Embed Size (px)
Citation preview

REFERENCES
SUMMARYThe current widespread usage of whole body 18F-FDG PET and 18F-FDG PET-CT studies as a screening tool for evaluation of malignant tumors has resulted in an increase in the detection of incidentally found thyroid lesions. Multiple studies have demonstrated that the prevalence of focal thyroid lesions incidentally found on 18F-FDG PET-CT ranges from 2.2-3.7% and that when tissue is obtained, cancer is identified from 14-47%. A small percentage of cancers may be secondary to metastatic lesions to the thyroid. Diffuse thyroid uptake in most instances is non-malignant. The role of SUV in determining malignancy is variable because papillary carcinoma may present with lower SUV levels and several benign thyroid lesions, such as Hürthle cell adenomas, may present with elevated SUV. Nevertheless, the consensus amongst most investigators is that histological analysis of a thyroid nodule with focal 18F-FDG uptake is of utmost importance to determine benign versus malignant etiologies of incidental thyroid lesions.
INTRODUCTION
Significance of Incidental FDG Thyroid Uptake: An Educational Exhibit. Garcia C1, Schneider M1, Van Nostrand D1, Burman K1, Wartofsky L1.
1Washington Hospital Center, Division of Nuclear Medicine
The current widespread usage of whole-body Fluorine-18 fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) studies in the evaluation of malignant tumors has resulted in an increase in the detection of incidentally found thyroid lesions. Multiple reports have documented these lesions which may be found in up to 50% of patients.1,2,3,4 When detected by 18F-FDG PET, they warrant a higher degree of suspicion than lesions detected by sonogram or CT alone.5,6,7 It is hypothesized that FDG-avid thyroid carcinomas are less well-differentiated, possess more aggressive histological features, and behave more aggressively. Incidental abnormalities of the thyroid gland are encountered at a rate of 16% on cross-sectional imaging, 27% on ultrasonography, and in 9.4% of carotid duplex scans.6,8 Ultrasound can detect 40% more nodules than CT, and unlike CT, can provide characterization of thyroid nodule features which may help determine the risk of malignancy. 9,10,11 Unlike sonography and CT imaging, 18F-FDG PET provides information about tumor location, biologic activity (Standard Uptake Value – SUV), and potential for aggressive behavior in patients with incidental thyroid lesions.11,12,13 Several authors report that elevated SUVs are associated with increased likelihood of thyroid malignancy, although the role of SUV in determining thyroid malignancy is variable. Several benign thyroid lesions, such as Hurthle cell adenomas, may present with elevated SUV, and primary thyroid tumors such as papillary carcinoma may present with lower SUV levels. The objective of this exhibit is to review the 18F-FDG PET and PET-CT detection of incidental uptake in the thyroid, the patterns of 18F-FDG PET uptake, the significance of the standard uptake value (SUV), and the management of 18F-FDG-PET incidental thyroid lesions.
THYROID FDG UPTAKE PATTERNS
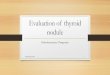
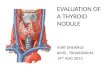
Chena et al.14 described two rare cases of diffuse 18F-FDG uptake in the thyroid that were related to malignancy; one case harbored a papillary carcinoma associated with Hashimoto’s thyroiditis, and the other case was a lung cancer metastasis. Although the rate of malignancy is very low in a diffuse goiter, one must always consider that a diffuse 18F-FDG uptake such as secondary to chronic thyroiditis could still obscure a thyroid nodule with focal 18F-FDG uptake.15 Focal thyroidal 18F-FDG uptake is not likely to be misinterpreted as adjacent nodal uptake or physiological activity when concurrent CT images are used. (see Figure 3).16,17
INCIDENTAL THYROID UPTAKE-SUVSeveral authors report that elevated SUVs are associated with increased likelihood of thyroid malignancy (Table 2), although this is controversial. The reasons for discrepancy are not entirely clear, but several areas have been analyzed: 1. The higher levels of 18F-FDG uptake do not necessarily imply malignancy - Hürthle cell adenomas may have an average SUV >5.20; 2. partial volume effects may underestimate SUV levels as seen in some papillary thyroid carcinomas; 3. TSH stimulates 18F-FDG uptake by differentiated thyroid carcinoma – increased SUV values and tumor to background ratios. The presence of any 18F-FDG uptake on PET scan, particularly focal, seems to be more important in terms of clinical decision making than the SUV level, but a histological diagnosis cannot be replaced or excluded to establish the true benign or malignant nature of a thyroid lesion.
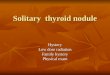
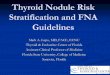
Fig. 1: Normal thyroid 18F-FDG uptake. Faintly visualized activity throughout both thyroid lobes with no regions of abnormal focal increased metabolic activity.
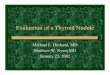
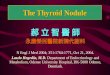
Fig. 2: Diffuse thyroid 18F-FDG PET uptake. Diffuse intense hypermetabolic activity seen throughout both thyroid lobes with no focal lesions.
Fig. 3: Focal thyroid 18F-FDG PET uptake. Thyroid Incidentaloma located in the mid-portion of the left thyroid lobe.
The normal thyroid gland typically has very low-grade or no uptake on an 18F-FDG PET scan (Fig. 1), and it is typically diffuse in nature. Bilateral, increased, diffuse 18F-FDG activity in the thyroid (Fig. 2) has been associated with chronic thyroiditis, Graves’ disease, or a normal variant. Kang et al.11 reported that the risk of malignancy is extremely low in patients with diffuse or bilateral uptake (1.4%). Are et al.12 reported that only 2 out of 162 patients with diffuse thyroid uptake harbored malignancy at a rate of 1.4%.
Table 3. Correlation of SUV and Incidental Thyroid Lesions Detected by 18F-FDG PET Imaging
Numerous guidelines exist that indicate the appropriate management of palpable thyroid nodules,26,27 but there are no accepted guidelines for incidental PET thyroid lesions,2,28,29despite their high prevalence of malignancy once tissue diagnosis has been established.12 The ATA and NCCN guidelines suggest observation and follow up for benign FNA results, and if nodule growth is observed, repeat FNA or surgical consideration is recommended; whereas other investigators suggest a hemithyroidectomy with intraoperative frozen section, and completion thyroidectomy if malignant results are observed.28 The 2011 ATA guidelines also state that in microcarcinomas (<1cm), a total thyroidectomy may not be necessary, advocating observation with regular ultrasound surveillance as primary management, even though most would perform surgical resection.30
INCIDENTAL LESION MANAGEMENT
THYROID FDG PATTERNS (cont…)
Abnormal focal uptake of 18F-FDG in the thyroid on PET or PET-CT has been reported in multiple series 16,17,21(see Table 1), demonstrating a low prevalence of 18F-FDG PET positive focal lesions, but a high prevalence of malignancy in patients with a tissue diagnosis.12,13,27,28,29 Not all focal 18F-FDG uptake found within the thyroid gland is related to a primary thyroid malignancy. Cancer metastasis to the thyroid gland is rare, accounting for 1.4 - 3% of thyroid malignancies.25 Data from autopsy series show that most metastatic disease in the thyroid originates from breast, melanoma and lung cancers, with lung neoplasms accounting for up to 43% of thyroid metastases.5,8,10,25
FREQUENCY OF INCIDENTAL LESIONS
Table 2. Incidence of Malignancy in Incidental Thyroid Lesions detected by 18F-FDG PET Imaging
PET
FUSEDCT
PET
FUSEDCT
PET
FUSEDCT
1. Mitchell J, Parangi S. The thyroid incidentaloma: an increasingly frequent consequence of radiologic imaging. Semin Ultrasound CT MR 2005; 26:37–46. Review.2. Gough J, Scott-Coombes D, Palazzo FF. Thyroid Incidentaloma: An Evidence-based Assessment of Management Strategy. World J Surg. 2008; 32:1264–1268.3. Van Den Bruel A, Maes A, De Potter T, Mortelmans L, Drijkoningen M, Van Damme B, Delaere P, Bouillon R. Clinical Relevance of Thyroid Fluorodeoxyglucose-Whole Body Positron Emission Tomography Incidentaloma. The Journal of Clinical Endocrinology & Metabolism. 2002; 87:1517–1520.4. Tan GH, Gharib H. Thyroid incidentalomas: management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann Intern Med. 1997; 126:226–231.5. Brander A,Viikinkoski P, Nickels J, Kivisaari L. Thyroid gland: US screening in a random adult population. Radiology. 1991; 181:683–687. 6. Youserm DM, Huang T, Loevner LA, Langlotz CP. Clinical and economic impact of incidental thyroid lesions found with CT and MR.AmJNeuroradiol.1997;18:1423–1428.7. Nishimori H, Tabah R, Hickeson M, How J. Incidental thyroid "PETomas": clinical significance and novel description of the self-resolving variant of focal thyroid uptake. Can J Surg. 2011; 54(2): 83-88.8. Steele SR, Martin MJ, Mullenix PS et al. The significance of incidental thyroid abnormalities identified during carotid duplex ultrasonography. Arch Surg. 2005; 140:981–985.9. Shetty SK, Maher MM, Hahn PF et al. Significance of incidental thyroid lesions detected on CT: correlation among CT, sonography, and pathology. AJR Am J Roentgenol. 2006; 187:1349–1356.10. Yi JG, Marom EM, Munden RF, Truong MT, Macapinlac HA, Gladish GW, Sabloff BS, Podoloff DA. Focal Uptake of Fluorodeoxyglucose by the Thyroid in Patients Undergoing Initial Disease Staging with Combined PET/CT for Non–Small Cell Lung Cancer. Radiology. 2005; 236:271–27511. Kang KW, Kim SK, Kang HS, et al. Prevalence and risk of cancer of focal thyroid incidentalomas identified by 18F-Fluorodeoxyglucose positron emission tomography for metastasis evaluation and cancer screening in healthy subjects. J Clin Endo Met. 2005; 88:4100–4104.12. Are C, Hsu JF, Schoder H, et al. FDG-PET detected thyroid incidentalomas: need for further investigation? Ann Surg Oncol. 2007; 14:239–247.13. Are C, Hsu JF, Ghossein RA, et al. Histological aggressiveness of fluorodeoxyglucose positron-emission tomogram (FDG-PET)-detected incidental thyroid carcinomas. Ann Surg Oncol. 2007; 14:3210–3215.14. Chena W, Parsonsa M, Torigiana DA, Zhuangb H, Alavi A. Evaluation of thyroid FDG uptake incidentally identified on FDG-PET/CT imaging. Nucl Med Commun. 2009; 30:240–244.15. Kim TY, Kim WB, Ryu JS, Gong G, Hong SJ, Shong YK. 18F-Fluorodeoxyglucose Uptake in Thyroid from Positron Emission Tomogram (PET) for Evaluation in Cancer Patients: High Prevalence of Malignancy in Thyroid PET Incidentaloma. Laryngoscope 2005; 115:1074–1078.16. Even-Sapir E, Lerman H, Gutman M, Lievshitz G, Zuriel L, Polliack A, et al. The presentation of malignant tumours and pre-malignant lesions incidentally found on PET-CT. Eur J Nucl Med Mol Imaging. 2006; 33:541–552.17. Bae JS, Chae BJ, Park WC, Kim JS, Kim SH, Jung SS, Song BJ. Incidental thyroid lesions detected by FDG-PET/CT: prevalence and risk of thyroid cancer. World Journal of Surgical Oncology. 2009; 7:63.18. Adler LP, Bloom AD. Positron emission tomography of thyroid masses. Thyroid. 1993; 3:195-200.19. Choi JY, Lee KS, Kwon OJ, et al. Improved detection of second primary cancer using integrated [18F] fluorodeoxyglucose positron emission tomography and computed tomography for initial tumor staging. J Clin Oncol. 2005; 23:7654–7659.20. Kresnik E, Gallowitsch HJ, Mikosch P, et al. Fluorine-18-fluorodeoxyglusocse positron emission tomography in the preoperative assessment of thyroid nodules in an endemic goiter area. Surgery. 2003; 133:294–299.21. Nakhjavani MK, Gharib H, Goellner JR, van Heerden JA. Metastasis to the thyroid gland: a report of 43 cases. Cancer. 1997; 79:574–578.22. Katz SC, Shaha A. PET-Associated Incidental Neoplasms of the Thyroid. J Am Coll Surg. 2008; 207:259–264.23. Ishimori T, Patel PV, Wahl RL. Detection of unexpected additional primary malignancies with PET/CT. J Nucl Med. 2005; 46:752–757.24. Ho TY, Liou MJ, Lin KJ, Yen TC. Prevalence and significance of thyroid uptake detected by (18)F-FDG PET. Endocrine (2011) 40:297–302.25. Chung AY, Tran TB, Brumund KT, Weisman RA, Bouvet M. Metastases to the Thyroid: A Review of the Literature from the Last Decade. Thyroid 2012; 22(3): 258-26826. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, Schlumberger M, Sherman SI, Steward DL, Tuttle RM. Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer The American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. Volume 19, Number 11, 2009.27. National Comprehensive Cancer Network (NCCN) Guidelines in Oncology. Thyroid Carcinoma. Version 3.2011.28. Eloy JA, Brett EM, Fatterpekar GM, Kostakoglu L, Som PM, Desai SC, Genden EM. The Significance and Management of Incidental [18F]Fluorodeoxyglucose–Positron-Emission Tomography Uptake in the Thyroid Gland in Patients with Cancer. AJNR Am J Neuroradiol. 2009; 30:1431–34.29. Deandreis D, Al Ghuzlan A, Auperin A, Vielh P, Caillou B, Chami L. Is 18F-Fluorodeoxyglucose-PET/CT Useful for Presurgical Characterization of Thyroid Nodules with Indeterminate Fine Needle Aspiration Cytology? Thyroid 2012; 22(2): 165-17230. Ito Y, Miyauchi A, Inoue H, et al. An observational trial for papillary thyroid microcarcinoma in Japanese patients. World J Surg. 2010; 34(1): 28-35.














![Approach to Thyroid Nodule[1]](https://img.pdfslide.net/doc/110x75/55286aea55034670588b47b5/approach-to-thyroid-nodule1.jpg)