Embed Size (px)
Citation preview

Fluid therapy in Paediatrics
Prepared by:
Ali Mazin
Saad Izzat
Supervised by : Dr.Ban

Composition of body fluids
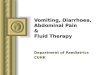
Total Body Water Water is the most plentiful constituent of the human body. Total body water (TBW) as a percentage of body weight varies with age (Figure 1). The fetus has a very high TBW, which gradually decreases to about 75% of birth weight
for a term infant. Premature infants have a higher TBW content than term infants. During the 1st year of
life, TBW decreases to about 60% of body weight and basically remains at this level until puberty, by the end of puberty TBW in boys remain at 60%, but TBW in girls decreases to about 50% of body weight, due to difference in body fat content.
The high fat content in overweight children leads to decrease in TBW as a percentage of body weight.
During dehydration the TBW decreases and, thus, is a smaller percentage of body weight

Figure 1: total body weight according to the age

Fluid Compartments TBW is divided between two main compartments: intracellular fluid (ICF)
and extracellular fluid (ECF). In the fetus and newborn, the ECF volume is larger than the ICF volume. By 1 year of age the ratio of the ICF volume to the ECF volume approaches
adult levels. The ECF volume is about 20-25% of body weight and the ICF volume is
about 30-40% of body weight, close to twice the ECF volume. The ECF is further divided into the plasma water and the interstitial fluid. The volume of plasma water can be altered by a variety of pathologic
conditions, including dehydration, anemia, polycythemia, heart failure, abnormal plasma osmolality, and hypoalbuminemia.
The interstitial fluid, normally about 15% of body weight, can increase dramatically in diseases associated with edema such as heart failure, liver failure, nephrotic syndrome, and other causes of hypoalbuminemia.

Electrolytes compositions

Fluid therapy Fluid therapy is used to correct body water and electrolytes disturbance, to restore and
maintain blood volume, osmolality, pH and electrolyte composition and to restore normal physiological function.

Types of fluid therapy:
1- Oral fluid therapy (oral rehydration solution) Glucose-based ORS Cereal -based ORS
2- Intravenous fluid therapy Crystalloids
Colloids

Oral fluid therapy (oral rehydration solution)
Glucose-based ORS Composition: According to WHO formula: Glucose:13.5-20 g NaCl : (2.6) 3.5 g KCl :1.5 g Na citrate (Bi) : 2.9 g Water 1 liter Indications:
1. Diarrhea and dehydration especially in infants and old age.
2. All cases of loss of body fluids in non-comatosed patients (Moderate dehydration & Acidosis)

Oral fluid therapy (oral rehydration solution)
Contraindications:
1. Coma
2. Severe uncontrolled vomiting.
3. Severe cases of dehydration that need IV therapy.
Advantages:
1. Effective in dehydration, preventing shock and even improving vomiting.
2. Less expensive than IV fluids
3. Easy; No need for expertise
4. Easily prepared
5. No need for sterilization
6. Given orally
7. No significant difference between IV & oral rehydration

Oral fluid therapy (oral rehydration solution)
Cereal -based ORS They contain rice powder, glycine, or starch (as a source of glucose) instead of
glucose Advantages:
1. More effective in decreasing vomiting
2. More effective in treating diarrhea than ORS
3. Shorten duration of illness
4. Glucose-based ORS → ↑ stool volume →increase diarrhea
5. More effective in treating diarrhea due to cholera Disadvantages:
1. Not readily available to use
2. Prepared by boiling
3. Should be prepared fresh (fermented 8-12 h).
4. Enzymes should be present (Amylase, maltase) not in infant. < 4 months

Intravenous fluid therapyIndications:
A.Diarrhea
1. Severe dehydration (> 10% of BW loss in infants)
2. Diarrhea is accompanied by severe uncontrolled vomiting
3. Inability to comply with oral fluids
B. Other indications:
4. Hemorrhage
5. Shock
6. Electrolyte disturbances
7. Supplying fluids and food for patients who are unable to maintain oral intake. In a collapsed patient IV fluids are given initially rapidly at a rate of 100 ml/min to
avoid hypovolemia and irreversible shock. Later on the fluid therapy is adjusted according loss in stools and sweat. Clinically by
noting the neck veins & urine output.

Plasma expanders These are substances of relatively high MW, which when infused into the blood
stream; remain there long enough to augment the volume of the circulating fluid by increasing its osmotic or oncotic pressure.
Properties of the ideal plasma expander:
1. High MW to be retained in circulation
2. Isotonic to that of plasma.
3. Not antigenic, allergic, or toxic
4. Not interfere with cross matching
5. Pharmacologically inert
6. Stable, easily sterilized,
7. A suitable viscosity.
8. Not affect any visceral function adversely.
9. Cheap, easily available.

Plasma expanders
crystalloids colloids
Plasma expanders

Crystalloids They are aqueous solutions containing electrolytes.. Isotonic solutions are the most
commonly used. These solutions contain sodium as the major osmotically active particle which contain either normal saline (0.9% Na Cl) or saline equivalent (lactated Ringer’s solution).
Advantages:
1. Readily available
2. Inexpensive
3. Easily stored
4. Reaction free.
5. Quickly Correct the extracellular electrolyte and fluid deficit.
6. Reduce blood viscosity
7. Recently recommended for initial resuscitation of all forms of hypo-volemic shocks. Disadvantages:
1. Large volumes are required to increase extravascular volume (edema)
2. Excess or too rapid infusion can cause peripheral and pulmonary edema.
3. If not proper Dose & Type, it will cause Electrolyte disturbances

Types of crystalloids1- Normal saline (NaCl 0.9%): Is the most commonly used, osmolality is 308 M osm/kg. Other forms of saline are (0.45% NaCl, .45% NaCl + Glucose 5%) Distribution: Stays almost entirely in the Extracellular space 1 liter of normal saline gives increase in the blood volume of 300 ml. Indications that circulation is improving include normalization of BP, pulse pressure,
heart rate, improvement in the mental status, warmth and color of the skin, improved acid-base balance, and increased urine output.
Replaces Na, cl, water Leaves the blood rapidly → short duration.

Types of crystalloids2- 0.45% Normal saline = ‘Half’ Normal Saline = hypotonic saline: Can be used in severe hyperosmolar states E.g. dehydration Leads to hyponatraemia if plasma sodium is normal (dilution if unchecked) May cause rapid reduction in serum sodium if used in excess or infused too rapidly.
This may lead to cerebral oedema and rarely, central pontine demyelinosis.

Types of crystalloids3- 1.8, 3.0, 7.0, 7.5 and 10% Saline = hypertonic saline: Reserved for plasma expansion with colloids or acute hyponatrema In practice rarely used in general wards; Reserved for high dependency, specialist
areas Distributed almost entirely in the ECF and intravascular space an osmotic gradient
between the ECF and ICF passage of fluid into the EC space. This fluid distributes itself evenly across the ECF and intravascualr space, in turn
leading to intravascular repletion. Large volumes will cause hypernatraemia and IC dehydration.

Types of crystalloids4- Glucose 5%, 10%, and 50% Glucose 5% is a source of water and nutrient Not optimal for volume replacement as its osmolality = 253 m osm/kg. 1 liter of glucose→100 ml blood volume. IV drugs could be mixed with it. Disadvantages: Cannot make blood volume Large amounts can cause water intoxication Hyperglycemia

Types of crystalloids 5- Ringer lactate - content: 0-10 gram glucose/100cc Na 130 mEq/L - NaHCO3 28 mEq/L as lactate K 4 mEq/L - 273 mOsm/L
6- Other crystalloid solutions Ringer acetate Sodium lactate

Types of crystalloids

Colloids
Colloids are solutions containing plasma proteins or other colloidal molecules. Albumin is relatively expensive and offers no advantage over cheaper, synthetic
colloids (solutions 5% to 25%) Colloids cause less extravascular water acumulation in the lung
Colloids could be used alone or in combination with hypertonic saline in resuscitatation of hypovolemic shock in cases of poor vascularity.

Types of colloids 1-dextran It is a complex polysaccharide extracted from beet sugar. There are two types: high molecular weight (70000) and low molecular weight
(40000). Dose: 10-20-ml/kg/ d IV infusions (For restoration of BV) Advantages:
1. Almost ideal
2. Easily sterilized
3. Easily stored for long time. Disadvantages:
1. Induce rouleoux of red cells which interferes with blood grouping and cross matching.
2. Interfere with platelets function and may be associated with abnormal bleeding. Contraindications: Hypersensitivity, Marked hemostatic defects, Heart Failure & Severe renal disease.

Types of colloids2- Gelatin (Haemaccel 30-35000): MW 5000 to 50000 (24000) Duration is about 2-5h Two types succinylated gelatin or polygeline Succinylated gelatin is less antigenic Haemaccel (Urea-linked gelatin) Conc. 3.5 % up to 2.5L/day. Stable for 3 years 60-80 % secreted by kidney Less antigenic Not interfere with cross matching. No bleeding

Types of colloids 3- Hydroxy ethyl starch:
Indications: Hypovolemic shock: (low Albumin-burns-nephrotic syndrome) Used as 6% IV
infusion in H shock Adverse effects: Like dextran (hypersensitivity, Bleeding (reduction of platelet count, increase in PT,
PTT, and decrease factor VIII) Expensive, with no advantage over gelatin and dextran.

Principles of fluid therapy:
1- MAINTENANCE THERAPY
2- DEFICIT THERAPY

Maintenance and replacement therapy
Goals of maintenance fluids:
1. Prevent dehydration
2. Prevent electrolyte disorders
3. Prevent ketoacidosis
4. Prevent protein degradation
Infants are more susceptible for water loss due to:
5. Physiological inability of their renal tubules to concentrate
6. Higher metabolic rate
7. Larger body surface area
8. Poorly developed thirst mechanism
9. Larger turnover water exchange

Maintenance fluid
Maintenance fluid volume is calculated according to body weight: Body Weight Fluid per Day 0-10 kg 100 mL/kg 11-20 kg 1,000 mL + 50 mL/kg for each kg > 10 kg > 20 kg 1,500 mL + 20 mL/kg for each kg > 10 kg
The maximum total fluid per day is normally 2,400 mL. Fluid of choice either : D5 ¼ NS + 20 mEq/L Kcl or D5 ½ NS + 20 mEq/L Kcl The maximum fluid rate is normally 100 mL/hr. 0-10 kg: 4 mL/kg/hr 10-20 kg: 40 mL/hr + 2 mL/kg/hr >20 kg: 60 mL/hr + 1 mL/kg/hr

Electrolytes maintenance:
Sodium, potassium, and chloride are given in maintenance fluids to replace losses from urine and stool.
Maintenance requirements for sodium and potassium. Sodium: 2-3 mEq/kg/24 hr
Potassium: 1-2 mEq/kg/24 hr Adequate chloride is provided as long as at least half of the sodium and potassium are
given as chloride salts. Glucose
Maintenance fluids usually contain 5% dextrose (D5), which provides 17 calories per 100 mL and close to 20% of the daily caloric needs.
This is enough to prevent ketone production and helps minimize protein degradation. It is a diet, and a child will lose weight on this regimen.

Conditions that cause fluid loss which require replacement therapy:
1)Diarrhea2)Emesis and Nasogastric Losses
3)Altered Renal Output

Diarrhea
Adjusting Fluid Therapy Diarrhea:
AVERAGE COMPOSITION OF DIARRHEA Sodium: 55 mEq/L
Potassium: 25 mEq/L Bicarbonate: 15 mEq/L
APPROACH TO REPLACEMENT OF ONGOING LOSSES
Solution: D5 1/4 NS + 15 mEq/L bicarbonate + 25 mEq/L KCl Replace stool mL/mL every 1-6 hr

Emesis and Nasogastric Losses
Adjusting Fluid Therapy for Emesis or Nasogastric Losses
AVERAGE COMPOSITION OF GASTRIC FLUID Sodium: 60 mEq/L
Potassium: 10 mEq/L Chloride: 90 mEq/L
APPROACH TO REPLACEMENT OF ONGOING LOSSES Solution: D5 1/2 NS + 10 mEq/L KCl Replace output mL/mL every 1-6 hr

Altered Renal Output
Adjusting Fluid Therapy for Altered Renal Output
OLIGURIA/ANURIA Place the patient on insensible fluids (1/3 maintenance) *RATE
Replace urine output mL/mL with 1/2 NS
POLYURIA Place the patient on insensible fluids (1/3 maintenance)
Measure urine electrolytes Replace urine output mL/mL with a solution that is based on the measured urine
Electrolytes.

Deficit therapy
Dehydration
Isonatriamaemic
HypernatriaemicHyponatriaemic

What is Dehydration?
Dehydration is simply the excessive loss of body water resulting a decrease in total body water
Total Fluid Loss > Total Fluid Intake
Fluid lost from both intravascular & extravascular compartments
Intravascular loss – Hypovolaemia & Serum osmolality
Extravascular loss – Impairment of cellular function & Loss of tissue laxity
Often there is an associated electrolyte loss with diarrhoea
Sodium is the most affected electrolyte – Hypernatremia or Hypernatremia

Approach to Dehydration
1) Initial Resuscitation
2) Determine % dehydration
3) Define the type of dehydration
4) Determine the type and rate of rehydration fluids

Initial Resuscitation

AssessmentHistory Examination
Increased thirsty Body weight loss
Reduced level of consciousness (Drowsy)
Anterior fontanelle - Sunken
Reduced urine output Sunken eyes
Reduced/Absent tears
Dry mucous membranes
Loss skin turgor
Pulse rate – Increased
Capillary refill time – Prolonged (>2 seconds)
Blood Pressure – Low
Respiration – Deep & Rapid

Clinical Evaluation of Dehydration
Mild dehydration (3-5%): normal or increased pulse, decreased urine output, thirsty, normal physical
examination
Moderate dehydration (7-10%): tachycardia, little or no urine output, irritable/lethargic, sunken eyes and
fontanel, decreased tears, dry mucous membranes, mild tenting of the skin, delayed capillary refill, cool and pale
Severe dehydration (10-15%): rapid and weak pulse, decreased blood pressure, no urine output, very sunken
eyes and fontanel, no tears, dry mucous membranes, tenting of the skin, very delayed capillary refill.


Isonatriamaemic dehydration The child with dehydration has lost water; there is almost always a concurrent loss of
sodium and potassium. Most patients have isotonic dehydration and therefore have normal serum sodium values.
Calculation of Deficits WATER DEFICIT: Percent dehydration × weight SODIUM DEFICIT: Water deficit × 80 mEq/L
POTASSIUM DEFICIT: Water deficit × 30 mEq/L

Isonatriamaemic dehydration
The child with dehydration requires acute intervention to ensure that there is adequate tissue perfusion. This requires restoration of the intravascular volume with an isotonic solution such as normal saline (NS) or Ringer lactate.
When there is adequate intravascular volume, it is appropriate to plan the fluid therapy for the next 24 hr.
The general approach is outlined as following: Restore intravascular volume Normal saline: 20 mL/kg over 20 min (Repeat until intravascular volume restored)
Calculate 24-hr water needs Calculate maintenance water Calculate deficit water

management Calculate 24-hr electrolyte needs Calculate maintenance sodium and potassium Calculate deficit sodium and potassium
Select an appropriate fluid (based on total water and electrolyte needs) Administer half the calculated fluid during the first 8 hr, first subtracting any
boluses from this amount Administer the remainder over the next 16 hrs
Replace ongoing losses as they occur

Hyponatremic dehydration:
The pathogenesis of hyponatremic dehydration is usually due to a combination of sodium and water loss and water retention to compensate for the volume depletion.
Occurs in children who have diarrhea and consume a hypotonic fluid (water or diluted formula).
The initial goal in treating hyponatremia is correction of intravascular volume depletion with isotonic fluid (NS or Ringer lactate).
The following formula can be used to calculate a patient's sodium deficit:
where [Na+]d = desired sodium concentration, [Na+]i = initial sodium concentration, and Wt = weight in kilograms.

Hyponatremic dehydration:
Rapid correction of hyponatremia (>12mEq/L/24hrs) thought to contribute to….
Central Pontine Myelinolysis Fluctuating LOC
Pseudobulbar palsy Quadraparesis

Hypernatremic Dehydration:
Hypernatremic dehydration is the most dangerous form of dehydration due to complications of hypernatremia and of therapy.
The movement of water from the intracellular space to the extracellular space during hypernatremic dehydration protects the intravascular volume. Thus, children with hypernatremia often appear less ill than children with a similar degree of isotonic dehydration.
Urine output may be preserved longer and there may be less tachycardia. Unfortunately, the milder manifestations often lead to children with hypernatremic dehydration being brought to medical attention with more profound dehydration.

Management Restore intravascular volume Normal saline: 20 mL/kg over 20 min (Repeat until intravascular volume restored)
Determine the time for correction based on the initial sodium concentration [Na]: 145-157 mEq/L: 24 hr [Na]: 158-170 mEq/L: 48 hr [Na]: 171-183 mEq/L: 72 hr [Na]: 184-196 mEq/L: 84 hr
Administer fluid at a constant rate over the time for correction Typical fluids: D5 1/4 NS or D5 1/2 NS (both with 20 mEq/L KCl unless
contraindicated) Typical rate: 1.25-1.5 times maintenance
Increase sodium concentration of intravenous fluid, or Decrease rate of intravenous fluid
Decrease sodium concentration of intravenous fluid, or Increase rate of intravenous fluid

Management
Follow serum sodium concentration Adjust fluid based on clinical status and serum sodium concentration
Signs of volume depletion: administer NS (20 mL/kg) Sodium decreases too rapidly Sodium decreases too slowly
Replace ongoing losses as they occur