Embed Size (px)
Citation preview

Stressors AffectingFluid & Electrolyte Balance
NUR 101FALL 2008LECTURE # 15 & #16K. Burger, MSEd, MSN, RN, CNE

Body Fluids Water= most important nutrient for life. Water= primary body fluid.
Adult weight is 55-60% water. Loss of 10% body fluid = 8% weight loss SERIOUS Loss of 20% body fluid = 15% weight loss FATAL Fluid gained each day should = fluid lost each day
(2 -3L/day average) What is the minimum output per hour necessary to
maintain renal function? 30ml/hr

Functions of Body Fluid Medium for transport Needed for cellular metabolism Solvent for electrolytes and other
constituents Helps maintain body temperature Helps digestion and elimination Acts as a lubricant

Mechanisms of Fluid Gain and Loss
Gain Fluid intake 1500ml Food intake 1000ml Oxidation of
nutrients 300ml(10ml of H20 per 100 Kcal)
Loss “Sensible”
Can be seen.Urine 1500mlSweat 100ml
“Insensible”Not visible.Skin (evaporation) 500mlLungs 400mlFeces 200ml

Regulation of Fluids
Hypothalmus –thirst receptors (osmoreceptors) continuosly monitor serum osmolarity (concentration). If it rises, thirst mechanism is triggered.+Vasopressin (AKA ADH )– increasing H20 reabsorption
Pituitary regulation- posterior pituitary releases ADH (antidiuretic hormone) in response to increasing serum osmolarity. Causes renal tubules to retain H20.
Thirst is a late sign of water deficit

Regulation of Fluids (continued )
Renal regulation- Nephron receptors sense decreased pressure (low osmolarity) and kidney secretes RENIN. Renin – Angiotensin I – Angiotensin II
Angiotensin II causes Na and H20 retention by kidneys AND…..
Stimulates Adrenal Cortex to secrete Aldosterone which causes kidneys to excrete K and retain Na and H20.

Consider This…. The Geriatric Client
-normal physiological aging results in decreased thirst mechanism decreased # of sweat glands decreased renal function-there also may be decreased mobility and/or cognitive function which impacts their ability to get adequate fluid intake.

Variations in Body Fluids
Elderly: Have lower % of total body fluid than younger adults
Women: Have lower % total body fluid than men
WHY DO YOU THINK THIS IS ?????Muscle tissue has more H20 content THAN adipose
tissue

Fluid CompartmentsIntracellular
fluid (ICF) Fluid inside
the cell Most (2/3) of
the body’s H20 is in the ICF.
Extracellular Fluid (ECF)
Fluid outside the cell. 1/3 of body’s H20 More prone to loss 3 types:Interstitial- fluid
around/between cellsIntravascular-
(plasma) fluid in blood vessels
Transcellular –CSF, Synovial fluid etc

Consider this…. Age variations exist in regards to
H20 content of fluid compartments Infants =
60% of H20 is found in ECF40% of H20 is found in ICF
What might this mean in regards to fluid loss for an infant? Reverse of adults!
Infant MORE PRONE to fluid LOSS!

Fluid Balance Dynamic process Balance between body fluids
and electrolytes Attraction between ions
(electrolytes) and water (fluids) causes fluids to move across membranes and leave their compartments.

Solvent (H20) Movement
Cell membranes are semipermeable allowing water to pass through
Osmosis- major way fluids transported Water shifts from low solute concentration to high solute concentration to reach homeostasis (balance).

Osmolarity
Concentration of particles in solution The greater the concentration (Osmolarity) of a
solution, the greater the pulling force (Osmotic pressure)
Normal serum (blood) osmolarity = 280-295 mOSM/kg
A solution that has HIGH osmolarity is one that is > serum osmolarity = HYPERTONIC solution
A solution that has LOW osmolarity is one that is < serum osmolarity = HYPOTONIC solution
A solution that has equal osmolarity as serum = ISOTONIC solution

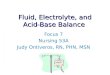
Hypertonic Fluids Hypertonic fluids have a higher
concentration of particles (high osmolality) than ICF
This higher osmotic pressure shifts fluid from the cells into the ECF
Therefore Cells placed in a hypertonic solution will shrink

Hypertonic Fluids
Used to temporarily treat hypovolemia Used to expand vascular volume Fosters normal BP and good urinary output
(often used post operatively) Monitor for hypervolemia !
Not used for renal or cardiac disease. THINK – Why not?
D5% 0.45% NS D5% NS D5% LR
Pulmonary Edema

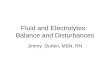
Hypotonic Fluids Hypotonic fluids have less
concentration of particles (low osmolality) than ICF
This low osmotic pressure shifts fluid from ECF into cells
Cells placed in a hypotonic solution will swell

Hypotonic Fluids Used to “dilute” plasma
particularly in hypernatremia Treats cellular dehydration Do not use for pts with increased
ICP risk or third spacing risk
0.45%NS 0.33%NS

Isotonic Fluid Isotonic fluids have the same
concentration of particles (osmolality) as ICF (275-295 mOsm/L)
Osmotic pressure is therefore the same inside & outside the cells
Cells neither shrink nor swell in an isotonic solution, they stay the same

Isotonic Fluid Expands both intracellular and
extracellular volume Used commonly for: excessive
vomiting,diarrhea 0.9% Normal saline D5W Ringer’s Lactate

Other Osmotic Factors ALBUMIN ( a serum protein ) Albumin in the serum has osmotic properties
called colloid pressure Albumin pulls H20 from the interstitial
compartments into the intravascular compartments (serum). Helps to maintain BP.
Persons with low serum albumin levels tend to retain fluid in their interstitial layers.
What abnormal assessments might you find in the client with low serum albumin levels?
Edema, hypotension

Hmmm……. What type of IV fluid
(hypotonic – isotonic – hypertonic)might be of benefit to this client with low albumin levels?

Consider this…. When tissue injury occurs, proteins
pathologically leak from the intravascular space into the intersititial space.Termed: Third spacing
This explains __________ as a sign of the inflammatory process.
EDEMA

Solute Movement - Diffusion
Movement of solutes from high concentration to low concentration
It is a PASSIVE movement DOWN the concentration gradiant. (requires no energy)
Many body processes use diffusion. Example: O2 and CO2 exchange
Rate is affected by: concentration gradiant, permeability-surface area-thickness of membranes, and size of particles. (Fick’s Law)

Solute Movement –other mechanisms
Active transport- requires energy (ATP) to move from low concentration to high concentration (uphill)Example: Na / K pump
May be enhanced by carrier molecules with binding sites on cell membraneExample: Glucose (Insulin promotes the insertion of binding sites for Glucose on cell membranes).

Filtration Solvent AND solute movement Passage from an area of High Pressure to an
area of Low Pressure Termed: Hydrostatic Pressure
Example:Arterioles have higher pressure than ICFFluid, oxygen and nutrients move into cellsVenules have lower pressure than ICFFluid, carbon dioxide and wastes move out of cells

Fluid volume deficit FVD (Hypovolemia) Loss of both H20 and
electrolytes from ECF. Causes include:
Increased output, Hemorrhage, vomiting, diarrhea, burns, OR
Fluid shift out of vascular space ( “third spacing” ) into interstitial spaces

Dehydration Isotonic dehydration = H20 &
electrolyte loss in equal amounts; diarrhea and vomiting
Hypertonic dehydration = H20 loss greater than electrolyte loss; excessive perspiration, diabetes insipidus

AssessmentFVD - Hypovolemia
Cardiovascular: Diminished peripheral pulses; quality 1+
(thready) Decreased BP & orthostatic hypotension Increased HR Flat neck & hand veins in dependent position Elevated Hematocrit (Hct)
Gastrointestinal: Thirst Decreased motility; diminished bowel sounds,
possible constipation

Assessment FVD – Hypovolemia (continued)
Neuromuscular: Decreased CNS activity
(lethargy to coma) Possible fever Skeletal muscle weakness Hyperactive DTRRenal: Decreased output Increased spec grav of
urine Weight loss Hypernatremia
Integumentary: Dry mouth & skin Poor turgor (tenting) Pitting edema Sunken eyeballs
Respiratory: Increased rate and depth

Nursing Diagnosis - FVD Deficient Fluid Volume
R/T loss of GI Fluids via vomitingAEB elevated Hct, dry mucous membranes, decreased output, thirst

Planning - FVD Client will demonstrate fluid
balance aeb moist mucous membranes, balanced I & O measurements, Hct WNL, by ….

Interventions for FVD - Hypovolemia
Prevent further fluid loss Oral rehydration therapy IV therapy Medications; antiemetics, antidiarrheals Monitor CV, Resp, Renal, GI status Monitor electrolytes – possible supplement rx MONITOR WEIGHT and I & O

NCLEX PracticeIntravenous fluids are ordered for your clientwho is experiencing diarrhea and vomiting for the past 2 days. Which IV solution would the nurse expect to see prescribed?a. D5NSb. 0.45%NSc. D51/2NSd. RL

Fluid Volume ExcessFVE - Hypervolemia
Fluid overload is an excess of body fluid - overhydration
Excess fluid volume in the intravascular area-hypervolemia
Excess fluid volume in interstitial spaces edema

Fluid Volume Excess Causes: Increased Na/H2O retention Excessive intake of Na (PO or IV) Excessive intake of H2O ( PO or IV)
(Water intoxication) Syndrome of inappropriate
antidiuretic hormone (SIADH) Renal failure, congestive heart failure

AssessmentFVE - Hypervolemia
CV: Elevated pulse; 4+ bounding, elevated BP, distended neck & hand veins, ventricular gallop (S3)Hyponatremia
Resp: Dyspnea, Moist Crackles,Tachypnea
Integumentary: Periorbital edemaPitting or Non-pitting edema
GI: Increased motilityStomach crampsNausea & Vomiting
Renal: Weight gainDecreased spec grav of urine
Neuromuscular: Altered LOC, headache, skeletal muscle twitching

Nursing Diagnosis - FVEFluid volume excess
R/T excessive H20 intake
AEB confusion, headache, muscle twitching, abdominal cramps, elevated BP and HR, hyponatremia.

Planning - FVE Client will demonstrate fluid
balance by balanced I & O measurements, Serum Na WNL, etc. by ….

Interventions FVE - Hypervolemia
Restore normal fluid balance, prevent further overload
Drug therapy; diuretics Diet therapy; decrease Na & fluids Monitor intake and output (I & O) Monitor weights Monitor electrolytes Monitor CV, Resp, Renal systems

Clinical Application You have been assigned to care for an 80y.o.
client admitted with hypernatremia that has an IV infusing 0.45% NS @ 100ml/hr via pump and an indwelling urinary catheter. At 11am you assess an output in the urinary drainage bag of 150ml dk amber urine. You also notice that the client is SOB while speaking on the phone to her daughter.
What do you think is happening?? What will you do??

SUMMARYWant more Information???
CHECK OUT THEWEBLINKS
For Chapter 41 on EVOLVE

Electrolytes Work with fluids to keep the body healthy
and in balance They are solutes that are found in
various concentrations and measured in terms of milliequivalent (mEq) units
Can be negatively charged (anions) or positively charged (cations)
For homeostasis body needs: Total body ANIONS = Total body CATIONS

ElectrolytesCations
Positively charged
Sodium Na+ Potassium K+ Calcium Ca++ Magnesium Mg++
AnionsNegatively charged
Chloride Cl- Phosphate PO4- Bicarbonate
HCO3-

Electrolyte Functions Regulate water distribution Muscle contraction Nerve impulse transmission Blood clotting Regulate enzyme reactions (ATP) Regulate acid-base balance

Sodium Na+ 135-145mEq/L Major Cation Chief electrolyte of the ECF Regulates volume of body fluids Needed for nerve impulse & muscle
fiber transmission (Na/K pump) Regulated by kidneys/ hormones

Hmmm…Hyper and Hypo Natremia are the most common electrolyte disturbances. Why do you think that is?
It is most abundant in the EXTRACELLULAR FLUID and therefore more prone to fluctuation.

Hyponatremia Serum Na+ <135mEq/L Results from excess of water or loss
of Na+ Water shifts from ECF into cells S/S: abd cramps, confusion, N/V,
H/A, pitting edema over sternum Tx: Diet/IV therapy/fluid restrictions

Lets think about …Hyponatremia
What are some medical conditions that may cause a dilutional hyponatremia?CHFRenal FailureSIADH ( Cancer, pituitary trauma )Addisons Disease ( hypoaldosteronism & Na loss )
What are some conditions that might cause actual loss of sodium from the body?GI losses – nasogastric suctioning, vomiting, diarrheaCertain diuretic therapies
Permanent neurological damage can occur when serum Na levels fall below 110 mEq/L. Why?Hypotonic environment swells cells, increasing ICP – brain damage

Hypernatremia Serum Na+> 145mEq/L Results from Na+ gained in excess of
H2O OR Water is lost in excess of Na+ Water shifts from cells to ECF S/S: thirst, dry mucous membranes &
lips, oliguria, increased temp & pulse,flushed skin,confusion
Tx: IV therapy/diet

Let’s think about….Hypernatremia
What are some medical conditions that may cause elevated serum Na?Renal failureDiabetes InsipidusDiabetes Mellitus ( hyperglycemic dehydration)Cushings syndrome (hyperaldosteronism)
What are some other patient populations at risk for hypernatremia?Elderly ( decreased thirst mechanism )Patient’s receiving:-tube feedings-corticosteroid drugs-certain diuretic therapies
Seizures, coma, death my result if hypernatremia is left untreated. Why?Cells loose fluid into the ECF causing irreversible cell damage.

Critical ThinkingHypo / Hyper Natremia
For the client experiencingFVE & hyponatremia d/texcessive intake of water, which IV solution would you expect the physician toorder?a. D5NS b. NSc. D5Wd. ½ NS
For the client experiencing
FVD and hypernatremia d/t excessive water loss, which IV solution would you expect the physician to order?a. D5 ½ NSb. D5RLc. D5Wd. ½ NS

Potassium K+ 3.5-5.0 mEq/L Chief electrolyte of ICF Major mineral in all cellular fluids Aids in muscle contraction, nerve &
electrical impulse conduction, regulates enzyme activity, regulates IC H20 content, assists in acid-base balance
Regulated by kidneys/ hormones Inversely proportional to Na

Hypokalemia Serum level < 3.5mEq/L Results from decreased intake, loss via
GI/Renal & potassium depleting diuretics Life threatening-all body systems affected S/S muscle weakness & leg cramps,
decreased GI motility, cardiac arrhythmias Tx: diet/supplements/IV therapy

Lets think about …Hypokalemia
What are some medical conditions that may cause a hypokalemia?Renal Disease / CHF (dilutional)Metabolic AlkalosisCushings Disease ( Na retention leads to K loss )
What are some conditions that might cause actual loss of potassium from the body?GI losses – nasogastric suctioning, vomiting, diarrheaCertain diuretic therapies Inadequate intake – ( body cannot conserve K, need PO intake)
Cardiac arrest may occur when serum K levels fall below 2.5 mEq/L. Why?Increased cardiac muscle irritability leads to PACs and PVCs, then AF

Hyperkalemia Serum level >5 mEq/L Results from excessive intake, trauma,
crush injuries, burns, renal failure S/S muscle weakness, cardiac
changes, N/V, parathesias of face/fingers/tongue
Tx:diet/meds/IV therapy/ possible dialysis

Lets think about …Hyperkalemia
What are some medical conditions that may cause hyperkalemia?Renal Disease=most common causeBurns and other major tissue traumaMetabolic Acidosis Addison’s Disease ( Na loss leads to K retention )
What are some conditions that might cause potassium levels to rise in the body?Certain diuretic therapies Excessive intake – ( inappropriate supplements)
Cardiac arrest may occur when serum K levels rise above mEq/L. Why?Decreased electrical impulse conduction leads to bradycardia and eventual asystole.

Critical ThinkingPotassium IV additives
Which of the following interventions will thenurse undertake when administeringparenteral K additives?Monitor the IV site for phlebitisPlace on cardiac monitor if > 10 mEqAssure of adequate mixing of K in solutionMonitor for elevated K levelsMonitor for decreased Na levelsAdminister potassium by slow IV push method
NEVER!!!

Calcium Ca++ 4.5-5.5mEq/L Most abundant in body but:
99% in teeth and bones Needed for nerve transmission,
vitamin B12 absorption, muscle contraction & blood clotting
Inverse relationship with Phosphorus Vitamin D needed for Ca absorption

Hypocalcemia Serum Ca < 4.3mEq/L Results from low intake, loop
diuretics, parathyroid disorders, renal failure
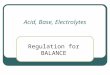
S/S osteomalacia, EKG changes, numbness/tingling in fingers, muscle cramps / tetany, seizures, Chovstek Sign & Trousseau Sign
Tx: diet/IV therapy

Chovstek Trousseau

Lets think about …Hypocalcemia
What are some medical conditions that may cause hypocalcemia?Hypoparathyroidism (low PTH levels = decreased release of Ca from bones)S/P thryoid surgery ( low Calcitonin = decreased release of Ca from bones) Acute pancreatitisCrohns DiseaseHyperphosphatemia ( ESRF)
What are some other conditions that might cause low Ca? GI losses – nasogastric suctioning, vomiting, diarrheaLong term immobilization Lactose intolerance
If hypocalcemia is prolonged, the body will utilize stored Ca from bones.What complication might arise?Fractures ( late sign )

Hypercalcemia Serum Ca > 5.3mEq/L Results from hyperparathyroidism,
some cancers, prolonged immobilization
S/S muscle weakness, renal calculi, fatigue, altered LOC, decreased GI motility, cardiac changes
Tx: medication/ IV therapy

Lets think about …Hypercalcemia
What are some medical conditions that may cause hypercalcemia?Hyperparathyroidism (high PTH levels = increased release of Ca from bones)Paget’s DiseaseSome Cancers – Multiple MyleomaChronic Alcoholism ( with low serum phosphorus )
What are some other conditions that might cause low Ca? Excessive intake of Ca OR Vitamin DExcessive intake of OTC antacids
If hypercalcemia is uncorrected, AV block and cardiac arrest may occur.

Magnesium Mg2+ 1.5-2.5mEq/L Most located within ICF Needed for activating enzymes,
electrical activity, metabolism of carbs/proteins, DNA synthesis
Regulated by intestinal absorption and kidney

Hypomagnesemia Serum < 1.5mEq/L Results from decreased intake, prolonged
NPO status, chronic alcoholism & nasogastric suctioning
S/S: muscle weakness, cardiac changes, mental changes, hyperactive reflexes & other hypocalcemia S/S.
Tx: replacement IV therapy restore normal Ca levels ( Mg mimics Ca) seizure precautions

Hypomagnesemia
Common in critically ill patients Associated with high mortality rates Increases cardiac irritability and
ventricular dysrhythmias - especially in patients with recent MI
Maintenance of adequate serum Mg has been shown to reduce mortality rates post MI

Hypermagnesemia Serum>2.5mEq/L Results from renal failure,
increased intake S/S: flushing, lethargy, cardiac
changes (decreased HR),decreased resp, loss of deep tendon reflexes
Tx: restrict intake diuretic rx

Chloride Cl- 95-105mEq/L Most abundant anion in ECF Combines with Na to form salts Maintains water balance, acid-base
balance, aids in digestion (hydrochoric acid) & osmotic pressure (with Na and H20)
Regulated by kidneys Follows Sodium (Na)

Hypochloremia Serum level 96mEq/L Results from prolonged vomiting &
suctioning S/S metabolic alkalosis, nerve
excitability, muscle cramps, twitching, hypoventilation, decreased BP if severe
Tx: diet/IV therapy

Hyperchloremia Serum level > 106mEq/L Results from excessive intake or
retention by kidneys – metabolic acidosis
S/S Arrhythmias, decreased cardiac output, muscle weakness, LOC changes, Kussmauls’s respirations
Tx: restore fluid & electrolyte balance

Phosphate PO4- 2.5-4.5mg/dl Needed for acid-base
balance,neurological & muscle function, energy transfer ATP & affects metabolism of carbs/proteins/lipids, B vitamin synthesis
Found in the bones Regulated by intake and kidneys Inversely proportional to Calcium
Therefore some regulation by PTH as well

Hypophosphatemia Serum level < 1.8mEq/L Results from decreased intestinal
absorption and increased excretion
S/S bone & muscle pain, mental changes, chest pain, resp. failure
Tx: Diet/ IV therapy

Hyperphosphatemia Serum level> 2.6mEq/L Results from renal failure, low intake of
calcium S/S: neuromuscular changes (tetany),
EKG changes, parathesia-fingertips/mouth Tx: Diet; hypocalcemic interventions
Medications: phosphate binding The body can tolerate hyperphosphatemia
fairly well BUT the accompanying hypocalcemia is a larger problem!

Critical Thinking - NCLEX The nurse is caring for a client with
renal failure whose magnesium level is 3.6 mg/dL. Which of the following signs would the nurse most likely expect to note in the client based on this Mg level?
a. Twitchingb. Hyperactive reflexesc. Irritabilityd. Loss of deep tendon reflexes

Electrolyte homeostasis This means to maintain
balance… to control by balancing the dietary intake of electrolytes with the renal excretion and reabsorption of electrolytes

Interventions for F/E balance
Assess patient carefully- note changes
Monitor I & O (Intake & Output) Monitor weight changes Monitor urine Monitor vs Monitor lab results and dx test Maintain proper IV therapy

Summary Fluid compartments in the body must
balance Body systems regulate F&E balance Assessment of body fluid is important
to determine causes of imbalance Interventions for imbalances are
based on the cause