Embed Size (px)
Citation preview

Febrile Seizure
Dr Mallikarjun DStudy Physician Dept Of Community MedicineKMC Manipal
Outline
Definitions Aetiology Classification Clinical presentation Treatment
Abnormal neuronal activity
A sudden biochemical imbalance at the cell membrane
Repeated abnormal electrical discharges
Seen clinically as changes in motor control, sensory perception and/or autonomic function
A Seizure Is:
Definition
Provoked seizures Seizures induced by somatic disorders
originating outside the brain E.g. fever, infection, syncope, head trauma,
hypoxia, toxins, cardiac arrhythmias
Definition
Epilepsy• Present when 2 or more unprovoked
seizures occur at an interval greater than 24 hours apart
Definition
Status epilepticus (SE) Continuous convulsion lasting longer than 30
minutes OR occurrence of serial convulsions between which there is no return of consciousness
Idiopathic SE Seizure develops in the absence of an underlying
CNS lesion/insult Symptomatic SE
Seizure occurs as a result of an underlying neurological disorder or a metabolic abnormality
Causes of seizures
Epileptic Idiopathic (70-80%) Cerebral tumor Neurodegenerative disorders Neurocutaneous syndromes Secondary to
Cerebral damage: e.g. congenital infections, HIE, intraventricular hemorrhage
Cerebral dysgenesis/malformation: e.g. hydrocephalus
Causes of seizures
Non-epileptic Febrile convulsions Metabolic
Hypoglycemia HypoCa, HypoMg, HyperNa, HypoNa
Head trauma Meningitis Encephalitis Poisons/toxins
Parents/caregivers may report seeing:
Repetitive non-purposeful movementsStaringRolling of Eye balls – Upwards Lip-smackingFalling down without causeStiffening of any or all extremitiesRhythmic shaking of any or all extremities
Clinical Presentation: Motor Changes
Parents/caregivers may report the child is:
Feeling nauseousFeeling odd or peculiarLosing control of bowel or bladderFeeling numbness, tinglingExperiencing odd smells or sounds
Clinical Presentation: Sensory and Autonomic
Consciousness is the usual alertness or responsiveness the child demonstrates.
Parents/caregivers may report or you may observe the child to have:Baseline alertness Diminished level of consciousnessUnresponsive and unconscious
Clinical Presentation:Consciousness
Apnea Breath Holding Dizziness Myoclonus Pseudoseizures Psychogenic Seizures
Rigors Syncope Transient Ischemic
Attacks
Clinical Presentation:Events That Mimic Seizures
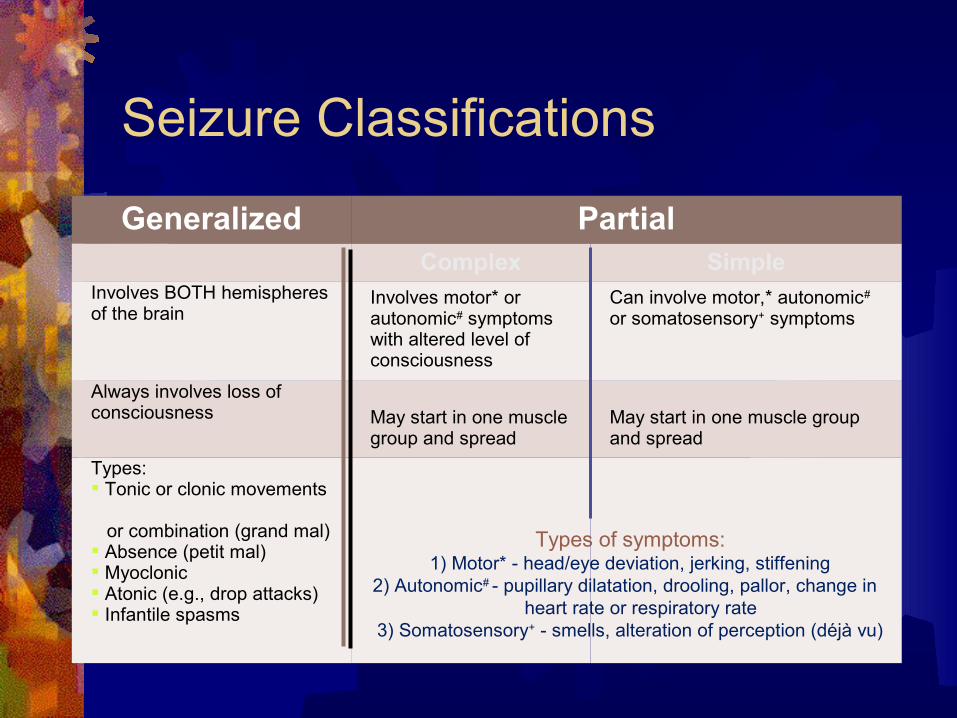
Seizure Classifications
Generalized PartialComplex Simple
Involves BOTH hemispheres of the brain
Involves motor* or autonomic# symptoms with altered level of consciousness
Can involve motor,* autonomic# or somatosensory+ symptoms
Always involves loss of consciousness May start in one muscle
group and spreadMay start in one muscle group and spread
Types: Tonic or clonic movements
or combination (grand mal) Absence (petit mal) Myoclonic Atonic (e.g., drop attacks) Infantile spasms
Types of symptoms:1) Motor* - head/eye deviation, jerking, stiffening
2) Autonomic# - pupillary dilatation, drooling, pallor, change in heart rate or respiratory rate
3) Somatosensory+ - smells, alteration of perception (déjà vu)

Febrile seizures are the most common seizure disorder in childhood, affecting 2 - 5% of children between the ages of
6 months and 5 years
Febrile Seizure5
Caused by the increase in the core body temperature greater than 100.4o F or 38o C
Threshold of temperature which may trigger seizures is unique to each individual
Can occur within the first 24 hours of an illnessCan be the first sign of illness in 25 - 50% of patients
Febrile Seizure6
Are benign
Occurrence: between 6 months to 5 years of age
May be either simple or complex type seizure
Seizure accompanied by fever (before, during or after) WITHOUT ANY Central nervous system infection Metabolic disturbance History of previous seizure disorder
Febrile Seizure: Characteristics
Simple Febrile
6 months – 5 years of age Febrile before, during or
after seizure Includes all of the following
Seizure lasting less than 15 minutes
Generalized seizure Occurs once in a 24-hour
period
Complex Febrile
6 months – 5 years of age Febrile before, during or
after seizure One or more of the
following Prolonged (lasting more
than 15 minutes) Focal seizure Occurs more than once in
24 hours
Febrile Seizure: Two Types5
Reassess temperature
Consider giving antipyretic if not previously administered
As source of fever is identified, treat appropriately
Simple Febrile Seizure:ED Ongoing Management
Here are some frequently asked questionsparents/caregivers may have prior to discharge:
Is my child brain damaged?There is no evidence of impact on learning abilities after seizure
from SFS.
Will this happen again?If child is under 12 months of age at time of first seizure,
recurrence rate is 50%If child is greater than 12 months of age at time of first seizure,
recurrence rate is 30%Most recurrences occur within 6-12 months of the initial febrile
seizure
Simple Febrile Seizure:Family Education5,7
Will my child get epilepsy?For simple febrile seizures, there is no increased risk of
epilepsy
Why not treat for possible seizures or fever?Anticonvulsants can reduce recurrence. However
potential side effects of medications outweigh the minor risk of recurrence
Prophylactic use of antipyretics does not have impact on recurrence
Simple Febrile Seizure:Family Education5,7 (cont.)
For complex febrile seizures, there is a slight increase in the risk of epilepsy.
For complex febrile seizures, there is a slight increase in the risk of epilepsy.
Instruct parent/caregivers to prevent injury during a seizure:
Position child while seizing in a side-lying position
Protect head from injuryLoosen tight clothing about the neck Prevent injury from fallsReassure child during eventDo not place anything in the child’s mouth
Simple Febrile Seizure:Family Education8 (cont.)
Prior to discharge home…
Educate regarding use of: ThermometerAntipyretics for fever managementWhen to contact 9-1-1 or ambulance
Identify a Primary Care Provider for follow-up appointment and stress importance of follow-up
Provide developmentally appropriate explanationof event for child and family members
Simple Febrile Seizure:Disposition