Embed Size (px)
Citation preview

FAILING RV IN PAH HOW TO MANAGE
FAILING RIGHT VENTRICLE IN PAH
HOW TO MANAGE DR KEERTHIKA
NIMS,HYDERBAD ,INDIA

FAILING RV IN PAH HOW TO MANAGE
RV FAILURE DUE TO PAH• Irreversible PAH
• Idiopathic PAH • Eisenmenger's syndrome
• Reversible PAH• CHD with shunts • PTE

FAILING RV IN PAH HOW TO MANAGE
Natural History of Idiopathic PAH In 1980, the National Institutes of Health (NIH) established a registry on primary pulmonary hypertension (PPH) that described the clinical characteristics of the disease and its natural history over a 5-year period. The median survival was 2.8 years, with survival rates of 68%, 48%, and 34% at 1, 3, and 5 years, respectively. Based on the data from this registry, an equation incorporating the pulmonary artery pressure, right atrial pressure, and cardiac index was developed to predict survival. Observed survival with epoprostenol therapy at 1, 2, and 3 years was 87.8%, 76.3%, and 62.8% and was significantly greater than the expected survival of 58.9%, 46.3%, and 35.4% based on historical data. Baseline predictors of survival included exercise tolerance, functional class, right atrial pressure, and vasodilator response to adenosine. Predictors of survival after the first year of therapy included functional class and improvement in exercise tolerance, cardiac index, and mean pulmonary artery pressure.

FAILING RV IN PAH HOW TO MANAGE
Natural History of Idiopathic PAH 1. Rich S, Dantzker R, Ayres S, et al. Primary pulmonary hypertension: a national prospective
study. Ann Intern Med. 1987; 107: 216–223.
2. D’Alonzo G, Bart R, Ayres S, et al. Survival in patients with primary pulmonary hypertension: results from a national prospective registry. Ann Intern Med. 1991; 115: 343–349.
3. Rich S, McLaughlin V. The effects of chronic prostacyclin therapy on cardiac output and symptoms in primary pulmonary hypertension. J Am Coll Cardiol. 1999; 34: 1184–1187.
4. McLaughlin, Vallerie V., Alicia Shillington, and Stuart Rich. "Survival in primary pulmonary hypertension the impact of epoprostenol therapy." Circulation 106.12 (2002): 1477-1482.

FAILING RV IN PAH HOW TO MANAGE
NORMAL RIGHT VENTRICLE
The RV pumps the same stroke volume of LV but with 25% of the stroke work because of the low resistance offered by pulmonary
vasculature.
Therefore, by virtue of the Laplace relationship, the right ventricle is more thin walled and compliant.
Longitudinal shortening is a greater contributor to right ventricular stroke volume than short-axis (circumferential)
shortening
Geometry of chamber is complex consisting of an inlet (sinus) portion and outlet (conus) sepatated by crista supraventricularis.

FAILING RV IN PAH HOW TO MANAGE
PHYSIOLOGY OF RV vs. LV
• RV filling normally STARTS BEFORE and FINISHES AFTER LV.• RV IVRT, filling velocities (E and A) and the E/A ratio are LOWER but • Respiratory Variations In Filling Velocities Are More Pronounced.• Compared with the LV, the RV demonstrates a HEIGHTENED
SENSITIVITY to afterload change

FAILING RV IN PAH HOW TO MANAGE
IT IS LINKED TO LEFT VENTRICLE BY
Shared wall (septum) ,
By mutually encircling epicardial fibers
By attachment of RV free wall to anterior and posterior septum
By sharing pericardial space

FAILING RV IN PAH HOW TO MANAGE
Perfusion of the RV
• (1) its lower oxygen consumption,• (2) its more extensive collateral
system, especially from• the moderator band artery, a
branch of the first septal perforator that originates from LAD,
• (3) its ability to increase oxygen extraction.
The relative
resistance of the RV
to irreversible
ischemic injury
explained by :

RV AND PAH
The right ventricle is exposed to pressure overload by chronic pulmonary hypertension from any cause .
In PAH initial adaptive response is that of MYOCARDIAL HYPERTROPHY followed by progressive contractile dysfunction and then chamber dilation
Chamber dilatation ensues to allow compensatory preload and maintain stroke volume despite reduced fractional shortening.(FRANKS STARLING)
FAILING RV IN PAH HOW TO MANAGE

FAILING RV IN PAH HOW TO MANAGE
DECOMPENSATED RIGHT VENTRICULAR FAILURE IS CHARACTERIZED BY
clinical evidence of rising filling pressures,
diastolic dysfunction
diminishing cardiac output,
tricuspid regurgitation
due to annular dilatation and poor leaflet coaptation.

FAILING RV IN PAH HOW TO MANAGE
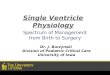
• The right ventricle in severe idiopathic pulmonary arterial hypertension assumes a spherical shape with a greater cross-sectional area than the left ventricle (LV).
• The more spherical-shaped right ventricle results IN ABNORMAL SEPTAL FUNCTION that also impairs left ventricle performance.

FAILING RV IN PAH HOW TO MANAGE
Norbert F. Voelkel et al. Circulation. 2006;114:1883-1891
Copyright © American Heart Association, Inc. All rights reserved.

FAILING RV IN PAH HOW TO MANAGE
VENTRICULAR INTERDEPENDENCE
• Ventricular interdependence is the phenomenon in which the size shape compliance of one ventricle may affect the size , shape & pressure volume relationship of other ventricle through direct mechanical interaction.
• Systolic ventricular interdependence mediated mainly through interventricular septum , pericardium in diastolic ventricular interdependence.
• About 20 – 40 % of RV systolic pressure and volume outflow results from LV contraction

FAILING RV IN PAH HOW TO MANAGE
In the presence of RV scarring also RV output is by septal interaction UNTIL RV IS DILATED .
• shifts the IVS to left , • alters LV geometry • increases pericardial constraint • results in decrease in LV compliance
leads to decreased LV preload • increased LV end diastolic pressure
or low cardiac output state.
In acute RV
pressure and
volume overload & dilation of
RV

FAILING RV IN PAH HOW TO MANAGE
Assessment of Ventricular Interdependence
Ventricular interdependence may be clinically assessed by considering
(1) The degree of reciprocal respiratory change in ventricular filling profiles,
(2) Ventricular coupling (in dimension or pressure), or(3) Abnormal septal motions (SEPTAL BOUNCE)

FAILING RV IN PAH HOW TO MANAGE
•RV FUNCTION IS THE MOST IMPORTANT DETERMINANT OF LONGTERM SURVIVAL IN PATIENTS WITH PAH

FAILING RV IN PAH HOW TO MANAGE
RV FAILURE
RV failure is a complex clinical syndrome that can result from any structural or functional cardiovascular disorder that impairs the ability of RV to fill or to eject blood

FAILING RV IN PAH HOW TO MANAGE
Right ventricular failure is the main cause of death in patients with PAH, the ability of the right ventricle to ADAPT to the progressive increase in PVR is the main determinant of a patient’s functional capacity and survival
Despite heterogeneous underlying aetiologies, all forms of PAH SHARE SIMILAR clinical and haemodynamic findings and identical pathological changes in the pulmonary vasculature.

FAILING RV IN PAH HOW TO MANAGE
• Vasoconstriction• Cell proliferation with in smooth muscle
cells and endothelial cell proliferation causing obstructive remodelling of the pulmonary blood vessal walls .
• Inflammation• In situ thrombosis
PATHOPHYSIOLOGY OF RV FAILURE

FAILING RV IN PAH HOW TO MANAGE
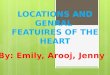
Figure 4. Postulated pathobiology of right ventricle failure in pulmonary hypertension.
Norbert F. Voelkel et al. Circulation. 2006;114:1883-1891
Copyright © American Heart Association, Inc. All rights reserved.

FAILING RV IN PAH HOW TO MANAGE
DETERMINANTS OF RV FUNCTION
RV SYSTOLIC FUNCTION IS A REFLECTION OF
Contractility Afterload Preload.

FAILING RV IN PAH HOW TO MANAGE
• HEART RHYTHM, • SYNCHRONY OF VENTRICULAR
CONTRACTION, • RV FORCE INTERVAL RELATIONSHIP &• VENTRICULAR INTERDEPENDENCE
RV PERFORMANCE influenced
by :

FAILING RV IN PAH HOW TO MANAGE
• Intravascular volume status, • Ventricular relaxation,• Chamber compliance, • Heart rate• Passive and active atrial characteristics,• LV filling,• Pericardial constraint & the filling period.
Factors influencin
g RV FILLING

FAILING RV IN PAH HOW TO MANAGE
Assessment of RV structure
• A change in RV shape and volume can be the FIRST SIGN of RV dysfunction, pressure or volume overload.

FAILING RV IN PAH HOW TO MANAGE
Assessment of RV Function
ECHO
RADIONUCLEOTIDE ANGIOGRAPHYMRI

FAILING RV IN PAH HOW TO MANAGE
RV contractility most commonly assessed : RVEF• highly dependent on loading conditions and • may not adequately reflect contractility.
• MRI : most accurate method for measuring RVEF
• Radionuclide angiography : gives RVEF free of geometric assumptions.
• 3D echo has also shown promising but variable correlations with RVEF.

FAILING RV IN PAH HOW TO MANAGE
ECHO: for RV Function
• 2D-RVEF : (SIMPSON METHOD) show moderate correlation with radionuclide /MRI-derived RVEF (correlations 0.65-0.80)
• RV fractional area change : the ratio of systolic area change to diastolic RV area.(n>32%), good correlation with RVEF

FAILING RV IN PAH HOW TO MANAGE
Tricuspid annular plane systolic excursion (TAPSE)
Longitudinal M mode systolic excursion of the lateral tricuspid valve annulus toward the apex in A4C view

FAILING RV IN PAH HOW TO MANAGE
RV myocardial performance index ( MPI )Ratio of isovolumic time intervals to ventricular ejection time.
Tei C et al, JASE 1996

FAILING RV IN PAH HOW TO MANAGE
RV pressure overload• Dilated pulmonary artery • RV enlargement ( RV ~2/3 of LV & doesn't form apex)• RV hypertrophy (RV free wall > 0.5 cm) • Decreased RV systolic function• Right atrial enlargement• Interventricular septal flattening (D-shaped LV)Rapid early systolic correction of diastolic septal flattening suggests RV volume overload, whereas failure of this suggests RV pressure overload

FAILING RV IN PAH HOW TO MANAGE
Eccentricity Index
A measure of septal displacement in systole or diastole
• Eccentricity Index EI = D2/D1
D1= minor axis diameter perpendicular to IVS
D2= minor axis diameter parallel to IVS
Ryan, T. et al. J Am Coll Cardiol 1985;5: 918-24

FAILING RV IN PAH HOW TO MANAGE
Doppler findings of increased Right sided pressure
• Best validated Doppler technique for PASP is - modified Bernoulli equation
ΔP = 4 TR Vmax2 • Change in RVOT Doppler velocity curve from rounded to rapid
acceleration• Short RVOT Doppler time of onset to peak velocity ( PAT< 90 ms)

FAILING RV IN PAH HOW TO MANAGE
OTHER TDI METHODS• Systolic signal of the tricuspid annulus (St) <11.5 cm/s identifies presence of
RV dysfunction with a sensitivity and specificity of 90% and 85%
• IVA( isovolumic myocardial accelaration ) : new TDI parameter of systolic performance calculated by dividing the maximal isovolumic myocardial velocity by the time to peak velocity

FAILING RV IN PAH HOW TO MANAGE
RV Diastolic Parameters and Estimation of Preload
The different parameters used include (1) RV end-diastolic or RA pressures, (2) RV volumes, (3) RV filling profiles.
2D-ECHO findings of elevated RAP• Enlarged RA & coronary sinus• Leftward bowing of IAS• Enlarged IVC (> 20 mm) with <50% diameter change with
inspiration (caval respiratory index)

FAILING RV IN PAH HOW TO MANAGE
Mean RAP (mmHg) IVC ∅ (mm) IVC Collapse 0 – 5 < 15 Complete5 – 10 15 – 25 > 50%10 – 15 15 – 25 < 50 %15 – 20 > 25 < 50 % > 20 >25 No change
Ommen SR. et al. Clin Proc 2000;75: 24-9.

FAILING RV IN PAH HOW TO MANAGE
Doppler findings of elevated RAP
Short RV rIVRT <60 ms
Tricuspid E/Ea >6 suggests mean RAP>10

FAILING RV IN PAH HOW TO MANAGE
ECHO ESTIMATION OF PVR
PVR = 10 x (TR Vmax m/s/ RVOT-VTI cm) + 0.16 wood units i.e. PVR TR VMAX/RVOTVTI∝
Abbas AE. et al. J Am Coll Cardiol 2003;41:1021-1027.

FAILING RV IN PAH HOW TO MANAGE
PREDICTORS OF RV FUNCTION IN 2D ECHO

FAILING RV IN PAH HOW TO MANAGE
Biomarkers of RV Failure
• BNP : useful in diagnosing RV failure associated with pulmonary hypertension & associated with worse survival.
• Elevated TROPONIN Levels have also been associated with worse outcome in pulmonary embolism and PAH.

FAILING RV IN PAH HOW TO MANAGE
MANAGEMENT OF Chronic and Acute RV Failure in PAH

FAILING RV IN PAH HOW TO MANAGE
GENERAL &SUPPORTIVE• DIEURETICS• DIGOXIN• ANTICOAGULATION
AFTERLOAD REDUCTION• PDE5 INHIBITORS• PROSTANOIDS• ENDOTHELIN
RECEPTOR ANTAGONIST
PREPARE FOR TRANSPLANTATION

FAILING RV IN PAH HOW TO MANAGE

FAILING RV IN PAH HOW TO MANAGE
Goals of Therapy
The goals of treating chronic right ventricular failure due to PAH are to
• 1) Relieve Symptoms, Improve Exercise Capacity, And Quality Of Life; • 2) Reduce Morbidity And Mortality • 3) Improve Cardiopulmonary Hemodynamics To Prevent Worsening
Of Right Heart Failure & Delay Disease Progression.

FAILING RV IN PAH HOW TO MANAGE
Acute Decompensated RV Failure
• The immediate goals of treating acute decompensated right ventricular failure (ADRVF), especially with hemodynamic compromise, are to
• 1) Restore Oxygenation;• 2) Treat Volume Overload; And • 3) Restore Vital Organ Perfusion.

FAILING RV IN PAH HOW TO MANAGE
ADRVF: Identification and Correction of Precipitating Factors
• Factors That Precipitate ADRVF In Patients With Chronic Right Ventricular Failure Are
• Dietary Indiscretion, • Intercurrent Infection, • Anemia/Erythrocytosis, • Thyroid Disorders, • Concomitant Pulmonary Embolus, And• Dysrhythmias. • Infection Must Be Considered In Patients With An Indwelling Central Venous
Catheter For Epoprostenol Infusion

FAILING RV IN PAH HOW TO MANAGE
infection
• Infection is poorly tolerated in patients with right ventricular failure .• The increase in right ventricular work associated with reduction in
SVR will result in systemic hypotension. • In this scenario, beta- and alpha- agonists such as dopamine or
norepinephrine are indicated as initial therapy to stabilize hemodynamics.

FAILING RV IN PAH HOW TO MANAGE
In the acutely decompensated PAH,
• The Most Useful Agents1. Inhaled Nitric Oxide,2. Intravenous Or Inhaled Epoprostenol,3. Iloprost, And4. Inotropic Support

FAILING RV IN PAH HOW TO MANAGE

FAILING RV IN PAH HOW TO MANAGE
Strategies
• To Prevent And Treat Chronic Right Ventricular Failure Are Aimed At
1. Reducing Right Ventricular Wall Stress,
2. Minimizing Myocardial Oxygen Consumption And Ischemia,
3. To Improve The Inotropic State Of The Right Ventricle.

FAILING RV IN PAH HOW TO MANAGE
Reduce wall stress
• Lower right ventricular afterload with chronic pulmonary arterial vasodilators:
1. O2 therapy,2. Endothelin receptor antagonists,3. Prostanoids4. Phosphodiesterase V inhibitors • Calcium channel blockers should be avoided in patients with marginal
blood pressure and• significant right heart failure right atrial pressures greater than15
mmHg and low cardiac index (less than 2.0 L/min/m2).

FAILING RV IN PAH HOW TO MANAGE

FAILING RV IN PAH HOW TO MANAGE
Combination therapy
• Describes the simultaneous use of more than one PAH-specific class of drugs, e.g. ERAS, PHOSPHODIESTERASE TYPE-5 INHIBITORS, PROSTANOIDS, AND NOVEL SUBSTANCES.
• Standard of care in many PAH centres.

FAILING RV IN PAH HOW TO MANAGE

FAILING RV IN PAH HOW TO MANAGE

FAILING RV IN PAH HOW TO MANAGE
The Relatively Small BREATHE-2 Study Showed A Trend To A Better Haemodynamic Effect Of The Initial Combination Of Epoprostenol-bosentan As Compared To Epoprostenol Alone.
The STEP-1 Study Addressed The Safety And Efficacy Of 12 Weeks Therapy With Inhaled Iloprost In Addition To Bosentan And Found A Marginal Increase In The Post-inhalation 6 Min Walk Distance.

FAILING RV IN PAH HOW TO MANAGE
Chronic anticoagulation
• Recommended To Prevent Pulmonary Arterial Thrombosis In Situ, • Which Contributes To Narrowing And Remodeling Of The Pulmonary
Arterial Bed,• Consequently Increasing Right Ventricular Outflow Impedance.

FAILING RV IN PAH HOW TO MANAGE
Preload optimisation
• Challenging :• May Differ In The Acute And Chronic Settings.
• Excessive volume loading may increase pericardial constraint and decrease LV preload and cardiac output through the mechanism of ventricular interdependence.
• Hypovolemia decrease RV preload and cardiac output.• Reduction in right ventricular preload and tricuspid regurgitation to reduce
right ventricular wall stress can be accomplished with diuretics.

FAILING RV IN PAH HOW TO MANAGE
Preload optimisation
• Chronic therapy with loop diuretics (furosemide, bumetanide, torsemide) alone or in combination with intermittent potent thiazide diuretics (ie, metolazone) and/or aldosterone antagonists (spironolactone, eplerenone) are effective at controlling volume overload.
• Right ventricular failure and hepatic congestion are associated with aldosterone activation. Use of aldosterone antagonists in appropriate doses and with close monitoring of electrolytes can potentiate diuresis in patients treated with loop diuretics.

FAILING RV IN PAH HOW TO MANAGE
• As aldosterone activation is associated with sodium/fluid retention, potassium/ magnesium wasting, increases in ventricular mass and fibrosis, and endothelial dysfunction, even nondiuretic neurohormonal blocking doses of the aldosterone antagonists (spironolactone or eplerenone at 12.5 to 50 mg daily) often exert beneficial effects in patients with right ventricular failure due to PAH.

FAILING RV IN PAH HOW TO MANAGE
Diuretics
• Although there are no RCTs of diuretics in PAH, clinical experience
shows clear symptomatic benefit in fluid-overloaded patients treated
with this therapy
• The addition of aldosterone antagonists should also be considered

FAILING RV IN PAH HOW TO MANAGE
alternative strategy
• When attempts to decrease right ventricular wall stress by pharmacologically manipulating right ventricular preload and afterload are inadequate, an alternative strategy is to improve right ventricular inotropy.

FAILING RV IN PAH HOW TO MANAGE
Contractility enhancemnt
• Dobutamine is the most commonly used inotrope in RV failure.
• The combination of dobutamine and nitric oxide in PH also has been shown to be beneficial. Vizza CD, Crit Care. 2001;5:355–361.
• Other inotropes used are dopamine, milrinone & digoxin.• Digoxin can produce a modest increase in cardiac output and it has
been shown to decrease circulating catecholamine levels.

FAILING RV IN PAH HOW TO MANAGE
DIGOXIN
• Digoxin has been shown to improve cardiac output acutely in IPAH
• It may be given to slow ventricular rate in patients with PAH who develop atrial
tachyarrhythmias.

FAILING RV IN PAH HOW TO MANAGE

FAILING RV IN PAH HOW TO MANAGE
Neurohormonal Modulation
• ACE-I & Beta blockers• In patients with biventricular failure, ACE-I have been shown to
increase RVEF and to reduce RVED volume and filling pressures. Massie B et al :Circulation. 1982;65:1374 –1381.
• Small studies have demonstrated that carvedilol or bisoprolol improves RV systolic function
Quaife RA et al :Am J Cardiol. 1998;81:247–250.
• The role of nesiritide is still not defined.

FAILING RV IN PAH HOW TO MANAGE
Atrial Septostomy
• It was first proposed by RICH and LAM in 1983 as palliative treatment of pulmonary hypertension
Current indications for BAS in PAH
1. Failure Of Medical Therapy 2. Persisting Right Heart Failure 3. Recurrent Syncope4. Bridging To Transplantation5. Absence Of Other Therapeutic Options

FAILING RV IN PAH HOW TO MANAGE
Hemodynamic impact of BAS in PAH
• Mean RA pressure falls at least 5mmhg • PA pressure - no significant impact expected• Tricuspid regurgitation regresses• Marginal reduction of RA,RV sizes • Cardiac output increases by 750 ml to 1 litre• Fall of systemic saturation should not be more than
10%

FAILING RV IN PAH HOW TO MANAGE
Follow up following BAS in PAH
• Greatest relief is from syncope.• Functional class improvement in >50% .• One year survival benefit is substantial (75-90%) • Late deterioration can occur as ASD gets closed in few cases

FAILING RV IN PAH HOW TO MANAGE
GOAL OF BALOON ATRIAL SEPTOSTOMY
• Goal of procedure is palliation and restoration of clinical stability until a transplant can be performed .
• Reported success rates for bridging patients to transplantation with septostomy range from 30- 40 %.
• Procedural mortality is around 15 %

FAILING RV IN PAH HOW TO MANAGE
Contraindications to BAS in PPH • Critical RV failure – BAS is not a procedure for dying
patients of PAH
• Mean RA pressure > 20mmhg
• Pulmonary vascular resistance index> 55 Wood units / sq.meter

FAILING RV IN PAH HOW TO MANAGE
iabp
• CIRCULATION

FAILING RV IN PAH HOW TO MANAGE
RV Assist Device
In patients with acute RVF refractory to medical treatment, mechanical support with an RV assist device may be used as
1. bridge to transplantation 2. Destination therapy

FAILING RV IN PAH HOW TO MANAGE
RV Assist Device

FAILING RV IN PAH HOW TO MANAGE
ecmo
• Venovenous Extracorporeal Membrane Oxygenation In patients with large PFO or ASD
• Venoarterial ECMO• Pulmonary Artery to Left Atrium ECLS

FAILING RV IN PAH HOW TO MANAGE
HEART LUNG TRANSPLANTATION
• NORMAN SHUMWAY , JOHN WALLWORK , BRUCE REITZ • in 1981 did first successful heart lung transplantation.
• JOEL COOPER reported first single lung transplant in pulmonary fibrosis 1986

FAILING RV IN PAH HOW TO MANAGE
• WHO functional class III & IV• Mean right atrial pressure >10 mm of hg• Mean PAP more than 50mm of hg• Cardiac index <2.5L/min/m2• Failure to improve despite maximal
medical therapy• Rapidly progressive disease
Guidelines to refer a
patient for transplant EVALUATIO
N

FAILING RV IN PAH HOW TO MANAGE
Single lung transplant
• ADVANTAGEOUS• Favourable in older patients and those with comorbidities due to
shorter time under anesthesia• Native lung may help patient sustain through early graft reaction• Two patients can be helped with single donar
• DISADVANTAGES• Monitoring of PFT in COPD will be unreliable

FAILING RV IN PAH HOW TO MANAGE
DOUBLE LUNG TRANSPLANT
• Survival is increased• Post transplant PFT monitoring is easy
• Longer duration of anesthesia increases risk

FAILING RV IN PAH HOW TO MANAGE
HEART LUNG TRANSPLANTATION
• ADVANTAGES• Patients with RV & LV dysfunction will not benefit from single or
double lung transplant
• DISADVANTAGES• Long waiting period• Poor survival

FAILING RV IN PAH HOW TO MANAGE
CONCLUSION
• RV physiology & function are different from LV• PAH with RV failure has worst prognosis and difficult to
manage• ECHO with Doppler & TDI is now the mainstay of routine RV
assessment• No convencing evidence to treat NYHA class I • Combination therapy is the standard of care in NYHA class II
& III .BREATHE 2 &STEP1 showed a trend to better hemodynamic effect

FAILING RV IN PAH HOW TO MANAGE
Be polite to your teacher even you are
smarter