Embed Size (px)
Citation preview

1
Epidemiology and Control of
Filariasis-Reshma Ann Mathew

2
FILARIASIS
Filariasis refers to infection with filarial worms.
It is transmitted to humans by the bite of infected
vector mosquitoes. Based on pathogenicity and habitat it classified
into:1) Lymphatic filariasis2) Subcutaneous filariasis3) Serous cavity filariasis4) Zoonotic filariasis

Lymphatic Filariasis
It is a public health problem in India.
Lymphatic filariasis is a vector-borne parasitic
disease.
The disease is caused by thread-like, parasitic
filarial worms: Wuchereria bancrofti(about 95%
cases), Brugia malayi, and Brugia timori.
3

4
Heavily infected areas include UP, Bihar,
Jharkhand, Andhra Pradesh, Orissa, TN,
Kerala and Gujarat.

5
It is endemic in many tropical & subtropical
countries like Africa, Asia, Western Pacific and
parts of America.

6
1.4 billion people live in areas with risk of infection
Out of them, 120 million are infected and need treatment
Out of them, 40 million people are with overt disease
15 million people with lymphoedema
25 million men with urogenital swelling mainly
scrotal hydrocele

7
Mass drug administration (MDA) of DEC was
implemented in India since 2004
In 2007, the strategy of MDA changed to DEC
plus albendazole.
In 2012, the prevalence of microfilaria reduced
to less than 1% in 192 out of 250 implementation
units.

8
The formal goal of the global lymphatic
filariasis programme:
i. to eliminate the disease as a public health
problem
ii. 2020 is the informal target date for interrupting
transmission.

9
Epidemiology1) AGENT FACTORS-
There are atleast 8 species of filarial parasites
that are specific to man.
They are Wuchereria bancrofti, Brugia malayi,
Brugia timori, Onchocerca volvulus, Loa loa, T
perstans, T streptocerca, Mansonella ozzardi
Out of these, the first 3 cause lymphatic
filariasis.

10
PERIODICITY-
Both the microfilaria(Mf) of W. bancrofti and B.
malayi occurring in India display nocturnal
periodicity, i.e. appear in large no. at night,
retreat from blood stream during the day.
The maximum density is reported between
10pm to 2am.
This is a biological adaption to the nocturnal
biting habits of the vector mosquitoes.

11
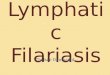
LIFE CYCLEDefinitive host-Man, Intermediate host- MosquitoThe adult worms (macrofilaria) are found in the
lymphatic system of man, where they may survive for 15yrs or more.
During their lifespan, after mating, female worms (viviparous) give birth to 50,000 immature microfilariae(mf) per day into the blood circulation via lymphatics. They may survive up to a year or more.
Some of these microfilariae may be ingested by the mosquitoes during their blood meal.

12
Stages in the mosquito-1) Exsheathing- The larva comes out of the sheath in
which it was enclosed. Occurs in stomach of the mosquito.
2) First stage larva-The larva penetrates the stomach wall of the mosquito, and migrate thoracic muscles where it develops into a short thick form
3) Second stage larva-The larva moults and increase in length
4) Third stage larva(INFECTIVE)-The larva moults and develops into a long thin form which migrates to the proboscis of the mosquito. The mosquito is said to be infected.

13

14
INCUBATION PERIOD
The time interval from invasion of infective
larvae to the development of clinical
manifestations-CLINICAL INCUBATION
PERIOD
It is about 8-16months

15
RESERVOIR OF INFECTION
Although filarial infection occurs in animals, human
filariasis is not usually a zoonosis.
In man, the source of infection is a person with
circulating Mf in peripheral blood.
In filarial disease (late obstructive stages), Mf are
not found in the blood.
The minimum level of Mf which will permit
infection of mosquitoes is not known.

16
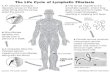
VECTORS OF LYMPHATIC FILARIASIS
In India,
i. Culex (C. quinquefasciatus)- vector for Bancroftian
filariasis
ii. Mansonia(M. annulifers & M. uniformis)- vector for
Brugian filariasis
Culex breeds in polluted water
Mansonia is associated with certain aquatic plants
(such as Pistia stratiotes)
Culex
Mansonia

17
2) HOST FACTORS-Man is a natural host.a) AGE All ages are susceptible to infection. The infection rates rise with age up to 20-30 yrs and
then level off
b) GENDER In most endemic areas, Mf rate is higher in men
c) MIGRATION Migration led to the extension of filariasis into non-endemic areas

18
d) IMMUNITY
Resistance is developed only after years of
exposure
e) SOCIAL FACTORS
Lymphatic filariasis is associated with poor
sanitation, urbanization, migration of people,
etc.

19
3) ENVIRONMENTAL FACTORSa) CLIMATE – It influences the breeding of mosquitoes, their longevity and
the development of parasite in insect vector. Max. prevalence of the mosquito was seen between 22-38 °C
and relative humidity of 70%
b) DRAINAGE – Vectors breed profusely in polluted water.
c) TOWN PLANNING – Inadequate sewage disposal and lack of town planning have
aggravated the problems of filariasis in India. The common breeding places are open ditches, septic tanks,
ill-maintained drains.

20

21
CLINICAL MANIFESTATIONS
Only a small proportion of infected individuals
exhibit clinical signs
They are of 2 types:
i. Lymphatic Filariasis- caused by the parasite in
the lymphatic system.
ii. Occult Filariasis- due to immune hyper-
responsiveness of the human host.

22
1) LYMPHATIC FILARIASIS-It has the following stages-a) Asymptomatic amicrofilaremia- does not show Mf or
clinical manifestations of the disease.
b) Asymptomatic microfilaremia- Asymptomatic, but blood is positive for Mf.
c) Stage of acute manifesations- Occurs in first few months and years Recurrent episodes of acute inflammation in lymph
glands & vessels Manifested as filarial fever, lymphangitis, lymphadenitis,
lymphoedema & epididymo-orchitis(male).

23
d) Stage of chronic obstructive manifestations-
Occurs 10-15yrs after the onset of first acute attack.
Causes permanent structural changes due to fibrosis
and obstruction
of lymphatic vessels.
Main clinical features are
hydrocele, elephantiasis &
chyluria.
In Brugian filariasis, genitalia are
rarely involved.

24

25

26
2) OCCULT FILARIASIS-
The classical clinical manifestations are NOT
PRESENT and Mf are NOT FOUND in the
blood.
Occurs due to hypersensitivity reaction to
filarial antigens derived from Mf.
Eg: Tropical pulmonary eosinophilia.

27
LYMPHOEDEMA MANAGEMENT1) Treatment for Uncomplicated ADLA( acute
dermato-lymphangioadenitis) Give analgesic-paracetamol (1g, 3-4times a
day) Give oral antibiotic-penicillin(1.5g in 3 divided
doses X 8days). In case of allergy to penicillin, give oral erythromycin(1g, 3times a day)
Clean the limb with antiseptic Check for any wounds, cuts, abscesses {give
antibiotic cream} and interdigital infection {give antifungal cream}.

28
Give advice on prevention of chronic lymphoedema
DO NOT give antifilarial medicine Home management- elevation of limb, drink
plenty of water, wriggling the toes, washing the limb.
Follow up after 2 days.

29
2) Management Of Severe ADLA Refer patient to physician, he is given-
i. IV benzylpenicillin (Penicillin G)-3g, 3 times a day, until fever subsides.
Then, oral phenoxymethylpenicillin (Penicillin V)-750mg to 1g, 3times a day X 8days
ii. In case of allergy to penicillin, IV erythromycin 1g 3times/day until fever subsides.
Then, oral erythromycin 1g, 3times a day. Give anagesic/antipyretic-paracetamol DO NOT give antifilarial medicine.

30

31

32
HYDROCELE MANAGEMENTThe individuals are referred for diagnosis and
surgery done if necessary.Men have a good prognosis with early
hydrocele and corrective surgery can be undertaken even with local anaesthetic.
Quality pre- and post-operative care are important components that help make this surgery successful. For other genital damage, more complicated surgery is often required.
Unfortunately, however, hydrocele surgery is often too expensive for those afflicted with LF.

33
Filaria SurveyIt is done for routine survey or survey for evalution.The NICD (National Institute of Communicable
Diseases) standard is to examine 5-7% of the population for routine surveys and 20% for evaluation studies.
It consists of-1) Mass blood survey2) Clinical survey3) Serological tests4) Xenodiagnosis5) Entomological survey

34
1) Mass Blood Survey- It depends upon the demonstration of living parasites
in the human body. Night blood surveys are donei. Thick film-
Most commonly used method 20mm3 of blood is collected by a deep finger
prick between 8.30pm and 12 mid-night. The blood films are dehaemoglobinised, stained,
dried and examined for Mf under low power.ii. Membrane filter concentration-
Most sensitive method for detecting low density microfilariaemia.

35
iii. DEC provocation test- Mf can be induced to appear in blood in
the daytime by administering DEC100mg orally.
Mf begin to reach their peak within 15minutes and begin to decrease 2hrs later.

36
2) Clinical SurveyPeople are examined for clinical manifestations
of filariasis.
3) Serological testsTo detect antibodies to Mf and adults using
immunoflorescent and complement fixing techniques.
But , CANNOT DISTINGUISH between past and present infection, and heavy and light parasite loads.

37
4) XenodiagnosisMosquitoes are allowed to feed on the patient, and
then dissected 2weeks later.
5) Entomological surveyIt consists of:
i. general mosquito collection from housesii. dissection of female vector species for detection
of developmental forms of the parasiteiii. Study of the extent and type of breeding places.

38
Assessment of Filarial Control Programmes
It can be assessed using:
1) Clinical parameters
2) Parasitological parameters
3) Entomological parameters

39
1) CLINICAL PARAMETERS Incidence of acute manifestations and
prevalence of chronic manifestations are measured.
2) PARASITOLOGICAL PARAMETERSi. Microfilaria rate- It is the % of people
showing Mf in their peripheral blood in the sample population.

40
ii. Filarial endemicity rate- It is the % of people examined showing microfilariae in their blood, or disease manifestation or both.
iii. Microfilarial density- It is the no. of Mf per unit volume of blood in samples from individual people. It indicates the intensity of infection
iv. Average infestation rate- It is the average no. of Mf per positive slide. It indicates the prevalence of microfilaraemia in
the population.

41
3) ENTOMOLOGICAL PARAMETERSThey comprise
i. Vector density per 10 man-hour catchii. % of mosquitoes positive for all stages of
developmentiii. % of mosquitoes positive for infective larvaeiv. Annual biting ratev. Types of larval breeding places

42
Control MeasuresPreviously, even after full regimen of
Diethylcarbamazine(DEC), some microfilariae still persisted in the body. So it was difficult to prevent the spread of filariasis.
So it is supplemented by an effective vector control programme.
The current strategy is based on-i. Chemotheraphyii. Vector control

43
CHEMOTHERAPY1) DEC
2) Filaria control in the communitya) Mass Therapy
b) Selective Treatment
c) DEC-medicated salt
3) Ivermectin

44
1) DECIt is safe and effective.
Given in divided doses after mealsRapidly absorbedReaches peak blood levels in 1-2hrsRapidly excreted
Filariasis Dose1) Bancroftian filariasis 6mg/kg body weight per
day orally for 12 days2) Brugian filariasis 3-6mg/kg body weight per
day orally for 12 days

45
DEC is effective in killing Microfilaria.Adverse effects-
i. Due to the drug itself- headache, nausea, vomiting, etc. They are seen few hours after the first dose, but do not last for more than 3 days.
ii. Allergic reactions due to destruction of microfilariae and adult worms-fever, local inflammations around dead worms, orchitis, lymphadenitis and hydrocele. They occur later and last longer.
If these drugs are given in spaced doses, the adverse reactions are much less frequent and less intense.

46
2) Filaria control in the community
2) Filaria control in the communitya) Mass Therapy
b) Selective Treatment
c) DEC-medicated salt

47
a) Mass therapy- DEC is given to everyone in the community
irrespective of whether they have microfilaraemia, disease manifestation or no signs of infection; except children under 2yrs, pregnant women and seriously ill patients.
Dose: DEC 6mg/kg body weight Indicated in highly endemic areas

48
b) Selective treatmentDEC given only to those who are Mf positive.More suitable in low endemicity areasDose: 6mg DEC per kg body weight daily for
12 dosesIn endemic areas, it should be repeated every
2yrs

49
3) DEC-medicated salt-Common salt is medicated with 1-4g of DEC per
kg.

50
3) IvermectinIt is a semisynthetic macrolide antibiotic with
broad spectrum activity against nematodes and ectoparasites.
It is NOT USED in India, used in AfricaIn normal people, there is no drug toxicity. But,
in microfilaraemic patients, there may be reactions due to inflammatory response due to the dying microfilariae.

51
Vector ControlVector control is beneficial when used in
conjunction with mass treatment.The most important step is to reduce the target
mosquito population to stop or reduce the transmission.
It consists of:i. Anti-larval measuresii. Anti-adult measuresiii. Personal prophylaxis

52
1) Anti-larval measure It consists of –
a) CHEMICAL CONTROL-i. Mosquito larvicidal oil
Active against all pre-adult stages Used to control Culex Very expensive than others
ii. Pyrosene oil-E It is a pyrethrum based emulsifiable larvicide
iii. OP larvicides Widely used, but resistance developed against many Eg: temephos, fenthion.
MLO
Temephos
Fenthion

53
b) REMOVAL OF PISTIA PLANT-To control breeding of Mansonia mosquitoesDone by either converting the pond to fish or
lotus culture (OR) using herbicides such as Shell Weed Killer D
c) MINOR ENVIRONMENTAL MEASURES-It includes:
i. Drainage of stagnant waterii. Adequate maintenance of septic tanks
Pistia plant

54
2) Anti-Adult measures
Previously, DDT was used. But, it has been discontinued
Pyrethrum is now used as a space spray.

55
3) Personal prophylaxis
Avoidance of mosquito bites by using mosquito nets
ScreeningRepellents

56
INTEGRATED VECTOR CONTROL
None of the vector controls applied alone is likely to bring about filariasis control. It has to be an integrated approach.
1) Development of annual drug treatment2) Intensive personal hygiene3) DEC-medicated salt4) Development of insecticide sprays

NATIONAL FILARIA CONTROL PROGRAMME
It is operational since 1955In June 1978, it was merged with malaria scheme.Filaria control strategy includes
i. vector control through anti-larval operationsii. Source reductioniii. Detection and treatment of microfilaria carriersiv. Morbidity management
57

58
The strategy is through:i. Annual Mass Drug Administration(MDA)ii. Home based management- of lymphoedema
and upscaling of hydrocele operations. To achieve elimination, in 2004 the Govt. of
India launched annual MDA with single dose of DEC along with home based foot care and hydrocele operation
The co-administration of DEC + Albendazole was introduced in 2007

59
Thank You