, air embolism, clot formation and embolizationand cardiopulmonary bypass-related cerebral blood flow alterations can alsocause neurological dysfunction.
Using TEE, aortic atheromas have been graded as follows. Grade I (small tomoderate wall thickening), grade II (severe aortic wall thickening), grade III(intraluminal protrusion < 5 mm), grade IV (intraluminal protrusion > 5 mm)and grade V (mobile intraluminal atheroma). Several investigators using TCDhave identified emboli traveling through the mid-cerebral artery [37,38].Important positive correlations have been made between the number ofimaged embolizing atherosclerotic debris and incidence of type I and/or type II neurological injury in these patients. In one of these studies [36], it was prospectively determined that the presence of grade I aortic atheroma isassociated with 0% neurological type I injury as opposed to a 30% incidence in patients with grade IV or V aortic atheromas. In most cardiac surgery centers, the introduction of the aortic cannula is preceded by manual aorticpalpation and selection of the optimal cannulation site. Several well-designedstudies [51–55] have proven that 30–70% of severe aortic atheromas cannot be localized effectively with manual palpation. In a series of 1200 patients to whom intraoperative epiaortic echocardiography was applied, 231 (19.25%) were found to have grade I–IV atheromas in areas that were by palpation characterized as ‘normal’ [56]. In 27 of these patients with grade IVatheromas, the ascending aorta was replaced with no incidence of type Iinjury. Yet, this aggressive approach has not been widely applied at other institutions.
In another series of 168 patients with less significant aortic disease, applica-tion of epiaortic echocardiography resulted in technical modifications, such as

Neurological complications in cardiac surgery 413
femoral cannulation, avoidance of specific areas for aortic cross-clamping,modification in the placement of proximal graft anastomoses or institution ofretrogradeainstead of antegradeacardioplegia [54]. All of these intraoperat-ive modifications of the operative technique resulted in a significant decreasein the incidence of type I and type II injury [54].
In a series of 130 patients undergoing CABG, specific attention was paid to those patients with grade V aortic atheromas. Modifications of operativetechnique in a group of these patients again resulted in significantly lowerstroke rate [53]. Additional studies have examined the role of intraoperativetechnique modifications, made based on epiaortic echo data, on the incidenceof neuropsychological complications. The addition of transcranial Dopplerdata in these patients gave additional information regarding the number ofaortic atherosclerotic debris flowing through the mid-cerebral artery. It wasconcluded [57] that the incidence of neuropsychological complications inpatients who had smaller numbers of embolizing particles (< 100) was < 10%,as opposed to patients with a higher number of particles (> 1000) that had as agroup a 40% incidence of neuropsychological morbidity. This provided directevidence correlating the amount of embolic debris load and postoperativeneurobehavioral outcome [58]. This work and other studies have demon-strated overwhelmingly the impact of aortic debris and embolization on neurological outcome and the dramatic importance of echocardiographic evaluation.
Prevention of air embolismBesides the traditional measures and air evacuation techniques, newerdevices, extensive external filter application and technique modifications havebeen gradually introduced into daily practice, aiming at the decrease of incid-ence of type I and type II injury [59].
Examples include newer arterial cannulas with vents, insertion of venouscannulas during positive end expiratory pressure in patients with suspectedatrial septal defect (ASD) or ventricular septal defect (VSD) or other intracar-diac shunts and almost complete replacement of bubble oxygenations. Morerecently, extensive use of carbon dioxide flooding in our institution has dramatically decreased (among others) the incidence of type I injury. Further-more, avoidance of gas exchange in venous return, use of bubble detectors andmultiple arterial filters, use of closed compressible venous reservoir and non-obstructive arterial pumps have been utilized in our institution [60,61].
Prevention of thrombus formationAvoidance of thrombus formation during cardiac surgery focuses mainly on three factors: perioperative recognition of patients with a higher potentialfor coagulation, achievement, maintenance and monitoring of systemic heparinization during cardiopulmonary bypass, and research and develop-ment of less thrombogenic or thrombo-resistant synthetic materials, such asheparin-coated perfusion equipment [62–64].

414 Chapter 21
Intra-aortic filtrationA new method of intra-aortic filtration has been developed and is undergoingtesting in European centers. This intra-aortic filter (Edwards EMBOL-X®)System, Edwards Lifesciences Corp., Irvine, CA, USA) is introduced through a modified 24 Fr aortic cannula after the optimal cannulation site has beenselected by palpation, TEE or intraoperative epiaortic echocardiography.Before aortic unclamping, this filter is introduced through a parallel port of the aortic cannula and expanded to cover the entire aortic lumen. The filter isremoved with the removal of the aortic cannula [65] (Figure 21.2).
The application of this intra-aortic filter device was presented for the firsttime in the USA by Dr J.A. Navia in a case demonstration of a low neurologicalinjury risk patient that underwent coronary artery bypass grafting (Figure21.3) [66].
The same was evident in a patient that underwent an aortic valve replace-ment [67]. At the same time, Reichenspurner and coworkers presented the firstgroup of 77 patients, undergoing coronary artery bypass or valve procedures,in which the intra-aortic filter was used. The authors did not focus on the incidence of type I and type II injury. They concluded that virtually all of the
Figure 21.2 Application of an Edwards EMBOL-X® System intra-aortic filter. Courtesy of EdwardsLifesciences.
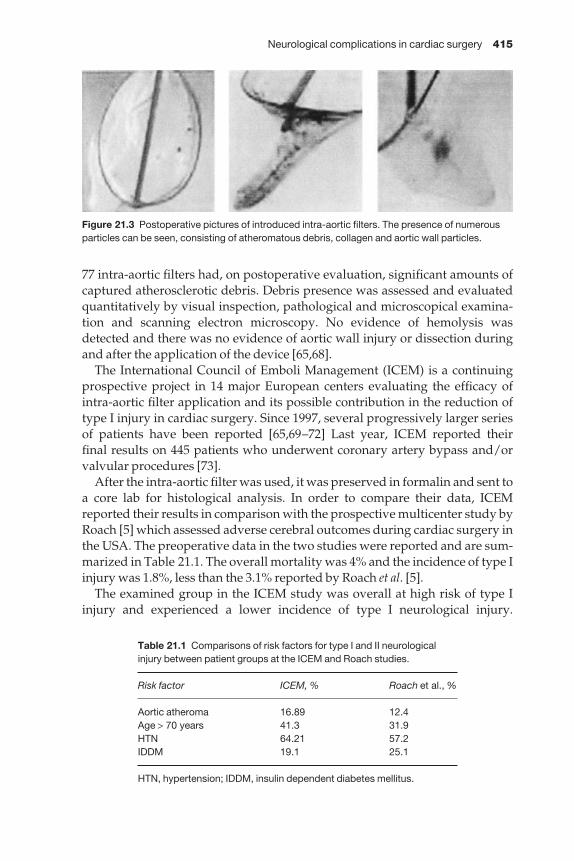
Neurological complications in cardiac surgery 415
77 intra-aortic filters had, on postoperative evaluation, significant amounts ofcaptured atherosclerotic debris. Debris presence was assessed and evaluatedquantitatively by visual inspection, pathological and microscopical examina-tion and scanning electron microscopy. No evidence of hemolysis wasdetected and there was no evidence of aortic wall injury or dissection duringand after the application of the device [65,68].
The International Council of Emboli Management (ICEM) is a continuingprospective project in 14 major European centers evaluating the efficacy ofintra-aortic filter application and its possible contribution in the reduction oftype I injury in cardiac surgery. Since 1997, several progressively larger seriesof patients have been reported [65,69–72] Last year, ICEM reported their final results on 445 patients who underwent coronary artery bypass and/orvalvular procedures [73].
After the intra-aortic filter was used, it was preserved in formalin and sent toa core lab for histological analysis. In order to compare their data, ICEMreported their results in comparison with the prospective multicenter study byRoach [5] which assessed adverse cerebral outcomes during cardiac surgery inthe USA. The preoperative data in the two studies were reported and are sum-marized in Table 21.1. The overall mortality was 4% and the incidence of type Iinjury was 1.8%, less than the 3.1% reported by Roach et al. [5].
The examined group in the ICEM study was overall at high risk of type Iinjury and experienced a lower incidence of type I neurological injury.
Figure 21.3 Postoperative pictures of introduced intra-aortic filters. The presence of numerousparticles can be seen, consisting of atheromatous debris, collagen and aortic wall particles.
Table 21.1 Comparisons of risk factors for type I and II neurologicalinjury between patient groups at the ICEM and Roach studies.
Risk factor ICEM, % Roach et al., %
Aortic atheroma 16.89 12.4Age > 70 years 41.3 31.9HTN 64.21 57.2IDDM 19.1 25.1
HTN, hypertension; IDDM, insulin dependent diabetes mellitus.
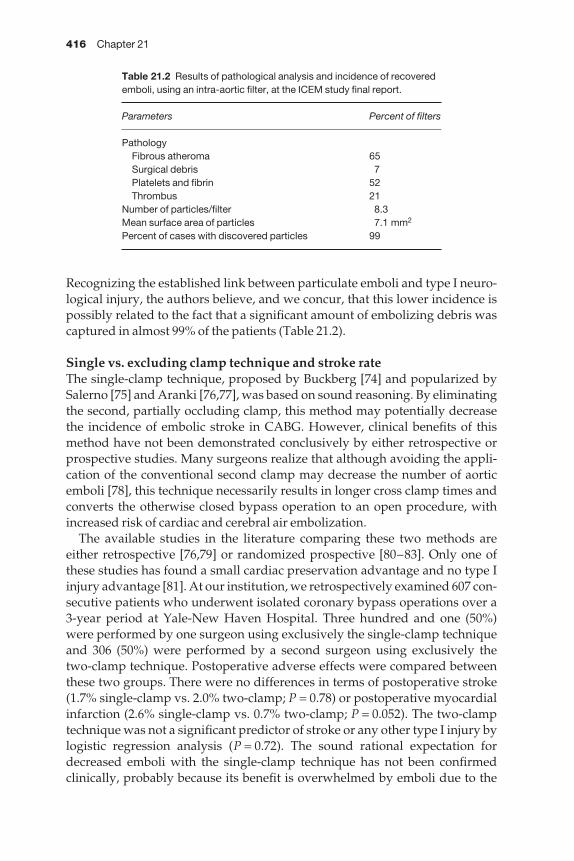
416 Chapter 21
Recognizing the established link between particulate emboli and type I neuro-logical injury, the authors believe, and we concur, that this lower incidence ispossibly related to the fact that a significant amount of embolizing debris wascaptured in almost 99% of the patients (Table 21.2).
Single vs. excluding clamp technique and stroke rateThe single-clamp technique, proposed by Buckberg [74] and popularized bySalerno [75] and Aranki [76,77], was based on sound reasoning. By eliminatingthe second, partially occluding clamp, this method may potentially decreasethe incidence of embolic stroke in CABG. However, clinical benefits of thismethod have not been demonstrated conclusively by either retrospective orprospective studies. Many surgeons realize that although avoiding the appli-cation of the conventional second clamp may decrease the number of aorticemboli [78], this technique necessarily results in longer cross clamp times andconverts the otherwise closed bypass operation to an open procedure, withincreased risk of cardiac and cerebral air embolization.
The available studies in the literature comparing these two methods areeither retrospective [76,79] or randomized prospective [80–83]. Only one ofthese studies has found a small cardiac preservation advantage and no type Iinjury advantage [81]. At our institution, we retrospectively examined 607 con-secutive patients who underwent isolated coronary bypass operations over a3-year period at Yale-New Haven Hospital. Three hundred and one (50%)were performed by one surgeon using exclusively the single-clamp techniqueand 306 (50%) were performed by a second surgeon using exclusively the two-clamp technique. Postoperative adverse effects were compared betweenthese two groups. There were no differences in terms of postoperative stroke(1.7% single-clamp vs. 2.0% two-clamp; P = 0.78) or postoperative myocardialinfarction (2.6% single-clamp vs. 0.7% two-clamp; P = 0.052). The two-clamptechnique was not a significant predictor of stroke or any other type I injury bylogistic regression analysis (P = 0.72). The sound rational expectation fordecreased emboli with the single-clamp technique has not been confirmedclinically, probably because its benefit is overwhelmed by emboli due to the
Table 21.2 Results of pathological analysis and incidence of recoveredemboli, using an intra-aortic filter, at the ICEM study final report.
Parameters Percent of filters
PathologyFibrous atheroma 65Surgical debris 7Platelets and fibrin 52Thrombus 21
Number of particles/filter 8.3Mean surface area of particles 7.1 mm2
Percent of cases with discovered particles 99
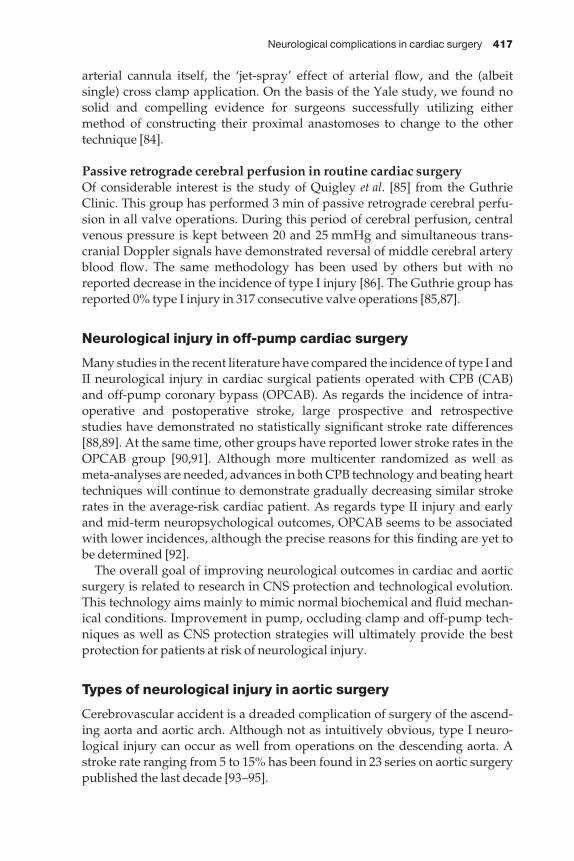
Neurological complications in cardiac surgery 417
arterial cannula itself, the ‘jet-spray’ effect of arterial flow, and the (albeit single) cross clamp application. On the basis of the Yale study, we found nosolid and compelling evidence for surgeons successfully utilizing eithermethod of constructing their proximal anastomoses to change to the othertechnique [84].
Passive retrograde cerebral perfusion in routine cardiac surgeryOf considerable interest is the study of Quigley et al. [85] from the GuthrieClinic. This group has performed 3 min of passive retrograde cerebral perfu-sion in all valve operations. During this period of cerebral perfusion, centralvenous pressure is kept between 20 and 25 mmHg and simultaneous trans-cranial Doppler signals have demonstrated reversal of middle cerebral arteryblood flow. The same methodology has been used by others but with noreported decrease in the incidence of type I injury [86]. The Guthrie group hasreported 0% type I injury in 317 consecutive valve operations [85,87].
Neurological injury in off-pump cardiac surgery
Many studies in the recent literature have compared the incidence of type I andII neurological injury in cardiac surgical patients operated with CPB (CAB)and off-pump coronary bypass (OPCAB). As regards the incidence of intra-operative and postoperative stroke, large prospective and retrospective studies have demonstrated no statistically significant stroke rate differences[88,89]. At the same time, other groups have reported lower stroke rates in the OPCAB group [90,91]. Although more multicenter randomized as well asmeta-analyses are needed, advances in both CPB technology and beating hearttechniques will continue to demonstrate gradually decreasing similar strokerates in the average-risk cardiac patient. As regards type II injury and earlyand mid-term neuropsychological outcomes, OPCAB seems to be associatedwith lower incidences, although the precise reasons for this finding are yet tobe determined [92].
The overall goal of improving neurological outcomes in cardiac and aorticsurgery is related to research in CNS protection and technological evolution.This technology aims mainly to mimic normal biochemical and fluid mechan-ical conditions. Improvement in pump, occluding clamp and off-pump tech-niques as well as CNS protection strategies will ultimately provide the bestprotection for patients at risk of neurological injury.
Types of neurological injury in aortic surgery
Cerebrovascular accident is a dreaded complication of surgery of the ascend-ing aorta and aortic arch. Although not as intuitively obvious, type I neuro-logical injury can occur as well from operations on the descending aorta. Astroke rate ranging from 5 to 15% has been found in 23 series on aortic surgerypublished the last decade [93–95].
418 Chapter 21
The same general classification of neurological injury pertinent to coronaryand valvular surgery applies to aortic surgery.
Prevention of neurological injury in aortic surgery
Type I neurological injuries in aortic surgery are mainly caused by one or moreof the following pathophysiological entities [96]:1 Systemic hypotension (especially with coexistent cerebrovascular disease).2 Embolism (air, debris).3 Reduced perfusion syndromes (in dissections).4 Inadequate cerebral protection during deep hypothermic circulatory arrest(DHCA).5 Reperfusion injury.The following will focus mainly on technical modifications for the preventionand intraoperative management of these entities.
Management of systemic hypotensionThe preoperative assessment of any cerebrovascular disease is as important inaortic surgery as in coronary or valvular surgery. Preoperative addressing ofsymptomatic or more hemodynamically significant (> 70%) asymptomaticcarotid disease is recommended, if the patient is stable and can tolerate thewaiting period between carotid endarterectomy and the aneurysm repair [96].
Preoperative arterial blood pressure patient readings constitute a usefulindicator of the blood pressure that should be maintained intraoperatively andimmediately postoperatively. Dramatically hypertensive patients may sufferat pressures of 80–120 mmHg.
Since bleeding is the most frequent etiology of hypotension in aorticsurgery, meticulous hemostasis emerges as the paramount factor for the maintenance of optimal intraoperative blood pressure. Additional hemostaticmeasures include (i) routine use of Teflon or pericardial strips for coronary(less accessible) button reinforcement, (ii) routine reinforcement of the pos-terior aortic anastomotic wall with interrupted pledgeted sutures in addition to the primary continuous suture line, (iii) wrapping of the anastomosis, particularly in cases of dissection, and (iv) utilization of the several availableglue materials.
Prevention of air or particulate embolismExperience has shown that although primary lining by thrombus is rare in the ascending aorta, atheromatous debris are common in this area and in the aortic arch. This material is easily dislodged during aortic replacementmanipulations. Patients with ascending aortic dissection usually have min-imal atherosclerosis and atheromatous embolism is of lesser magnitude. Useful techniques to minimize atheromatic debris embolization include (i)meticulous cleaning and irrigation of the open aorta, (ii) head vessel exclusion,and (iii) retrograde cerebral perfusion.
Neurological complications in cardiac surgery 419
Embolization of atheromatous debris is somewhat counterintuitive in operations of the descending aorta because the descending aorta, being downstream from the head vessels, might not be expected to be a significantsource of air or particulate matter in such operations [96]. In our experience,strokes do indeed occur with frequency in operations of the descending aorta.We believe that manipulation of the aortic arch for proximal control andfemoral artery retrograde perfusion are two important causes of type I neurological injury in descending aortic operations.
Technical modifications in aortic surgery to reduce type I neurologicalinjury from particulate or air embolism include:1 Avoidance of left atrial appendage cannulation in atrial fibrillation (Figure21.4a).2 Cannulation of the (L) superior or inferior pulmonary vein in these cases, oravoidance of cannulation entirely.3 Subclavian (instead of femoral) artery cannulation in ascending aortic pro-cedures in which descending or abdominal atheroma is detected.4 In descending aortic procedures, application of proximal cross clamp beforethe initiation of (left atrial to femoral artery) CPB and removal of the clampafter discontinuation of CPB (Figure 21.4b).5 Steep Trendelenburg positioning.6 Carotid vessel occlusion during DHCA.7 Carbon dioxide flooding of the operative field.8 Meticulous and prolonged venting during rewarming.9 Wide open de-airing through the suture line.10 Trickle flow from below, to allow the atrial tree to fill slowly, like a well.11 Repositioning of the arterial perfusion cannula from the femoral artery(used initially) to the graft itself (or to a side arm, small-caliber prefabricatedgraft) when perfusion is restarted in case of severe atherosclerotic debris (96).
Prevention of malperfusion syndromesCerebral malperfusion syndromes can present before, during and after aortic operation. For dissections, Griepp has described intraoperative cerebralmalperfusion as an ‘insidious problem with catastrophic consequences’.Fortunately, cerebral malperfusion is infrequent in aortic dissection at initialpresentation. In the unfortunate event that a patient presents to the hospitalwith cerebral malperfusion, the treatment is immediate operation withascending aortic replacement, as long as there is no evidence of completedstroke with cerebral necrosis.
Malperfusion may present intraoperatively at two district phases: at the ini-tiation of perfusion (usually via the femoral artery), and after the completion ofthe anastomoses of the ascending aortic graft when perfusion is resumed. In the first case of early intraoperative malperfusion, the femoral cannula mayhave been unintentionally misplaced in the false lumen. This can be recog-nized by a flaccid ascending aorta or head vessels after institution of perfusion.Corrective action should be taken immediately, before brain death results.
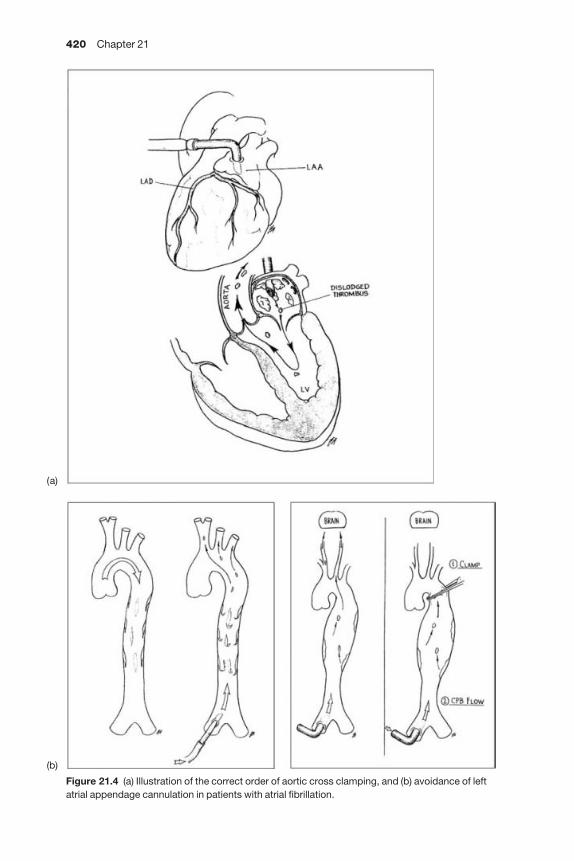
420 Chapter 21
Figure 21.4 (a) Illustration of the correct order of aortic cross clamping, and (b) avoidance of leftatrial appendage cannulation in patients with atrial fibrillation.
(b)
(a)
Neurological complications in cardiac surgery 421
Two alternative options exist. First one may cannulate the opposite femoralarteryaalthough there is sometimes no guarantee that this cannulation willrecruit the true lumen. Alternatively, we recommend the selective cannulationof the carotid arteries to ensure cerebral perfusion, with simultaneous rightradial artery blood pressure monitoring, which indicates the status of theinnominate artery perfusion.
In the case of cerebral malperfusion after completed replacement of theascending aorta for type I dissection, early TEE and transcranial Dopplerechocardiographic application can recognize and quantify cerebral malperfu-sion once the proximal and distal anastomoses are completed and circulationresumed for rewarming.
If malperfusion is detected by the anesthesiologist after unclamping the newaorta, the cannula should immediately be replaced in the graft, thus restoringantegrade cerebral blood flow by decompressing the false channel and reliev-ing the obstruction.
If cerebral malperfusion is not recognized until the ICU after the entire operation is completed, immediate carotid fenestration or grafting are indic-ated, but almost invariably with poor results and a very high incidence ofresidual incapacitating neurological type I injury.
In chronic type A dissections, inappropriate restoration of ‘single-barrel’ aortacan potentially cause a massive type I neurological injury. For acute type A dissections, we always reconstitute a single-barrel aorta by re-approximatingthe two dissected aortic wall layers. But in the case of chronic type A dis-section, the chronic double-barrel aorta must be preserved. We fenestrate thedistal flap and sew the graft to the adventitia only. By the chronic stage, important organs, including the brain and the kidneys, may be completelydependent on the false lumen for their perfusion [96].
Prevention of inadequate cerebral protection during DHCADeep hypothermia and circulatory arrest is a term used when the circulation isdeliberately suspended at pharyngeal temperatures < 20 °C. Hypothermia isachieved by cold perfusion in combination with ice packing around the headand a cooling blanket [97]. To prevent the numerous adverse reactions andtheir effects on cerebral homeostasis, numerous interventions must be under-taken. These practices include progressive vs. rapid systemic cooling [98],acid-base balance monitoring and correction [99], avoidance of hyperglycemia[100] and an arrest time of ≤ 45 min to ensure minimal cerebral side-effects. Ifperiods of ≥ 60 min are anticipated (infrequent event), one has the followingoptions: retrograde perfusion via the superior vena cava (SVC) or selectiveantegrade cerebral perfusion. If the right subclavian artery was cannulatedalready for CPB, simply resuming low flow in the arterial line and clampingacross the base of the innominate artery will restore perfusion.
The following additional cerebral protection guidelines in patients in whomDHCA was utilized have been proposed by Ergin and coworkers [101]:1 Maintenance of cerebral perfusion pressure of 40–50 mmHg (by right radialartery trace) during selective cerebral perfusion.
422 Chapter 21
2 Application of brief retrograde cerebral perfusion before antegrade perfu-sion in case of patients with a high risk of type I neurological injury (extensiveatheroma).3 Occlusion of inferior vena cava when retrograde cerebral perfusion is used.4 Avoidance of high pressures during continuous retrograde cerebral perfu-sion to avoid cerebral edema.5 Avoidance of hyperglycemia and aggressive correction of acidosis.
Retrograde cerebral perfusionRetrograde cerebral perfusion, originally described by Mills [102] and popu-larized by Ueda [103] combined with hypothermia, is an alternative methodfor brain protection during DHCA. The SVC is perfused with cold blood at apressure of 20–30 mmHg and a resultant flow of 250–800 ml/min. Numerousstudies show that only a fraction of this flow actually perfuses the brain[104–106]. Nevertheless, several investigators have demonstrated brain oxy-genation [107] and reduced type I neurological injury after aortic arch opera-tions utilizing retrograde cerebral perfusion [104,105,108].
Direct antegrade cerebral perfusionDirect antegrade cerebral perfusion was first introduced by DeBakey [109]under normothermic conditions and was associated with high mortality andhigh incidence of type I neurological injury. In theory, direct antegrade cerebral perfusion should provide the best CNS protection, especially whencombined with hypothermia. Bachet [110] renewed interest in the technique,demonstrating acceptable mortality and low incidence of type I injury (5%).Since then, multiple studies have shown benefits of direct antegrade cerebralperfusion [111–114] mainly by extending the ‘safe’ interval of DHCA for pro-cedures on the aortic arch. Severe drawbacks of this method are its obligatorymanipulation of the head vessels (with increased risk of embolization, walltrauma, or even dissection), the variability of perfusion protocols, and thecumbersome nature of the lines and cannulas. In any configuration the methodrelies on an intact circle of Willis for full brain perfusion. Despite favorableincidence of reported type I neurological injuries, direct antegrade cerebralperfusion is not universally practiced because of the enhanced potential of the dangers inherent in direct vessel manipulation and the cumbersome apparatus.
Regarding the choice between deep hypothermic circulatory arrest, retro-grade cerebral perfusion and direct antegrade cerebral perfusion, it is safe tosay that knowledgeable experts prefer each technique. No advantage of oneover another has been documented.
Prevention of stroke in aortic surgeryathe Yale experienceWe reviewed 317 thoracic aortic operations performed at Yale-New HavenHospital with regard to incidence of stroke [115]. From these procedures, 206(64.9%) were performed electively and 97 (35.1%) emergently. The overall incid-ence of stroke was 7.3%. When classified as emergent, the stroke incidence
Neurological complications in cardiac surgery 423
was 16.5% as opposed to 3.4% in elective procedures. When classified asascending vs. descending aortic procedures, the stroke rate was 6.9% and8.1%, respectively. Univariate analysis showed that only a preoperative his-tory of diabetes was a significant preoperative risk factor for stroke. Of all thestrokes encountered, 65.2% were embolic, 13% were ischemic and 13% werehemorrhagic. Patients with a stroke remained intubated an average of 8.9 dayslonger than those without a stroke (12.7 vs. 3.8 days) and stayed 17.1 dayslonger in the hospital after the operation, than those without (31.4 vs. 14.3 days).Long-term survival in stroke patients was dismal. Because intraoperativeemboli were the overwhelming source of stroke in our study, we focusedintensively on anti-embolic precautions and modifications to our operativetechnique. The following specific technical alterations were incorporated andare recommended:1 Mobilizationaeven mobilization for operations on severely diseaseddescending aortas can liberate debris. The aortic arch should be gently mani-pulated for proximal control in descending aortic operations.2 Debridementaon severely diseased aortic cuffs before anastomosis andrestoration of circulation, meticulous debridement is essential.3 Echocardiographyatransesophageal and epiaortic echocardiographic selec-tion of the aortic cannulation site. In patients with severe, mobile atheroma of the descending aorta, avoidance of femoral cannulation and alternative perfusion through the subclavian or axillary artery are recommended.4 Carbon dioxide flooding of the operative field, which displaces air and isquickly absorbed in case of air embolism, is strongly recommended.5 Order of clamping in descending aortic surgery is paramount. We recom-mend the application of the proximal clamp before the initiation of femoralperfusion and similarly discontinuation of perfusion before the release of theproximal clamp. In this way, liberated debris is obligated away from the brain.6 Avoidance of the left atrium (LA) in atrial fibrillation. In patients with atrialfibrillation, the appendage may contain clot. It is best to avoid cannulation ofsuch an appendage for LA-femoral bypass. The clamp and sew technique of femoral artery-femoral vein bypass may be preferable.
We observed a significant decrease in stroke rate for operations on thedescending aorta in the time period after the embolic nature of stroke was documented and systemic anti-embolic measures instituted [115].
Mechanisms of spinal cord injury in aortic surgery
Risk factors for spinal cord ischemia during aortic surgeryParaplegia and parparesis represent a devastating neurological complicationin thoracic and thoraco-abdominal aortic surgery, and their incidence in thethoraco-abdominal literature varies from 4 to 38% [116].
Factors that affect these percentages are total aortic clamp time, extent of aortareplaced and the presence or absence of dissection [117]. From an operativestandpoint, patients with few or no patent segmental arteries in the replacedaortic segment (especially in the T8–L2 region) have better neurological

424 Chapter 21
outcome, especially when atrio-femoral bypass is used [118]. Depending onthe Crawford classification, the average incidence of spinal cord injury is11–13% for type I, 28–30% for type II, 6–8% for type III, and 3–5% for type IV.Operation for extensive acute type B aortic dissection carries an exceptionallyhigh risk of paraplegia or paraparesis.
More recently, a biochemically medicated reperfusion spinal cord injury hasbeen identified to play an important role in a subgroup of patients whodevelop deficits soon after surgery [119].
Pathophysiology of spinal cord injuryThe occurrence and the degree of spinal cord injury is dependent upon:1 Duration of reduced blood flow.2 Presence of collateral flow (with atrio-femoral bypass), or steal phenomena.3 Neuronal metabolic rate.4 Rate and amount of CSF pressure increase.5 Rate and intensity of reperfusion injuries (neutrophil glutamate action).
The exact pathophysiological cellular and subcellular mechanisms that are involved in spinal cord injury have not been completely elucidated. Theamino acid glutamate has emerged as a basic mediator with an important role in acute spinal cord injury during ischemia and reperfusion [120]. Theamino acids glutamate and aspartate are widely spread spinal cord neuro-transmitters. Despite that, increased intraneuronal levels of these two aminoacids have been shown to be highly neurotoxic to hypoxic or anoxic neurons.Under normal conditions, a well-perfused spinal cord has protective mech-anisms to keep intraneuronal aspartate and glutamate levels to a minimum. In hypoxia, anoxia, or spinal cord trauma or severe inflammation, the energy(ATP)-dependent neuronal reabsorption systems fail and the intraneuronalglutamate level rises to a three to four-fold level even for 60–90 min afterreperfusion. Glutamate exerts its action through three classes of receptors. The NMDA classes of receptors are membrane receptors connected toCa2+/Na+ channels and glutamate action to these receptors leads to rapidinflux of Ca2+, Na+ and Cl– into the neuronal cell with resulting intracellularedema and lysis. A delayed secondary form of spinal cord neuronal cell injuryresults from the rapid intracellular rise in Ca2+ concentration [121]. Ca2+
concentrations lead to phospholipid membrane disruption, arachidonic acidrelease and irreversible mitochondrial injury [122]. Specific pharmacologicalinhibitors of the above events are being developed and tested in animal models. These substances are either competitive or non-competitive inhibitorsand blockers of the NMDA receptors. Competitive blockers have in generalreduced in vivo potential because of their inability to effectively cross the blood–brain barrier. In contrast, non-competitive NMDA blockers arelipophilic and easily cross the blood–brain barrier with resultant high con-centrations at the site of the injury [120]. Dextrophan has been shown toreverse glutamate-mediated neuronal injury in neuronal cell cultures and also in rabbit models.
Similar results have been achieved with the administration of MK-801 in
Neurological complications in cardiac surgery 425
mice. In other studies, in patients under hypothermic circulatory arrest,besides glutamate, nitric oxide seems to be highly neurotoxic [121,122].
Spinal cord protection during aortic surgery
The currently used clinical or evolving laboratory techniques for spinal cordprotection include the following:1 Pharmacological.2 Mechanical.
(a) CSF drainage(b) Peripheral perfusion(c) Hypothermia
(i) Systemic(ii) Local
(d) Sensory evoked potentials (SEP)/motor evoked potentials (MEP) guidedintercostal artery ligation(e) Adamkiewicz artery imaging(f) Segmental artery reimplantation (T7–LI).
Pharmacological interventionsMultiple pharmacological agents have been tested in animal and human studies. These include allopurinol, superoxide dismutase, naloxone, barbitur-ates, steroids, manitol, gangliosides, ACE inhibitors, NMDA inhibitors such as dextrophan, and MK-801 and adenosine [123]. Ongoing research suggeststhat a combination of different agents rather than a single agent may be themost effective for pharmacological protection and treatment of spinal cordinjury in the future.
MechanicalCerebrospinal fluid drainageIt is known that the decrease in spinal cord perfusion is partially due to anincrease in CSF pressure during the ischemic period. This is especially truewhen vasodilatation is used to decrease the proximal aortic pressure [124].Sodium nitroprusside is frankly contraindicated (for this reason) in aorticsurgery. In the 1960s, Blaisdell, Cooley [125] and Miyamoto [126] introducedCSF drainage during aortic cross clamping. Although these initial studies wereoptimistic, the efficacy of CSF drainage has not been tested alone. Favorableresults have been reported regarding CSF drainage in combination with nalox-one infusion [126] or the use of atriofemoral bypass [127] or intrathecalpapaverin injection [118,128].
At our institution, CSF drainage is routinely employed for thoracic and thor-acoabdominal aneurysms intraoperatively and for 48 h postoperatively. Wetry to maintain an intrathecal pressure of < 10 Torr.
Peripheral perfusionThe high incidence of neurological injury during and after repairs for
426 Chapter 21
Crawford type I and type II thoracoabdominal aneurysms has resulted in theapplication of partial (atriofemoral) bypass during the repair of theseaneurysms by the majority of reporting groups. Left atrial to femoral arterybypass is routinely used in our institution in these cases with mild hepariniza-tion and distal flow of 2.5–3.5 l. In the reported series, partial bypass is com-bined with CSF drainage [118,129] or concurrent aggressive reattachment oflower thoracic and upper lumbar arteries. This is our policy. We prefer a‘cobrahead’ technique for safe, expedient intercostal reimplantation.
HypothermiaHypothermia reduces metabolic demands at a cellular level. A 60% reductionin spinal cord metabolic rate has been observed in local hypothermia of28–30°C. Hypothermia also increases spinal cord tolerance to ischemia bydecelerating the membrane degeneration process, influx of Ca2+ ions, ATPstorage depletion, and enzyme deactivation rate.
There are four described hypothermia techniques aiming at reducing spinalcord injury.
Total hypothermia with cardiopulmonary bypass Total hypothermia withcardiopulmonary bypass has been used with proven results in reducing post-operative paraplegia. The preferred method involves partial (atrio-femoral)bypass with mild hypothermia [31–33%] [130]. Arrhythmias are occasionallyencountered. Risk of postoperative myocardial infarction is also increased.
Local epidural cooling Local epidural cooling causing regional spinal cordhypothermia during aortic cross clamping has been effective in preventingspinal cord injury in animal models [131–133]. This technique has the mainadvantage of avoiding the undesirable side-effects of systemic hypothermia.The potential theoretical disadvantage of this method is that epidural adminis-tration of a cold solution could potentially cause a sharp rise in CSF pressure.Davidson and coworkers [133] have reported favorable results using this protection technique in eight patients with no adverse spinal cord results.
Local aortic cold solution infusion Local aortic cold solution perfusion at anisolated aortic segment that gives vessels to the spinal cord has been utilized inanimal models The main disadvantage of this method is that it incorporates a period of aortic perfusion during which the aorta is closed, with resultantprolongation of ischemia time and operation. There are no current clinicalapplications of this method today.
Hypothermic circulatory arrest Hypothermic circulatory arrest was initiallyreported by Crawford and coworkers [134] in the late 1980s. Swensson and coworkers reported on 656 patients with a mean circulatory arrest time of 31 min. This study involved patients who had several types of aortic pathology, including ascending, aortic arch, and thoracoabdominal aneurysm
Neurological complications in cardiac surgery 427
patients. This study proved that the incidence of central and spinal cord injury significantly increases after 40 min of circulator arrest. Furthermore, the overall operative mortality increases markedly after 65 min of circulatoryarrest.
In a series of 96 patients with thoracoabdominal aneurysm repair,Kouchoukos and coworkers [135] reported a mortality of 7.3% and an incid-ence of paraplegia/paraparesis of 3.3%. Hypothermic circulatory arrest maybe associated with a series of complications such as parenchymal pulmonaryhemorrhage, acute respiratory distress syndrome and other pulmonary com-plications [134,136,137]. Several experts do not routinely use hypothermic circulatory arrest and prefer to use this method when (i) there is a need for aortic arch pathology repair, or (ii) there is difficulty in aortic cross clampingbecause of either rupture or extensive atherosclerosis [138]. For descendingaortic operations we recommend deep hypothermic circulatory arrest whenproximal control and repair involve the distal aortic arch.
Evoked potentialsIt has been shown in experiments since the 1960s that stimulation of the upperthoracic spinal cord and synchronous functional monitoring is a reliable indi-cator of ischemic injury based on the changes in the evoked potentials of thelower extremity skeletal muscles (MEPs). Also, sensory potentials (SEPs) havebeen monitored. Several technical modifications have been described. These ingeneral involve modifications of neuromuscular blocking agent administra-tion by the anesthesiologist and synchronous monitoring at the lower extremi-ties. Hypothermia, anesthetics and intrathecal medications may affect evokedpotentials and have to be accounted for when interpreting the evoked poten-tial derived data [139.] When an intercostal vessel needs to be sacrificed priorto induction to CPB, one should proceed with temporary occlusion of the ves-sel, and then proceed with the division of this vessel [140]. SEP monitoringwhen employed is prudent to continue for the first 2–3 postoperative days.
SEPs are not widely employed because of the technical complexity andbecause most surgeons see no impact on management: this surgical proceduremust be performed as quickly and as safely as possible in all patients, not justthose who manifest abnormal SEPs.
Adamkiewicz artery imaging and intercostal artery reimplantationIn 90% of patients, the artery of Adamkiewicz starts between T7 and L1 and in 80% of cases this artery branches from the left segmental intercostal or thelumbar artery [141]. Although opinions vary [142], in the majority of cases intercostal artery reimplantation between T7 and L1 is performed. This reimplantation is not necessary when severe disease of the central portion ofthe descending aorta is present and has already obliterated the intercostal vessels. As regards the preoperative imaging of the Adamkiewicz artery,although technically feasible, it is time consuming and is associated with asmall incidence of paraplegia or paraparesis. Because of that, it is not widely

428 Chapter 21
used [143]. As a technical means of re-implantation of the intercostal arteries,at our institution we use a ‘cobrahead’ technique [144].
Future directions
The evolution in pump technology, pump materials, intraoperative tech-niques, neuroprotective agent development, and a more in-depth understand-ing of neuronal molecular mechanisms of injury, apoptosis and death seem tohold the key to the future decrease in the incidence in neurological injury incardiac surgery. After death itself, neurological injury is the most devastatingcomplication of cardiac surgery. With the advent of the 21st century, neurolo-gical injury remains essentially an unconquered frontier for the cardiac surgeon. The thoughtful, systematic, detailed investigation of perioperativestroke by our specialty has led to the observations and recommendationsmade in this chapter.
References
1 Gilman S. Cerebral disorders after open-heart operation. N Engl J Med 1965; 272: 489–498.2 Javid H, Tufo HM, Najafi H et al. Neurologic abnormalities following open-heart
surgery. J Thorac Cardiovasc Surg 1969; 58: 502–509.3 Mills SA. Cerebral injury in cardiac operations. Ann Thorac Surg 1993; 56: 586–591.4 Utley JR, Leyland SA, Johnson HD et al. Correlation of preoperative factors, severity of
disease, type of oxygenation, and perfusion times with mortality and morbidity of cor-onary bypass. Perfusion 1991; 6: 15–22.
5 Roach GW, Kanchuger M, Mangano CM et al. for the multicenter Study of PerioperativeIschemia Group and Ischemia Research Foundation. Adverse cerebral outcomes aftercoronary bypass surgery. N Engl J Med 1996; 335: 1857–1863.
6 Rothenburger M, Soeparwata R, Deng MC et al. Prediction of clinical outcome after car-diac surgery: the role of cytokines, endotoxin, and antiendotoxin antibodies. Shock 2001;16 (S1): 44–50.
7 Rothenburger M, Soeparwata R, Deng MC et al. The impact of antiendotoxin core anti-bodies and cytokine release and ventilation time after cardiac surgery. J Am Coll Cardiol2001; 38: 124–130.
8 Markewitz A, Lante W, Franke A, Marohl K, Kuhlmann WD, Weihold C. Alterations ofcell-mediated immunity following cardiac operations: clinical implications and openquestions. Shock 2001; 16: 10–15.
9 Sablotzki A, Mann V, Simm A, Czeslick E. Changes in the cytokine network throughescalating SIRS after heart surgery. Anas Intens Notfall Schmerz 2001; 36: 522–529.
10 Marie C, Muret J, Fitting C, Payen D, Cavaillon JM. Interleukin-1 receptor antagonistproduction during infectious and noninfectious SIRS. Crit Care Med 2000; 28: 2277–2282.
11 Hamano K, Kawamura T, Gohra H et al. Stress caused by minimally invasive cardiacsurgery versus conventional cardiac surgery: incidence of SIRS. W J Surg 2001; 25: 117–121.
12 Vallely MP, Bannon PG, Kritharides L. The systemic inflammatory response syndromeand off pump surgery. Heart Surg For 2001; 4: 7–13.
13 Boeken U, Feindt P, Mohan E et al. Post-perfusion syndrome and disturbed microcircula-tion after cardiac surgery: the role of angiotensin-converting enzyme inhibitors. ThoracCardiovasc Surg 1999; 47: 347–351.
Neurological complications in cardiac surgery 429
14 Boeken U, Feindt P, Zimmermann N et al. Increased preoperative CRP-values withoutsigns of an infection and complicated course after cardiopulmonary bypass operations.Eur Jr Cardiothorac Surg 1998; 13: 541–545.
15 Furunaga A, Tsuboi H, Itoh H et al. Significance of SIRS at cardiopulmonary bypass. J JapAss Thorac Surg 1996; 44: 790–794.
16 Agnilar MJ, Gerbone F, Hill J. Neuropathologic complications of cardiac surgery. J ThoracCardiovasc 1971; 61: 676–685.
17 Sotaniemi KA. Brain damage and neurological outcome after open-heart surgery. JNeurol Neurosurg Psychiatry 1980; 43: 127–135.
18 Shaw PJ, Bates D, Cartlidge NEF et al. An analysis of factors predisposing to neurologicalinjury in patients undergoing coronary bypass operations. Q R Med 1989; 267: 633–646.
19 Levy DE, Bates D, Carponna JJ et al. Prognosis in non-traumatic coma. Ann Intern Med1981; 94: 293–302.
20 Shaw PJ, Bates D, Cartlidge NEF et al. Neuro-ophthalmological complications of cor-onary artery bypass graft surgery. Acta Neurol Scand 1987; 76: 1–7.
21 Magee KR. Clinical analysis of reflexes. In: Vinken PJ, Bruyn GW, eds. Handbook ofClinical Neurology, Vol. 1. Amsterdam: North Holland, 1969; 237–256.
22 Shaw PJ, Bates D, Cartlidge NEF et al. Early neurological complications of coronaryartery bypass surgery. Br Med J 1985; 291: 1384–1387.
23 Newman S. The incidence and nature of neuropsychological morbidity following car-diac surgery. Perfusion 1989; 4: 93–100.
24 Stump DA, Rogers TA, Hammon WJ et al. Cerebral emboli and cognitive outcome aftercardiac surgery. J Cardiothorac Vasc Anesthesia 1996; 10: 113–119.
25 Shaw PJ, Bates D, Cartlidge NEF et al. Neurologic and neuropsychological morbidity fol-lowing major surgery. Comparison of coronary artery bypass and peripheral vascularsurgery. Stroke 1987; 18: 700–707.
26 Stump D, Newman S, Coker L et al. Persistence of neuropsychol deficits followingCABG. Anesthesiol 1990; 73: A113.
27 Stump DA, Hart S, Ruby BJ et al. New neuropsychol deficits one month following CABG.Anesth Anal 1994; 78: 5419.
28 Rabiner CJ, Willner AE, Fishman J. Psychiatric complications following coronary bypasssurgery. J Nerv Ment Dis 1975; 160: 342–348.
29 Mills S, Prough D. Neuropsychiatric complications following cardiac surgery. SeminCardiovasc Surg 1991; 3: 39–46.
30 Aberg H, Torkel. Deviations of the normal postoperative course regarding cerebral func-tion. American Association for Thoracic Surgery, Neurologic Injury during CardiacSurgery III. New Orleans, April 16, 1999.
31 Morin JE, Lang R, Elleker MG et al. Upper extremity neuropathies following median ster-notomy. Ann Thorac Surg 1982; 34: 181–185.
32 Lederman RJ, Breuer AC, Hanson MR et al. Peripheral nervous system complications ofcoronary artery bypass graft surgery. Ann Neurol 1982; 12: 297–302.
33 Newman MF, Wolman R, Kanchuger M et al. Multicenter preoperative stroke risk indexfor patients undergoing coronary artery bypass graft surgery. Multicenter Study ofPerioperative Ischemia (McSPI) Research Group. Circulation 1996; 94 (Suppl. II): 74–80.
34 Roach GW. Neurologic injury in cardiac surgery: incidence, risk factors and cost impact.American Association for Thoracic Surgery, Neurologic Injury during Cardiac SurgeryIII. New Orleans April 16, 1999.
35 Wolman RL, Nussmeien N, Aggarwal A et al. For the Multicenter Study of PerioperativeIschemia Group and the Ischemia Research Foundation. Cerebral injury after cardiacsurgery: identification of a group at extraordinary risk. Stroke 1999; 30: 514–522.
430 Chapter 21
36 Barbut D. Aortic atheroma. Single largest predictor of stroke in cardiac surgery.American Association for Thoracic Surgery, Neurologic Injury during Cardiac SurgeryIII. New Orleans, April 16, 1999.
37 Llinas R, Barbut D, Caplan LR. Neurologic complications of cardiac surgery. ProgCardiovasc Dis 2000; 43: 101–112.
38 Barbut D, Lo YW, Hartman GS et al. Aortic atheroma is related to outcome but not num-bers of emboli during coronary bypass. Ann Thorac Surg 1997; 64: 454–459.
39 Eugleman D, Cohn LH, Rizzo RJ. Incidence and predictors of transient ischemic attachand strokes following coronary artery bypass grafting. Report and collective review.American Association for Thoracic Surgery, Neurological Injury During CardiacSurgery V, San Diego, May 5, 2001.
40 Eugleman D, Cohn LH, Rizzo RJ. Incidence and predictors of transient ischemic attachand strokes following coronary artery bypass grafting: report and collective review.Heart Surg Forum 1999; 2: 242–245.
41 Read GL, Scager GE, Picard EH et al. Stroke following coronary artery bypass surgery. NEngl J Med 1988; 319: 246–250.
42 Faggioli GL, Curl GR, Ricotta JJ. The role of carotid screening before coronary arterybypass. J Vasc Surg 1990; 12: 724–731.
43 North American Symptomatic Carotid Endarterectomy Trial Collaborations. Beneficialeffect of carotid endarterectomy in symptomatic patients with high-grade stenosis. NEngl J Med 1991; 325: 445–453.
44 European Carotid Surgery Trialists’ Collaborative Group. MRC European CarotidSurgery Trial: interim results for symptomatic patients with severe (70–90 percent) orwith mid (0–29 percent) carotid stenosis. Laucet 1991; 337: 235–243.
45 Hobson RW, Weiss DG, Fields WS et al. Efficacy of carotid endarterectomy for asymp-tomatic carotid artery stenosis. N Engl J Med 1993; 328: 221–227.
46 Executive Committee for the Asymptomatic Carotid Endarterectomy Study. Endar-terectomy for asymptomatic carotid artery stenosis. JAMA 1995; 273: 421–428.
47 Hetzer NR, Loop FD, Beven EG et al. Surgical staging for simultaneous coronary andcarotid disease. A study including prospective randomization. Vasc Surg 1989; 9:455–463.
48 Akins CW, Moncure AC, Daggett WM et al. Safety and efficacy of concomitant carotidand coronary artery operations. Ann Thorac Surg 1985; 60: 311–318.
49 Daily PO, Freeman RK, Dembitsky EWP et al. Cost reduction by combined carotidendarterectomy and coronary artery bypass grafting. J Thorac Cardiovasc Surg 1996; 111:185–193.
50 Akins CW. The case for combined carotid and coronary artery surgery. Adult CardiacSurgery Symposium. 79th Annual Meeting, American Association for Thoracic Surgery,New Orleans, April 18. 1999.
51 Davila-Roman VG, Barzilai B, Wareing TH, Murphy SF, Kouchoukos NT. Intraoperativeultrasonographic evaluation of the ascending aorta in 100 consecutive patients undergo-ing cardiac surgery. Circulation 1991; 84 (Suppl. III): 47–53.
52 Ribakove GH, Katz ES, Galloway AC et al. Surgical implications of transesophagealechocardiography to grade the atheromatous aortic arch. Ann Thorac Surg 1992; 53:758–763.
53 Katz ES, Tunick PA, Rusinek H, Ribakove G, Spencer FC, Kronzon I. Protruding aorticatheromas predict stroke in elderly patients undergoing cardiopulmonary bypass: experi-ence with intraoperative transesophageal echocardiography. J Am Coll Cardiol 1992; 20:70–77.
Neurological complications in cardiac surgery 431
54 Wareing TH, Davila-Roman VG, Barzilai B, Murphy SF, Kouchoukos NT. Managementof the severely atherosclerotic ascending aorta during cardiac operations. J ThoracCardiovasc Surg 1992; 103: 453–462.
55 Nicolosi AC, Aggarwai A, Almassi GH, Olinger GN. Intraoperative epiaortic ultrasoundduring cardiac surgery. J Card Surg 1996; 11: 49–55.
56 Wareing TH, Davila-Roman VG, Daily BB et al. Strategy for the reduction of stroke incid-ence in cardiac surgical patients. Ann Thorac Surg 1993; 55: 1400–1407.
57 Pugsley W, Klinger L, Paschalis C, Treasure T, Harisson M, Newman S. The impact ofmicroemboli during cardiopulmonary bypass on neuropsychological functioning. Stroke1994; 25: 1393–1399.
58 Murkin JM. Methods of stratifying patients at risk for neurological injury: visualizing theaorta in cardiac surgery. In: Neurological Injury During Cardiac Surgery III. MobilizingMultidisciplinary Resources. New Orleans, April 16, 1999; 35–39.
59 Tovar EAI, Campo C, Bosari A et al. Postoperative management of cerebral air embolism.Ann Thorac Surg 1995; 60: 1138–1142.
60 Mueller X, Tevaearai H, VanNess K et al. Air trapping ability of the Spiral GoldTM mem-brane oxygenator. Perfusion 1998; 13: 53–57.
61 Von Segesser LK, Ruchat P. Reduction of embolus production and prevention of neuro-logic injury. In: Neurologic Injury During Cardiac Surgery IV. Mobilizing MultidisciplinaryResources. Glascow, Scotland, September 4, 1999; 18–21.
62 Ruchat P, Bogousslawsky J, Hurni M et al. Systematic surgical closure of patent foramenovale in selected patients with cerebrovascular events due to paradoxical embolism. EurJ Cardiothorac Surg 1997; 11: 824–827.
63 Von Segesser LK, Weiss B, Pasic M et al. Risk and benefit of low systematic hepariniza-tion during open heart operations. Ann Thorac Surg 1994; 58: 391–398.
64 Von Segesser LK. Rationale for surface modification of arterial filter media. In: NeurologicInjury During Cardiac Surgery III. Mobilizing Multidisciplinary Resources. New Orleans,April 16, 1999; 44–45.
65 Reichenspruner H. Intraaortic filtration captures significant particulate debris duringcardiac surgery. In: Neurologic Injury During Cardiac Surgery III. Mobilizing Multidisciplin-ary Resources. New Orleans, April 16, 1999; 46–49.
66 Navia JA. Intraaortic filtration. Case demonstration of effective capture of particulateemboli. In: Neurologic Injury During Cardiac Surgery III. New Orleans: AmericanAssociation for Thoracic Surgery, April 16, 1999.
67 Navia JA. Video demonstration of a new surgical method of intraaortic filtration duringcardiopulmonary bypass. In: Neurologic Injury During Cardiac Surgery III. A Call to Arms.Washington, DC: May 5, 1988.
68 Reichenspurner H, Navia JA, Berry G et al. Particulate emboli capture by an intraaorticfilter device during cardiac surgery. J Thorac Cardiovasc Surg 2000; 119: 233–241.
69 Reichenspurner H. Arterial filtration during cardiac surgery. Report of the first series of patients. In: Neurologic Injury During Cardiac Surgery I. American Association forThoracic Surgery Meeting, 1997.
70 Reichenspurner H. Validating emboli management during cardiac surgery: initial clinicalexperience with a new aortic filter device. A feasibility study. In: Neurologic Injury DuringCardiac Surgery II. A Call to Arms. American Association for Thoracic Surgery Meeting, 1998.
71 Moritz A. International Council for Emboli Management (ICEM): a prospective observa-tional studyathe Frankfurt experience. In: Neurologic Injury During Cardiac Surgery III.Mobilizing Multidisciplinary Resources. American Association for Thoracic SurgeryMeeting, 1999.
432 Chapter 21
72 Wimmer-Greineker G, Gerber J, Dietrich M et al. Extraction of particulate emboli duringcardiac surgery: International Council of Emboli Management Study Group Report. In:Neurologic Injury During Cardiac Surgery IV. Emerging Consensus. American Associationfor Thoracic Surgery Meeting, 2000.
73 Reichenspurner H. Risk factors and neurologic outcomes: International Council ofEmboli Management Study Group results. In: Neurologic Injury During Cardiac Surgery.V. American Association for Thoracic Surgery Meeting, 2001.
74 Buckberg GD. A proposed solution to the cardioplegia controversy. J Thorac CardiovascSurg 1979; 77: 803–815.
75 Salerno TA. Single aortic cross-clamping for distal and proximal anastomeses in coronarysurgery: an alternative to conventional techniques. Ann Thorac Surg 1982; 33: 518–520.
76 Aranki SF, Rizzo RJ, Adams DH et al. Single-clamp technique: an important adjunct tomyocardial and cerebral protection in coronary operations. Ann Thorac Surg 1994; 58:296–303.
77 Aranki SF, Sullivan TE, Cohn LH. The effect of the single aortic cross-clamp technique on cardiac and cerebral complications during coronary bypass surgery. J Card Surg 1995;10: 498–502.
78 Barbut D, Hinton RB, Szatrowski TP et al. Cerebral emboli detected during bypasssurgery are associated with clamp removal. Stroke 1994; 25: 2398–2402.
79 Yamaguchi A, Katamura N, Kawashima M et al. Clinical preeminence of single aorticcross-clamping for proximal anastomoses in coronary artery bypass surgery. NipponKyobu Geka Gakkai Zasshi (J Jpn Assoc Thorac Surg) 1993; 41: 1194–1198.
80 Rajalin A, Kuttila K, Niinikoski J et al. Myocardial reperfusion after coronary arterybypass surgery. suture of only distal of all anastomoses with the aorta cross-clamped?Scand J Thorac Cardiovasc Surg 1995; 29: 175–180.
81 Bertolini P, Santini F, Montalbano G et al. Single aortic cross-clamp technique in coronaryartery surgery: a prospective randomized study. Eur J Cardiovasc Surg 1997; 12: 413–419.
82 Hammon JW Jr, Stump DA, Kon ND et al. Risk factors and solutions for the developmentof neurobehavioral changes after coronary artery bypass grafting. Ann Thorac Surg 1993;63: 1613–1618.
83 Musumeci F, Feccia M, MacCarthy PA et al. Prospective randomized trial of single-clamptechnique versus intermittent ischemic arrest: myocardial and neurological outcome.Eur J Cardiothorac Surg 1998; 13: 702–709.
84 Kim RW, Mariconda DC, Tellides G et al. Single-clamp technique does not protectagainst cerebrovascular accident in coronary artery bypass grafting. Eur J CardiothoracSurg 2001; 20: 127–132.
85 Quigley RL, Fuller BC, Sampson LN, Reitknecht FL. Passive retrograde cerebral perfu-sion during routine cardiac valve surgery reverses middle cerebral artery blood andreduces the risk of stroke. J Heart Valve Dis 1997; 6: 288–291.
86 Diesfeld T, Lajos TZ, Schimert G. Arterial venous bridge on cardiopulmonary bypass. J Card Surg 1994; 9: 128–130.
87 Quigley RL, Pym J, Highbloom YR et al. Passive retrograde cerebral perfusion followingroutine cardiac surgery may eliminate risk of perioperative embolic cerebral vascularaccidents. In: Neurologic Injury During Cardiac Surgery V. American Association forThoracic Surgery Meeting, San Diego, May 2001.
88 Iaco AL, Contini M, Theodori G et al. Off or on bypass? What is the safety threshold? AnnThorac Surg 1999; 68: 1486–1489.
89 Kshettry VR, Flavin TH, Emery RW, Nicoloff DM. Does multivessel, off-pump coronaryartery bypass (OPCAB) reduce postoperative morbidity? 36th Annual Meeting of theSociety of Thoracic Surgeons, Fort Lauderdale, FL, Jan 31–Feb 2, 2000.
Neurological complications in cardiac surgery 433
90 BhaskerRao B, VanHimbergen D, Edmonds HL et al. Evidence of improved cerebralfunction after minimally invasive bypass surgery. J Card Surg 1998; 13: 27–31.
91 Bergsland J, Hasnain S, Lajos TZ, Salerno TA. Elimination of cardiopulmonary bypass: aprime goal in reoperative coronary artery bypass surgery. Eur J Cardiothorac Surg 1998;14: 59–62.
92 Hernandez F, Cohn W, Baribeau YR et al. In-hospital outcomes of off-pump versus on-pump coronary bypass procedures: a multicenter experience. Ann Thorac Surg 2001;72:1528–1534.
93 Miller DC. Surgical management of aortic dissection: indications, perioperative manage-ment and long-term results. In: Doroghazi RM, Slater EE, eds. Aortic Dissection. NewYork: McGraw-Hill, 1983; 193–245.
94 Miller DC, Mitchell RS, Oyer PE et al. Independent determinants of operative mortalityfor patients with aortic dissections. Circulation 1984; 70: 1–153.
95 Griepp RB, Ergin MA, Lansman SL et al. The physiology of hypothermic circulatoryarrest. Sem Thorac Cardiovasc Surg 1991; 3: 188.
96 Elefteriades JA. Postgraduate Lecture on ‘Cerebral Protection in Aortic Surgery’: 1999American Association for Thoracic Surgery Meeting, New Orleans, April, 1999.
97 Griepp RB, Ergin MA, Lansman JL et al. The physiology of hypothermic arrest. SemThorac Cardiovasc Surg 1991; 3: 188–194.
98 Daries LK. Hypothermia: physiology and clinical use. In: Gravlee GP, Davis RF, Utley JR,eds. Cardiopulmonary Bypass. Baltimore: Williams & Wilkins, 1993; 140–150.
99 Swan H. The importance of acid-base management for cardiac and cerebral presentationduring open heart operations. Surg Gynecol Obstet 1984; 158: 391–395.
100 Ekroth R, Thompson RJ, Lincoln C et al. Elective deep hypothermia with total circulatoryarrest: changes in plasma creatine kinase BB, blood glucose and clinical variables. JThorac Caridovasc Surg 1989; 97: 30–36.
101 Ergin MA, Galla JD, Lansman SL et al. Hypothermic circulatory arrest in operations onthe thoracic aorta. Determinants of operative mortality and neurologic outcome. J ThoracCardiovasc Surg 1994; 107: 788–789.
102 Mills NL, Ochsyer JL. Massive air embolism during cardiopulmonary bypass: causes,prevention and management. J Thorac Cardiovasc Surg 1980; 80: 708–714.
103 Ueda Y, Miki S, Kusuhara K et al. Surgical treatment of aneurysm of dissection involvingthe ascending aorta and aortic arch, utilizing circulatory arrest and retrograde cerebralperfusion. J Thorac Cardiovasc Surg 1982; 82: 249–257.
104 Lytle BW, McCarthy PM, Meaney KM et al. Cardiopulmonary bypass myocardial man-agement and support techniques. J Thorac Cardiovasc Surg 1995; 109: 738–749.
105 Deep GM, Jenkins E, Bolling SF et al. Retrograde cerebral perfusion during hypothermiccirculatory arrest reduces neurologic morbidity. J Thorac Cardiovasc Surg 1995; 109:259–265.
106 de Brux JL, Subayi JB, Pegis JD, Pillet J. Retrograde cerebral perfusion. Anatomic study ofthe distribution of blood to the brain. Ann Thorac Surg 1995; 60: 1294–1302.
107 Winsborrow BG, Koslowski P, Figueiras CL et al. 31P Spectroscopic imaging of pig brainsduring circulatory arrest. Can J Appl Spect 1994; 39: 135–140.
108 Ergin MA, Griepp RB, Lansman SL et al. Hypothermic circulatory arrest and other methodsof cerebral protection during operations on the thoracic aorta. J Cardiac Surg 1994; 9: 525–532.
109 Debakey ME, Crawford ES, Cooley DA et al. Successful resection of fusiform aneurysmof aortic arch with replacement with homograft. Surg Gynecol Obstet 1957; 105: 657–701.
110 Bachet J, Guilment D, Boudot B et al. Cold cerebroplegia: a new technique for cerebralprotection during operations on the transverse aortic arch. J Thorac Cardiovasc Surg 1991;102: 85–92.
434 Chapter 21
111 Kazui T, Kimura N, Yamada O, Komatsu S. Surgical outcome of aortic arch aneurysmsusing selective cerebral perfusion. Ann Thorac Surg 1994; 57: 904–911.
112 Alamanni F, Agrifoglio M, Pompilio G et al. Aortic arch surgery: pros and cons of select-ive cerebral perfusion: a multivariate analysis for cerebral injury during hypothermic cir-culatory arrest. J Cardiovasc Surg 1995; 36: 31–39.
113 Kazui T, Yamada O, Komatsu S. Emergency graft replacement of the aortic arch for acutetype A dissection. J Cardiovasc Surg 1992; 33: 211–218.
114 Tabayashi K, Ohmi M, Togo T et al. Aortic arch aneurysm repair using selective cerebralperfusion. Ann Thorac Surg 1994; 57: 1305–1311.
115 Goldstein LJ, Davies RR, Rizzo JA et al. Stroke in surgery of the thoracic aorta: incidence,impact, etiology and prevention. J Thorac Cardiovasc Surg 2001; 122: 935–945.
116 Panneton JM, Hollier LH. Basic data underlying clinical decision making. Section d. AnnVasc Surg 1995; 9: 503.
117 Coselli JS. Thoracoabdominal aortic aneurysms: experience with 372 patients. J Card Surg1994; 9: 638–643.
118 Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HI. Experience with 1509 patientsundergoing thoracoabdominal aortic operations. J Vasc Surg 1993; 17: 357–370.
119 Olney JW, Ho OL, Rhee V et al. Neurotoxic effects of glutamate. N Engl J Med 1973; 289:374–375.
120 Kern JA. Mechanisms of spinal cord injury. In: Adult Cardiac Surgery Symposium. 79thAnnual Meeting, American Association for Thoracic Surgery, New Orleans, April 18–21,1999.
121 Brock MV, Blue ME, Lowenstein CJ et al. Induction of neuronal nitric oxide followinghypothermic circulatory arrest. Ann Thorac Surg 1996; 62: 313–320.
122 Tseng EE, Brock MV, Lange MS et al. Neuronal nitric synthase inhibition reduces neu-ronal apoptosis after hypothermic circulatory arrest. Ann Thorac Surg 1997; 64: 639–647.
123 Swensson LG. New and future approaches for spinal cord protection. Semin ThoracCardiovasc Surg 1997; 9: 18–33.
124 Gelman S, Reves JG, Fowler K et al. Regional blood flow during aortic crossclamping ofthe thoracic aorta and infusion of sodium nitroprusside. J Thorac Cardiovasc Surg 1983; 85:287–293.
125 Blaisdell FW, Cooley DA. The mechanisms of paraplegia after temporary thoracic aorticocclusion and its relationship to spinal fluid pressure. Surgery 1962; 51: 351–355.
126 Miyamoto K. A new and simple method of preventing spinal cord damage followingtemporary occlusion of the thoracic aorta by draining the cerebrospinal fluid. J CardiovascSurg 1960; 16: 188–199.
127 Safi HI. Neurologic deficit in patients at high risk with thoracoabdominal aorticaneurysms: the role of cerebral spinal fluid drainage and distal aortic perfusion. J VascSurg 1994; 20: 343–443.
128 Mantrand-Workshop Group. Thoracoabdominal aortic aneurysms with special refer-ence to technical problems and complications. Eur J Vasc Surg 1993; 7: 725–730.
129 Safi HI, Campbell MP, Miller CC et al. Cerebral spinal fluid drainage and distal aorticperfusion decrease the incidence of neurological deficit: the results of 343 descending andthoracoabdominal aortic aneurysm repairs. Eur J Vasc Endovasc Surg 1997; 14: 118–124.
130 Frank SM, Parker SD, Rock P et al. Moderate hypothermia, with partial bypass and seg-mental sequential repair for thoracoabdominal aortic aneurysm. J Vasc Surg 1994; 19:687–683.
131 Berguer R, Porto J, Fedoronko B et al. Selective deep hypothermia of the spinal cord pre-vents paraplegia after aortic crossclamping in the dog model. J Vasc Surg 1992; 15: 62–68.
Neurological complications in cardiac surgery 435
132 Wisselink W, Becker MO, Nguyen JH et al. Protecting the ischemic spinal cord duringaortic clamping: the influence of selective hypothermia and spinal cord perfusion pres-sure. J Vasc Surg 1994; 19: 788–794.
133 Marsala M, Vanicky I, Galik J et al. Panmyelic epidural cooling protects against ischemicspinal cord damage. J Vasc Surg 1994; 20: 304–310.
134 Crawford ES, Coselli JS, Safi HJ. Partial cardiopulmonary bypass, hypothermic circulat-ory arrest and posteriolateral exposure for thoracic aortic aneurysm operation. J ThoracCardiovasc Surg 1987; 94: 824–831.
135 Rokkas CK, Kouchoukos NT. Profound hypothermia with spinal cord protection inoperations on the descending thoracic and thoracoabdominal aorta. Semin ThoracCardiovasc Surg 1998; 10: 57–60.
136 Szempetery S, Crisler C, Grinnan GLB. Deep hypothermic arrest and left thoracotomyfor repair of difficult thoracic aneurysms. Ann Thorac Surg 1993; 55: 830–833.
137 Safi HI, Miller CC III, Subramanian MH et al. Thoracic and thoracoabdominal aorticaneurysm repair using cardiopulmonary bypass, profound hypothermia, and circulat-ory arrest via left side of the chest incision. J Vasc Surg 1998; 28: 591–598.
138 Coselli JS. Left atrial to femoral bypass vs circulatory arrest. In: Adult Cardiac SurgerySymposium. 79th Annual Meeting, American Association for Thoracic Surgery, NewOrleans, April 18–21, 1999.
139 Svensson LG. Commentary on the DeHaan and colleagues: efficacy of the transcranialmotor evoked myogenic potentials to detect spinal cord ischemia during operations forthoracoabdominal aneurysms. J Thorac Cardiovasc Surg 1997; 113: 100–101.
140 Galla JD, Ergin MA, Sadeghi AM et al. A new technique using somatosensory evokedpotential guidance during descending and thoracoabdominal aortic repairs. J Card Surg1994; 9: 662–667.
141 Svensson LG, Crawford ES. Cardiovascular and Vascular Disease of the Aorta. Philadelphia:W.B Saunders, 1997.
142 Griepp RB, Ergin MA, Galla JD et al. Looking for the artery of Adamkiewicz: a quest to minimize paraplegia after operations for aneurysms of the descending thoracic andthoracoabdominal aorta. J Thorac Cardiovasc Surg 1996; 112: 1202–1213.
143 Svensson LG. Intraoperative identification of spinal cord blood supply during descend-ing and thoracoabdominal aortic repairs. J Thorac Cardiovasc Surg 1996; 112: 1455–1461.
144 Elefteriades JA, Coady MA, Nikas DJ, Kopf GS, Gusberg RJ. ‘Cobrahead’ graft for inter-costal artery implantation during descending aortic replacement. Ann Thorac Surg 2000;69: 1282–1284.

Index
Note: page numbers in italics refer to figures, those in bold refer to tables.
alveolopleural fistula 77–8aminopyrine breath test 162amiodarone 57, 274analgesia
antireflux surgery 199chest wall reconstruction 157epidural 94, 119lung volume reduction procedures
118–19, 121postoperative optimization 38thoracic surgery 252
ancrod 302anemia correction 391aneurysmal disease 349, 351, 355, 356, 358,
364CSF drainage 425infected 353thoracic aorta 355, 425thoracoabdominal aorta 349, 355, 356, 358
CSF drainage 425hypothermic circulatory arrest 426–7repair 425–6
angina, unstable 412angiotensin converting enzyme (ACE) 315annuloplasty 377
Carpentier–Edwards 380–1Cosgrove 381DeVega 380Kay–Reed measured 376Puig–Massana 381ring size 378
antibioticsbronchopleural fistula 81, 82pneumonia 395, 396
nosocomial 120postoperative 39
thoracotomy wound infections 29–30anticoagulation
cardiopulmonary bypass 300–5oral 164reversal 303–5
antidiuretic hormone (ADH) 314antifibrinolytic therapy 305–6
aortic surgery 360antiplatelet therapy 399antireflux surgery 183–200
analgesia 199bleeding 197
437
abdominal herniation 150abscess, subphrenic 191achalasia 186
pneumatic dilatation 209undiagnosed in antireflux surgery 186
activated clotting time (ACT) 302Adamkiewicz artery imaging 427adenosine 59adrenal hormones 314adrenocorticotrophic hormone (ACTH) 314adult respiratory distress syndrome (ARDS)
396–7amiodarone 57
air embolismlung transplantation 128–9massive in cardiopulmonary bypass
293–5postoperative treatment 295, 296
prevention 413, 418–19venous 284
air leaksbronchoplasty 96chest tube 77, 78, 117hypocapnia 117intraoperative management 112–13, 114,
115–17lung volume reduction procedures 109,
112–13, 114, 115–18massive 109peri-extubation period 117persistent 75postoperative management 117–18prolonged 77–8tracheal resection 104
air swallowers 195airway
compression 233late complications in lung transplantation
132–3management 101–2measurement 101postoperative from tracheal
resection/reconstruction 103–4resistance reduction 392stenosis 132
airway pressure release ventilation 40aldosterone 315Allen test 259, 295
438 Index
antireflux surgery (cont’d)bowel dysfunction 198–9cardiopulmonary complications 194complete obstruction 197dysphagia 195–6, 196endoscopy 185esophageal injuries 191–2external fistulization 198failure 199flatulence 195gas bloat 194–5gastric perforations 192herniated wrap 195, 196, 197internal fistulization 197, 198intraoperative pitfalls 188–9leaks 198motility disorders 186operation selection 187–8outcome 183paraesophageal herniation 192–3perioperative complications 189–94postoperative complications 194–9post-thoracotomy neuralgia 199preoperative evaluation 184–6preoperative strictures 196redo 197, 199vascular injuries 190, 191visceral perforation 192
antithrombin III (ATIII) 301Anton syndrome 408anxiety disorders, preoperative 126aorta/aortic surgery 349–60
air embolism 418–19anastomotic complications 352–3antibiotic-impregnated grafts 353ascending
aneurysmal disease 349, 351atheroembolization 258calcification 364, 371replacement 273
atheroma 412–13embolization 418–19
atherosclerosis 410bleeding 418calcified 258cannulation 263–4, 287–8
air introduction 293complications 288
cardiac catheterization 354cardioplegia 323cardiopulmonary bypass 350cerebral ischemia 356–8circulatory arrest 359clamping 423coronary arteriography 353debridement 423descending 264, 423
aneurysmal disease 349cross clamp 419
double-barrel 421
emboli 410, 412, 413, 418–19intra-aortic filtration 414–16
embolizationdistal 350retrograde 351
femorofemoral bypass 359hematological complications 359–60hemostasis 418injury 236–7intramural hematoma 288local cold solution infusion 426long-term surveillance 352malperfusion syndromes 350–1mobilization 423myocardial complications 353–4neurological complications 356–9neurological injury 417–19, 420, 421–3
prevention 418–19, 420, 421–3systemic hypotension management
418partial left heart bypass 350patch repairs 273pericardial patch 273plaque 272post-stenotic dilatation 364pseudoaneurysms 352–3pulmonary complications 354–5renal dysfunction 355–6repair of friable-debrided areas 365shaggy intraluminal disease 351single-barrel 421spinal cord cooling 359spinal cord injury 423–7
mechanical interventions 425–7pathophysiology 424–5pharmacological interventions 425prevention 425–7risk factors 423–4
stroke prevention 422–3tears 273–4thoracic 354, 355
occlusion 359thoracoabdominal 349, 355, 356, 358
hypothermic circulatory arrest426–7
profound hypothermia for operations325
surgery 354thrombosis 350tube graft 274vascular access 350–2vascular complications 349–53see also aneurysmal disease
aortic archatheroembolization 258atherosclerotic disease 237profound hypothermia for operations
325reconstruction 357
aortic regurgitation 354
Index 439
aortic rootaneurysmal disease 349calcification 364de-airing 274dissection 274replacement 352–3, 363small 367–9venting 292
aortic valve/aortic valve surgery 362–9anatomy 362bioprosthetic 367–8
stented 367, 368too large 369
calcification 365combined mitral valve surgery 375–6incisions 362–3insufficiency 365pledgets 366, 367removal 365–6replacement 323–4, 366–7
small aortic root 367–9aortotomy 363–5
transverse 364–5aorto–ventriculo–septoplasty 369aprotinin 305–6, 320, 354
aortic surgery 360argatroban 302arrhythmias, post-operative 48–62
atrial 48–9, 51, 52–5, 250characteristics 48–50drug prophylaxis 56–9hemodynamic stability 59incidence 48–50influence on outcome 51mechanisms 51–6post-esophagectomy 163post-sympathectomy 250postpericardiotomy syndrome 386pulmonary artery catheter insertion 299risk factors 50–1supraventricular 48–9, 51, 52treatment 59, 60, 61–2ventricular 50, 55–8, 123, 274, 277
malignant 61see also atrial fibrillation
arterial cannulation 286–9arterial catheters, continuous blood pressure
monitoring 295, 297arteriotomy, distal 271Ashman’s phenomenon 56Aspergillus 132asthma, atelectasis 37, 38atelectasis, postoperative 36–9, 390, 392–4
absorption 392bronchoplasty 99cardiopulmonary bypass 316–17compressive 392esophageal resection 167etiology 69fibrotic structures 97
lobar torsion differential diagnosis 87management 37–9mediastinal surgery 251passive 392predisposing factors 392preoperative conditioning 391prevention 69, 317pulmonary resection 67, 68, 69, 70recurrent 393susceptibility 36–7thoracoscopy 143treatment 69
atherosclerotic diseaseaorta 410aortic arch 237
atrial fibrillation 48, 51, 52–3, 54electrical cardioversion 62flecainide 58left atrial cannulation avoidance 419,
420left atrium avoidance 423lung volume reduction 123, 124mediastinal surgery 250–1
atrial flutter 53–4atrial natriuretic factor 315atrial premature contractions 52, 53atrial tachycardia, multifocal 55atrioventricular groove 370
hemorrhage/hematoma 375atrioventricular node 52
block 53conduction depression 61refractory 52
atrium, rightinner wall puncture 325venous cannulas 284
axillary artery cannulation 289azygos vein tears 236
Babinski reflex, bilateral 408balloon dilating systems 202, 203, 222
achalasia 209barotrauma 402Barrett’s esophagus 185, 196Belsey Mark IV repair 187, 189, 190, 191
internal fistulization 198post-thoracotomy neuralgia 199
Belsey’s artery 191Bioglue® 365blindness, cortical 408blood
autologous predonation 306, 308scavenging 291ultrafiltration 307
blood pressurearterial 315continuous monitoring 295, 297
blood product transfusion 305, 307reduction 306–9trigger points 309
440 Index
blood transfusionautotransfusion of shed mediastinal
blood 309avoidance of allogeneic 306–9
bone resorption 10bougies, mercury-filled 202–3brachial plexus damage 89, 409
sympathectomy 250brachiocephalic vessels, cannulation 357brain, systemic inflammatory response
320, 406bronchial anastomosis
complications in lung transplantation130–1
tension avoidance 94–5bronchial dehiscence 152bronchial fistula closure 75, 79bronchial granulation 97bronchial laceration 238bronchial stenosis 99
bronchoscopy 102bronchial stents 97, 133bronchial strictures 97, 99
bronchoscopy 102bronchiolitis, lymphocytic 133bronchiolitis obliterans/bronchiolitis
obliterans syndrome 133bronchitis, acute 111–12bronchodilators 391, 392, 393
pneumonia prevention 395bronchomalacia 132bronchoplasty 92
anesthetic management 94complication management 97–8dehiscence of anastomosis 97–8morbidity/mortality 99–100patient evaluation 93postintubation pneumonia 94surgical technique 94–7
bronchopleural fistula 77, 78–82drainage 81infection control 81management 98prevention 145treatment 80–2
bronchopulmonary secretions 38bronchoscopy
bronchoplasty patient evaluation 93bronchopleural fistula 80pleural effusion 137tracheal pathology evaluation 101, 102tracheal resection 104tracheobronchial resection 97–8tube placement 94
bronchoscopy, fiberoptic 38, 39atelectasis 70bronchial anastomotic complications 131intrapleural spaces 75
bronchospasm 391bronchovascular fistula 98
C-reactive protein 406calcium ion concentrations 424calcium levels 315–16Candida 132capillary leak 397carbon dioxide
intra-abdominal insufflation 194operative field flooding 293, 413, 419, 423respiratory failure 391, 392
carbon dioxide retention 109, 121lung volume reduction procedure 120–1
cardiac catheterization 251cardiac herniation 84–6
extrapleural pneumonectomy 150, 151–2cardiac index 275cardiac tamponade
coronary artery bypass graft 277extrapleural pneumonectomy 150postpericardiotomy syndrome 387
cardiomegaly, postpericardiotomysyndrome 386
cardioplegia 280–1antegrade 292, 322–4aorta 323aortic valve surgery 363cold solutions 322complications 321–5delivery 264, 323–4mitral valve surgery 371–2myocardial protection 322–5neurological protection 325, 413retrograde 323–4, 324–5retrograde cerebral perfusion 325techniques 281
cardiopulmonary bypass 237, 280–1acute lung injury 317–18adrenal hormones 314adult respiratory distress syndrome 396anemia toleration 307anticoagulation 300–5
monitoring 302–3antifibrinolytic therapy 305–6aortic surgery 350aortic valve surgery 362–3arterial cannulas/cannulation 286–9
aortic 286–8axillary 289femoral 288–9
arterial catheters 295, 297atrial natriuretic factor 315bleeding 305blood conservation techniques 306–9blood–surface interface 309–12calcium levels 315–16cardiotomy suction 291catheters 284cell saver 291central venous catheters 297–8central venous pressure 285cerebral hypoperfusion 320
Index 441
circuit components 281, 282, 283–93circulatory arrest 313–14complement pathways 310–11continuous positive airway pressure 393electrical failure 293endothelial cells 312failure to separate from 275–6heat exchanger 290hemodilution 313, 318hypothermia 312–14, 318
total 426lung effects 316–18lymphocytes 312magnesium levels 316massive air embolism 293–5
postoperative treatment 295, 296mechanics 281, 282, 283–93
complications 293–5metabolic consequences 314–16mitral stenosis 378mitral valve surgery 370–2monitoring 295, 297–300monocytes 312neurocognitive complications 319–20neurological complications 319–21neuroprotective agents 320neutrophils 312organ ischemic injury protection 312–14pathophysiological consequences
309–21perfusion circuit filters 318peripheral cannulation 284pH management 320–1pituitary hormones 314platelets 312potassium levels 316pulmonary artery rupture 299pulmonary edema 397pump oxygenator 289–90, 294renal effects 318–19renin–angiotensin–aldosterone axis 315rewarming 320systemic heparinization 413systemic inflammatory response 405–6thyroid hormones 315transesophageal echocardiography
299–300tricuspid valve surgery 379–80ultrafiltration of blood 307venous cannulas/cannulation 283–4,
371venous drainage 285
augmented 285–6venous reservoir 285venting of left heart 291–3
cardiopulmonary compromise 298Cardiopulmonary Risk Index (CPRI) 50cardiotomy suction 291, 307cardioversion
chemical 60, 61–2
DC synchronous electrical 60, 61semielective electrical 62
carotid disease 411–12carotid endarterectomy 258
neurological injury prevention 411–12carotid fenestration 421carotid stenosis 258Carpentier–Edwards annuloplasty 380–1cartilage resorption 10Celestin tube 206–7, 213–14cell saving 291, 307central nervous system, systemic
inflammatory response-inducedchanges 406
central venous catheters 297–8central venous pressure (CVP) 276, 285cerebral artery, middle 413
blood flow reversal 417cerebral hypoperfusion 320cerebral infarction 406–7cerebral ischemia, aortic surgery 356–8cerebral malperfusion see malperfusion
syndromescerebral perfusion
antegrade 422selective 421
retrograde 325, 357, 422passive 417
cerebral vessel embolism 407cerebrospinal fluid (CSF) drainage 425cerebrovascular accident 417
focal 407see also stroke
Chamberlain procedure seemediastinotomy, anterior
chemotherapyesophageal stents 222germ cell tumors 244, 245–6seminomas 244teratoma 244
chest tubeair leak 77, 78, 117bronchopleural fistula 81coronary artery bypass graft 278drainage of esophagectomy leak 165pneumothorax 131
chest wall defects 155chest wall reconstruction 155–9
local cancer recurrence 158with lung resection 158, 159mortality 158outcome 158–9prosthetic materials 156, 157seroma 157soft tissue reconstruction 156–7suction drains 156
chest wall resection 157atelectasis susceptibility 36
childrenaorto–ventriculo–septoplasty 369
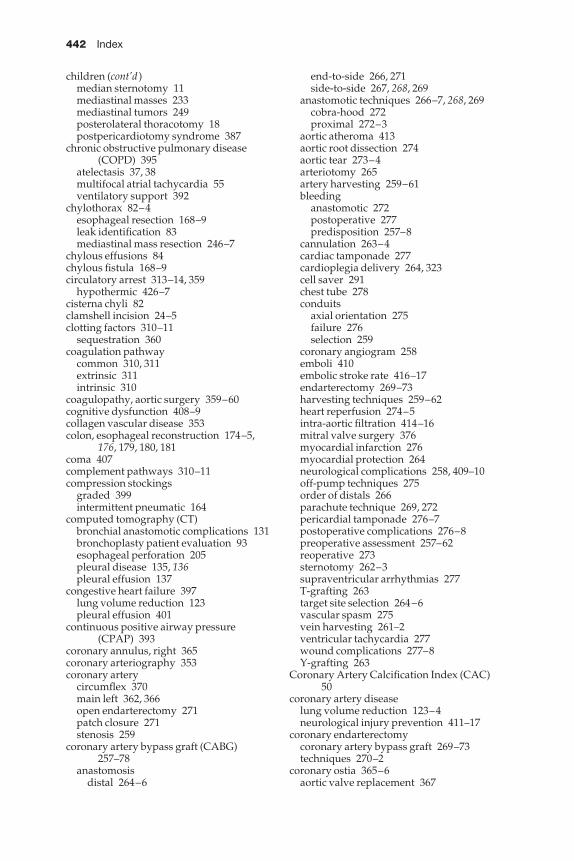
442 Index
children (cont’d)median sternotomy 11mediastinal masses 233mediastinal tumors 249posterolateral thoracotomy 18postpericardiotomy syndrome 387
chronic obstructive pulmonary disease(COPD) 395
atelectasis 37, 38multifocal atrial tachycardia 55ventilatory support 392
chylothorax 82–4esophageal resection 168–9leak identification 83mediastinal mass resection 246–7
chylous effusions 84chylous fistula 168–9circulatory arrest 313–14, 359
hypothermic 426–7cisterna chyli 82clamshell incision 24–5clotting factors 310–11
sequestration 360coagulation pathway
common 310, 311extrinsic 311intrinsic 310
coagulopathy, aortic surgery 359–60cognitive dysfunction 408–9collagen vascular disease 353colon, esophageal reconstruction 174–5,
176, 179, 180, 181coma 407complement pathways 310–11compression stockings
graded 399intermittent pneumatic 164
computed tomography (CT)bronchial anastomotic complications 131bronchoplasty patient evaluation 93esophageal perforation 205pleural disease 135, 136pleural effusion 137
congestive heart failure 397lung volume reduction 123pleural effusion 401
continuous positive airway pressure(CPAP) 393
coronary annulus, right 365coronary arteriography 353coronary artery
circumflex 370main left 362, 366open endarterectomy 271patch closure 271stenosis 259
coronary artery bypass graft (CABG)257–78
anastomosisdistal 264–6
end-to-side 266, 271side-to-side 267, 268, 269
anastomotic techniques 266–7, 268, 269cobra-hood 272proximal 272–3
aortic atheroma 413aortic root dissection 274aortic tear 273–4arteriotomy 265artery harvesting 259–61bleeding
anastomotic 272postoperative 277predisposition 257–8
cannulation 263–4cardiac tamponade 277cardioplegia delivery 264, 323cell saver 291chest tube 278conduits
axial orientation 275failure 276selection 259
coronary angiogram 258emboli 410embolic stroke rate 416–17endarterectomy 269–73harvesting techniques 259–62heart reperfusion 274–5intra-aortic filtration 414–16mitral valve surgery 376myocardial infarction 276myocardial protection 264neurological complications 258, 409–10off-pump techniques 275order of distals 266parachute technique 269, 272pericardial tamponade 276–7postoperative complications 276–8preoperative assessment 257–62reoperative 273sternotomy 262–3supraventricular arrhythmias 277T-grafting 263target site selection 264–6vascular spasm 275vein harvesting 261–2ventricular tachycardia 277wound complications 277–8Y-grafting 263
Coronary Artery Calcification Index (CAC)50
coronary artery diseaselung volume reduction 123–4neurological injury prevention 411–17
coronary endarterectomycoronary artery bypass graft 269–73techniques 270–2
coronary ostia 365–6aortic valve replacement 367
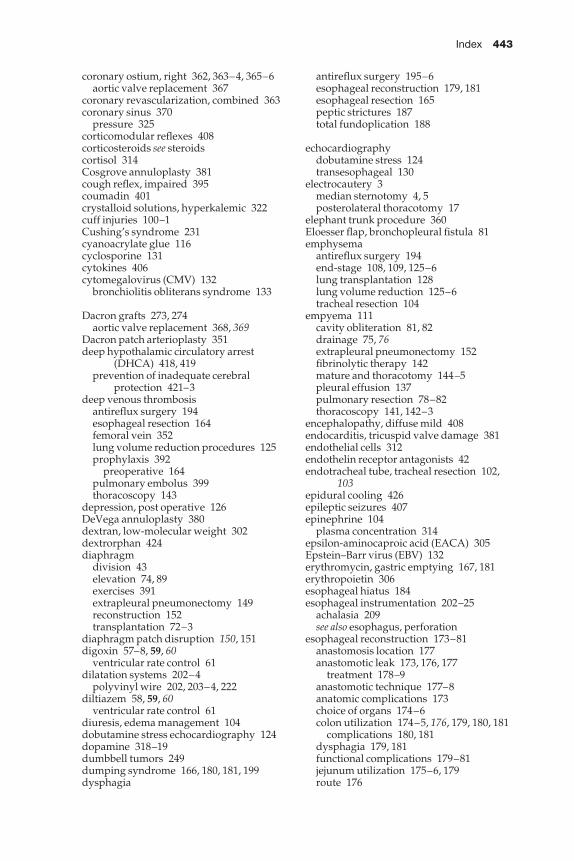
Index 443
coronary ostium, right 362, 363–4, 365–6aortic valve replacement 367
coronary revascularization, combined 363coronary sinus 370
pressure 325corticomodular reflexes 408corticosteroids see steroidscortisol 314Cosgrove annuloplasty 381cough reflex, impaired 395coumadin 401crystalloid solutions, hyperkalemic 322cuff injuries 100–1Cushing’s syndrome 231cyanoacrylate glue 116cyclosporine 131cytokines 406cytomegalovirus (CMV) 132
bronchiolitis obliterans syndrome 133
Dacron grafts 273, 274aortic valve replacement 368, 369
Dacron patch arterioplasty 351deep hypothalamic circulatory arrest
(DHCA) 418, 419prevention of inadequate cerebral
protection 421–3deep venous thrombosis
antireflux surgery 194esophageal resection 164femoral vein 352lung volume reduction procedures 125prophylaxis 392
preoperative 164pulmonary embolus 399thoracoscopy 143
depression, post operative 126DeVega annuloplasty 380dextran, low-molecular weight 302dextrorphan 424diaphragm
division 43elevation 74, 89exercises 391extrapleural pneumonectomy 149reconstruction 152transplantation 72–3
diaphragm patch disruption 150, 151digoxin 57–8, 59, 60
ventricular rate control 61dilatation systems 202–4
polyvinyl wire 202, 203–4, 222diltiazem 58, 59, 60
ventricular rate control 61diuresis, edema management 104dobutamine stress echocardiography 124dopamine 318–19dumbbell tumors 249dumping syndrome 166, 180, 181, 199dysphagia
antireflux surgery 195–6esophageal reconstruction 179, 181esophageal resection 165peptic strictures 187total fundoplication 188
echocardiographydobutamine stress 124transesophageal 130
electrocautery 3median sternotomy 4, 5posterolateral thoracotomy 17
elephant trunk procedure 360Eloesser flap, bronchopleural fistula 81emphysema
antireflux surgery 194end-stage 108, 109, 125–6lung transplantation 128lung volume reduction 125–6tracheal resection 104
empyema 111cavity obliteration 81, 82drainage 75, 76extrapleural pneumonectomy 152fibrinolytic therapy 142mature and thoracotomy 144–5pleural effusion 137pulmonary resection 78–82thoracoscopy 141, 142–3
encephalopathy, diffuse mild 408endocarditis, tricuspid valve damage 381endothelial cells 312endothelin receptor antagonists 42endotracheal tube, tracheal resection 102,
103epidural cooling 426epileptic seizures 407epinephrine 104
plasma concentration 314epsilon-aminocaproic acid (EACA) 305Epstein–Barr virus (EBV) 132erythromycin, gastric emptying 167, 181erythropoietin 306esophageal hiatus 184esophageal instrumentation 202–25
achalasia 209see also esophagus, perforation
esophageal reconstruction 173–81anastomosis location 177anastomotic leak 173, 176, 177
treatment 178–9anastomotic technique 177–8anatomic complications 173choice of organs 174–6colon utilization 174–5, 176, 179, 180, 181
complications 180, 181dysphagia 179, 181functional complications 179–81jejunum utilization 175–6, 179route 176
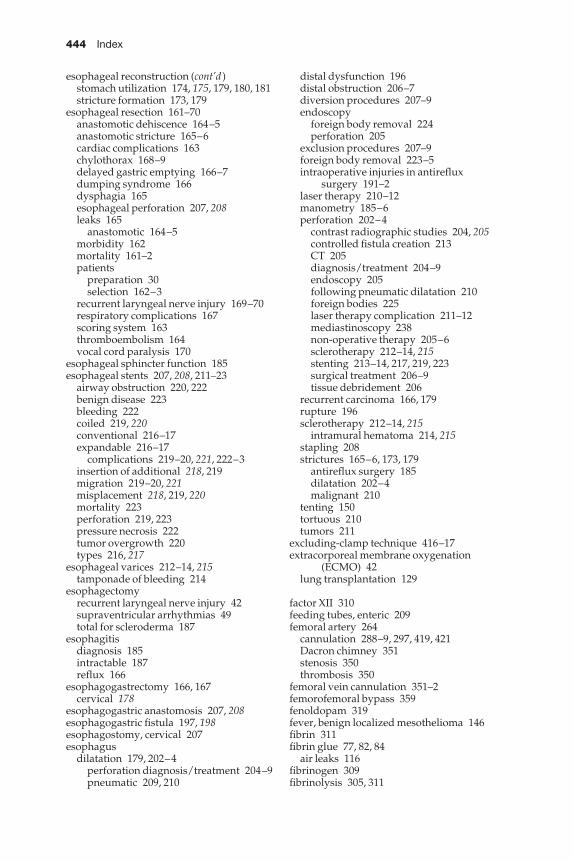
444 Index
esophageal reconstruction (cont’d)stomach utilization 174, 175, 179, 180, 181stricture formation 173, 179
esophageal resection 161–70anastomotic dehiscence 164–5anastomotic stricture 165–6cardiac complications 163chylothorax 168–9delayed gastric emptying 166–7dumping syndrome 166dysphagia 165esophageal perforation 207, 208leaks 165
anastomotic 164–5morbidity 162mortality 161–2patients
preparation 30selection 162–3
recurrent laryngeal nerve injury 169–70respiratory complications 167scoring system 163thromboembolism 164vocal cord paralysis 170
esophageal sphincter function 185esophageal stents 207, 208, 211–23
airway obstruction 220, 222benign disease 223bleeding 222coiled 219, 220conventional 216–17expandable 216–17
complications 219–20, 221, 222–3insertion of additional 218, 219migration 219–20, 221misplacement 218, 219, 220mortality 223perforation 219, 223pressure necrosis 222tumor overgrowth 220types 216, 217
esophageal varices 212–14, 215tamponade of bleeding 214
esophagectomyrecurrent laryngeal nerve injury 42supraventricular arrhythmias 49total for scleroderma 187
esophagitisdiagnosis 185intractable 187reflux 166
esophagogastrectomy 166, 167cervical 178
esophagogastric anastomosis 207, 208esophagogastric fistula 197, 198esophagostomy, cervical 207esophagus
dilatation 179, 202–4perforation diagnosis/treatment 204–9pneumatic 209, 210
distal dysfunction 196distal obstruction 206–7diversion procedures 207–9endoscopy
foreign body removal 224perforation 205
exclusion procedures 207–9foreign body removal 223–5intraoperative injuries in antireflux
surgery 191–2laser therapy 210–12manometry 185–6perforation 202–4
contrast radiographic studies 204, 205controlled fistula creation 213CT 205diagnosis/treatment 204–9endoscopy 205following pneumatic dilatation 210foreign bodies 225laser therapy complication 211–12mediastinoscopy 238non-operative therapy 205–6sclerotherapy 212–14, 215stenting 213–14, 217, 219, 223surgical treatment 206–9tissue debridement 206
recurrent carcinoma 166, 179rupture 196sclerotherapy 212–14, 215
intramural hematoma 214, 215stapling 208strictures 165–6, 173, 179
antireflux surgery 185dilatation 202–4malignant 210
tenting 150tortuous 210tumors 211
excluding-clamp technique 416–17extracorporeal membrane oxygenation
(ECMO) 42lung transplantation 129
factor XII 310feeding tubes, enteric 209femoral artery 264
cannulation 288–9, 297, 419, 421Dacron chimney 351stenosis 350thrombosis 350
femoral vein cannulation 351–2femorofemoral bypass 359fenoldopam 319fever, benign localized mesothelioma 146fibrin 311fibrin glue 77, 82, 84
air leaks 116fibrinogen 309fibrinolysis 305, 311
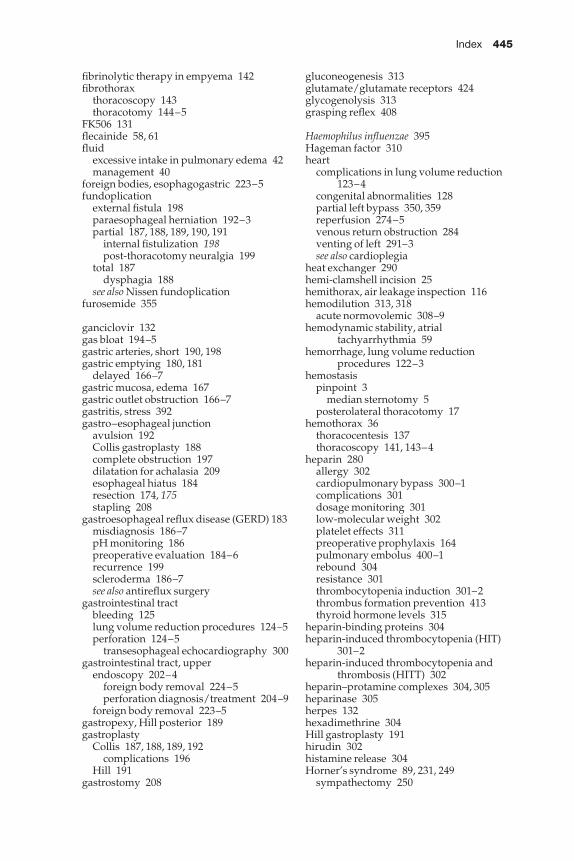
Index 445
fibrinolytic therapy in empyema 142fibrothorax
thoracoscopy 143thoracotomy 144–5
FK506 131flecainide 58, 61fluid
excessive intake in pulmonary edema 42management 40
foreign bodies, esophagogastric 223–5fundoplication
external fistula 198paraesophageal herniation 192–3partial 187, 188, 189, 190, 191
internal fistulization 198post-thoracotomy neuralgia 199
total 187dysphagia 188
see also Nissen fundoplicationfurosemide 355
ganciclovir 132gas bloat 194–5gastric arteries, short 190, 198gastric emptying 180, 181
delayed 166–7gastric mucosa, edema 167gastric outlet obstruction 166–7gastritis, stress 392gastro–esophageal junction
avulsion 192Collis gastroplasty 188complete obstruction 197dilatation for achalasia 209esophageal hiatus 184resection 174, 175stapling 208
gastroesophageal reflux disease (GERD) 183misdiagnosis 186–7pH monitoring 186preoperative evaluation 184–6recurrence 199scleroderma 186–7see also antireflux surgery
gastrointestinal tractbleeding 125lung volume reduction procedures 124–5perforation 124–5
transesophageal echocardiography 300gastrointestinal tract, upper
endoscopy 202–4foreign body removal 224–5perforation diagnosis/treatment 204–9
foreign body removal 223–5gastropexy, Hill posterior 189gastroplasty
Collis 187, 188, 189, 192complications 196
Hill 191gastrostomy 208
gluconeogenesis 313glutamate/glutamate receptors 424glycogenolysis 313grasping reflex 408
Haemophilus influenzae 395Hageman factor 310heart
complications in lung volume reduction123–4
congenital abnormalities 128partial left bypass 350, 359reperfusion 274–5venous return obstruction 284venting of left 291–3see also cardioplegia
heat exchanger 290hemi-clamshell incision 25hemithorax, air leakage inspection 116hemodilution 313, 318
acute normovolemic 308–9hemodynamic stability, atrial
tachyarrhythmia 59hemorrhage, lung volume reduction
procedures 122–3hemostasis
pinpoint 3median sternotomy 5
posterolateral thoracotomy 17hemothorax 36
thoracocentesis 137thoracoscopy 141, 143–4
heparin 280allergy 302cardiopulmonary bypass 300–1complications 301dosage monitoring 301low-molecular weight 302platelet effects 311preoperative prophylaxis 164pulmonary embolus 400–1rebound 304resistance 301thrombocytopenia induction 301–2thrombus formation prevention 413thyroid hormone levels 315
heparin-binding proteins 304heparin-induced thrombocytopenia (HIT)
301–2heparin-induced thrombocytopenia and
thrombosis (HITT) 302heparin–protamine complexes 304, 305heparinase 305herpes 132hexadimethrine 304Hill gastroplasty 191hirudin 302histamine release 304Horner’s syndrome 89, 231, 249
sympathectomy 250
446 Index
hypercalcemia 231hypercapnia
lung volume reduction procedure 120–1,122
permissive 40, 392hyperglycemia 313hypertension 231
postoperative 315hypocapnia, air leaks 117hypoglycemia, benign localized
mesothelioma 146hypothermia 312–14, 318
circulatory arrest 426–7phrenic nerve dysfunction 402profound 313–14
circulatory arrest 325spinal cord protection during aortic
surgery 426–7hypoventilation, lung volume reduction
procedure 121hypovolemia, thoracocentesis complication
137hypoxia, postoperative 394
ibutilide 61ICU psychosis 409immunoglobulin E (IgE) 304immunosuppression, lung transplantation
131imuran 131incisional hernia, median sternotomy 11infection
bronchopleural fistula 81lung transplantation 131–2pleural 137pleural spaces 135subphrenic abscess 191thoracoscopy port site 141thoracotomy incisions 29–30see also respiratory tract infection; wound
infectionsinferior vena cava
cannulation for mitral valve surgery371–2
entrapment 150inflammation/inflammatory disease
intrapleural space risk 71trachea 101
inflammatory cascade 396innominate artery injury 236–7intercostal artery reimplantation 427intermittent positive pressure ventilation
(IPPV) 40, 393atelectasis 38
International Council of EmboliManagement (ICEM) 415–16
intra-aortic balloon pump 275intra-aortic filtration 414–16intra-operative epiaortic echocardiography
(IEE) 412–13, 423
intra-operative epiaortic ultrasound 258intraperitoneal hematoma 87intrapleural spaces 71–5, 76
prevention 71–4recurrent 78reduction 75see also pleural spaces
inverse ratio ventilation 40
jejunostomy, feeding 209jejunum, esophageal reconstruction
175–6, 179
kallikrein 310Karnofsky index 162keloid 13ketorolac 119kidneys
aortic surgery 355–6cardiopulmonary bypass 318–19
Klebsiella pneumoniae 395
Langer’s lines 3, 13laser ablation
bronchial neoplasms 92esophageal 210–12
leukocyte filters 318leukocytosis, postpericardiotomy
syndrome 386Linton tube 214lobectomy
air leak closure 115atelectasis 70atrial arrhythmias 48–9bronchopleural fistula 80sleeve 92
tumor recurrence 98low cardiac output syndrome 321
mitral valve replacement/repair 378lung(s)
acute injury 317–18cardiopulmonary bypass effects 316–18compliance loss 71expansion 142functional residual capacity 317gangrene 87, 88hernia with thoracotomy incisions 28injury 401lobar torsion 86–8parenchymal hematoma 123re-expansion 115–16, 143resection with chest wall reconstruction
158, 159torn tissue 115see also lobectomy
lung cancerbronchoplasty 99, 100lymph node classification for staging
234, 235recurrence with sleeve lobectomy 98
Index 447
resectionapical 89atrial arrhythmias 51recurrent laryngeal nerve injury 89
lung clamps 115lung transplantation 128–33
acute rejection 131, 133atelectasis susceptibility 36bronchiolitis obliterans/bronchiolitis
obliterans syndrome 133early complications 128–31immunosuppression 131infection 131–2late complications 131–3retransplantation 133vascular anastomotic complications 130
lung volume reduction procedures108–26
complications 112–13, 114, 115–26extubation 121morbidity 111mortality 109, 110, 111nutritional supplementation 111preoperative preparation 111–12reintubation for respiratory failure 120,
121staple line buttress 113, 114, 115
lymph node classification for lung cancerstaging 234, 235
lymphocytes 312
magnesium levels 316magnetic resonance imaging (MRI), pleural
disease 135malperfusion syndromes 350–1
prevention 419, 421mammary artery grafts 259, 316Marfan syndrome 353meat bolus obstruction 225mediastinal cysts 230mediastinal masses 230–4, 235, 236–8
cervical mediastinoscopy 233–4, 235choriocarcinomas 245clinical features 231diagnosis 231–3embryonal cell carcinoma 245germ cell tumors 243–6
metastases 245serum markers 244, 245–6
imaging 232lesion biopsy 232–3lymph nodes 234, 235malignant neoplasms 231needle biopsy 232resection
anterior 241–8complications 246–8posterior 248–9
seminomas 244, 245serologic evaluation 232
teratomas 243–4, 245thoracoscopic sympathectomy 249–50see also thymoma
mediastinal surgery 230–52mediastinal tumors 230, 231
fibrosis 238metastases 248
incisional 238neurogenic 248–9resection 43, 246, 247–8, 249spinal column extensions 249
mediastinitis 7, 111post-thymectomy 241
mediastinoscopy 25–7bronchoplasty patient evaluation 93cervical 233–4, 235complications 236–8contraindications 234esophageal perforation 238hemorrhage 236incisional metastases 238mediastinal masses 232–3
mediastinotomy 25–7, 232anterior 43parasternal 26–7
mediastinum 230germ cell tumors 243–6medical complications of surgery 250–2post-cardiopulmonary bypass bleeding
305meningitis, post-thoracotomy 29mental dysfunction 408–9mesothelioma, benign localized 146mesothelioma, malignant 135, 139
diagnosis 145extrapleural pneumonectomy 146,
148–52pleural 146–7pleurectomy/decortication 147–8port site recurrence 141recurrence 148surgery 145–52
mesothelium 146methotrexate 133metoclopramide 181metoprolol 59
ventricular rate control 61microaspiration 395milrinone 394mitral stenosis 378mitral valve 362
anatomy 369–70calcification 373–4insufficiency 376, 378myxomatous 376
mitral valve surgery 369–78annuloplasty 376cardiopulmonary bypass 370–2combined aortic surgery 375–6commissurotomy 372–3
448 Index
mitral valve surgery (cont’d)incisions 370–2operations 372–6posterior annulus length reduction 376,
377postpericardiotomy syndrome 385reconstruction 376, 377repair 376–8
cardioplegia 324indications 376posterior leaflet 376, 377
replacement 373–6bioprostheses 374–5prostheses 373, 375
venous cannulation 371–2MK-801 425mobilization, early 119monocytes 312motility disorders 186mucociliary clearance, impaired 395multiple organ dysfunction syndrome
(MODS) 406muscle flaps
bronchoplasty 97bronchopleural fistula 82chest wall reconstruction 156–7intrapleural spaces 75median sternotomy 10, 11muscle-sparing incisions 23
myasthenia gravisthymectomy 238–41thymoma 241, 242
mycophenilate mofetil 131myocardial infarction
coronary artery bypass graft 276esophageal resection 163lung volume reduction 123, 124mediastinal surgery 251
myocardial ischemialung volume reduction 123, 124pathophysiology 321
myocardial protection 264, 322–5aortic valve surgery 363
myocardial stunning 321myocardium
cardioplegia solution distribution 323oxygen consumption 321
myocutaneous flaps, median sternotomy11
myoplasty, empyema cavity obliteration81
naso-tracheal suctioning, lung volumereduction procedures 119–20
National Emphysema Treatment Trial(NETT) 108
nerve injury 89neuralgia
intercostal 28upper limb 250
neurocognitive deficit 408–9neurological complications 405neurological injury, postoperative 406–10
air embolism prevention 413aortic surgery 417–19, 420, 421–3embolic 412intra-aortic filtration 414–16intra-operative prevention 412–17off-pump cardiac surgery 417passive retrograde cerebral perfusion 417prevention 411–17
preoperative 411–12risk factors 409–10type I 406–7, 410
prevention 419, 420type II 408–10
neuromuscular transfer 89neuroprotective agents 320neutrophils 312nimodipine 320Nissen fundoplication 185, 187–8, 189, 191
gas bloat 194–5reherniation 193slipped 196, 197
nitric oxideinhaled 42, 129, 392neurotoxicity 425
nitroglycerin 394nitroprusside 394NMDA receptors 424Nocardia 132nutritional supplementation in lung volume
reduction procedures 111
off-pump coronary artery bypass (OPCAB)417
omentumbronchopleural fistula closure 81, 82chest wall reconstruction 156–7intrapleural space obliteration 75
ophthalmological disorders 408orgaran 302osteoarthropathy, pulmonary 146osteochondritis 10osteomyelitis, median sternotomy 7, 8, 10osteoporosis of sternum 13oxygen, myocardial consumption 321
Pancoast’s syndrome 249panic attacks 126papaverine 275papillary muscles 370paraesophageal hernia 192–3paraplegia
post-thoracotomy 29thoracoabdominal aortic aneurysm repair
358patient positioning
intermittent prone 40supine 390
Index 449
peptic strictures, dysphagia 187perfusion scintigraphy, dipyridamole
thallium-201 124pericardectomy 86pericardial defect closure 85–6pericardial effusion 401
postpericardiotomy syndrome 386, 387pericardial friction rub 386pericardial inflammation, pleural effusion
401pericardial patch 86
dehiscence 150, 151–2replacement in empyema 152
pericardiocentesis 387peripheral nervous system complications
409peripheral perfusion, spinal cord protection
during aortic surgery 426peristalsis, intermittent mass 181peroneal nerve injury 409phenylephrine 119phospholipids 310photopheresis 133phrenic nerve
conduction velocity 402crush 72
phrenic nerve injury 42–3, 89, 240–1, 409mediastinal mass resection 246paralysis 322postoperative 402
physiotherapypneumonia prevention 395, 396postoperative 38, 39, 393
lung volume reduction procedures 119preoperative 391
pituitary hormones 314plasmapheresis 240plasmin 311platelet factor 4 305platelet-rich plasma, preoperative
harvesting 308platelets 311–12pleura 135
abrasion 117excessive drainage 41infection 137malignant mesothelioma 146–7sarcoma 148solitary fibrous tumour 135thickening 135, 136
pleural diseaseadhesive 113bulky 137, 139diagnosis 135, 136malignant 137postoperative 401thoracoscopy 138–42thoracotomy 144
pleural effusion 137bronchoscopy 137
esophageal anastomotic leak 165loculated 138malignant 142percutaneous drainage 139postoperative 401postpericardiotomy syndrome 386ring enhancement 145thoracoscopy 139
pleural envelope resection 148pleural fluid collections 135, 136, 137pleural spaces 135–52
drainage 299infection 135obliteration 113surgical evaluation 137–42see also intrapleural spaces
pleural tent 72, 117pleurectomy 117
parietal 144pleurectomy/decortication, malignant
pleural mesothelioma 146, 147–8pleurodesis 84
talc use 141, 142, 146pleuroperitoneal shunts 84Pneumocystis carinii pneumonia (PCP) 132pneumomediastinum, antireflux surgery 194pneumonectomy 39
arrhythmias 51atrial arrhythmias 49bronchopleural fistula 79–80, 81chylothorax 82completion 97, 98extrapleural
complications 150–2malignant pleural mesothelioma 146,
148–52pain management 151
pulmonary artery injury 237pulmonary edema 41–2recurrent laryngeal nerve injury 42, 89
pneumoniabronchoplasty 99diagnosis 395esophageal resection 167lung volume reduction procedures 118nosocomial 120, 122postintubation 94postobstructive 97postoperative 39, 394–6risk factors 395susceptibility 36thoracoscopy 143
pneumonitis 132radiation 148
pneumoperitoneum 72, 74lung volume reduction 125
pneumothorax 36antireflux surgery 194central venous catheters 298chest tube 131
450 Index
pneumothorax (cont’d)esophageal anastomotic leak 165management 402mediastinoscopy 238pleural disease 135, 136postoperative 401–2tension 298thoracocentesis complication 137, 138
positive end-expiratory pressure (PEEP)392, 394
postcardiotomy syndrome 401postpericardiotomy syndrome (PPS) 385–7
antibodies 385potassium levels 316premature ventricular complex 55–6
flecainide 58procainamide 59, 61–2propafanone 61propofol 320propranolol 58–9prostacyclins 302prostanoid drugs 42protamine 303–4protamine–heparin complexes 304, 305Pseudomonas aeruginosa 395Pseudomonas nosocomial pneumonia 120psychiatric complications 409
lung volume reduction procedures 125–6Puig–Massana annuloplasty 381pulmonary artery
air removal 298anastomosis 129flow 130injury 237pressure 276resistance 41rupture 299thrombosis 130
pulmonary artery catheters 251, 298–9pulmonary capillary leak syndrome 129pulmonary disease, aortic surgery 354–5pulmonary dysfunction, adult respiratory
distress syndrome 396pulmonary edema 397
post-pneumonectomy 41–2pulmonary embolus 397, 398, 399–401
antireflux surgery 194classification 400–1diagnosis 399, 400esophageal resection 164lung volume reduction procedures 125mortality 397pleural effusion 401preoperative prophylaxis 164prevention 399–400
pulmonary fibrosis 71, 74lung transplantation 128
pulmonary function tests 93lung transplantation 133
pulmonary hypertension, primary 128
pulmonary infarction 37pulmonary ligament, inferior 113
division 114pulmonary rehabilitation, atelectasis
prevention 393pulmonary resection 67–89
alveolopleural fistula 77–8atelectasis 67, 68, 69, 70atrial arrhythmias 51bronchopleural fistula 78–82cardiac herniation 84–6chylothorax 82–4incidence of complications 68intrapleural spaces 71–5, 76lobar torsion 86–8nerve injury 89risk factors for complications 67
pulmonary vascular disease 128pulmonary vascular recruitment 42pulmonary vein cannulation 419pump lung 317pump oxygenator 280–1, 289–90
bubble 289bypass 289–90centrifugal pump 290heparin-coated 289membrane 289roller pump 290, 294
pump suction see cardiotomy suctionpyloromyotomy 167, 180pyloroplasty 167, 180, 181
bowel dysfunction 199pylorospasm 180pylorus, endoscopic balloon dilatation 181
QRS complex 53premature ventricular complex 55, 56ventricular tachycardia 57
quinidine 61, 62
radial artery catheter 295, 297radial artery graft 259
harvesting 259–60T-grafting 263
radiation therapybronchial healing effects 97bronchoplasty 97esophageal stents 222seminomas 244teratoma 244thymoma 243
re-sternotomy see sternotomy incisions, redorecurrent laryngeal nerve 102
palsy 237recurrent laryngeal nerve injury 42–3, 89,
409esophageal resection 169–70mediastinal mass resection 246mediastinoscopy 237thymectomy 240–1
Index 451
red cellsaplasia 241, 242autologous predonation 306
renal failure, postoperative with cardiacsurgery 318
renin–angiotensin–aldosterone axis 315reperfusion response in lung
transplantation 129–30respiratory complications 36–43
esophageal resection 167preoperative risk factors 40
respiratory failureacute 40–1aortic surgery 354cardiopulmonary bypass 317lung volume reduction procedures 120–2postoperative 390–2risk 391thymectomy for myasthenia gravis 240
respiratory insufficiencyesophageal resection 167extrapleural pneumonectomy 151
respiratory quotient analysis 391–2respiratory tract infection
management 120nosocomial in lung volume reduction
109, 118–20rib fractures, thoracoscopy 144Robicsek weaving technique 9, 13
modification 10, 11
saphenous vein grafts 259closure 271–2
saphenous vein harvesting 409scapula, winging 20scars, hypertrophied 13scleroderma 186–7sclerotherapy, esophageal varices 212–14,
215seizure disorders 407, 408Sengstaken–Blakemore tube 214septic syndrome, thoracoscopy 143sequential compression devices 399seroma
chest wall reconstruction 157extrapleural pneumonectomy 152muscle-sparing thoracotomy 19
shoulder complications in thoracotomy 18,19, 20
shunting 394single-clamp technique 416–17sino–tubular junction 362
calcification 364sinus rhythm 62sinuses of Valsalva 362
calcification 364sleeve pulmonary resection 36, 38somatosensory evoked potentials (SSEPs)
427d-sotalol 61
spinal column hematoma 249spinal cord
compression 249cooling 359hypothermia 426–7injury 407
aortic surgery 423–7peripheral perfusion 425–6
ischemia 358neurotransmitters 424protection during aortic surgery 425–7
spirometry, incentive 38, 119, 391, 393esophageal resection 167pneumonia prevention 395
spleenantireflux surgery 189–91hematoma 197
Staphylococcus aureus 395stapling devices 77stellate ganglion, sympathectomy 250stenting
bronchial 97, 133esophageal 207, 208, 211–23
sternal wiresclamshell incision 24, 25median sternotomy 6, 9, 10, 11, 12–13partial sternotomy 14, 15redo sternotomy 13
sternotomybleeding 262coronary artery bypass graft 262–3median 109, 128, 233, 237
aortic valve surgery 363mediastinal tumor resection 246mitral valve surgery 370sternal wires 6, 9, 10, 11, 12–13
partial 14, 15redo 13respiratory failure 390thymectomy for myasthenia gravis 239tracheoinnominate artery fistula 105
sternotomy incisions 3–16bilateral submammary vertical 13–14median 3–11, 13
advantages 4antibiotic irrigation 9muscle flap coverage 10operative technique 4–7patient preparation 4suture technique 6–7wound complications 7–11
median–bilateral subcostal 15–16indications 15–16
partial 14–15redo 12–13
sternumclosure
median sternotomy 6–11median sternotomy–bilateral subcostal
incision 16
452 Index
sternum (cont’d)partial sternotomy 14redo sternotomy 13
debridement of infected 277–8dehiscence 7, 8, 9osteoporosis 13removal 10separation 10–11
steroids 392bronchial healing effect 97edema management 104immunosuppression 131weaning prior to lung volume reduction
procedures 111stomach
esophageal reconstruction 174, 179, 180,181
functional complications 180intraoperative injuries in antireflux
surgery 191–2Streptococcus pneumoniae 395stroke 407
clamp techniques 416–17coronary artery bypass graft 258, 413,
416–17mediastinoscopy 237prevention in aortic surgery 422–3risk 410, 411
subarachnoid–pleural fistula withpneumocephalus 29
subclavian arterycannulation 264, 351, 419revascularization 248
subclavian vein division/revascularization248
subcutaneous hematoma 137subphrenic abscess 191sucking reflex 408superior vena cava
cannulation 283mitral valve surgery 371–2
obstruction 233persistent left 284retrograde perfusion 421, 422
superior vena caval syndrome 231, 233suprahyoid laryngeal release 104supraventricular arrhythmias 277supraventricular tachycardia
esophageal resection 163lung volume reduction 123, 124
surgical site 390suture technique
aortic valve replacement 366, 367, 368aortotomy 364–5bronchoplasty 95–6extrapleural pneumonectomy 152median sternotomy 6–7median sternotomy–bilateral subcostal
incision 16mitral valve
repair 376, 377replacement 373, 374, 375
pledgets 366, 367plication for air leaks 116posterolateral thoracotomy 18–19thoracoabdominal incision 23–4tricuspid valve surgery 381, 382wound infections 30
swallowing disorders 392see also dysphagia
Swan–Ganz catheter see pulmonary arterycatheters
systemic inflammatory response 320, 396,397, 405–6
diagnosis 405systemic sclerosis 186–7
talc 141, 142, 145pleurodesis for malignant pleural
mesothelioma 146thiopental 320thoracentesis 139thoracic artery, internal
flow capacity 273graft anastomosis 266harvesting 260–1, 401–2pedicle 263
mobilization 261skeletonization 261spasm 275T-grafting 263
thoracic duct 83injury 83–4, 168ligation 84, 168surgical closure 247trauma 247
thoracoabdominal incision 23–4thoracocentesis 137–8thoracoplasty 72, 73–4
empyema cavity obliteration 81intrapleural spaces 75
thoracoscopycomplications 141–2drainage of esophagectomy leak 165empyema 141, 142–3fibrothorax 143hemothorax 143–4indications 139malignant pleural effusion 142mediastinal masses 232, 233, 249multiport video 140–2, 143pleural disease 138–42port site infection 141rib fractures 144single-port 139, 140, 142, 143
mesothelioma diagnosis 145sympathectomy 249–50talc poudrage 141, 142, 145thymectomy for myasthenia gravis
239–40
Index 453
tumor seeding in tract 141video-assisted thoracic surgery (VATS)
27, 81pleural disease 138–42
thoracosternotomy, bilateral 24–5thoracostomy
bronchopleural fistula 81pneumothorax 402
thoracostomy tube 299thoracotomy
air removal from pulmonary artery298
chylothorax 168epidural analgesia 94fibrothorax 144–5mature empyema 144–5mediastinal masses 232, 233neuralgia 199pleural disease 144reoperative for esophagectomy leak
165respiratory failure 40–1, 390–1supraventricular arrhythmias 49suture closure 152vascular anastomosis complications
130thoracotomy incisions 16–30
anterolateral 18infections 29–30lung hernia 28muscle-sparing 19–23neurological sequelae 29posterolateral 16–19, 22
patient preparation 16–17technique 17–18
reoperative 18vertical axillary 19–20
thoraxclosure 18–19, 152incisions 3–30
sternotomy 3–16thoracotomy 16–30video-assisted 27
malignancy 25, 26surgery
analgesia 252side of operation 51
thrombin 310, 311thrombocytopenia, heparin-induced
301–2thrombosis
aorta 350femoral artery 350pulmonary artery 130
thrombus formation prevention 413thymectomy 239–41
myasthenia gravis 238–41thymoma
myasthenia gravis 241, 242radiation therapy 243
recurrence 243resection 241–3, 247surgical excision 242surgical resection 243
thyroid hormones 315thyroplasty technique 89thyrotoxicosis 231thyrotropin 315thyroxine (T4) 315tissue plasminogen activator (t-PA) 311torsade de pointes 61trachea 100–1
burned 100cuff injuries 100–1high-risk conditions 100inflammation 101laceration 238pathology evaluation 101stenosis 104, 105
tracheal resection/reconstruction 100–1airway management 101–2complications management 103–5, 106edema 104granulations 104postoperative airway 103–4stenosis 104surgical technique 102–3
tracheo-esophageal groove 102dissection in recurrent laryngeal nerve
injury 42vocal cord paralysis 170
tracheobronchial resection 92–106complication management 97–8management 92stenosis 97see also bronchoplasty
tracheobronchial tree compression 249tracheoinnominate artery fistula 105tracheostomy, percutaneous 39
airway management 102tracheal resection 103, 104tracheoinnominate artery fistula 105
tranexamic acid 305transbronchial biopsy 131, 132transcranial Doppler echocardiography
412, 413, 417cerebral malperfusion 421
transdiaphragmatic access 43transesophageal echocardiography (TEE)
aortic atheroma 412aortic cannulation 287, 294, 423cardiopulmonary bypass 299–300cardiopulmonary bypass catheters 284cerebral malperfusion 421de-airing maneuvers 293descending aorta 264intraoperative 300mitral valve repair 376, 378odynophagia 300
transesophageal endocardiography 275
454 Index
transjugular intrahepatic portal systemicshunting (TIPS) 212
trap door incision 25triangle of Koch 379tricuspid valve
anatomy 379insufficiency 382leaflets 379
tricuspid valve surgery 379–82annuloplasty techniques 380–1bicuspidization 380bioprosthesis 382commissurotomy 381incisions 379–80prognosis 382repair 380–1replacement 381–2
triiodothyronine (T3) 315tube graft 274tuberculous disease, advanced refractory
148two-clamp technique 416–17
ultrasonographyintraoperative epiaortic 258pleural disease 135
vagotomy 180vagus nerve injury 89, 196, 199vasopressin see antidiuretic hormone (ADH)venous cannulation 283–6venous thrombosis
venous catheterization 298see also deep venous thrombosis
ventilation, mechanical 38, 40, 392air leaks 117–18liquid 42lung volume reduction 116tracheal resection 102, 103
ventilation–perfusion (VQ) mismatch 394ventilation–perfusion (VQ) scan 400ventilator dependence 391ventricle, left
aortic valve removal 365–6hypertrophy 354
outflow tract obstruction 378venting 292–3
ventricle, right, failure 382ventricular complex, premature 55–6
flecainide 58lung volume reduction 123
ventricular fibrillation 274ventricular rate control 61ventricular rupture, posterior 375ventricular tachycardia 56, 57
coronary artery bypass graft 277ventricular vent, left 363verapamil 59, 60
ventricular rate control 61video-assisted thoracic surgery (VATS) 27
bronchopleural fistula 81lung volume reduction procedures 109,
112, 113vital capacity, esophageal resection 162vocal cord medialization 89, 105vocal cord paralysis 89, 104–5
esophageal resection 170mediastinoscopy 237
von Willebrand factor 311, 314
warfarin 302wound complications
coronary artery bypass graft 277–8lung volume reduction procedures 125median sternotomy 7–11
wound infectionschest wall reconstruction 157coronary artery bypass graft 277–8drainage 30healing 30median sternotomy 7–8, 9
diagnosis 9incisional hernia 11rate 5
mediastinoscopy/mediastinotomy 26sternal 125thoracoabdominal incision 23thoracotomy incisions 29–30tracheal resection 104video-assisted thoracic surgery 27