- 1. Guillain-Barr syndrome (GBS) is an acute, frequentlysevere,
and fulminant polyradiculoneuropathy that isautoimmune in nature.
Males are at slightly higher risk for GBS than females,and in
Western countries adults are more frequentlyaffected than
children.
2. Subtypes 3. Antecedent events Approximately 70% of cases of
GBS occur 13 weeks after anacute infectious process, usually
respiratory orgastrointestinal. Viruses e.g human herpes virus
infection, CMV, Epstein-Barr virus and Mycoplasma pneumoniae;
Infection or reinfection with Campylobacter jejuni ,
recentimmunizations. The swine influenza vaccine, administered
widely in theUnited States in 1976, is the most notable example.
Older-type rabies vaccine, prepared in nervous systemtissue, the
mechanism is presumably immunization againstneural antigens. 4. GBS
occurs more frequently in patients with lymphoma (including
Hodgkins disease), HIV-seropositive individuals, Patients with
systemic lupus erythematosus. C. jejuni has been implicated in
summer outbreaks of AMAN among children and young adults exposed to
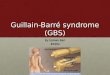
chickens in rural China. 5. Panel A shows the immunopathogenesis of
acuteinflammatory demyelinating polyneuropathy. Autoantigens
unequivocally identified, autoantibodiesbind to myelin antigens and
activate complement. Formation of membrane- attack complex (MAC)
onthe outer surface of Schwann cells and the initiation ofvesicular
degeneration. Macrophages subsequently invade myelin and act
asscavengers to remove myelin debris. 6. Panel B shows the
immunopathogenesis of acutemotor axonal neuropathy. Myelinated
axons are divided into four functionalregions: the nodes of
Ranvier, paranodes,juxtaparanodes, and internodes. Gangliosides GM1
and GD1a are strongly expressed atthe nodes of Ranvier, where the
voltage-gated sodium(Nav) channels are localized. Contactin
associated protein (Caspr) and voltage-gated potassium (Kv)
channels are respectively presentat the paranodes and
juxtaparanodes. 7. IgG anti-GM1 or anti-GD1a autoantibodies bind to
thenodal axolemma, leading to MAC formation. Results in the
disappearance of Nav clusters and thedetachment of paranodal
myelin, which can lead tonerve-conduction failure and muscle
weakness. Axonal degeneration may follow at a later stage.
Macrophages subsequently invade from the nodes intothe periaxonal
space, scavenging the injured axons. 8. Neuropathies 9.
Gangliosides 10. Gangliosides, which are composed of a
ceramideattached to one or more sugars (hexoses) and containsialic
acid (N-acetylneuraminic acid) are importantcomponents of the
peripheral nerves. Four gangliosides GM1, GD1a, GT1a, and GQ1b
differwith regard to the number and position of their sialicacids,
where M, D, T, and Q represent mono-, di-, tri-,and quadri-sialosyl
groups. 11. IgG autoantibodies to GM1 and GD1a are associated
withacute motor axonal neuropathy and its subtypes; Subtypes More
extensive acute motor-sensory axonal neuropathy Less extensive
acute motor conduction-block neuropathy,not with acute inflammatory
demyelinatingpolyneuropathy. Motor and sensory nerves express
similar quantities of GM1and GD1a, but their expression within
various tissues maydiffer. This explains the preferential motor
axon injury seen inacute motor axonal neuropathy 12. IgG
autoantibodies to GQ1b, which cross-react withGT1a, are strongly
associated with the Miller Fishersyndrome. Patients with
pharyngealcervicalbrachial weakness More likely to have IgG
anti-GT1a antibodies, whichmay cross-react with GQ1b, Less likely
to have IgG anti-GD1a antibodies, whichsuggests a link to the
axonal GuillainBarr syndrome Glossopharyngeal and vagus nerves
strongly expressGT1a and GQ1b, possibly accounting for dysphagia
inthis subtype. 13. Guillain-Barr syndrome (GBS), Miller Fisher
syndrome (FS) andBickerstaff brainstem encephalitis represent a
spectrum of acutepost-infectious immune-mediated diseases. Miller
Fisher syndrome (MFS) is characterized by an acute onsetof ataxia,
areflexia without weakness and ophthalmoplegia. Miller Fisher
syndrome (MFS) can be broadly categorized in totwo part, More
extensive form, Bickerstaff brainstem encephalitis
(BBE)characterized by Miller Fisher syndrome with impairment
ofconsciousness 14. Incomplete form Acute ophthalmoparesis without
ataxia Acute onset ataxia neuropathy withoutophthalmoplegia
Anti-GQ1b antibody syndrome includes Miller Fisher syndrome, Acute
ophthalmoparesis, without ataxia Acute ataxic neuropathy, without
ophthalmoplegia Bickerstaffs brain-stem encephalitis
Pharyngealcervicalbrachial weakness. 15. Anti-GQ1b IgG antibodies
are found in >90% of patientswith MFS and titers of IgG are
highest early in the course. GQ1b is strongly expressed in the
oculomotor, trochlear,and abducens nerves, and muscle spindles in
the limbs. EO motor nerves are enriched in GQ1b gangliosides
incomparison to limb nerves. Pharyngealcervicalbrachial weakness
categorized aslocalized form of acute motor axonal neuropathy or
anextensive form of the Miller Fisher syndrome. Half of patients of
pharyngealcervicalbrachial weaknesshave IgG anti-GT1a antibodies,
which often cross-react withGQ1b. 16. Clinical symptoms Rapidly
evolving hypo to areflexic motor paralysis withor without sensory
disturbance. Although hyporeflexia or areflexia is a hallmark of
theGBS, 10% of patients have normal or brisk reflexesduring the
course of illness. Ascending paralysis, noticed as rubbery legs.
The legs are usually more affected than the arms. Facial diparesis
is present in 50% of affectedindividuals. 17. The lower cranial
nerves frequently involved, causingbulbar weakness. Mistaken for
brainstem ischemia. Bladder dysfunction may occur in severe cases
but isusually transient. Autonomic involvement is common Loss of
vasomotor control with wide fluctuation inblood pressure, postural
hypotension, and cardiacdysrhythmias. 18. Fever and constitutional
symptoms are absent Deep tendon reflexes attenuate or disappear
withinthe first few days of onset Functions subserved by large
sensory fibers, such asdeep tendon reflexes and proprioception, are
affected. 19. Diagnostic criteria 20. GBS disability score 0, A
healthy state; 1, Minor symptoms and capable of running; 2, Able to
walk 10 meters or more without assistancebut unable to run; 3, Able
to walk 10 meters across an open space withhelp; 4, Bedridden or
chair bound; 5, Requiring assisted ventilation for at least part of
theday; 6, Dead. 21. Criteria for mechanical ventilationin absence
of clinical respiratorydistress Major Hypercarbia (partial pressure
> 48 mm hg) Hypoxemia (partial pressure 20% drop inCMAP negative
spike duration, or baselineto- peak amplitude.3. Abnormal temporal
dispersion and possible conduction block CMAP duration difference
between the above proximal anddistal sites of stimulation is >
15%; and > 20% drop in CMAP negative spike duration or
baseline-topeakamplitude. 53. Prolonged distal motor latencies
(DML) in 2 ormore nerves 1. If CMAP amplitude is > 80% of LLN,
the DML mustbe > 125% of the upper limit of normal (ULN). 2. If
the CMAP is < 80% of LLN, the DML must be >150% of ULN.
Prolonged minimum F-wave latency or absent F-wave 1. F-waves
performed in 2 or more nerves (1015 trials) 2. If the CMAP
amplitude is > 80% of LLN, the F-wavelatency must be > 120%
of ULN. 3. If CMAP amplitude is < 80% of LLN, the F-wavelatency
must be > 150% of ULN. 54. Salient features of NCS in GBS The
most common EDX abnormalities seen in the first 2weeks of illness
are absent H reflex and absent,delayed orimpersitent F
waves,finding that are common inpolyneuropathies but not specific
for demyelinating type. Reduced CMAP amplitude or SNAPs in upper
extremitycombined with normal Sural SNAPs (sural sparing)
arechanges highly specific for diagnosis of AIDP and occurs in50%
of patient in first 2 weeks of illness Sural sparing combined with
abnormal F waves has veryhigh sensitivity but occurs in only a
third of patients duringfirst 2 weeks of illness. 55. Conduction
block of motor axons-recognised asdecrease of greater than 50% in
CMAP amplitude fromdistal to proximal stimulation in the absence
oftemporal dispersion. Conduction block is highly specific for
demyelinationbut occurs in only 15-30% of early GBS. 56. CSF
EXAMINATION Classic finding is elevated CSF protein with normal
cell count (albumino cytological dissociation). Occurs in up to 90%
at week 1 after symptom onset. CSF protein is usually normal within
the first 2 to 3 days but then begins to rise very quickly,
reaching a peak at 4 to 6 weeks and then persisting at a variably
elevated level for many weeks. 57. CSF protein level varies from
0.45 to 3.0 g/L (45-300 mg/dL), but levels as high as 10 g/L (1000
mg/dL) can be seen. Around 59% of patients with Bickerstaff
brainstem encephalitis (BBE) have elevated protein in CSF 58.
Around 10% will not have a protein elevation and thisincludes
patients with the Miller-Fisher variant. Cell counts are typically
6.4 kPa [48 mm Hg]), hypoxemia (