Embed Size (px)
DESCRIPTION
Cours de Croissance et développement aux étudiants en médecine dentaire. MDD 20049 Partie 2: Développement squelettique
Citation preview

Croissance et Développement
MDD 200492-0 Développement squelettique

©Dr Sylvain Chamberland;sylvainchamberland.com
Croissance squelettique
• Au niveau cellulaire
✦ Hypertrophie: augmentation de la dimension des cellules
✦ Hyperplasie: augmentation du nombre de cellules
✦ Sécrétion de matière extracellulaire: Augmentation de la dimension indépendamment du nombre ou de la dimension des cellules
• Ces 3 processus surviennent dans la croissance squelettique avec prédominance de sécrétion extracellulaire, suivi d’hyperplasie et peu d’hypertrophie. 2

©Dr Sylvain Chamberland; sylvainchamberland.com
• Tissus dur = os, dents, cartilages
• Tissus mous= tout le reste
✦ Le cartilage participant à la croissance doit être considéré comme un tissu mou
• Croissance interstitielle
✦ Croissance se produit par une combinaison d’hyperplasie et d’hypertrophie partout dans le tissu
✦ Caractéristique de la croissance de presque tous les tissus mous et du cartilage non-calcifié du squelette
3

©Dr Sylvain Chamberland; sylvainchamberland.com
• Tissus durs minéralisés (os)
✦ Croissance interstitielle impossible
✦ Hyperplasie, hypertrophie et sécrétion extracellulaire possible en surface et non à l’intérieur de la substance minéralisée
✦ Périoste (membrane de t. mous): croissance interstitielle possible
✓ Permet apposition d’os en surface
✓ Formation de nouvelles cellules et sécrétion de matière extracellulaire ➡ minéralisation ➡nouvel os = Apposition de surface ou directe
4

©Dr Sylvain Chamberland;sylvainchamberland.com
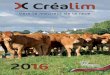
• 8 à 12 semaines intra-utérin
• Plaque cartilagineuse avasculaire s’étendant de la capsule nasale jusqu’au foramen occipital
✦ Nourri par diffusion
• Au 4e mois in utero
✦ Invasion d’éléments vasculaires
✦ Ce qui devient des centres d’ossifications➡ formation d’îlots osseux entourés de cartilage
Chondrocrâne
5

©Dr Sylvain Chamberland; sylvainchamberland.com
• Croissance continue et rapide du cartilage qui est remplacé aussi rapidement par de l’os
• Le chondrocrâne est remplacé graduellement par de larges sections osseuses : os occipital, sphénoïde, ethmoïde, vomer, partie mastoïde & pétreuse du temporal
• La croissance aux jonctions cartilagineuses avec ces os se fait comme pour la croissance des membres
6

©Dr Sylvain Chamberland; sylvainchamberland.com
• Embryogenèse du tissu squelettique crâniofacial
✦ Chondrogenèse
✓ Formation de cartilage
✦ Ossification endochondrale
✓ Conversion du cartilage en os
✦ Ossification intramembraneuse
✓ Formation d’os à partir de mesenchyme indifférencié
7

©Dr Sylvain Chamberland;sylvainchamberland.com
• Chondroblastes produisent une matrice ➙sécrétion extracellulaire
• Cellules emprisonnées dans la matrice = chondrocytes
✦ Périchondre produit d’autres chondroblastes en surface
• Hypertrophie des chondrocytes et sécrétion de matrice➙croissance interstitielle
• La matrice demeure non calcifiée
• La membrane couvre la surface mais n’est pas essentielle. Le cartilage est tolérant à la pression (articulation)
Chondrogénèse
8

©Dr Sylvain Chamberland;sylvainchamberland.com
• Centre d’ossification au centre de l’os (diaphyse) et aux extrémités (épiphyses)
• Plaque épiphysaire entre les 2
✦ Cartilage épiphysaire➡ Hyalin➡Hypertrophie➡Minéralisation intracellulaire➡os spongieux
• Cartilage épiphysaire responsable de la croissance des os en longueur
• Périoste: croissance en épaisseur et remodelage externe
Croissance des os longs
Rakosi et al, Orthodontic -Diagnosis, p. 11, Thieme, 19939

©Dr Sylvain Chamberland;sylvainchamberland.com
Ossification endochondraleCroissance épiphysaire
• Prolifération cellulaire
• Hypertrophie
• Sécrétion de matrice extracellulaire
• Minéralisation, invasion de vaisseaux sanguins➡différenciation d’ostéoblastes ➙calcification de substances ostéoïdes ➙formation osseuse
• Membrane essentielle pour la survie de l’os10

©Dr Sylvain Chamberland;sylvainchamberland.com
• Os long: cartilage hyalin
• Condyle: fibrocartilage
11

©Dr Sylvain Chamberland;sylvainchamberland.com
Ossification intramembraneuse
• Sécrétion de matrice osseuse dans le tissu conjonctif sans l’intermédiaire du cartilage
• Survient dans la voûte crânienne et dans les maxillaires
12

©Dr Sylvain Chamberland;sylvainchamberland.com
Ossification intramembraneuse
• Différentiation d’ostéoblastes à partir du mésenchyme et production de tissus ostéoïdes
• Les cellules et vaisseaux sanguins sont emprisonnés ➙ostéocytes et système haversien➙croissance par apposition provenant des ostéoblastes du périoste
• Calcification de la substance ostéoïde. Ce sont les vaisseaux sanguins englobés qui assure la nutrition des cellules
• Membrane essentielle à la survie de l’os (endoste et périoste) 13

©Dr Sylvain Chamberland;sylvainchamberland.com
Ossification intramembraneuse
• Croissance interstitielle impossible
• Formation osseuse entièrement par apposition d’os nouveau en surface
• Changement de forme = Remodelage
✦ Résorption osseuse (vieil os) à certains endroits
✦ Apposition osseuse (nouvel os) à d’autres endroits
• Remodelage osseux: autant dans l’os endochondral que l’os membraneux
14

©Dr Sylvain Chamberland;sylvainchamberland.com
Mandibule
• Procès mandibulaire du 1re arc branchial
• Entièrement croissance intramembraneuse
• Condensation du mésenchyme latéralement au cartilage de Meckel qui régresse
✦ Résidus: 2 osselets de l’oreille moyenne (marteau et enclume) et ligament sphénomandibulaire
• Ce cartilage se désintègre à mesure que la mandibule se développe
15

©Dr Sylvain Chamberland; sylvainchamberland.com
• Cartilage condylien:
✦ Cartilage secondaire indépendant qui fusionne avec la branche montante mandibulaire
✓ A: zone de condensation séparée de mésenchyme
✓ B: Fusion avec le corps mandibulaire 4 mois in utéro
✓ C: Présentation à la naissance
16

©Dr Sylvain Chamberland;sylvainchamberland.com
• Centre de condensation mésenchymateux dans les procès maxillaires du 1re arc branchial
• Latéralement à la capsule nasale
✦ Le cartilage nasal participe à l’allongement de la face et au déplacement antérieur du maxillaire, mais ne participe pas à la formation du maxillaire
Maxillaire
17

©Dr Sylvain Chamberland;sylvainchamberland.com
Croissance du complexe crâniofacial
• À comprendre
✦ Site de croissance
✦ Type de croissance aux différents sites
✦ Facteurs de contrôle de cette croissance
18

©Dr Sylvain Chamberland;sylvainchamberland.com
Croissance du complexe crâniofacial
• Voûte crânienne
✦ Au dessus et autour du cerveau
• Base crânienne
✦ Sous le cerveau et divisant le crâne de la face
• Complexe nasomaxillaire
✦ Nez, maxillaire et les os associés
• Mandibule
19

©Dr Sylvain Chamberland;sylvainchamberland.com
Voûte crânienne
• Os plats formés par ossification intramembraneuse sans cartilages précurseurs
• Centres d’ossification dont la croissance se fait par activité périostéale sur les surfaces externes et internes
• Le remodelage et la croissance se fait à la jonction des différents os crâniens (sutures crâniennes), par apposition sur la surface externe et résorption à la face interne
• Croissance complétée à 90% à 5 ans et 98% à 15 ans20

©Dr Sylvain Chamberland;sylvainchamberland.com
Voûte crânienne
• Matrice neurocrânienne: expansion de la masse neurale
• Séparation des os de la voûte (a et b)
• Croissance suturale (c)
• Transformation par apposition et résorption périostéale et endostéale (d)
Rakosi et al, Orthodontic -Diagnosis, p. 34, Thieme, 1993
21

©Dr Sylvain Chamberland;sylvainchamberland.com
Base crâninenne
• Initialement, cartilage qui se transforme en os par ossification endochondrale
• Centre d’ossification joint par des synchondroses
✦ Synchondrose intersphénoïde (fermeture à la naissance), sphéno-ethmoïdale (fermeture à 6 ans) et sphéno-occipital (fermeture à 13-15 ans)
✦ Synchondrose : semblable à une plaque épiphysaire à 2 côtés
✓ Bande d’hyperplasie cellulaire au centre avec 2 bandes de cellules cartilagineuses maturant et s’allongeant dans 2 directions pour se transformer en os
22

©Dr Sylvain Chamberland;sylvainchamberland.com
Complexe naso-maxillaire
• Ossification entièrement intramembraneuse
• Croissance
✦ Apposition d’os aux sutures de la voûte et de la base crânienne
✦ Remodelage de surface (résorption de la partie antérieure)
• Le maxillaire est déplacé antéro-inférieurement lors de sa croissance
✦ Croissance du vomer, de la lame perpendiculaire de l’ethmoïde et du cartilage nasal
23

©Dr Sylvain Chamberland; sylvainchamberland.com
• Apposition d’os aux sutures
✦ Allongement des apophyses maxillaires
✦ Tubérosités: espace pour les dents primaires et permanentes
• Le maxillaire est déplacé antérieurement lors de sa croissance
✦ Translation antérieure
• Remodelage de surface:
✦ Résorption de la surface antérieure en même temps que le maxillaire se déplace antérieurement
24

©Dr Sylvain Chamberland; sylvainchamberland.com
• Plancher palatin
✦ Déplacement antérieur et inférieur avec le maxillaire
✓ Résorption osseuses du côté nasal
✓ Apposition du côté oral
‣ Résorption de la surface supérieure et apposition sur la face inférieure en même temps que le palais se déplace inférieurement
• Antérieurement
✦ Résorption de la partie antérieure du procès alvéolaire sous l’épine nasale, annulant partiellement la translation antérieure
25

©Dr Sylvain Chamberland; sylvainchamberland.com
• Changement en largeur du maxillaire
✦ Élargissement en vue frontale à mesure que la voûte palatine se déplace inférieurement
✦ Croissance à la suture interpalatine et intermaxillaire jusqu’à ~ 5 ans
✦ Après: apposition osseuse sur la face externe du maxillaire et éruption buccale des dents
26

©Dr Sylvain Chamberland;sylvainchamberland.com
• Croissance par activité
✦ Endochondrale
✓ Fibrocartilage à l’ATM
✦ Périostéale (apposition et remodelage)
✓ Toutes les autres parties de la mandibule
• La croissance se fait par les condyles, le corps mandibulaire et le procès alvéolaire et non pas par apposition au niveau du menton
Mandibule
27

©Dr Sylvain Chamberland;sylvainchamberland.com
Mandibule
• Corps de la mandibule
✦ Allongement par apposition périostéale sur la surface postérieure
✦ Résorption de la partie antérieure de la branche montante
✦ Zone de résorption sur la face antérieure au dessus du menton
• Branche montante
✦ Allongement par croissance endochondrale
28

©Dr Sylvain Chamberland;sylvainchamberland.com
• Croissance des condyles
✦ s’exprime en direction supérieure, postérieure ou antérieure
• Croissance mandibulaire
✦ s’exprime en direction inférieure et antérieure
• Ce déplacement mandibulaire et la croissance du complexe nasomaxillaire permet la croissance de la langue, du pharynx et des autres structures reliées
Translation mandibulaire
29

©Dr Sylvain Chamberland; sylvainchamberland.com
• Croissance du procès alvéolaire
✦ 100% dépendant de la présence et de l’éruption des dents
✦ Suivant une extraction: résorption alvéolaire
✦ L’accroissement de la hauteur faciale est le résultat de la croissance des procès alvéolaires maxillaire et mandibulaire qui est associée à l’éruption des dents
30

©Dr Sylvain Chamberland;sylvainchamberland.com
• Résorption osseuse sur la face externe du V
• Apposition osseuse sur la face interne
• Le V se déplace postérieurement et s’élargit simultanément
• Déplacement et augmentation de la dimension sont unifiés dans un seul procédé
• Relocalisation continue
Principe du V
31

©Dr Sylvain Chamberland
Principe du V• Mandibule
• Maxillaire
• Condyle
• Voûte palatine
32

©Dr Sylvain Chamberland;sylvainchamberland.com
Principe de surface
• La surface en direction de la croissance est sujette à la déposition
• La surface opposée à la croissance est sujette à la résorption
• La direction de croissance n’est pas la même pour toutes les surfaces
• Des aires de dépositions et de résorptions peuvent se juxtaposer
33

©Dr Sylvain Chamberland;sylvainchamberland.com
Croissance périoste vs endoste
• Corticale en direction de la croissance
✦ Périoste = apposition
✦ Endoste = résorption
• Corticale opposée à la direction de croissance
✦ C’est l’inverse
• Ligne d’inversion (*) = ∆ direction de croissance
✦ Partie antérieure du maxillaire se déplace inférieurement avec la voûte palatine
34

©Dr Sylvain Chamberland;sylvainchamberland.com
Site & centre de croissance• Site
✦ Région où se produit de la croissance
✓ Ex: sutures du maxillaire, sutures crâniennes
• Centre
✦ Endroit où une croissance contrôlée génétiquement se produit
✓ Ex: plaque épiphysaire, synchondrose crânienne, cartilage nasal
‣ Mais pas le cartilage condylien: régénérescence lors de fracture en bas âge
• Tous les centres de croissances sont des sites, mais l’inverse n’est pas vrai.
35

©Dr Sylvain Chamberland;sylvainchamberland.com
Rôle des cartilages primaires
• Centre de croissance, prédisposition génétique
• Agit comme un tissu autonome lors de la croissance
• Capable de croissance interstitielle
• Tolérant à la pression, non-calcifié, flexible, avasculaire, ne requiert pas de membrane nutritive
• Synchondrose sphéno-occipitale contribue à la croissance crâniofaciale jusqu’à l’âge de 6 ans (faible contribution par la suite)
36

©Dr Sylvain Chamberland;sylvainchamberland.com
Bibliographie
• Proffit WR, Fields HW, Sarver DM, Contemporary Orthodontics, 4e éd, St-Louis: Mosby Elsevier, 2007; ISBN-13: 978-0-323-04046-4
✦ Section II, chapitre 3: Early stages of development
✦ Section II, chapitre 4: Later stages of development
• Bishara SE, Textbook of Orthodontics, Philadelphie: WB Saunders, 2001; ISBN: 0-7216-8289-8
✦ Chapitre 1: Overview of embryology and head and neck development
✦ Chapitre 4: Introduction to the growth of the face
37

©Dr Sylvain Chamberland;sylvainchamberland.com
Annexe
• Référence
• Contemporary Orthodontics 4e édition
38

Figure 2-5 Growth can be plotted in either height or weight at any age (the black line here) or the amount of change in any given interval (the maroon line here, showing the same data as the black line). A curve like the black line is called a "distance curve," whereas the maroon line is a "velocity curve." Plotting velocity rather than distance makes it easier to see when accelerations and decelerations in the rate of growth occurred. These data are for the
growth of one individual, the son of a French aristocrat in the late eighteenth century, whose growth followed the typical pattern. Note the acceleration of growth at adolescence, which occurred for this individual at about age 14. (Redrawn from Tanner JM. Growth at Adolescence, 2nd ed. Oxford: Blackwell Scientific Publications; 1962.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 2 January 2008 05:23 PM)© 2007 Elsevier

Figure 2-1 Schematic representation of the changes in overall body proportions during normal growth and development. After the third month of fetal life, the proportion of total body size contributed by the head and face steadily declines. (Redrawn from Robbins WJ, et al. Growth. New Haven: Yale University Press; 1928.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 04:19 PM)© 2007 Elsevier

Figure 2-6 Growth velocity curves for early-, average-, and late-maturing girls. It is interesting to note that the earlier the adolescent growth spurt occurs, the more intense it appears to be. Obviously, at age 11 or 12, an early maturing girl would be considerably larger than one who matured late. In each case, the onset of menstruation (menarche) (M1, M2, and M3) came after the peak of growth velocity.
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 2 January 2008 05:23 PM)© 2007 Elsevier

Figure 2-11 If growth velocity data for a group of individuals with a different timing of the adolescent growth spurt are plotted on a chronologic scale, it is apparent that the average curve is not an accurate representation of the pattern of growth for any particular individual. This smoothing of individual variation is a characteristic of cross-sectional data and a major limitation in use of the cross-sectional method for studies of growth. Only by following
individuals through time in a longitudinal study is it possible to see the details of growth patterns.
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 2 January 2008 05:23 PM)© 2007 Elsevier

Figure 3-14 Graphs of growth in length and weight in infancy for boys (the curves for girls are almost identical at these ages). Note the extremely rapid growth in early infancy, with a progressive slowing after the first 6 months. (Based on data from the National Center for Health Statistics.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 3 January 2008 03:36 PM)© 2007 Elsevier

Figure 4-2 Growth curves for the maxilla and mandible shown against the background of Scammon's curves. Note that growth of the jaws is intermediate between the neural and general body curves, with the mandible following the general body curve more closely than the maxilla. The acceleration in general body growth at puberty, which affects the jaws, parallels the dramatic increase in development of the sexual organs. Lymphoid involution also occurs at
this time.
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 3 January 2008 03:57 PM)© 2007 Elsevier

Figure 4-3 Velocity curves for growth at adolescence, showing the difference in timing for girls and boys. Also indicated on the growth velocity curves are the corresponding stages in sexual development (see text). (From Marshall WA, Tanner JM. Puberty. In: Falkner F, Tanner JM, eds. Human Growth, vol 2, ed 2. New York: Plenum Publishing; 1986.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 3 January 2008 04:22 PM)© 2007 Elsevier

Figure 4-5 On the average, the spurt in growth of the jaws occurs at about the same time as the spurt in height, but it must be remembered that there is considerable individual variation. (From Woodside DG. In: Salzmann JA, ed. Orthodontics in Daily Practice. Philadelphia: JB Lippincott; 1974.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 3 January 2008 07:08 PM)© 2007 Elsevier

Figure 2-18 Development and maturation of the chondrocranium (cartilage: light blue; bone: stippled dark blue). A, Diagrammatic representation at about 8 weeks. Note that an essentially solid bar of cartilage extends from the nasal capsule anteriorly to the occipital area posteriorly. B, Skeletal development at 12 weeks. Ossification centers have appeared in the midline cartilage structures, and, in addition, intramembranous bone formation of the jaws
and brain case has begun. From this point on, bone replaces cartilage of the original chondrocranium rapidly, so that only the small cartilaginous synchondroses connecting the bones of the cranial base remain.
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 07:03 PM)© 2007 Elsevier

Figure 2-19 A, Endochondral ossification at an epiphyseal plate. Growth occurs by proliferation of cartilage, occurring here at the top. Maturing cartilage cells are displaced away from the area of proliferation, undergo hypertrophy, degenerate, and are replaced by spicules of bone, as seen in the bottom. B and C, Endochondral ossification in the head of the condyle. A layer of fibrocartilage lies on the surface, with proliferating cells just beneath. Maturing and
degenerating cartilage cells can be seen toward the area of ossification.
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 07:03 PM)© 2007 Elsevier

•Orthodontic Diagnosis–Rakosi T., Jonas I., Graber TM, Thieme 1993

Figure 2-21 Diagrammatic representation of the relation of initial bone formation in the mandible to Meckel's cartilage and the inferior alveolar nerve. Bone formation begins just lateral to Meckel's cartilage and spreads posteriorly along it without any direct replacement of the cartilage by the newly forming bone of the mandible. (Redrawn from Ten Cate AR. Oral Histology: Development, Structure and Function, 5th ed. St. Louis: Mosby; 1998.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 07:03 PM)© 2007 Elsevier

Figure 2-22 The condylar cartilage (blue) develops initially as a separate area of condensation from that of the body of the mandible, and only later is incorporated within it. A, Separate areas of mesenchymal condensation, at 8 weeks. B, Fusion of the cartilage with the mandibular body, at 4 months. C, Situation at birth (reduced to scale).
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 07:03 PM)© 2007 Elsevier

Figure 2-24 Diagrammatic representation of the synchondroses of the cranial base, showing the locations of these important growth sites.
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 07:03 PM)© 2007 Elsevier

Figure 2-25 Diagrammatic representation of growth at the intersphenoid synchondrosis. A band of immature proliferating cartilage cells is located at the center of the synchondrosis, while a band of maturing cartilage cells extends in both directions away from the center, and endochondral ossification occurs at both margins. Growth at the synchondrosis lengthens this area of the cranial base. Even within the cranial base, bone remodeling on surfaces is also
important-it is the mechanism by which the sphenoid sinus(es) enlarges, for instance.
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 07:03 PM)© 2007 Elsevier

Figure 2-26 As growth of surrounding soft tissues translates the maxilla downward and forward, opening up space at its superior and posterior sutural attachments, new bone is added on both sides of the sutures. (Redrawn from Enlow DH, Hans MG. Essentials of Facial Growth. Philadelphia: WB Saunders; 1996.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 09:04 PM)© 2007 Elsevier

Figure 2-27 As the maxilla is carried downward and forward, its anterior surface tends to resorb. Resorption surfaces are shown here in dark yellow. Only a small area around the anterior nasal spine is an exception. (Redrawn from Enlow DH, Hans MG. Essentials of Facial Growth. Philadelphia: WB Saunders; 1996.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 09:04 PM)© 2007 Elsevier

Figure 2-28 Surface remodeling of a bone in the opposite direction to that in which it is being translated by growth of adjacent structures creates a situation analogous to this cartoon, in which the wall is being rebuilt to move it backward at the same time the platform on which it is mounted is being moved forward. (Redrawn from Enlow DH, Hans MG. Essentials of Facial Growth. Philadelphia: WB Saunders; 1996.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 09:04 PM)© 2007 Elsevier

Figure 2-29 Remodeling of the palatal vault (which is also the floor of the nose) moves it in the same direction as it is being translated; bone is removed from the floor of the nose and added to the roof of the mouth. On the anterior surface, however, bone is removed, partially canceling the forward translation. As the vault moves downward, the same process of bone remodeling also widens it. (Redrawn from Enlow DH, Hans MB. Essentials of Facial Growth.
Philadelphia: WB Saunders; 1996.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 09:04 PM)© 2007 Elsevier

Figure 2-30 A, Growth of the mandible, as viewed from the perspective of a stable cranial base: the chin moves downward and forward. B, Mandibular growth, as viewed from the perspective of vital staining studies, which reveal minimal changes in the body and chin area, while there is exceptional growth and remodeling of the ramus, moving it posteriorly. The correct concept of mandibular growth is that the mandible is translated downward and forward
and grows upward and backward in response to this translation, maintaining its contact with the skull.
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 09:04 PM)© 2007 Elsevier

Figure 2-31 As the mandible grows in length, the ramus is extensively remodeled, so much so that bone at the tip of the condylar process at an early age can be found at the anterior surface of the ramus some years later. Given the extent of surface remodeling changes, it is an obvious error to emphasize endochondral bone formation at the condyle as the major mechanism for growth of the mandible. (Redrawn from Enlow DH, Hans MB. Essentials of
Facial Growth. Philadelphia: WB Saunders; 1996.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 09:04 PM)© 2007 Elsevier

Figure 3-5 Scanning electron micrographs of mouse embryos (which are very similar to human embryos at this stage of development), showing the stages in facial development. A, Early formation of the face about 24 days after conception in the human. B, At a stage equivalent to about 31 days in the human, the medial and lateral nasal processes can be recognized alongside the nasal pit. C, Fusion of the median nasal, lateral nasal, and maxillary
processes forms the upper lip, while fusion between the maxillary and mandibular processes establishes the width of the mouth opening. This stage is reached at about 36 days in the human. (Courtesy Dr. K. Sulik.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 08:04 PM)© 2007 Elsevier

Figure 3-6 Schematic representations of fusion of the facial processes. A, Diagrammatic representation of structures at 31 days, when fusion is just beginning. B, Relationships at 35 days, when the fusion process is well-advanced. C, Schematic representation of the contribution of the embryonic facial processes to the structures of the adult face. The medial nasal process contributes the central part of the nose and the philtrum of the lip. The lateral nasal
process forms the outer parts of the nose, and the maxillary process forms the bulk of the upper lip and the cheeks. (B, Redrawn from Ten Cate AR. Oral Histology, ed 3. St Louis: Mosby; 1989; C, redrawn from Sulik KK, Johnston MC. Scan Elect Microsc 1:309-322, 1982.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 6 January 2008 08:04 PM)© 2007 Elsevier

Figure 4-7 Diagrammatic representation of a major mechanism for growth of the maxilla: Structures of the nasomaxillary complex are displaced forward as the cranial base lengthens and the anterior lobes of the brain grow in size. (Redrawn from Enlow DH, Hans MG. Essentials of Facial Growth. Philadelphia: WB Saunders; 1996.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-8 As the maxilla is translated downward and forward, bone is added at the sutures and in the tuberosity area posteriorly, but at the same time, surface remodeling removes bone from the anterior surfaces (except for a small area at the anterior nasal spine). For this reason, the amount of forward movement of anterior surfaces is less than the amount of displacement. In the roof of the mouth, however, surface remodeling adds bone, while bone is
resorbed from the floor of the nose. The total downward movement of the palatal vault, therefore, is greater than the amount of displacement. (Redrawn from Enlow DH, Hans MG. Essentials of Facial Growth. Philadelphia: WB Saunders; 1996.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-10 Average changes in mandibular canine and molar widths in both sexes during growth. Molar widths are shown in blue, canine widths in green. (From Moyers RE, et al. Standards of Human Occlusal Development. Ann Arbor, Mich: University of Michigan Center for Human Growth and Development; 1976.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 10 January 2008 10:01 PM)© 2007 Elsevier

Figure 4-11 Mean growth tracks of anterior and posterior maxillary implants relative to the cranial base and its perpendicular, in a group of Danish girls. The two tracks are shown with their origins superimposed to facilitate comparison. Note that the posterior implant moves down and forward more than the anterior one, with growth continuing into the late teens at a slow rate. (Courtesy Dr. B. Solow.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 10 January 2008 10:01 PM)© 2007 Elsevier

Figure 4-12 The mandible can be visualized as consisting of a core of bone surrounding the inferior alveolar neurovascular bundle and a series of functional processes: the alveolar process, serving the function of mastication; the muscular processes, serving for muscle attachments; and the condylar process, serving to articulate the bone with the rest of the skull.
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-13 Internal rotation of the mandible (i.e., rotation of the core relative to the cranial base) has two components: A, Rotation around the condyle, or matrix rotation. B, Rotations centered within the body of the mandible, or intramatrix rotation. (Redrawn from Bjork A, Skieller V. Eur J Orthod 5:1-46, 1983.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-14 Superimposition on implants for an individual with a normal pattern of growth, showing surface changes in the mandible from ages 4 to 20 years. For this patient there was -19 degrees internal rotation but only -3 degrees change in the mandibular plane angle. Note how the dramatic remodeling (external rotation) compensates for and conceals the extent of the internal rotation. (From Bjork A, Skieller V. Eur J Orthod 5:1-46, 1983.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-15 Superimposition on implants in the maxilla reveals that this patient experienced a small amount of backward internal rotation of the maxilla (i.e., down anteriorly). A small amount of forward rotation is the more usual pattern, but backward rotation occurs frequently. (From Bjork A, Skieller V. Am J Orthod 62:357, 1972.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-16 Cranial base superimposition shows the characteristic pattern of forward mandibular rotation in an individual developing in the "short face" pattern. The forward rotation flattens the mandibular plane and tends to increase overbite. (From Bjork A, Skieller V. Am J Orthod 62:344, 1972.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-17 The pattern of jaw rotation in an individual with the "long face" pattern of growth (cranial base superimposition). As the mandible rotates backward, anterior face height increases, there is a tendency toward anterior open bite, and the incisors are thrust forward relative to the mandible. (From Bjork A, Skieller V. Eur J Orthod 5:29, 1983.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-19 Superimposition on mandibular implants shows the lingual positioning of the mandibular incisors relative to the mandible that often accompanies forward rotation during growth. (From Bjork A, Skieller V. Am J Orthod 62:357, 1972.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-20 Cranial base superimposition for a patient with the short face pattern of growth. As the mandible rotates upward and forward, the vertical overlap of the teeth tends to increase, creating a deep bite malocclusion. In addition, even though both the upper and lower teeth do move forward relative to cranial base, lingual displacement of incisors relative to the maxilla and mandible increases the tendency toward crowding. (From Bjork A, Skieller V.
Am J Orthod 62:355, 1972.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier

Figure 4-21 Superimposition on the maxilla reveals uprighting of the maxillary incisors in the short face growth pattern (same patient as Figure 4-20). This decreases arch length and contributes to progressive crowding. (From Bjork A, Skieller V. Am J Orthod 62:355, 1972.)
Downloaded from: Proffit: Contemporary Orthodontics, 4th edition (on 9 January 2008 02:11 AM)© 2007 Elsevier