Embed Size (px)
Citation preview
CONGENITALHYPOTHYROIDISM
• Dr C Naveen Kumar,
• PG in Pediatrics
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Contents
Brief review of Thyroid physiology
Etiology of Congenital hypothyroidism
Clinical features
Post-natal changes in thyroid hormone levels
Screening Approaches for Congenital Hypothyroidism
Approach to a newborn with positive screening test
Antenatal Diagnosis
Treatment and monitoring of Congenital hypothyroidism
Prognosis
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Thyroid Physiology
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Introduction
The gland has two primary functions.
The first is to secrete the thyroid hormones, which maintain the level of metabolism in the tissues that is optimal for their normal function.
Second function of the thyroid gland is to secrete calcitonin, a hormone that regulates circulating levels of calcium.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Iodide transport across the thyrocyte Iodine is an essential raw material for thyroid hormone
synthesis.
Dietary iodide is absorbed by the intestine and enters the circulation.
The basolateral membrane of thyrocytes facing the capillaries contain Na+ / I – symporter (NIS) that transports two Na + ions and one I – ion into the cell with each cycle, against the electrochemical gradient for I –.
The process involved is secondary active transport, with the energy provided by Na+ K+ ATPase.
Cl – / I – exchanger known as Pendrin is present on the apical membrane of thyrocytes.
It mediates transport of iodide out of thyrocyte into the lumen, where colloid (Thyroglobulin - TG) is located.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
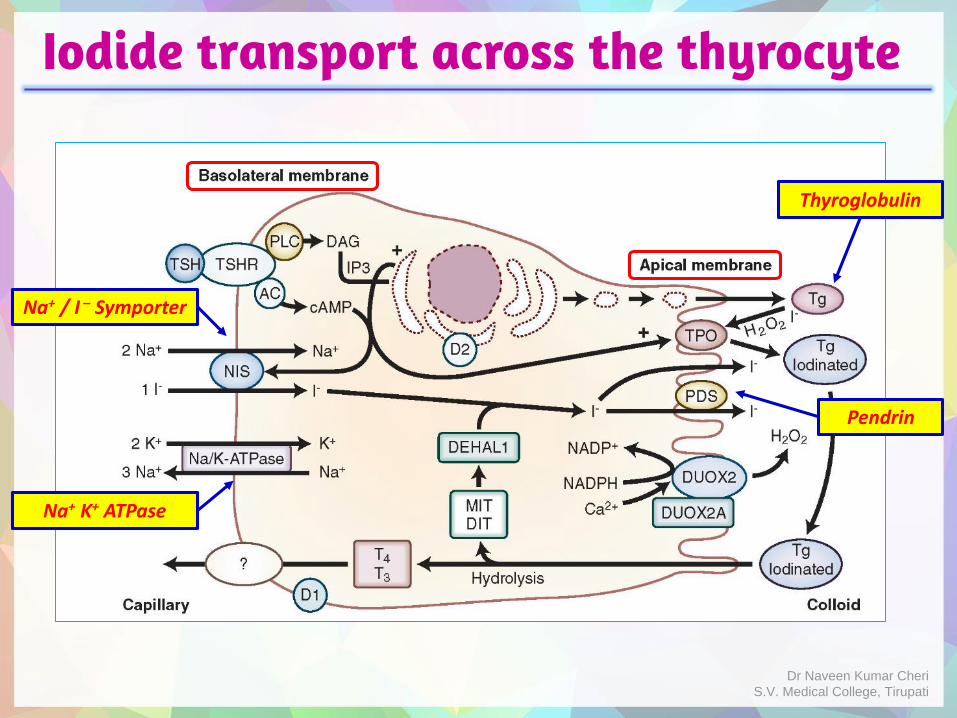
Iodide transport across the thyrocyte
Na+ / I – Symporter
Na+ K+ ATPase
Pendrin
Thyroglobulin
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Synthesis & secretion of thyroid hormone As soon as iodide reaches apical membrane of thyrocyte, it
undergoes a two step process called organification.
First, it is oxidized to iodine.
Next step is incorporation of iodine into tyrosine residues of thyroglobulin.
DUOX2 (Dual Oxidase-2) located in the apical membrane generates H2O2, which utilized by thyroid peroxidase (TPO) for oxidation of iodide into iodine.
Thyroid peroxidase (TPO) also catalyzes incorporation of iodine into tyrosine residues of thyroglobulin.
The thyroid hormones so produced remain part of the thyroglobulin molecule (colloid) until needed.
Colloid represents a reservoir of thyroid hormones, which can serve body requirements up to 2 months.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
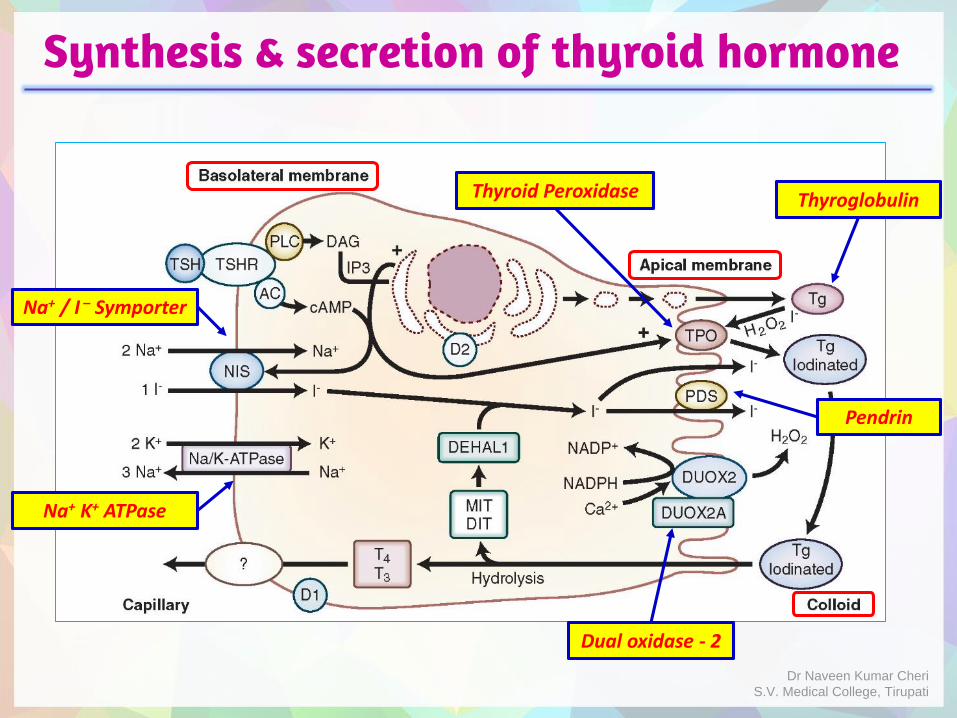
Synthesis & secretion of thyroid hormone
Na+ / I – Symporter
Na+ K+ ATPase
Pendrin
Thyroglobulin
Dual oxidase - 2
Thyroid Peroxidase
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
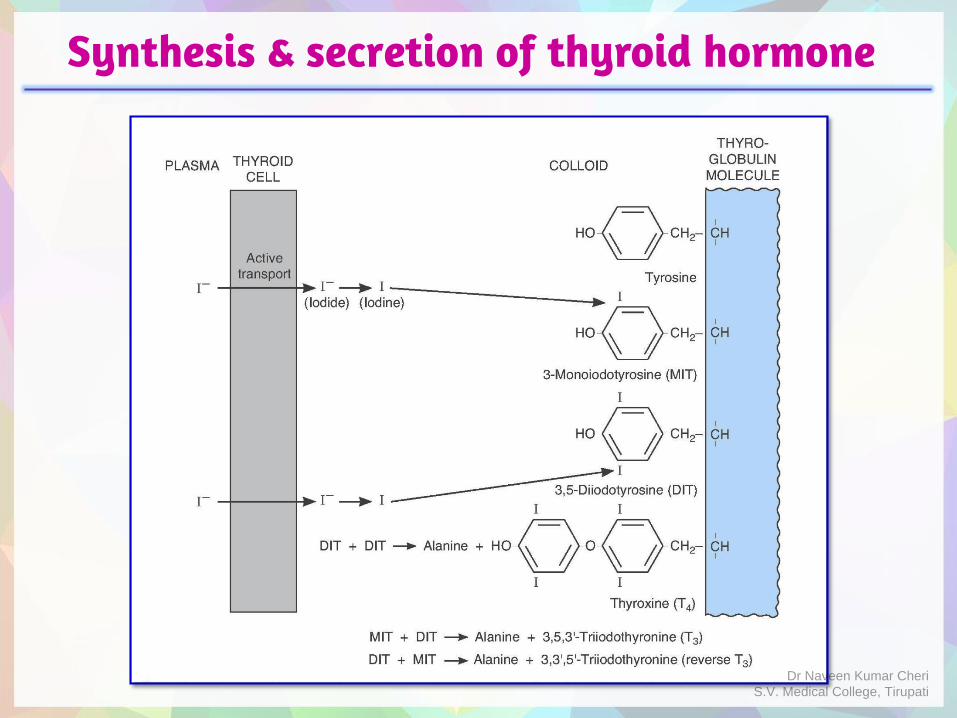
Synthesis & secretion of thyroid hormones
• During incorporation of iodine into Tyrosine residues of Thyroglobulin, following molecules are formed:
o 3-iodo tyrosine – Monoiodotyrosine (MIT)
o 3,5-di-iodo tyrosine – Diiodotyrosine (DIT)
o Condensation of two DITs - 3,5,3',5'-Tetraiodothyronine (T4)
o Condensation of MIT with DIT - 3,5,3'-Triodothyronine (T3)
o Condensation of DIT with MIT - 3, 3',5'-Triodothyronine (RT3)
Whenever is a need for thyroid hormone secretion, colloid is internalized by endocytosis.
Lysosomal degradation of thyroglobulin occurs. T4 (80 μg/day), T3 (4 μg/day) & RT3 (2 μg/day) are secreted into circulation.
MIT and DIT are not secreted, they are deiodinated by a microsomal iodotyrosine deiodinase and are reutilized.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Synthesis & secretion of thyroid hormone
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Transport & metabolism of thyroid hormones
T4 and T3 are relatively lipophilic, their free forms in plasma are in equilibrium with a much larger pool of protein-bound thyroid hormones in plasma.
Protein binding:
Maintains large pool of hormone that can readily be mobilized as needed.
Prevents excess uptake by the first cells encountered and promotes uniform tissue distribution
The plasma proteins that bind thyroid hormones are Albumin, Transthyretin (Thyroxine-binding Prealbumin) and Thyroxine-Binding Globulin (TBG).
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
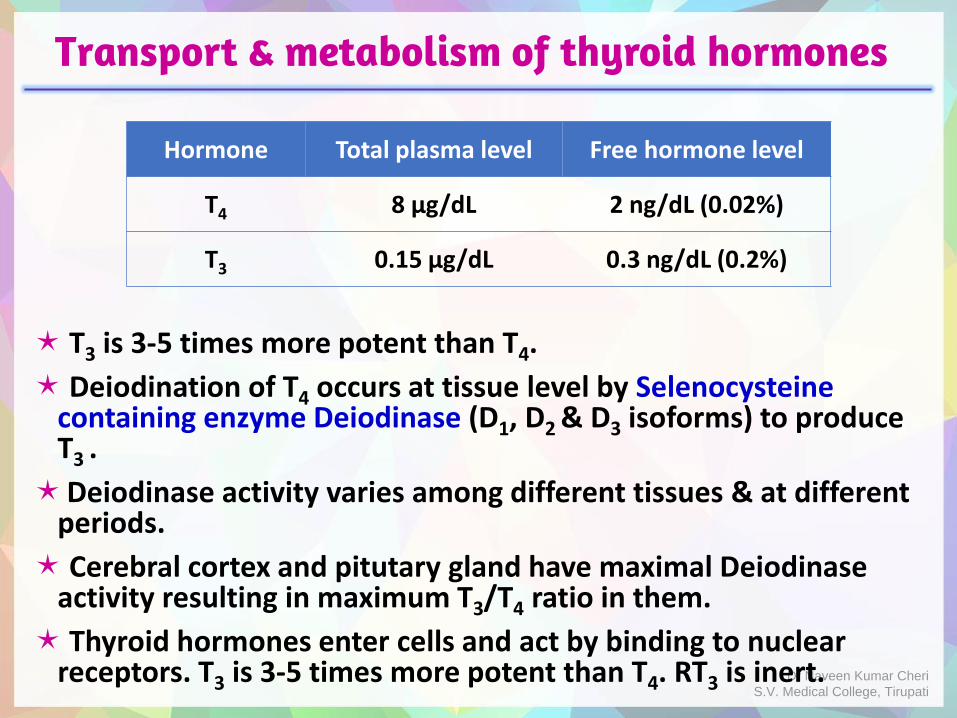
Transport & metabolism of thyroid hormones
T3 is 3-5 times more potent than T4.
Deiodination of T4 occurs at tissue level by Selenocysteinecontaining enzyme Deiodinase (D1, D2 & D3 isoforms) to produce T3 .
Deiodinase activity varies among different tissues & at different periods.
Cerebral cortex and pitutary gland have maximal Deiodinaseactivity resulting in maximum T3/T4 ratio in them.
Thyroid hormones enter cells and act by binding to nuclear receptors. T3 is 3-5 times more potent than T4. RT3 is inert.
Hormone Total plasma level Free hormone level
T4 8 μg/dL 2 ng/dL (0.02%)
T3 0.15 μg/dL 0.3 ng/dL (0.2%)
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
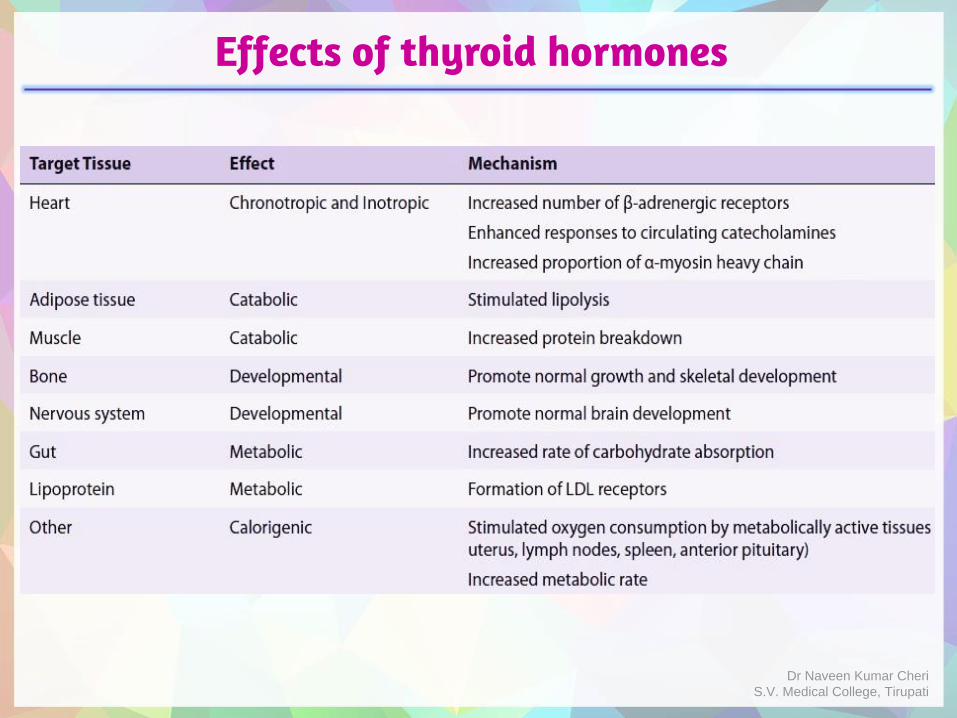
Effects of thyroid hormones
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Congenital hypothyroidism
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Introduction
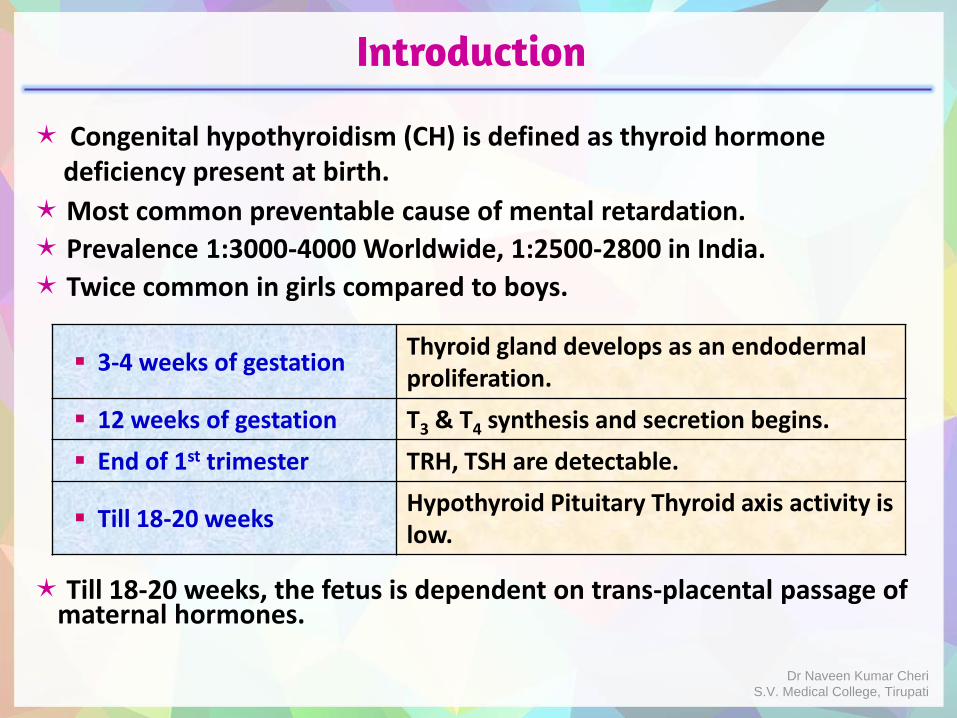
Congenital hypothyroidism (CH) is defined as thyroid hormone deficiency present at birth.
Most common preventable cause of mental retardation.
Prevalence 1:3000-4000 Worldwide, 1:2500-2800 in India.
Twice common in girls compared to boys.
Till 18-20 weeks, the fetus is dependent on trans-placental passage of maternal hormones.
3-4 weeks of gestationThyroid gland develops as an endodermal proliferation.
12 weeks of gestation T3 & T4 synthesis and secretion begins.
End of 1st trimester TRH, TSH are detectable.
Till 18-20 weeksHypothyroid Pituitary Thyroid axis activity is low.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Congenital Hypothyroidism - Terminology
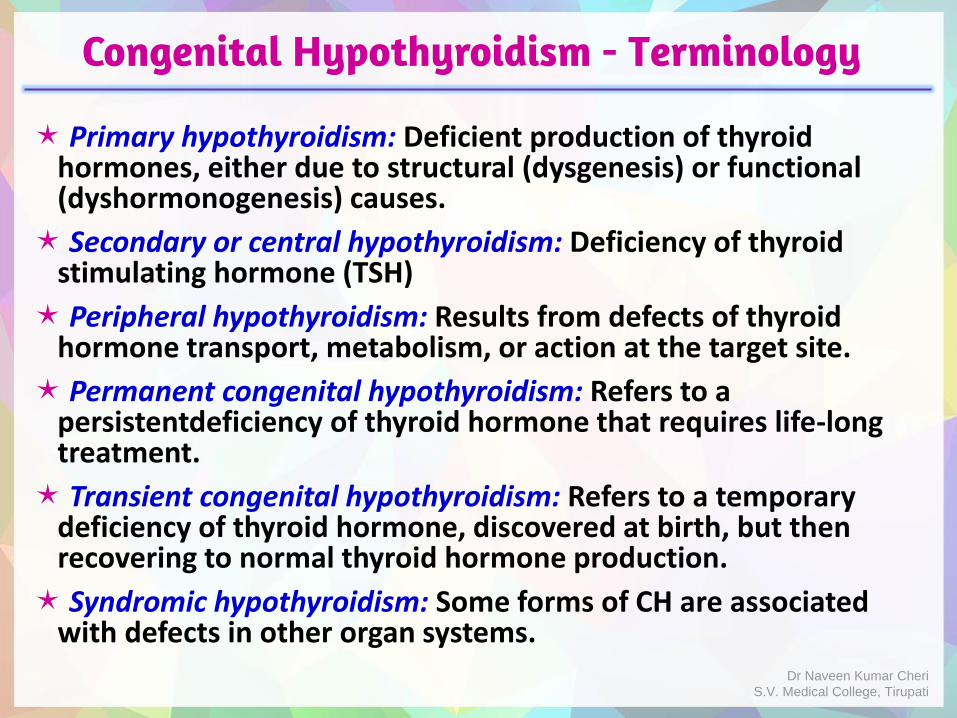
Primary hypothyroidism: Deficient production of thyroid hormones, either due to structural (dysgenesis) or functional (dyshormonogenesis) causes.
Secondary or central hypothyroidism: Deficiency of thyroid stimulating hormone (TSH)
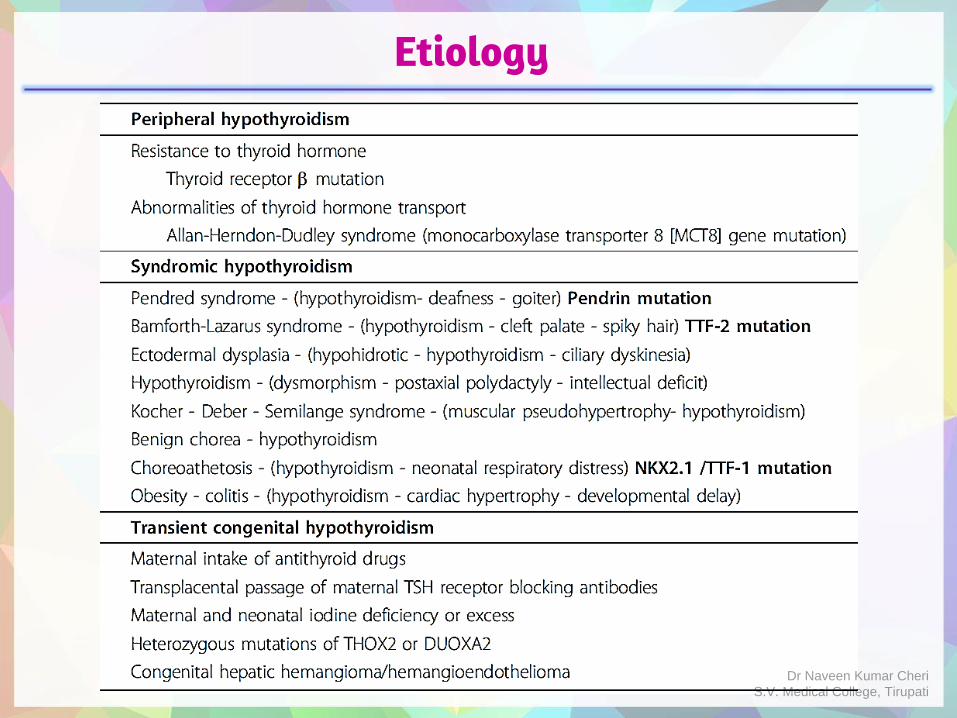
Peripheral hypothyroidism: Results from defects of thyroid hormone transport, metabolism, or action at the target site.
Permanent congenital hypothyroidism: Refers to a persistentdeficiency of thyroid hormone that requires life-long treatment.
Transient congenital hypothyroidism: Refers to a temporary deficiency of thyroid hormone, discovered at birth, but then recovering to normal thyroid hormone production.
Syndromic hypothyroidism: Some forms of CH are associated with defects in other organ systems.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
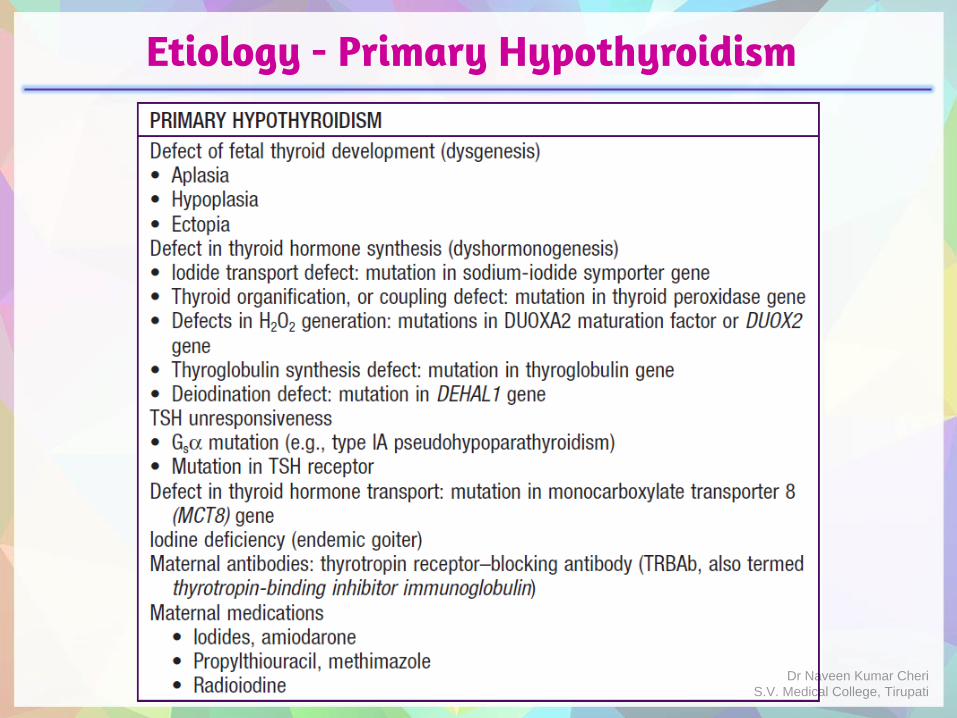
Etiology - Primary Hypothyroidism
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
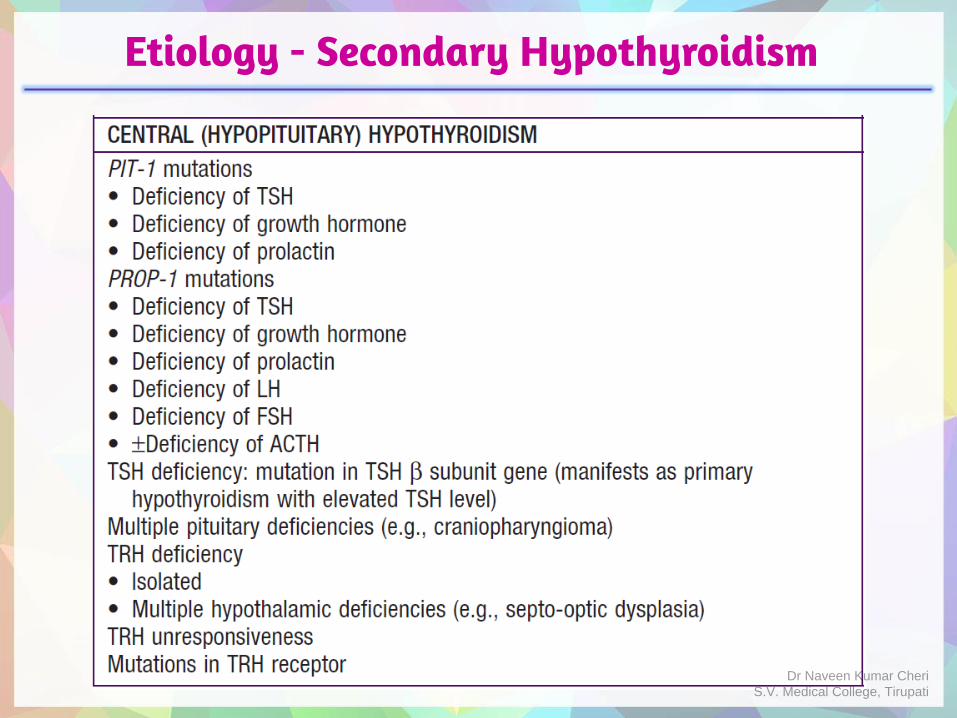
Etiology - Secondary Hypothyroidism
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Etiology
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Thyroid dysgenesis
It is the cause of > 85% cases of permanent hypothyroidism.
Includes aplasia, hypoplasia and dysplasia.
Dysplasia includes failure to descend - Ectopy
Always sporadic, no increased risk in subsequent siblings.
2:1 female to male preponderance.
Rarely associated with abnormality in transcription factors PAX8, TTF-2, NKX 2.1 etc.
No goiter, low total and free T4 levels, elevated TSH, and normal TBG.
Thyroglobulin (TG) is low in aplasia and hypoplasia. It reflects the amount of thyroid tissue present.
Diagnosis: is by Ultrasound and/or thyroid scintiscanning ( Radioactive iodine (RAI) or Pertechnetate - 99mT c)
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Thyroid dyshormonogenesis
Responsible for 10-15 % cases of permanent hypothyroidism.
Synthetic defects in thyroid hormone production.
Abnormal thyroid peroxidase activity is the commonest one, leading to impaired oxidation and organification of iodine.
Autosomal Recessive inheritance, 25% increased risk in subsequent siblings.
Goiter may be present, low total and free T4 levels, elevated TSH, and normal TBG.
Thyroglobulin (TG) is low in TG synthetic defects and is high in other thyroid hormone synthetic defects.
Imaging: Normally placed thyroid gland, which may be of normal size or enlarged.
In cases with partial deficiency, onset of signs and symptoms is delayed. Dr Naveen Kumar Cheri
S.V. Medical College, Tirupati
Primary hypothyroidism - etiology
Defects of organification and coupling: These are the most common of the T4 synthetic defects.
After iodide is trapped by the thyroid, it is rapidly oxidized to reactive iodine, which is then incorporated into tyrosine units on thyroglobulin.
This process requires generation of H2O2, thyroid peroxidase, DUOX2 Dual Oxidase 2 and hematin (an enzyme cofactor).
Defects can involve each of these components.
DUOX2 defects are transmitted in autosomal dominant manner.
Normal or increased uptake of radioiodine is seen.
Increased discharge in perchlorate discharge test.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Perchlorate Discharge Test
Perchlorate discharge test: A test dose of radioiodine administered first, and then 2 hrs later Potassium perchlorate or thiocyanate is administered.
• Perchlorate or thiocyanate is a competitive inhibitor of iodine transport into thyrocyte.
• In normal individuals in whom the organification and coupling remain intact only <10% of radioiodine is discharged (leaked), when iodine transport is inhibited.
• In individuals with defective organification and coupling, 40-90% of radioiodine is discharged (leaked), when iodine transport is inhibited.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Primary hypothyroidism - etiology
Pendred syndrome:
Autosomal recessive, mutations in PDS gene 7q31 (which encodes Pendrin - Chloride Iodine exchanger). Bilateral sensorineuronalhearing loss and congenital hypothyroidism with goiter.
Defect of Iodide Trasport :
Mutations in the sodium-iodide symporter.
The energy-dependent mechanisms for concentrating iodide are defective in the thyroid and salivary glands.
Uptake of radioiodine and pertechnetate is low.
Eutopic and normal or enlarged gland on sonography.
Defects of Thyroglobulin (TG) synthesis:
Characterized by goiter, elevated TSH, low T4 levels, and absent or low levels of thyroglobulin (TG).
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Secondary hypothyroidism - etiology
Thyrotropin and Thyrotropin Releasing Hormone deficiency :
They can occur in any of the conditions associated with developmental defects of the pituitary or hypothalamus.
Usually present with multiple pituitary enzyme deficiencies.
Features: Hypoglycemia (Growth hormone and ACTH deficiency), micropenis (gonadotropin deficiency) in association with septo-optic dysplasia (de Morsier syndrome - optic nerve hypoplasia, agenesis of septum pellucidum and hypopituitarism), midline cleft lip.
PIT-1 & PROP-1 mutations – multiple hormone deficiencies
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Peripheral hypothyroidism - etiology
Includes
Defects in deiodination :
DEHAL1 gene (encodes Iodotyrosine deiodinase) mutations.
Defects in transport :
Monocarboxylase Trasporter 8 is required to transport T3 into neurons.
MCT8 mutations lead X Linked hypothyroidism Allan-Herndon-Dudley syndrome.
It is characterized by mental retardation, quadriplegia, elevated serum T3 levels, low T4 and normal TSH.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Peripheral hypothyroidism - etiology
Thyroid hormone unresponsiveness :
Autosomal dominant disorder.
Mutations in the thyroid hormone receptor.
Most patients have a goiter.
Levels of T4, T3, free T4, and free T3 are elevated.
TSH levels are also elevated.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Transient congenital hypothyroidism
Transfer of maternal blocking antibodies - Maternal antithyroid antibodies can cross the placenta and block the TSH receptor in the neonatal thyroid. This effect can last up to 3 to 6 months after birth as maternal antibody levels fall.
Fetal exposure to antithyroid drugs – They can decrease neonatal thyroid hormone synthesis which lasts for a few days to two weeks after birth.
Maternal iodine exposure - Maternally administered Amiodarone may cause transient hypothyroidism in infants. This seems to resolve at around 4-5 months of age. Iodinated contrast material and iodinated antiseptics administered to mother can also cause transient hypothyroidism in the infant, depending on dose and severity of exposure.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Transient congenital hypothyroidism
• Neonatal Iodine exposure - Exposure of newborns to high amounts of iodine can cause hypothyroidism. (Wolff –Chaikoff effect).
This can occur especially in preterm infants.
• Liver hemangiomas - Congenital liver hemangiomas produce large amounts of the enzyme Type 3 iodothyroninedeiodinase. This produces a consumptive type of hypothyroidism in which large doses of thyroxine are required to maintain euthyroidism. Serum T4 levels are low, TSH is elevated, and reverse T3 levels are also increased.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Bamforth - Lazarus Syndrome
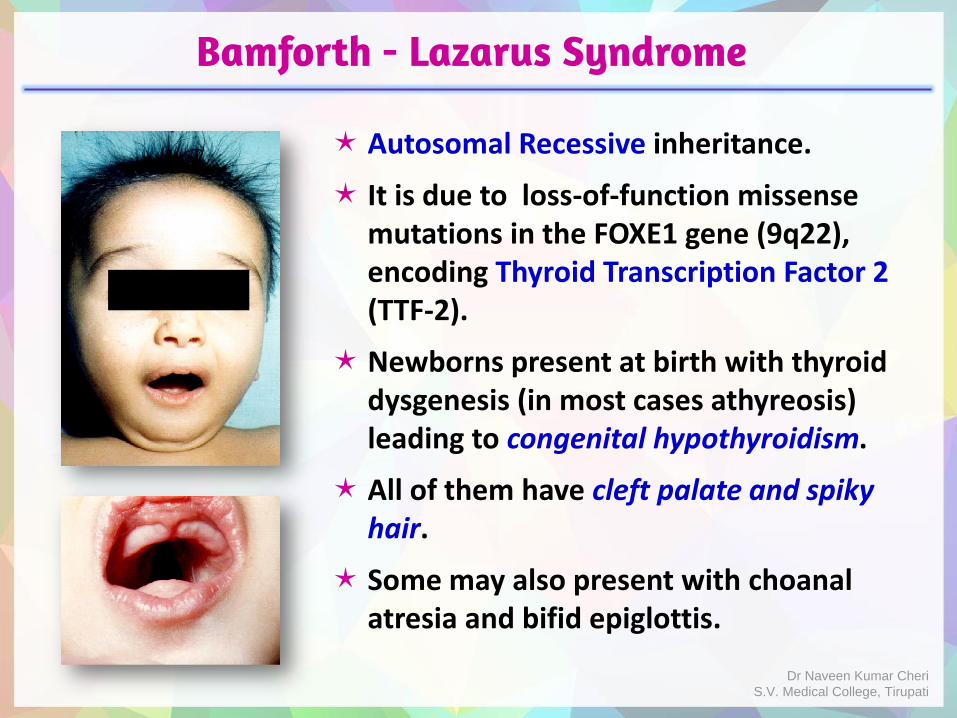
Autosomal Recessive inheritance.
It is due to loss-of-function missense mutations in the FOXE1 gene (9q22), encoding Thyroid Transcription Factor 2 (TTF-2).
Newborns present at birth with thyroid dysgenesis (in most cases athyreosis) leading to congenital hypothyroidism.
All of them have cleft palate and spiky hair.
Some may also present with choanalatresia and bifid epiglottis.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
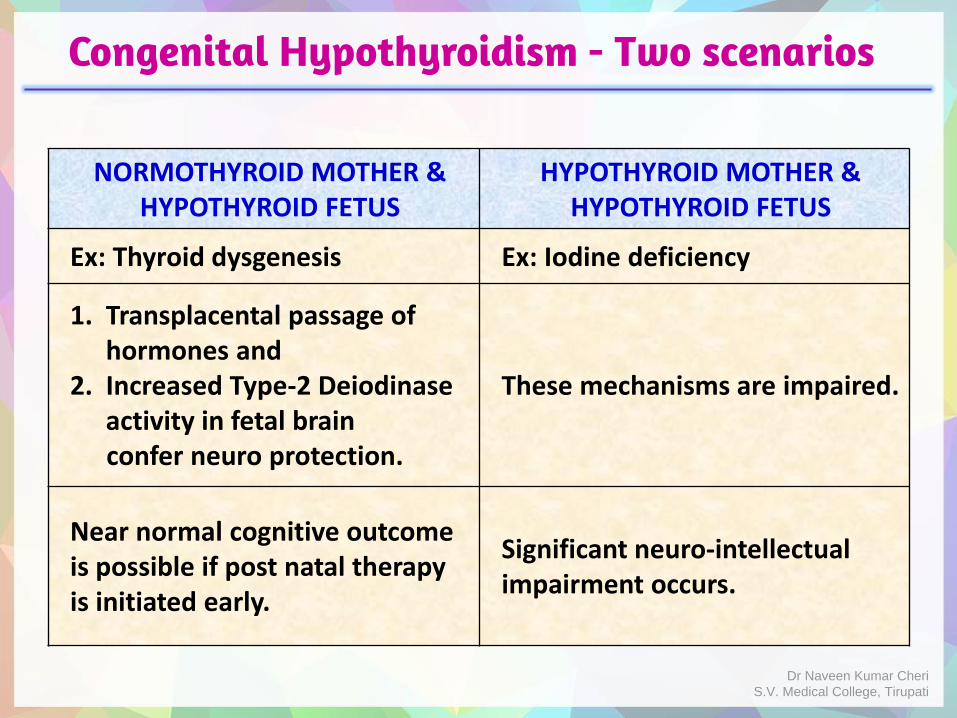
Congenital Hypothyroidism - Two scenarios
NORMOTHYROID MOTHER &HYPOTHYROID FETUS
HYPOTHYROID MOTHER &HYPOTHYROID FETUS
Ex: Thyroid dysgenesis Ex: Iodine deficiency
1. Transplacental passage of hormones and
2. Increased Type-2 Deiodinaseactivity in fetal brainconfer neuro protection.
These mechanisms are impaired.
Near normal cognitive outcome is possible if post natal therapy is initiated early.
Significant neuro-intellectual impairment occurs.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Clinical features of Congenital Hypothyroidism
Most infants with congenital hypothyroidism are asymptomatic at birth to the trans-placental passage of maternal T4.
Post maturity (In 20%, gestation extends beyond 42 weeks)
Birth weight and length are normal.
Head size may be slightly increased because of myxedema of the brain.
Wide posterior fontanelle
Prolongation of physiologic jaundice. (Immaturity of hepatic glucuronyl transferase).
Sluggishness, cry little
Poor appetite - feeding difficulties
Lack of interest, Somnolence
Protruberent abdomen, umbilical hernia
Macroglossia
Cold or mottled skin, hypotonia
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
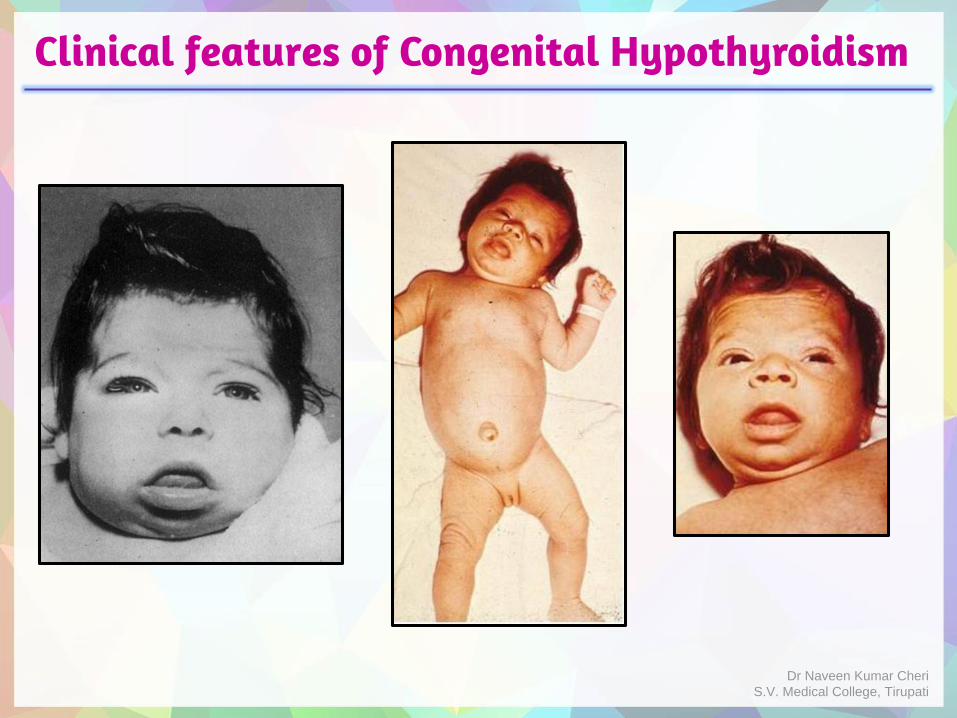
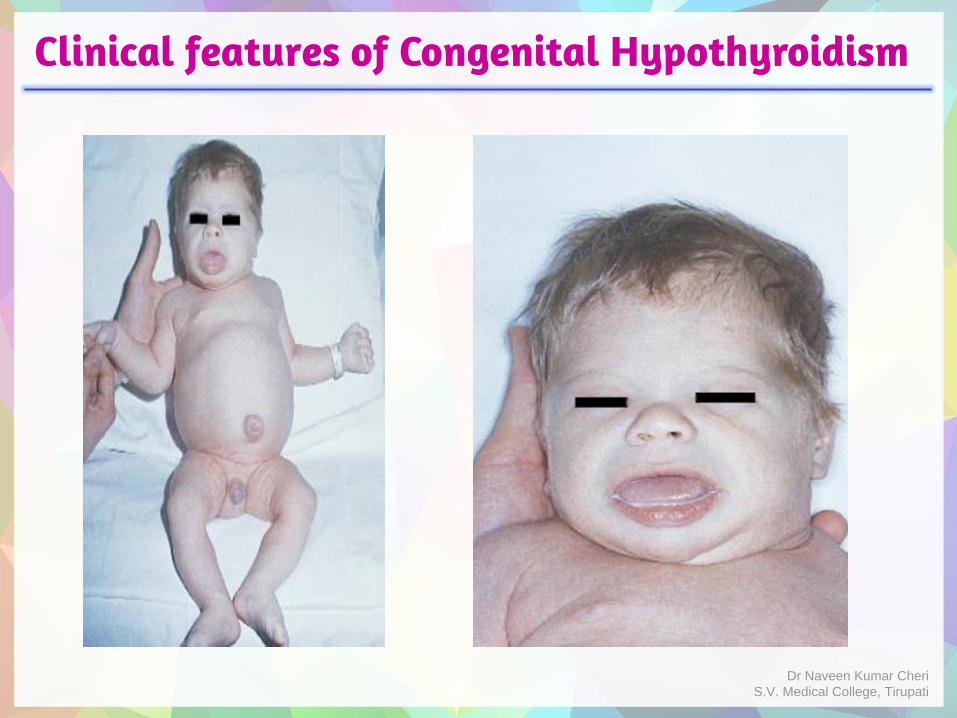
Clinical features of Congenital Hypothyroidism
By 3-6 mo of age the clinical picture is fully developed, if untreated.
The child’s growth will be stunted, the extremities are short, and the head size is normal or even increased.
Coarse facial features: The eyes appear far apart, and the bridge of the broad nose is depressed. The palpebral fissures are narrow and the eyelids are swollen. The mouth is kept open, and the thick, broad tongue protrudes.
Dentition will be delayed.
The neck is short and thick, and there may be deposits of fat above the clavicles and between the neck and shoulders.
The hands are broad and the fingers are short. The skin is dry and scaly, and there is little perspiration.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Clinical features of Congenital Hypothyroidism
Myxedema is manifested, particularly in the skin of the eyelids, the back of the hands, and the external genitals.
Carotenemia can cause a yellow discoloration of the skin, but the sclerae remain white.
The scalp is thickened, and the hair is coarse, brittle, and scanty. The hairline reaches far down on the forehead.
Development is delayed.
Voice is hoarse.
Sexual maturation may be delayed.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Clinical features of Congenital Hypothyroidism
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Clinical features of Congenital Hypothyroidism
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Post natal changes in Thyroid hormones
TSH
• Within 30-60 min after delivery, there is an early post natal surge upto 60-80 mU/L in response to cold in utero environment.
• Rapid fall to 20 mU/L in 24 hours.
• Falls to 10 mU/L by one week.
T4
• Peaks to 17 μg/dL at 24-36 hours.
• Gradual decline over 4-5 weeks.
Pre-terms exhibit similar but blunted response.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
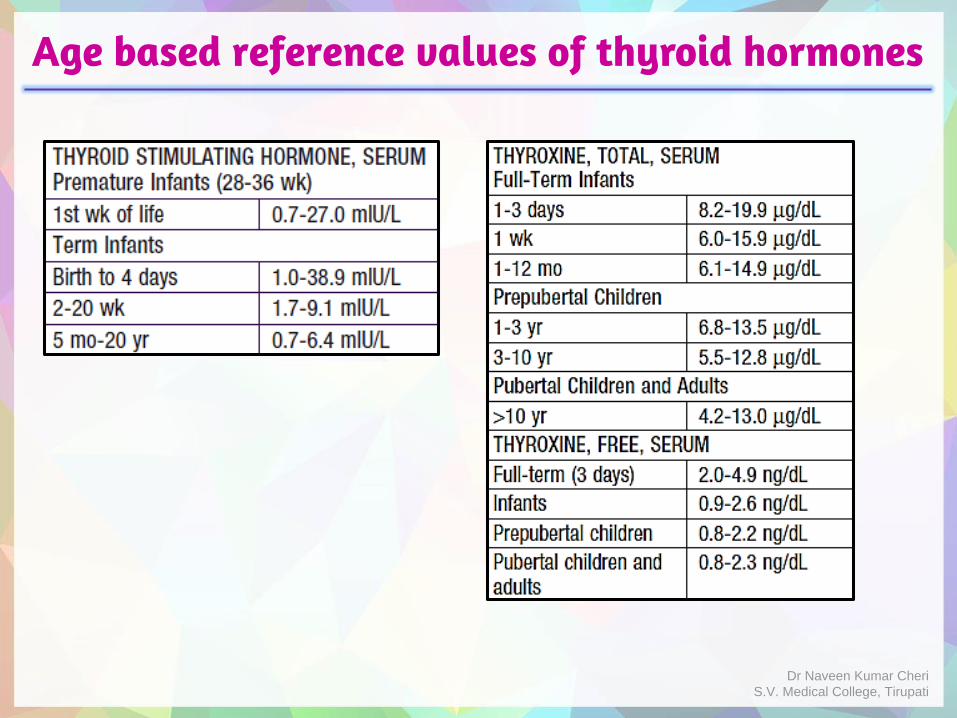
Age based reference values of thyroid hormones
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Screening for Congenital Hypothyroidism
Ideal is universal newborn screening at 3-4 days of age.
Universal screening: Most cases are sporadic in Iodine sufficient areas and intellectual impairment can be prevented if treatment is initiated early.
In the absence of universal screening, newborns with following indications must be screened:
1. Having clinical features of congenital hypothyroidism or family history.
2. History of thyroid disease or anti-thyroid medication intake in mother.
3. Presence of other conditions like Down’s syndrome, trisomy 18, neural tube defects, congenital heart disease, metabolic disorders, familial autoimmune disorders and Pierre- Robin syndrome which are associated with higher prevalence of congenital hypothyroidism.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
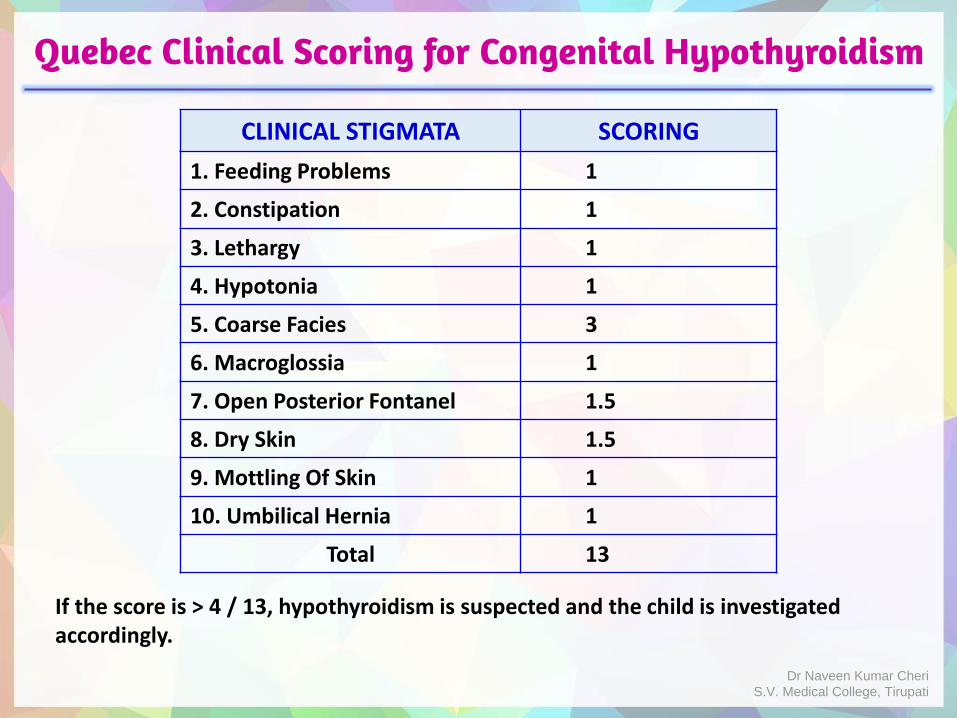
Quebec Clinical Scoring for Congenital Hypothyroidism
CLINICAL STIGMATA SCORING
1. Feeding Problems 1
2. Constipation 1
3. Lethargy 1
4. Hypotonia 1
5. Coarse Facies 3
6. Macroglossia 1
7. Open Posterior Fontanel 1.5
8. Dry Skin 1.5
9. Mottling Of Skin 1
10. Umbilical Hernia 1
Total 13
If the score is > 4 / 13, hypothyroidism is suspected and the child is investigated accordingly.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Screening Approaches
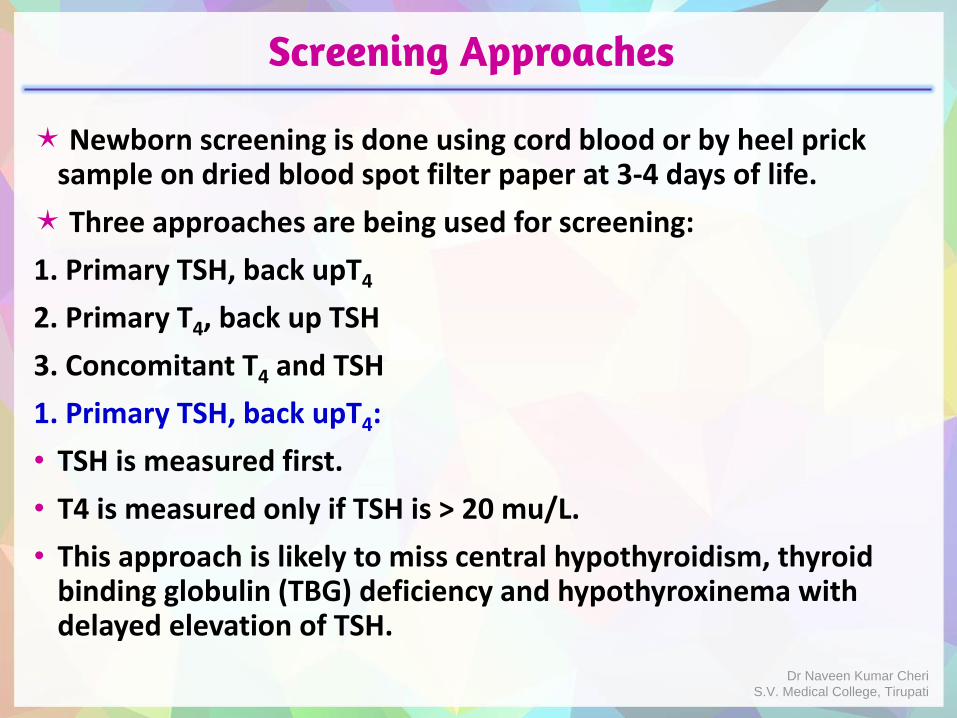
Newborn screening is done using cord blood or by heel prick sample on dried blood spot filter paper at 3-4 days of life.
Three approaches are being used for screening:
1. Primary TSH, back upT4
2. Primary T4, back up TSH
3. Concomitant T4 and TSH
1. Primary TSH, back upT4:
• TSH is measured first.
• T4 is measured only if TSH is > 20 mu/L.
• This approach is likely to miss central hypothyroidism, thyroid binding globulin (TBG) deficiency and hypothyroxinema with delayed elevation of TSH.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Screening Approaches
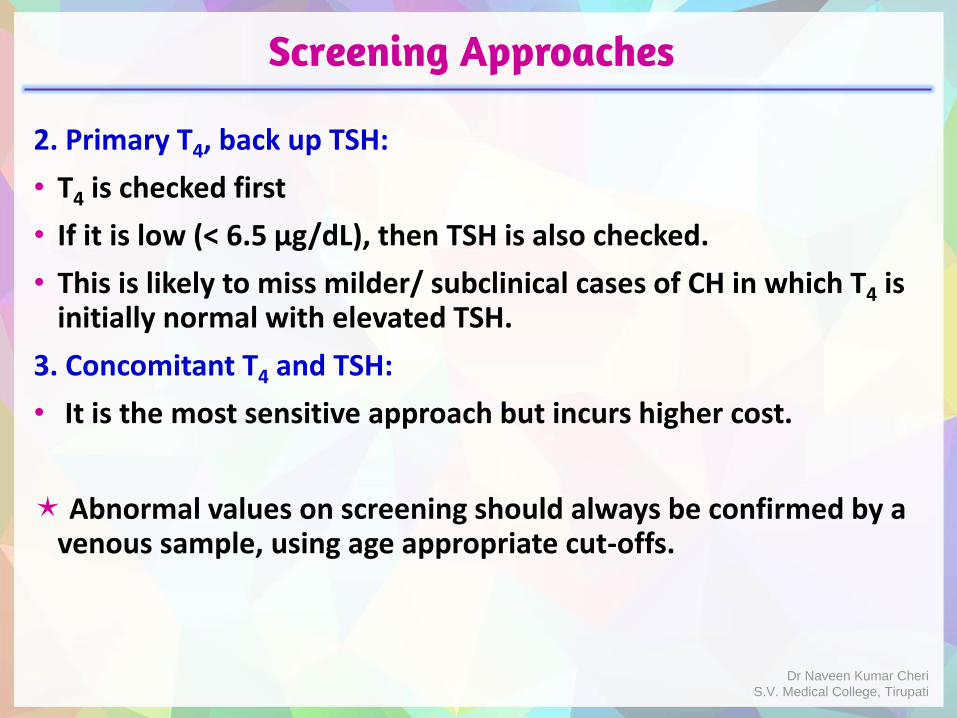
2. Primary T4, back up TSH:
• T4 is checked first
• If it is low (< 6.5 μg/dL), then TSH is also checked.
• This is likely to miss milder/ subclinical cases of CH in which T4 is initially normal with elevated TSH.
3. Concomitant T4 and TSH:
• It is the most sensitive approach but incurs higher cost.
Abnormal values on screening should always be confirmed by a venous sample, using age appropriate cut-offs.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Significance of free T4 levels
In most situations, total T4 is sufficient for diagnosis and monitoring treatment.
But Free T4 is a more robust marker, as represents the bioavailable fraction of T4.
In following situations, it is preferable to use free T4:
Premature or sick newborns: Immature liver function, under-nutrition & proteinuria >>> Low levels of TBG (Thyroxine Binding Globulin) or abnormal protein binding.
Low total T4 and normal TSH:
a) If free T4 is normal >>> Congenital complete or partial TBG deficiency.
b) If free T4 is low >>> Suspect central hypothyroidism.
During post treatment monitoring:
First post treatment measurement should include free T4 or TBG.Dr Naveen Kumar Cheri
S.V. Medical College, Tirupati
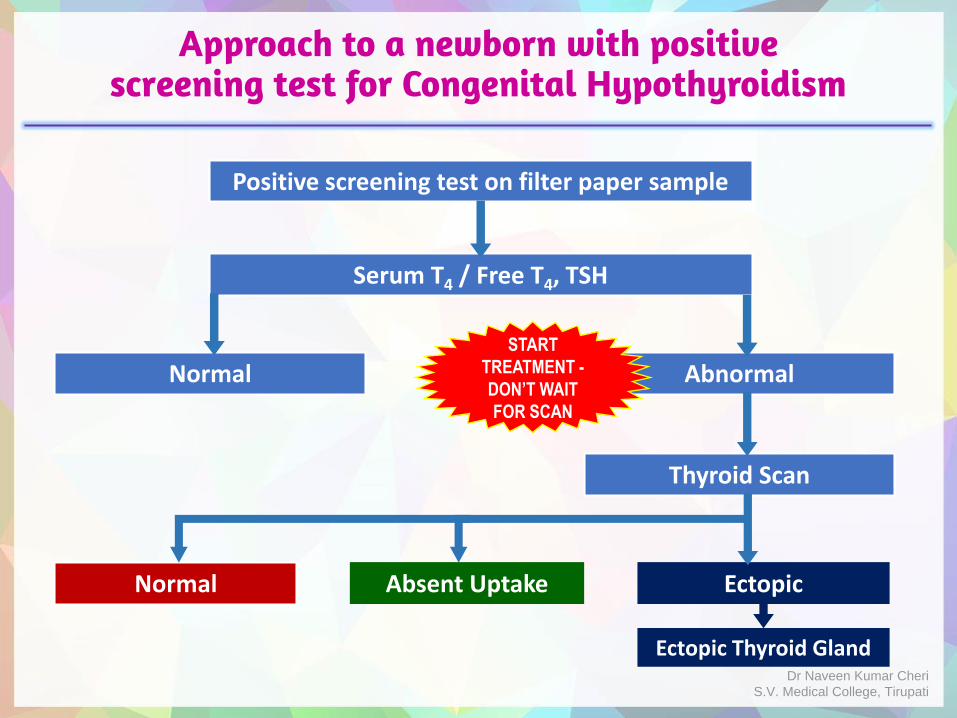
Approach to a newborn with positive screening test for Congenital Hypothyroidism
Positive screening test on filter paper sample
Serum T4 / Free T4, TSH
Normal Abnormal
Thyroid Scan
Normal EctopicAbsent Uptake
Ectopic Thyroid Gland
START
TREATMENT -
DON’T WAIT
FOR SCAN
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
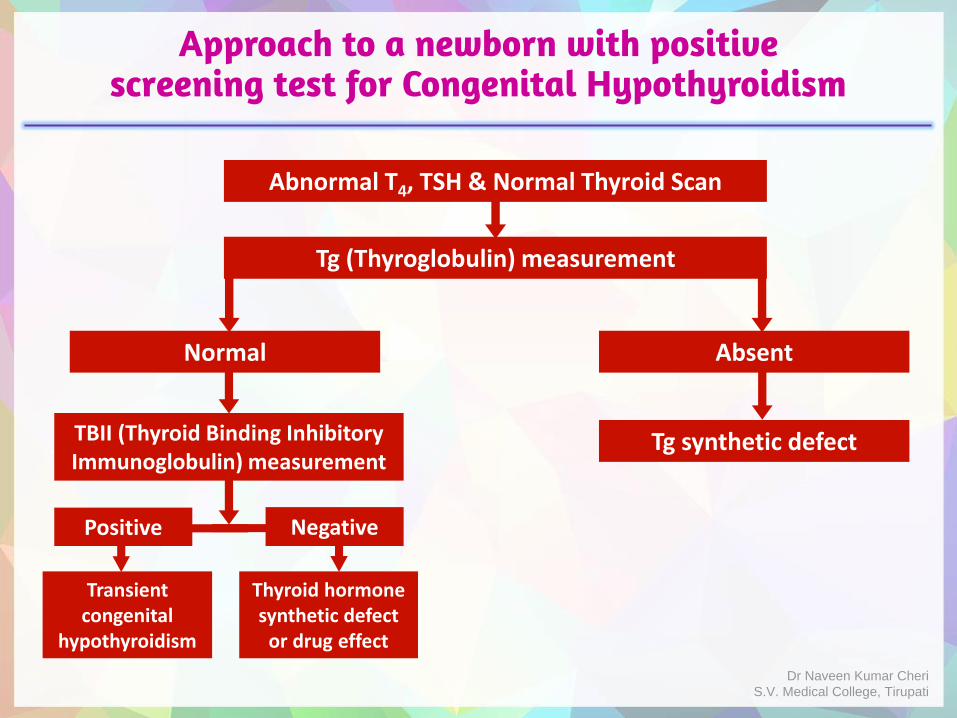
Approach to a newborn with positive screening test for Congenital Hypothyroidism
Abnormal T4, TSH & Normal Thyroid Scan
Tg (Thyroglobulin) measurement
Normal Absent
Tg synthetic defect
Transient congenital
hypothyroidism
Thyroid hormone synthetic defect
or drug effect
TBII (Thyroid Binding Inhibitory Immunoglobulin) measurement
Positive Negative
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
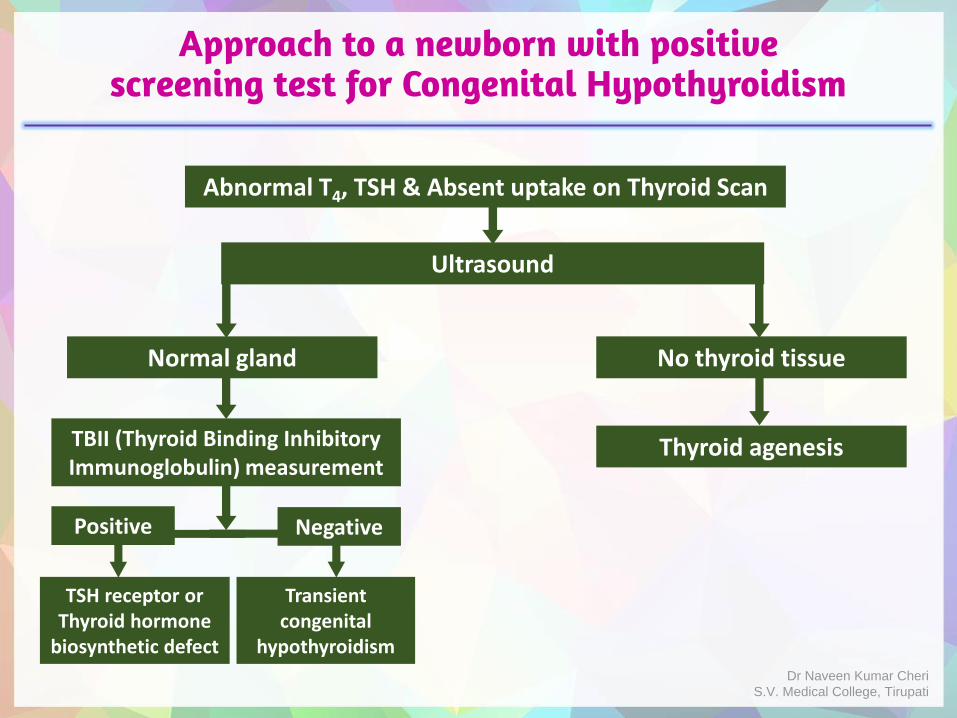
Approach to a newborn with positive screening test for Congenital Hypothyroidism
Abnormal T4, TSH & Absent uptake on Thyroid Scan
Ultrasound
Normal gland No thyroid tissue
Thyroid agenesis
TSH receptor or Thyroid hormone
biosynthetic defect
Transient congenital
hypothyroidism
TBII (Thyroid Binding Inhibitory Immunoglobulin) measurement
Positive Negative
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Role of investigations other than serum tests in CH
Tests other than T4 & TSH are not needed to initiate treatment in congenital hypothyroidism.
They are required to confirm the etiological diagnosis.
Useful to take treatment decision in cases with borderline test results.
Useful to separate transient & permanent cases.
If a familial form is encountered, useful for genetic counseling.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Antenatal Diagnosis
Majority of cases of congenital hypothyroidism are sporadic, not heritable.
Women who are at high risk for fetal hypothyroidism are:
Previous infant with congenital hypothyroidism (resulting from dyshormonogenesis or maternal TRB-Ab)
Pregnant woman with Graves’ disease and treated with anti-thyroid drugs
Iodide exposure during pregnancy, inadvertent treatment with radioactive iodine (RAI) after 8-10 weeks gestation.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Antenatal Diagnosis
Hypothyroidism is suspected if there is fetal goiter, increased amniotic fluid and fetal bradycardia.
Measurement of amniotic fluid TSH or thyroid hormone levels are not reliable, and fetal umbilical cord blood levels are necessary to diagnose fetal hypothyroidism.
Genetic testing on fetal cells obtained by amniocentesis confirms the diagnosis.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Congenital Goiter
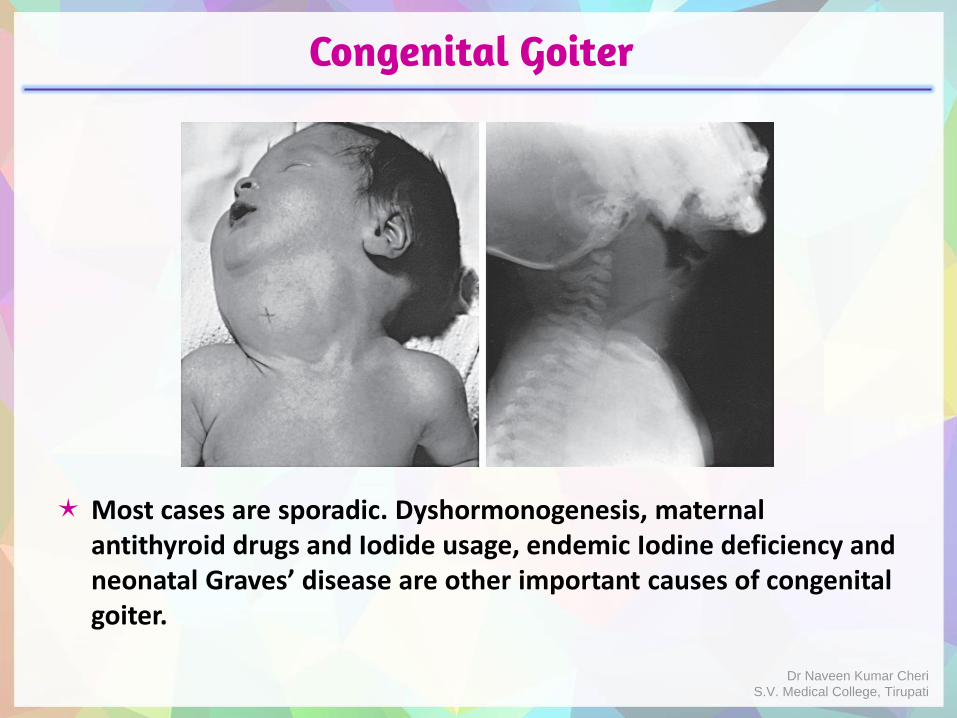
Most cases are sporadic. Dyshormonogenesis, maternal antithyroid drugs and Iodide usage, endemic Iodine deficiency and neonatal Graves’ disease are other important causes of congenital goiter.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Treatment of fetal hypothyroidism
Significant enlargement of the thyroid at birth may lead to respiratory distress and can even cause death. Partial thyroidectomy may be needed in such cases.
Hypothyroidism diagnosed antenatally is treated with weekly intra-amniotic injections of L-thyroxine. Initial dose is 250 mcg of L-thyroxine per week (range 250 to 600 mcg).
Subsequent dosing was based on the treatment effect in reducing the size of the fetal and on repeat fetal cord blood thyroid tests.
Main aim of antenatal therapy is to shrink the goiter. Role in long term neuro cognitive outcome is questionable.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Treatment of congenital hypothyroidism
Infants with low T4 and elevated TSH should be started on L-Thyroxine as soon as the diagnosis is made.
Initial dose of L-Thyroxine is 10-15 μg/Kg/day.
Infants with severe hypothyroidism (very low T4, very high TSH and absence of distal femoral and proximal tibial epiphyses on radiograph of knee) should be started with the highest dose of 15μg/Kg/day.
Preferred preparation is Sodium Levothyroxine. It has uniform potency, reliable absorption and good bioavailability.
Daily dose should be crushed and placed directly on the tongue in the morning.
Iron and Calcium preparations interfere with its absorption.
If a dose is missed, then double dose should be given on the next day. Dr Naveen Kumar Cheri
S.V. Medical College, Tirupati
Treatment of congenital hypothyroidism
Goal of therapy: T4 should be kept in the upper half of normal range (10-16 μg/dL) or free T4 in the 1.4-2.3 ng/dl range with the TSH suppressed in the normal range.
It takes less than a week for T4 to raise and 4-5 weeks for TSH to normalize.
Monitoring: T4 and TSH should be monitored according to following schedule.
Growth and development of infant should be monitored.
Overtreatment: Premature fusion of cranial sutures, acceleration of skeletal maturation, problems with temperament and behavior.
0 to 6 months Every 6 weeks
6 months to 3 years Every 3 months
Beyond 3 years Every 6 months
6 to 8 weeks after any dose change.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Treatment of congenital hypothyroidism
In case of permanent hypothyroidism, the care givers should be counselled regarding the nature of the condition, need for life long therapy, compliance and therapeutic monitoring.
Transient hypothyroidism presumed to be due to maternal goitrogenic drugs: It needs to be treated, if low T4 and high. Therapy can be discontinued after 8-12 weeks, if values return to normal.
Intake of anti-thyroid drugs can be continued by the hyperthyroid mothers during breast feeding because concentration of these drugs is very low in breast milk.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Treatment of congenital hypothyroidism
Transient hypothyroidism presumed to be due to maternal autoimmune thyroiditis:
If TBII (Thyroxine Binding Inhibitory Immunoglobulin) are documented in infant, treatment should be started if T4 is low and continued for 3-6 months.
If it is not possible to document TBII, continue treatment till the age of 3 years and then give a trial off therapy for 6 weeks followed by retesting of T4 and TSH to determine the need for continuation of therapy. If they are normal, monitor TSH annually.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Prognosis
It depends on age of onset of treatment, starting dose of l-Thyroxine & severity of hypothyroidism.
Age of onset of treatment : In infants in whom treatment was started between birth and 3 months of age, the mean IQ was 89; between 3 and 6 months of age, the mean IQ was 71; while if treatment did not start until after 6 months of age, the mean IQ dropped to 54.
Starting done of l-Thyroxine : Outcome is better in children a “high” dose 10.1-15 mcg/kg/day than “low” dose 6-8 mcg/kg/day and “intermediate” dose 8.1-10.0 mcg/kg/day.
Severity of hypothyroidism : Neonates having complete athyreosis, very low pre-treatment T4 levels and presenting with epiphyseal dysgenesis have poorer outcome.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Key messages
Congenital hypothyroidism is quite common in Indians and is the most common reversible congenital cause of mental retardation.
Early identification and intervention is important as Thyroid dependent brain development is complete by 3 years of age.
Universal screening is ideal as most cases are sporadic.
Positive cases on screening by filter paper test should be confirmed by serum levels estimation.
Serum Thyroid hormone levels are of primary importance in diagnosing and managing this condition, other investigations are ancillary.
Age based reference values must be followed in interpreting the results.
Timely monitoring (serum hormone levels, compliance, growth & development) and adequate counseling of care givers are key in managing this condition.
Dr Naveen Kumar CheriS.V. Medical College, Tirupati
Thank you
Dr Naveen Kumar CheriS.V. Medical College, Tirupati