Embed Size (px)
Citation preview
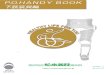
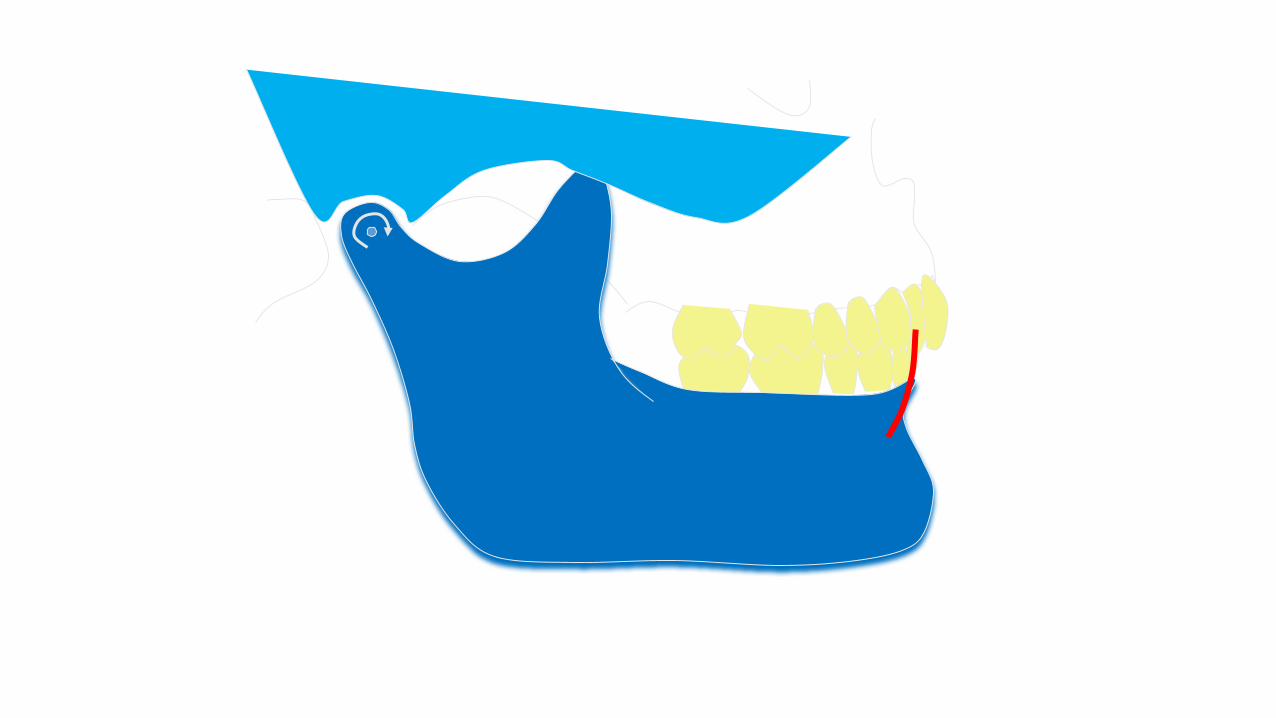
Hinge axis
Contents
1) Introduction 2) Definitions3) Mandibular movements 4) History 5) Theories of hinge axis 6) Method of locating hinge axis7) Clinical value of hinge axis 8) Summary 9) Reference
Definition
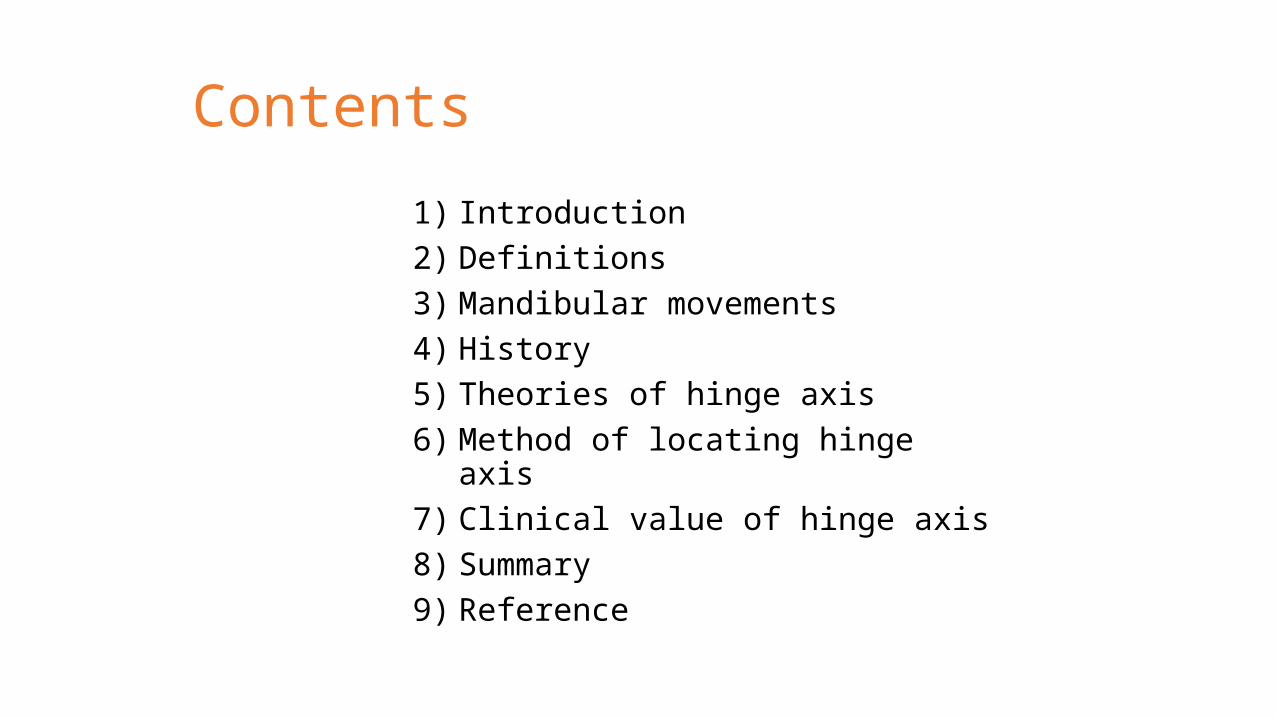
• “Imaginary line between mandibular condyles around which the mandible can
rotate within the sagittal plane” GPT—8
Terminal hinge axis = Transverse axis = Transverse horizontal axis = Transverse
hinge axis
• Pure rotation of condyles prior to translation
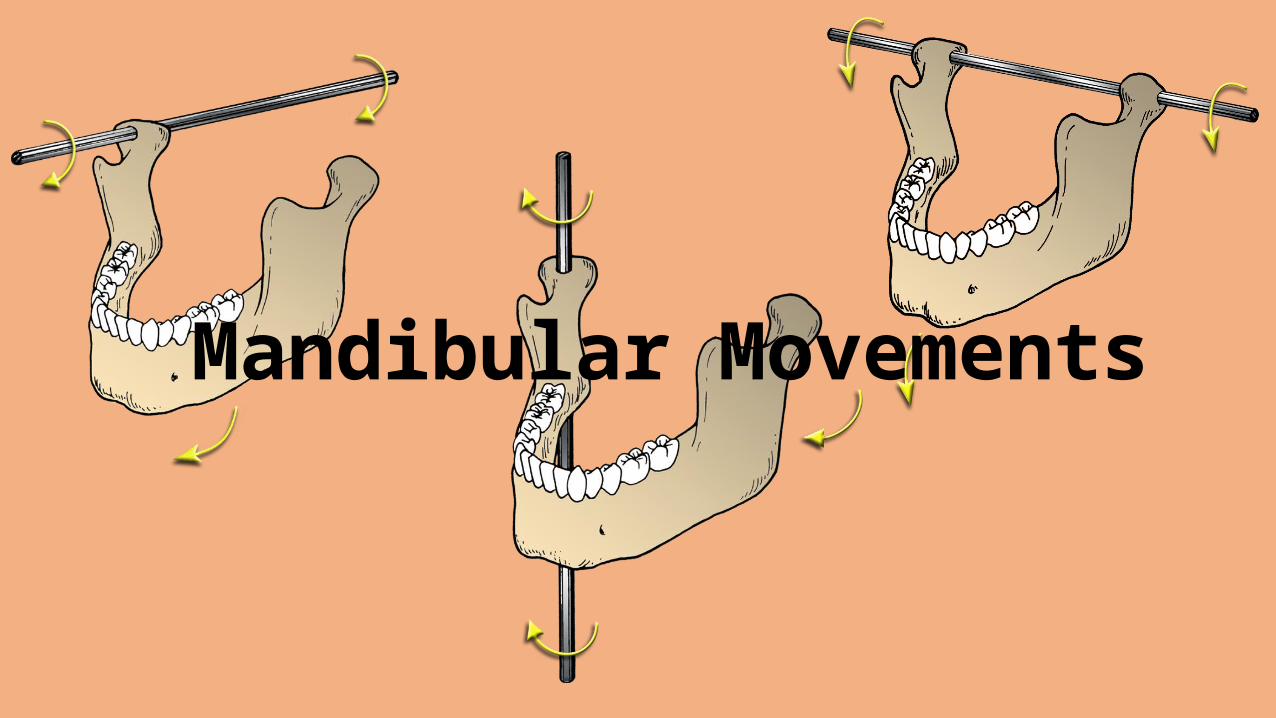
Mandibular Movements
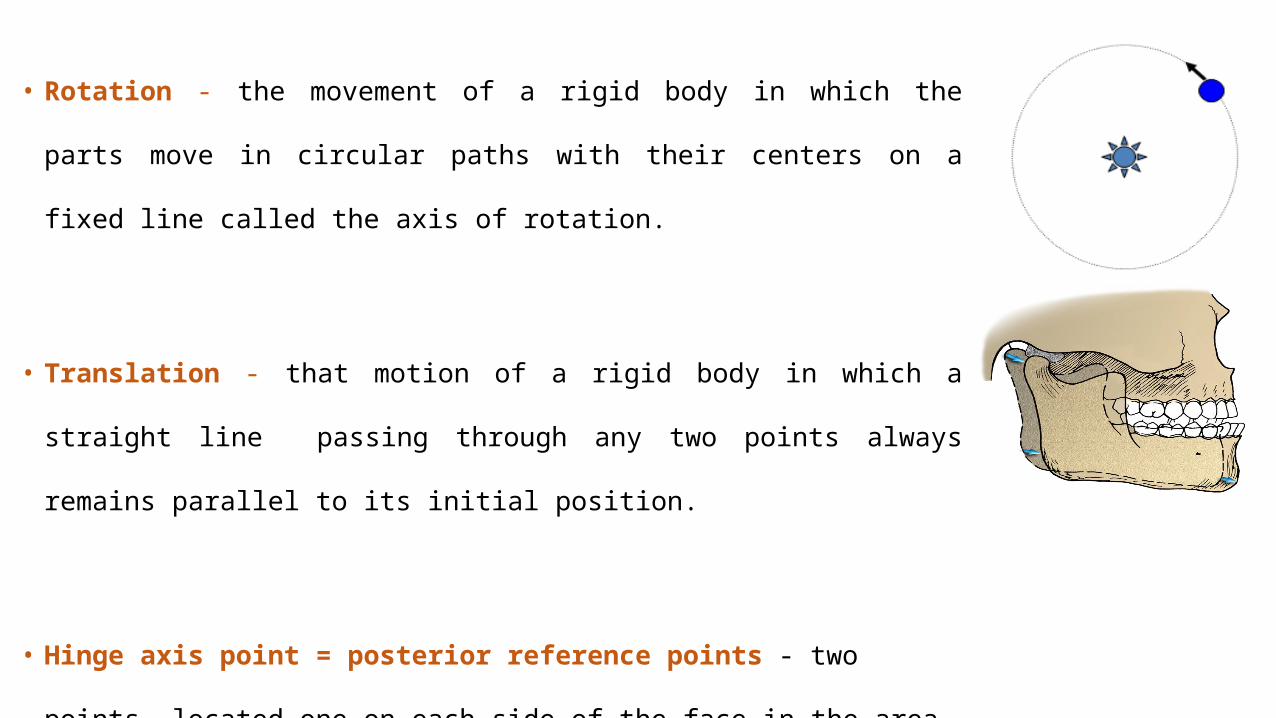
• Rotation - the movement of a rigid body in which the parts move in circular paths
with their centers on a fixed line called the axis of rotation.
• Translation - that motion of a rigid body in which a straight line passing through any
two points always remains parallel to its initial position.
• Hinge axis point = posterior reference points - two points, located one on each side
of the face in the area of the transverse horizontal axis, which together with an
anterior reference point, establish the horizontal reference plane.
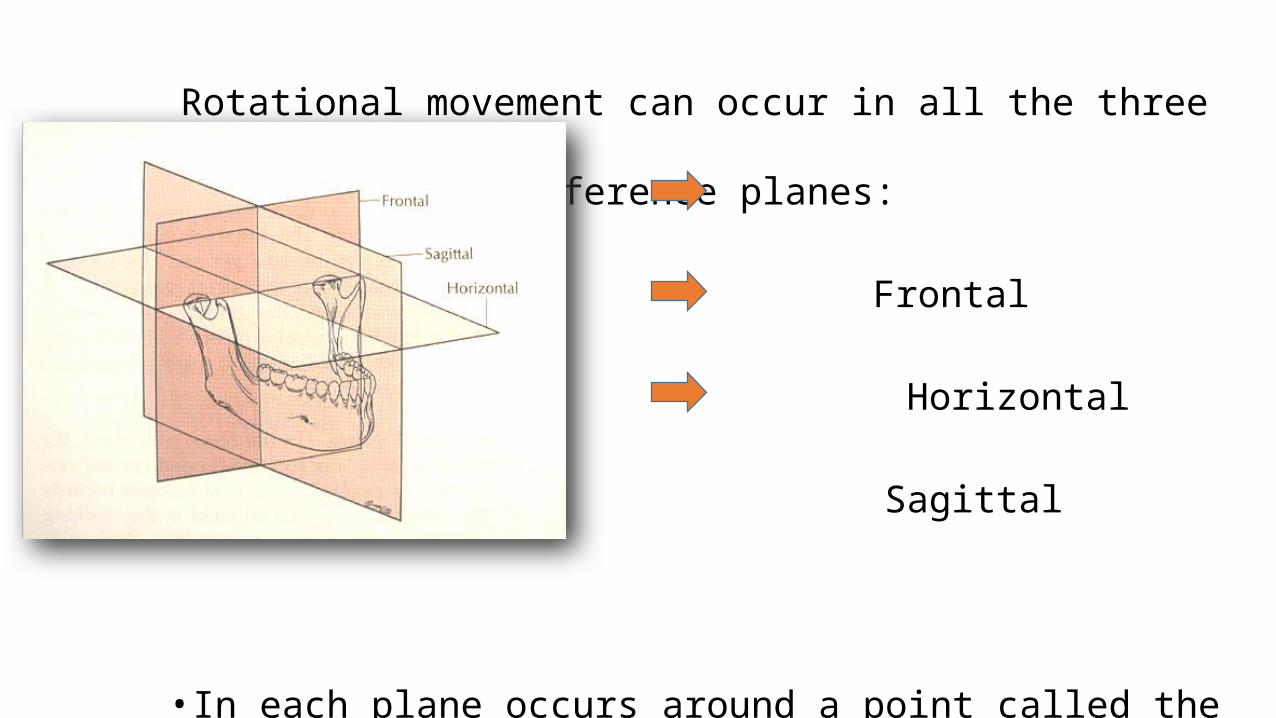
Rotational movement can occur in all the three reference planes:
Frontal
Horizontal
Sagittal
• In each plane occurs around a point called the axis
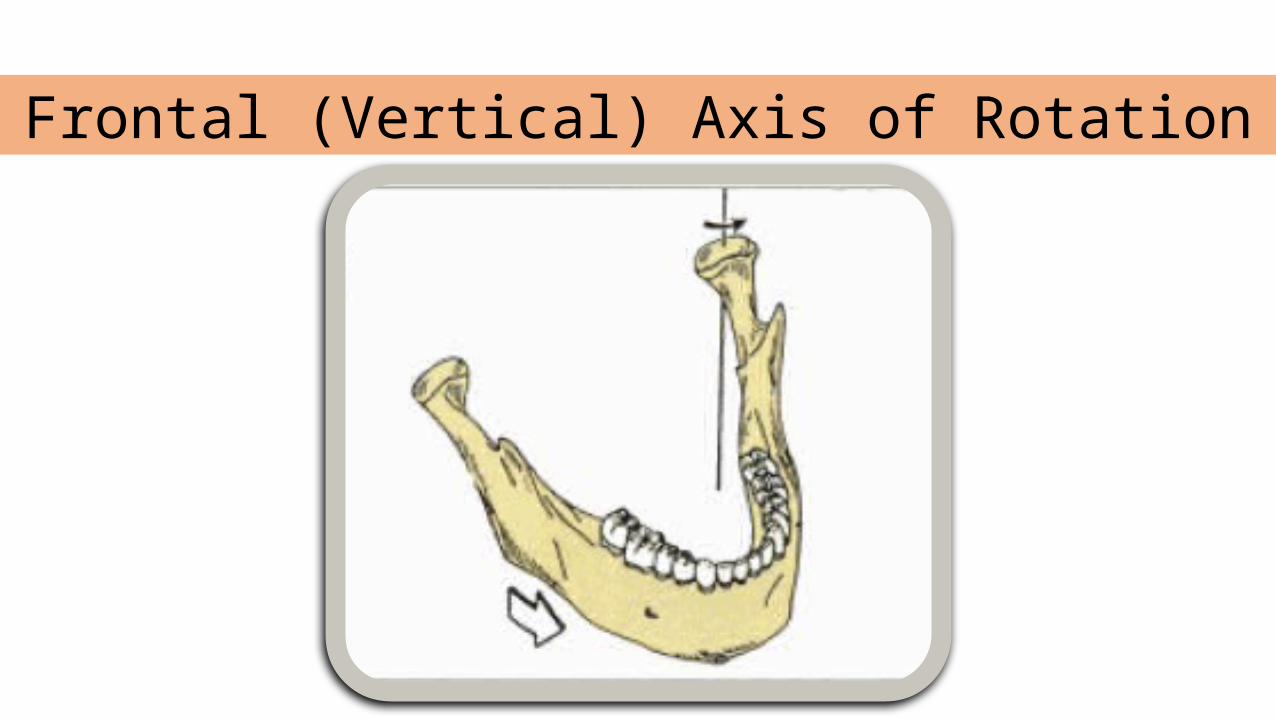
Frontal (Vertical) Axis of Rotation
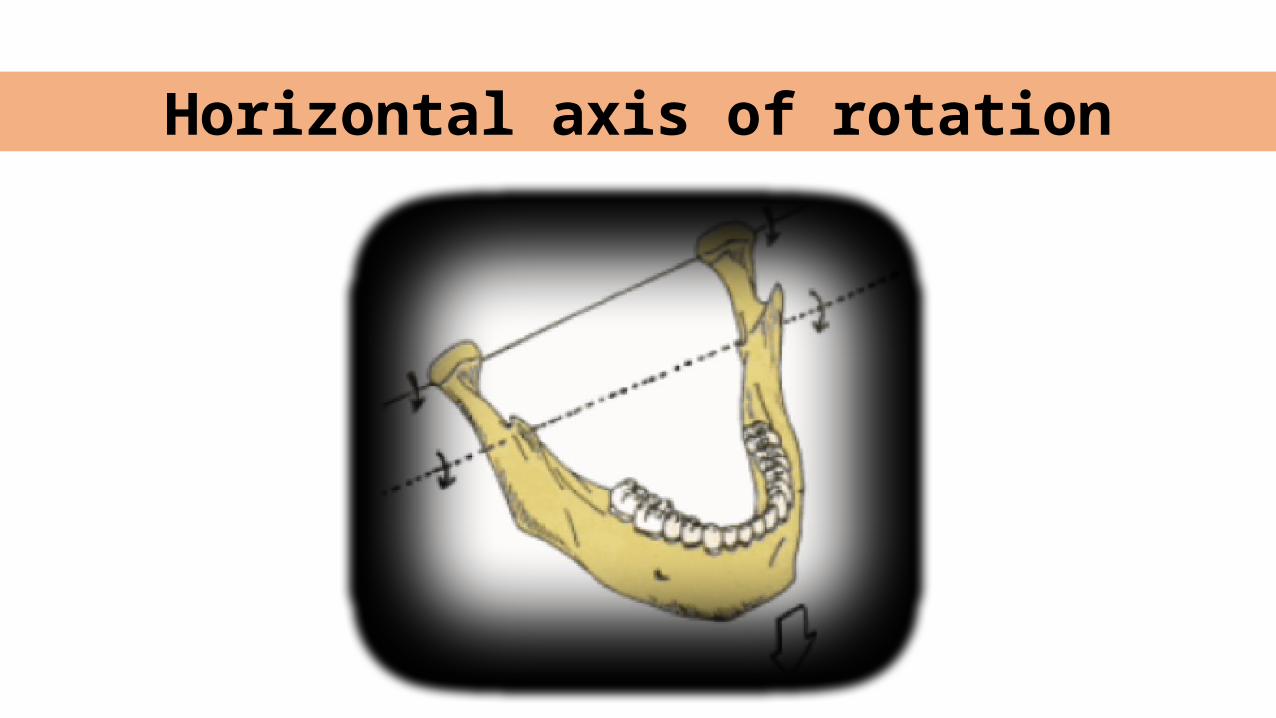
Horizontal axis of rotation
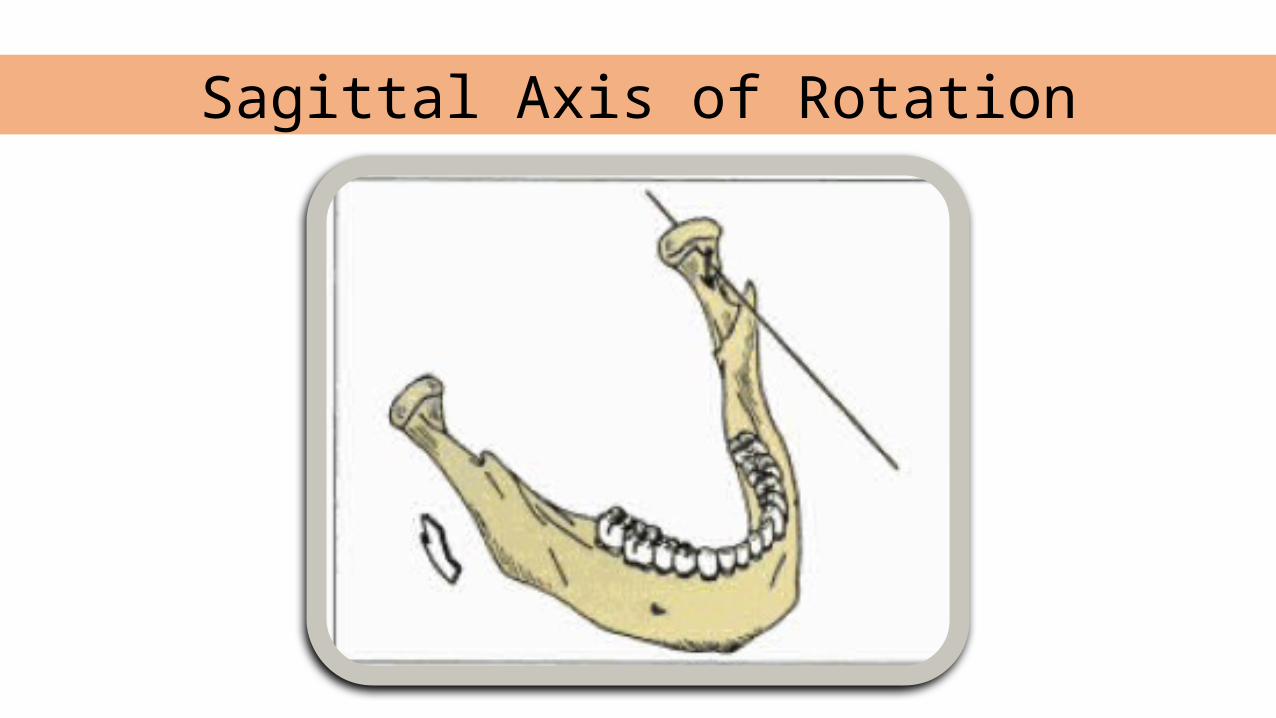
Sagittal Axis of Rotation
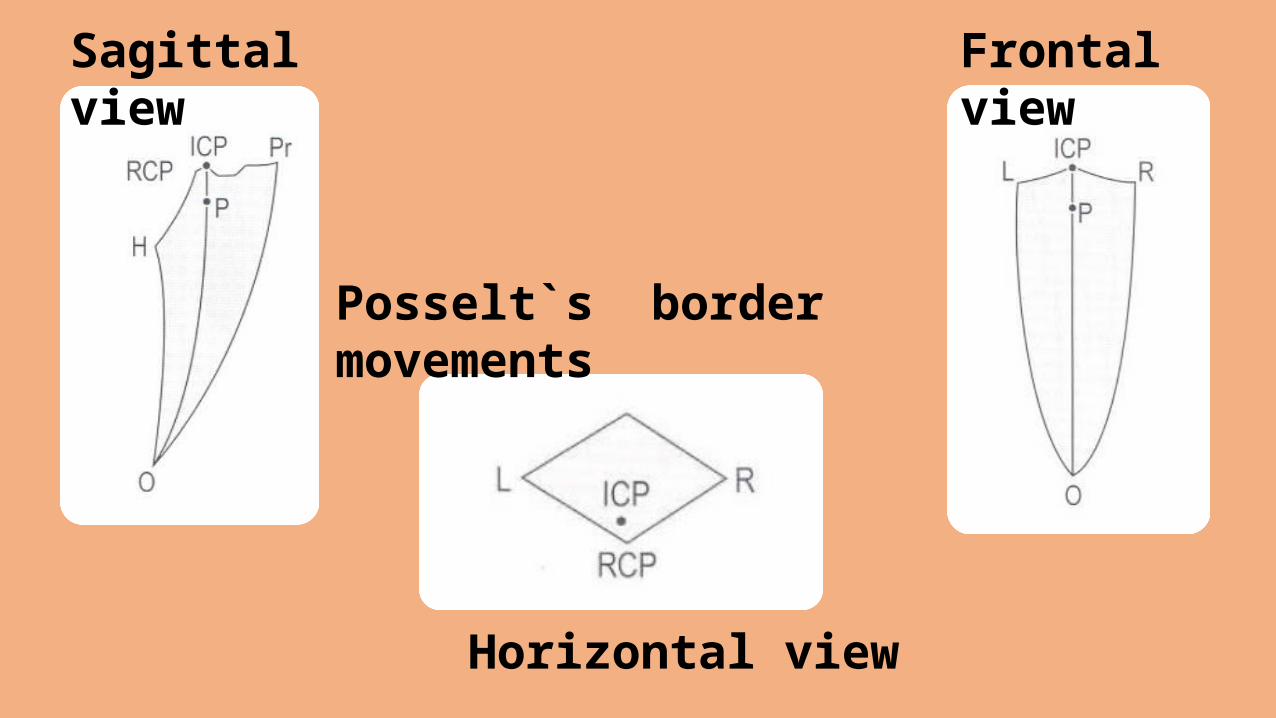
Sagittal view Frontal view
Horizontal view
Posselt`s border movements
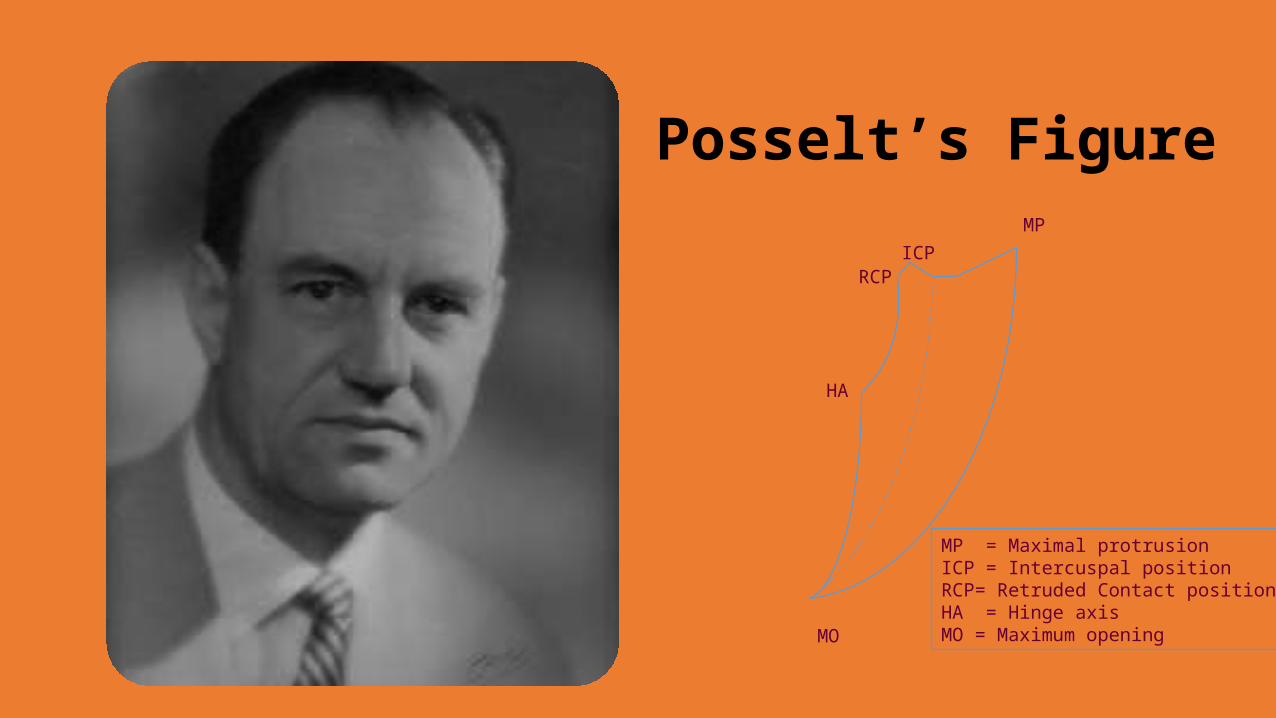
Posselt’s FigureMP
MO
ICPRCP
HA
MP = Maximal protrusionICP = Intercuspal positionRCP= Retruded Contact position HA = Hinge axisMO = Maximum opening
History
• Campion ( 1902-1905 ) – No axis, but movement is complex one.
Consisting first of rotation and secondly of a forward and downward movement
• Bennett ( 1908 ) - no single fixed rotation, since center of rotation constantly shifted for movements in sagittal plane,
mandible was capable of two independent movements
1. Angular rotation 2. Translation movement
• Gysi ( 1920 ) – Natural condyles are not considered as true rotation points, but as fixed guides of the mandible
"The mandible opens/closes and rotates on another rotational center which has no influence in the setting up of the teeth on articulators. Therefore, need not be considered in the construction of an articulator.”
• Needles ( 1923 ) - agrees with Bennett: Hinge Joint + Sliding Joint. No center of rotation in temporomandibular joint itself.
Instant and constantly shifting centers
• Wadsworth (1925) – Anatomist's conclusion
1st movement around transverse axis passing through condyles which remain seated in fossae.
2nd movement on articular eminence
• Hall ( 1929 ) – concluded that “condyle is not center of rotation”
`
McCollum ( 1939 )• Leading advocate of the hinge-axis theory• Definite opening and closing axis by using facebow • External landmarks are of little use. • Rotation occurs during 0.5 inch at incisors for most people, some can open
1 inch.
Stuart ( 1939 ) • Completed work of McCollum • Pioneers of gnathology • Movements were reproduced on articulator to duplicate the jaw movements
McLean ( 1944 )" The diagnosis of pathological occlusion depended on the fact that the final phase of jaw closure was pure hinge movement.“
Lauritzen ( 1951 )
• He thought articulation would be understood more easily if the joint were regarded as two separate joints• The only movement which could take place in the 'menisco-condylar'
part of the joint while opening and closing - a purely rotational movement. • In all patients, the anterior teeth could be separated by at least 12
mm in the rotational hinge relation.
Posselt (1952) • Hinge opening is obtained if patient is in passive, or trained active motion.• He could not prove this movement was habitual. • Hinge-axis opening = 19.2mm ± 1.9mm.
Kornfield & Granger ( 1955 ) • The only position at which it was possible to locate & reproduce the hinge axis
was at centric relation
Trapozzano ( 1955 )• Hinge-axis represented a border movement that could be recorded
repeatedly with unfailing accuracy
• It was essential to use trained mandibular hinge movement
• Recording was static starting point • Much of concept was based on
asymmetry of condyles• Off-Centre opening and closing
movements were perpendicular to hinge axis
• Movement in one direction in the plane could have only one axis of rotation
Weinberg ( 1959 )
Theories Of Hinge axis
The absolute location of hinge axis
school
The arbitrary
axis school
The non-believers
The split hinge axis
school
Aull ( 1963 )
Four schools of thought
•The hinge axis is a component of every masticatory movement and can not be disregarded.
•If the hinge axis of the articulator is not the same as the hinge axis of the patient then the mechanical reproduction of jaw motions are impossible.
•Believe that there is a definitive transvers axis and should be located
Absolute location of the axis
• The value of actually locating the exact hinge axis is not worth the effort. This group fails to recognize that if the hinge axis of the articulator does not coincide with the hinge axis of the patient, the paths of closure will not be the same.
Arbitrary location of axis
• This group does not believe the hinge axis can be accurately
located or believes other movements are involved and can not be
reproduced by an articulator simulating one axis
Non-Believers in the transverse axis location
• This group believes there are two axis of rotation ( one in each condyle) and they parallel
each other.
1. The horizontal axis is a hypothetical line connecting the two horizontal rotation centers of
the two condyles of the mandible.
2. There is one hinge location!
Split axis theory
METHOODS OF LOCATING HINGE AXIS
Arbitrary methodsKinematic methodsModified methods
1. loma-linda hinge axis device and method2. Buhnergraph intraoral method
3. Technique using geometric principle to locate hinge axis4. Abdal-Hadi’s method for locating arbitrary hinge axis
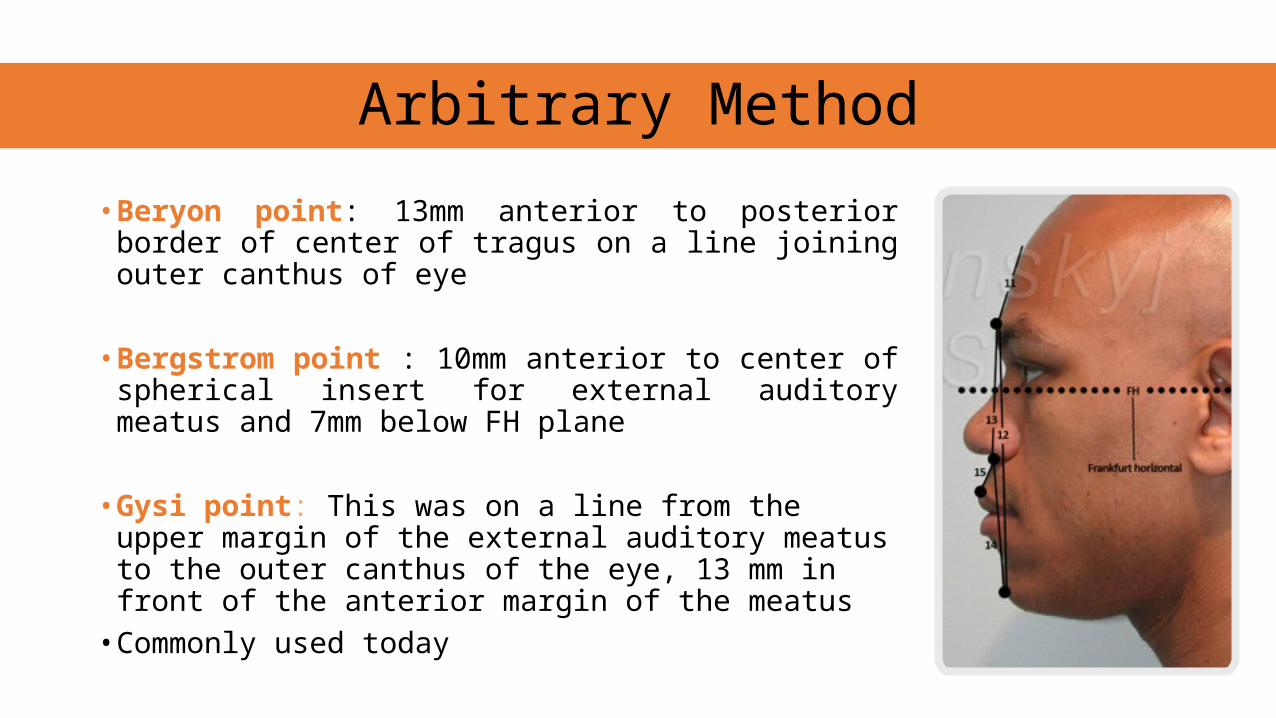
• Beryon point: 13mm anterior to posterior border of center of tragus on a line joining outer canthus of eye
• Bergstrom point : 10mm anterior to center of spherical insert for external auditory meatus and 7mm below FH plane
• Gysi point: This was on a line from the upper margin of the external auditory meatus to the outer canthus of the eye, 13 mm in front of the anterior margin of the meatus • Commonly used today
Arbitrary Method
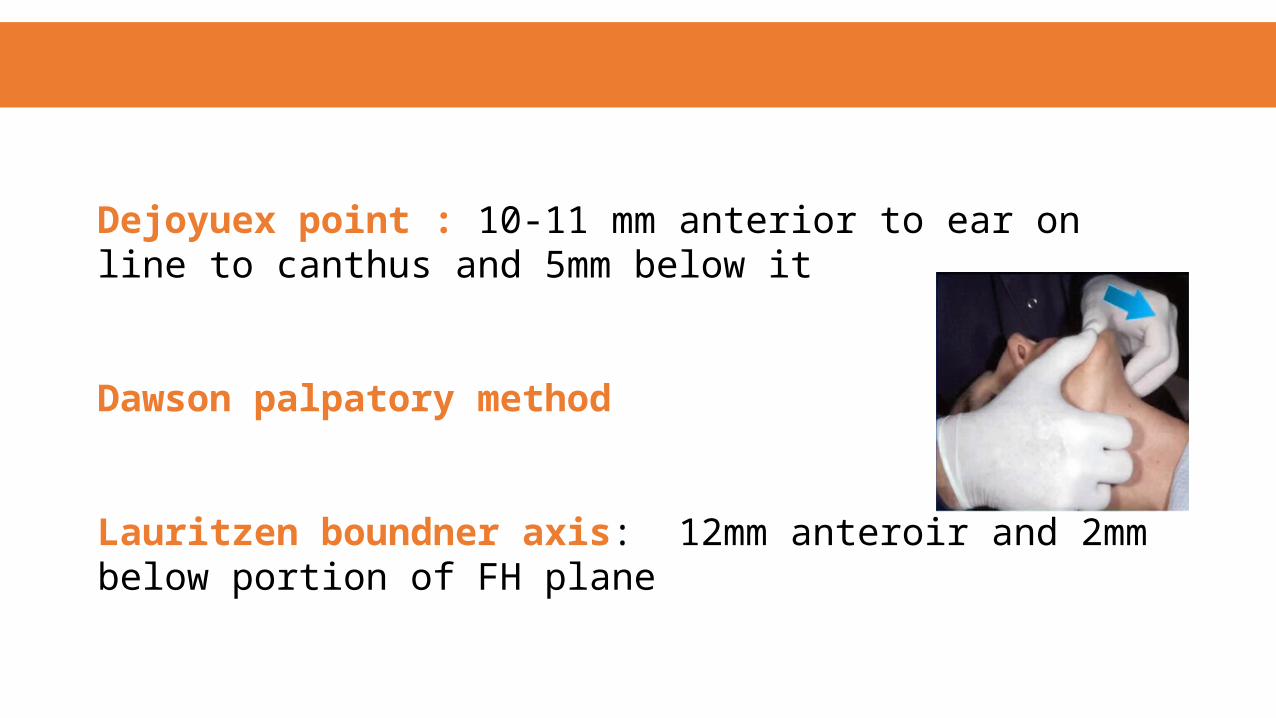
Dejoyuex point : 10-11 mm anterior to ear on line to canthus and 5mm below it
Dawson palpatory method
Lauritzen boundner axis: 12mm anteroir and 2mm below portion of FH plane
Two theorems of geometry are used in this technique• 1. A line drawn through the center of a circle perpendicular to chord
meets it at its midpoint• 2. The line joining the center of a circle to the mid point of a chord is
perpendicular to the chord.
Kinematic methods
Instruments
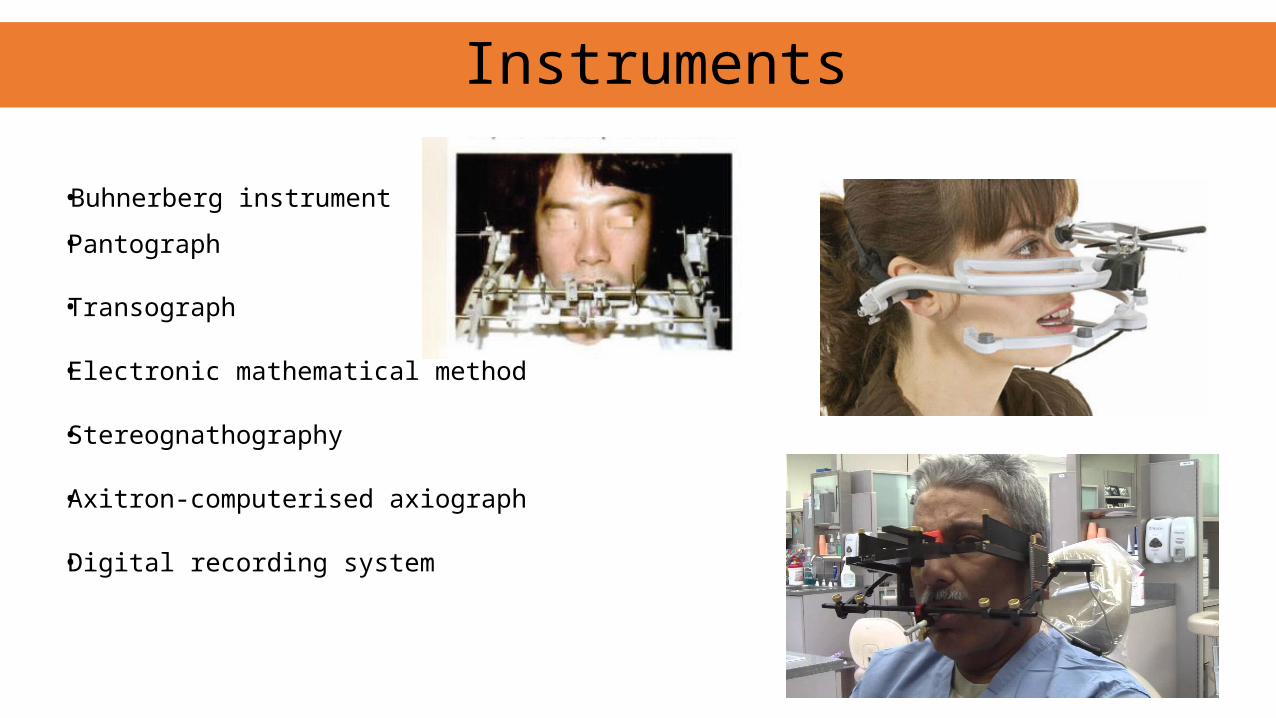
• Buhnerberg instrument
• Pantograph
• Transograph
• Electronic mathematical method
• Stereognathography
• Axitron-computerised axiograph
• Digital recording system
Step wise method of recording
1. Recording hinge axis points
2. Transfer to the articulator
3. Mounting of upper casts and
4. Mounting of lower casts with centric record
• T.M.J instrument
• Hinge axis locator
Hinge axis bow
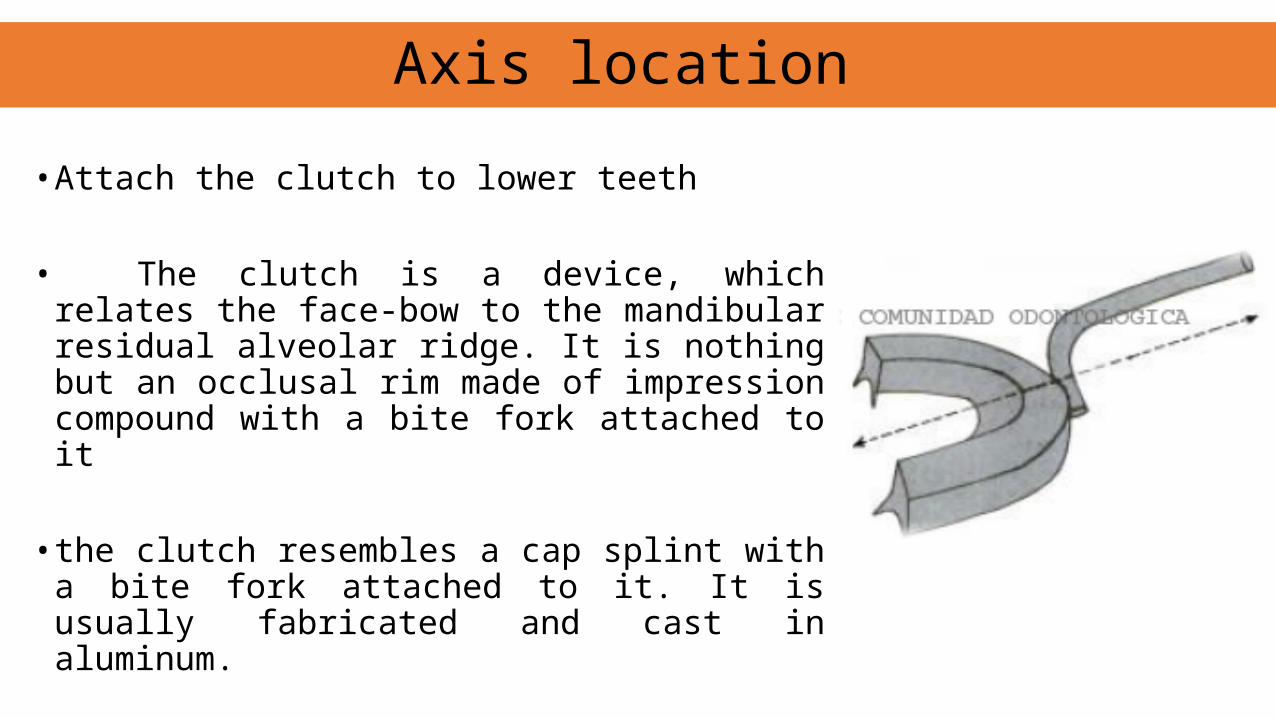
• Attach the clutch to lower teeth
• The clutch is a device, which relates the face-bow to the mandibular residual alveolar ridge. It is nothing but an occlusal rim made of impression compound with a bite fork attached to it
• the clutch resembles a cap splint with a bite fork attached to it. It is usually fabricated and cast in aluminum.
Axis location
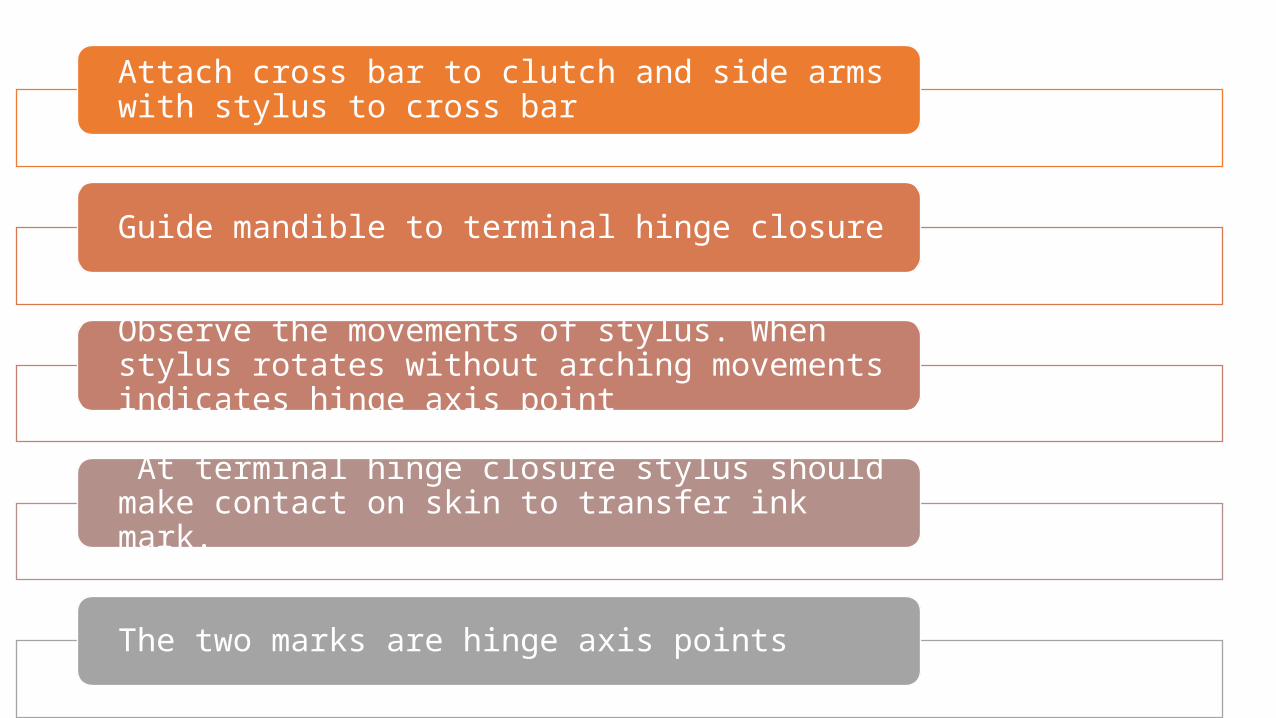
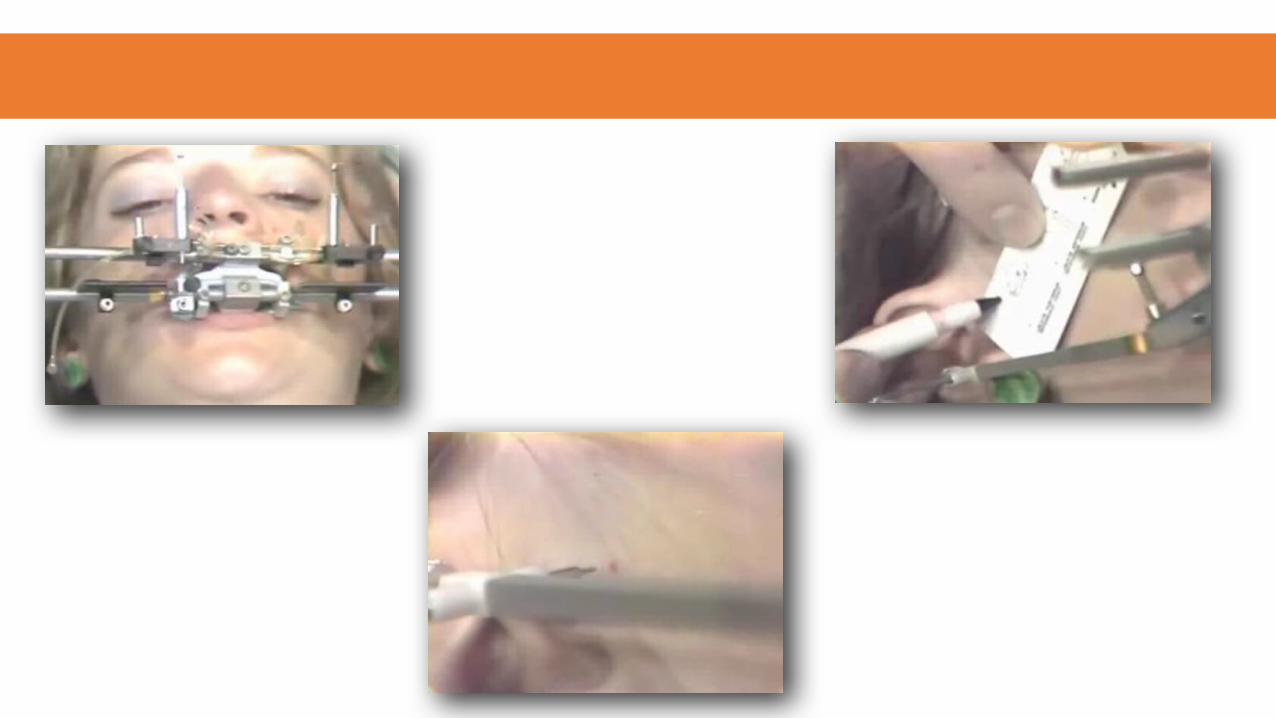
Attach cross bar to clutch and side arms with stylus to cross bar
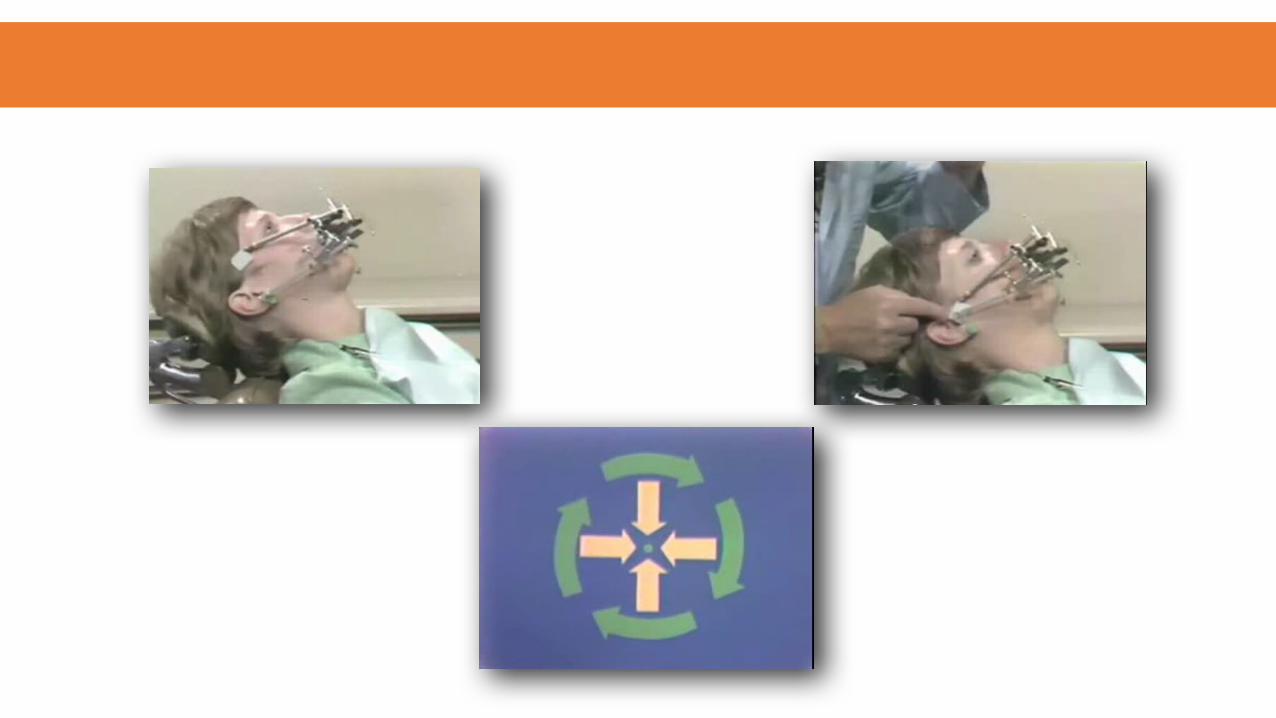
Guide mandible to terminal hinge closure
Observe the movements of stylus. When stylus rotates without arching movements indicates hinge axis point
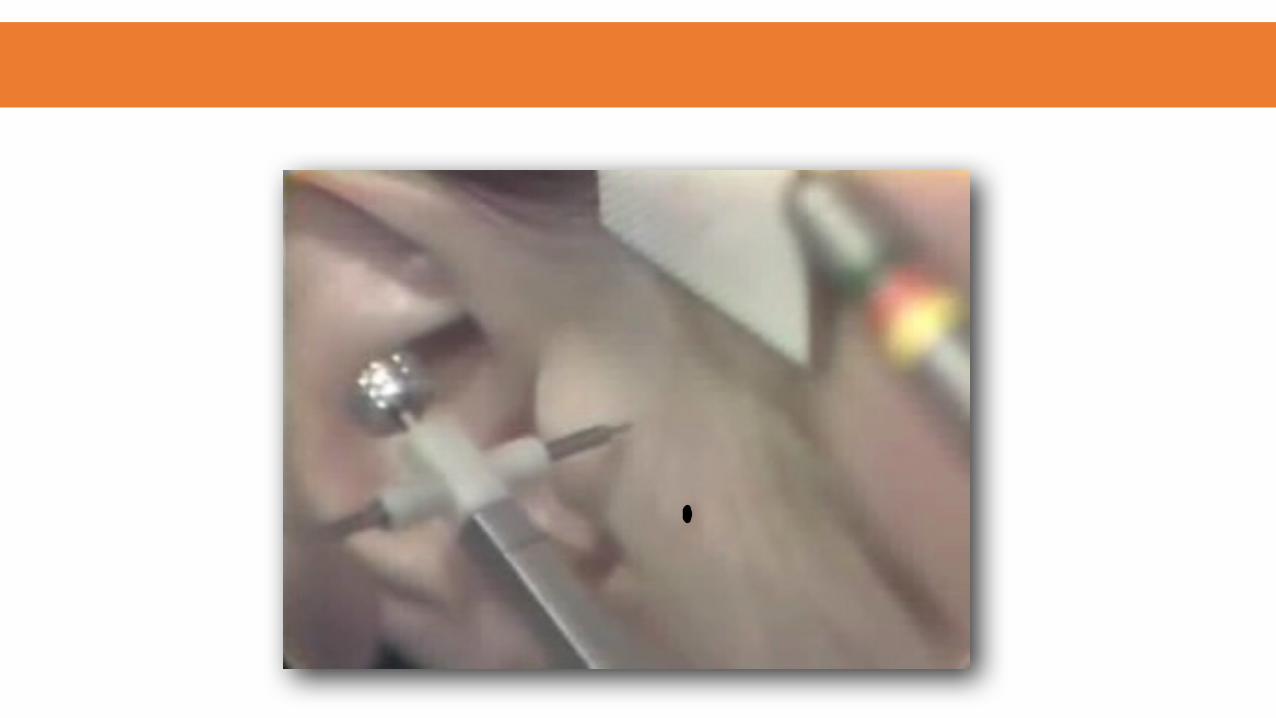
At terminal hinge closure stylus should make contact on skin to transfer ink mark.
The two marks are hinge axis points
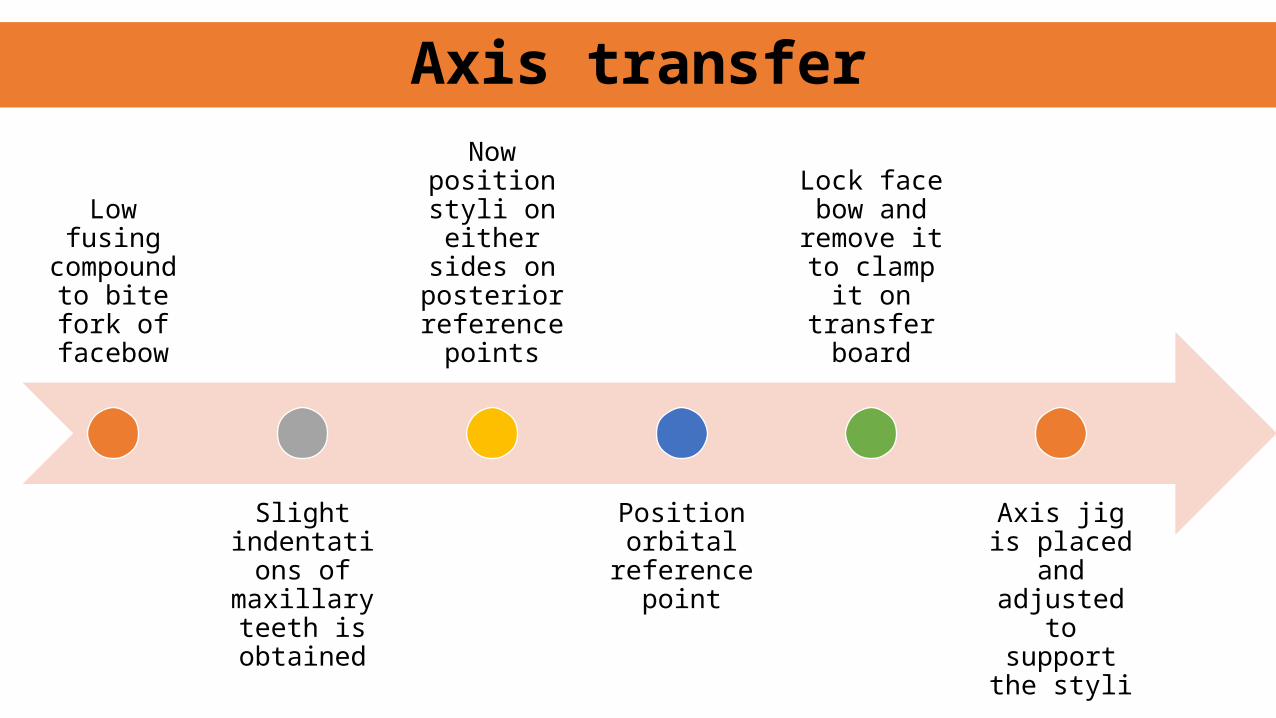
Low fusing compound to
bite fork of facebow
Slight indentations of maxillary
teeth is obtained
Now position styli on either
sides on posterior reference
points
Position orbital
reference point
Lock face bow and
remove it to clamp it on
transfer board
Axis jig is placed and adjusted to support the
styli
Axis transfer
Loma-linda hinge axis recording device and method
• The opponents of use of a kinematic hinge-axis location for edentulous patients point to its unreliability because of the resiliency of the oral mucosa.• the added weight of the recording clutch which tends to shift the
denture base
Modified method
• Dentist called Buhnergraph
• Buhnergraph instrument consists of a U-shaped piece of aluminum
• Attached to the underside of the lower member of a Whip Mix articulator. On each side is attached an adjustable arm containing a pointed shaft which moves in and out.
Buhnergraph intraoral method
• New arbitrary method• Y = 9.5 c 0.95 (X)
Y = width profile of the face measured from the ectocanthion to the center of the external auditory meatus
X = anterioposterior position
Abdal-Hadi's technique

Clinical value of Hinge Axis
• Allows for correct recording of centric relation and its transfer to the articulator• Starting point of lateral movements• Permits a change in vertical dimension• If transferred to articulator—teeth contact each other in the articulator
exactly as they do in the mouth• Helps in diagnosis and treatment planning
Variables affecting hinge axis location
Patient variables affecting the T.H.A.• locations Condyle • Asymmetry
• Inability to locate a true hinge axis• Myospasm or joint pathosis• Emotional conditions of patient
Factors of the recording system affecting THA• Right angle non-right angle system of the bow• Length of stylus arms and sharpness of styli
• A minimal error of 5 mm can be expected no matter what arbitrary position might be chosen. • Placement of the tragus-canthus line at the superior border of the
tragus of the ear will contribute to greater inaccuracy in most patients.• The largest percentage of true axis locations will be inferior to the
tragus-canthus line at the superior border of the tragus of the ear
summary
• In the final analysis, the true value of our individual work can be measured only by the degree of fineness with which we practice the art of dentistry rather than by the particular school of thought to which we adhere.
conclusion
• Jeffery P. Okeson. Management of temporomandibular disorders and occlusion, 5th edition • Zarb bolender-prosthodontic treatment for edentulous patients-12th
edition• Shillingberg• Heartwell• Terminal hinge movement of the mandible J Prosthet Dent 1957;7:787-97.• Winstanley, R. B. The hinge-axis: A review of the literature. J Oral Rehabil
12:135-159, 1985.• Hinge axis overview ; ashu sharma int journal of clinical dentistry• Vol 5, no, 3 : 2012
reference

Thank you