Embed Size (px)
DESCRIPTION
محاضرات عين شمس
Citation preview

Colorectal Polyps
Ahmed A Abou-Zeid
Professor of Surgery
Ain Shams University

What is a Polyp
• Any lesion that is elevated above the mucosal surface of the bowel

Classification• Neoplastic
– Single• Adenomatous polyps• Connective tissue polyps (fibroma, lipoma, leiomyoma,
lymphoma)
– Polyposis Syndromes• FAP• HNPCC
• Non- neoplastic• Hamartomas• Metaplastic polyps• pseudopolyps

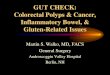
Adenomatous polyps
• Tubular adenoma
• Tubulovillous adenoma
• Villous adenoma

Adenomatous polyps
Tubular Adenoma Villous Adenoma

Adenomatous Polyps Clinical Picture
• Symptomless
• Bleeding
• Discharge
• Prolapse
• Obstruction/Intussusception
• Hypokalemia/Hypoproteinemia

Polyp - Cancer Sequence
• Circumstantial evidence– Similar anatomical distribution– Adenomas can harbour foci of carcinoma – Polyp patients are 8-10 years younger– 30% of CRC have synchronous polyps– Metachronous cancer is twice as high in
those cancers with associated polyps– Prophylactic polypectomy decrease incidence
of subsequent cancer

Adenoma-Carcinoma Sequence
Normal
Dysplasia
Adenoma
Carcinoma

Suspicious Polyp
• Size
• Age of polyp
• Histology

Initial ManagementEndoscopic Procedures
Endoscopic Polypectomy
Pedunculated Sessile
Endoscopic Submucus Resection

Initial ManagementTransanal Procedures
Endoanal Submucus Resection
Transanal Endoscopic Microsurgery (TEM)

Initial ManagementAbdominal Procedures
• Colotomy/Colectomy• Proctotomy/Proctectomy

The Polyp With a Malignant Focus

Management of Malignant Polyp
• Polypectomy- Pedunculated- Well differentiated- In Head or stalk,
away from resection margin
- No vascular or lymphatic invastion
- Clear resection margins
• Radical Resection
- Sessile
- Poor differentiation
- Low in stalk
- Vascular or lymphatic invasion
- Involved resection margin

Further Management of Malignant Polyp
Radical Resection
• Site of resection entitled by site of the polyp
• Radicality of resection entitled by extent of the polyp
• India ink injection in the era of laparoscopic surgery

Follow Up After Polypectomy
• Benign polyp - Yearly endoscopy after positive complete clearance- Three yearly endoscopy after negative complete clearance- Five yearly therafter
• Malignant polyp - Follow guidelines of cancer management

Metaplastic Polyps
• Also known as hyperplastic polyps• Usually minute (2-5mm), plaque like,
same colour of mucosa• Asymptomatic, do not turn malignant• Elongated tubules, scanty goblet cells,
hyperplastic cells at the base of crypts• Management depends on individual
policy

Hamartomatous Polyps• Juvenile polyps
• Peutz-Jeghers polyps

Juvenile Polyps• Seen in infants and children less than 10 y• Mostly situated in the rectum• Usually stalked, head covered by granulation tissue• Cut surface shows dilated cystic spaces, bulk of
polyp made up of connective tissue full of acute & chronic inflammatory cells
• Rectal bleeding, polyp prolapse• Not pre-malignant• Treatment by colonoscopy & polypectomy

Peutz Jeghers Syndrome
• Autosomal dominant inheritance• Pigmentation• Polyps• Symptoms of rectal bleeding and recurrent
intussusception• Debate considering the malignant potential• Conservative management versus more
aggressive endoscopic management

Peutz Jeghers Syndrome

Inflammatory Polyps
• Accompany Chronic inflammatory process of the bowel
• Composed of oedamatous mucosal tags
• Not premalignant
• Treatment of the cause

Inflammatory Polyps

Connective Tissue Polyps
Submucuos Lipoma

Connective Tissue Polyps
• Can be benign or malignant
• Size dictates symptomatology in benign lesions
• Commonly present by obstructive symptoms
• Treatment: Segmental resection

Familial AdenomatousPolyposis
• Autosomal dominant inheritance• Mutation in APC gene• Easily recognized by its phenotypic
features– CR polyps and cancer– Extracolonic lesions
• 100% penetrance• 1 in 8,300 to 1 in 14,025 live births

Familial AdenomatousPolyposis

FAP/Extracolonic Lesions
• Desmoids
• CHRPE
• Duodenal adenomas
• Gastric glandular hypertrophy
• Osteomas/Neuromas
• Other tumours

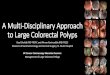
FAP/Extracolonic Lesions
CHRPE Intra-abdominal Desmoid

FAP/Diagnosis
• Clinical diagnosis– Colonic lesions
– Extra-colonic lesions
• Sigmoidoscopy/Colonoscopy
• Genetic diagnosis
• Surveillance

FAP/Treatment
• Prococolectomy/ Brook’s ileostomy
• Restorative proctocolectomy
• Total colectomy/ileorectal anastomosis

HNPCC• Characterized by
– Autosomal dominant inheritance– Mutation in MMR gene– Early onset CR cancer and polyps– Extracolonic cancers
• Diagnosis: Less evident phenotypic features– Family history criteria– Pathology criteria– Genetic criteria

Family History
• Amsterdam criteria
– CRC in 3 family members
– One member 1st degree relative to other two
– Two successive generations
– One cancer diagnosed less than 40
– FAP excluded
• Others (less strict criteria)

Pathology Criteria
• Young age of onset
• Right sided tumors
• Multiple colonic tumors
• Extra-colonic tumors
• Aggressive histopathology features
• Good prognosis

Genetic Criteria
• Disordered mismatch repair genes– hMLH1– hMSH2– hPMS1– hPMS2– hMSH3– hMSH6

Extracolonic Tumours in HNPCC
• Small intestine
• Endometrium
• Urothelium
• Biliary tree
• Gastric mucosa
• Others

Treatment of HNPCC
• Total colectomy/ileorectal anastomosis
• Restorative proctocolectomy
• Surveillance