Embed Size (px)
Citation preview
DISTAL END HUMERUS FRACTURES
BY:-Dr. Anshu sharmaGuide:- Dr.A.K. Mathur
• Fractures of adult distal humerus are Fractures of adult distal humerus are relatively uncommon comprising relatively uncommon comprising approximately 2%of all fractures and one-approximately 2%of all fractures and one-third of all humerus fractures. third of all humerus fractures.
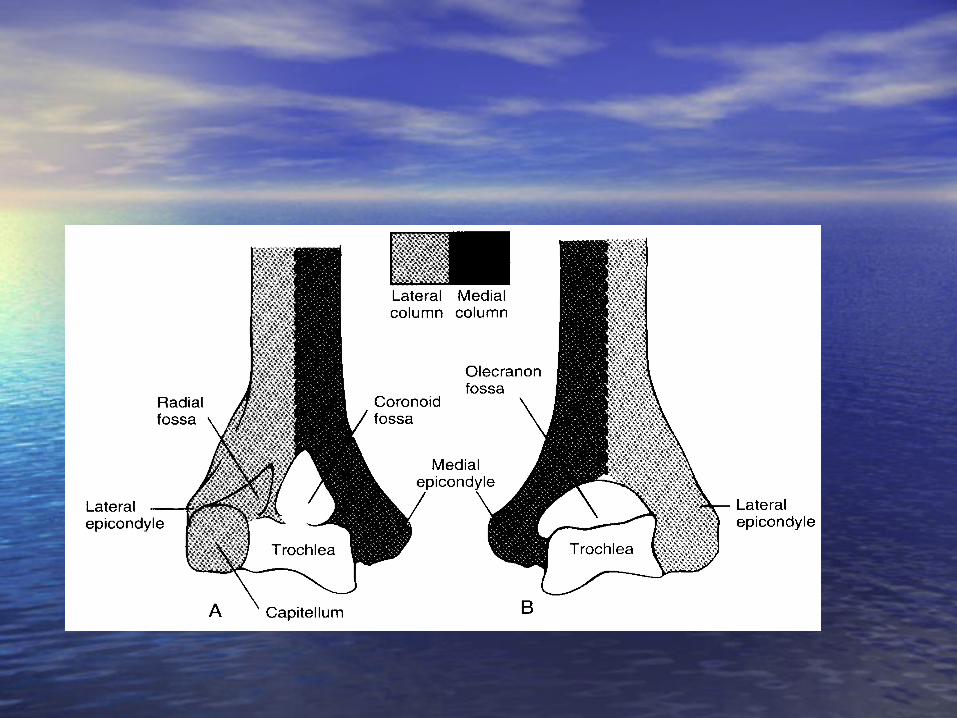
Anatomy of Distal HumerusAnatomy of Distal Humerus-->The lower end of the humerus forms the condyles -->The lower end of the humerus forms the condyles
which is expended from side to side, and has articular which is expended from side to side, and has articular and nonarticular parts.and nonarticular parts.
-->The articular parts are:--->The articular parts are:- Capitellum articulate with head of radius,Capitellum articulate with head of radius, Trochlea articulate with trochlear notch of ulna.Trochlea articulate with trochlear notch of ulna.
-->The non-articular parts are:--->The non-articular parts are:- Medial and lateral supra condylar ridge,Medial and lateral supra condylar ridge, Medial and lateral epicondyles,Medial and lateral epicondyles, Coronoid fossa,Coronoid fossa, Radial fossa,Radial fossa, Olecranon fossa.Olecranon fossa.
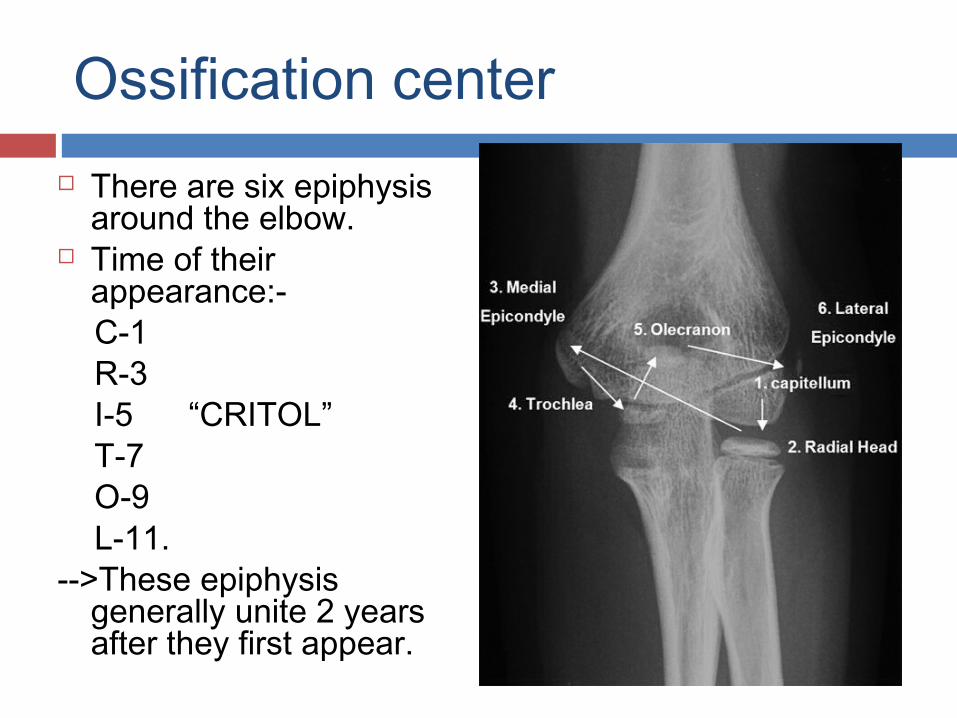
Ossification center There are six epiphysis
around the elbow. Time of their
appearance:- C-1 R-3 I-5 “CRITOL” T-7 O-9 L-11.-->These epiphysis
generally unite 2 years after they first appear.
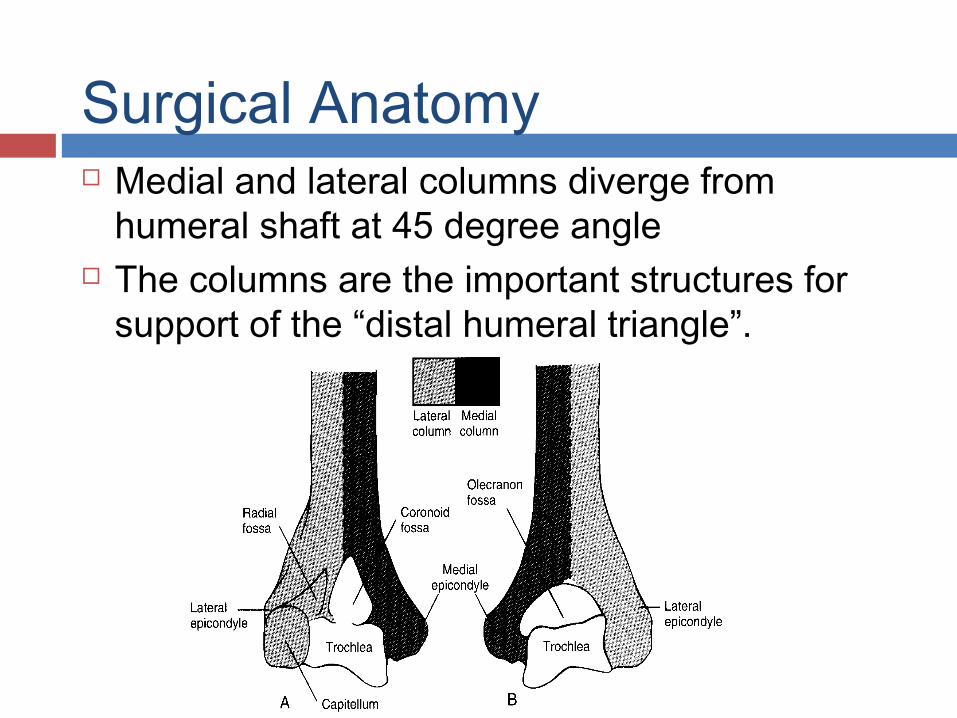
Surgical Anatomy Medial and lateral columns diverge from
humeral shaft at 45 degree angle The columns are the important structures for
support of the “distal humeral triangle”.
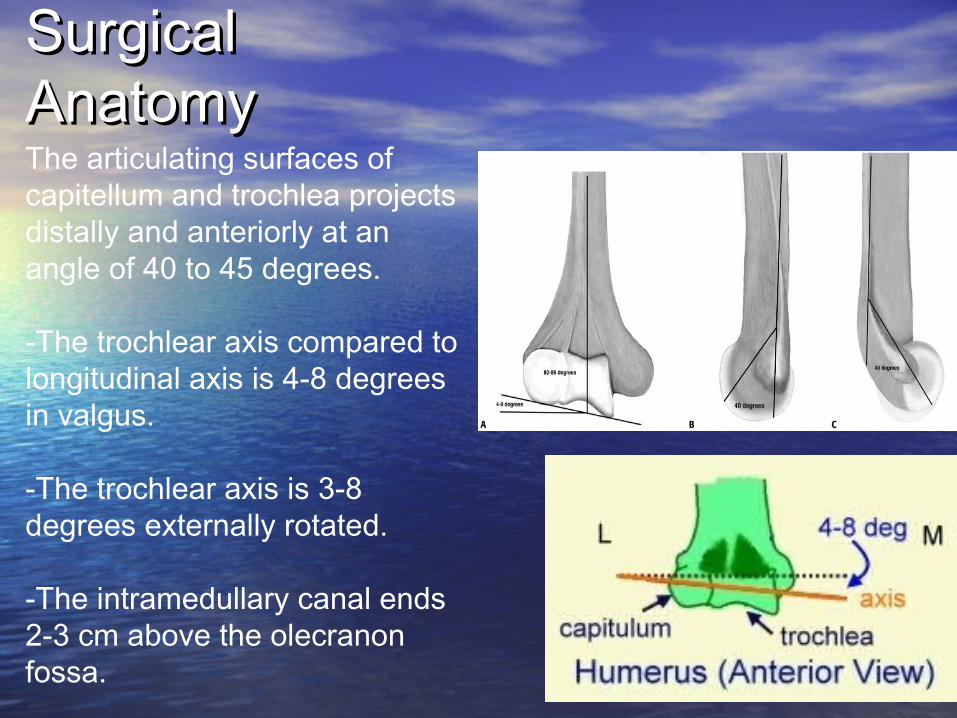
Surgical Surgical AnatomyAnatomyThe articulating surfaces of capitellum and trochlea projects distally and anteriorly at an angle of 40 to 45 degrees.
-The trochlear axis compared to longitudinal axis is 4-8 degrees in valgus.
-The trochlear axis is 3-8 degrees externally rotated.
-The intramedullary canal ends 2-3 cm above the olecranon fossa.
distal humeral triangle
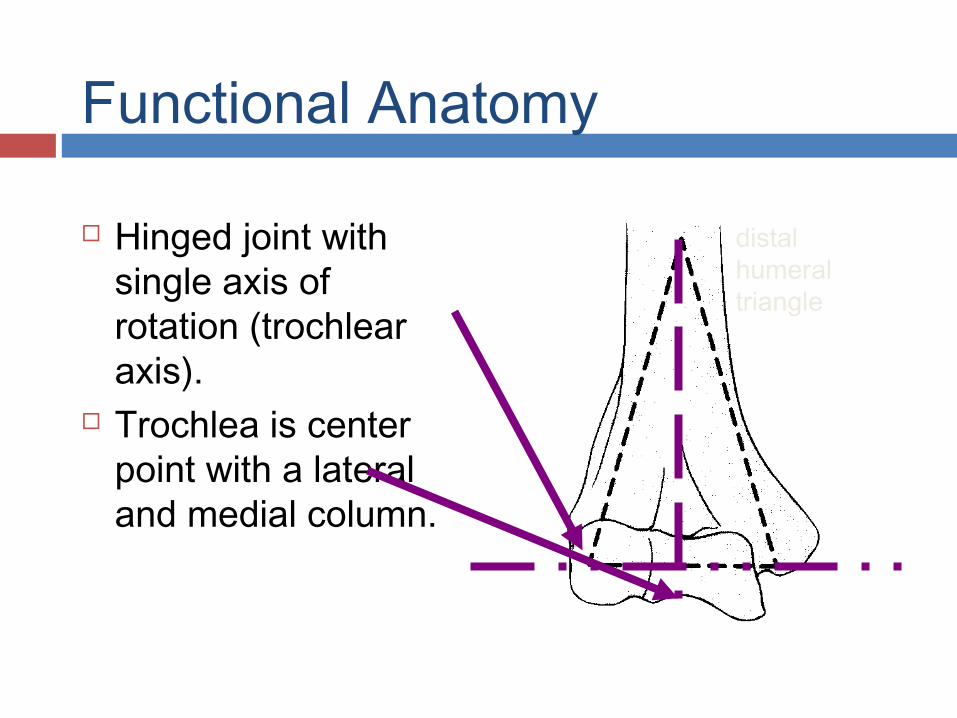
Functional Anatomy
Hinged joint with single axis of rotation (trochlear axis).
Trochlea is center point with a lateral and medial column.
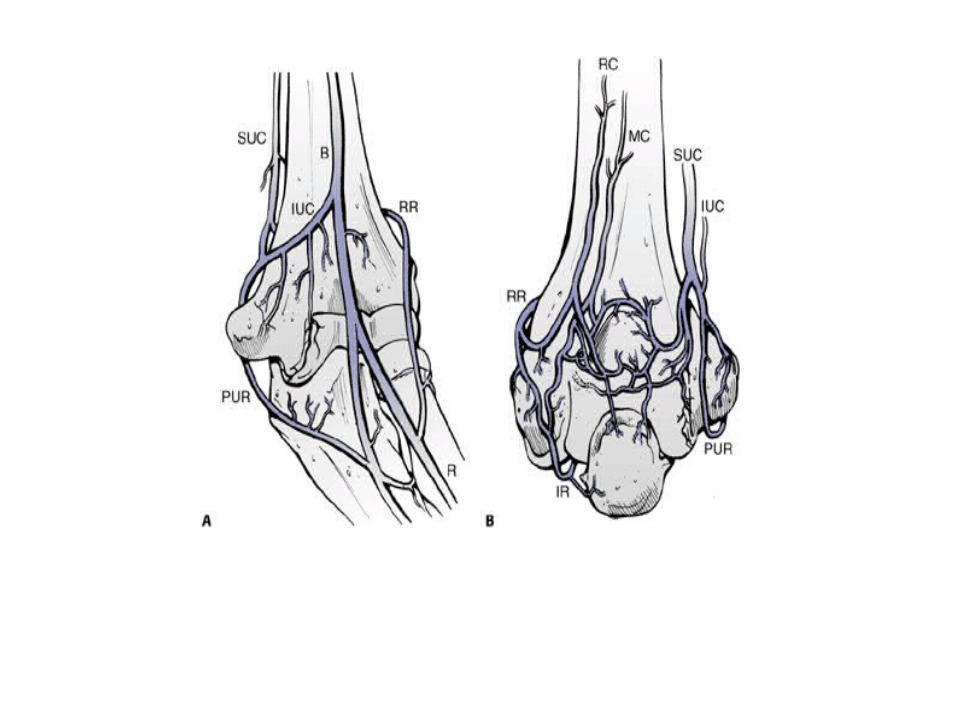
The blood supply of the distal humerus. A. Anterior view. B. Posterior view. SUC, superior ulnar collateral artery; B, brachial artery; IUC, inferior ulnar collateral artery; RR, radial recurrent artery; PUR, posterior ulnar recurrent artery; R, radial artery; RC, radial collateral artery; MC, middle collateral artery; IR, interosseous recurrent artery.
Blood supplyBlood supply
• The distal humerus thus has a rich The distal humerus thus has a rich anastomotic blood supply and problems anastomotic blood supply and problems with healing and osteonecrosis are with healing and osteonecrosis are therefore relatively uncommon.therefore relatively uncommon.
• During reduction and internal fixation of During reduction and internal fixation of complex closed distal humeral fractures, complex closed distal humeral fractures, retention of even completely retention of even completely devascularized fragments is appropriate if devascularized fragments is appropriate if they are large and contributing to the they are large and contributing to the stability of the reconstruction.stability of the reconstruction.
• Chances of Revascularization of these Chances of Revascularization of these fragments subsequently are very high.fragments subsequently are very high.
Imaging Imaging • RadiographsRadiographs
– recommended viewsrecommended views• obtain AP and lateral of humerus and elbow.obtain AP and lateral of humerus and elbow.• include entire length of humerus and forearm.include entire length of humerus and forearm.
– additional viewsadditional views• obtain wrist radiographs if elbow injury present or distal tenderness on examobtain wrist radiographs if elbow injury present or distal tenderness on exam• oblique radiographs may assist in surgical planningoblique radiographs may assist in surgical planning• traction radiographs may assist in surgical planningtraction radiographs may assist in surgical planning
– specifically evaluate if there is continuity of the trochlear fragment to medial specifically evaluate if there is continuity of the trochlear fragment to medial epicondylar fragment, this can influence hardware choiceepicondylar fragment, this can influence hardware choice
• CTCT– often obtained for surgical planning.often obtained for surgical planning.– especially helpful when shear fractures of the capitellum and trochlea especially helpful when shear fractures of the capitellum and trochlea
are suspected.are suspected.– 3D CT scan.3D CT scan.
• MRIMRI– usually not indicated in acute injury.usually not indicated in acute injury.
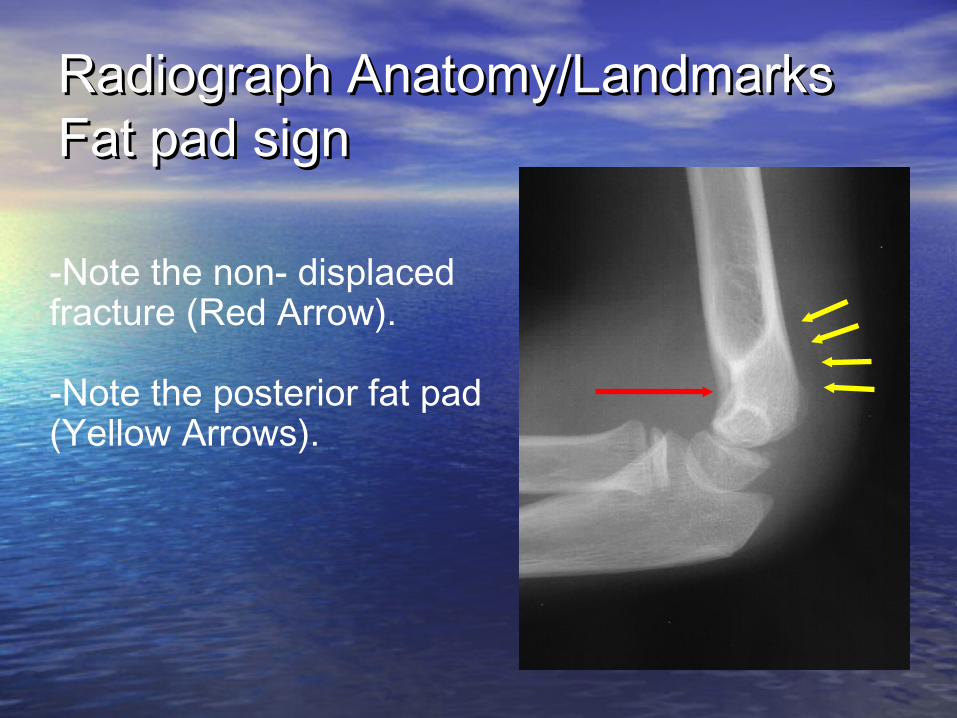
Radiograph Anatomy/LandmarksRadiograph Anatomy/LandmarksFat pad signFat pad sign
-Note the non- displaced fracture (Red Arrow).
-Note the posterior fat pad (Yellow Arrows).
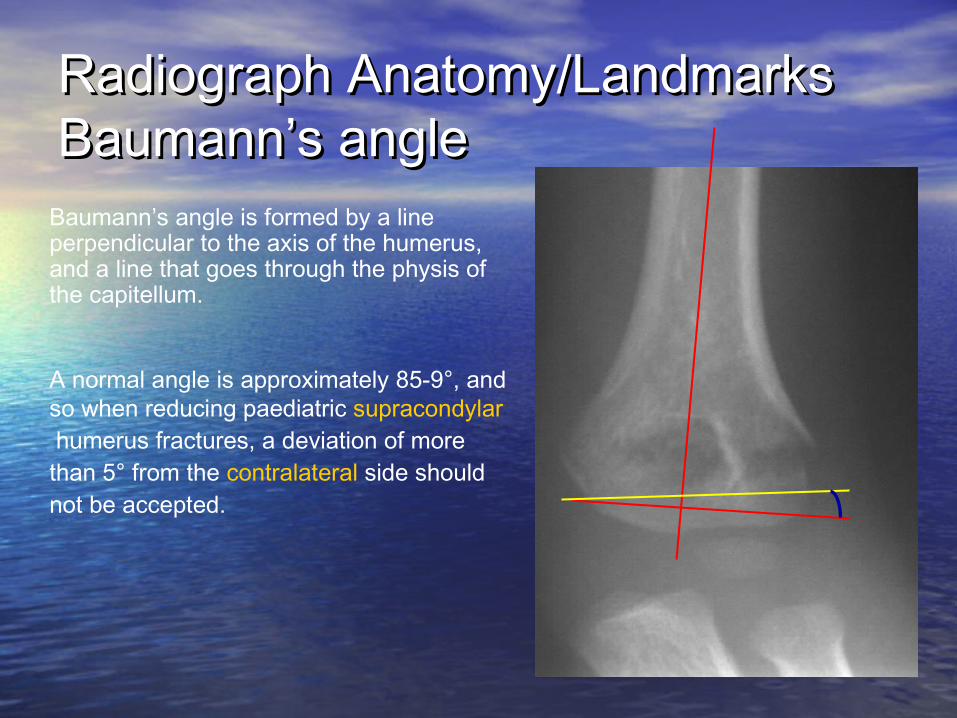
Radiograph Anatomy/Landmarks Radiograph Anatomy/Landmarks Baumann’s angleBaumann’s angle
Baumann’s angle is formed by a line perpendicular to the axis of the humerus, and a line that goes through the physis of the capitellum.
A normal angle is approximately 85-9°, and so when reducing paediatric supracondylar humerus fractures, a deviation of more than 5° from the contralateral side should not be accepted.
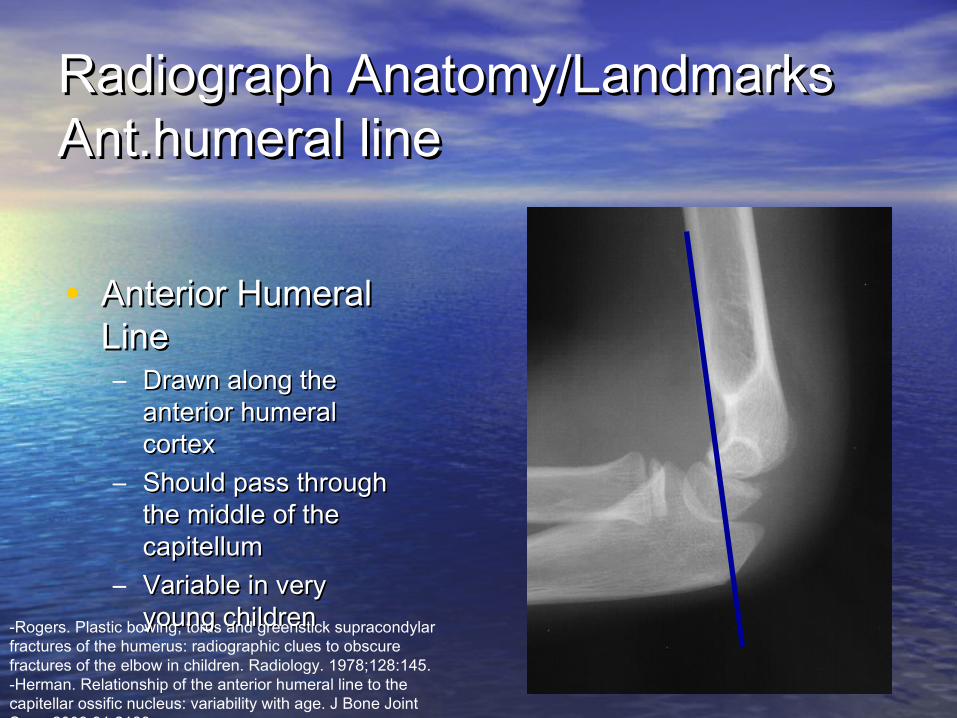
Radiograph Anatomy/LandmarksRadiograph Anatomy/LandmarksAnt.humeral lineAnt.humeral line
• Anterior Humeral Anterior Humeral LineLine– Drawn along the Drawn along the
anterior humeral anterior humeral cortexcortex
– Should pass through Should pass through the middle of the the middle of the capitellumcapitellum
– Variable in very Variable in very young children young children -Rogers. Plastic bowing, torus and greenstick supracondylar
fractures of the humerus: radiographic clues to obscure fractures of the elbow in children. Radiology. 1978;128:145.-Herman. Relationship of the anterior humeral line to the capitellar ossific nucleus: variability with age. J Bone Joint Surg. 2009;91:2188.
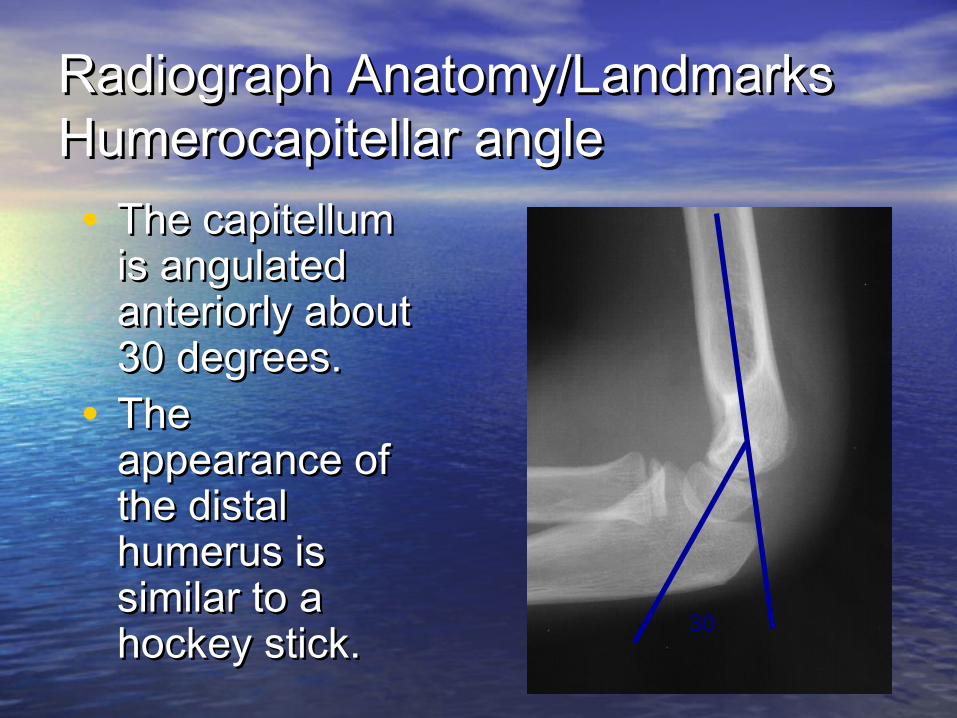
Radiograph Anatomy/LandmarksRadiograph Anatomy/LandmarksHumerocapitellar angleHumerocapitellar angle• The capitellum The capitellum
is angulated is angulated anteriorly about anteriorly about 30 degrees.30 degrees.
• The The appearance of appearance of the distal the distal humerus is humerus is similar to a similar to a hockey stick.hockey stick. 30
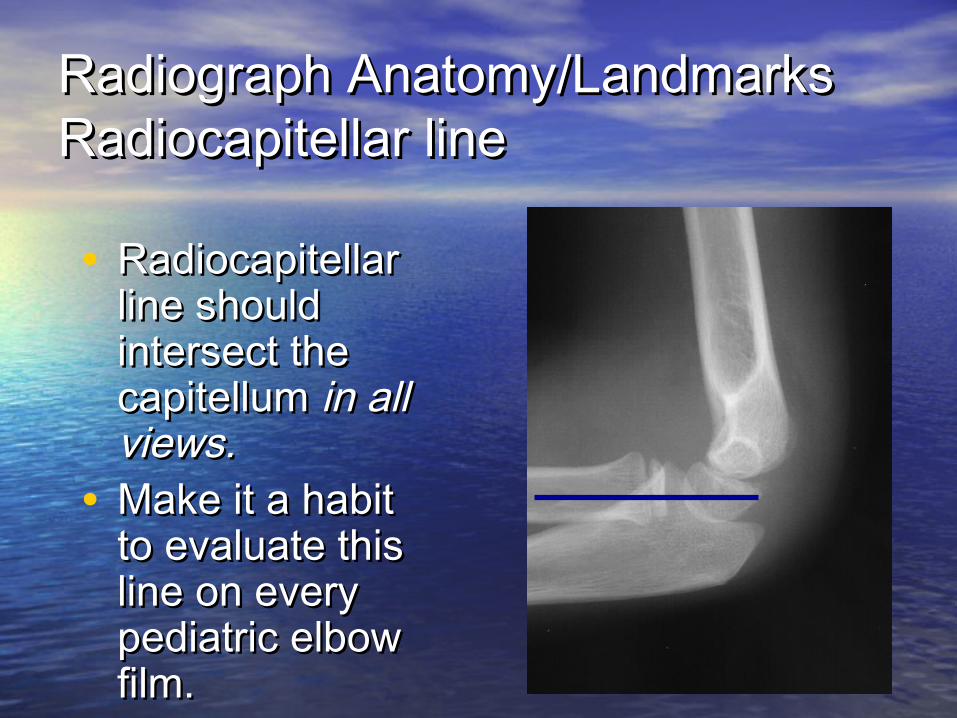
Radiograph Anatomy/LandmarksRadiograph Anatomy/LandmarksRadiocapitellar lineRadiocapitellar line
• Radiocapitellar Radiocapitellar line should line should intersect the intersect the capitellum capitellum in all in all views.views.
• Make it a habit Make it a habit to evaluate this to evaluate this line on every line on every pediatric elbow pediatric elbow film.film.
Classification of FracturesClassification of Fractures
• The AO-ASIF Group have defined three The AO-ASIF Group have defined three types of distal humeral fractures:-types of distal humeral fractures:-
-->Type A-An extra articular supracondylar -->Type A-An extra articular supracondylar fractures,fractures,
-->Type B-An intracondylar unicondylar -->Type B-An intracondylar unicondylar fractures,fractures,
-->type C-Bicondylar fractures with varying -->type C-Bicondylar fractures with varying degree of comminution.degree of comminution.
Supracondylar Humerus FracturesSupracondylar Humerus Fractures
• Most common fracture around the elbow in Most common fracture around the elbow in children.children.– 60 percent of elbow fractures.60 percent of elbow fractures.
• 95 percent are extension type injuries.95 percent are extension type injuries.– Produces posterior angulation/displacement of the Produces posterior angulation/displacement of the
distal fragment.distal fragment.
• Occurs from a fall on an outstretched hand.Occurs from a fall on an outstretched hand.– Ligamentous laxity and hyperextension of the elbow Ligamentous laxity and hyperextension of the elbow
are important mechanical factors.are important mechanical factors.
• May be associated with a distal radius or May be associated with a distal radius or forearm fractures.forearm fractures.
Supracondylar Humerus Fractures Supracondylar Humerus Fractures Associated InjuriesAssociated Injuries• Nerve injury incidence is high, between 7 and 16 %. Nerve injury incidence is high, between 7 and 16 %.
– Radial nerve,Radial nerve,– Median nerve,Median nerve,– Ulnar nerve (flexion type).Ulnar nerve (flexion type).
• Radial nerve injury is most commonly injured nerve.Radial nerve injury is most commonly injured nerve.• In many cases, assessment of nerve integrity is limited In many cases, assessment of nerve integrity is limited
because children can not always cooperate.because children can not always cooperate.• 5% have associated distal radius fracture.5% have associated distal radius fracture. Physical exam of distal forearm and Radiographs if Physical exam of distal forearm and Radiographs if
needed.needed.• Vascular injuries are rare, but pulses should always be Vascular injuries are rare, but pulses should always be
assessed before and after reduction.assessed before and after reduction.• In the absence of a radial and/or ulnar pulse, the In the absence of a radial and/or ulnar pulse, the
fingers may still be well-perfused, because of the fingers may still be well-perfused, because of the excellent collateral circulation around the elbow.excellent collateral circulation around the elbow.
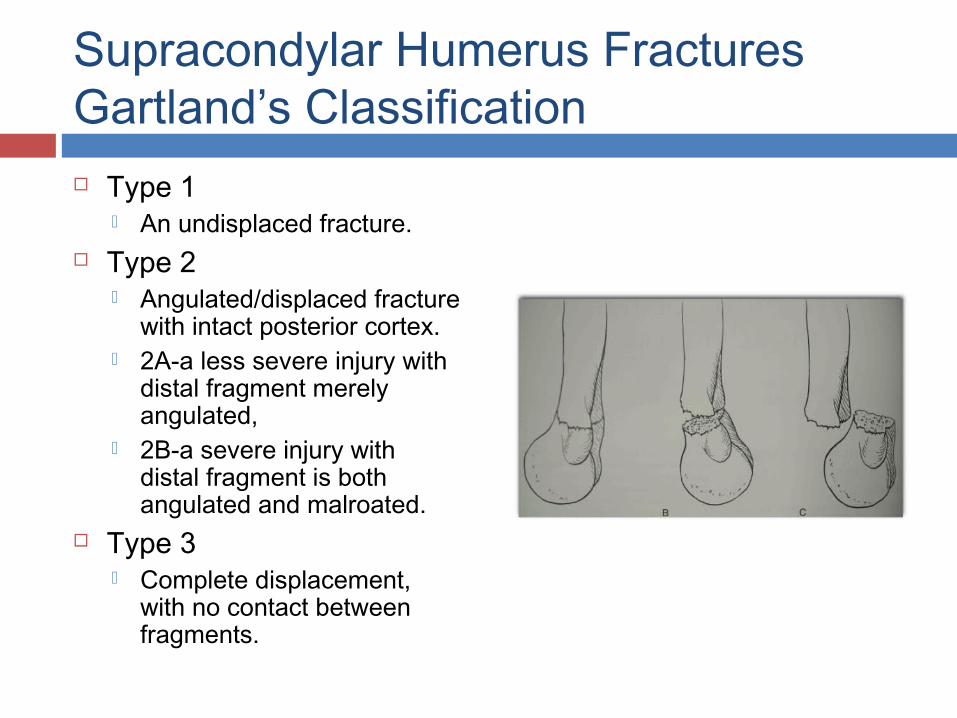
Supracondylar Humerus FracturesGartland’s Classification Type 1
An undisplaced fracture. Type 2
Angulated/displaced fracture with intact posterior cortex.
2A-a less severe injury with distal fragment merely angulated,
2B-a severe injury with distal fragment is both angulated and malroated.
Type 3 Complete displacement,
with no contact between fragments.
Supracondylar Humerus Fractures Supracondylar Humerus Fractures TreatmentTreatment
• Type 1 FracturesType 1 Fractures– In most cases, these can be treated with In most cases, these can be treated with
immobilization for approximately 3 weeks, at 90 immobilization for approximately 3 weeks, at 90 degrees of flexion.degrees of flexion.
– If there is significant swelling, do not flex to 90 If there is significant swelling, do not flex to 90 degrees until the swelling subsides.degrees until the swelling subsides.
– It is essential to obtain an x ray 5-7 days later to It is essential to obtain an x ray 5-7 days later to check that there has been no displacement.check that there has been no displacement.
Supracondylar Humerus Fractures Supracondylar Humerus Fractures TreatmentTreatment
• Type 2 Fractures: Posterior AngulationType 2 Fractures: Posterior Angulation– If minimally displaced (anterior humeral line hits If minimally displaced (anterior humeral line hits
part of capitellum)part of capitellum)• Immobilization for 3 weeks. Immobilization for 3 weeks. • Close follow-up is necessary to monitor for loss of Close follow-up is necessary to monitor for loss of
reduction.reduction.– Displaced (anterior humeral line misses Displaced (anterior humeral line misses
capitellum)capitellum)• Reduction may be necessary.Reduction may be necessary.
Type 2 FracturesType 2 FracturesTreatmentTreatment• Reduction of these fractures is usually not Reduction of these fractures is usually not
difficultdifficult– Maintaining reduction usually requires flexion beyond Maintaining reduction usually requires flexion beyond
90°90°
• Excessive flexion may not be tolerated Excessive flexion may not be tolerated because of swellingbecause of swelling– May require percutaneous pinning to maintain May require percutaneous pinning to maintain
reduction reduction
• Most authors suggest that percutaneous Most authors suggest that percutaneous pinning is the safest form of treatment for pinning is the safest form of treatment for many of these fracturesmany of these fractures– Pins maintain the reduction and allow the elbow to be Pins maintain the reduction and allow the elbow to be
immobilized in a less flexed position.immobilized in a less flexed position.
Supracondylar Humerus Fractures Supracondylar Humerus Fractures TreatmentTreatment
• Type 3 FracturesType 3 Fractures– These fractures have a high risk of neurologic and/or These fractures have a high risk of neurologic and/or
vascular compromise.vascular compromise.– Can be associated with a significant amount of Can be associated with a significant amount of
swelling.swelling.– Current treatment protocols use percutaneous pin Current treatment protocols use percutaneous pin
fixation in almost all cases.fixation in almost all cases.– In rare cases, open reduction may be necessary.In rare cases, open reduction may be necessary.
• Especially in cases of vascular disruption.Especially in cases of vascular disruption.
Supracondylar Humerus FracturesSupracondylar Humerus FracturesPin FixationPin Fixation
• Different authors have recommended Different authors have recommended different pin fixation methods.different pin fixation methods.
• The medial pin can injury the ulnar and The medial pin can injury the ulnar and median nerve.median nerve.– Some advocate 2 or 3 lateral pins to avoid injuring the Some advocate 2 or 3 lateral pins to avoid injuring the
nerve.nerve.• Space pins as widely as possibleSpace pins as widely as possible
– If the lateral pins are placed close together at the If the lateral pins are placed close together at the fracture site, the pins may not provide much fracture site, the pins may not provide much resistance to rotation and further displacement.resistance to rotation and further displacement.
• Some recommend one lateral, and one Some recommend one lateral, and one medial pinmedial pin
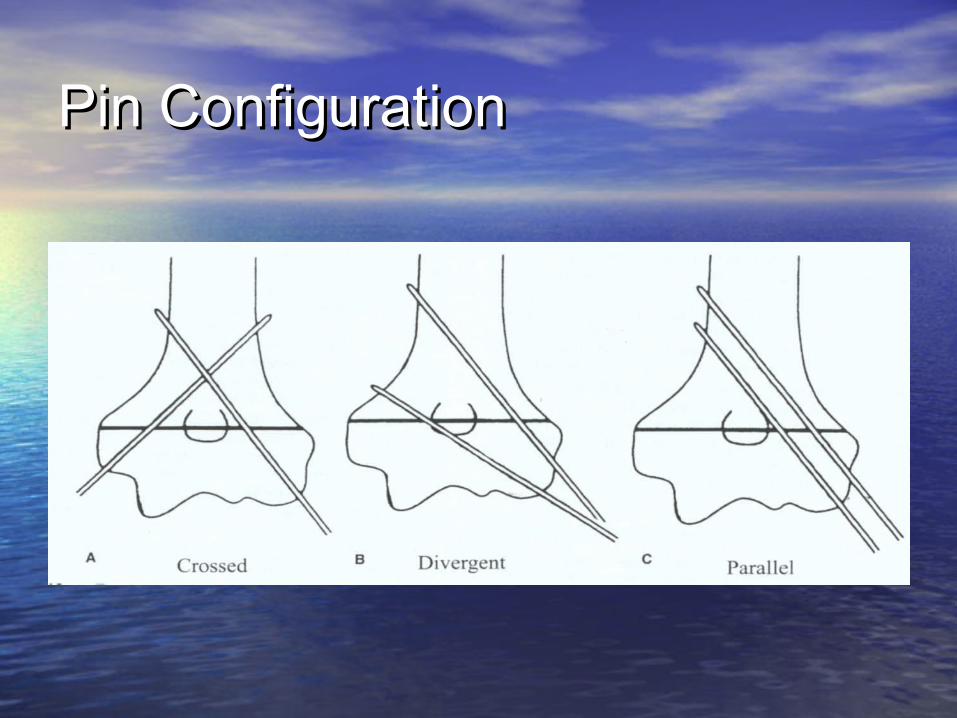
Pin ConfigurationPin Configuration
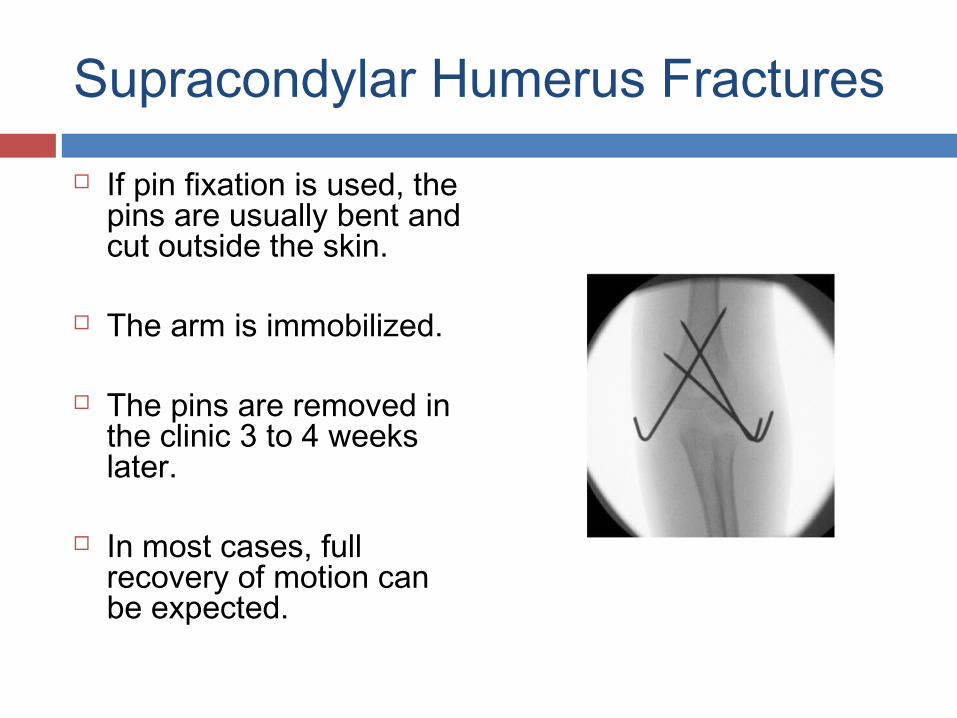
Supracondylar Humerus Fractures
If pin fixation is used, the pins are usually bent and cut outside the skin.
The arm is immobilized.
The pins are removed in the clinic 3 to 4 weeks later.
In most cases, full recovery of motion can be expected.
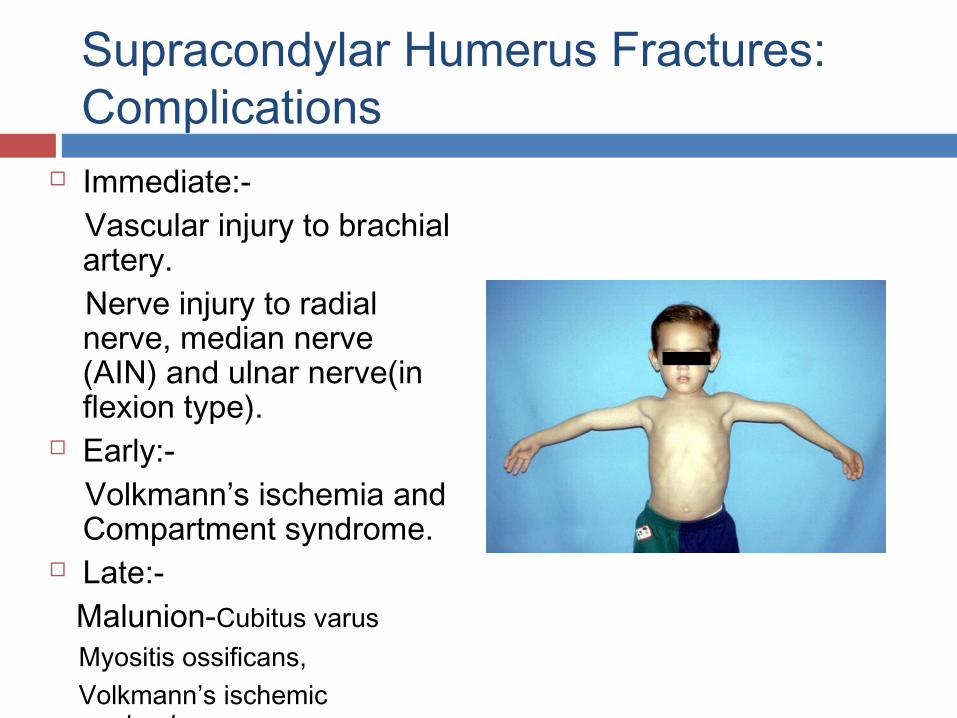
Supracondylar Humerus Fractures:Complications
Immediate:- Vascular injury to brachial
artery. Nerve injury to radial
nerve, median nerve (AIN) and ulnar nerve(in flexion type).
Early:- Volkmann’s ischemia and
Compartment syndrome. Late:- Malunion-Cubitus varus Myositis ossificans, Volkmann’s ischemic
contracture.
Intercondylar fractureIntercondylar fracture
• Most common distal humeral fracture in adults.Most common distal humeral fracture in adults.• Comminution is common.Comminution is common.• Fracture fregments are often displaced by Fracture fregments are often displaced by
unapposed muscle pull at the medial and lateral unapposed muscle pull at the medial and lateral epicondyles which rotate the articular surfaces.epicondyles which rotate the articular surfaces.
Mechanism of injury:Mechanism of injury: ForceForce is directed against the posterior aspect of is directed against the posterior aspect of an elbow which is flexed > 90° which causes an elbow which is flexed > 90° which causes the ulna the ulna to driveto drive into the into the trochlea. trochlea.
Clinical FeaturesClinical Features
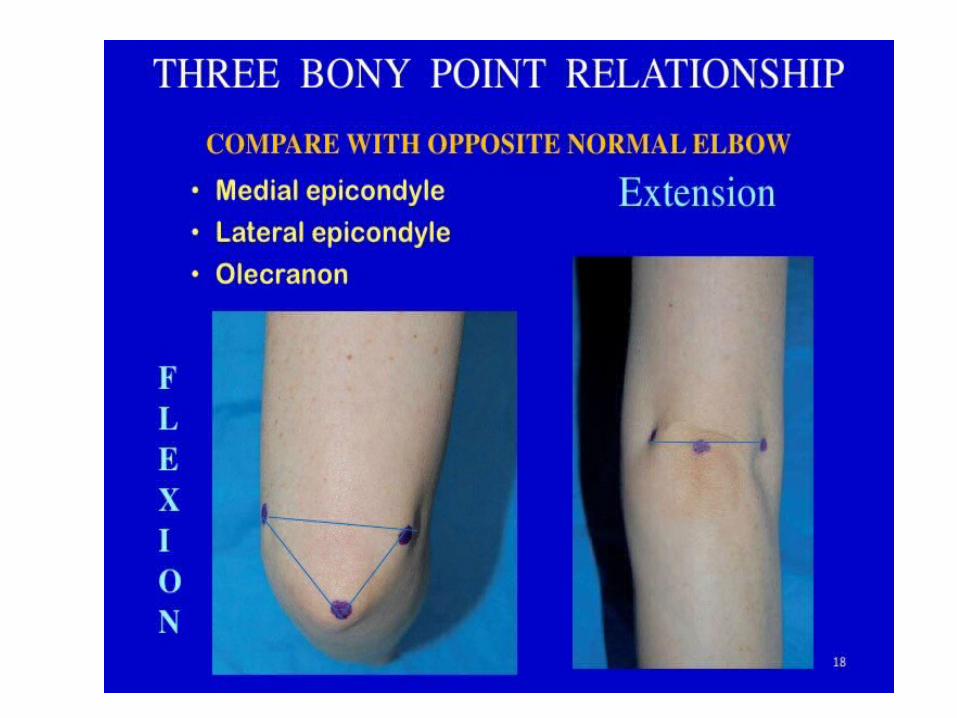
1. The elbow maybe held in 90° flexion 1. The elbow maybe held in 90° flexion and forearm is kept pronated.and forearm is kept pronated.2. Crepitus may be elicited.2. Crepitus may be elicited.3. Independent mobility of the medial and 3. Independent mobility of the medial and lateral condyle can be elicited.lateral condyle can be elicited.4. The normal 3 point bony relationship 4. The normal 3 point bony relationship between the olecranon, medial epicondyle between the olecranon, medial epicondyle and lateral epicondyle is lost.and lateral epicondyle is lost.
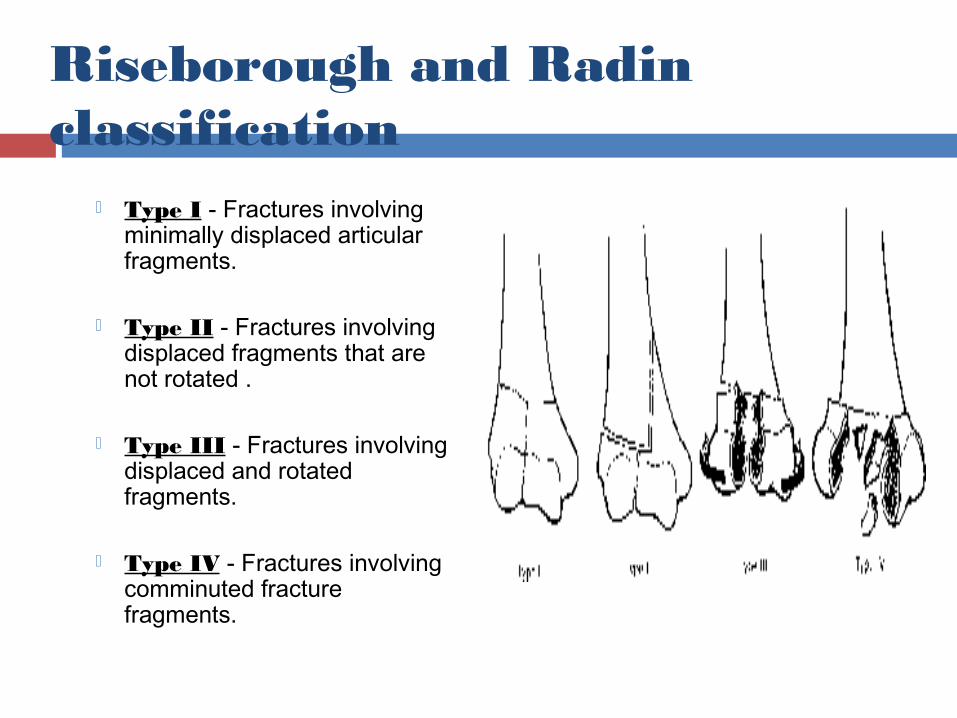
Riseborough and Radin classification
Type I - Fractures involving minimally displaced articular fragments.
Type II - Fractures involving displaced fragments that are not rotated .
Type III - Fractures involving displaced and rotated fragments.
Type IV - Fractures involving comminuted fracture fragments.
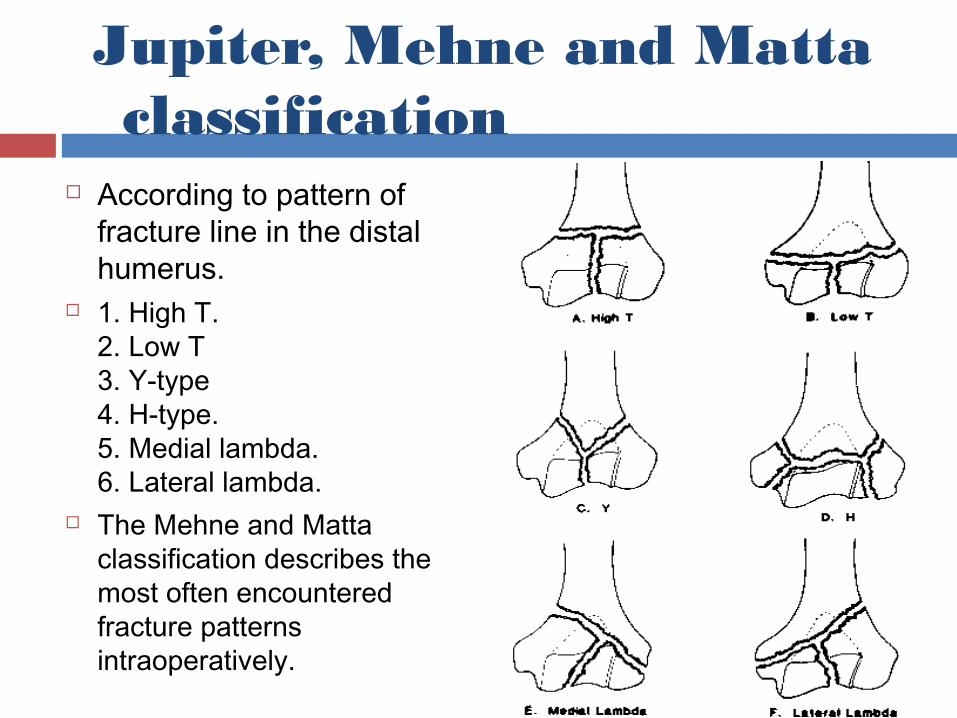
Jupiter, Mehne and Matta classification
According to pattern of fracture line in the distal humerus.
1. High T.2. Low T3. Y-type4. H-type.5. Medial lambda.6. Lateral lambda.
The Mehne and Matta classification describes the most often encountered fracture patterns intraoperatively.
Nonoperative TreatmentNonoperative Treatment-->Nonoperative treatment indicated in:--->Nonoperative treatment indicated in:- -Nondisplaced fractures,-Nondisplaced fractures, -Elderly patients with displaced fractures and severe -Elderly patients with displaced fractures and severe
osteopenia and comminution,osteopenia and comminution, -Patients with significant co-morbid conditions.-Patients with significant co-morbid conditions.
-->Non operative methods are:--->Non operative methods are:--Cast immobilization:- rarely indicated.-Cast immobilization:- rarely indicated. “ “worst of both worlds”worst of both worlds” inadequate reduction and prolonged immobilization. inadequate reduction and prolonged immobilization. -Bag of bones:-arm is placed in a collar and cuff with as -Bag of bones:-arm is placed in a collar and cuff with as
much flexion as possible after initial reduction.much flexion as possible after initial reduction. Aim is to obtain a painless pseudoarthrosis by Aim is to obtain a painless pseudoarthrosis by
gravity traction effect. gravity traction effect.
Operative treatmentOperative treatment
• Indicated in displaced reconstructible fracture.Indicated in displaced reconstructible fracture.• Aim is to restore articular congurity and to Aim is to restore articular congurity and to
secure supracondylar component.secure supracondylar component.• Methods of fixation:-Methods of fixation:- -Interfragmentry screws,-Interfragmentry screws, -Dual plate fixation by olecranon osteotomy -Dual plate fixation by olecranon osteotomy
approach or triceps sparing extensile posterior approach or triceps sparing extensile posterior approach.approach.
-->Total elbow arthroplasty in markedly -->Total elbow arthroplasty in markedly comminuted fractures and with osteoporosis.comminuted fractures and with osteoporosis.
ComplicationsComplications
• Elbow stiffness,Elbow stiffness,• Failure of fixation,Failure of fixation,• Nerve injury to ulnar nerve,Nerve injury to ulnar nerve,• Posttrumatic arthritis,Posttrumatic arthritis,• Heterotopic bone formation,Heterotopic bone formation,• Nonunion of osteotomy,Nonunion of osteotomy,• Infection.Infection.
Condylar fracturesCondylar fractures• Rare in adults and more common in Rare in adults and more common in
pediatric age group.pediatric age group.• Medial condyle fractures include trochlea Medial condyle fractures include trochlea
and medial epicondyle fractures.and medial epicondyle fractures.• Lateral condyle fractures include Lateral condyle fractures include
capitellum and lateral epicondyle capitellum and lateral epicondyle fractures.fractures.
• Lateral fractures are more common than Lateral fractures are more common than medial.medial.
• MOI-abduction or adduction of the forearm MOI-abduction or adduction of the forearm with elbow extension.with elbow extension.
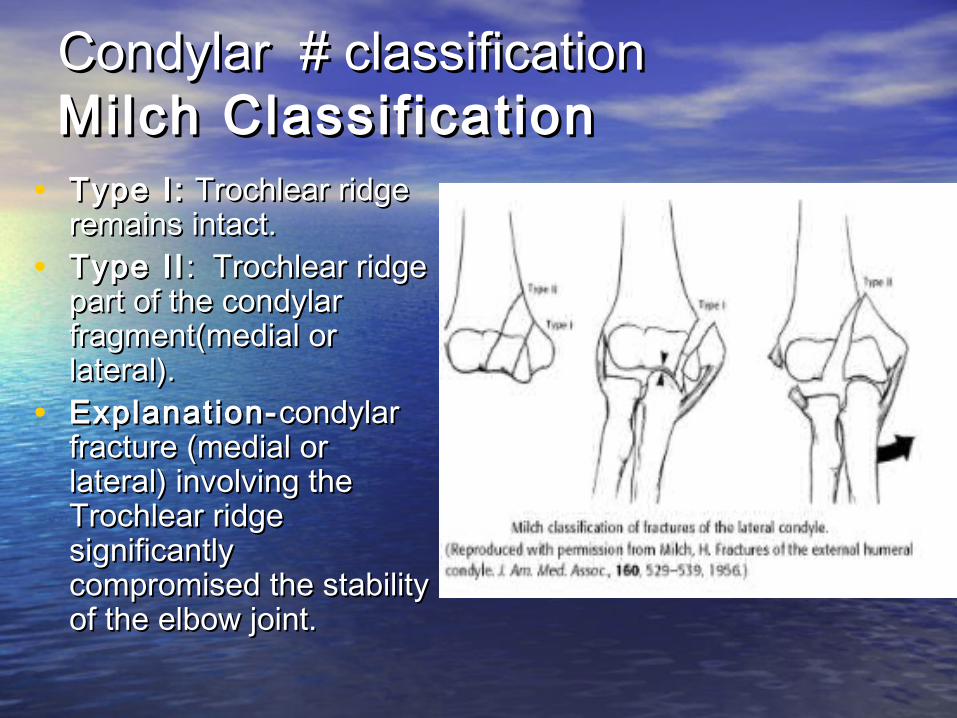
Condylar # classificationCondylar # classificationMilch Classif icationMilch Classif ication
• Type I:Type I: Trochlear ridge Trochlear ridge remains intact.remains intact.
• Type IIType II : Trochlear ridge : Trochlear ridge part of the condylar part of the condylar fragment(medial or fragment(medial or lateral).lateral).
• Explanation-Explanation- condylar condylar fracture (medial or fracture (medial or lateral) involving the lateral) involving the Trochlear ridge Trochlear ridge significantly significantly compromised the stability compromised the stability of the elbow joint.of the elbow joint.
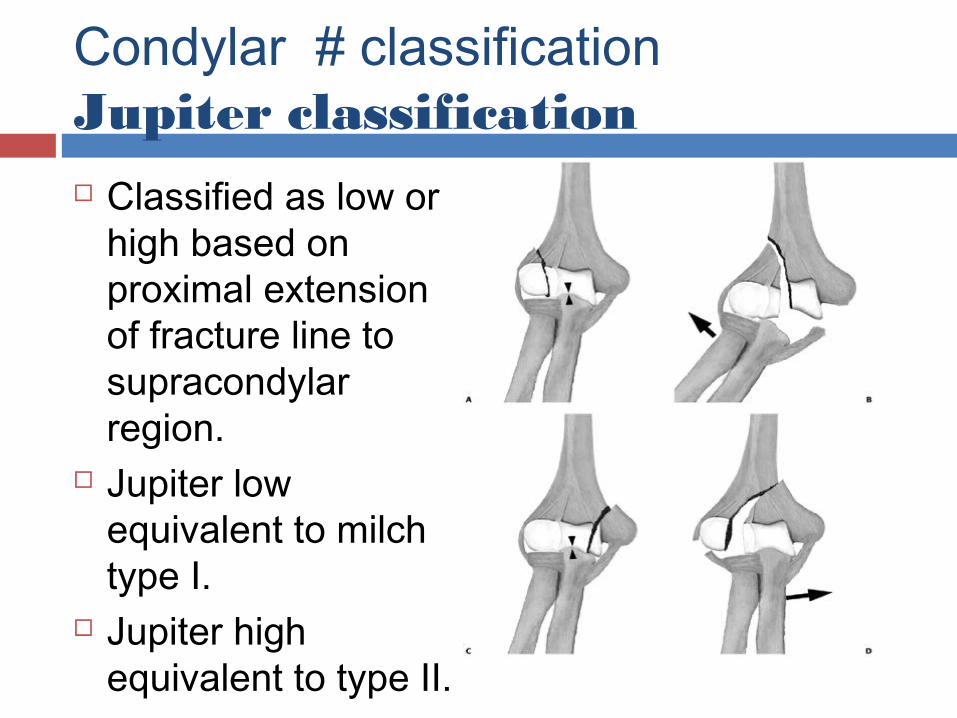
Condylar # classificationJupiter classification Classified as low or
high based on proximal extension of fracture line to supracondylar region.
Jupiter low equivalent to milch type I.
Jupiter high equivalent to type II.
Condylar fracturesCondylar fracturesTreatmentTreatment• Non operative for nondisplaced or minimally Non operative for nondisplaced or minimally
displaced fractures by posterior splintng with displaced fractures by posterior splintng with the elbow flexed to 90* and the forearm in the elbow flexed to 90* and the forearm in supination for lateral condylar # or in supination for lateral condylar # or in pronation for medial condylar #.pronation for medial condylar #.
• Operative is indicated in open or displaced # Operative is indicated in open or displaced # by screw fixation with or without collateral by screw fixation with or without collateral ligament repair.ligament repair.
• Range of motion exercises should be started Range of motion exercises should be started as soon as the patient can tolerate therapy as soon as the patient can tolerate therapy usually after 4 weeks.usually after 4 weeks.
Condylar fracturesCondylar fracturesComplicationsComplications
• Lateral condyle #- Improper reduction or Lateral condyle #- Improper reduction or failure of fixation may result in cubitus failure of fixation may result in cubitus valgus and tardy ulnar nerve palsy.valgus and tardy ulnar nerve palsy.
• Medial condyle #-Medial condyle #- --posttraumatic arthritis,--posttraumatic arthritis, --ulnar nerve symptoms with excess callus --ulnar nerve symptoms with excess callus
formation,formation, --cubitus varus with Improper reduction or --cubitus varus with Improper reduction or
failure of fixation.failure of fixation.
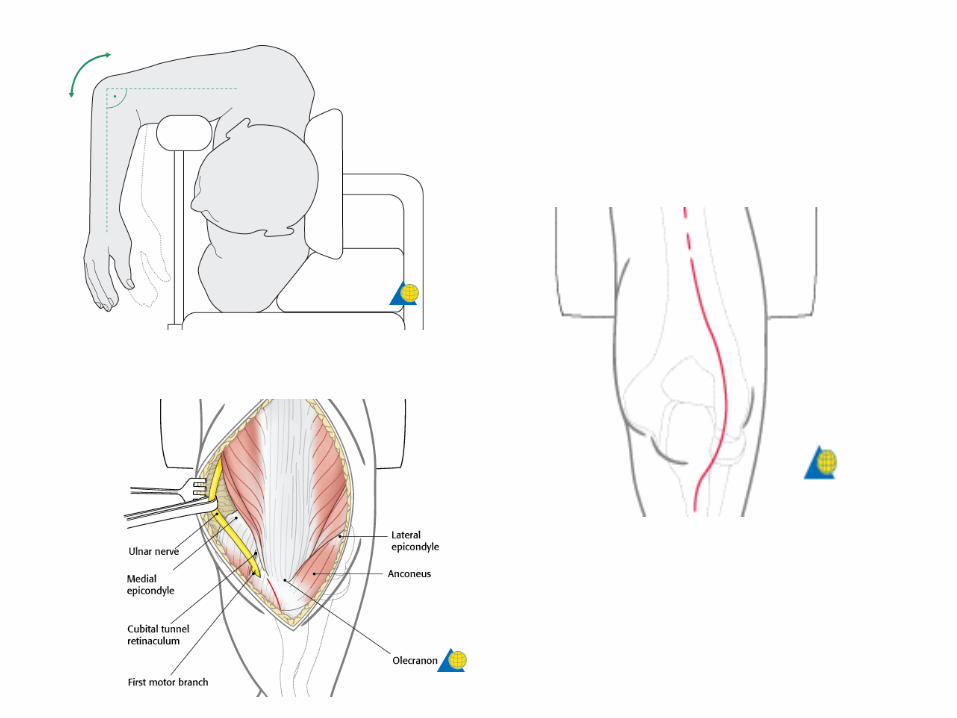
Posterior Approaches to Distal Posterior Approaches to Distal HumerusHumerus• A posterior approach to the elbow can be made A posterior approach to the elbow can be made
with the patient in the lateral decubitus position, with the patient in the lateral decubitus position, with the arm supported by a padded post.with the arm supported by a padded post.
• All posterior approaches use a longitudinal All posterior approaches use a longitudinal midline incision over the posterior aspect of the midline incision over the posterior aspect of the elbow beginning at the junction of the middle elbow beginning at the junction of the middle and distal thirds of the humeral shaft. and distal thirds of the humeral shaft.
• Some surgeons make a straight incision, Some surgeons make a straight incision, whereas others prefer to curve the incision whereas others prefer to curve the incision around the olecranon to the radial side. around the olecranon to the radial side.
• The incision ends over the ulnar The incision ends over the ulnar diaphysis,approximately 5 cm distal to the tip of diaphysis,approximately 5 cm distal to the tip of the olecranon.the olecranon.
• The ulnar nerve should be routinely The ulnar nerve should be routinely identified behind the medial epicondyle, identified behind the medial epicondyle, and protected in all posterior approaches and protected in all posterior approaches to the elbow.to the elbow.
• Extensive dissection of the nerve is Extensive dissection of the nerve is inadvisable, as this increases the risk of inadvisable, as this increases the risk of tethering and damage to its vascularity.tethering and damage to its vascularity.
• However, adequate exposure of the nerve However, adequate exposure of the nerve is required to reduce the risk of its injury if is required to reduce the risk of its injury if olecranon osteotomy or insertion of olecranon osteotomy or insertion of hardware is required.hardware is required.
• There are several variations of approach to There are several variations of approach to gain access to the posterior aspect of the distal gain access to the posterior aspect of the distal humerus,there are four main types of posterior humerus,there are four main types of posterior approach:-approach:-
• Olecranon Osteotomy,Olecranon Osteotomy,• Triceps-sparing Approach,Triceps-sparing Approach,• Triceps-Split t ing Approach,Triceps-Split t ing Approach,• Triceps-Reflecting Approach.Triceps-Reflecting Approach.
Olecranon OsteotomyOlecranon OsteotomyMACAUSLAND & MULLER’S MACAUSLAND & MULLER’S APPROACHAPPROACH
• Reflection of the triceps tendon and its bony insertion, by Reflection of the triceps tendon and its bony insertion, by use of an olecranon osteotomy, most widely used use of an olecranon osteotomy, most widely used approach to the elbow.approach to the elbow.
• The triceps insertion is isolated and the joint surfaces on The triceps insertion is isolated and the joint surfaces on either side of the trochlear notch are identified by either side of the trochlear notch are identified by opening joint capsule.opening joint capsule.
• An elevator or gauze swab is then inserted from medial An elevator or gauze swab is then inserted from medial to lateral through the joint across the notch.to lateral through the joint across the notch.
• This serves to protect the articular surfaces during the This serves to protect the articular surfaces during the subsequent osteotomy, and also facilitates the accurate subsequent osteotomy, and also facilitates the accurate placement of the osteotomyplacement of the osteotomy..

--The approach initially recommended by the AO group was an extra-articular oblique osteotomy of the olecranon, although the approach more commonly used is an intra-articular osteotomy, through the mid-portion of the greater sigmoid notch.--The osteotomy must be proximal to the coronoid process, to provide a balance between an osteotomy that is too small, which may compromise the exposure of the articular surfaces, and one that is too large, which may cause an inadvertent osteotomy at the level of the coronoid and destabilize the elbow.--Predrilling and tapping of the olecranon should be performed if screw fixation of the osteotomy is planned.
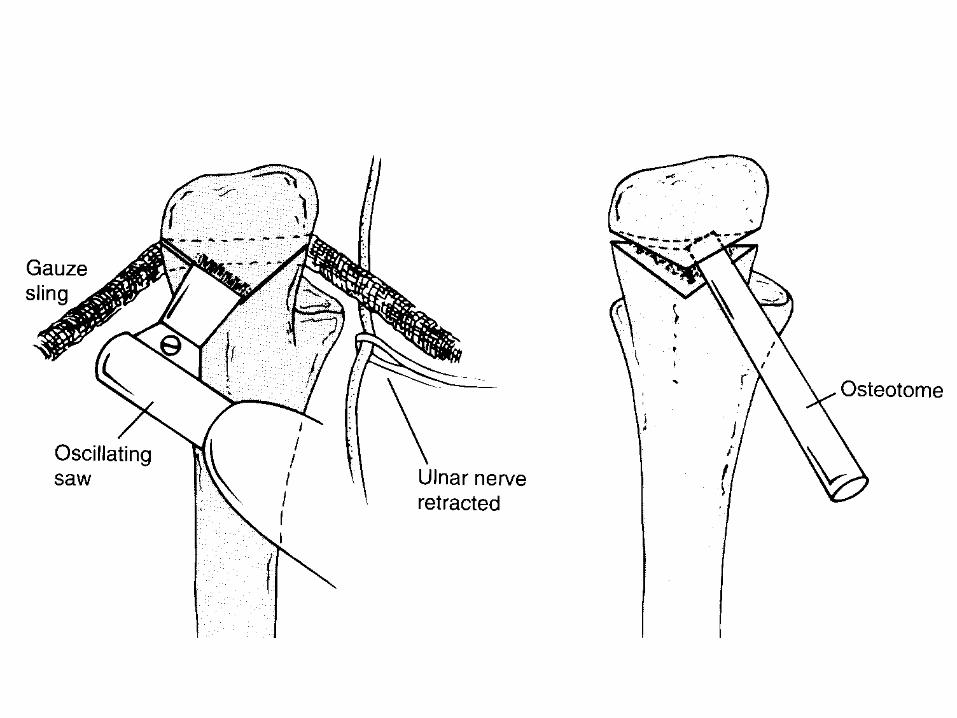
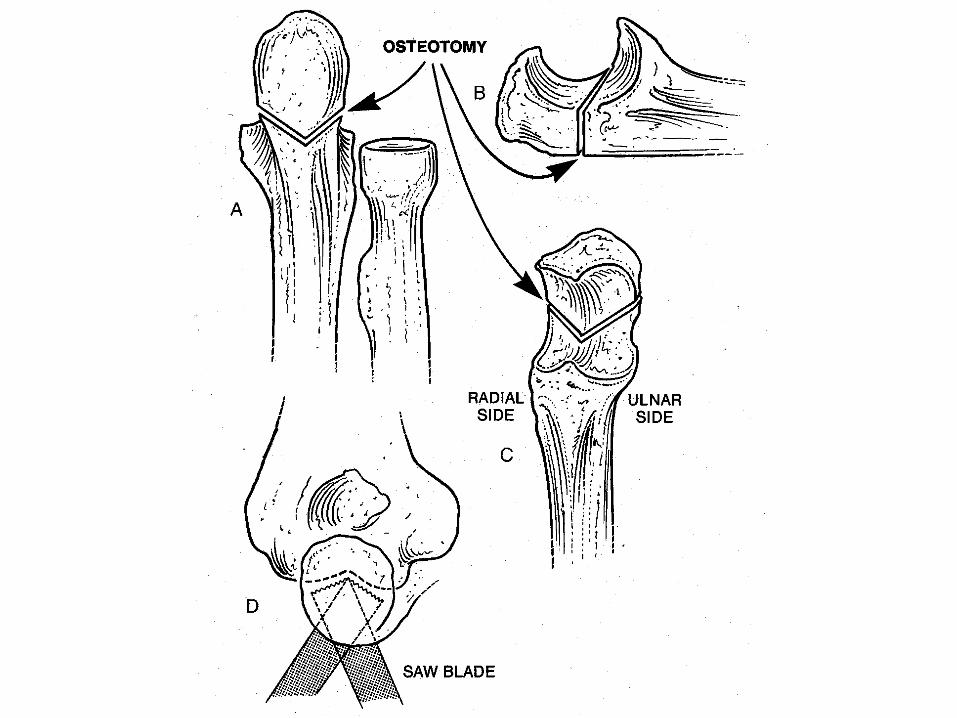

--The osteotomy should be performed as a chevron, with its apex directed distally, perpendicular to the long axis of the shaft of the ulna.--The chevron facilitates reduction and fixation of the osteotomy and also provides a greater surface area of cancellous bone over which healing can occur. --The osteotomy is performed using a narrow saw and completed using an osteotome, to “crack” through the articular surface.--This maneuver facilitates subsequent anatomic reconstruction of the osteotomy fragments.--At the completion of surgery, the osteotomy can be secured either with an intramedullary 6.5-mm, partially threaded cancellous screw, or using two K-wires and a tension-banding technique.
• The approach has the advantage of providing The approach has the advantage of providing excellent access to the whole of the distal excellent access to the whole of the distal humerus, especially to view the distal posterior humerus, especially to view the distal posterior articular surfaces.articular surfaces.
• It provides only limited exposure of the It provides only limited exposure of the capitellum, but its major drawback is the capitellum, but its major drawback is the postoperative morbidity, which is associated postoperative morbidity, which is associated with the internal fixation of the osteotomy.with the internal fixation of the osteotomy.
Triceps-Sparing approachTriceps-Sparing approachBryan-Morrey approachBryan-Morrey approach
– Posterior Midline incision,Posterior Midline incision,– Ulnar nerve identified and mobilized,Ulnar nerve identified and mobilized,– Medial edge of triceps and distal forearm fascia Medial edge of triceps and distal forearm fascia
elevated as single unit off olecranon and reflected elevated as single unit off olecranon and reflected laterally,laterally,
– Resection of extra-articular tip of olecranon.Resection of extra-articular tip of olecranon.
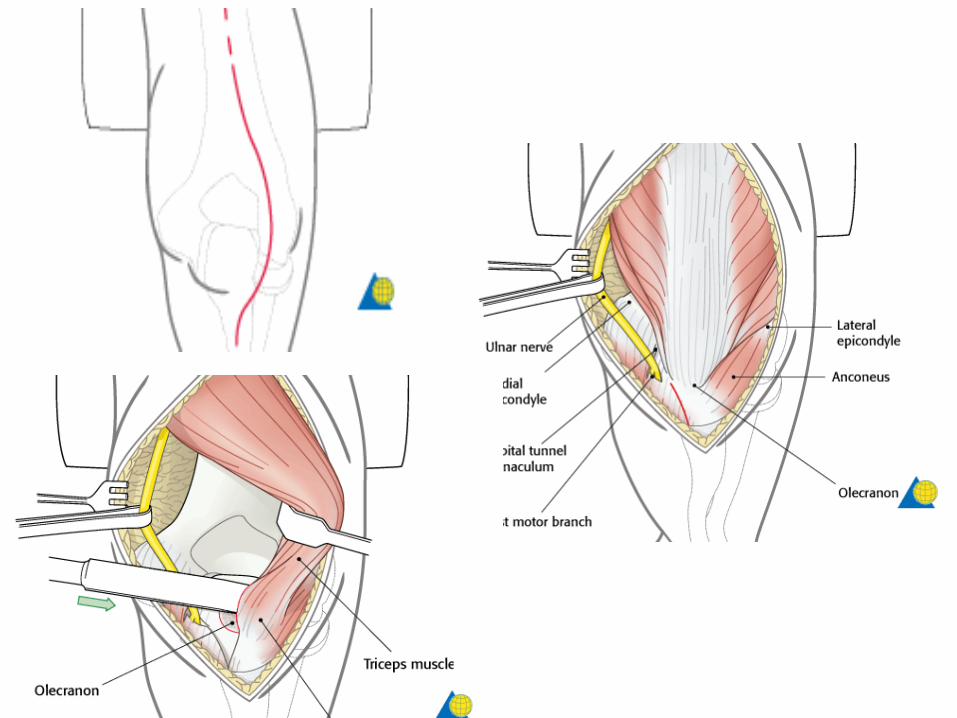
• Incise the fascia over the flexor carpi ulnaris muscle at Incise the fascia over the flexor carpi ulnaris muscle at the border of the ulnar bone, as the first step in the border of the ulnar bone, as the first step in the preparation of the extensor apparatus flap.the preparation of the extensor apparatus flap.
• The fascia is detached subperiosteally from the ulna The fascia is detached subperiosteally from the ulna towards the radial side.towards the radial side.
• At the level of the olecranon the extensor apparatus is At the level of the olecranon the extensor apparatus is detached together with a sliver of bone using a fine detached together with a sliver of bone using a fine chisel.chisel.
• Proximal to the olecranon the posterior capsule is Proximal to the olecranon the posterior capsule is incised.incised.
• At the level of the humerus the extensor muscles are At the level of the humerus the extensor muscles are freed from the bone.freed from the bone.
• Now the entire extensor apparatus flap can be retracted Now the entire extensor apparatus flap can be retracted to the radial side.to the radial side.
• To enhance visualization of the articular surface, the To enhance visualization of the articular surface, the elbow should be flexed beyond 100 degrees.elbow should be flexed beyond 100 degrees.
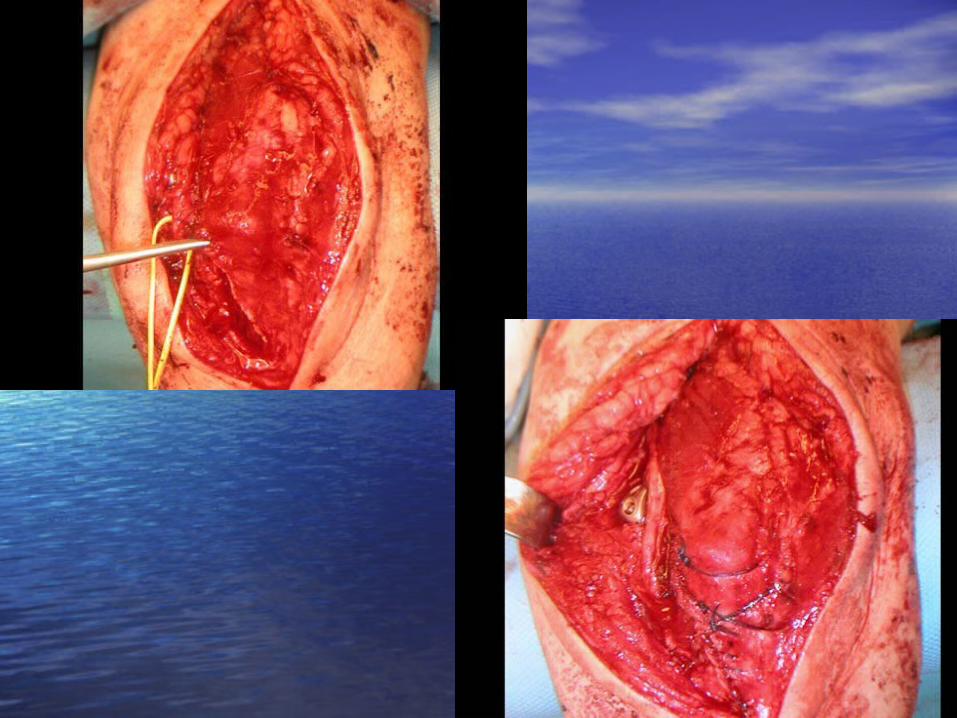
• For closure, the extensor apparatus is pulled For closure, the extensor apparatus is pulled into place using a clamp.into place using a clamp.
• Some surgeons place the ulnar nerve back in Some surgeons place the ulnar nerve back in the cubital tunnel, whereas other surgeons the cubital tunnel, whereas other surgeons perform an anterior subcutaneous perform an anterior subcutaneous transposition.transposition.
• The bone sliver is reattached to the The bone sliver is reattached to the olecranon with transosseous sutures.olecranon with transosseous sutures.
• Distally, the incision of the flexor carpi ulnaris Distally, the incision of the flexor carpi ulnaris fascia is closed.fascia is closed.
Triceps-Splitt ing ApproachesTriceps-Splitt ing ApproachesCampbell approachCampbell approach• The triceps-splitting approach has been The triceps-splitting approach has been
developed to attempt to overcome the morbidity developed to attempt to overcome the morbidity associated with the use of olecranon osteotomy.associated with the use of olecranon osteotomy.
• It is made by fashioning a direct midline It is made by fashioning a direct midline posterior split in the triceps.posterior split in the triceps.
• Distally sharp dissection is used to reflect the Distally sharp dissection is used to reflect the triceps insertion off the olecranon and proximal triceps insertion off the olecranon and proximal ulna medially and laterally .ulna medially and laterally .
• A thin wafer of bone may be detached from the A thin wafer of bone may be detached from the olecranon at the level of the triceps insertion.olecranon at the level of the triceps insertion.
• The triceps may also be detached as a distally The triceps may also be detached as a distally based “tongue” muscle flap with splitting of only based “tongue” muscle flap with splitting of only its deeper portion.its deeper portion.
• The limited access to the joint surfaces The limited access to the joint surfaces can be improved by flexing the elbow and can be improved by flexing the elbow and grasping and posteriorly retracting the grasping and posteriorly retracting the olecranon with reduction forceps.olecranon with reduction forceps.
• Meticulous repair of the tendon through Meticulous repair of the tendon through drill holes in the olecranon must be drill holes in the olecranon must be performed at the conclusion of surgery, to performed at the conclusion of surgery, to minimize the risk of triceps tendon pull-off.minimize the risk of triceps tendon pull-off.
• This approach does not appear to be detrimental This approach does not appear to be detrimental to elbow function and reduces the risk of later to elbow function and reduces the risk of later hardware complications, encountered with the hardware complications, encountered with the use of an olecranon osteotomy.use of an olecranon osteotomy.
• Another major advantage of this approach is that Another major advantage of this approach is that it allows greater intraoperative flexibility, it allows greater intraoperative flexibility, because either internal fixation or total elbow because either internal fixation or total elbow arthroplasty (TER) can be performed.arthroplasty (TER) can be performed.
• This is particularly useful if there is uncertainty This is particularly useful if there is uncertainty as to whether reduction and internal fixation of as to whether reduction and internal fixation of the fracture will be technically feasible, and TER the fracture will be technically feasible, and TER might be required.might be required.
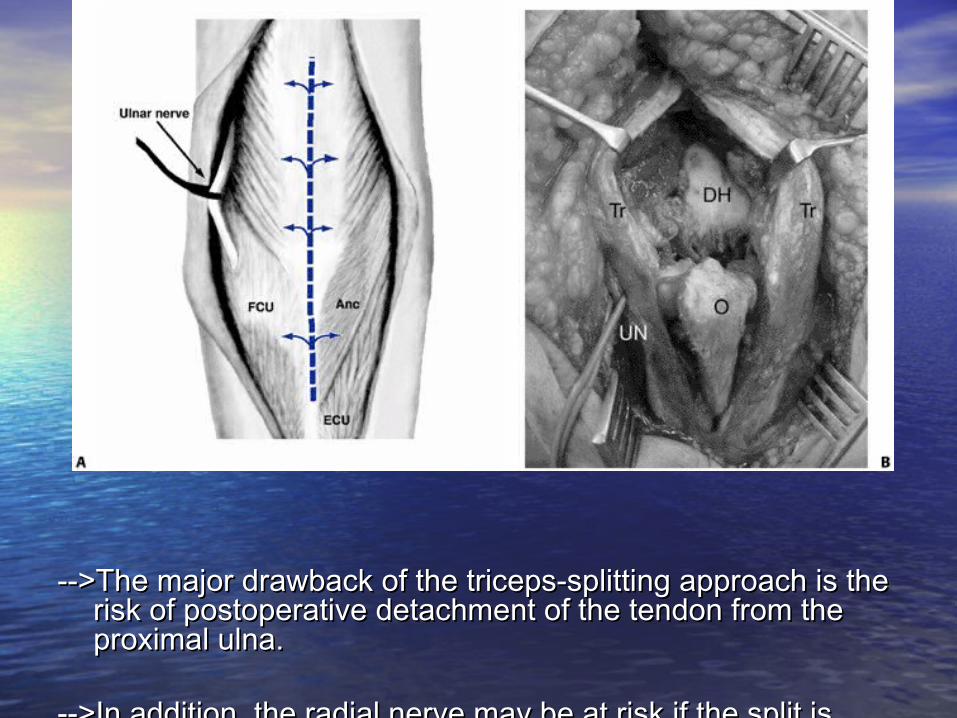
-->The major drawback of the triceps-splitting approach is the -->The major drawback of the triceps-splitting approach is the risk of postoperative detachment of the tendon from the risk of postoperative detachment of the tendon from the proximal ulna.proximal ulna.
-->In addition, the radial nerve may be at risk if the split is -->In addition, the radial nerve may be at risk if the split is continued too far proximally, and care must be taken to continued too far proximally, and care must be taken to avoid this.avoid this.
Triceps-Reflecting Triceps-Reflecting ApproachesApproaches• The approach has been used less frequently for The approach has been used less frequently for
open reduction with internal fixation (ORIF), open reduction with internal fixation (ORIF), because of the limited exposure of the lateral because of the limited exposure of the lateral column that it provides,and it should only be column that it provides,and it should only be used if the surgeon is convinced that a TER will used if the surgeon is convinced that a TER will be required.be required.
• The whole of the triceps is reflected as a The whole of the triceps is reflected as a continuous cuff of tissue, from medial to lateral.continuous cuff of tissue, from medial to lateral.
• The medial aspect of the triceps is sharply The medial aspect of the triceps is sharply reflected off the proximal ulna at its insertion, reflected off the proximal ulna at its insertion, taking care to only continue dissection until taking care to only continue dissection until adequate exposure of the joint has been adequate exposure of the joint has been obtained.obtained.
• Several variations of this approach have been Several variations of this approach have been described:-described:-
--As originally described there is a risk of ulnar --As originally described there is a risk of ulnar nerve palsy from retraction during surgery. To nerve palsy from retraction during surgery. To protect against this the triceps may be split so protect against this the triceps may be split so that 75% of the muscle lies laterally and 25% that 75% of the muscle lies laterally and 25% medially .medially .
The triceps is then reflected laterally as for the The triceps is then reflected laterally as for the standard technique. The ulnar nerve and its standard technique. The ulnar nerve and its blood supply are protected from traction injury blood supply are protected from traction injury by the medial triceps during surgery.by the medial triceps during surgery.
--A wafer of bone carrying the triceps insertion --A wafer of bone carrying the triceps insertion may be detached, to facilitate later closure. The may be detached, to facilitate later closure. The triceps is then reflected laterally as an “osteo-triceps is then reflected laterally as an “osteo-anconeus flap” to provide exposure of the lateral anconeus flap” to provide exposure of the lateral column.column.
As with the triceps-splitting approach, careful repair of As with the triceps-splitting approach, careful repair of
the triceps tendon through drill holes is required to the triceps tendon through drill holes is required to reduce the risk of postoperative tendon pull-off.reduce the risk of postoperative tendon pull-off.
ORIF WITH PLATINGORIF WITH PLATINGPRINCIPLESPRINCIPLES
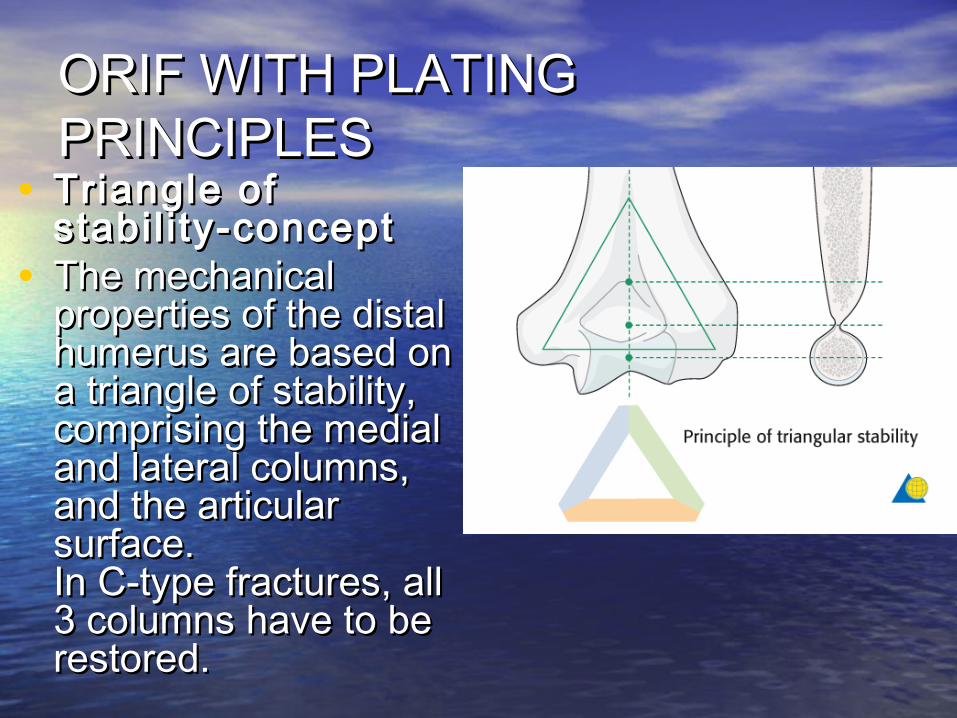
• Triangle of Triangle of stabil i ty-conceptstabil i ty-concept
• The mechanical The mechanical properties of the distal properties of the distal humerus are based on humerus are based on a triangle of stability, a triangle of stability, comprising the medial comprising the medial and lateral columns, and lateral columns, and the articular and the articular surface.surface.In C-type fractures, all In C-type fractures, all 3 columns have to be 3 columns have to be restored.restored.
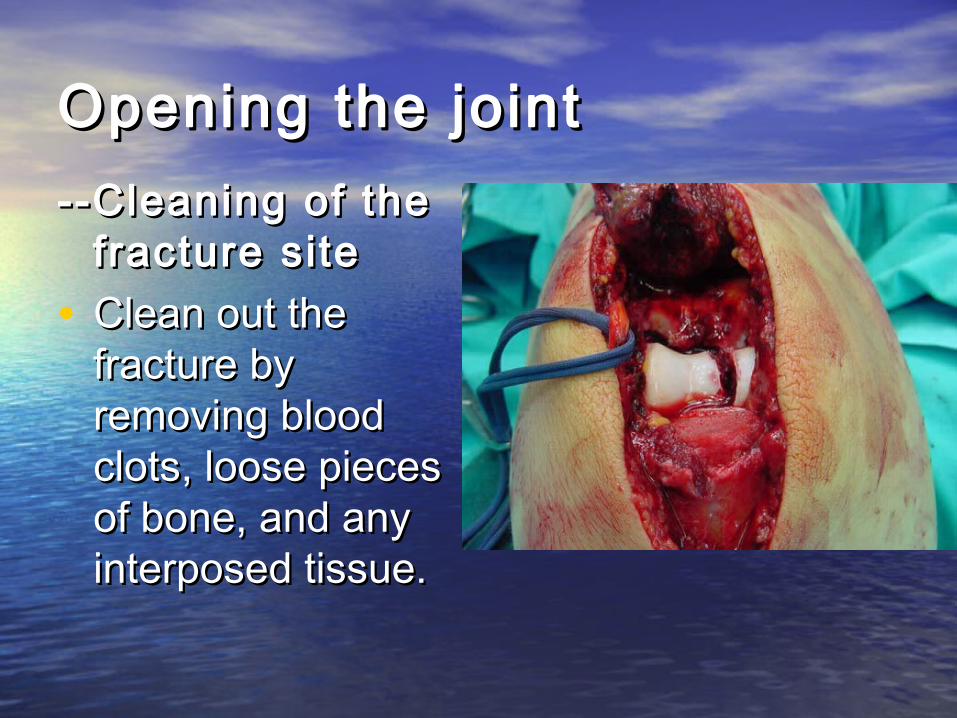
Opening the jointOpening the joint--Cleaning of the --Cleaning of the
fracture sitefracture site• Clean out the Clean out the
fracture by fracture by removing blood removing blood clots, loose pieces clots, loose pieces of bone, and any of bone, and any interposed tissue.interposed tissue.
Reconstruction of the Reconstruction of the art icular surfacearticular surface
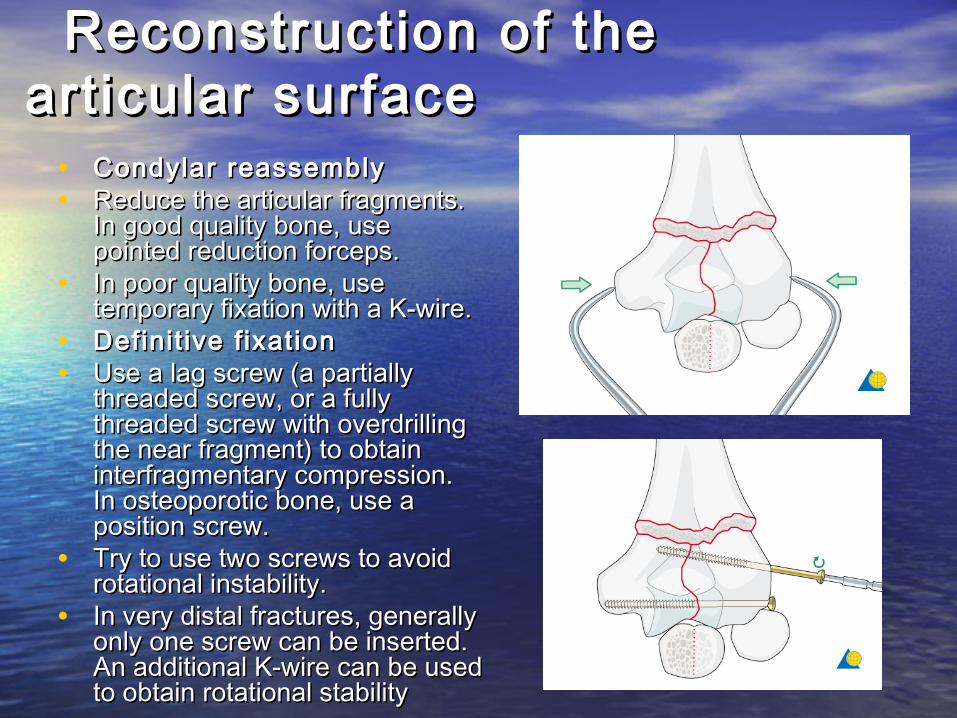
• Condylar reassemblyCondylar reassembly• Reduce the articular fragments. Reduce the articular fragments.
In good quality bone, use In good quality bone, use pointed reduction forceps.pointed reduction forceps.
• In poor quality bone, use In poor quality bone, use temporary fixation with a K-wire.temporary fixation with a K-wire.
• Definit ive fixationDefinit ive fixation• Use a lag screw (a partially Use a lag screw (a partially
threaded screw, or a fully threaded screw, or a fully threaded screw with overdrilling threaded screw with overdrilling the near fragment) to obtain the near fragment) to obtain interfragmentary compression.interfragmentary compression.In osteoporotic bone, use a In osteoporotic bone, use a position screw.position screw.
• Try to use two screws to avoid Try to use two screws to avoid rotational instability.rotational instability.
• In very distal fractures, generally In very distal fractures, generally only one screw can be inserted.only one screw can be inserted.An additional K-wire can be used An additional K-wire can be used to obtain rotational stabilityto obtain rotational stability
Condylar reattachmentCondylar reattachment
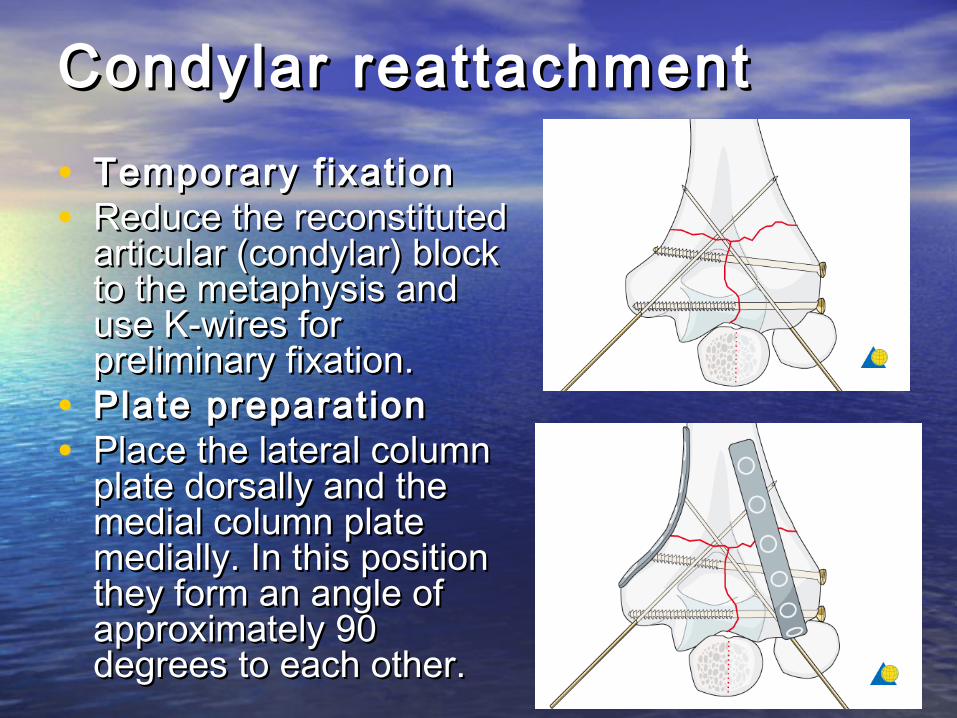
• Temporary fixationTemporary fixation• Reduce the reconstituted Reduce the reconstituted
articular (condylar) block articular (condylar) block to the metaphysis and to the metaphysis and use K-wires for use K-wires for preliminary fixation.preliminary fixation.
• Plate preparationPlate preparation• Place the lateral column Place the lateral column
plate dorsally and the plate dorsally and the medial column plate medial column plate medially. In this position medially. In this position they form an angle of they form an angle of approximately 90 approximately 90 degrees to each other.degrees to each other.
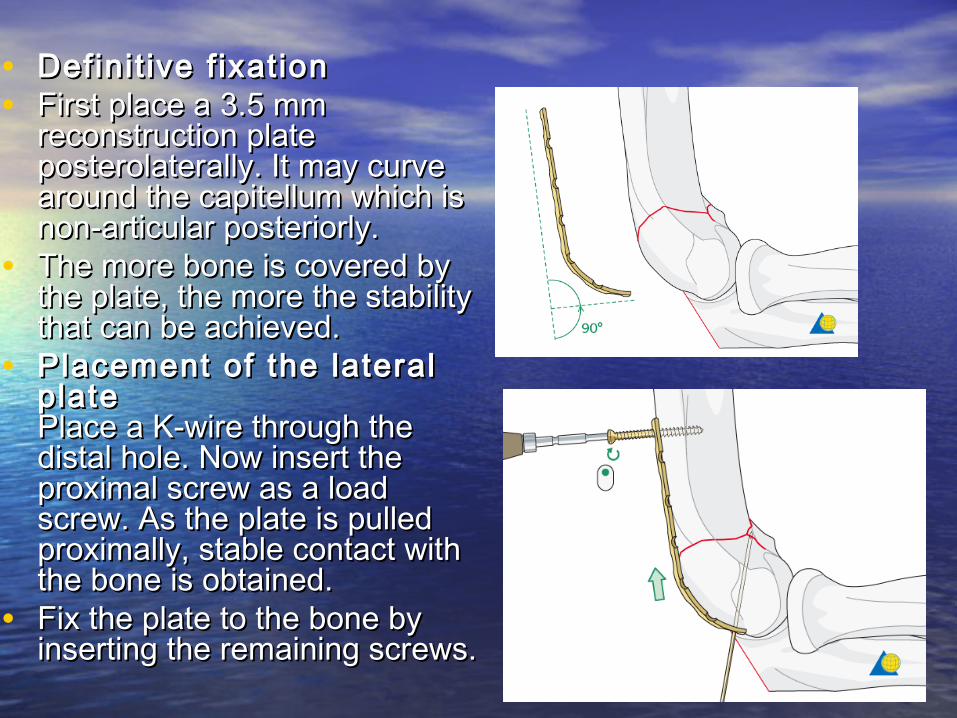
• Definit ive f ixationDefinit ive f ixation• First place a 3.5 mm First place a 3.5 mm
reconstruction plate reconstruction plate posterolaterally. It may curve posterolaterally. It may curve around the capitellum which is around the capitellum which is non-articular posteriorly.non-articular posteriorly.
• The more bone is covered by The more bone is covered by the plate, the more the stability the plate, the more the stability that can be achieved.that can be achieved.
• Placement of the lateral Placement of the lateral plateplatePlace a K-wire through the Place a K-wire through the distal hole. Now insert the distal hole. Now insert the proximal screw as a load proximal screw as a load screw. As the plate is pulled screw. As the plate is pulled proximally, stable contact with proximally, stable contact with the bone is obtained.the bone is obtained.
• Fix the plate to the bone by Fix the plate to the bone by inserting the remaining screws.inserting the remaining screws.
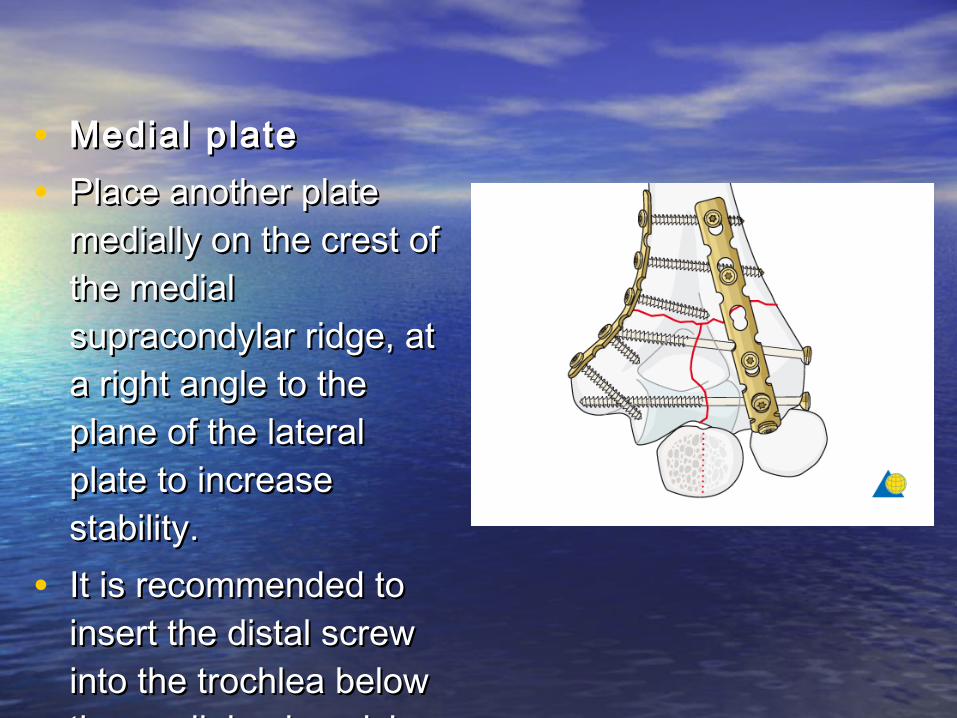
• Medial plateMedial plate• Place another plate Place another plate
medially on the crest of medially on the crest of the medial the medial supracondylar ridge, at supracondylar ridge, at a right angle to the a right angle to the plane of the lateral plane of the lateral plate to increase plate to increase stability.stability.
• It is recommended to It is recommended to insert the distal screw insert the distal screw into the trochlea below into the trochlea below the medial epicondyle.the medial epicondyle.
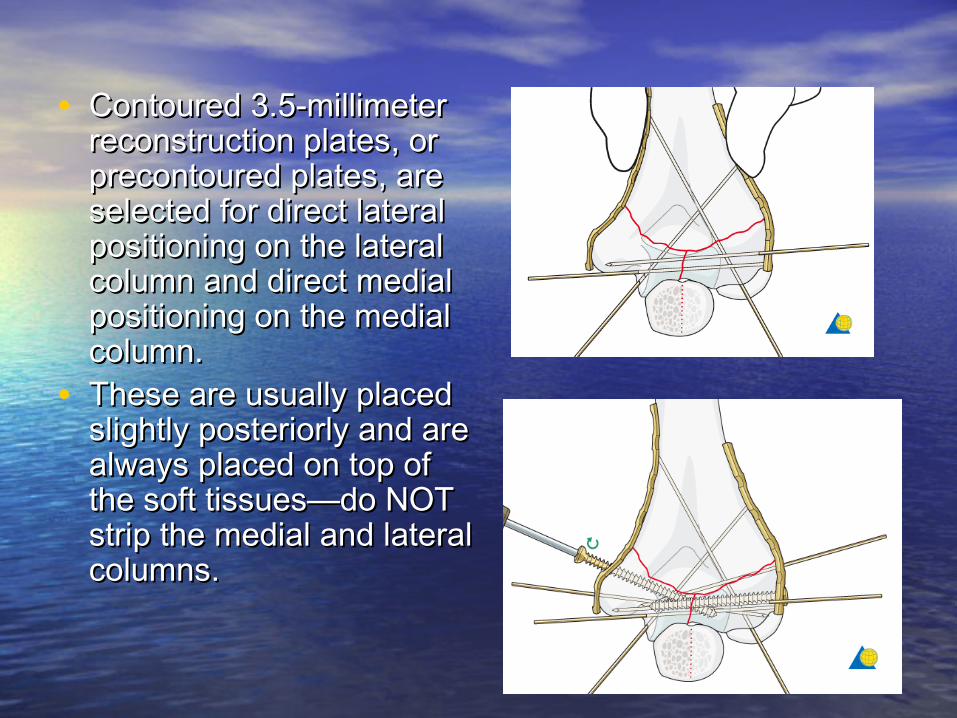
• Contoured 3.5-millimeter Contoured 3.5-millimeter reconstruction plates, or reconstruction plates, or precontoured plates, are precontoured plates, are selected for direct lateral selected for direct lateral positioning on the lateral positioning on the lateral column and direct medial column and direct medial positioning on the medial positioning on the medial column.column.
• These are usually placed These are usually placed slightly posteriorly and are slightly posteriorly and are always placed on top of always placed on top of the soft tissues—do NOT the soft tissues—do NOT strip the medial and lateral strip the medial and lateral columns.columns.
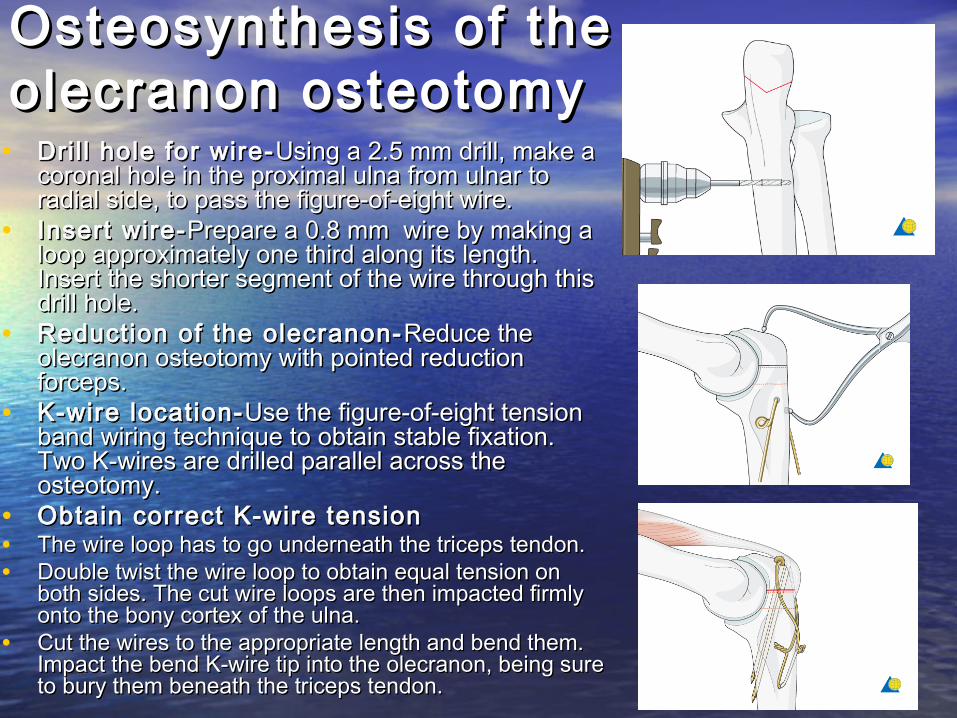
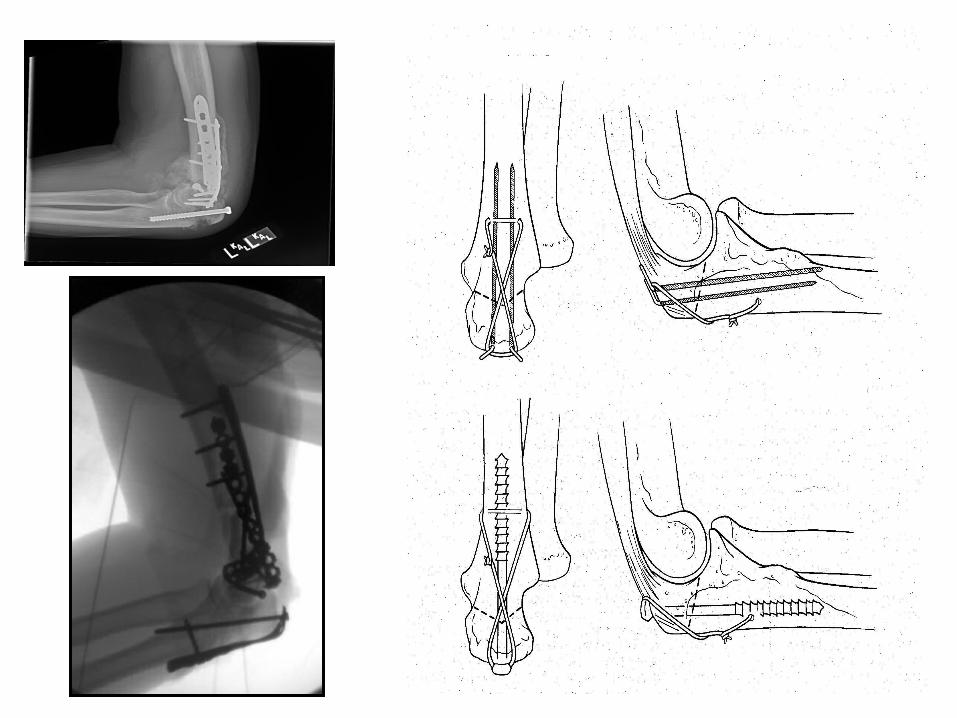
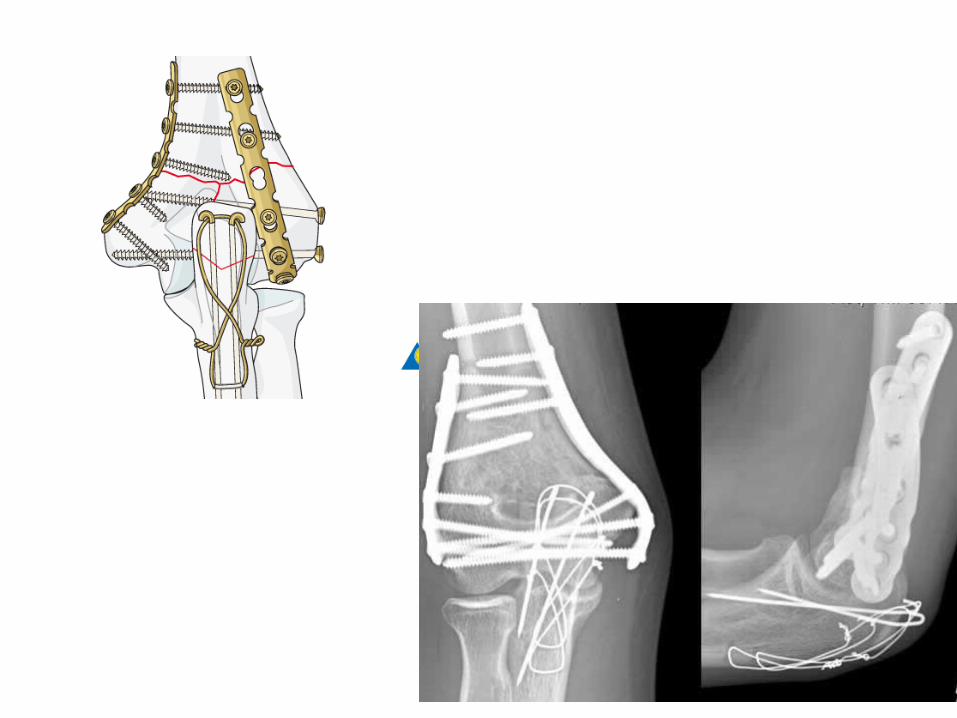
Osteosynthesis of the Osteosynthesis of the olecranon osteotomyolecranon osteotomy
• Drill hole for wire-Dril l hole for wire- Using a 2.5 mm drill, make a Using a 2.5 mm drill, make a coronal hole in the proximal ulna from ulnar to coronal hole in the proximal ulna from ulnar to radial side, to pass the figure-of-eight wire.radial side, to pass the figure-of-eight wire.
• Insert wire-Insert wire- Prepare a 0.8 mm wire by making a Prepare a 0.8 mm wire by making a loop approximately one third along its length. loop approximately one third along its length. Insert the shorter segment of the wire through this Insert the shorter segment of the wire through this drill hole.drill hole.
• Reduction of the olecranon-Reduction of the olecranon- Reduce the Reduce the olecranon osteotomy with pointed reduction olecranon osteotomy with pointed reduction forceps.forceps.
• K-wire location-K-wire location- Use the figure-of-eight tension Use the figure-of-eight tension band wiring technique to obtain stable fixation. band wiring technique to obtain stable fixation. Two K-wires are drilled parallel across the Two K-wires are drilled parallel across the osteotomy.osteotomy.
• Obtain correct K-wire tensionObtain correct K-wire tension• The wire loop has to go underneath the triceps tendon.The wire loop has to go underneath the triceps tendon.• Double twist the wire loop to obtain equal tension on Double twist the wire loop to obtain equal tension on
both sides. The cut wire loops are then impacted firmly both sides. The cut wire loops are then impacted firmly onto the bony cortex of the ulna.onto the bony cortex of the ulna.
• Cut the wires to the appropriate length and bend them. Cut the wires to the appropriate length and bend them. Impact the bend K-wire tip into the olecranon, being sure Impact the bend K-wire tip into the olecranon, being sure to bury them beneath the triceps tendon.to bury them beneath the triceps tendon.
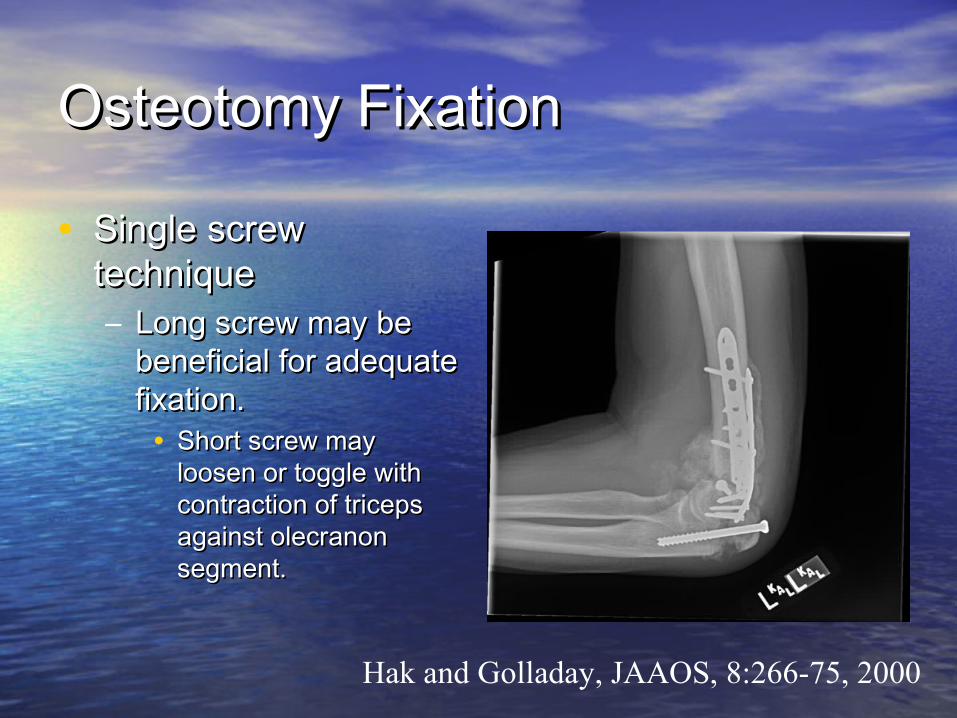
Osteotomy FixationOsteotomy Fixation
• Single screw Single screw techniquetechnique– Long screw may be Long screw may be
beneficial for adequate beneficial for adequate fixation.fixation.• Short screw may Short screw may
loosen or toggle with loosen or toggle with contraction of triceps contraction of triceps against olecranon against olecranon segment.segment.
Hak and Golladay, JAAOS, 8:266-75, 2000
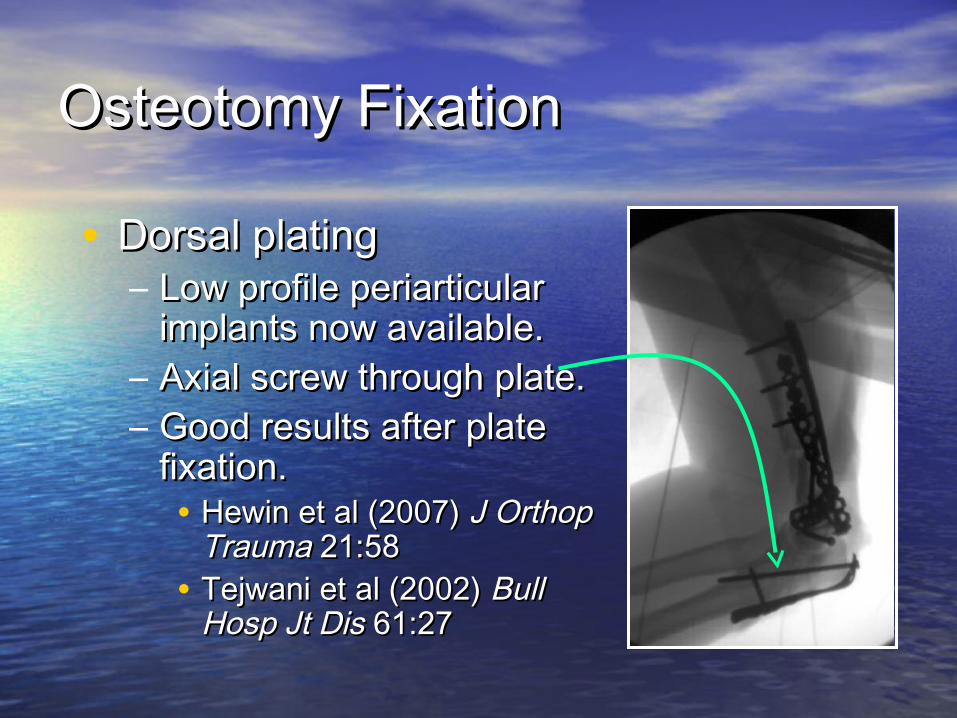
Osteotomy FixationOsteotomy Fixation
• Dorsal platingDorsal plating– Low profile periarticular Low profile periarticular
implants now available.implants now available.– Axial screw through plate.Axial screw through plate.– Good results after plate Good results after plate
fixation.fixation.• Hewin et al (2007) Hewin et al (2007) J Orthop J Orthop
TraumaTrauma 21:58 21:58• Tejwani et al (2002) Tejwani et al (2002) Bull Bull
Hosp Jt DisHosp Jt Dis 61:27 61:27
THANK YOU…..!!!!!THANK YOU…..!!!!!