Embed Size (px)
Citation preview
Pediatric Cysts &TumorsPresented by : Rahaf Najjar & Shimaa Ibrahim
Supervised By: Dr. Medhat Abdallah & Dr. Omar El Meligy
Presentation outline
1. Odontogenic cysts.
2. Non odontogenic cysts.
3. Benign tumors of the oral soft tissues.
4. Malignant tumors.
5. Odontogenic tumors.
6. Non odontogenic tumors.
7. Tumors of the bone.
8. Infections.
9. Vesiculobullous lesions.
10. White lesions.
Odontogenic Cysts
1. Primordial Cyst.
2. Dentigerous Cyst.
3. Eruption Cyst or Eruption Hematoma.
4. Odontogenic Keratocyst.
1 )Primordial Cyst Origin:
• Formed by cystic degeneration of the enamel organ (primordium) before the formation of enamel or dentin.
Epidemiology:
• Uncommon.
1 )Primordial Cyst Location:
• Third molar region OR any location where a permanent tooth would have formed.
Clinical Findings:
• Asymptomatic
1 )Primordial Cyst Radiographic
Findings:• Found on routine
radiographic examination.
• well circumscribed , unilocular- or multilocular- radiolucent lesion.
1 )Primordial Cyst
Treatment:
• Surgical removal.
• Extremely large bone-destructive lesion
Cystotomy & polyethylene drain
Cystectomy ( manageable size )
1 )Primordial Cyst
Prognosis:
• If the lesion is found histologically to be an Odontogenic Keratocyst Recurrence is high.
2) Dentigerous Cyst
• Found with crown of an impacted, embedded, or unerupted tooth.
Epidemiology:
• Most common .
• 2nd to 3rd decades.
• More in Males.
2 )Dentigerous Cyst
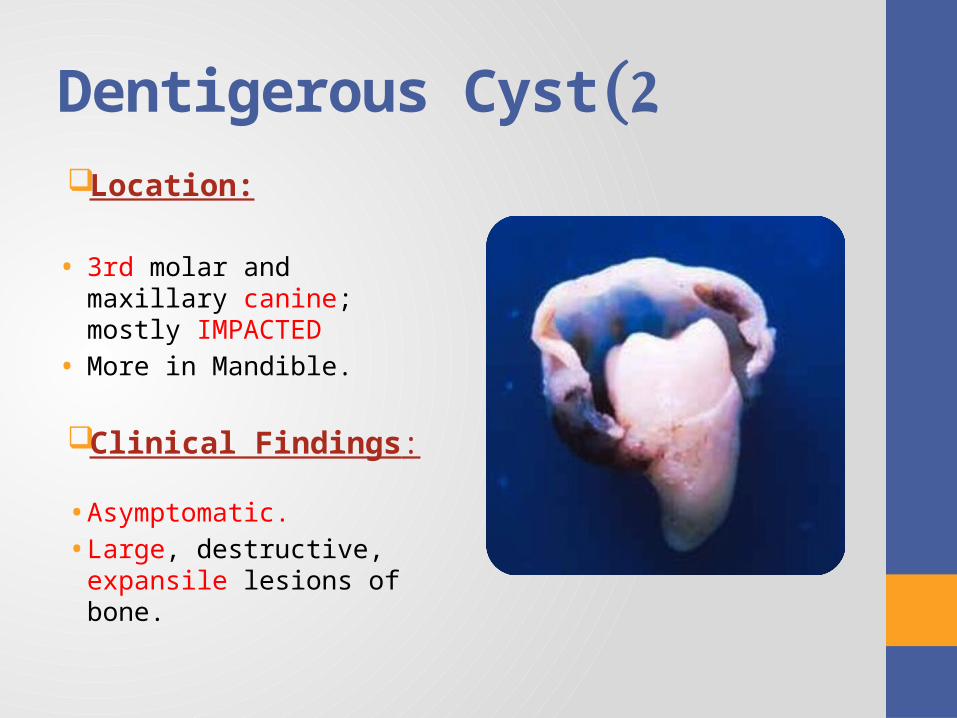
Location:
• 3rd molar and maxillary canine; mostly IMPACTED
• More in Mandible.
Clinical Findings:
• Asymptomatic.
• Large, destructive, expansile lesions of bone.
2 )Dentigerous Cyst
Radiographic Findings:• Found on routine radiographic.
• Well defined radiolucent lesion unilocular or multilocular radiolucency.
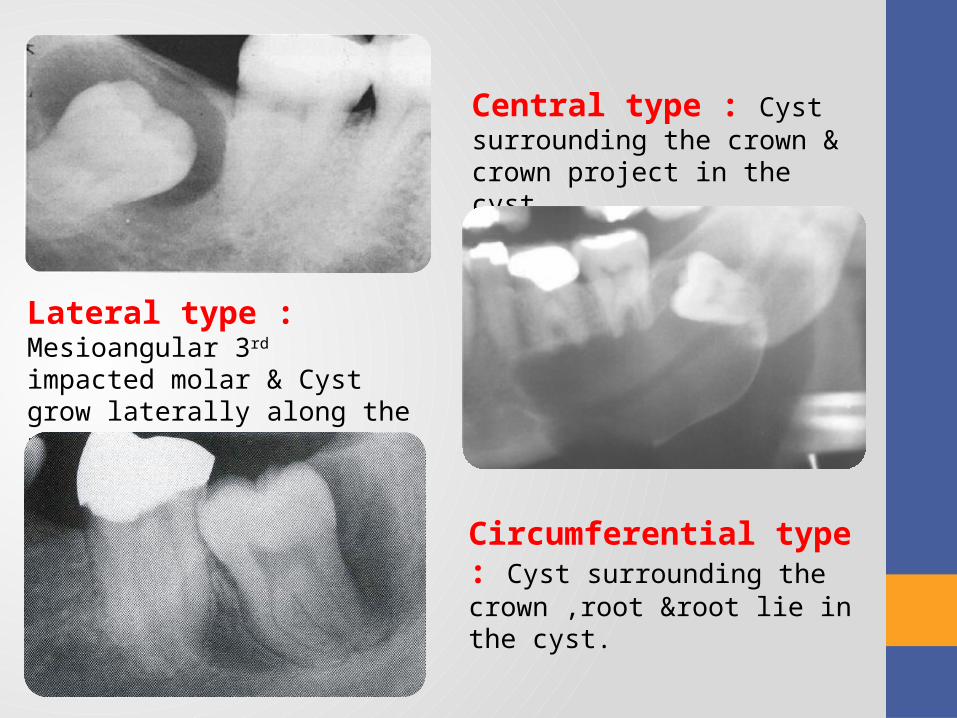
Central type : Cyst surrounding the crown & crown project in the cyst.
Lateral type : Mesioangular 3rd impacted molar & Cyst grow laterally along the root and partially the crown .
Circumferential type : Cyst surrounding the crown ,root &root lie in the cyst.
2 )Dentigerous Cyst
Treatment:
• Surgical removal.
Prognosis:Changed to: • Odontogenic keratocyst.• Ameloblastoma. • Mucoepidermoid carcinoma.
•
3) Eruption Cyst or Eruption Hematoma
Epidemiology:• Children >10 years.
Location:• Most commonly with 1st molar & maxillary incisors .
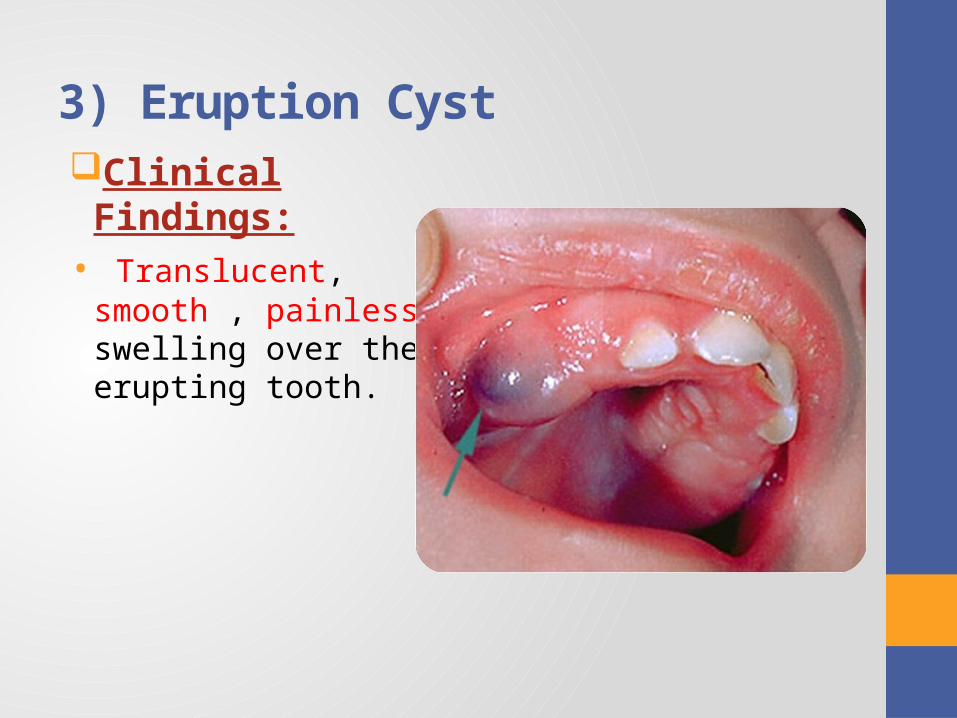
3) Eruption Cyst Clinical Findings:• Translucent, smooth ,
painless swelling over the erupting tooth.
Eruption Hematoma
•If bleeding in cystic space
Blue to blue-black
Eruption hematoma
3) Eruption Cyst or Eruption Hematoma
Treatment:• NO treatment Cyst raptures spontaneously.
4) Odontogenic Keratocyst
Epidemiology:• 2nd & 3rd decades.
• 17% > 20 years.
Location:• Mandible< Maxilla
4) Odontogenic Keratocyst
Clinical Findings:
• Half of the patients symptomatic.
• Swelling and drainage the most common clinical findings.
• May exhibit aggressive clinical behavior.
• Associated with nevoid basal cell carcinoma (Gorlin syndrome).
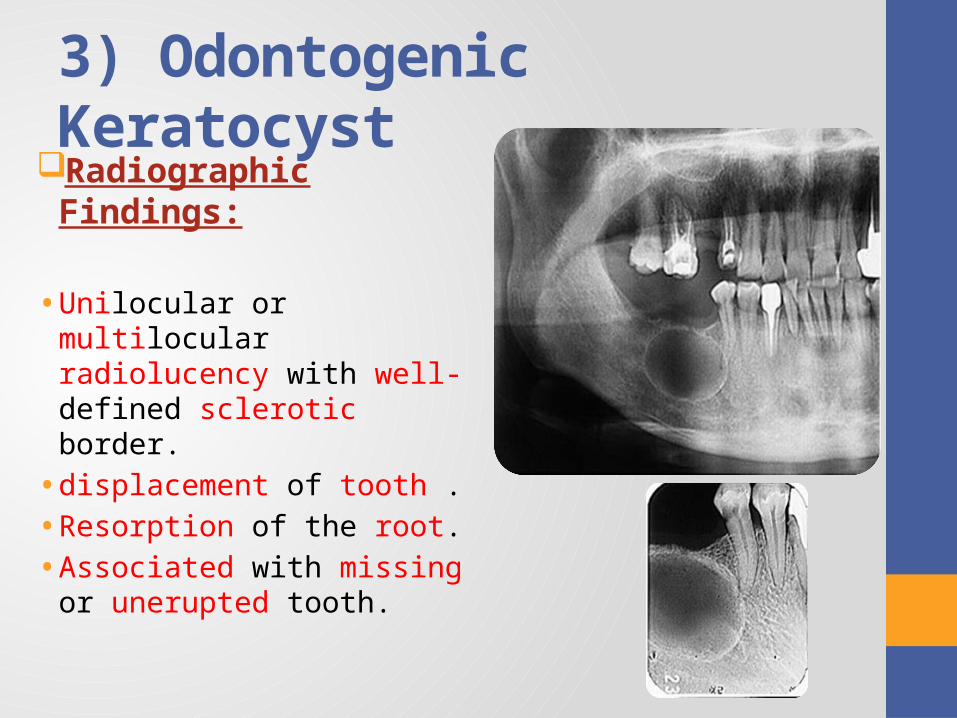
3) Odontogenic KeratocystRadiographic Findings:
• Unilocular or multilocular radiolucency with well-defined sclerotic border.
• displacement of tooth .
• Resorption of the root.
• Associated with missing or unerupted tooth.
4) Odontogenic Keratocyst
Treatment:
• Surgical excision with peripheral osseous curettage • Osteoectomy is the preferred method of management.• In large cyst; Marsupilization, followed by Enucleation.
4) Odontogenic Keratocyst
Prognosis:
• High rate of recurrence.• Potential to become an aggressive (bone-destructive
lesion).
Nevoid Basal Carcinoma )Gorlin Syndrome )
Oral – multiple odontogenic keratocysts, cleft lip or palate.
Skin – multiple nevoid basal cell carcinoma.
Skeletal – rib anomalies, vertebral deformities, polydactyly (Birth defect characterized by the presence of more than the normal number of fingers or toes)
Central nervous system – calcified falx cerebri, brain tumors.


Multiple keratocysts in a childwith Gorlin’s syndrome.
Basal cell tumors ofthe skin in the child
Non Odontogenic Cysts
1. Palatal and gingival cysts of newborns.
2. Dermoid cyst.
3. Thyroglossal duct (tract) cyst.
4. Trumatic bone cyst
5. Nasolabiale cyst.
6. Nasoplatine duct cyst.
7. Median platine cyst.
1) Palatal and gingival cysts of newborns
Epidemiology:• Common (more than half of neonates).
Location:• Midline of the palate or laterally in the hard and soft plat.
• Mucosa overlying alveolar process in the new born.
• Max. < Mand.
.
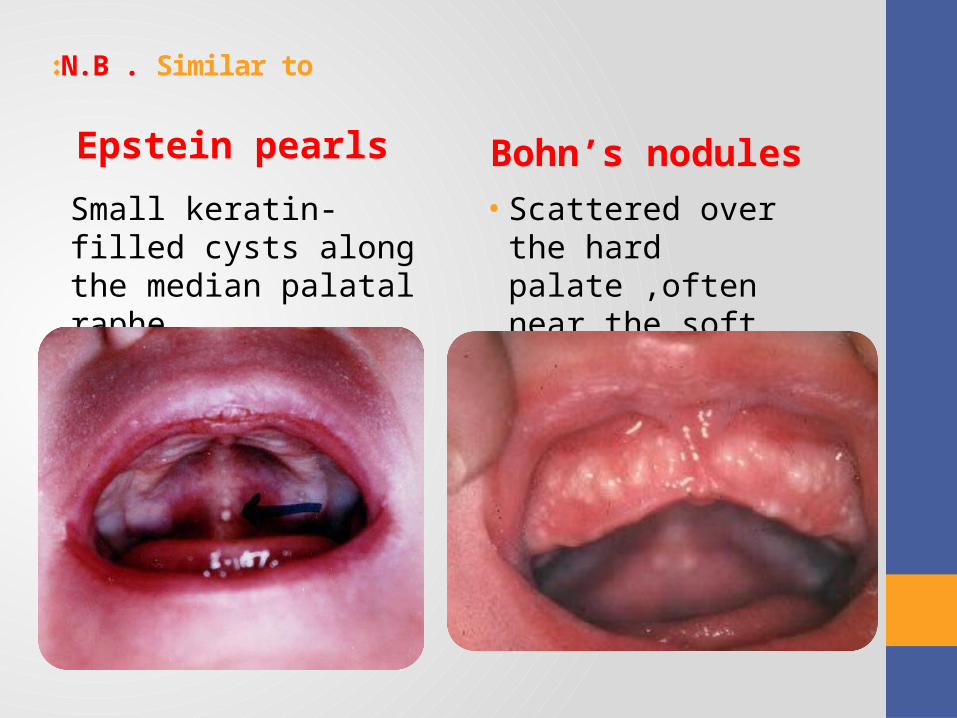
N.B . Similar to :
Epstein pearls
Small keratin-filled cysts along the median palatal raphe.
Bohn’s nodules
• Scattered over the hard palate ,often near the soft palate junction .
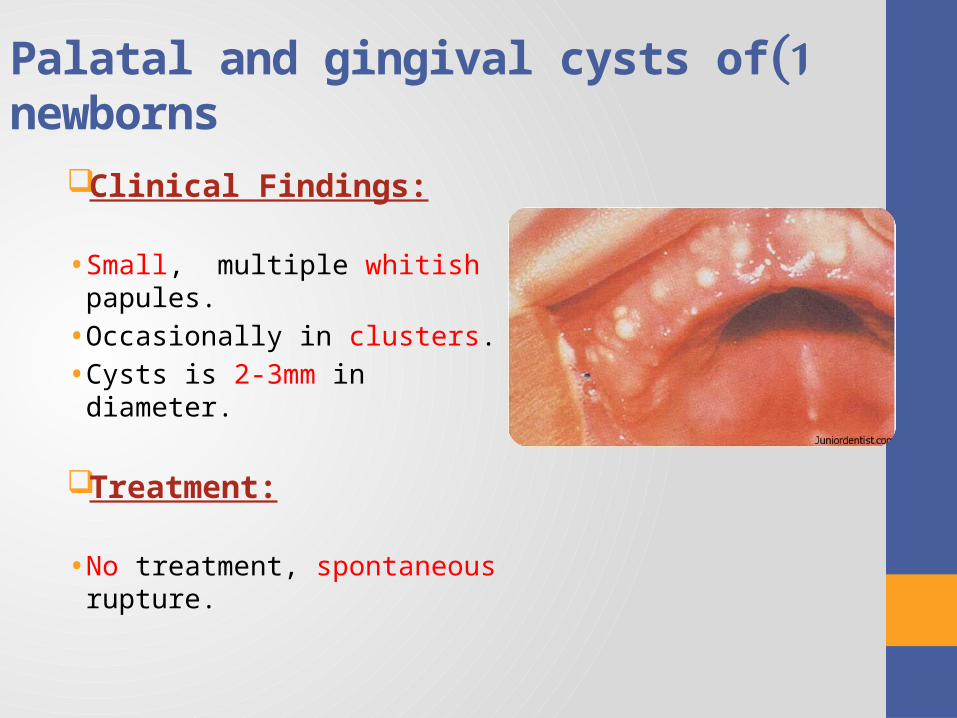
1 )Palatal and gingival cysts of newborns
Clinical Findings:
• Small, multiple whitish papules.
• Occasionally in clusters.
• Cysts is 2-3mm in diameter.
Treatment:
• No treatment, spontaneous rupture.
2) Dermoid cystEpidemiology:• Uncommon.
Location:
• Mostly occur in the midline of the floor of the mouth above or below the geniohyoid muscle.
.
2 )Dermoid cyst
Clinical Findings:
• Generally classified as Teratoma.
• Simple in structure than complex Teratomas(DON’T contain tissue from all 3 germ layer).
• Slow growing &painless.
• Rubbery texture.
2 )Dermoid cyst
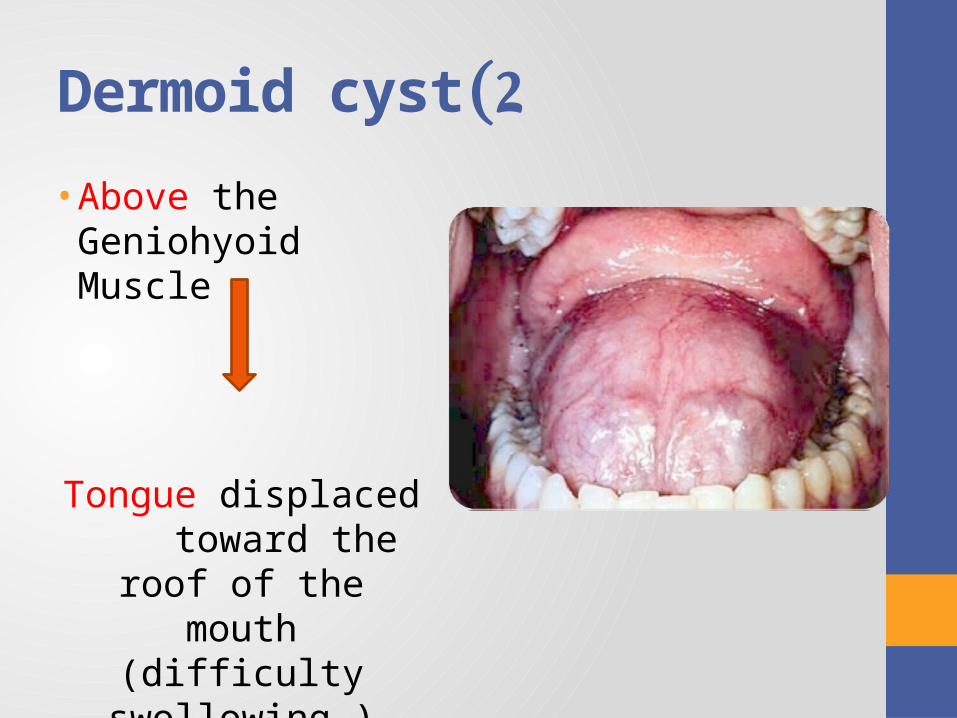
• Above the Geniohyoid Muscle
Tongue displaced toward the roof of the
mouth (difficulty swollowing )
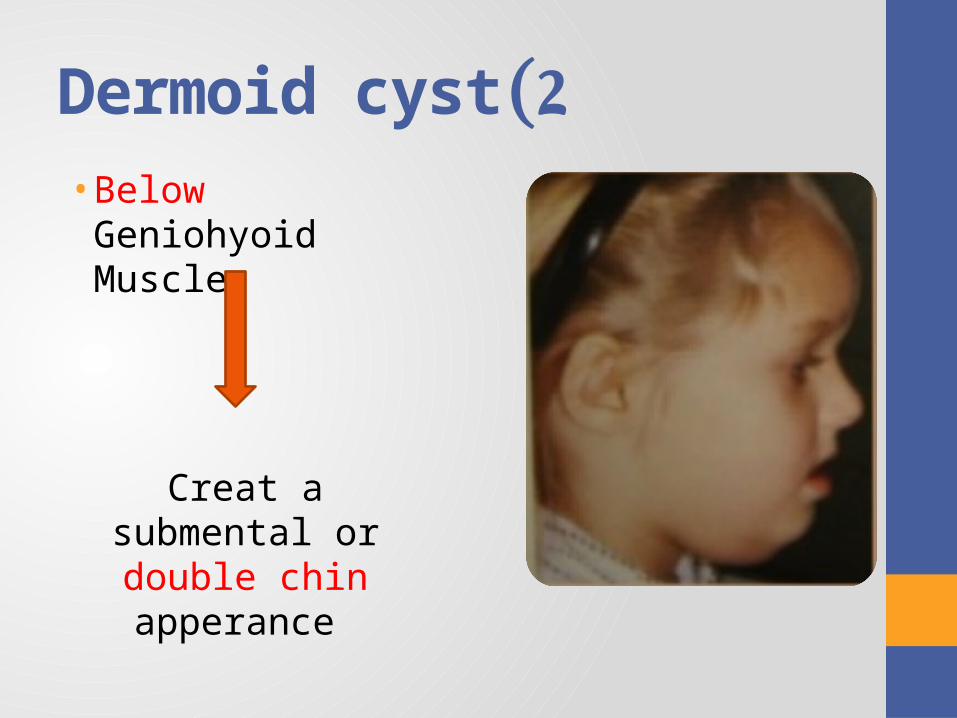
2 )Dermoid cyst• Below Geniohyoid
Muscle
Creat a submental or double chin apperance
2 )Dermoid cyst
Treatment:
• Complete surgical removal.
Prognosis:
• Recurance is uncomon.
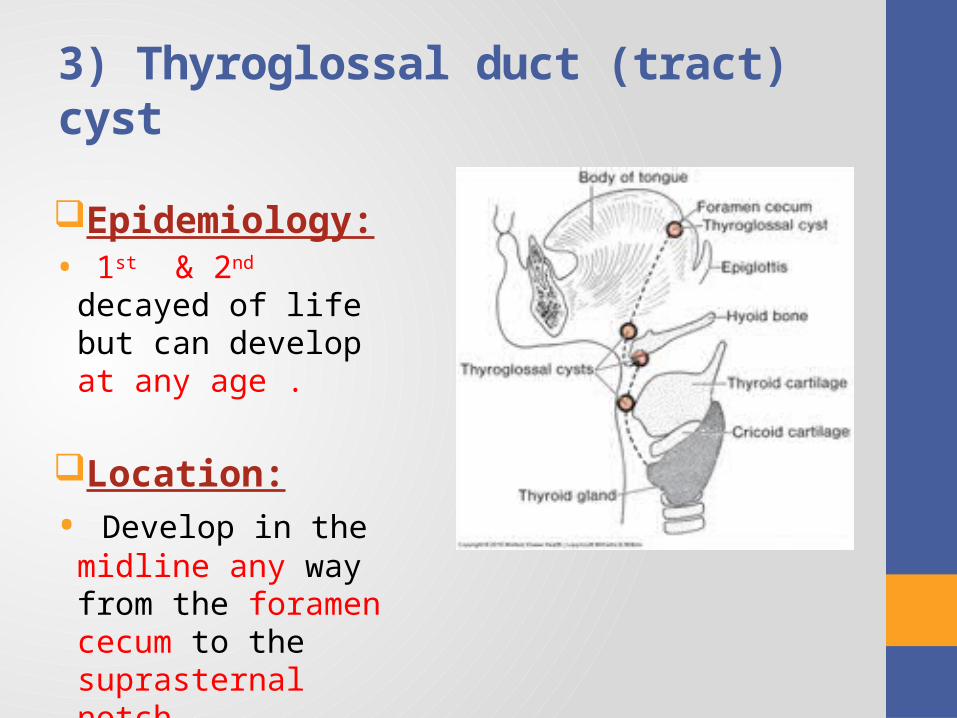
3) Thyroglossal duct )tract) cyst
Epidemiology:• 1st & 2nd decayed of life
but can develop at any age .
Location:
• Develop in the midline any way from the foramen cecum to the suprasternal notch.
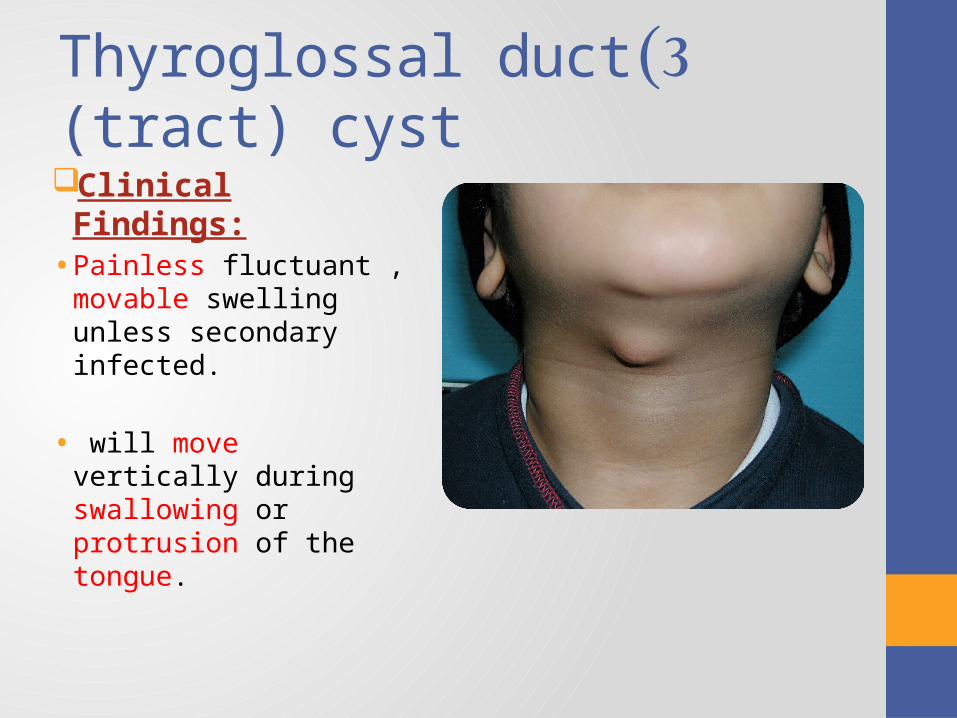
3 (Thyroglossal duct (tract) cyst
Clinical Findings:• Painless fluctuant ,
movable swelling unless secondary infected.
• will move vertically during swallowing or protrusion of the tongue.
Treatment:• Best treated by Sistrunk Procedure ( removes cyst and midline
segment of the hyoid bone).
Prognosis: • Recourence rat > 10%
3) Thyroglossal duct )tract) cyst
Epidemiology:• 2nd decayed of life.• More in Male.
Location: • Maxilla.
Clinical findings:• Accident finding.
4) Traumatic bone cyst
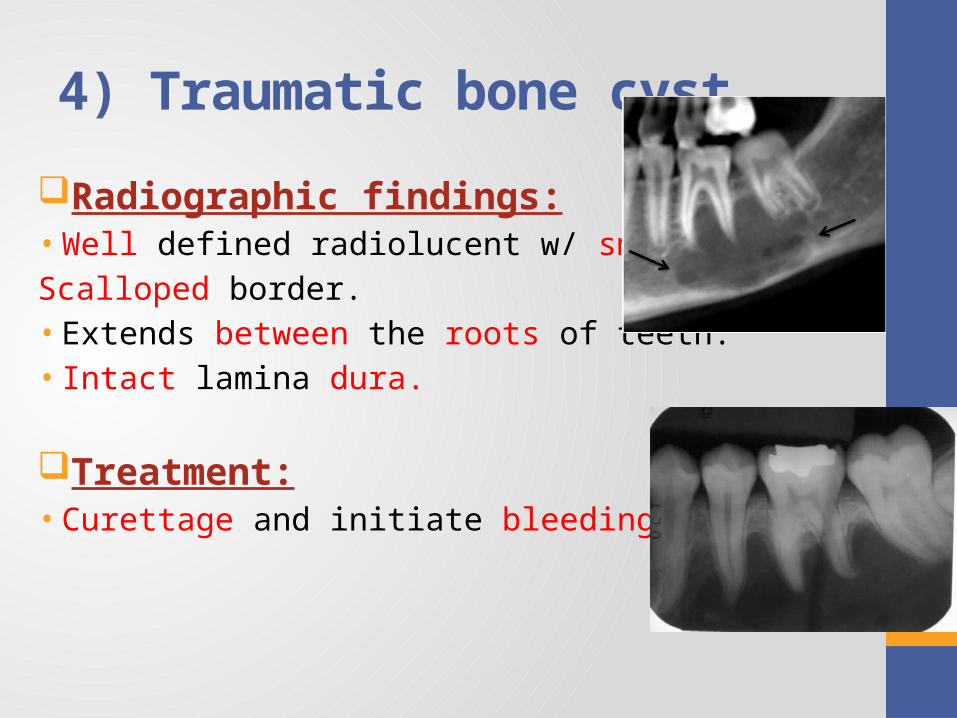
Radiographic findings:• Well defined radiolucent w/ smooth thin,
Scalloped border.• Extends between the roots of teeth.• Intact lamina dura.
Treatment: • Curettage and initiate bleeding.
4) Traumatic bone cyst
5) Nasolabial cyst
Epidemiology:• Rare.• Most commnly in adult .
Location: • Upper lip.
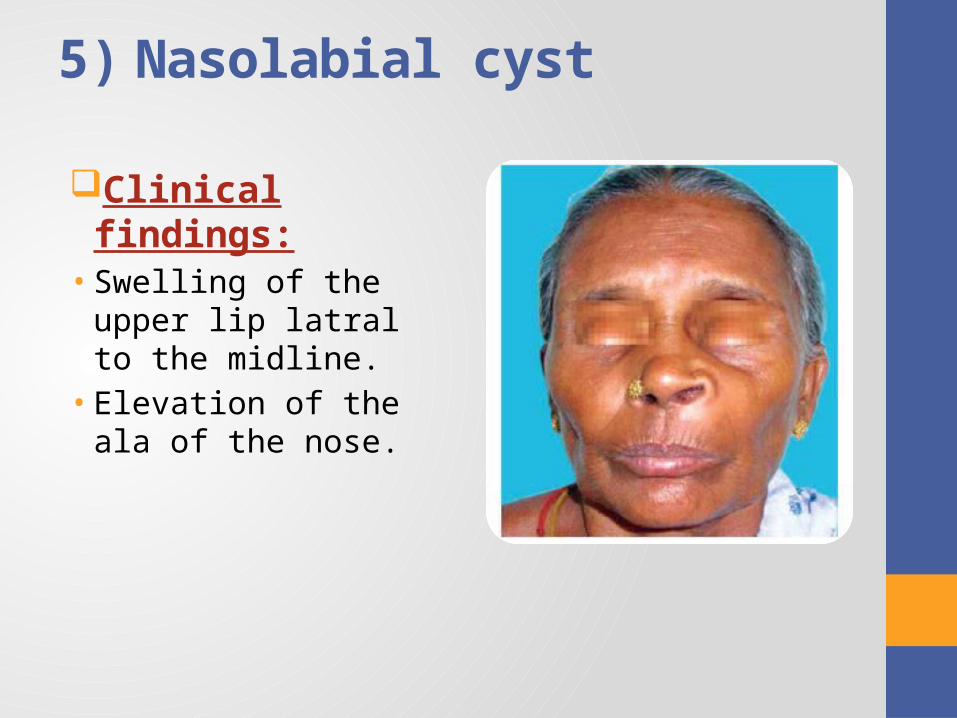
5) Nasolabial cyst
Clinical findings:• Swelling of the upper lip
latral to the midline. • Elevation of the ala of
the nose.
5) Nasolabial cyst
Treatment: • Surgical excision.
Prognosis: • Recurrence are rare.
6) Nasoplatine duct cyst.
Epidemiology:• 4th 6th decayed of life .
Location: • Palate.
6) Nasoplatine duct cyst.
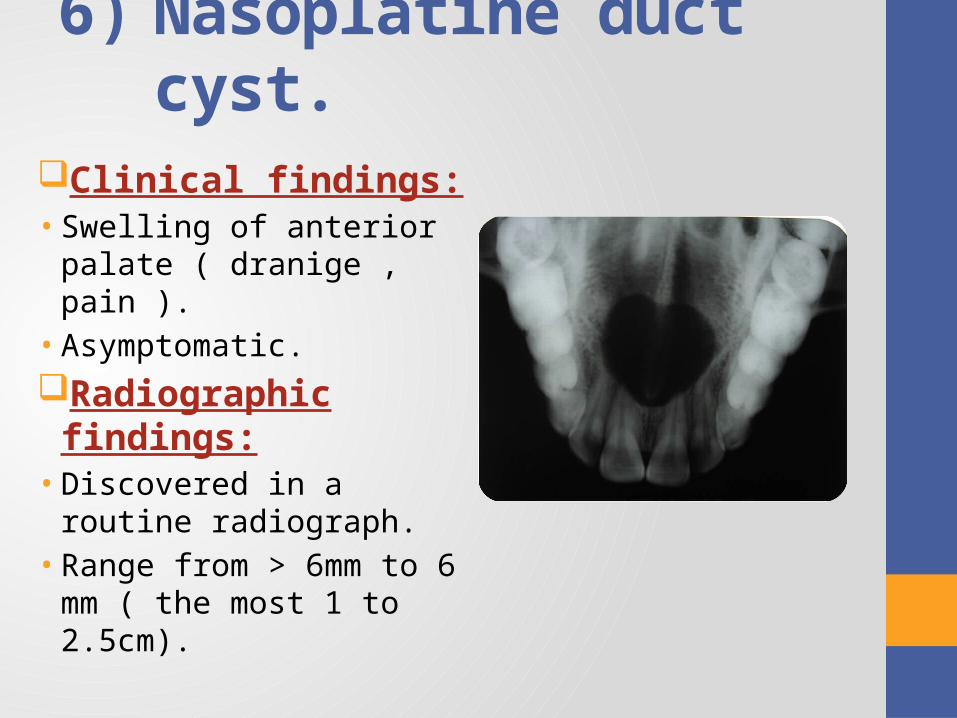
Clinical findings:• Swelling of anterior palate
( dranige , pain ).• Asymptomatic.
Radiographic findings:• Discovered in a routine
radiograph. • Range from > 6mm to 6 mm
( the most 1 to 2.5cm).
6) Nasoplatine duct cyst.
Treatment: • Surgical inculcation
Prognosis: • Recurrence is rare
7-Median platine cyst.
Epidemiology:• Adult.
Location: • Midline of the hard palate.
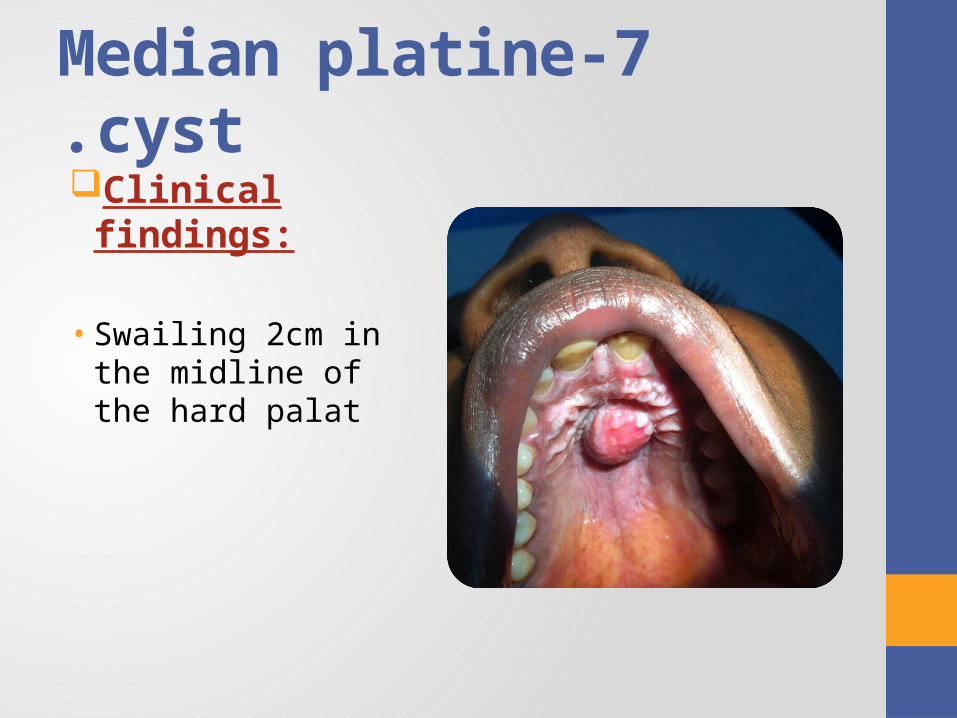
7-Median platine cyst.Clinical findings:
• Swailing 2cm in the midline of the hard palat
7-Median platine cyst.Radiographic findings:• Well circumscribed radiolucency
Treatment: • Surgical inculcation Prognosis: • Recurrence is rare
Benign Tumors Of The Oral Soft Tissue
1. Fibroma.
2. Pyogenic Granuloma & Peripheral Giant Cell Granuloma.
3. Peripheral Ossifying Fibroma & Peripheral Odontogenic Fibroma (WHO type).
4. Hemangioma.
5. Lymphangioma.
6. Mucocele.
7. Ranula.
1 )Fibroma ) focal fibrous hyperplasia)
Epidemiology:• Most common benign soft tissue.• Any age.
Location: • Sites predisposed to irritation or trauma.• Buccal mucosa, lip, tongue, gingiva, and hard palate.
1 )Fibroma ) focal fibrous hyperplasia)
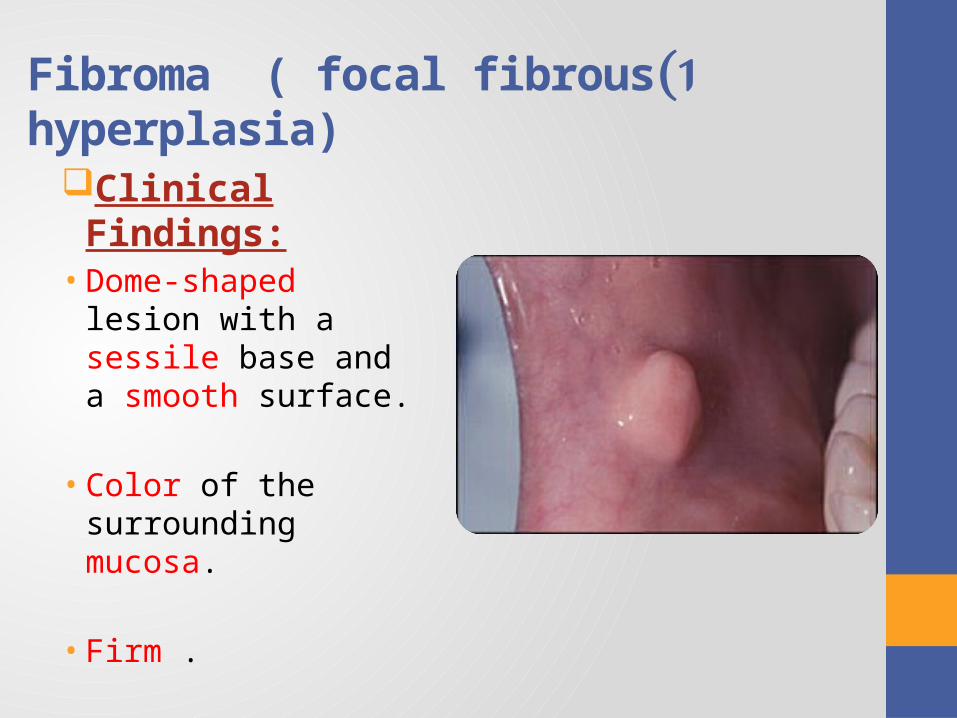
Clinical Findings:• Dome-shaped lesion with
a sessile base and a smooth surface.
• Color of the surrounding mucosa.
• Firm .
1) Fibroma ) focal fibrous hyperplasia)
Treatment:• Simple surgical excision.
Prognosis: • There is little chance to recurrence.
2) Pyogenic Granuloma, Peripheral Ossifying Fibroma, Peripheral Odontogenic Fibroma )WHO type), and Peripheral Giant Cell Granuloma
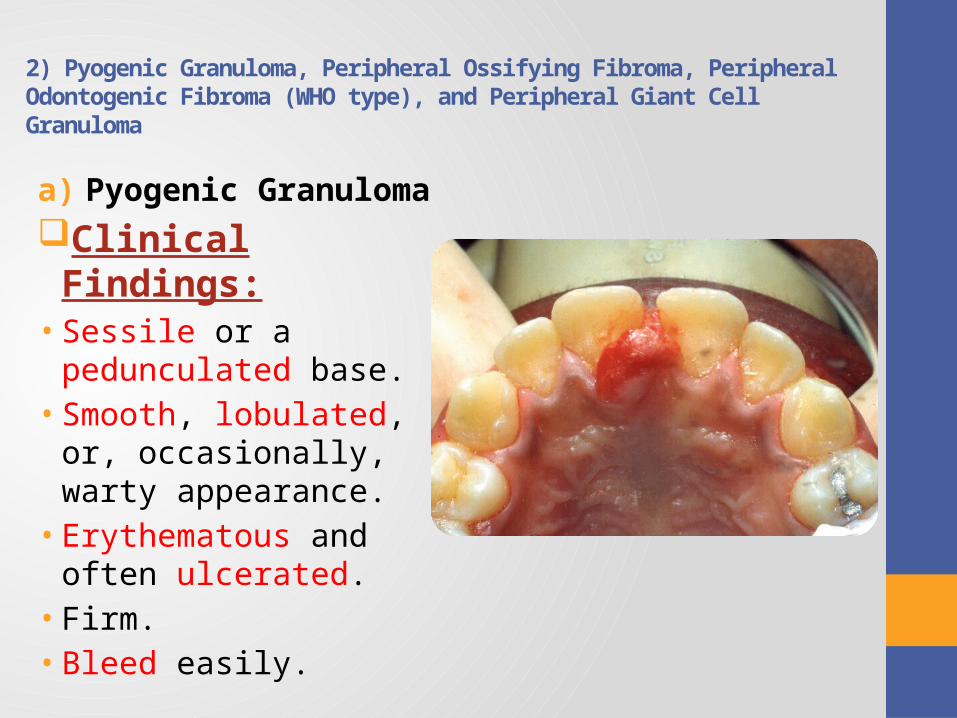
a) Pyogenic GranulomaEpidemiology:
• Common.
Location:• 70% gingiva, maxillary anterior labial gingiva.
• lips, tongue, buccal mucosa, palate, mucolabial or mucobuccal fold, and alveolar mucosa of edentulous Areas.
2) Pyogenic Granuloma, Peripheral Ossifying Fibroma, Peripheral Odontogenic Fibroma )WHO type), and Peripheral Giant Cell Granuloma
a) Pyogenic Granuloma
Clinical Findings:• Sessile or a pedunculated
base.• Smooth, lobulated, or,
occasionally, warty appearance.
• Erythematous and often ulcerated.
• Firm.• Bleed easily.
2) Pyogenic Granuloma, Peripheral Ossifying Fibroma, Peripheral Odontogenic Fibroma )WHO type), and Peripheral Giant Cell Granuloma
a) Pyogenic Granuloma
Treatment:• Surgical excision. • Remove any local irritant.
3) Peripheral Ossifying Fibroma and Peripheral Odontogenic Fibroma )WHO type)
Epidemiology:• Between 5 - 25 years of age • Peak incidence at 13 years.• Women < Men.
Location:• Gingiva.
• Maxilla= Mandible.
• Incisor- cuspid area .
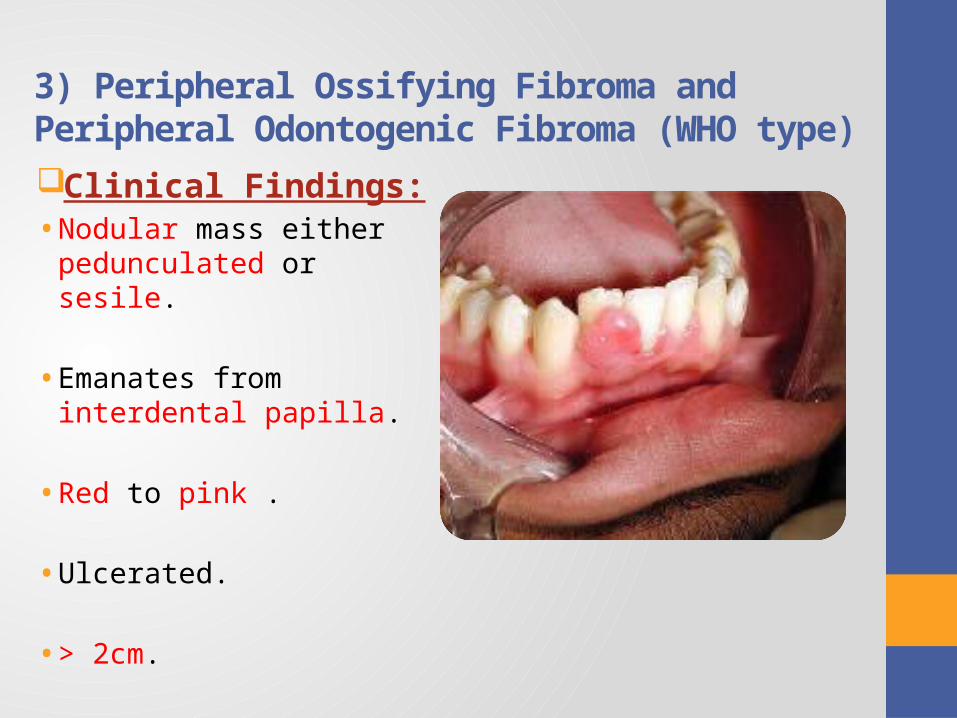
3) Peripheral Ossifying Fibroma and Peripheral Odontogenic Fibroma )WHO type)Clinical Findings:• Nodular mass either
pedunculated or sesile.
• Emanates from interdental papilla.
• Red to pink .
• Ulcerated.
• > 2cm.
3) Peripheral Ossifying Fibroma and Peripheral Odontogenic Fibroma )WHO type)
Treatment:• Surgical excision.
Prognosis :• Recurrences are common.
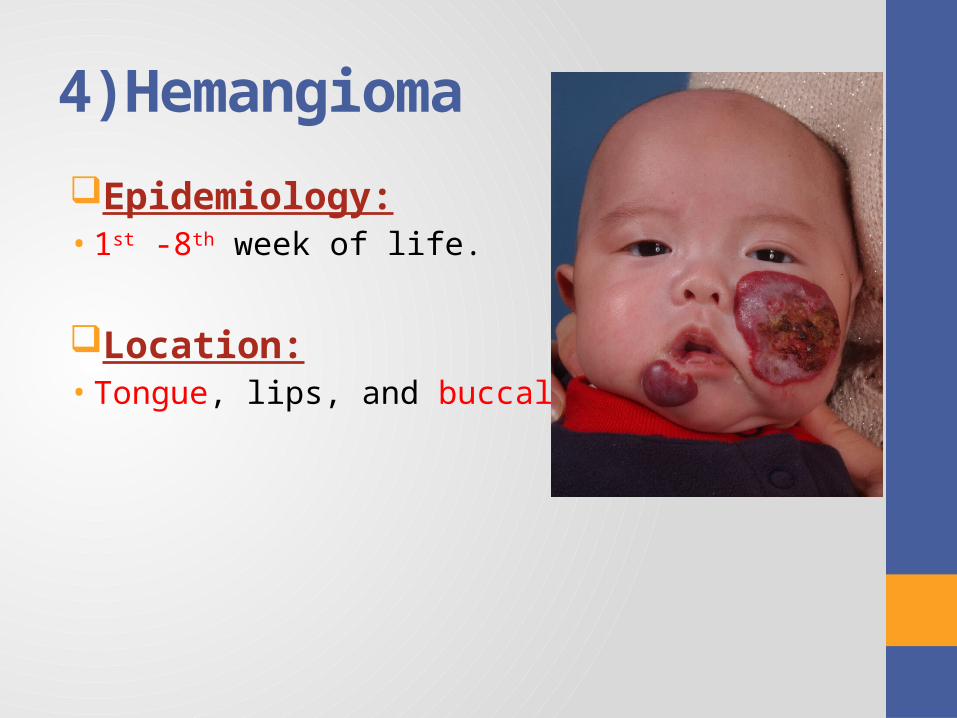
4)Hemangioma
Epidemiology: • 1st -8th week of life.
Location:• Tongue, lips, and buccal mucosa.
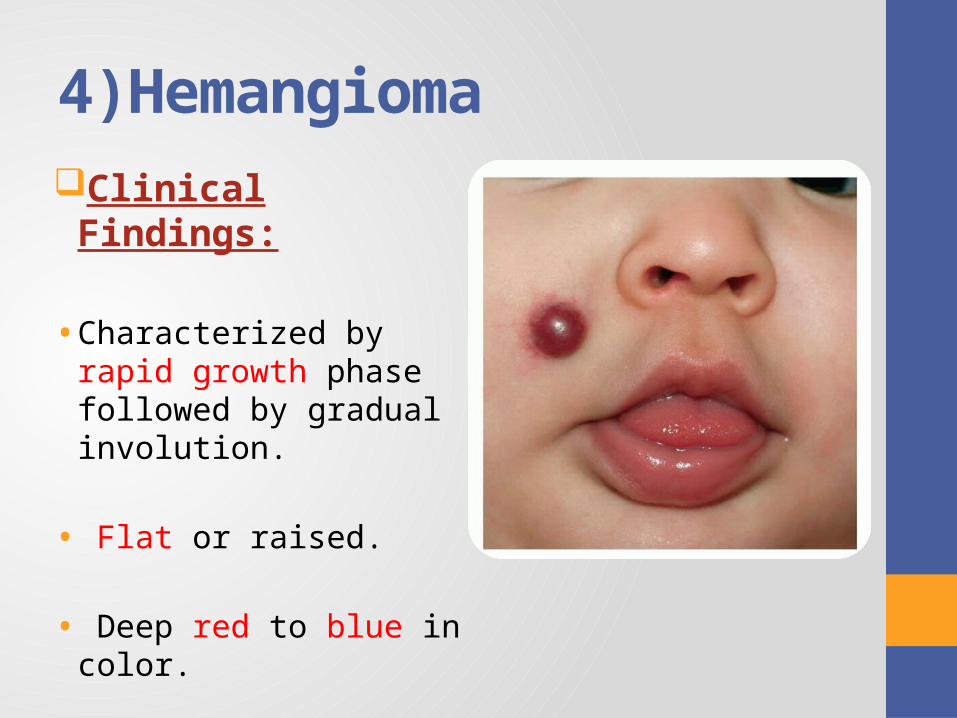
4)HemangiomaClinical Findings:
• Characterized by rapid growth phase followed by gradual involution.
• Flat or raised.
• Deep red to blue in color.
4)Hemangioma
Treatment:
• Many lesions spontaneously involute with age.
• Others require no treatment because of their small size and innocuous nature.
5) LymphangiomaEpidemiology:• Rare.• 2/3 of cases present at birth .• 90% being present by the second year of life.
Location:• Head & Neck.• Tongue, lips, and buccal mucosa.
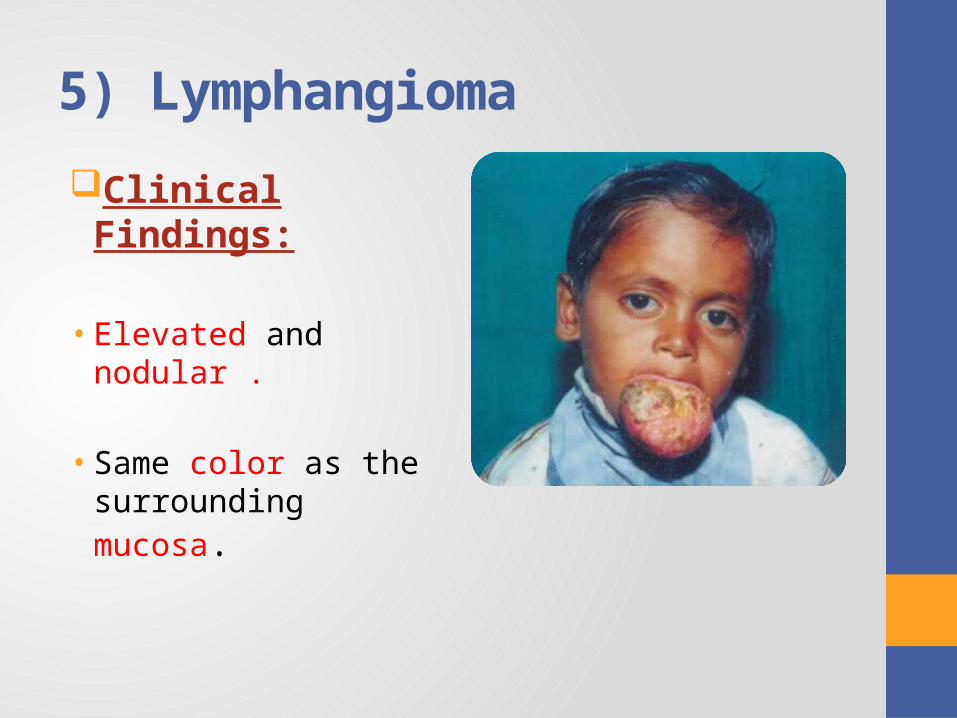
5) Lymphangioma
Clinical Findings:
• Elevated and nodular .
• Same color as the surrounding mucosa.
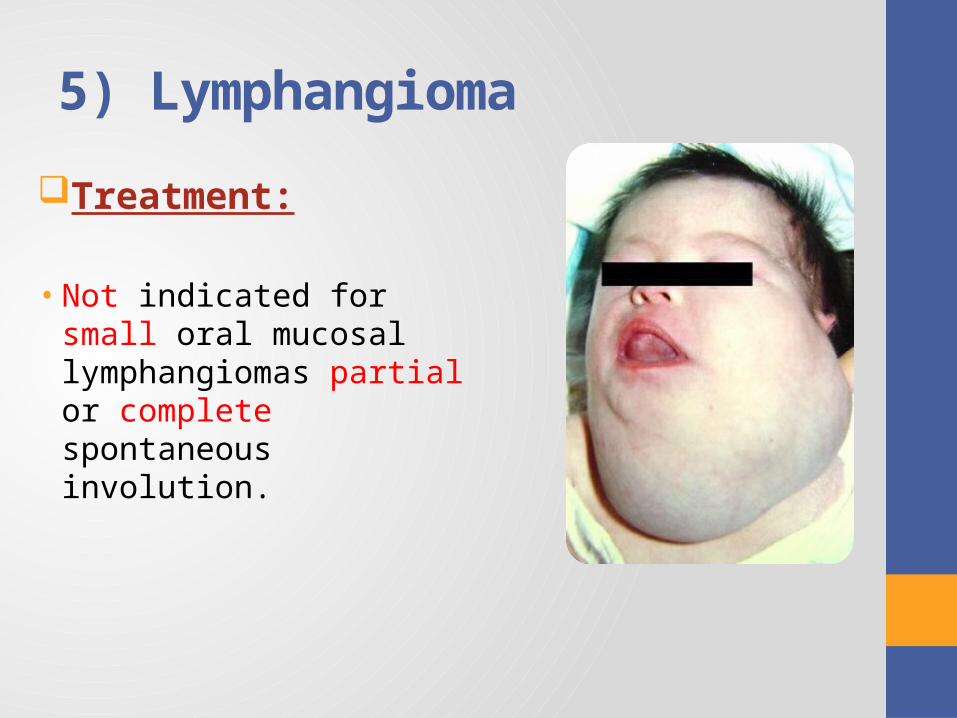
5) Lymphangioma
Treatment:
• Not indicated for small oral mucosal lymphangiomas partial or complete spontaneous involution.
6) Mucocele
Epidemiology:• Any age ( present at birth & 2nd and 3rd).
Location:• Lower lip, floor of the mouth and buccal mucosa.
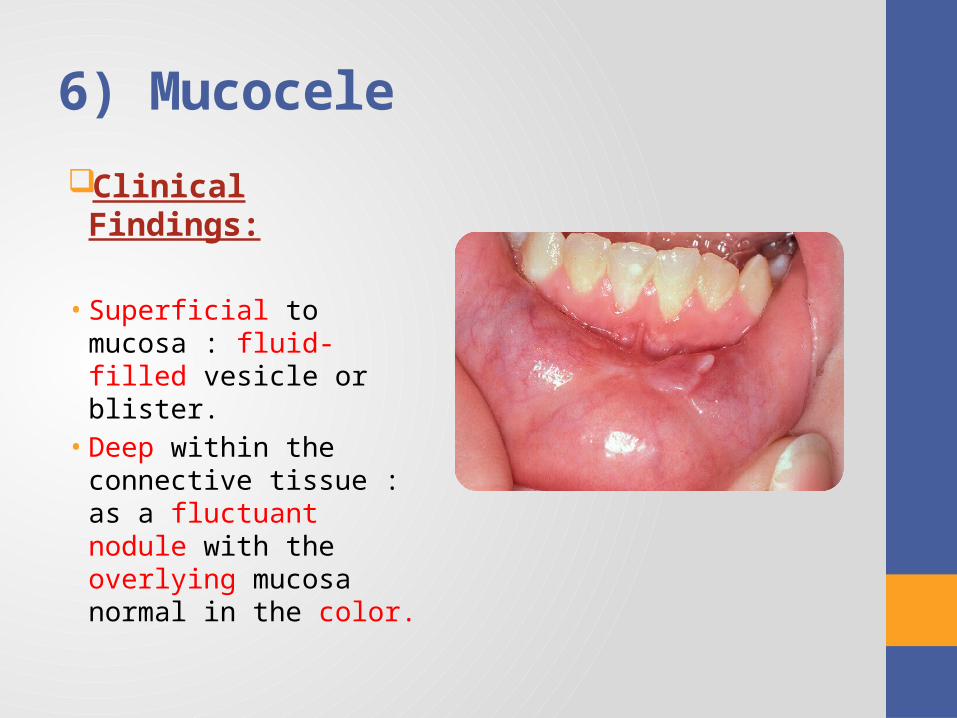
6) Mucocele
Clinical Findings:
• Superficial to mucosa : fluid-filled vesicle or blister.
• Deep within the connective tissue : as a fluctuant nodule with the overlying mucosa normal in the color.
6) Mucocele
Treatment:• Surgical excision with removal of the involved accessory
salivary gland.
7) Ranula
Epidemiology:• Any age.
Location:• Occurring to one side of the midline of the floor of the
mouth.
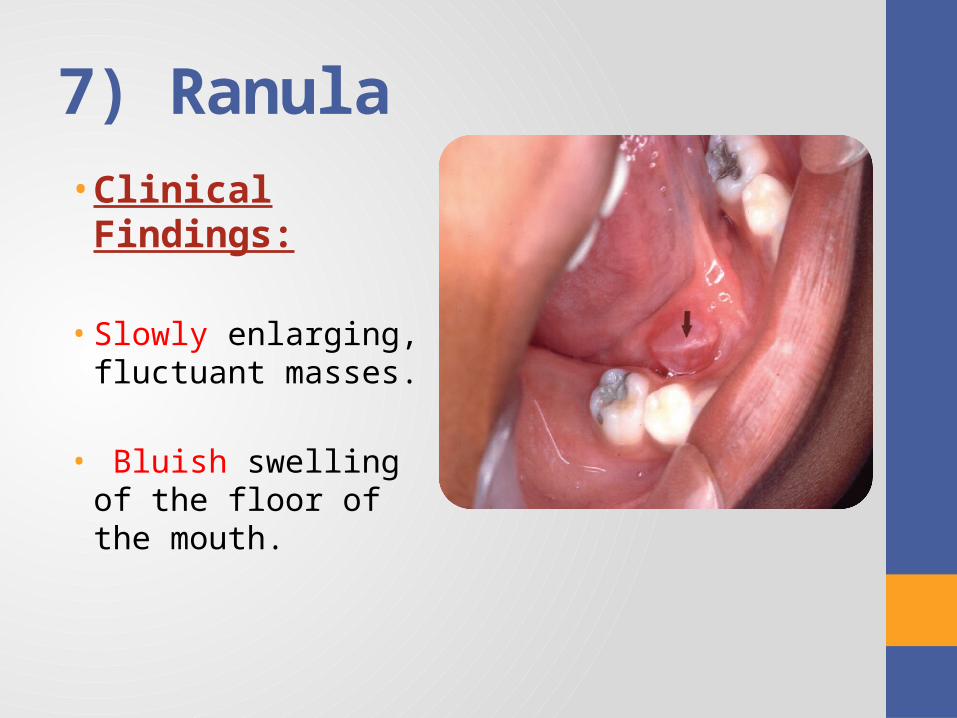
7) Ranula• Clinical Findings:
• Slowly enlarging, fluctuant masses.
• Bluish swelling of the floor of the mouth.
7) RanulaTreatment:• Marsupialization.
Prognosis:
• Occasional recurrence.• Chronic recurrence may require excision of the entire
involved gland.
NON ODONTOGENIC TUMORS
1. Melanotic neuroectodermal tumor of infancy
2. Cherubism
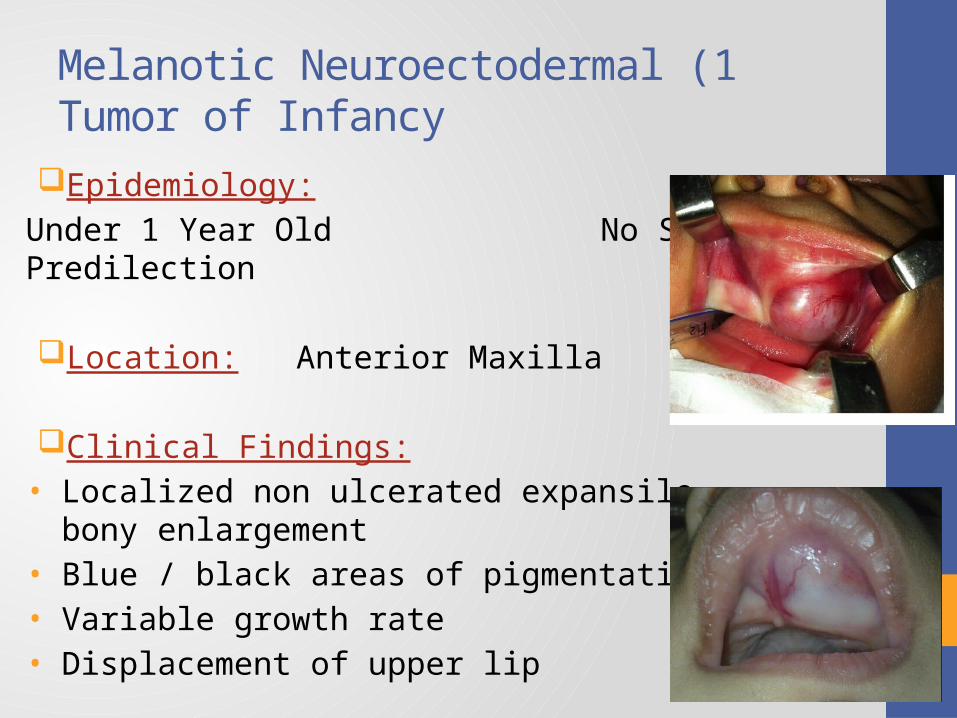
1 )Melanotic Neuroectodermal Tumor of Infancy
Epidemiology:
Under 1 Year Old No Sex Predilection
Location: Anterior Maxilla
Clinical Findings:• Localized non ulcerated expansile bony
enlargement• Blue / black areas of pigmentation• Variable growth rate• Displacement of upper lip
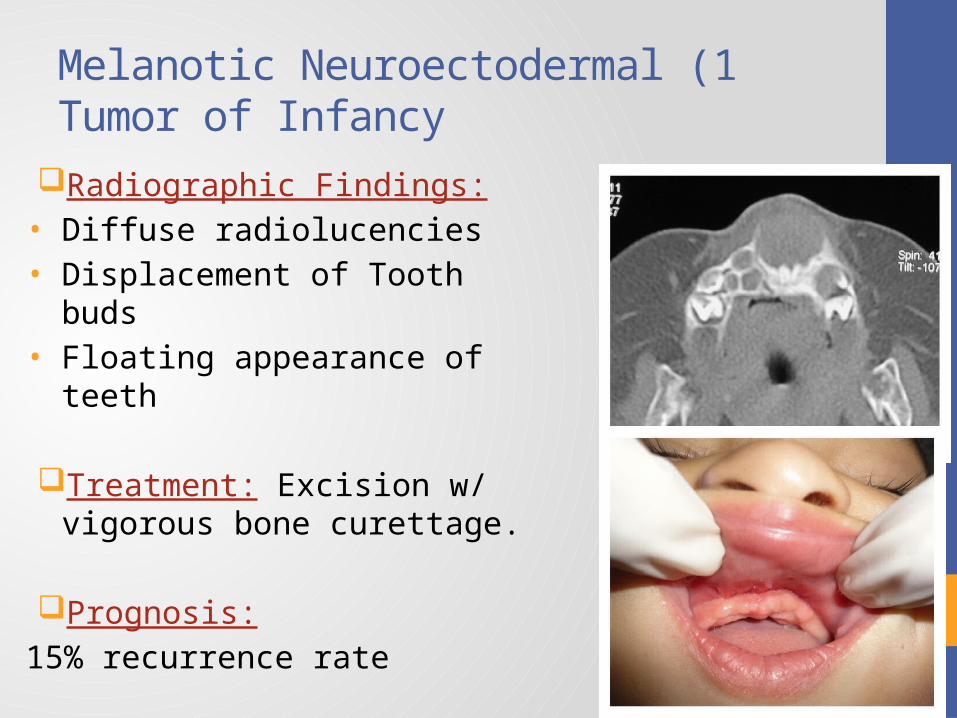
1 )Melanotic Neuroectodermal Tumor of Infancy
Radiographic Findings:• Diffuse radiolucencies• Displacement of Tooth buds• Floating appearance of teeth
Treatment: Excision w/ vigorous bone curettage.
Prognosis:
15% recurrence rate
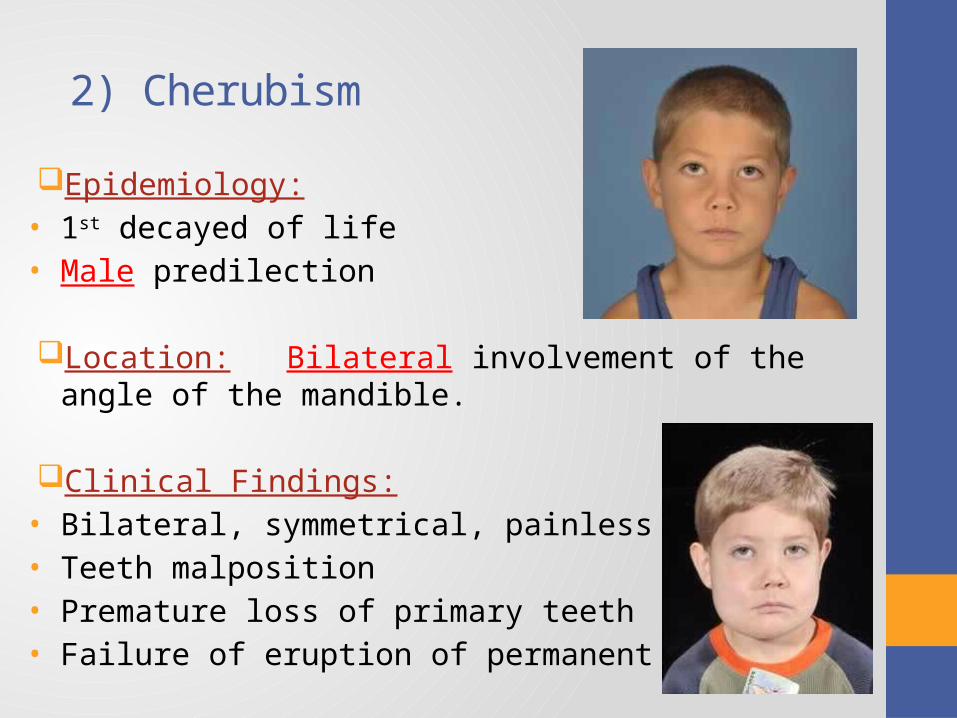
2) Cherubism
Epidemiology:• 1st decayed of life• Male predilection
Location: Bilateral involvement of the angle of the mandible.
Clinical Findings:• Bilateral, symmetrical, painless enlargement• Teeth malposition• Premature loss of primary teeth• Failure of eruption of permanent teeth
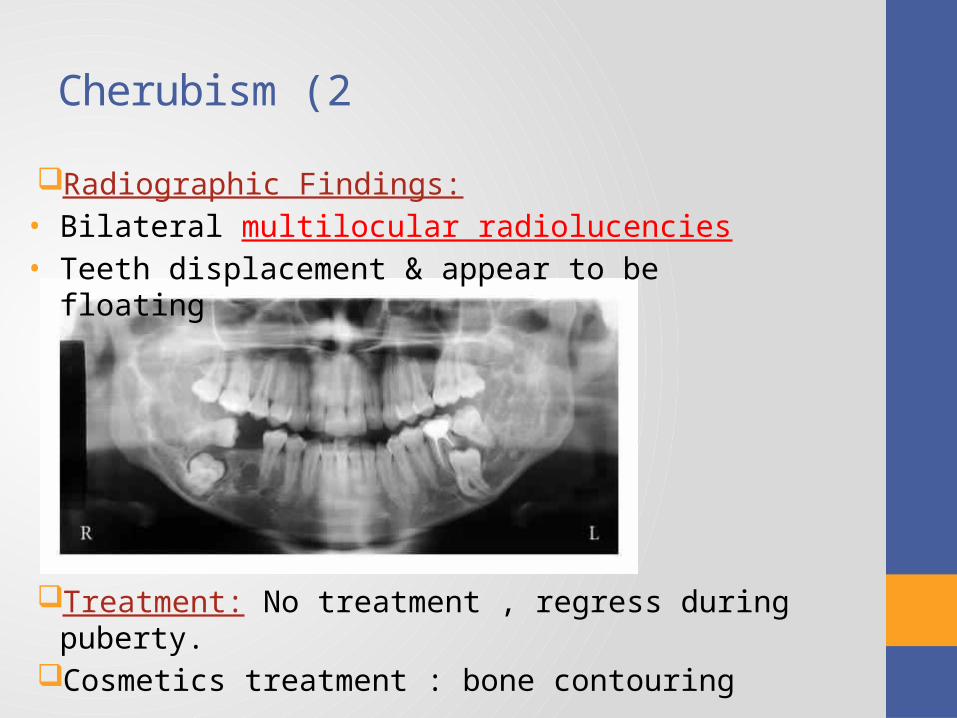
2 )Cherubism
Radiographic Findings:• Bilateral multilocular radiolucencies• Teeth displacement & appear to be floating
Treatment: No treatment , regress during puberty.Cosmetics treatment : bone contouring
ODONTOGENIC TUMORS
1. Ameloblastoma
2. Adenomatoid Odontogenic Tumor
3. Ameloblastic Fibroma
4. Ameloblastic Fibro-Odontoma
5. Odontoma
6. Myxoma
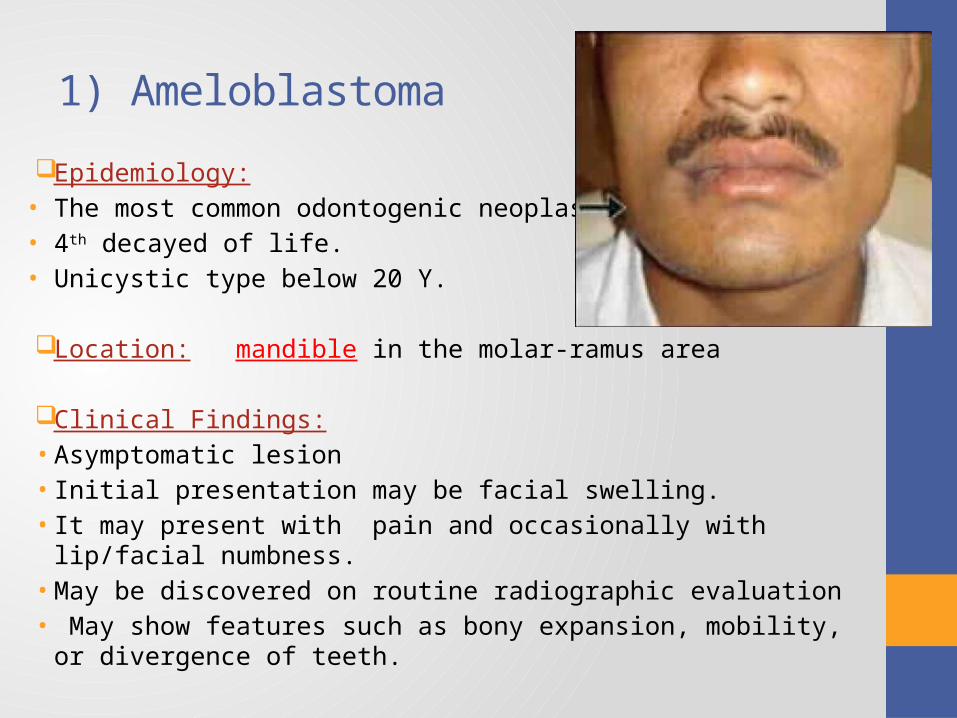
1) Ameloblastoma
Epidemiology:• The most common odontogenic neoplasm• 4th decayed of life.• Unicystic type below 20 Y.
Location: mandible in the molar-ramus area
Clinical Findings:• Asymptomatic lesion• Initial presentation may be facial swelling. • It may present with pain and occasionally with lip/facial numbness.• May be discovered on routine radiographic evaluation • May show features such as bony expansion, mobility, or divergence of
teeth.
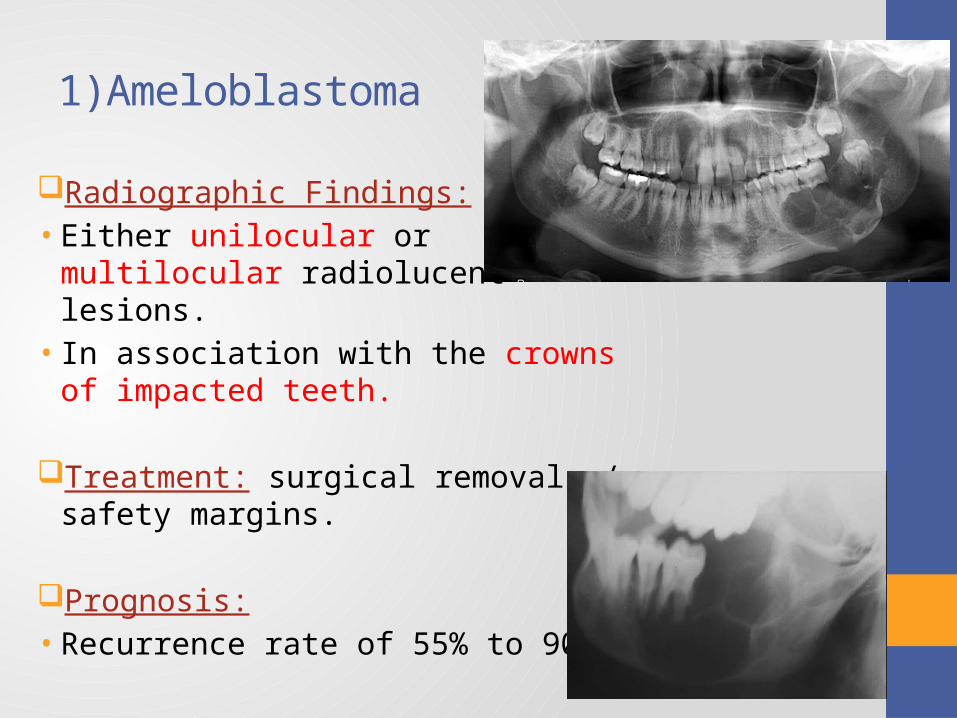
Radiographic Findings:• Either unilocular or multilocular
radiolucent lesions.• In association with the crowns of impacted
teeth.
Treatment: surgical removal w/ safety margins.
Prognosis: • Recurrence rate of 55% to 90%
1)Ameloblastoma
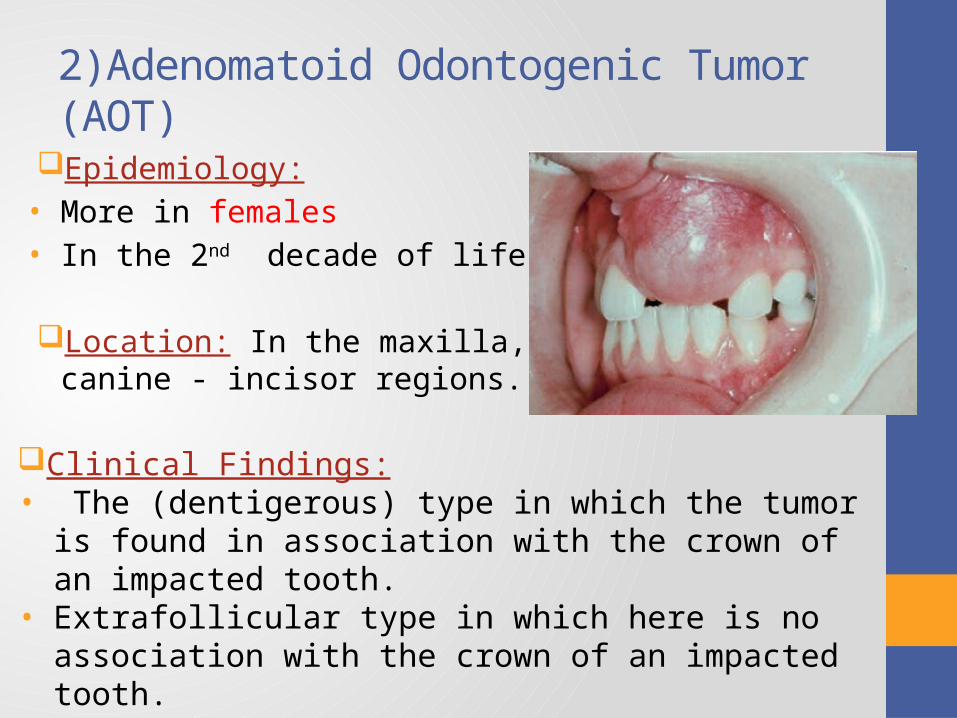
2)Adenomatoid Odontogenic Tumor (AOT)
Epidemiology:• More in females• In the 2nd decade of life.
Location: In the maxilla, in canine - incisor regions.
Clinical Findings:• The (dentigerous) type in which the tumor is found in
association with the crown of an impacted tooth.• Extrafollicular type in which here is no association with the
crown of an impacted tooth.• The peripheral or extraosseous variant.
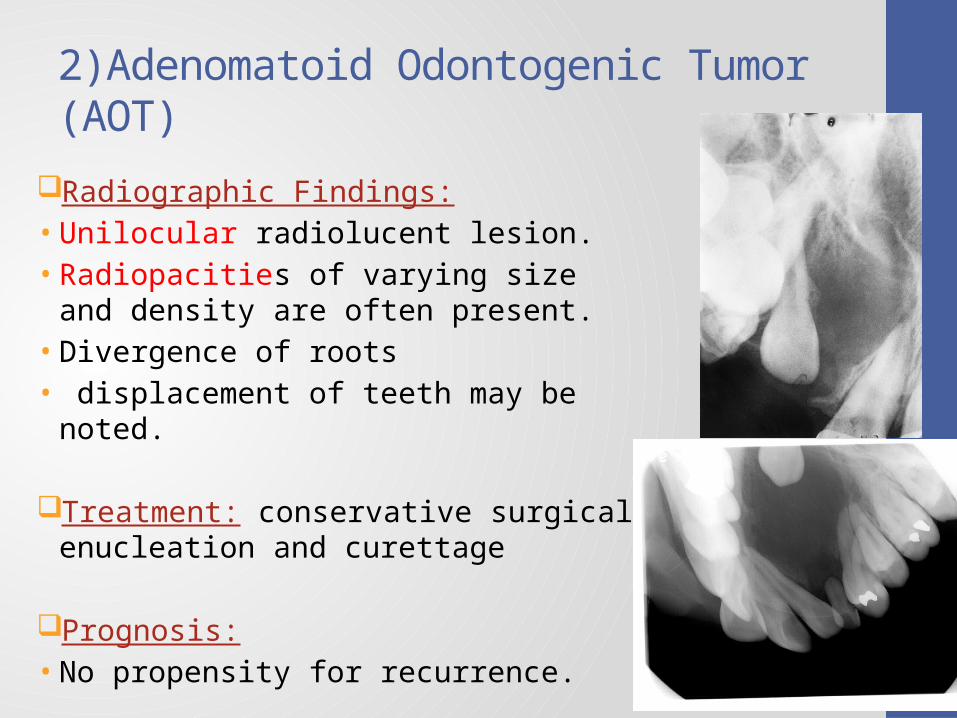
Radiographic Findings:• Unilocular radiolucent lesion.• Radiopacities of varying size and density are
often present.• Divergence of roots • displacement of teeth may be noted.
Treatment: conservative surgical enucleation and curettage
Prognosis: • No propensity for recurrence.
2)Adenomatoid Odontogenic Tumor (AOT)
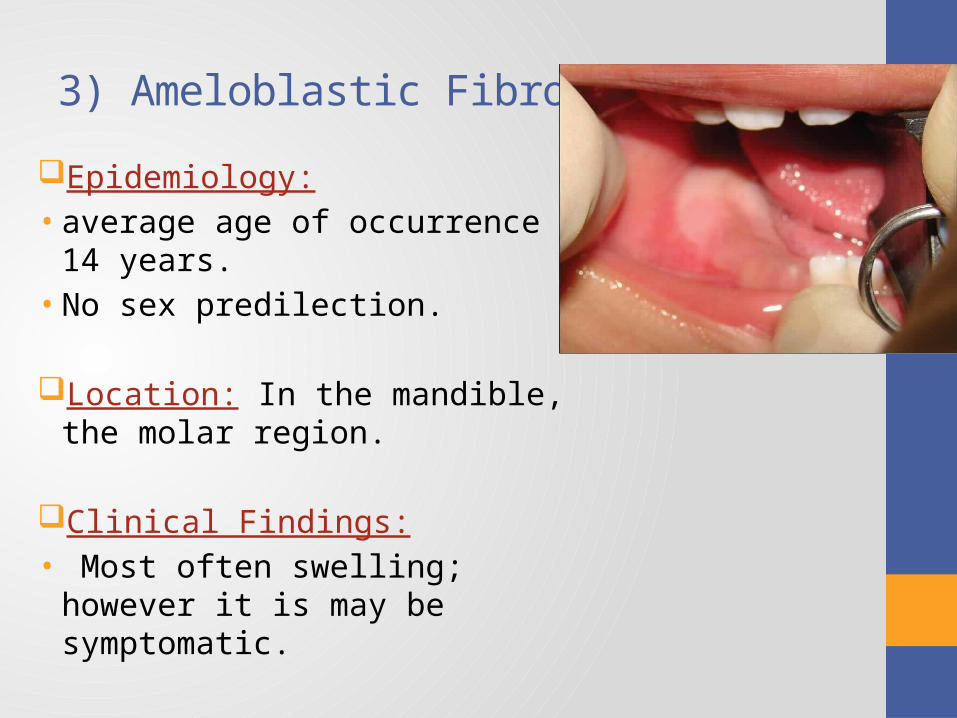
3) Ameloblastic Fibroma
Epidemiology:• average age of occurrence is 14 years.• No sex predilection.
Location: In the mandible, the molar region.
Clinical Findings:• Most often swelling; however it is may
be symptomatic.
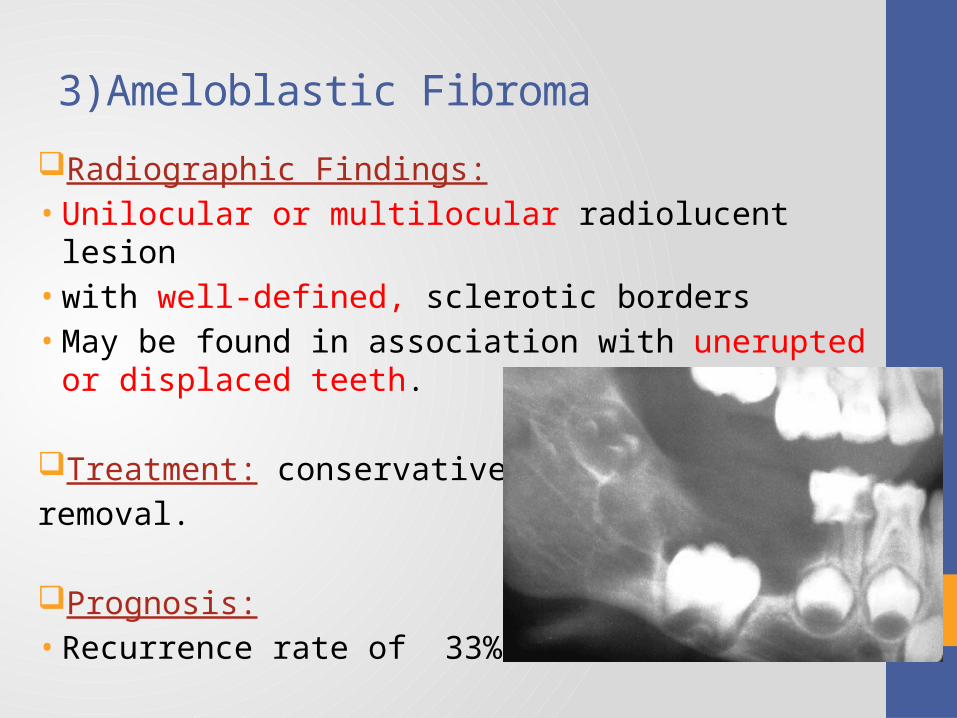
Radiographic Findings:• Unilocular or multilocular radiolucent lesion• with well-defined, sclerotic borders• May be found in association with unerupted or displaced teeth.
Treatment: conservative surgical
removal.
Prognosis: • Recurrence rate of 33%
3)Ameloblastic Fibroma
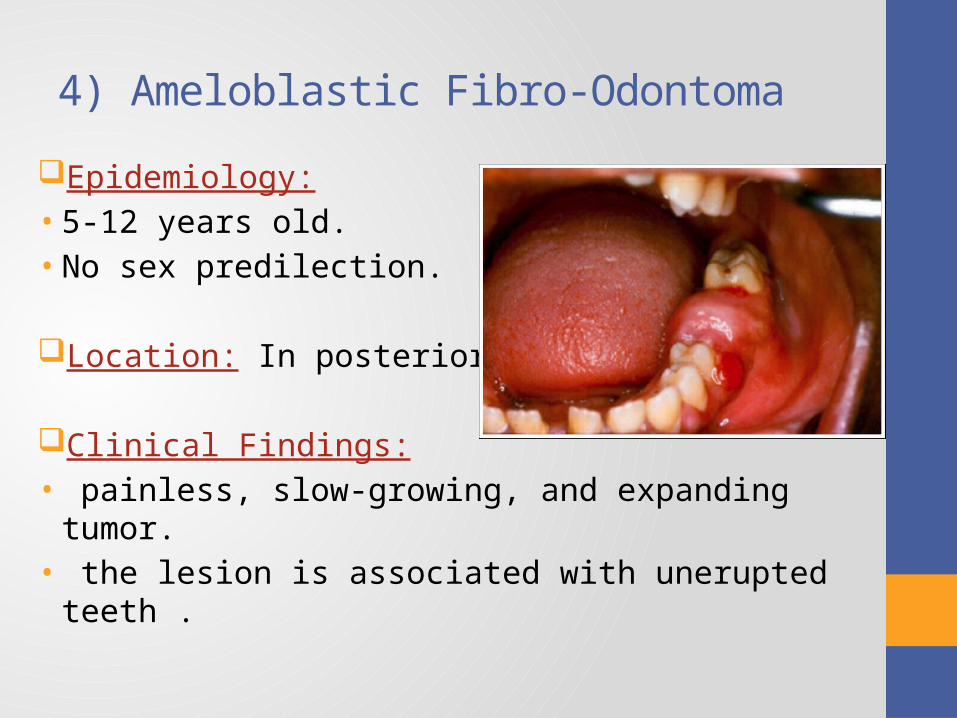
4) Ameloblastic Fibro-Odontoma
Epidemiology:• 5-12 years old.• No sex predilection.
Location: In posterior mandible.
Clinical Findings:• painless, slow-growing, and expanding tumor.• the lesion is associated with unerupted teeth .
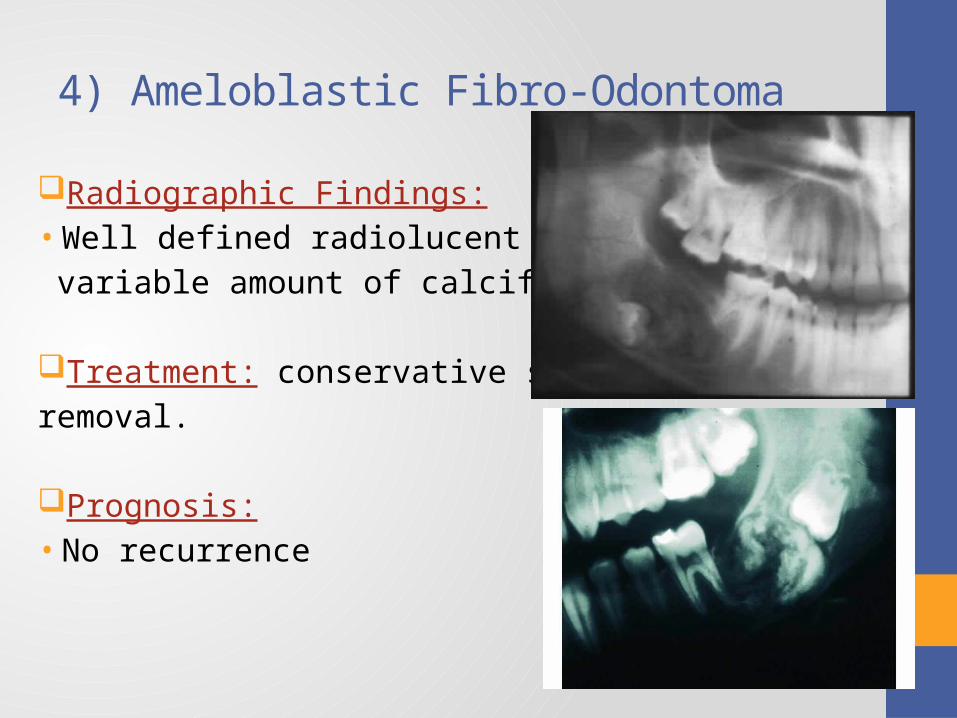
Radiographic Findings:• Well defined radiolucent lesion w/
variable amount of calcified material.
Treatment: conservative surgical
removal.
Prognosis: • No recurrence
4) Ameloblastic Fibro-Odontoma
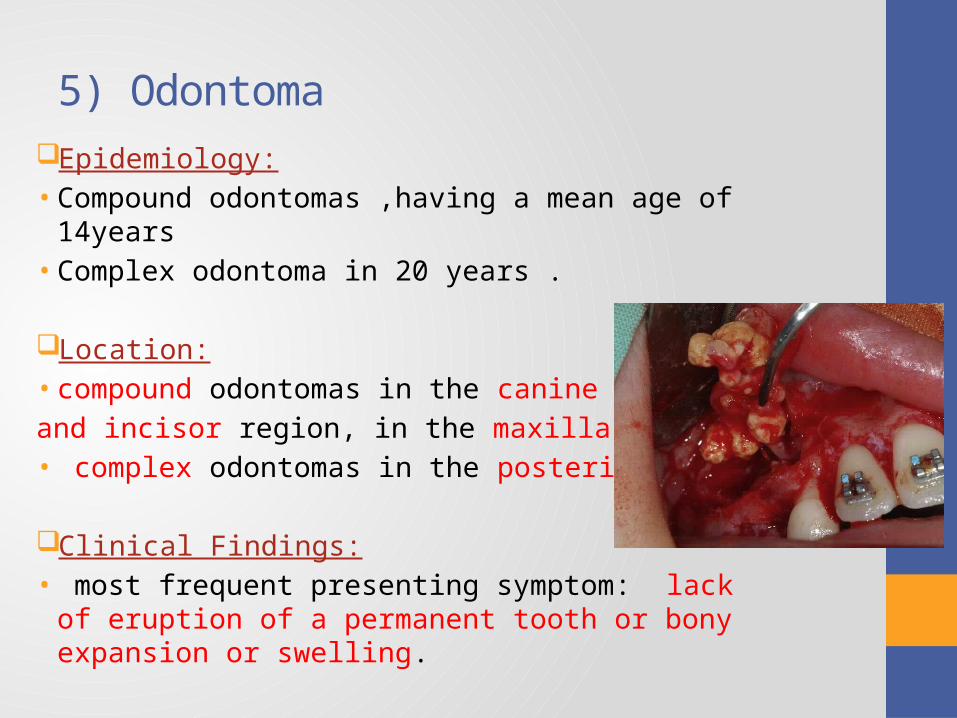
5) Odontoma
Epidemiology:• Compound odontomas ,having a mean age of 14years • Complex odontoma in 20 years .
Location: • compound odontomas in the canine
and incisor region, in the maxilla• complex odontomas in the posterior jaws
Clinical Findings:• most frequent presenting symptom: lack of eruption of
a permanent tooth or bony expansion or swelling.
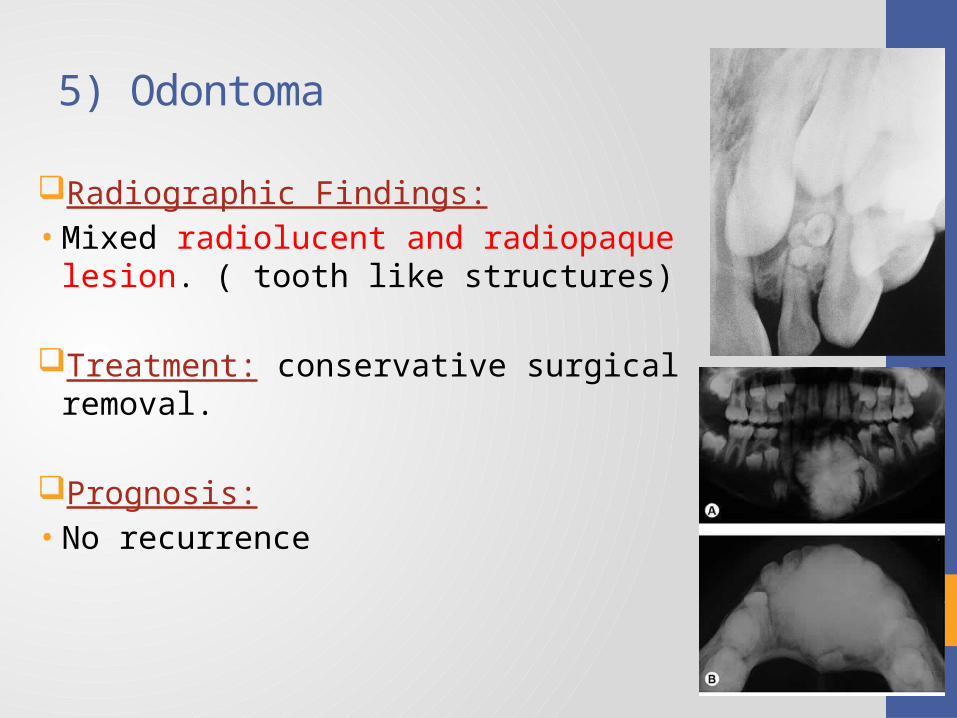
Radiographic Findings:• Mixed radiolucent and radiopaque lesion. ( tooth
like structures)
Treatment: conservative surgical removal.
Prognosis: • No recurrence
5) Odontoma
6) Odontogenic Myxoma
Epidemiology:• 2nd – 4th decayed of life .
• Location: more in the mandible . molar
and premolar region
Clinical Findings:• usually painless,• slow-growing lesions .• noticeable signs and symptoms such as swelling or mobility and
divergence of teeth• Several cases occurring in association with impacted or missing
teeth
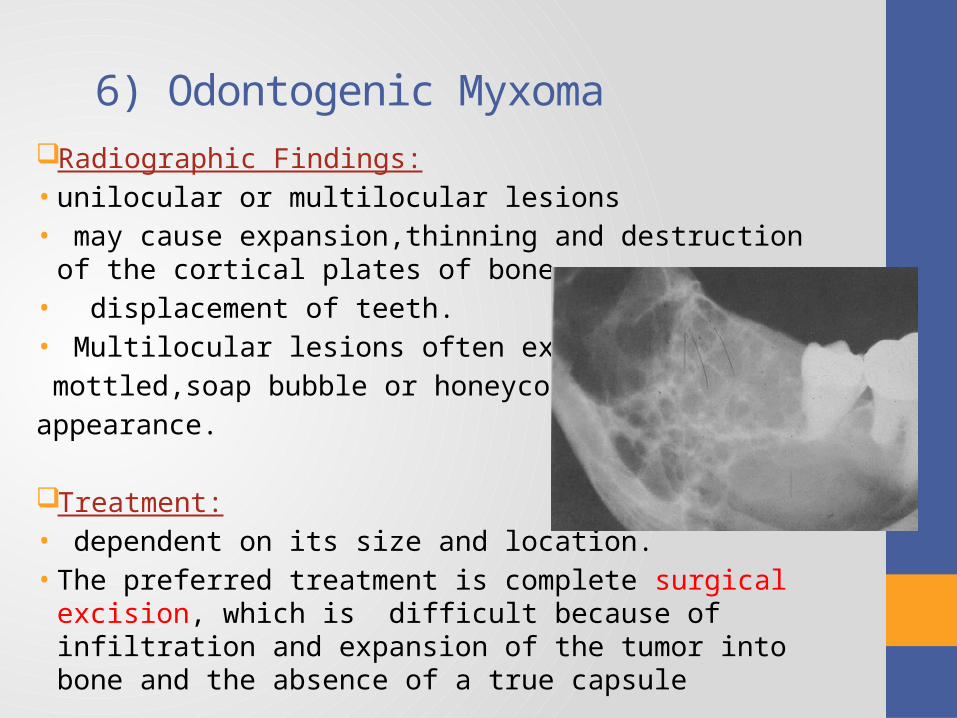
6) Odontogenic Myxoma
Radiographic Findings:• unilocular or multilocular lesions • may cause expansion,thinning and destruction of the
cortical plates of bone• displacement of teeth.• Multilocular lesions often exhibit a
mottled,soap bubble or honeycombed
appearance.
Treatment:• dependent on its size and location. • The preferred treatment is complete surgical excision,
which is difficult because of infiltration and expansion of the tumor into bone and the absence of a true capsule
TUMORS OF BONE
1. Fibrous Dysplasia
2. Juvenile Ossifying Fibroma
3. Central Giant Cell Granuloma
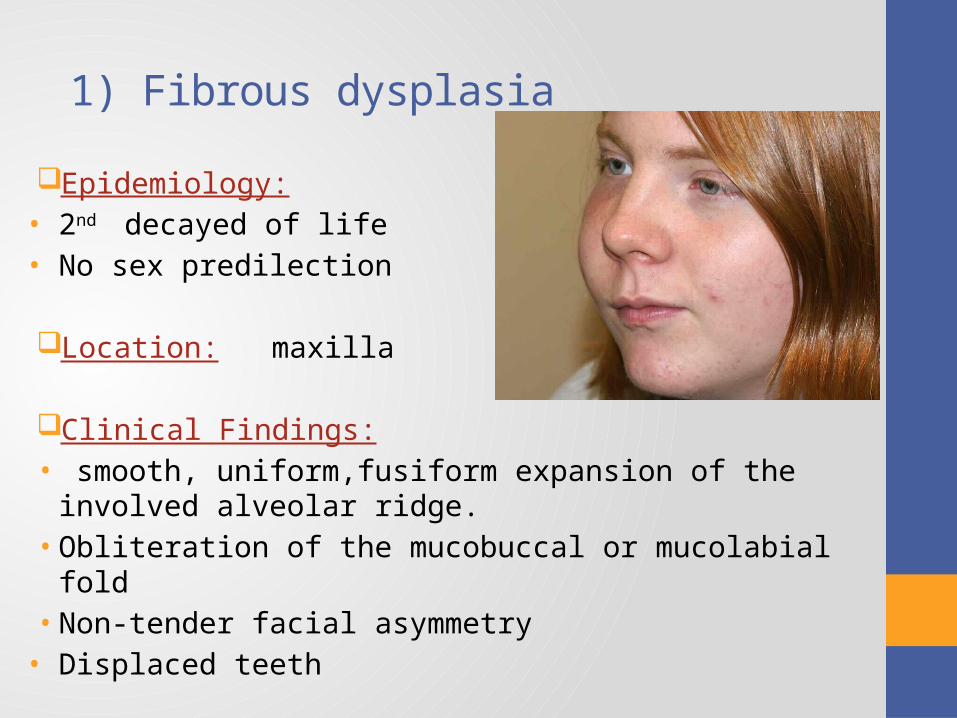
1) Fibrous dysplasia
Epidemiology:• 2nd decayed of life• No sex predilection
Location: maxilla
Clinical Findings:• smooth, uniform,fusiform expansion of the involved alveolar
ridge. • Obliteration of the mucobuccal or mucolabial fold • Non-tender facial asymmetry
• Displaced teeth
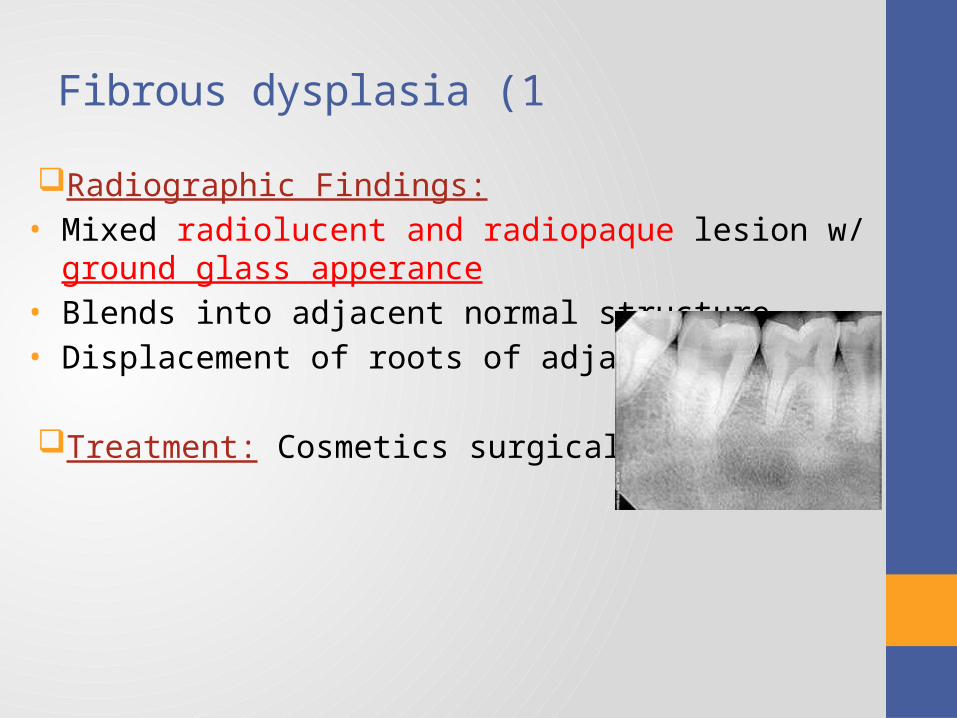
1 )Fibrous dysplasia
Radiographic Findings:• Mixed radiolucent and radiopaque lesion w/ ground glass
apperance• Blends into adjacent normal structure• Displacement of roots of adjacent teeth
Treatment: Cosmetics surgical reduction
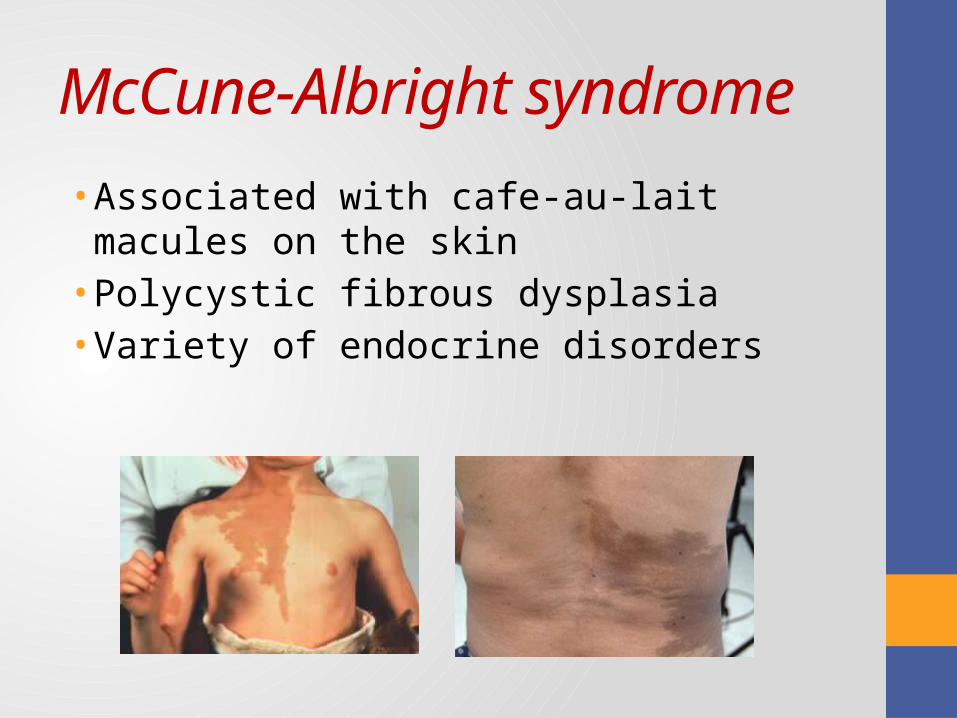
McCune-Albright syndrome
• Associated with cafe-au-lait macules on the skin • Polycystic fibrous dysplasia• Variety of endocrine disorders
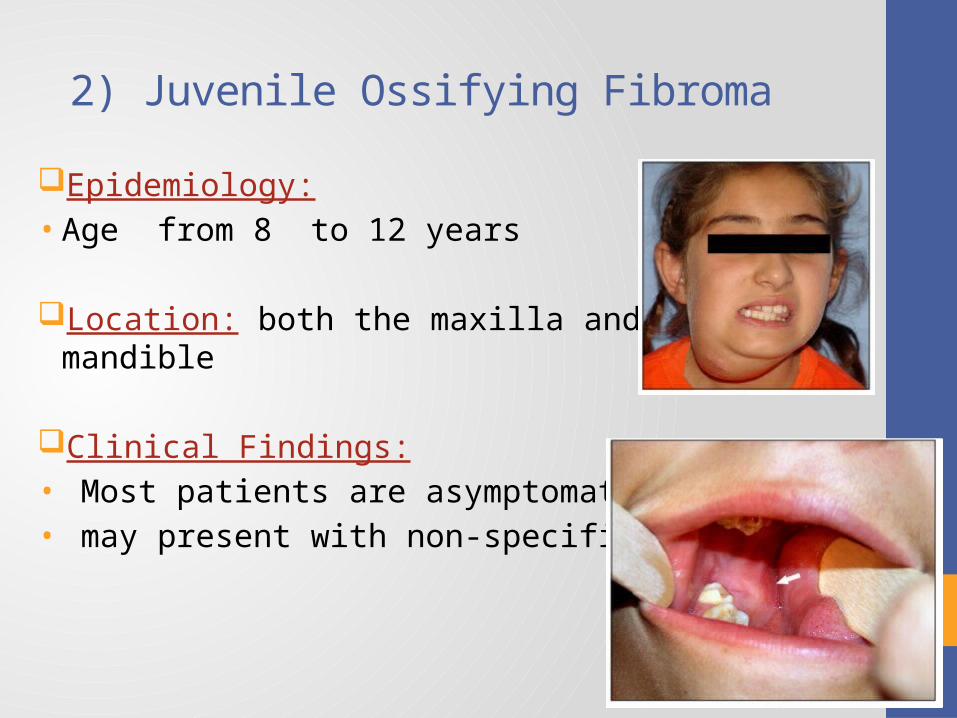
2) Juvenile Ossifying Fibroma
Epidemiology:• Age from 8 to 12 years
Location: both the maxilla and the mandible
Clinical Findings:• Most patients are asymptomatic.• may present with non-specific symptoms.
2) Juvenile Ossifying Fibroma
Radiographic Findings:• well demarcated, expansile mass with an ossified rim at the
periphery
Treatment:
surgical excision
3) Central Giant Cell Granuloma
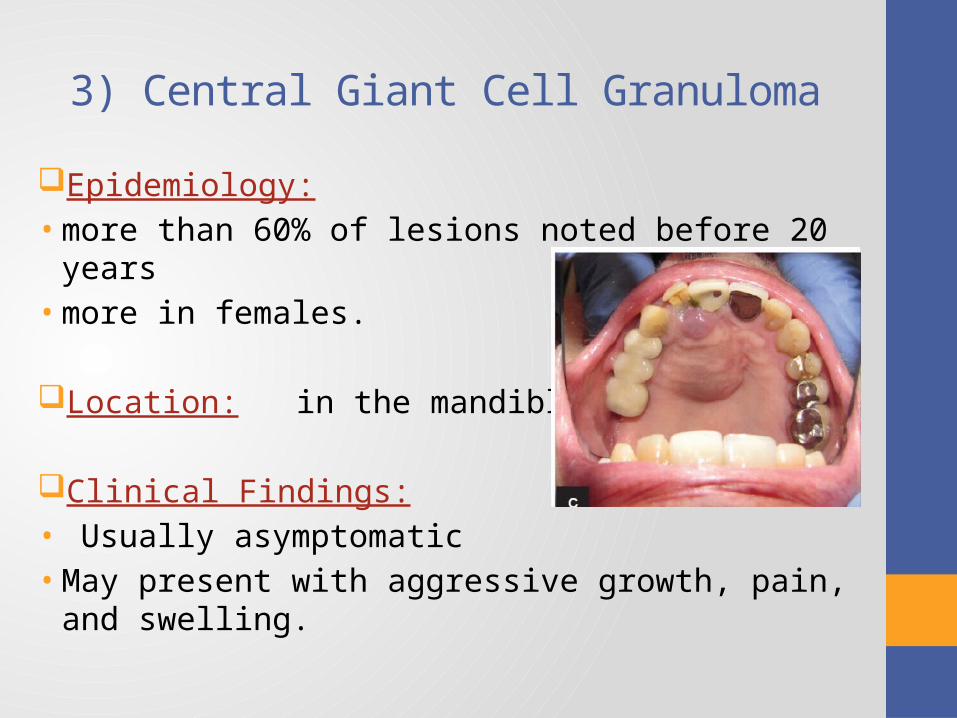
Epidemiology:• more than 60% of lesions noted before 20 years• more in females.
Location: in the mandible .
Clinical Findings:• Usually asymptomatic• May present with aggressive growth, pain, and swelling.
3) Central Giant Cell Granuloma
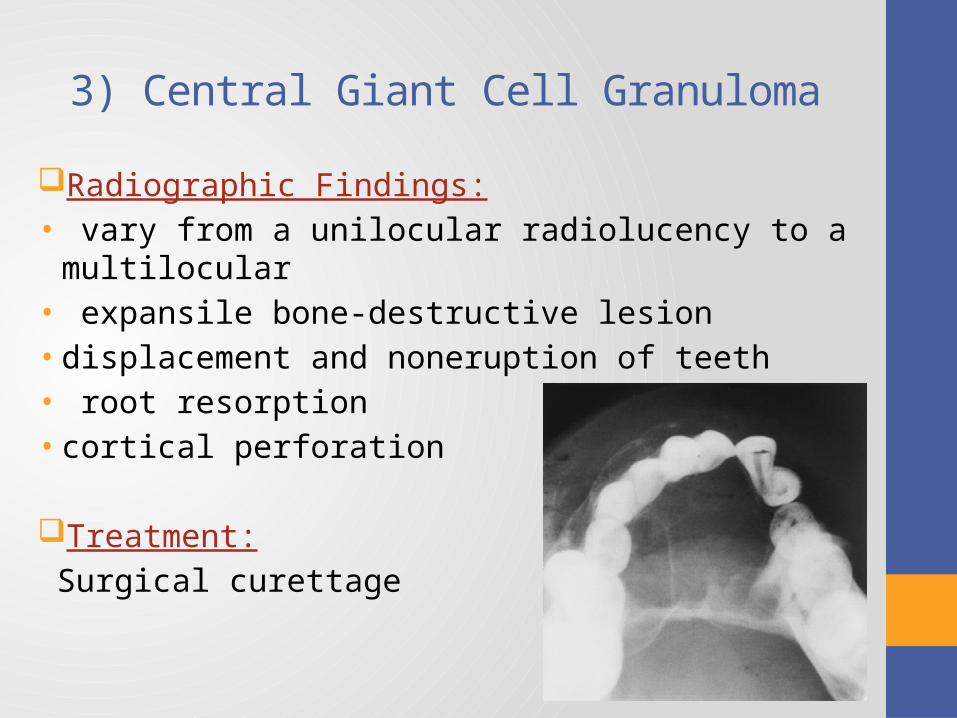
Radiographic Findings:• vary from a unilocular radiolucency to a multilocular• expansile bone-destructive lesion • displacement and noneruption of teeth• root resorption• cortical perforation
Treatment:
Surgical curettage
MALIGNANT TUMORS
1. Fibromatosis
2. Malignant Lymphoma
3. Rhabdomyosarcoma
4. Osteosarcoma
5. Ewing’s Sarcoma
6. Langerhans Cell Histiocytosis (Histiocytosis X )
1) Fibromatosis
Soft tissue :• juvenile or aggressive fibromatosis• locally aggressive in behavior with a tendency for recurrence.
not metastasize.• they can kill by local infiltration and extension into vital
structures.In bone:• Desmoplastic fibromas • the mandible is the most common site of involvement
Epidemiology: 1st decade of life.
1) Fibromatosis
Clinical Findings:• most commonly present as a painless mass• involving the cheek, tongue, or submandibular region• with erosion of bone • arising in soft tissue adjacent to the jaws
Radiographic Findings:• unilocular to multilocular with borders that may vary from ill-
defined to well demarcated.Treatment:
complete surgical excision with a safety margin
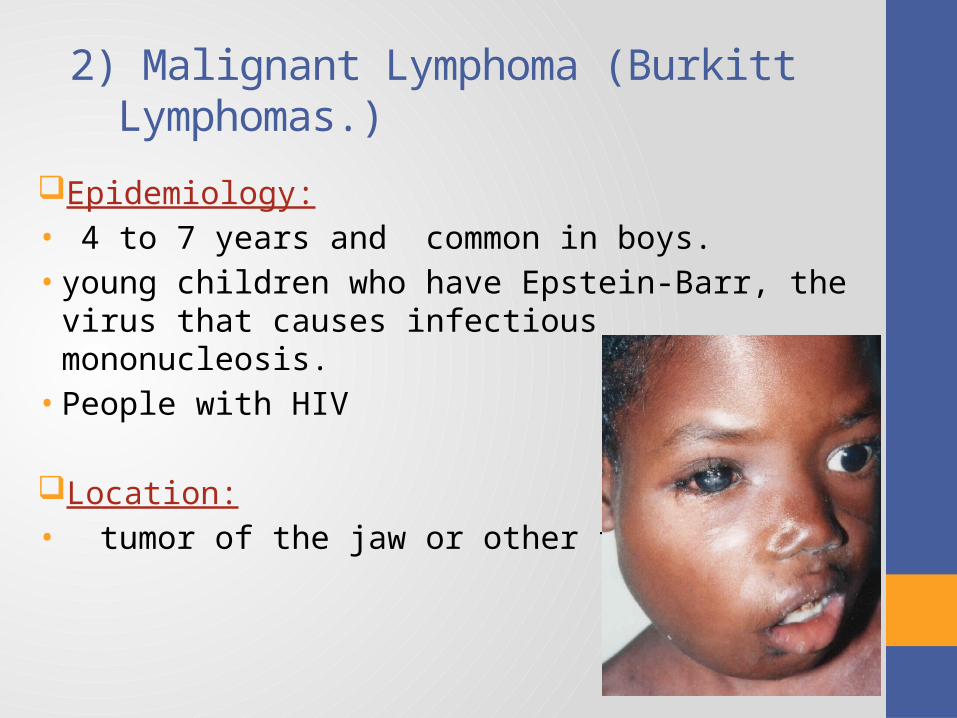
2) Malignant Lymphoma (Burkitt Lymphomas.)
Epidemiology:• 4 to 7 years and common in boys. • young children who have Epstein-Barr, the virus that
causes infectious mononucleosis.• People with HIV
Location: • tumor of the jaw or other facial bones.
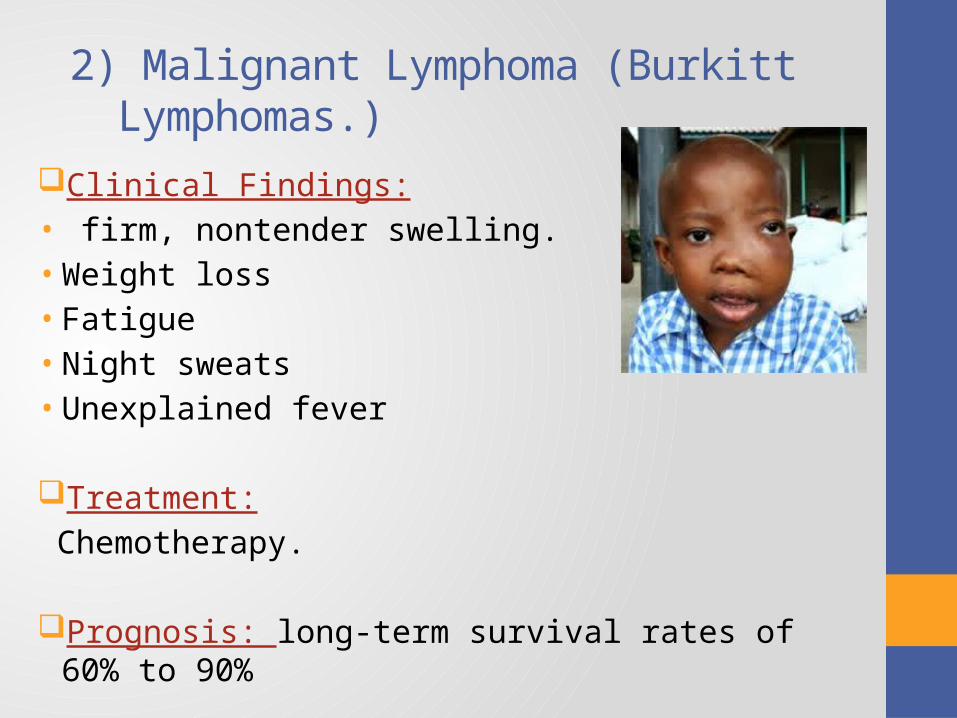
2) Malignant Lymphoma (Burkitt Lymphomas.)
Clinical Findings:• firm, nontender swelling.• Weight loss• Fatigue• Night sweats• Unexplained fever
Treatment:
Chemotherapy.
Prognosis: long-term survival rates of 60% to 90%
3) Rhabdomyosarcoma
Epidemiology:• 2 to 6 years.• a malignant neoplasm of skeletal muscle origin.• is the most common soft tissue sarcoma in children.
Location: Head and neck is most common location.• in children: the eyelid and orbit, parameningeal.• In oral cavity: the soft palate and tonsillar region, tongue.
Clinical Findings:• rapidly growing, nonulcerated soft tissue mass.• Hearing loss & Neurologic symptoms • Extensive destruction of the bone at base of skull.• Metastasis to lung
3) Rhabdomyosarcoma
Treatment:• based primarily on the extent of disease using multiagent
chemotherapy, surgery, and external-beam radiation therapy .
• Prognosis: Good prognosis (~70% 5-year survival)• dependent on age, stage and site• orbital lesions having the highest survival rates • parameningeal tumors having a worse prognosis.
4) Osteosarcoma
Epidemiology:• the modal age of incidence being 16 years for girls and 18 for
boys.
Location: The mandible.
Clinical Findings:• Swelling with or without pain is the most frequently described
early symptom. • Paresthesia, anesthesia and loosening of the teeth .
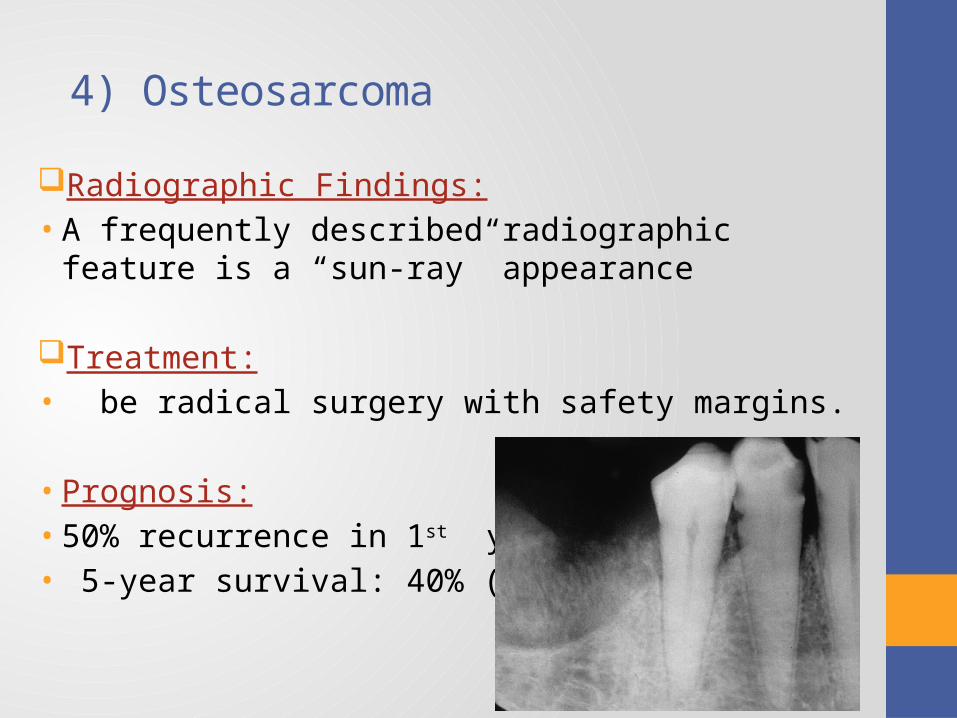
4) Osteosarcoma
Radiographic Findings:• A frequently described radiographic feature is a “sun-ray”
appearance
Treatment:• be radical surgery with safety margins.
• Prognosis:• 50% recurrence in 1st year • 5-year survival: 40% (< 5 cm) .
5) Ewing’s Sarcoma
Epidemiology:• the second most common primary
malignancy of bone.• the average age to be 15 years• More in male.
Location: bones of the head and neck, with the
skull being the most frequent site, then the posterior mandible.
Clinical Findings:• Localized swelling and pain are the most frequent complaints.• paresthesia• tooth mobility • The soft tissue overlying the lesion may be erythematous and warm to the
touch,
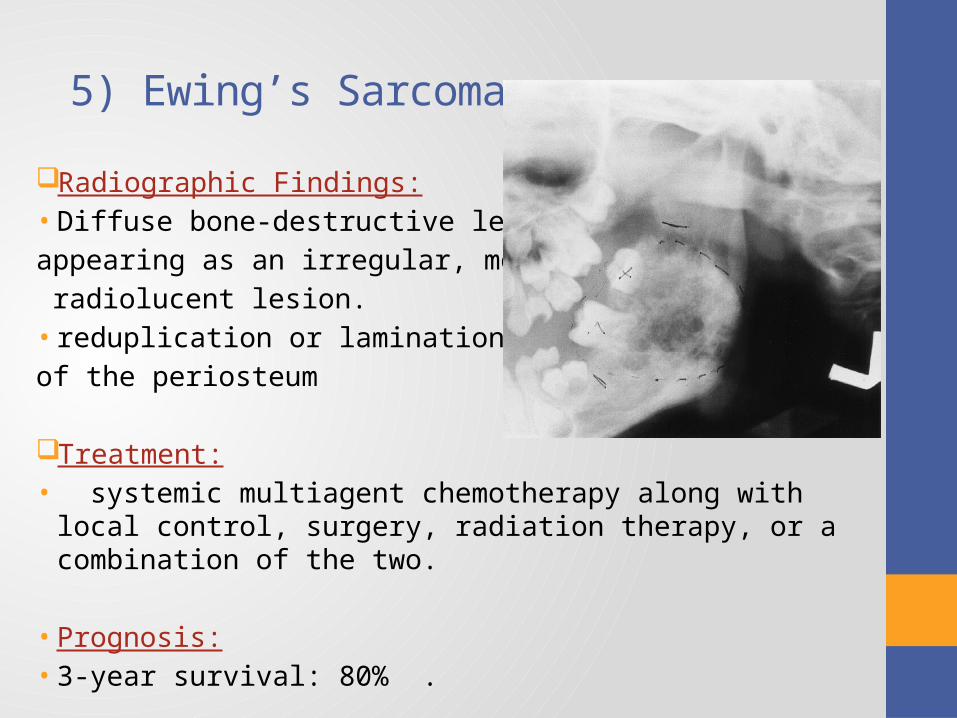
5) Ewing’s Sarcoma
Radiographic Findings:• Diffuse bone-destructive lesion,
appearing as an irregular, mottled,
radiolucent lesion.• reduplication or lamination
of the periosteum
Treatment:• systemic multiagent chemotherapy along with local control,
surgery, radiation therapy, or a combination of the two.
• Prognosis:• 3-year survival: 80% .
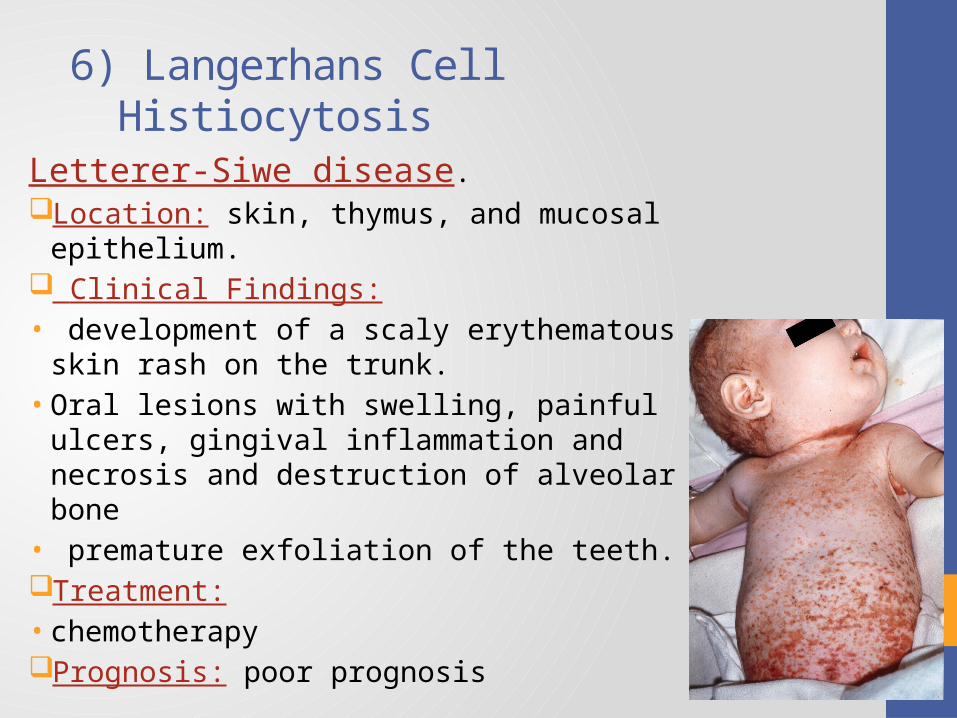
6) Langerhans Cell Histiocytosis
Letterer-Siwe disease.Location: skin, thymus, and mucosal epithelium. Clinical Findings:• development of a scaly erythematous skin rash
on the trunk.• Oral lesions with swelling, painful ulcers,
gingival inflammation and necrosis and destruction of alveolar bone
• premature exfoliation of the teeth.Treatment:• chemotherapyPrognosis: poor prognosis
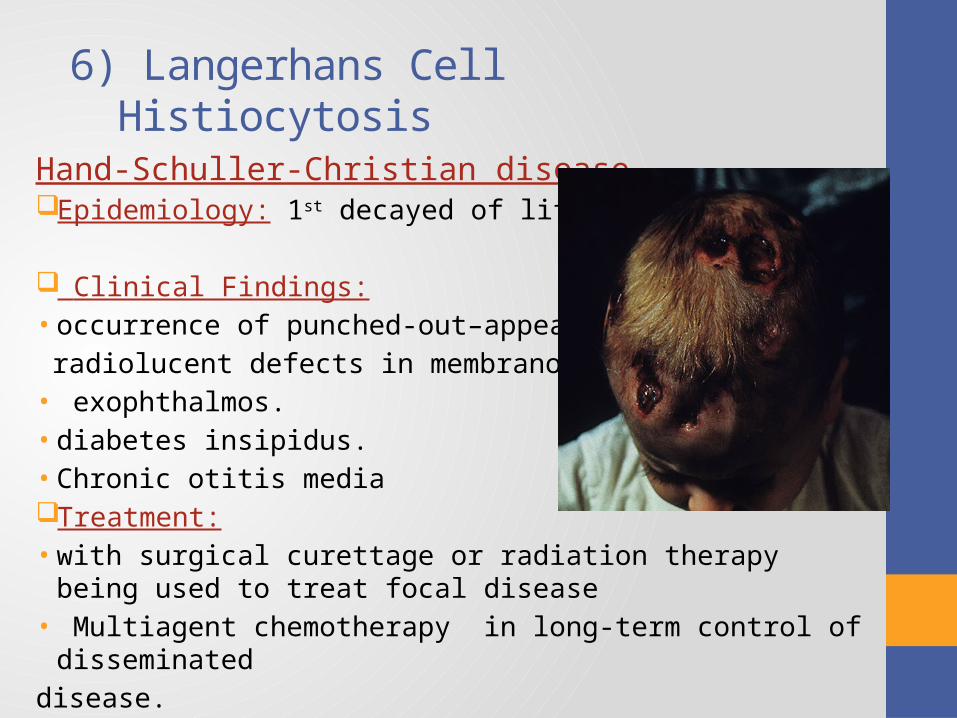
6) Langerhans Cell Histiocytosis
Hand-Schuller-Christian diseaseEpidemiology: 1st decayed of life
Clinical Findings:• occurrence of punched-out–appearing
radiolucent defects in membranous bones• exophthalmos.• diabetes insipidus. • Chronic otitis media Treatment:• with surgical curettage or radiation therapy being used to treat focal
disease• Multiagent chemotherapy in long-term control of disseminated
disease.
6) Langerhans Cell Histiocytosis
Eosinophilic granulomaEpidemiology: most common and also least
severe form.• Older children and young adults
Location: the mandible and skull.
Clinical Findings: pain and swelling.
Radiographic Findings: single or multiple well-defined radiolucent bony lesions.
Treatment:• the lesion may be left alone for observation• it may be surgically curetted or excised,• intralesional injections of corticosteroids
InfectionsA. Viral infections :1. Herpetic infections primary herpes simplex infection.
2. Secondary herpes simplex infection.
3. Herpes varicella-zoster.
4. Mumps.
5. Measles.
6. Rubella.
7. Herpangina.
8. Hand, foot & mouth disease.
9. Infectious mononucleosis.
10. Human papiloma virus.
Infections
B. Bacterial infection:
1. Staphylococcal infections.
2. Streptococcal infection.
3. Congenital syphilis.
4. Tuberculosis.
5. Cat-scratch disease.
Infections
C. Fungal infections:1. Candida.
2. Actinomycosis.
3. Protozoal infections.
Vesiculobullous lesions
1. Epidermolysis bullosa .
2. Erythema multiforme.
3. Pemphigus.
4. Pemphigoid.
White lesions
1. White spongy naevus .
2. Leucoedema.
3. Candidiasis.
4. Geographic tongue.
References
• McDonald and Avery Dentistry for the Child and Adolescent, Jeffrey A. Dean, David R. Avery, Ralph E. McDonald; 9th edition, chapter 8.
• Pediatric Dentistry: Infancy through Adolescence, Paul S. Casamassimo , Henry W., Jr. Fields , Dennis J. McTigue , Arthur Nowak ; 5th edition.