Embed Size (px)
DESCRIPTION
An attempt at designing a device that can aid the administration of CPR
Citation preview

Automated Cardiopulmonary Resuscitation
Device Mita Bhowmick, Meryl Rodrigues, Rishabh Shetty, Ashish Vaswani
Department of Biomedical Engineering, Thadomal Shahani Engineering College, Bandra, Mumbai
Abstract- In India, general awareness of
Cardiopulmonary Resuscitation (CPR) techniques
is limited to physicians and paramedics. There
exists a shocking lack of awareness about
resuscitation techniques in common public circles.
When administered precisely, CPR can save
thousands of lives each year that are lost due to
causes ranging from physiological shocks such as
asphyxiation due to drowning; to even sudden
myocardial infarction/ cardiac arrest (SCA).It is
proposed that designing a device which can
administer the technique with minimal human
intervention can help reduce failure rates
drastically. This is because manual CPR, when
performed even by qualified professionals does
have enough room for error. Automated CPR
aims to eliminate these errors, thereby reducing
failure rates. The objective is to make the
technique available in rural areas where there is
acute shortage of basic healthcare facilities. To
achieve this goal, it is intended to design an easy-
to-use device that can even be operated by a lay
man.
Keywords- Cardiopulmonary Resuscitation,
Automated CPR
I. INTRODUCTION
Manual CPR when performed even by qualified
professionals does have enough room for error.
Automated CPR aims to eliminate these errors,
thereby reducing failure rates. The objective is to
make the technique available in rural areas where
there is acute shortage of basic healthcare facilities.
To achieve this goal, it is intended to design an easy-
to-use device that can even be operated by a lay man.
When done manually, it is difficult to abide by WHO
standards since it is a life-saving technique and will
need to be carried out with the required specifications
for as long as needed. This is very difficult to achieve
manually. Hence, the objective is to study the
principle of administering cardiopulmonary
resuscitation manually, thereby extending the
technique mechanically by use of an automated
apparatus that uses inexpensive mechanisms to
achieve the same.
This involves calculating the displacement, force and
frequency of chest compressions prescribed as per
WHO standards. To identify target areas that such
equipment can cater to. For example, beaches,
swimming pools, aircraft, ambulances, etc. The final
objective of the project is to study the practical
viability of implementing microcontroller-based
timing devices to drive the mechanism for predefined
periods of time as required.
II. REVIEW OF LITERATURE
Before conceiving a new and efficient design, it was
important to review the existing products in the
market. Here is a comparison between the three
available products currently in use in the US market:
The Zoll Autopulse uses an inflatable belt that
autonomously surrounds the chest. This belt
compresses the entire thoracic area. Due to this, cases
of rib fracture have been reported in patients who
have been administered automated chest
compressions using this device.
Michigan Instruments’ Lifestat is a device that
administers localized compression only on the
desired region. However, the piston-like action of the
Lifestat is triggered using a pneumatic cylinder which
is heavy. Due to this, it scores low on the portability
count.

Another competing product is the Lucas, which is
similar in principle to the Lifestat. Oral resuscitation
is also taken care of in this model. The common
shortcoming associated with all the three devices is
their high cost. Average cost of existing models is
around Rs. 12 lakh.
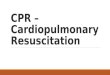
III. SYSTEM DESIGN
The block diagram below illustrates the flow of the
project with the various Electronic and Mechanical
components used and their functional description
A. Power Supply
In the current prototype, an AC to DC alternator is
being used to get power from mains and drive the DC
motor. In the final product, a DC battery can be used.
This battery could be lithium ion or lead acid type,
depending on feasibility and cost considerations.
B. Electronic control
Currently, IC 555 is being used as a timer to adhere
to the compression criteria mentioned by the World
Health Organization. In the future, more specialized
microcontrollers and timing devices can be used to
replace it.
C. Mechanical elements
The base plate, disc, rod and the L-arm form the
basic building blocks of the device.
Before zeroing in on any one design for the project,
we analyzed various options before short listing one
that fulfilled all requirements satisfactorily, while
also being practically feasible.
DESIGN 1:
This design involves the use of a lower unit that is
slid under the patient. An upper unit is fit with a

toothed gear motor and two gear tracks- surrounding
the gear from above and below respectively. These
two tracks are secured to the lower unit with the help
of hooks. When the gear moves anticlockwise, the
tracks advance in opposite directions linearly.
Because of this, the upper unit compresses the
patient’s chest. When the motor rotates in the
clockwise direction, it returns to its original elevated
position. This process is repeated continually to
achieve sustained compressions. A major drawback
of this design is the point of application is not
localized to the heart. It is bulky and involves the
implementation of a gear that moves electronically in
one direction, as well as mechanically in the other.
This forced us to look for other designs to implement
our idea.
DESIGN 2:
Our second design consideration consisted of a motor
around whose axle, a high tension cord is wound.
This cord passes through a tensile spring and an
applicator cushion is attached at its end. A narrow
opening in the base on which the motor rests, restricts
the compression of the spring beyond a particular
limit. When the motor rotates in the anticlockwise
direction, the spring compresses by about 2 inches.
This raises the applicator cushion just above the
patient’s chest. When the motor is switched off, the
spring expands freely in the absence of a puling force
from the motor, which causes the applicator cushion
to compress the patient’s chest. Finding a suitable
spring that matches the requirements of stipulated
Young’s modulus and rigidity was a major hurdle in
this design and was more of a trial and error exercise
than a calculated inference. Wear and tear of the
spring could reduce the life of the spring and in
course of time, the response of the spring to the load
would considerably vary than what is expected.
DESIGN 3:
The third design involves the use of a cam which has
a groove of a suitable depth to facilitate a
displacement of 2 inches as previously mentioned. A
rod suspended vertically at the apex of the spring (or
any mechanically compressible element) would move
about its fulcrum to give us the required linear
motion. At the other end of the rod, the applicator
cushion would be attached. According to the position
of the fulcrum, the displacement could be magnified.
The number of grooves could be increased to provide
us with an increased number of compressions. Again,
the use of a spring poses a hurdle to the life span of
the apparatus
DESIGN 4:
A few design options using magnets surrounded by
intermittent magnetic fields that drive the
compression rod were also considered. One of the
ideas involved the use of two magnetic fields that are
two inches apart from each other. These two fields
are switched on alternately. When the upper field is
switched on, the rod is pulled up and when it is
switched off, the lower magnetic field pulls it down.
The upper magnetic field could be replaced by a
spring to pull the rod up. A motor rotating in the
anticlockwise direction could also be used for the
same.
Another design makes use of two ferromagnetic
elements, one forming the core of an induced

magnetic field formed by a conducting wire wound
around it. By using Faraday’s Law of
Electromagnetic Induction, an AC supply when
passed through the conducting wire would magnetize
the core and this would attract the other
ferromagnetic block whose other end would be
connected to the applicator cushion i.e. when the
field is produced the cushion is pulled up and when it
is switched off, the cushion compresses the chest.
A major disadvantage of this system is the fall of the
rod that is controlled only by the lower magnetic
field. To produce an effective weight 11 kg, a very
heavy rod would have to be used which could harm
the patient. Switching magnetic fields on and off is
easier said than done. The magnetic core takes a
considerable amount of time to get magnetized after
current is supplied to the coil. This design was
theoretically appealing but practically challenging.
DESIGN 5:
The final design that could be implemented is using
two rotating discs driven by two motors. These two
discs could either be cams or could 0have projections
on them. There would be a rod in between the two
discs which would have projections on it. The two
motors should move in opposite directions. The
distance between the projections/grooves should be
such that the required displacement is achieved.
When one motor propels the rod in the forward
direction, after the maximum displacement, the other
motor will pull it back to its original position. As a
result of this, by suspending this apparatus vertically,
using an element to prevent free fall of the rod, the
required compressions can be obtained.
The drawback of this design is that two motors are
used and that would increase expenses and
mechanical liability
FINAL DESIGN:
After analyzing the pros and cons of each of the
above ideas, we came across the works of an
American scientist, William Clark who has
developed various mechanical assemblies that
convert rotational motion to rectilinear motion. One
of these completely suited our needs of achieving
vertical displacement driven by a motor that is
controlled electronically.
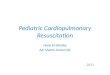
A rod is provided with a projection at one end and a
restrictor block at the other. A disc is fit with two
diametrically opposite projections which drive the
vertical rod. An L-arm is placed on a pivot that
moves in tandem with the projections on the disc.
This motion can be better
explained with the diagram below:

RESULT:
Circular Disc- Since this was the most important
component of the device which would be driven by
the motor and would consequently drive the
applicator rod, we took extra care to provide it with
the right kind of support, without friction. For this,
we drilled a hole at the center of the disc, on the base
plate, welded a rod onto a small circular disc
(smaller than our circular disc) through a shaft on the
front side and the same way on the back side. This
meant that we had stability and at the same time,
freedom of movement for the disc.
Using nuts and bolts with washers we mounted our
main circular disc onto this assembly. We also made
two readymade Teflon projections on the disc for
contact with the L-arm and Applicator rod during the
actual working. The instruments used for this purpose
were the Welding Machine, Drilling Machine,
Tapping screws and the Lathe Machine.
The patient plate was again fabricated using an
aluminium plate which was sawed and filed to get
blunt edges and then it was bent at an angle of 16
degrees to accommodate the feet of the stand which
would be shifted into it while setting up the device
for use.
The Stand was made by using two hollow tubes
which were welded onto bases which resembled the
front ends of shoes. A handle was also welded at the
end of the tube for easy handling. Springs were used
to make easy adjustments when the base plate was
mounted onto the stands.
The Base plate with all its components safely
mounted on it was now ready to be mounted on the
stand to make the device fully functional. This was
achieved by screwing to it two wing-like projections
from either side. The unscrewed ends of these
projections were welded to hollow tubes which were
slightly larger in diameter than the tubes of the stand.
This meant that the tubes could easily slide and then
be tightened wherever necessary on the stand, which
lent the all-important feature of height adjustment
to our device. Again, free fall was prevented by the
springs on the stands.
By simply placing the base plate under the patient’s
chest, placing the base plate on the stands, locking in
the base of the stands on the under-side of the patient
plate and tightening the base plate to maintain its
position, the system would become one piece and
function as a single unit by providing the motor with
power supply.
Timing the compressions:
For the purpose of abiding by the standards set by the
WHO regarding the time for which the compressions
must be given and then paused while the paramedic
checks for the patient’s pulse, we used a simple IC
555 timer in the astable mode so that we could
control the On and Off times of the multivibrator.
The IC 555 is not capable of sourcing enough current
to drive the motor. We needed a current source in
order to drive the motor. This current source should
be able to take in logic command from the IC, then
boost current and drive the motor accordingly. We
had to select the IC for motor driving as per the
requirement of current of motor.
The L293D is a monolithic integrated high voltage,
high current four-channel driver designed to accept
standard DTL or TTL logic levels. It is designed to
drive inductive loads such as relay solenoids,

DC/stepper motors and switching power transistors.
The L293D’s ability to handle the load of my DC
motor makes it an ideal IC for driving our main
motor.
FUTURE SCOPE:
Using more versatile materials such as titanium, hard
PVC and other plastic in place of aluminium may be
beneficial to add rigidity and stability to the design.
Materials that can make the product light-weight
should be probed into.
Research could be initiated in this direction to look
for alternate materials that could be used to design
the skeleton of the device. With the help of
paramedical staff, an efficient mouth-to-mouth
resuscitator can be added as an accessory to make the
product a suitable replacement for manual CPR.
The stand can be calibrated so that it becomes easier
for the attendant paramedical staff to adjust the stand
to suit the patient’s physical characteristics.
Another area that can be worked on is the software
part, wherein, a microcontroller can be used to drive
the motor instead of the IC 555 which is being
employed currently. This would have the advantage
of making the system dynamic by interfacing the
microcontroller to an LCD interface and allowing the
paramedical staff to tweak the number of
compressions being given.
CONCLUSION: The objective of the project was
to achieve a product which would be economically
viable so that the general population could use it;
at the same time an important consideration to be
kept in mind was to achieve a displacement and
timing of compressions as close to WHO
standards as possible.
The approach selected to achieve automated chest
compressions was fabricated using aluminium,
stainless steel and inexpensive hardware. The project
was successfully implemented so that it could
circumvent the problems faced while administering
Manual CPR and also be easy to use with a minimal
amount of training. Any mechanical changes that
need to be made are easily achievable owing to the
fact that the mounting of all the components on the
base plate is done keeping that very idea in mind.
With access to better hardware and raw materials, a
marketable product can be designed in the future. The
mouth-to-mouth resuscitation part of CPR can be
looked into to make this design robust and worthy of
competing with the Michigan Instruments’ LifeStat.