Embed Size (px)
Citation preview

Correcting Presbyopia – Modern Options
Jason Higginbotham BSc (Hons) MCOptom FBDOHead of Clinical Affairs

What is Presbyopia?First noticed by the ancient Greeks, Presbyopia was considered to be a deficiency in the eyes ‘energy’ in focussing rays FROM the eyes onto near objects and that the weaker energy in the old meant that these rays could only be focussed on more distant objects and still be seen. Presbyopia, a natural age-related condition, is the result of a gradual decrease in accommodative amplitude, from about 15 dioptres (D) in early childhood to 1 D before the age of 60 years. An irreversible, normal physiologic condition that affects all primates, it impairs the ability to see clearly at near. If presbyopia is uncorrected, a significant functional visual disability is likely to develop. (AOA.ORG)Beers AP, van der Hiejde GL. Age-related changes in the accommodation mechanism. Optom Vis Sci 1996; 73:235-42.
Hamasaki D, Ong J, Marg E. The amplitude of accommodation in presbyopia. Am J Optom Arch Am Acad Optom 1956; 33:3-14.
Ramsdale C, Charman WN. A longitudinal study of the changes in the static accommodation response. Ophthalmic Physiol Opt 1989;9:255-63.

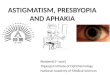
What is Presbyopia?In 1922, Duane did extensive research on amplitude of accommodation on some 4200 eyes.
AGE
AMPL
ITU
DE O
F AC
COM
MO
DATI
ON
(D) High Amplitude in childhood, but
reduction in amplitude begins very early on.
Presbyopia begins around the early forties, where the reduction in amplitude becomes symptomatic.
Depth of focus seems responsible for what little accommodation remains beyond around 50 years.
*With thanks to Leon Davies at Aston University

How does Accommodation work?Scheiner (1619) first suggested and proved some form of active mechanism was at work in the eye to change the total dioptric power of the eyes focussing system.
Descartes suggested the lens was responsible. Others also suggested a change in axial length of the eye, axial position of the lens, curvature change of internal refracting surfaces and change in pupil size were responsible.
We now know there is an element of a few of these at play – lens curvature change and thickness, slight movement of lens axial position and pupil size change.
Myopia studies also now show that there is a change in axial length of the eye to maintain internal ocular volume constants.

Accommodative Apparatus Revisited
Pardue and Sivak 2000
Longitudinal fibres (L)
Radial fibres (R)
Circular fibres (C)
When the ciliary muscle is relaxed, the circular and radial fibres pull the zonules tight and the zonules hold the lens capsule flatter. This keeps the lens in its unaccommodated state.
The longitudinal fibres seem to also produce some effects on the choroid and sclera which in turn can affect the vitreous pressure axially. It appears that during accommodation, there is some anterior axial pressure from the vitreous onto the lens, pushing it forward slightly and increasing positively the effective power of the total optical system.

Accommodative Apparatus Revisited
Lens anatomy is thought to be pivotal in how accommodation works via the recoil of parts of the lens capsule.
Lens Capsule anatomy after Fincham (1926)
Anterior
Posterior
The areas of highest thickness produce changes to the lens thickness and curvature as well as a reduction in equatorial diameter of the lens.

The Helmholtz Theory of AccommodationThe Helmholtz Theory is sometimes referred to as the relaxation theory of accommodation.
It postulates that the elastic capsule surrounding the crystalline lens is the driver of positive accommodation. As the ciliary muscle contracts and moves inwards, the tension on the zonules is released; allowing the lens capsule to recoil and try and take on a more circular shape. This forces the lens into a more steep curvature, with reduction in the equatorial lens diameter and an increase in the lens axial thickness.
Other theories exist, but for the purpose of this lecture and in accordance still with modern consensus, the Helmholtz Theory shall be taken as the most likely to be correct.

The Helmholtz Theory of AccommodationClassic ‘Relaxed versus Contracted’ diagram of Accommodation
Split MRI images of same eye in relaxed (right half) and accommodated state (left half).

PseudoaccommodationEssentially, Pseudoaccommodation in phakic patients can be defined as the ability of the unaccommodated emmetropic eye to view ‘near’ objects.
Ultimately, the primary factor in this is pupil size and thus depth of focus.
Pallikaris et al (2011) described Pseudoaccommodation in pseudophakes as a complex phenomenon that can be attributed to several static (i.e. pupil size, against-the-rule cylindrical refractive error, multifocality of the cornea) and dynamic (i.e. anterior movement of the implant itself) factors.

Methods of Correcting PresbyopiaThree Principal Approaches (Pallikaris et al 2008)
1) Provide functional multifocality in the visual system
2) Provide binocular divergence with one eye viewing Distant objects and the other eye viewing Near objects (i.e. MONOVISION)
3) Attempt to restore normal accommodation to the eye
Static – Surgical and non surgical
Static – Surgical and non surgical
Dynamic – Surgical only

Static techniques• Spectacles
- Reading glasses, or over refraction readers for CL’s- Bifocals- PAL’s (Progressive addition lenses)- Half eyes or monocles- Intermediate / occupational lenses
• Contact lenses- Monovision- Bifocal or Multifocal - Enhanced monovision multifocal
• Surgical- Corneal options- IOL’s (pIOL’s, mIOL’s, monovision, etc)- Scleral implants

Corneal Surgical Static techniquesThere are several corneal techniques which can be used to provide some form of presbyopia correction; these include:
• Corneal inlays (CI’s) / onlays (KAMRA)
• Laser ablation (LASIK or LASEK)
• Conductive keratoplasty (CK)
• Corneal implant lenses (Raindrop lens)
• Intrastromal Femtosecond Ring Incisions (INTRACOR)

Corneal Inlays / OnlaysKAMRA – This uses a circular ultrathin biomimetic stromal implant which has a small central aperture. This is normally implanted in the non dominant eye to improve depth of focus and provide a form of monovision through pseudoaccommodation.

Corneal Inlays / OnlaysPresbia Flexivue lens – This is what is often termed an Onlay as normally femtosecond laser is used and a small pocket is created to slip the tiny lens into. The lens is 3.5mm in diameter and has a central hole surrounded by a plano zone for distance vision. Beyond this is the optic zone which has a refractive addition power.
3.5mm
Pseudophakic patient with Presbia lens.

Corneal Inlays / OnlaysRaindrop Near Vision Inlay – This is an onlay that is tiny and is a centre near design optic. The raindrop ‘lens’ increases central corneal curvature and looks similar to a blended lenticular lens, adding power progressively from outside the optic zone to the central constant curve.
Implant lens is 2mm in diameter. Usually, a femtosecond laser is used to produce a pocket for lens implantation.Phakic patient with
raindrop lens implanted.

Corneal Laser AblationThe most basic option is to provide Monovision correction, usually with the dominant eye corrected fully for Distance and the other eye left myopic to between -1.00 and -2.50 DS usually.
Multifocal ablation or PRESBYLASIK involves ablating the cornea so that it has two focal zones, one Distance and the other Near.

PresbyLasikNidek use a Peripheral Presbyopic LVC approach with a clear distance central zone and a blended mid peripheral corneal near zone.
Supracor (Technolas) and Pulsar (CV Laser) use a Central Presbyopic LVC approach.

PresbyMax (Schwind)
Intermediate
Transition
This uses a blended central hyperpositive zone with a blended transition to distance in the pericentral cornea. There is also an element of monovision to maximise results; the central near zone being more myopic in the non dominant eye.

Presbyond (Zeiss)Often termed Laser Blended Vision, this also relies in part on the Monovision approach. The dominant eye is corrected almost to plano whilst the non dominant eye is given a -1.50DS Add, but this is added along a continuous refractive power gradient for the whole optic zone.

INTRACOR (Technolas)INTRASTROMAL FEMTOSECOND RING INCISIONS – Intracor. This uses five concentric rings created in the corneal stroma from around 2 to 4 mm from the optic axis/corneal intersection. These rings cause localised steepening, leading to concentric Distance / Near corrected zones. Normally this would be done on emmetropic patients or on pseudophakic emmetropic patients.

Conductive Keratoplasty (CK)This technique uses low frequency radio waves instead of laser thermokeratoplasty. The radio is applied to the peripheral cornea on 8 to 32 points. The heat causes localised shrinking of the tissue and this leads to overall steepening of the cornea. Essentially, this is used with a monovision approach on the non dominant eye to render it myopic.

Lenticular Surgical Static techniquesThere are several techniques which can be used to provide some form of static presbyopia correction with intra ocular lenses; these include: • Monofocal IOL’s using a monovision approach
• Multifocal IOL’s
• Phakic multifocal PIOL’s (anterior and posterior chamber)

Monovision with IOL’sJust as with contact lenses or with simple LASIK monovision, monovision IOL’s use the principle of correcting the dominant eye for distance and then leaving the non dominant eye myopic to some extent.
In any monovision surgical procedure, it is very common, if not essential, to have the patient trial the effect using contact lenses. Often these days, the patient is given high water content high DK/t Silicone Hydrogel CL’s to wear constantly for up to two weeks whilst they adapt to and trial the monovision effect. Sometimes, subtle alterations are still needed to give the patient the best result.

Pseudophakic Multifocal IOL’s (MIOL’s)MIOL’s can be broadly divided into two categories:
• Refractive• Diffractive
• Concentric• Sectorial
RefractiveMIOL’s
• Fully Diffractive• Partially Diffractive
Diffractive MIOL’s
All MIOL’s utilise simultaneous vision correction.

Concentric Refractive MIOL’sConcentric Refractive MIOL’s use multiple simultaneous zones of near and distance corrections. They are rotationally symmetrical. There are only a small number of zones and they are dependent on pupil size.
Refractive IOL in vivo
DIST
NEAR
DND

Sectorial Refractive MIOL’sSectorial Refractive MIOL’s use a more classic bifocal, rotationally asymmetrical style arrangement as below.
This lens produces fewer photic effects such as glare and dsyphotopsia due to only the near portion occurring inferiorly.

Diffractive MIOL’s
As the name suggests, these lenses use a continuous step concentric diffractive groove array, similar to a Fresnel lens. The width and height of the steps affect the effective power of the step. Ultimately, simultaneous focal lengths for distance and near occur at the same time with very little dependency on pupil size.

Fully Diffractive MIOL’sFully diffractive MIOL’s have the Fresnel steps over the whole optic zone of the lens.
Example include the Abbott Tecnis lens.

Partial Diffractive MIOL’sPartial diffractive MIOL’s have the Fresnel steps over the central portion of the optic zone of the lens.
Example include the Alcon Acrysof Restor MIOL.

Dynamic Presbyopia Correction
Dynamic Presbyopia correction (accommodative) is always surgical. This is roughly split into Lenticular and Scleral treatments. These include:
• AIOL’s• Piggy back• Lens Refilling• Lentotomy
Lenticular
• LAPR• Scleral Expansion bandsScleral

AIOL’sThere are two different principles used in AIOL design.
• Axial shift designs. These use a single or dual optic implanted lens which is moved anteriorly during accommodation, adding greater effective power to the eye.
• Curvature shift designs. These tend to still be in their experimental and testing phases at present.
Currently, the majority of AIOL’s are axial shift and use a single optic lens. The dual optic designs that are available tend to be large and sometimes problematic to implant.

Axial Shift AIOL’sAs mentioned earlier, during the process of accommodation, as well as the ciliary muscle constricting and the sphincter reduces in diameter, the vitreous is also shown to move forwards anteriorly.
It is not totally clear if axial shift lenses work solely because of vitreous shift, ciliary constriction, a combination of the two or even due to some other as yet unknown cause(s).
3-dimensional (3-D) view of merged full anterior segment image 3-D opticalcoherence tomography postoperatively in the same patient implanted with the Crystalens IOL for 3 different accommodative efforts (Susana Marcos et al Ophthalmology 2014;121:45-55 ª 2014 by the American Academy of Ophthalmology.)

Single Optic Axial Shift AIOL’s
Crystalens (Bausch and Lomb)Single Optic
Tetraflex (Lenstec)Single Optic
1CU(Human Optics)Single Optic

Dual Optic Axial Shift AIOL’s
Synchrony (AMO)Dual Optic
Sarfarazi (Shenasa Medical)Dual Optic

Curvature Shift AIOL’sThese AIOL’s are still really only in developmental stages. Ultimately, these are dynamic accommodating AIOL’s whereby, due to changes in the ciliary muscles during accommodation, movement of fluid and other mechanics changes the curvature of one or more optical surfaces to increase convex dioptric power. Accommodation gained can range from 5 to 10D.
Fluid Vision Lens (Powervision)Dual Optic
Fluid Vision Lens (Powervision)Dual Optic

Lens Refilling
For decades, attempts have been made to replace the lens contents with some form of gel like substance that acts in a similar fashion to the natural lens fibrils.
Medennium (California) now produces what it calls a ‘smart’ hydrophobic acrylic material which reacts to heat from the body’s temperature (thermo-dynamic). The accommodation then occurs naturally in the same way as would occur via the elastic capsule.
The capsule is ‘repaired’, but there are instances of the material leaking. There is little data to show how effective this treatment is.

Lentotomy
Lentotomy is often referred to as lens softening and uses a femtosecond laser to produce a series of cuts or voids within the lens following the curvature of the fibrils.
These voids allow for the multiple lens layers to more easily slide over each other, allowing the lens to become more flexible again.

Scleral Modification - Theory
As briefly mentioned earlier, Schachar has postulated that accommodation is driven by zonular traction pulling the lens into a more convex shape due to the physiology of the capsule. He suggests that the increase in equatorial lens diameter means there is less zonular tension later in life, leading to presbyopia.
Schachar developed a surgical scleral technique in the 1980’s to increase the tension and zonular ‘pull’ via the longitudinal ciliary muscles.

Scleral Expansion Bands
Essentially, this involves inserting PMMA bands just under the Sclera near the ciliary muscle. The effect seems to pull the zonular anchors further away from the lens equator, supposedly increasing the tension and their effectiveness.

LAPR
LAPR stand for Laser Assisted Presbyopia Reversal. Essentially, this too is based on the Schachar theory. A fibre-optic YAG laser is used to ablate a series of laser spots into several regions of the scleral near to the ciliary longitudinal muscle insertions and the ora serata.
It is thought that due to shrinking / scarring of the tissue, the position of the zonular anchor is moved in such a way as to increase the tension it provides to the capsule and thus increase the accommodative amplitude.
Results have shown an increase of around 1.5D of accommodation in patients, though there is little data in total.

Presbyopia Control Techniques
Some non peer reviewed sources have suggested that there are methods and ways to avoid presbyopia. These suggestions include:
• Wearing sunglasses far more often to reduce UV and blue light damage to the crystalline lens
• Change the diet to improve lens structure and health• Use of vitamins and supplements to improve lens structure• Exercises, such as the ‘Read without Glasses Method’
Currently, I can find little in the way of papers that provide any evidence to support any of these suggestions. There is evidence that some patients using the exercises are simply overcoming underlying binocular function deficits and that this reduces near vision related asthenopia.

Thank you for listening

References• Girish G Kamath, Somdutt Prasad, Amanda Danson, Russell P Phillips Visual outcome with the Array
multifocal intraocular lens in patients with concurrent eye disease J Cataract Refract Surg. 2000 Apr;26(4):576-81.
• Raquel Gil-Cazorla, Shehzad A. Naroo, Sunil Shah A review of the surgical options for the correction of presbyopia Br J Ophthalmol doi:10.1136/bjophthalmol-2015-306663
• Ian L. Bailey a, Jan E. Lovie-Kitchin Visual acuity testing. From the laboratory to the clinic Vision Research Volume 90, 20 September 2013, Pages 2–9
• Navneet Gupta Functional near visual assessment in presbyopia Aston University 2008• Wright KW, Guemes A, Kapadia MS, Wilson SE. Binocular function and patient satisfaction after
monovision induced by myopic photorefractive keratectomy. J Cataract Refract Surg 1999; 25:77–82.• Buckhurst PJ1, Wolffsohn JS, Gupta N, Naroo SA, Davies LN, Shah S. Development of a questionnaire to
assess the relative subjective benefits of presbyopia correction. J Cataract Refract Surg. 2012 Jan; 38(1):74-9. doi: 10.1016/j.jcrs.2011.07.032. Epub 2011 Nov 10.
• Navneet Gupta, James S Wolffsohn, Shehzad A. Naroo, , , Leon N. Davies, George A. Gibson, Sunil Shah Development of a near activity visual questionnaire to assess accommodating intraocular lenses Contact Lens and Anterior Eye Volume 30, Issue 2, May 2007, Pages 134–143
• Ioannis G.Pallikaris, Georgios A. Kontadakis and Dimitra M. Portaliou Real and Pseudoaccommodation in Accommodative Lenses Institute of Vision and Optics Journal of Ophth – Volume 2011, Article ID 284961

• Review of Optometry Product Review. 15.12.15 • Sergio Barbero, Susana Marcos and Ignacio Jime´nez-Alfaro Optical aberrations of intraocular lenses
measured in vivo and in vitro Opt. Soc. Am. A Vol. 20, No. 10/October 2003/J. • Beata Żelichowska, MD, Marek Rękas, PhD, , Andrzej Stankiewicz, PhD, Alejandro Cerviño, PhD, Robert
Montés-Micó, PhD Apodized diffractive versus refractive multifocal intraocular lenses: Optical and visual evaluation Journal of Cataract & Refractive Surgery Volume 34, Issue 12, December 2008, Pages 2036–2042
• Michael Mrochen, Maik Kaemmerer, Theo Seiler Clinical results of wavefront-guided laser in situ keratomileusis 3 months after surgery Journal of Cataract & Refractive Surgery Volume 27, Issue 2, February 2001, Pages 201–207
• Achim Langenbucher, Susanne Goebels, Nóra Szentmáry, Berthold Seitz and Timo Eppig Vignetting and Field of View with the KAMRA Corneal Inlay Biomed Res Int. 2013; 2013: 154593.
• Amy L Sheppard, Abar Bashir, James S Wolffsohn, Leon N Davies Accommodating intraocular lenses: a review of design concepts, usage and assessment methods Clin Exp Optom 2010; 93: 6: 441–452
• Gupta N, Wolffsohn J, Naroo SA. Optimizing measurement of subjective amplitude of accommodation with defocus curves. J Cataract Refract Surg. 2008 Aug;34(8):1329-38. doi: 10.1016/j.jcrs.2008.04.031.
References (cont.)