Embed Size (px)
Citation preview

Hemolytic anemiasextracorpuscular
defectsDr Vijay Shankar S

What is destroying these
R B C’s

IMMUNE MECHANISMS
NON IMMUNEMECHANISMS
AUTOIMMUNE
DRUGINDUCED
ALLOIMMUNE
1. Warm antibody
2. Cold antibody
1. H D N2. Blood
transfusion
1. Penicillin
2. Methyl dopa
1. Drugs2. Toxins3. Trauma4. M A H A5. Infections6. Membrane
defects7. Hypersplenis
m

Immune hemolytic anemias
These anemias result from a shortened RBC survival mediated by the immune response, specifically humeral antibodies.
There are three broad categories.1. Autoimmune 2. Alloimmune3. Drug induced immune hemolytic
anemia.

AUTOIMMUNE HEMOLYTIC ANEMIA
Warm antibody autoimmune hemolytic anemia Idiopathic Systemic lupus erythematosus (SLE) Evans' syndrome (antiplatelet antibodies and
hemolytic antibodies) Cold antibody autoimmune hemolytic
anemia Idiopathic cold hemagglutinin syndrome Infectious mononucleosis and mycoplasma
( atypical) pneumonia Paroxysmal cold hemoglobinuria (rare)

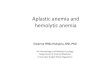
Warm antibody autoimmune hemolytic
anemia In this type of immune hemolytic
anemia the serologic reactivity of the IgG antibody involved is optimal at 370 C. ( body temperature)
In both the primary and secondary form of the disease, most hemolysis is extravascular.

Lab findings. The anemia is moderate to severe,
the RBCs are normochromic, normocytic with polychromasia (increased reticulocytes).
Spherocytes, schistocytes, etc. may be seen and are indicative of the hemolytic process.
Direct Coombs test is positive.

Warm antibody autoimmune hemolytic anemia

Cold autoimmune hemolytic anemia
pathologic cold autoantibodies are usually IgM antibodies that fix complement and are optimally reactive below 300 C.
IgM attaches to the erythrocytes in the cold. After warming , the cold reacting antibody dissociates from the cell, but the complement remains , causing direct cell lysis or initiating extravascular hemolysis.

The pathologic forms can be divided into three types:
Cold agglutinin syndrome – This is idiopathic, chronic, usually in individuals older than 50, and usually due to an IgM monoclonal antibody.
Secondary, cold autoimmune hemolytic anemia – due to polyclonal IgM antibodies that develop with Mycoplasma pneumonia infections, infectious mononucleosis, or lymphoproliferative disease. Is usually transient.
Paroxysmal cold haemoglobinuria(PCH) the cold Ab is IgG which is directed against P blood group antigen and brings about complement mediated hemolysis

In both a and b the extent of the disease is related to the thermal amplitude of the antibody – if it reacts at 30-320 C, it can cause problems when the peripheral circulation cools to that temperature:
IgM binds and fixes complement, upon warming the antibody dissociates, but complement remains bound leading to either intravascular or extravascular hemolysis.

The patient may experience acrocyanosis of hands, feet, ears, and nose (with agglutination blood flow slows down, the skin turns white and then blue; upon warming, the skin turns red
Blood counts are difficult to perform unless the blood is warmed.
The Coombs test with anti-complement antibody is positive.

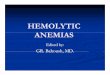
Paroxysmal cold hemoglobinuria
The third type of cold autoimmune hemolytic anemia) – is found in association with viral disorders and syphilis and may be chronic.
This is characterized by massive, intermittent, acute intravascular hemolysis and hemoglobinuria upon exposure to cold.
It is caused by a biphasic IgG antibody that binds at low temperature and fixes complement.

Upon warming, to body temperature, the intravascular hemolysis occurs and is accompanied by fever, shaking chills, and abdominal and back cramps.


ALLO IMMUNE HEMOLYTIC ANEMIA
Caused by acquiring isoantibodies or alloantibodies by
1. blood transfusions, 2. pregnancies and in 3. hemolytic disease of the newborn.

Drug induced immune hemolytic anemia
Penicillin – resembles that of warm antibody AIHA
Methyl dopa
Discontinuation of the drugs results in gradual disappeareance of hemolysis.

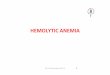
'''Non-immune mediated haemolytic anaemia''' (direct
Coombs test is negative)
Drugs (i.e., some drugs and other ingested substances lead to hemolysis by direct action on RBCs)
Toxins (e.g., snake venom) Trauma
Mechanical (heart valves, extensive vascular surgery, microvascular disease)
Microangiopathic hemolytic anemia : caused by abnormalities in the microvasculature.(a specific subtype with causes such as TTP, HUS, DIC and HELLP syndrome)

InfectionsMalariaBabesiosisSepticaemia

Thank you