Embed Size (px)
Citation preview

Systematic ECG interpretation
SCGH CME
March 17 2016

Components of ECG Rate Rhythm Axis P PR QRS QT ST
Other waves Delta Epsilon Osborne U


Rate Small square 0.04 Big square 0.2
Slow 300/big square Fast 1500/small
square Irregular – count
complexes on rhythm strip x 6 gives average rate
Big squares rate
2 1502.5 1203 1003.5 864 754.5 665 605.5 546 506.5 467 42

Axis https://www.youtu
be.com/watch?v=_CCUWdAaQoA

Axis differentials Left -30 to -90 LBBB LAFB LVH Inferior MI Paced rhythm
Right +90 to +180 RVH LPFB Lateral MI Lung disease –
acute/chronic Hyperkalemia Na channel blockade Dextrocardia NORMAL IN INFANTS and
skinny adults

P WAVE PR interval
120 – 200 msec Long – any heart
block Short – WPW, pre-
excitation Elevation/
depression - pericarditis
Width < 120 msec Amplitude <2.5mm in limb
leads <1.5mm in
precordial leads V1 biphasic Avf inverted


QRS Amplitude Duration Q wave R wave Hypertrophy Bundle branch block J point


Q wave Pathological if >40 ms wide >2mm deep >0.25% QRS Present in leads v1-v3
> 2mm Can be normal in leads III /avR

R wave in V1 RVH - PE Posterior MI RBBB HOCM WPW Dextrocardia Normal in Kids

R WaveR wave in AVR
Na channel blockade
VT Dextrocardia Limb lead reversal
R wave progression
R wave <3mm in V3
Signifies anteroseptal MI
LVH

Left Ventricular hypertrophy
Voltage + non voltage Muscle wall thickens Leading to increased S
wave amplitude in right sided leads
Increased R wave amplitude in left sided leads
Prolonged depolarisation Repolarisation
abnormalities in lateral leads
Causes HTN AR/AS MR HOCM

LVHvoltage
S in V1 + R in V5/V6 > 35mm
AVL R wave 11mm
Non voltage ST depression/T
wave inversion in lateral leads
Increased R wave peak time > 50msec in V5 V6

LVH

RVH Right axis Dominant R in V1 > 7mm or RS ratio >1 Dominant S in V6 > 7mm or RS ratio <1 RV strain – ST depression in V1-4 and
inferiorly

Causes PE Chronic lung disease Pulmonary HTN Mitral stenosis Congenital heart disease Arrythmogenic RV cardiomyopathy

RVH

BBB


ST segment

J pointNotching - BER
Osborne wave - hypothermia




QT Ventricular depolarisation and repolarisation Calculate in lead 2 or V5 V6 Include U waves 440 msec for women 450msec for men Prolongs at slower HR QT> 500 increased risk of toursades Bezetts formula accurate over HR 60-100 HR nomogram for toxicology for risk of
toursades

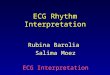
Long QT


T waves Inverted in V1 and AVR Can be – flat, biphasic, inverted, camel
humped or hyperacute Dynamic change most important Don’t miss Wellens syndrome

Wellens Syndrome

Other Waves


Rhythm Regular, irregular, regularly irregular
Heart block Atrial , AVNRT, Accessory pathways Junctional rhythm Ventricular rhythms Distinguish VT from SVT with BBB



AIVR


VT or SVT with abberancy If >35 or Hx of IHD – likely VT Look for Width > 160msec QRS VT likely Concordance Fusion beats Capture beats Right/left axis AV dissociation – p waves notching the QRS First rabbit ear taller RSR1




Children Right sided dominance as infants Should be normal by age 3-4 Rate age dependent Inverted T waves V1-4 can be normal Infant QT 490 https://www.starship.org.nz/for-health-
professionals/starship-clinical-guidelines/e/electrocardiograph-ecg/

QUIZ TIME