Embed Size (px)
DESCRIPTION
Citation preview

HIV associated thrombocytopenia

Clinical case presentation

Presenting complaint38 year old admitted to sugical ward with frank hematuria and generalized weakness
Admitted with a history of:Passing blood in urine for a week
Tiredness and feeling weak
Physical ExamPallorNo thrush
No splenomegaly

HPI
• 38 year old male not known to have any chronic illnesses presented to ER with c/c/o passing blood in urine for past one week which is getting worse for past 2 days.
• Patient is also complaining of generalized weakness and feel tired all the day

HPI
• Patient denies any bleeding from gums and no red/black spots noted on skin.
• Denies any blood in stool• Denies any loose stools/vomitings• No fever/rash/joint pains• Patient is also complaining of weight loss and
says it is negligible.

Physical examination
• Middle age male in nil CPDM/M : pale/ moist/anicteric acyanotic
• Chest: BAE+ clear• Cardiac: Unremarkable• Neuro: Unremarkable• Abdomen: Soft ,nontender, No organomegaly• 300 cc of frank blood noted in Urinary bag

LABORATORY (ONADMISSION)
HbMCVWCCPlateletsDiff. count:LFT:U+E:LFT: PT/PTT/INR
11.3 g/dl100
4.89 109/l6.000/μlnormalnormalNormalNormal Not available

Imaging
• U/S KUB: NORMAL STUDY

Other blood workup
• HIV- Reactive• VDRL- Non reactive

Diagnosis
• HIV Thrombocytopenia

Treatment
• Patient was started on Oral steroids(Prednisone), ZIDOLAM-N and vitamin suppelements

Hospital course
• Within 4 days of steroid and ART patient clinical symptoms were totally resolved and Platelets improved to 70000 by the time of discharge

Thrombocytopenia
• Normal platelet count= 150 000 – 450 000
• Mean values :
-Males 237 000-Females 266 000
• Plt count < 150 000 = thrombocytopenia
• Recent fall > 50% within normal rangeheralds severe clinical problems

Megakaryocyte and Platelets

PLATELET KINETICS• Megakaryocytes produce platelets by cytoplasmic shedding
directly into bone marrow sinusoids
• About 1 000 – 5 000 plts are produced by each MK beforeundergoing apoptosis
• In normal individuals plt production is approx 35000 –50000 microL of whole blood /day
• Above value ↑ more than 8x with increased demand
• Plt production rate can be ↑ 20-fold with exogenousthrombopoietin (TPO)
• Youngest plts contain RNA (reticulated plts) analogous toreticulocytes

• Thrombocytopenia is one of the most frequently observed haematological complications of HIV infection.
• The incidence increases among patients not receiving adequate antiretroviral treatment and does not appear to vary according to the mode of acquisition of HIV.

• HIV-related thrombocytopenia has been generally
attributed to two different mechanisms: • First, an immunologically driven destruction
of the platelets and second, an insufficient platelet production by the mega - karyocytes.
• While in early HIV infection increased platelet
destruction appears to be predominant, production failure is often the main cause of thrombocytopenia in late-stage patients.

A 10-yearcumulative incidence of up to 45% has been reportedA 10-yearcumulative incidence of up to 45% has been reported
Prevalence of thrombocytopeniain HIV patients
• It can be an initial manifestation in as manyas 10% of HIV patients
• Affects approx. 40% of HIV patients anytime during their illness

HIV associatedthrombocytopenia
Primary HIV-associated thrombocytopenia (PHAT)
• Most common• Resembles Idiopathic Thrombocytopenia• Complex etiology
Secondary thrombocytopenia
• Result of underlying pathologies (malignancies, OI, autoimmune diseases,lymphoproliferative disorders, myelodysplastic syndromes, chronic HCV,H. Pylori and drugs)
• Heparin-induced thrombocytopenia (HIT) more common in HIV• Thrombotic-thrombocytopenic purpura-hemolytic uremic syndrome (TTP-
HUS)
EDTA associated Pseudothrombocytopenia


Pathophysiology
• increased number of BM megakaryocytes driven by:
• increased endogenous thrombopoietin, but:
• ineffective delivery of viable platelets by MK
• doubled splenic sequestration of platelets
• shortened lifespan of platelets by two thirds
Primary HIV-associated thrombocytopenia(PHAT)

Ineffective platelet production
• HIV is able to directly infect megakaryocytes
• HIV transcripts are present in MK in PHAT
• Disturbance of MK function (plateletdevelopment and maturation)
• Increased MK apoptosis
Primary HIV-associated thrombocytopenia(PHAT)

Primary HIV-associated thrombocytopenia(PHAT)
Shortened platelet life span
• Probably the result of anti-platelet antibodies (IgG and IgM)• Platelet-associated IgG antibodies cross-react with PLT GPIIb/IIIa
and HIV env GP 160/120• Such AB are found in >70% in PHAT
• Anti-HIV antibodies binding to normal control platelets were morefrequent in PHAT compared to non-PHAT patients (50% versus5%)

Primary HIV-associated thrombocytopenia(PHAT)
Clinical manifestation
• Marked inter-patient variability• Abrupt to insidious• Incidental mild thrombocytopenia to severe bleeding
Expected:Common:Rare:Uncommon:
Petechiae, purpura, easy bruisingEpistaxis, gingival bleeding, menorrhagiaGastrointestinal bleeding, gross hematuriaIntracranial hemorrhage

Primary HIV-associated thrombocytopenia(PHAT)
Differential Diagnosis
• Opportunistic infectionsMAC, disseminated TB, leishmania, septicemia, histoplasmosis, CMV,EBV, Rubella…
• MalignanciesNHL, KS…
• Co-morbidity resulting in hypersplenismPortal hypertension (chronic hepatitis/cirrhosis…)
• Drug associated thrombocytopeniaHeparin induced thrombocytopenia (HIT), TMP-SMX, Ketoconazole,Gancyclovir, Pentamidine, Acyclovir, PZA, RFM, RFB, Valgancyclovir…
• TTP-HUSRare in HIV

Diagnosis:
• No gold-standard• Clinical diagnosis (usually isolated thrombocytopenia)• Exclude secondary thrombocytopenia
Pseudo-thrombocytopenia, drugs, HCV, H.pylori, CMV, MAC,Lymphoma, SLE, Immunothyroiditis, Heparin-inducedthrombocytopenia, TTP-HUS, Hypersplenism
• Not recommended: anti-platelet antibody testing
Primary HIV-associated thrombocytopenia(PHAT)

Thrombotic thrombocytopenic purpura (TTP)Hemolytic uremic syndrome (HUS)
Diagnosis:
•••••
ThrombocytopeniaMicroangiopathic hemolytic anemiaPresence of fragmented red cells (schistocytes)Abnormalities of coagulation in DICADAMTS13 measurement is uncertain
The recommended treatment for TTP is plasmapheresis and plasmaexchange.

HCV-ASSOCIATEDTHROMBOCYTOPENIA
• HCV infection evolves towards a chronic state in approx85% of patients
• Long-term complications of chronic HCV infectioninclude liver cirrhosis, end-stage liver disease andhepatocellular carcinoma
• Mechanism: sequestration of plt by hypersplenismresulting from portal hypertension.
• Treatment: Corticosteroids, interferon-alfa, eltrombopag,IVIG or anti-RhD immunoglobulin

EDTA dependantpseudothrombocytopenia
Pathophysiology:
• In vitro clumping of healthy platelets, in the presence of plateletagglutinating antibodies and EDTA
• Incidence ~ 0.1% in the general population• gpIIb/IIIa important factor in physiological haemostasis as receptor
for fibrinogene and VWF• EDTA binds the Ca++ which is required for normal gpIIb/IIIa
function• Lack of Ca++ results in vitro malfunction and malformation of the
gpIIb/IIIa receptor that can be now recognised by plateletagglutinin antibodies

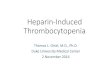
EDTA dependantpseudothrombocytopenia
Left: peripheral blood smear fromroutine blood sample, anticoagulatedwith EDTA
Electronic counting: 44.000/μl
Right: second blood sample from thesame patient, anticoagulated withheparine
Electronic counting: 560.000/μl
Source: Shalev O, Lotman A. NEJM, 1993; 329: 1467

EDTA dependantpseudothrombocytopenia
Consequences:
• Wrongly diagnosing an individual with normal platelets as havingsevere thrombocytopenia
Unnecessary evaluation procedures (BM, blood tests…)Unwarranted treatment (steroids, platelets…)Unwarranted splenectomyNeedless expenses to the patient and the health system
• Know about it!Diagnostic hint: low platelets without any signs of bleeding
• How to diagnose it?Do blood smear and watch out for platelet clumpingRe-do electronic counting of platelets from citrate or heparin blood

DRUG-INDUCEDTHROMBOCYTOPENIA
• The 1st case of drug-induced thrombocytopenia (DITP)was identified with quinine 140 years ago
• Several therapeutic agents have been implicated but fewreports are compelling
• Diverse mechanisms have been postulated:
- BM toxicity
- immune-mediated destruction of platelets
- Anti-drug-specific antibodies
FIRST STEP IN MANAGING DITP = STOP INCITINGDRUG(S)

HEPARIN-INDUCEDTHROMBOCYTOPENIA
• Develops in 1% to 3% of patients receiving unfractionatedheparin (UFH) for a minimum of 5 days
• Prevalence < in patients exclusively treated with low-molecular-weight heparin
• Incidence is highest in patients undergoingcardiopulmonary bypass and orthopedic surgery
• Mechanism: UFH binds to platelet factor 4 producingimmune complex for which antibody is specific; immunecomplex activates platelets through Fc receptors

Considerations for Treatment ofPHAT
• The patient's current platelet count
• The potential toxicities of therapy
• Other co-morbid conditions that increasethe risk of bleeding complications (eg,hemophilia, metastatic malignancy)
• A spontaneous remission in almost 20% ofpatients with PHAT

Asymptomatic andthrombocytes >30,000/μl
ART
Thrombocytes <30,000/μl orthrombocytes <50,000/μl andsignificant mucous membrane bleeding
ART plusFirst-line therapy: glucocorticoidsSubsequent therapies*: intravenous immunoglobulins,anti-(Rh)D, rituximab, splenectomy
Severe bleeding Platelet transfusions, high-dose glucocorticoids,intra-venous immunoglobulins, either aloneor in combination

Treatment Options for PHAT
• Stop potentially implicated drugs
• Non-life threatening (>20,000 & not bleeding)– Observation without specific therapy
– AZT-containing antiretroviral therapy
• Severe or life threatening (<10,000 or bleeding)– Corticosteroids (1 mg/kg prednisone)
– IVIG
– Anti-D Immunoglobulin (if RH + & notsplenectomized)

PRE-AZT ERA
Steroids
Pre-AZT (early 1980s)Steroids, only!
Mean: 10 monthsMedian: 5 months
20/24 clinical sequelae:“moon face”oral candidiasis,
reactivation of HSVetc…

AZT-MONOTHERAPY1988: 10 patients with PHAT, PLT 20-100, AZT-Monotherapy
•••
5 patients: 2g AZT 2/52, 1g AZT 6/52, placebo 8/525 patients: placebo 8/52, 2g AZT 2/52, 1g AZT 6/52Platelets increased by 50.000 to 100.000/μl in all in the AZT group, but not in theplacebo group, platelets remained increased for 4 weeks in 3/5, 1/5 anemia +neutropenia
••••
10 patients: 250mg qid (1g/day) after 12 weeks: 12 → 5724 patients: 500mg tid (1.5g/day) after 12 weeks: 20 → 77Platelets increased in both groups1 patient was stopped b/o toxicity, 4 patients discontinued
•••
Ann Intern Med, 1988; 109: 718
1989: 34 patients with PHAT, PLT<50, AZT
Ann Intern Med, 1989; 110: 365
1993: 86 patients with PHAT, PLT<50, AZTRandomized to two regimen (AZT 500mg/day or AZT 1000mg/day)In both groups response rate was ~65%Those on higher regimen responded quicker, better and more lasting at month 6
AIDS, 1993; 7: 209

HAART IN PHAT
Summary:
•
•
•
•
•
•
•
ART is clearly beneficial
Proven for AZT (various dosages)
Other ART regimen also work
High dose AZT is more efficient than normal dose AZT
Keep AZT side-effects in mind
The lower the platelets the more delayed the response
Response is to be expected within 1-3 months

ADDITIONAL THERAPY
Therapy I – what additional therapy?
• Steroidsif platelets < 30.000/μl (HIV.NET), after HAART (Zambia)Prednisone 1g/kg/day - taper down once platelets are 60.000/μl80-90% response, “quick” response, sustained response uncertain(10%)possible risk for Kaposi’s sarcoma if given long term
• Packed erythrocytes and plateletsfor active bleeding plus
• Intravenous Immunoglobulins (IVIG)for acute life threatening bleeding
• Anti-(Rh)D (WinRho anti-(Rh)DTM))seems even better and less expensive than IVIG, only for Rh-positivepatients, problem: lowers HB up to 2mg/l, intravasal hemolysis~0.7%

ADDITIONAL THERAPYCONT.....
• Other…Dapsone: 9/11 patients with inadequate response respondedDanazol: 2/8 patients respondedINF-α: 13/13 and 9/13 respondedmuch more… but small numbers/experimental
• Splenectomyonly in refractory cases,if possible allow 3-6 months conventional treatmentgood and sustained response in 50% (Scaradavou, 2004) 60% (Zambia) 80-100% (HIV.NET).risk of post-splenectomy syndrome (OPSI) seems lowprior vaccination against Pneumococci, HiB, Meningococciprotection in patients with CD4 less than 400 uncertain…

Lessons learned concerning AZThigh dose treatment:
• High dose AZT was highly effective in this case inincreasing initial very low platelet count significantly
• Make sure that those following-up the patient arefamiliar with the AZT high dose treatment:
2 weeks: 1.8g/day (900mg bd) followed by:6 weeks: 1.2g/day (600mg bd), then 600mg/day
(300mg bd)• Although good response with regard to platelets, high
risk of AZT associated anemia and neutropenia if notmonitored properly
• Medium dose AZT seem to keep platelets up with nosignificant drop in Hb

THANK YOU