Embed Size (px)
Citation preview
FACIAL PAIN
FACIAL PAIN
• A frequently encounteredneurological symptom
• Seldom associated with significantneurological disease unlessaccompanied by other symptoms orneurological signs
CausesTrigeminal neuralgia
Migranous neuralgia
Post herpetic neuralgia
Psychogenic (Atypical facial pain)
Tempomandibular arthritis
Malocclusion
PATHPHYSIOLOGY
• Within the skull, the dura(including thedural sinuses and falx cerebri) and theproximal parts of large blood vessels arethe main structures sensitive to pain
• Mostly innervated by the branches of thetrigeminal nerve
This probably accounts for the patterns of painreferral seen in intracranial disease whenthese pain sensitive parts of the intracranialcontent are stretched,distended or otherwiseirritated.
Diagnostic approach
• Important points in history
• Over-all pattern
• Tempo of onset
• Time of day of onset of maximal pain
• Effect of posture, coughing and straining
• Location of pain
• Associated symptoms
TRIGEMINAL NEURALGIA
• A disorder of the trigeminal nerve (fifth) that causes
episodes of sharp, stabbing pain in the cheek, lips,
gums, or chin on one side of the face.
• People with this pain often wince or twitch, which is where
trigeminal neuralgia gets itsFrench nickname
‘tic douloureux’, meaning "painful twitch”.
• Commonly in middle aged or elderly people
• F>M

Forms of TN:
1) TYPICAL TN
2) ATYPICAL TN
3) PRE-TN
4) MULTIPLE-SCLEROSIS-RELATED TN
5) SECONDARY TN
6) POST-TRAUMATIC TN (TRIGEMINAL NEUROPATHY)
7) FAILED TN
Typical Trigeminal Neuralgia (Tic Douloureux)
Most common form of TN, that has previouslybeen termed Classical, Idiopathic and EssentialTN.
Mostly caused by blood vessels compressingthe trigeminal nerve root as it enters the brainstem.
This neurovascular or microvascularcompression at the trigeminal nerve root entryzone may be caused by arteries of veins, large orsmall, that may simply contact or indent thetrigeminal nerve.

Normal people without TN TN sufferers
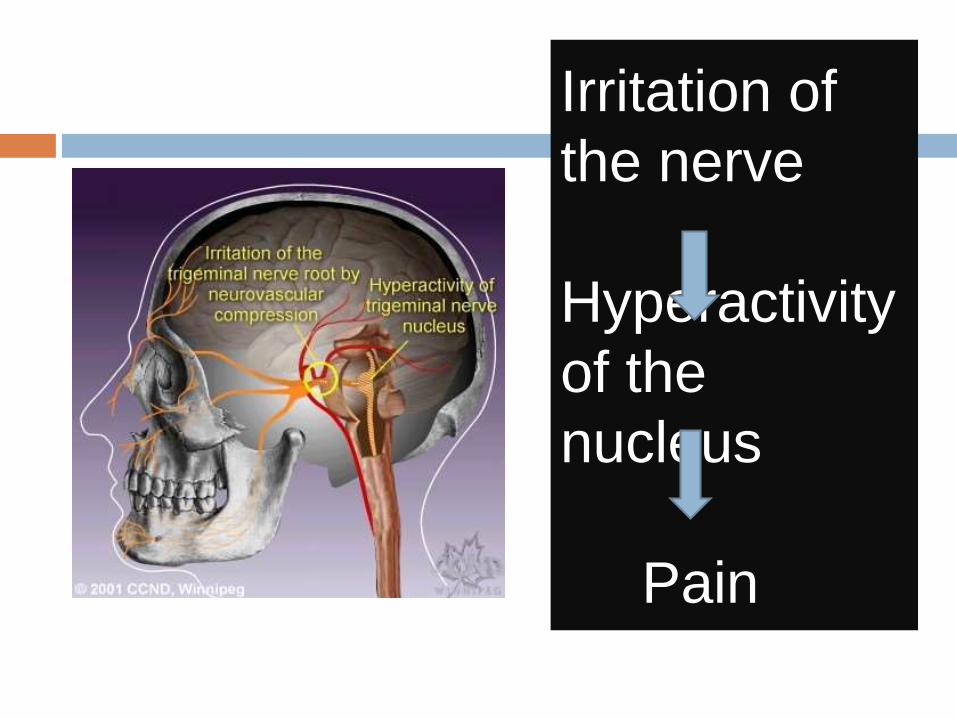
Irritation of
the nerve
Hyperactivity
of the
nucleus
Pain
1. Degeneration
2. Pressure
3. Irritation of the nerve.
4. Pressure from a nearby abnormally-formed artery lying too close to the nerve.
ETIOLOGYUncertain but may be caused by
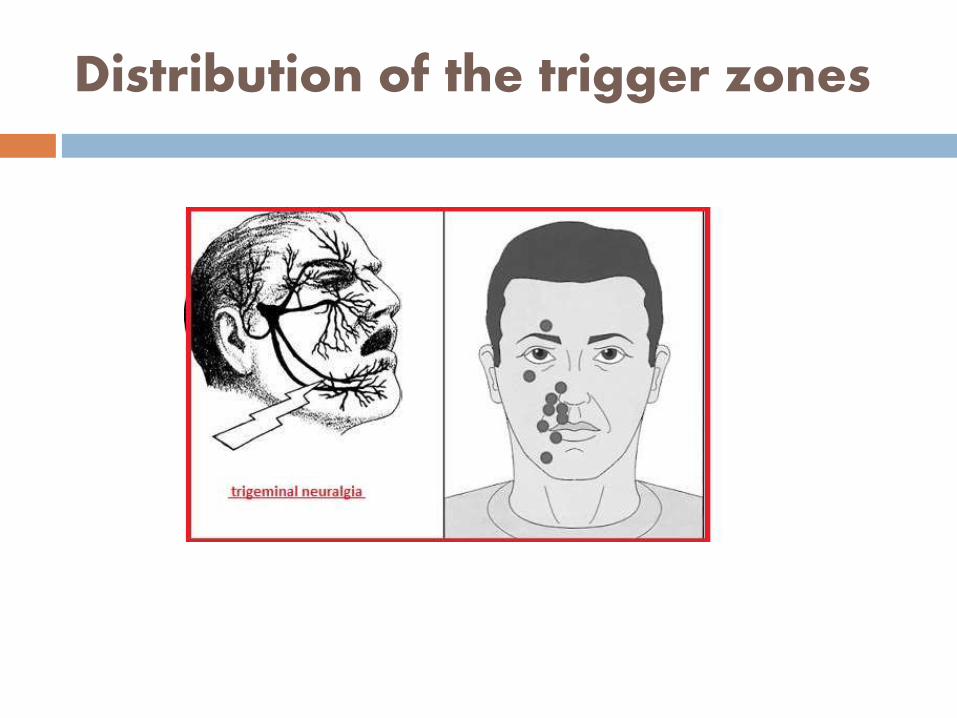
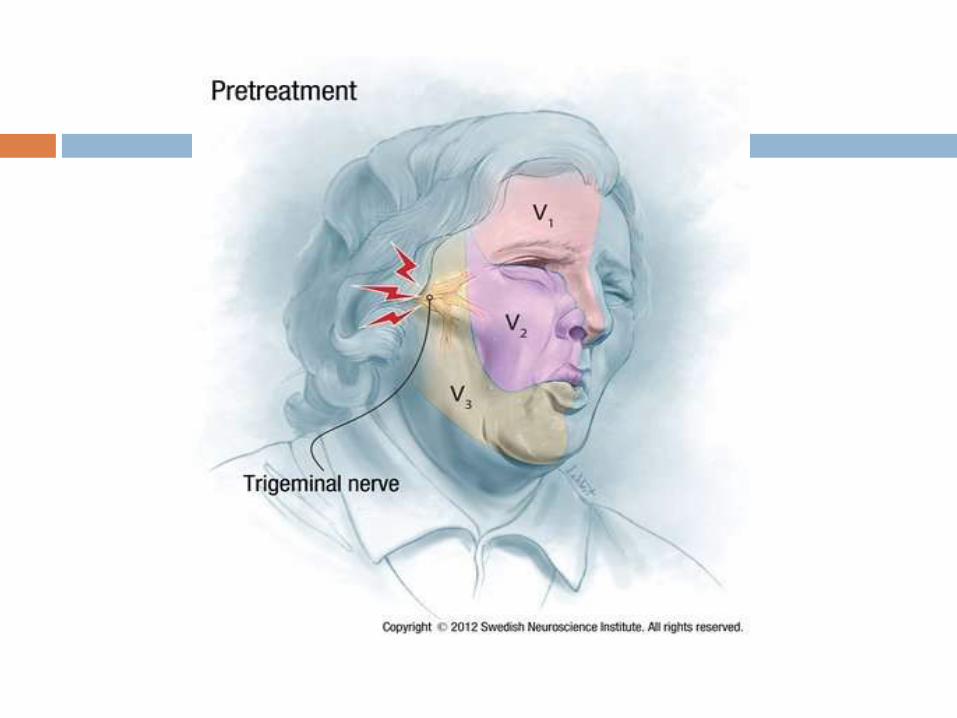
Distribution of the trigger zones
TRIGGER FACTORS
Touching Washing of
faceShaving
Teeth cleaning
Cold breeze Eating
TalkingApplication of
lotions and cosmetics
Clinical features
• Pain is a characteristic symptom
• Occurs in bouts or paroxysms, sharp orlancinating in character
• Radiates to the territory of one or moredivisions of a trigeminal nerve
• Patient is disturbed , feels totally shaken
• The first episodes are usually fairly mild
and brief, and it may be minutes, hours,or weeks before the next attack.
However, attacks tend to occur in clumpsthat may last for weeks at a time.
With age, the episodes become more
frequent and painful, until the person
begins to live in constant fear of the next one.
The momentary bursts of pain usually
begin from the same spot on the face each
time.
• May show simultaneous remissionsin early stages but as the diseaseadvances, become less frequent.
• No sensory loss over face
If sensory loss or motor symptoms orsigns accompany , then it’s called theSecondary neuralgia.
Secondary to certain neurological diseasesuch as multiple sclerosis andmeningioma of a trigeminal nerve.
Secondary Trigeminal Neuralgia
Treatment
1. Medical
2. Surgical
SURGICAL
1. Injection of phenol or alcohol into a trigeminal ganglion
2. Radiofrequency coagulation of a branch
3. Sectioning of sensory root of trigeminal ganglion inside the
cranium
4. Microvascular decompression
PREVENTION
While the condition itself can't be prevented, there area number of things patients can do to avoid triggering attacks:
Wash with cotton pads and warm water over the
face
Rinse the mouth with water after eating, if tooth-brushing triggers pain
Eat and drink food and beverages at room temperature
Chew on the unaffected side
Eat soft foods, if eating is becoming a problem
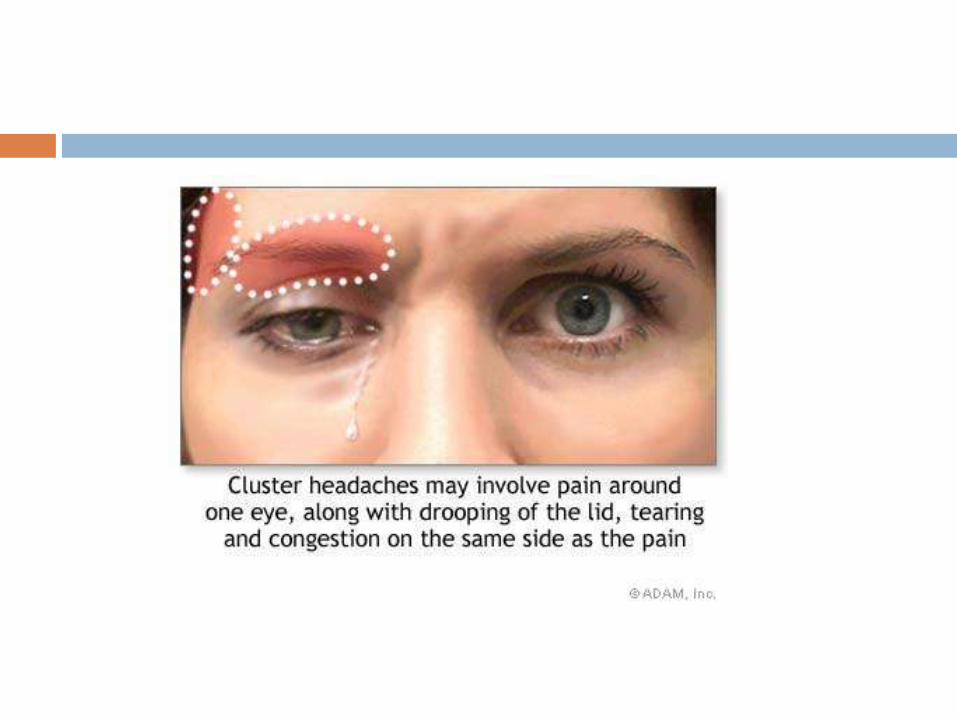
MIGRANOUS NEURALGIA
An exquisitely painful affliction of the mid faceand upper face, particularly in and around theeye.
The name is derived from the fact that theheadache occurs in temporal groups or‘clusters’ with extended periods of remisssionbetween attacks.
TRIGGER FACTORS
Alcohol , cigarette smoking
High altitudes
Bright light
Exertion (physical activity)
Heat (hot weather,
hot baths)
Foods high in nitrites (such as
bacon and preserved
meats)Certain medicine
s
Cocaine
CLINICAL FEATURES
May occur at any age, although it usually affectspersons in the 3rd and 4th decade of life .
M > F (6:1)
They tend to run in families, passed down through genes.
The pain is described as paroxysmal ( abrupt onset) and intense, with a burning or lancinatingquality and without a trigger zone.
The pain occurs on one side of the head.
It may be described as:
Burning
Sharp
Steady
The pain may occur in, behind, and around oneeye.
May involve one side of the face from neck totemples.
SIGNS AND SYMPTOMS
Conjunctival injection
Excessive tearing
Lacrimation
Forehead/
facial sweating
Rhinorrhea
Ptosis
MiosisEyelid edema
Red flushed
face
TREATMENT
Ergotamine tartarate
Oxygen inhalation
Serotonin antagonists
PROPHYLAXIS
β blockers
Steroids
Methylsergide
Lithium carbonate
ATYPICAL FACIAL PAIN
A pain disorder of the face, is often compared to trigeminal neuralgia but is a different entity.
Symptoms are more persistent, with few, if any, periods of remission.
CAUSESOnce thought to be psychological in origin, now recognized
as a neurological disease with a large number of possible causes including:
1. Sinus infections
2. Dental infections
3. Ernest Syndrome
4. Temporal tendonitis
5. Vagus nerve tumors
6. Trigeminal ganglia compression
7. Facial trauma
8. Trigeminal nerve trauma
9. Cervical spine disorders
Symptoms
Usually localized to one side of the face
Can be described as sharp, dull, crushing,aching, burning, pulling or squeezing.
Often occurs over the region of the trigeminalnerve, but the pain can also affect the scalp andneck.
The condition is different from other facial painsyndromes by its persistent presence; with noremissions.
Diagnosis
The first step in diagnosing atypical facial pain is a neurological examination.
The physician will try to rule out similar conditions such as trigeminal neuralgia, temporomandibular joint syndrome, migraines and cluster headaches.
Finally, imaging may help pinpoint the cause:
X-Rays of the skull
MRI/CT scan
Treatment
Medications:
• Amitriptyline (antidepressant)
• Gabapentin (anticonvulsant)
• Carbamazepine(anticonvulsant)
• Baclofen (muscle relaxant/antispasmodic)
• Clonazepam (muscle relaxant/anticonvulsant)
• Valproic (anticonvulsant)
Invasive Procedures:
• Microvasculardecompression
• Glycerol injection
• Balloon compression
• Peripheral nerve stimulation
• Stereotactic radiosurgery
• Percutaneous trigeminal tractotomy
• Motor cortex stimulation

TEMPOROMANDIBULAR ARTHRITIS
• KNOWN AS COSTEN’S SYNDROME
• PAIN is severe aching,
• Gets intensified by chewing, movement of jaw
• Occurs at the temporomandibular joint
• Usually unilateral
Includes:
Loss of dental occlusal support
Ear symptoms (pain, tininitus)
Sinus Pain
Causes
Costen's syndrome arises from faultyarticulation of the temporomandibularjoint caused by one or more of:
dental malocclusion
emotional stress producing masseterspasm
Treatment
Short term treatment consists of a very soft diet and simple analgesia, and may be sufficient for mild symptoms.
Long term treatment may involve dental correction or stress relaxation.
Referral to a specialist clinic may be needed.
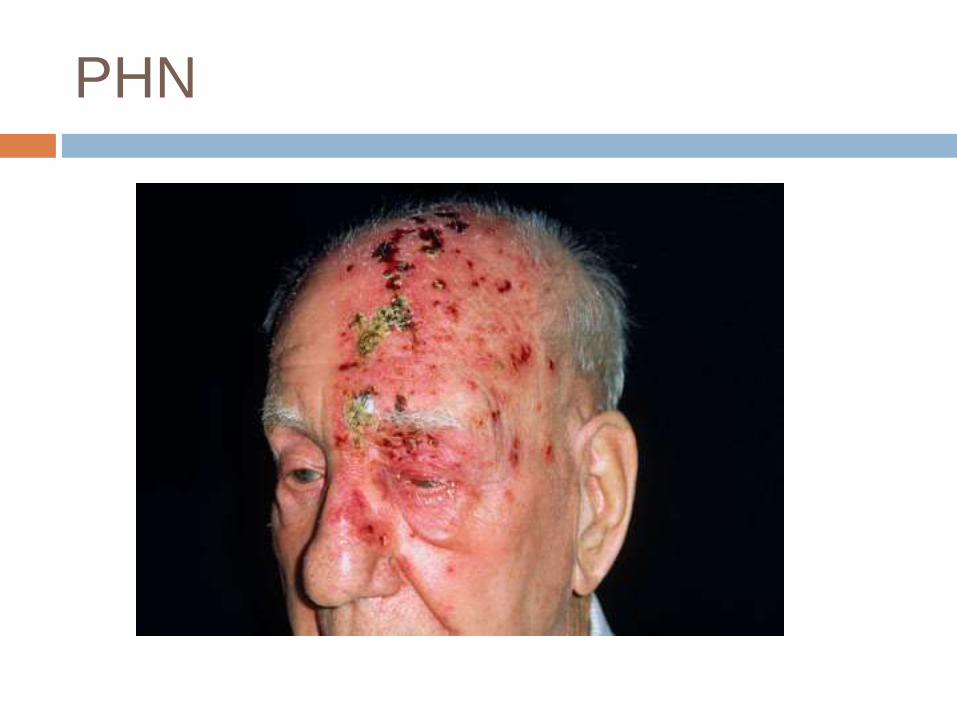
Post herpetic neuralgia
• A nerve pain due to damage caused bythe varicella zoster virus.
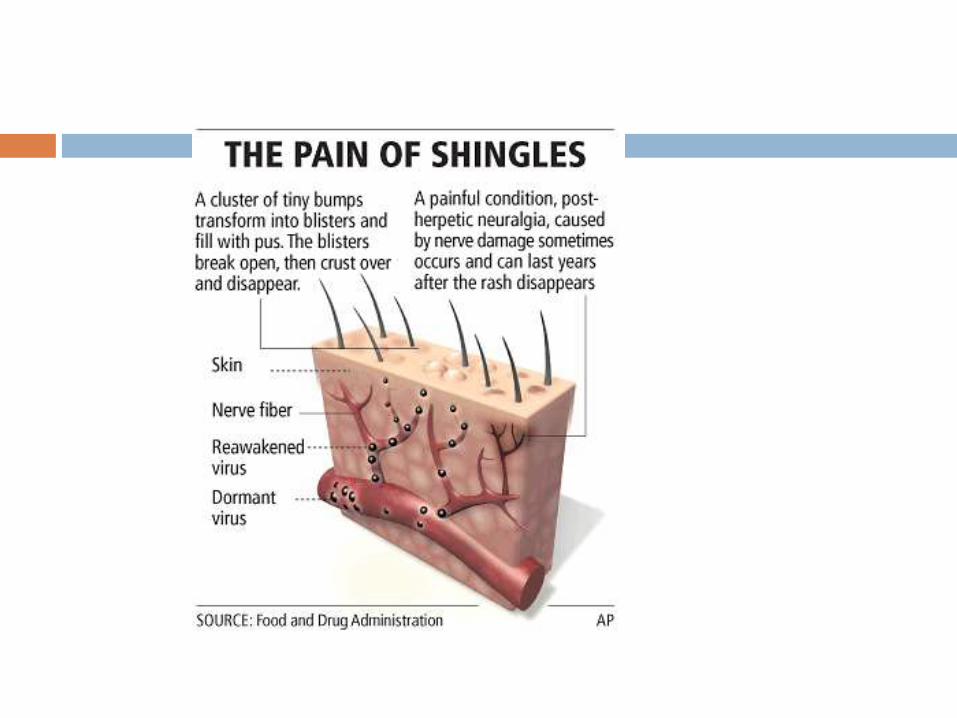
• Typically, the neuralgia is confined toa dermatomic area of the skin and follows anoutbreak of herpes zoster (shingles) in thatsame area.
• The neuralgia typically begins when the herpeszoster vesicles have crusted over and begun toheal, but it can begin in the absence of herpeszoster.
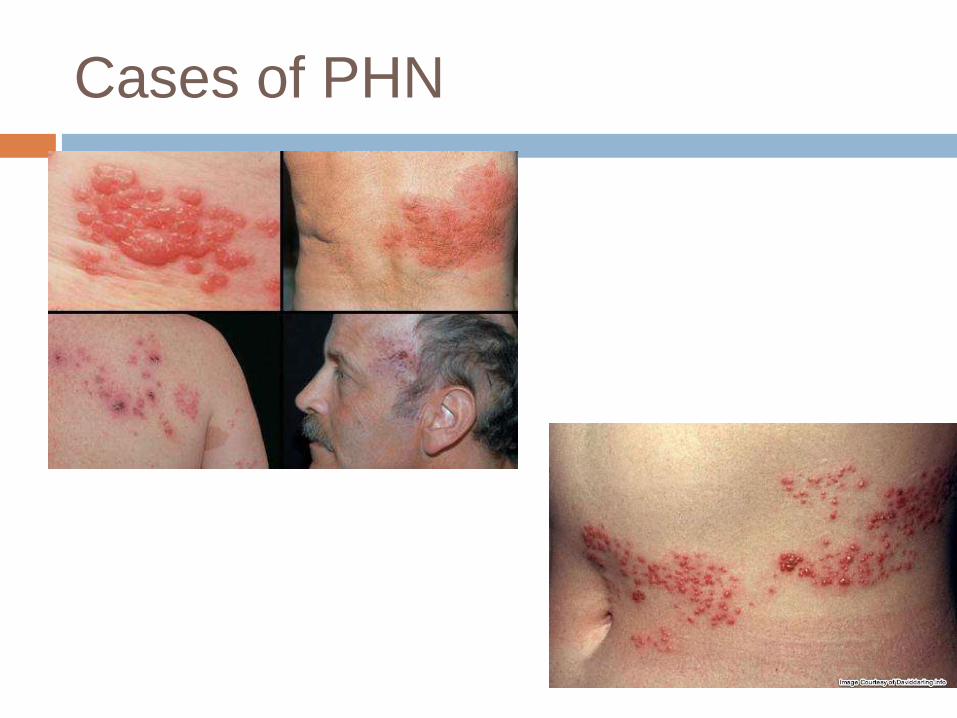
Cases of PHN
Pain for three months or more
Stabbing or burning pain
Rashes on the chest, forehead, stomach, or any parts of the body
Formation of blisters that eventually will heal but pain lingers
People with PostHerpetic Neuralgia are sensitive to touch because of the sensitivity of the nerves
People who have this disease are also sensitive to temperature changes.
Feeling of numbness if the nerves involved control the movement of an individual
Itchiness and headaches
Signs and symptoms
PHN
Treatment
• CARBAMAZEPINE
• PHENYTOIN
• ANTIDEPRESSANTS

Some measures you can take to reduce pain are described below.
Wear comfortable clothing
Cover sensitive areas
Use cold packs
GENERAL ADVICE
1. Practicing healthy habits healthy diet
2. Maintain a regular sleep routine and good sleephygiene (avoiding tea, coffee, etc)
3. Engage in regular exercise
4. Relaxation techniques hypnosis, meditation,and visualization.
5. Abstain from the triggering foods
6. Stay educated by joining support groups,speaking with your doctor.