Embed Size (px)
Citation preview

Adrenal insufficiency
Pratap Sagar Tiwari, MD, Lecturer
Department of Internal Medicine

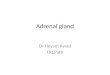
Adrenal Gland
Pic taken from: www.gru.edu
Pic taken from: uvahealth.com
Pic taken from: http://en.wikivet.net/Adrenal_Glands_-_Anatomy_%26_Physiology
A
B
C
A.www.adrenalfatigue.co.nzB.www.gru.eduC.http://en.wikivet.net/Adrenal_Glands_-_Anatomy_%26_Physiology

Primary adrenal insufficiency (Addison's disease)
Autoimmune adrenalitis Polyglandular autoimmune syndrome
Infectious adrenalitis TuberculosisDisseminated fungal infectionHIV infection and AIDSSyphilis
Metastatic cancer Primarily lung, breast, stomach and colon cancer or lymphoma
Adrenal hemorrhage or infarction
Drugs

Causes : Drugs
Drugs
KetoconazoleFluconazoleRifampinPhenytoinBarbituratesMegestrol acetateEtomidate, metyrapone, mitotane

Secondary/tertiary Adrenal insufficiency
• Hypothalamic /pituitary disease• Withdrawal of
suppressive glucocorticoid therapy
• Secondary AI can be caused by interference with corticotropin (ACTH) secretion by the pituitary gland.• Tertiary can be caused by interference with corticotropin-releasing hormone (CRH) secretion by the hypothalamus.

Clinical features
Weakness, tiredness, fatigueAnorexiaGastrointestinal symptoms•Nausea, Vomiting, Constipation•Abdominal pain, Diarrhea
Electrolyte disturbancesHyponatremia, Hyperkalemia, HypercalcemiaAnemia
Weight lossHyperpigmentation (1)Hypotension Vitiligo
Salt cravingPostural dizzinessMuscle or joint pains

Approach to DIAGNOSIS
1. Demonstrating low cortisol secretion
2. Determining whether the cortisol deficiency is dependent on or independent of ACTH deficiency .
3. Seeking a treatable cause of the primary disorder (eg, histoplasmosis involving the adrenal glands or a pituitary adenoma compromising normal pituitary function)

• Serum cortisol concentration: An early morning low serum cortisol concentration (less than 3 mcg/dL [80 nmol/L]) is strongly suggestive of adrenal insufficiency.
• Morning salivary cortisol concentration• Urinary cortisol measurementsNote: Caution should be taken in interpreting the results in patients
with abnormalities of cortisol binding globulin (CBG) or albumin, such as pts with cirrhosis or nephrotic syndrome, or those taking
oral estrogens.

ACTH stimulation testS. Cortisol Plasma ACTH
Low High primary adrenal insufficiency
Low Low Secondary/tertiary Adrenal Insufficiency
250 μg ACTH1-24 (Synacthen) IM•Cortisol levels fail to ↑ in response to ex ACTH in pt with 1 or 2 AI. •Can be distinguished by mx of ACTH (which is ↓ in ACTH def & ↑ in AD. •If an ACTH assay is unavailable, then a long ACTH stimulation test (1 mg depot ACTH i.m. daily for 3 d); •In 2 AI :there is a progressive ↑ in plasma cortisol with repeated ACTH administration, •whereas in AD, cortisol remains <25.4 μg/Dl.

Adrenal Crisis
The syndrome of adrenal crisis (acute adrenal insufficiency) in adults may occur in the following situations:
1.In a previously undiagnosed pt with primary AI who has been subjected to serious infection or major stress.2.In a pt with known primary AI who does not take more glucocorticoid during an infection or other major illness.3.After bilateral adrenal infarction or bilateral adrenal hemorrhage.4.In patients who are abruptly withdrawn from doses of glucocorticoid that cause secondary AI.

Clinical and laboratory findings suggesting adrenal crisis
• Dehydration, hypotension• Nausea and vomiting with a history of weight loss
and anorexia• Abdominal pain, so-called "acute abdomen"• Unexplained hypoglycemia• Unexplained fever• Hyponatremia, hyperkalemia, hypercalcemia• Hyperpigmentation or vitiligo

Management of Adrenal Crisis
Correct volume depletion I.v. saline
Replace glucocorticoids I.v. hydrocortisone succinate 100 mg stat Continue parenteral hydrocortisone (50-100 mg i.m. 6-hourly) until the pt is well enough for reliable oral therapy
Correct other metabolic abnormalities
Acute hypoglycaemia: i.v. 10% glucose
Identify and treat underlying cause
Consider acute precipitant, e.g. infection
Source: Davidson. 21st ed. THE ADRENAL GLANDS

Management of Adrenal insufficiency
Replacement
Glucocorticoid Hydrocortisone is the DOC.In someone who is not critically ill, hydrocortisone should be given by mouth, 15 mg on waking and 5 mg at around 1800 hrs.
Mineralocorticoid Fludrocortisone 0.05-0.1 mg daily
Androgen DHEA (approximately 50 mg/day)
Source: Davidson. 21st ed. THE ADRENAL GLANDS

Thankyou
• Davidsons• Uptodate 20.31. Lynnette K Nieman. Clinical manifestations of adrenal insufficiency in adults.
2. Lynnette K Nieman. Causes of primary adrenal insufficiency (Addison's disease).
3. Lynnette K Nieman. Diagnosis of adrenal insufficiency in adults
4. Lynnette K Nieman. Treatment of adrenal insufficiency in adults
• Medscape1. George T Griffing. Addison Disease
2. Elizabeth A Liotta. Dermatologic Aspects of Addison Disease