Embed Size (px)
DESCRIPTION
Trial RUn
Citation preview

CVR Conditions
Wiki/You tube: bronchoscopy/ABG demo/CPAP/BIPAP/AUSCULTATION/Incentive spirometry/IPPB Bird/Couch Assist/Chest Physical Therapy/Suctioning Mobility
& ICU/COPD Living/Cardiac or pulmonary rehabilitationBlackboard: Differences in Children

NORMAL VALUES - AdultsABG’s• pH 7.35-7.45• PaO2 10.7-13.3 kPa Av 11• PaCO2 4.7-6.0 kPa Av 5.1• HCO3 – 22-26 mmol/l• Base Excess -2 - +2• Sa02 > 95%
Other• Heart Rate 50-90• RR 12-15 (30+ hyper)• BP 120/80• Temp 37.2• Hb Average 12-14• Wcc 4-11• CRP < 10• Urine 30-50mls p/h
If CO2 and pH go in opposite direction – Respiratory Problem
If PaCO2 Resp ACIDOSIS If PaC02 Resp ALKALOSIS
If HC03 Metabolic ACIDOSIS If HC03 Metabolic ALKALOSIS

COPD• Bronchi and Alveoli Afffected• Chronic inflammation - chronic bronchitis and
emphysema• Bronchioles – destruction of
elastin/decilliation/increased numbers of goblet cells - lining becomes irritated and inflamed producing excess mucus that blocks the airways.
• Alveoli – destruction of alveolar septum, reduced transfer of O2 and CO2, bullae, floppy airways prone to collapse
• Slow progressive disease• THE EFFECTS OF COPD MEAN THAT LESS
OXYGEN PASSES INTO YOUR BLOOD . less gas exchange area and reduced surface area for gas exchange/reduced compliance of lungs? Alveolar interdependence affected too

COPD• Mechanical effects• HYPERINFLATION
– Passive - Diaphragm is flat (due to increased size of lungs pushing down on it)
– Dynamic- they develop hyperinflation during the dynamic aspect of physical activity and, therefore, the problem gets worse or develops with tasks.
– Costophrenic angle reduced– So need use of accessory muscles – bent over/hunch over
to try and dome the diaphragm
• Other Effects:• Cor Pulmonale (Enlargement of R ventricle in
response to increased resistance/High BP• Stress incontinence• Constipation• Anxiety/Depression• CAUSES• Smoking is the major cause of COPD. • Other factors can be occupation, gender (males
more likely), climate and childhood respiratory conditions.
• Repeated infections

COPD – S&S• -Using accessory muscles• -Purse lip breathing (stops collapse of floppy airways)• -Barrel chest• -Ribs in at the bottom when breathing in (paradoxical
breathing)• -Chronic dirty phlegm• -Wheezing or a whistling sound when breathing• -Feeling tired / Losing weight without trying• Hypercapnia (Hich PaCo2 in advanced disease) use hypoxic
drive to trigger breathing

COPD- Complications/TreatmentTREATMENT• Quit smoking – advice on smoking cessation• Adopt a healthy lifestyle to prevent infectionsMedications-• Bronchodilators (inhaler) treat SOB • corticosteroid pills prevent and treat COPD flare ups• antibitotics treat infections that cause flare ups• flu and pneumonia vaccines• supplemental oxygen

COPD- Physio• PHYSIOTHERAPY• -Pulmonary rehabilitation therapy• Postural/gravity assisted position• -Exercise is very important to help stay
fitter for longer and improve breathlessness• -Diaphragmatic breathing• -Active cycle of breathing• -Controlled coughing to get rid of mucus
and prevent infections• -Percussion techniques• Long term O2• EXACERBATION – clear secretions and
reduce WOB. Non – invasive ventilation• BIPAP• Bear in mind what their NORMAL o2 sat is
(some use low O2 sats to trigger breathing)• MRC Dysponea scale

Primary Ciliary Dyskinesia (PCD)• Primary Sructures affected: Cilia• Pathological process: uncoordinated
ciliary beat leads to excess secretions. Inability to remove mucous
• Clinical S&S:Recurrent infections of ears/sinuses and lungs. In children- perpetual runny nose/glue ear/chest infections
• Potential Problems: Increased mucous• Radiology: N/A• Auscultation: Crackles due to excess
mucous?• Predisposing Factors/Causes: Inherited
condition
• Management: Not a progressive disorder. Antibiotics and physio needed to delay onset of bronchiectasis.
• Chest Physical Therapy to aid mucous removal• Cough Assist?????

Bronchiectasis• Primary Sructures affected: chronic
irreversible distortion/dilation of bronchi• Pathological process: Chronic
inflammation damages elastic/muscular components of airways. Warm environment of lungs + excess mucus-infection-inflammation obstruction viscous circle. Cilia are damaged. Progressive destruction occurs. Advanced disease= pulmonary heart disease
• Clinical S&S: Large quantities sputum. Mucosal ulceration can cause haemoptysis. Finger clubbing. Dyspnoea (SOB)
• Potential Problems: Fatigue. Loss appetite. • Radiology: ??• Auscultation: Secretions and collapsing
airways on expiration cause coarse wheezes and crackles
• Predisposing Factors/Causes: severe respiratory infection/foreign body inhalation/ CF/TB/smoke inhalation/primary ciliary dyskinesia
• Management: Antibiotics for infections. Inhaled steroids for inflammation and reduction of sputum.
• Reduces mucus clearance by 15% - patients need education in sputum clearance.
• Postural drainage in severe cases• Hydration.ACB.Exercise Programme – lifelong
programme required!

Pulmonary Tuberculosis (TB)• Primary Sructures affected: Lungs• Pathological process: bacterial infection from
TB bacillus.• Clinical S&S: Fever/Night Sweats/Cough/Chest
wall pain/Weight Loss/Haemoptysis and SOB, fatigue
• Potential Problems: Tissue destruction and necrosis are balanced by healing and fibrosis.Affected tissue is replaced by scarring and cavities filled with cheese-like white necrotic material. During active disease, some of these cavities are joined to the air passages bronchi and this material can be coughed up. It contains living bacteria and can therefore pass on infection. Treatment with appropriate antibiotics kills bacteria and allows healing to take place. Upon cure, affected areas are eventually replaced by scar tissue.
• Radiology: • Auscultation:• Predisposing Factors/Causes: 1/3 of
population is infected with TB, which can become active if the hosts defence mechanisms are compromised due to poor living/drug dependency/HIV. Diabetes.Low Weight
• Management: Antibiotics for up to 6 months – very resilient
• Devise exercise regimes within isolations rooms• Air – filtered mask to be worn at all times!!

Asthma• Asthma is a long-term condition• Bronchioles are affected in asthma • Chronic inflammatory with airway narrowing
and mucus plugging• Pathological process:• an asthma trigger stimulates excess
immunoglobulin E (IgE) in serum. This fixes to Mast cells which then react to antigens and release bronchorestrictor substances- histamine
• the muscles around bronchioles tighten airways become narrower and the lining of the airways becomes inflamed and starts to swell.
• air flow can further be decreased by inflammation or excess mucus secretion
• PERSISTENT INFLAMMATION leads to fibrosis of airway walls and irreversibility
• Common triggers include house dust mites animal fur, pollen, tobacco smoke, exercise, cold air and chest infections.

Asthma – S& S
• Clinical S&S: :• SOB• Tightening of the chest• Wheezing which can make a whistling sound when you breathe. • Coughing• Features of acute asthma:• PaO2 ↓ RR >25 PaCO2 ↓ Pulse>110 BP↑ • DIAGNOSIS• The spirometer takes two measurements: the volume of air you can breathe out in one
second (called the forced expiratory volume in one second or FEV1) and the total amount of air you breathe out (called the forced vital capacity or FVC). This can be done by the GP.
• Predisposing Factors/Causes: A family history, Prolonged exposure to tabacco smoke as a child, Food allergy, Bronchiolitis as a child, Prem baby, Anxiety

Asthma - ManagementManagement: . Asthma can be well controlled in most people
most of the time. • Inhalers• Inhaling a drug is an effective way of taking an asthma
medicine as it goes straight to the lungs, with very little ending up elsewhere in the body. The drug used is Salbutomol – widens airways
• Steroids are also used but these can have side effects in the long term.
• PHYSIOTHERAPY MANAGEMENT• Breathing techniques can be used to help the patient to
relax and feel in control - simple gentle abdominal breathing is used.
• Exercise can help if aerobic training is used.

Asthma

Cystic Fibrosis

Cystic Fibrosis
• Primary Structures affected: • It is a chronic progressive obstructive disorder affecting
the exocrine glands. It is an inherited disease. Cystic Fibrosis affects the internal organs, especially the lungs and digestive system, by clogging them with thick sticky mucus. This makes it hard to breathe and digest food.
• Pathological process: CF is caused by a mutation in the gene for required to regulate the components of sweat, digestive juices, and mucus.

Cystic Fibrosis- S&S
• Clinical S&S: Symptoms of CF can include a troublesome cough, repeated chest infections, prolonged diarrhoea and poor weight gain. These symptoms are not unique to Cystic Fibrosis – difficult diagnosis
• CF affects the pancreas, which makes it difficult for people with CF to digest food. This can cause malnutrition, which can lead to poor growth, physical weakness and delayed puberty.

Cystic Fibrosis- Physio• Predisposing Factors/Causes: Genetic• Management:• Chest physiotherapy is important
because helps to prevent the thick, sticky lung secretions from blocking the air tubes. This helps to reduce infection and prevent lung damage.
• ACTIVE CYCLE OF BREATHING• POSITIVE EXPIRATORY PRESSURE• OSCILLATING POSITIVE EXPIRATORY
PRESSURE e.g. acapella, flutter.• Teach family how to do percussions
etc• The patient needs to do exercise to
keep the lungs from deteriorating and to improve physical strength and bullk.
• Stretching exercises and being taught correct posture can help.

Acute Renal Failure• Primary Sructures affected: rapid loss of kidney function

Acute Renal Failure

Acute Renal Failure• S&S: Puffy ankles as kidneys not removing proteins so BCOP goes up – more
fluid pushed into interstitial fluid space?? Also fluid retention causes oedema
• Potential Problems: metabolic acidosis ( Kidneys retaining acid), high potassium levels, uremia, changes in body fluid balance, and effects to other organ systems.
• Management: hinges on identification and treatment of the underlying cause. In addition to treatment of the underlying disorder, management of AKI routinely includes the avoidance of substances that are toxic to the kidneys, called nephrotoxins. These include NSAIDs such as ibuprofen, iodinated contrasts such as those used for CT scans, and others.Monitoring of renal function, by serial serum creatinine measurements and monitoring of urine output, is routinely performed. In the hospital, insertion of a urinary catheter helps monitor urine output and relieves possible bladder outlet obstruction, such as with an enlarged prostate.

Diabetes
• Primary Sructures affected:
• Pathological process:• Clinical S&S• Potential Problems• Radiology• Auscultation• Predisposing
Factors/Causes• Management

Pulmonary Fibrosis/ idiopathic pulmonary fibrosis
Primary structures effected:Lung tissuePathological progress: is caused by repeated injury to small
areas of lung. Results in inflammation of lungs causing scarring and stiffness.
Clinical signs and symptoms:Thickened lung tissues cause
decreased oxygen uptake from blood, brain and other organs don’t get enough oxygen.
SOB, clubbing of nails, shallow breathing . Aching muscles and joints, decreased exercise tolerance
Potential problems :decreased o2 to the brain, chronic dry cough.
In severe cases, symptoms can be significantly worse and may include congestive heart failure, respiratory failure, and strokes


Radiograpy:• 10% of patients with IPF have normal
chest x-rays. X-ray usually reveals shadows, mostly in the lower part of the lungs. In addition, lung size tends to appear smaller than normal.
Auscultation: may present with crackles heard late in inspiration.
Predisposing factors/Causes:No common cause known, can be a
side effect of medication, expositor to pollution, smoking, viral infections.
Management:• Allergen avoidance.• At present for IPF, there is no treatment
available which has been shown to improve the condition.
• Counselling may be required in view of the poor prognosis.
• Supportive therapy may be helpful in the form of oxygen therapy and physiotherapy if bronchiectasis is present.
• Patients should be encouraged to take regular exercise to maintain their exercise tolerance.
• Patients should be encouraged to be vaccinated against influenza and
• Lung transplant is the only option which improves long-term survival.3
• (patient.uk)

• The pulmonary fibrosis organisation suggests:
• Pulmonary rehabilitation :exercise training; breathing exercises and retraining; anxiety, stress and depression management; and nutritional counseling, to name a few.

PneumoniaPrimary Sructures affected: lung tissue
Pathological process:• infection of one or both lungs which is usually caused by bacteria, viruses, or
fungi. contracted by breathing in small droplets that contain the organisms that can cause pneumonia. Normally immune system would suppress virus. if a person is in a weakened condition from another illness, a severe pneumonia can develop.
• Alveoli fill with fluidClinical S&S: • symptoms of cold, high fever, shaking, discolored sputum production, sharp
chest pain, skin color may change due to deoxygenatingPotential Problems:• if the spongy tissue of the lungs that contain the air sacs is more involved.,
oxygenation can be impaired, along with stiffening of the lung, which results in SOB. if low immune response pneumonia may be life threatening.

• Radiology:• Auscultation: fine crackles,
sometimes pleural rub.• Predisposing Factors/Causes:
very young, very old, if immune system is weakened by any predisposing factors like long term illness
• Management: oral or intervenous fluids
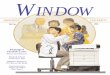
A)Normal chest, B) pneumonia

• Antiviral/antibacterial drugs• Oxygen if indicated• In acute stage physio is limited to positioning to much Va/Q and
CPAP if hypoxemia persists despite 40% oxygen.
• Modified postural drainage - this allows gravity to drain secretions from specific segments of the lungs
• IPPB Machine• Shaking and vibes - to mobilize secretions • Coughing and huffing exercises - to expectorate secretions • Administer humidification - to mobilize secretions • Breathing exercises - Localized and Diaphragmatic • IPPB administration - to increase lung volumes • Mobilization of the patient - done to increase air entry, increase
chest expansion, and to loosen secretions

PneumothoraxPrimary Sructures affected: pleural cavity between
lung and chest wallPathological process: may occur spontaneously
(primary) or in people with lung conditions (secondary). If either pleural layer is ruptured gas rushes into the pleural space either from inside the lung or from outside. the tear often occurs at the site of a tiny 'bullae' on the edge of a lung
• Clinical S&S:• The typical symptom is a sharp, stabbing pain
on one side of the chest which suddenly develops.
• The pain is usually made worse by breathing in (inspiration).
• Pt may become breathless. As a rule, the larger the pneumothorax, the more breathless .
• Pt may have other symptoms if an injury or a lung disease is the cause. For example, cough or fever.

Potential Problems: breathlessness, collapsed lung
Radiology:Auscultation: decreased or absent
breath soundsPredisposing Factors/Causes: may
occur spontaneously in healthy fit people(primary) or in people with lung conditions (secondary)
Management: • small pneumothorax is left to
heal• Larger pneumothorax can be
treated with a ‘Heimlich valve’ which allows air to escape but not to re-enter.

• Chest drains may be used • Physio is based on education in chest drain management• Positioning: lying on good side often most comfortable and
best for VA/Q , lying of affected side my speed absorbition of air.
• Precautions include avoidance of positive pressure techniques.

Pleural Effusion
Primary Sructures affected:Pleural spacePathological process: excess
fluid in pleural cavity caused by disturbed osmotic or hydrostatic pressure in plasma or changes in membrane permeability.
Clinical S&S: dull percussion note, SOB, sometimes chest pain

Potential Problems: those of underlying illness, decrease lung function
Radiology: ?fluide line tracking up the pleura laterally?
Auscultation: decreassed breath sounds, bronchial breathing
Predisposing Factors/Causes: malignancy causes 25% of pleural effusion other causes are heart, kidney, or liver failure, abdominal or cardiac surgery, pneumonia or TB
Management:On large effusions, drainage of chest
wall.Smaller effusions may just left under
observation.

• Deep breathing exercises can not expand the lungs under pressure of fluid.
• People with moderate unilateral effusion may benefit from side-lying affected side upmost as both ventilation and perfusion are greater in lower lung.
• Large effusions are likely to show improved PaC2 with effusion downwards to minimize compression of unaffected lung.

Pulmonary EmbolusPrimary Sructures affected: blood vessels in the
lungPathological process: blockage of an artery in the
lungs by fat, air, a blood clot
Clinical S&S:include unexplained shortness of breath, problems breathing, chest pain, coughing, or coughing up blood. An arrhythmia (an irregular heartbeat) also may indicate PE. In some cases, the only signs and symptoms are related to deep vein thrombosis (DVT). These include swelling of the leg or along the vein in the leg, pain or tenderness in the leg,
• Potential Problems: Severe breathlessness.• Feeling faint, feeling unwell, or a collapse. This
is because a large blood clot interferes with the heart and blood circulation, causing the blood pressure to drop dramatically.
• Rarely, in extreme cases, a massive PE can cause cardiac arrest, where the heart stops pumping due to the clot. This can result in death, even if resuscitation is attempted

Radiology:?Auscultation: decrease in breath soundsPredisposing Factors/Causes: • most commonly deep vain thrombosis, blood clot breaks off and travels
to the lung.• Other causes : Fatty material from the marrow of a broken bone (if a
large, long bone is broken - such as the femur (thigh bone).• Foreign material from an impure injection. For example, with drug
misuse.• A small piece of tumour (cancer) that has broken off from a larger tumour
in the body.Management: • Anticoagulant treatment.• Oxygen given in the early stages to help with breathlessness and low
oxygen levels.Hough ( p. 114, 2001) ‘..any active physiotherapy is considered risky until
anticoagulation therapy is established.’

CCF/LVF/RVF• CCF• Both left and right
heart failure with congestions in pulmonary and systemic circulation
• Pulmonary Oedema (extravascular water in lungs) caused by back pressure from failing Left side
• LVF• Usually caused
by coronary heart disease – failing LV forces up pressure in left atrim and pulmonary vasculature = pulmonary oedema
• Pitting Oedema
• RVF• Can be caused
by LVF or Chronic pulmonary hypertension caused by hypoxic conditions (pulmonary vasculature constrict if 02 reduced)

Smoking• Primary Sructures affected:Lungs!• Pathological process: inflammation/damage to
cilia/surfactant/Alveoli /Smooth muscle hypertrophy• Increase in secretions but decreased ability of mucocilliary
escalator• Alveolar gas exchange decreased/ V/Q Matching• Fibrotic changes from ongoing inflammation• Increase in IgE and IgM – markers of increased sensitivity• Immune responses decreased – more infections• LUNG CLOSING VOLUMES INCREASED – more airway collapse
will result• Narrowing/Clogging of arteries/atherosclerosis/increase
cholesterol/stiffening arteries

Peripheral Vascular Disease
• Chain of events leading to amputation:– Obstruction/
resistance/stasis of blood – CLOT
– Pain– Skin Breakdown– Infection– Amputation
• Risk factors:• smoking- roughening means
lipids stick more easily• BP- stress on
vessels/perpetuates atherosclerosis
• Diabetes-glucose causes vessel damage/ Plasma viscosity increases/diabetic neuropathy – can’t feel - infections

Peripheral Vascular Disease
• Thrombus – occludes vessel reducing blood flow= ischaemia
• Vessel wall changes/blood flow stasis/changes in blood composition
• Buerger’s disease – vessels become inflamed/ clots form/lumen obstructed/fibrous tissue forms

Ischaemia
• Pain• Altered sensation• Loss of peripheral
pulses• Decreased muscular
strength• Necrosis• Intermittent
Claudication
• INVESTIGATIONS– Dopler– Pulses

AtherosclerosisPrimary Sructures affected: medium and large
arteriesPathological process: become clogged up by
fatty substances, such as cholesterol. These substances are called plaques or atheromas.
Clinical S&S• Atherosclerosis does not usually produce
any symptoms until your blood circulation becomes restricted, or blocked, leading to the onset of cardiovascular disease (CVD). The type of CVD and its associated symptoms will depend on where the blockage occurs.

AtherosclerosisPotential Problems: • peripheral arterial disease: where the blood supply to your legs is blocked, causing
muscle pain (intermittent caludication?)• coronary heart disease: where the main arteries that supply your heart (the
coronary arteries) become clogged up with plaques• stroke: a very serious condition where the blood supply to your brain is interrupted• heart attack: a very serious condition where the blood supply to your heart is
blocked • Angina• AneurysmPredisposing Factors/Causes:High fat diet/cholesterol/High Blood
Pressure/Smoking/Diabetes/no exercise/Alcohol/family historyManagement: Medication for BP/cholesterol. Lifestyle changes/Diet/Smoking
cessation/Alcohol

Arteriosclerosis and atherosclerosis
Arteriosclerosis and atherosclerosis are two terms that are sometimes used interchangeably. However, they are different.
Arteriosclerosis is a general term that describes any group of diseases where there is a thickening, and a loss of elasticity, of
the walls of the arteries it is degenerative
Diabetes is a major factor leading to to it arteriosclerosis

Diaphragmatic Breathing
This deep breathing is marked by expansion of the abdomen
rather than the chest when breathing. It is generally
considered a healthier and fuller way to ingest oxygen

ABGS
• Low 02 - -Hypoxemia (poor gas exchange)• Co2 – – High Hypercapnia (not breathing enough/poor gas
exchange – become acidotic)– Low Hypocapnia (breathing too fast/a lot and blowing it
off)