Embed Size (px)
Citation preview
2
3
4
• Percutaneous Biopsies
• Percutaneous Nephrostomy (PCN)
• Percutaneous Renal Tumor Ablation (Using
Radiofrequency Or Cryoablation)
Occlude Pathological
Arteries
• Bleeding Arteries
• Arterio-venous Fistulae
• Tumour Feeding Artery
Restoring Caliber of Narrow
Arteries
Renal Angioplasty with or without Stent
Insertion
• Renal bleeding can occur after
abdominal trauma, which can be
blunt or penetrating.
• Penetrating trauma include iatrogenic trauma following percutaneous procedures such as biopsy, percutaneous nephrostomy and percutaneous nephrolithotomy
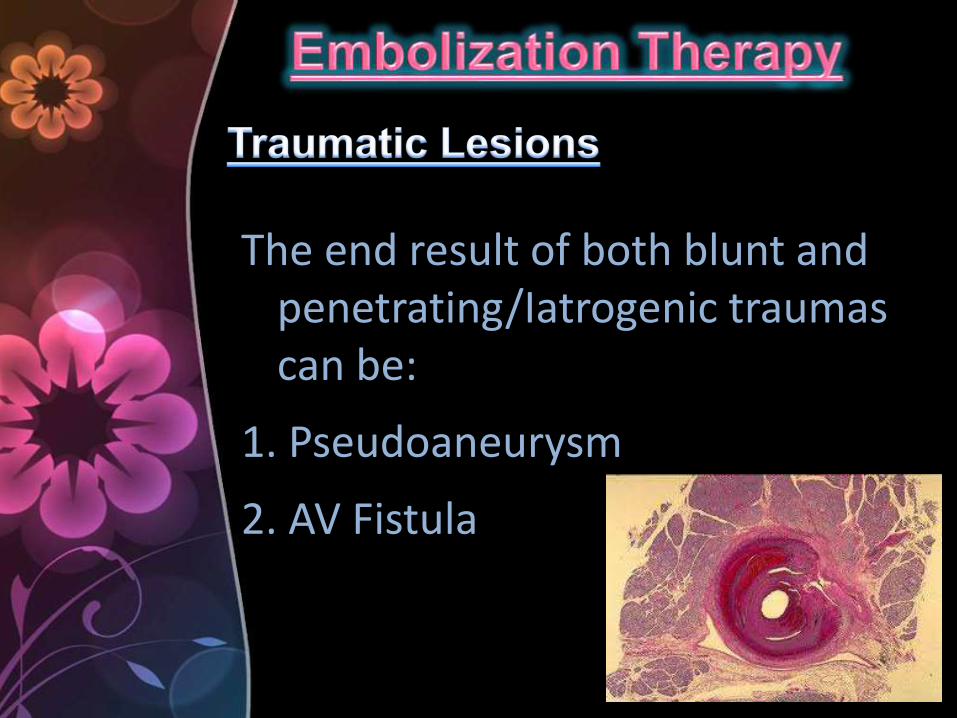
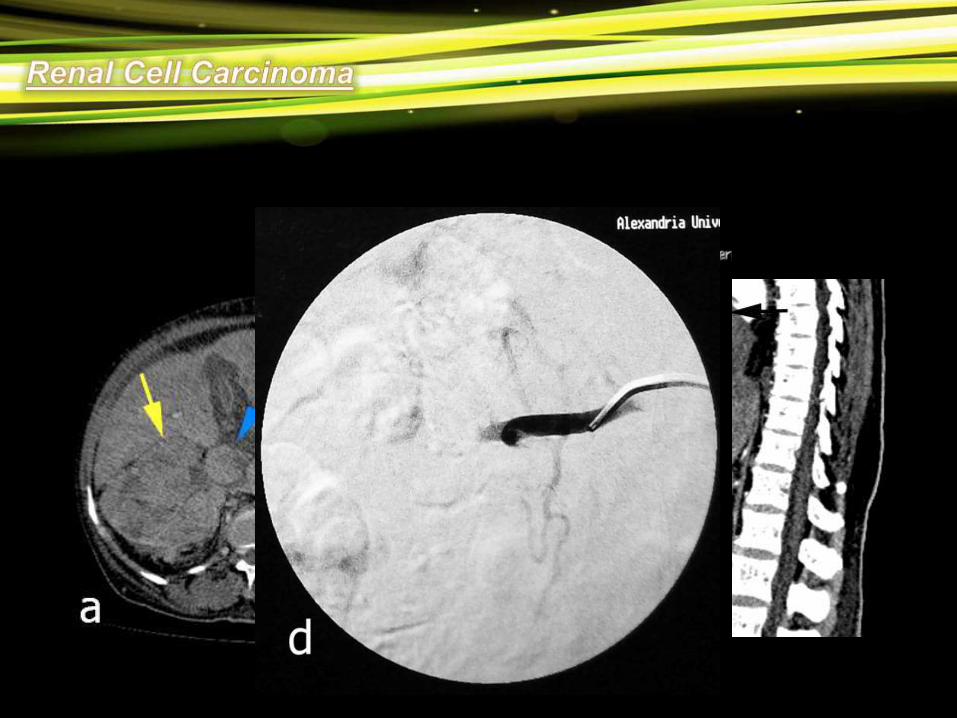
The end result of both blunt and penetrating/Iatrogenic traumas can be:
1. Pseudoaneurysm
2. AV Fistula

Both pseudoaneurysms and AV Fistulas can bleed around the injured kidney leading to retroperitoneal hematoma
Also both pseudoaneurysms and AV Fistulas can bleed into the collecting system when a concomitant injury to a calyx co-exists leading to hematuria
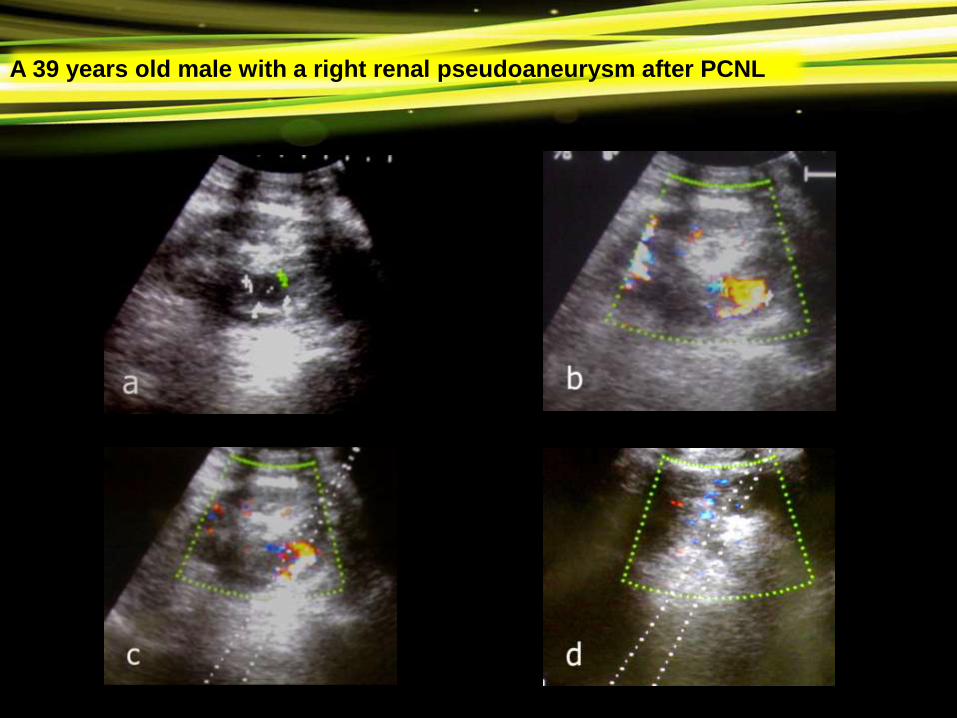
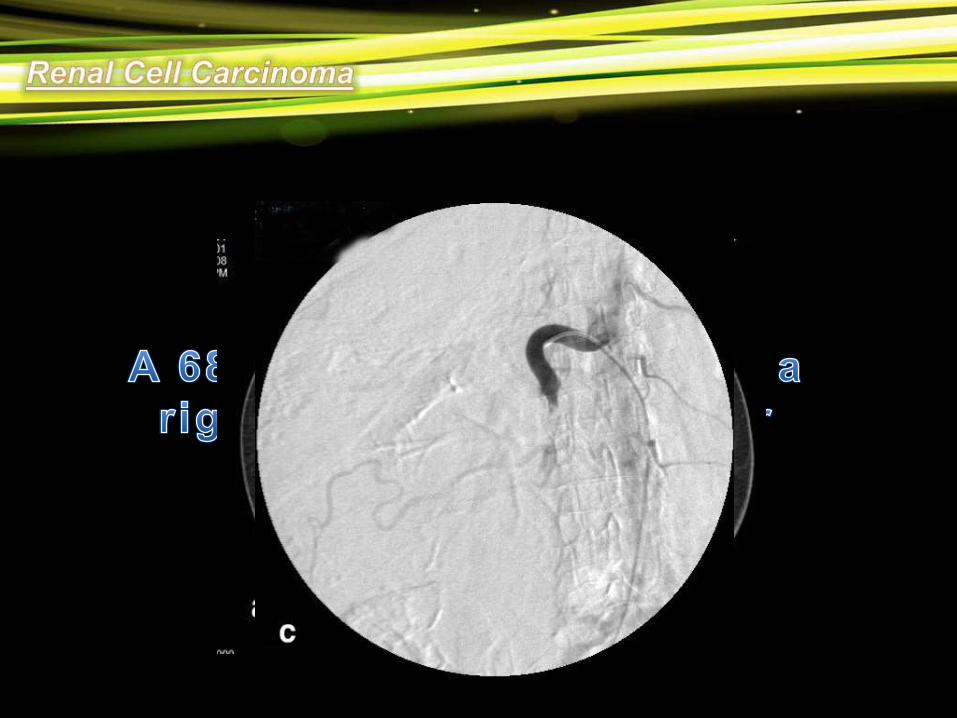
A 39 years old male with a right renal pseudoaneurysm after PCNL
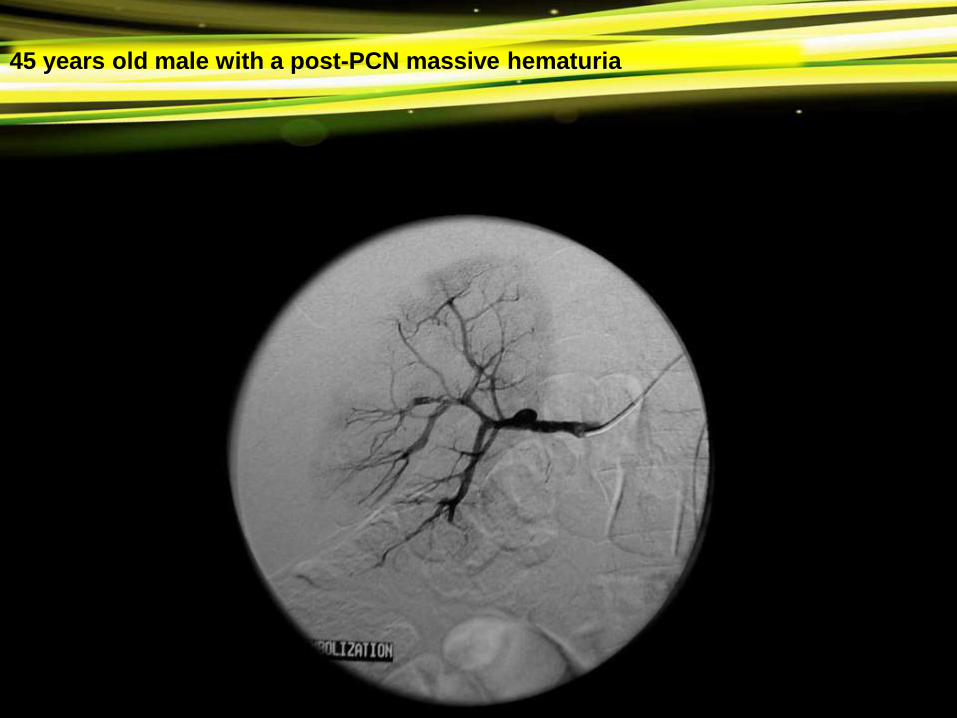
45 years old male with a post-PCN massive hematuria
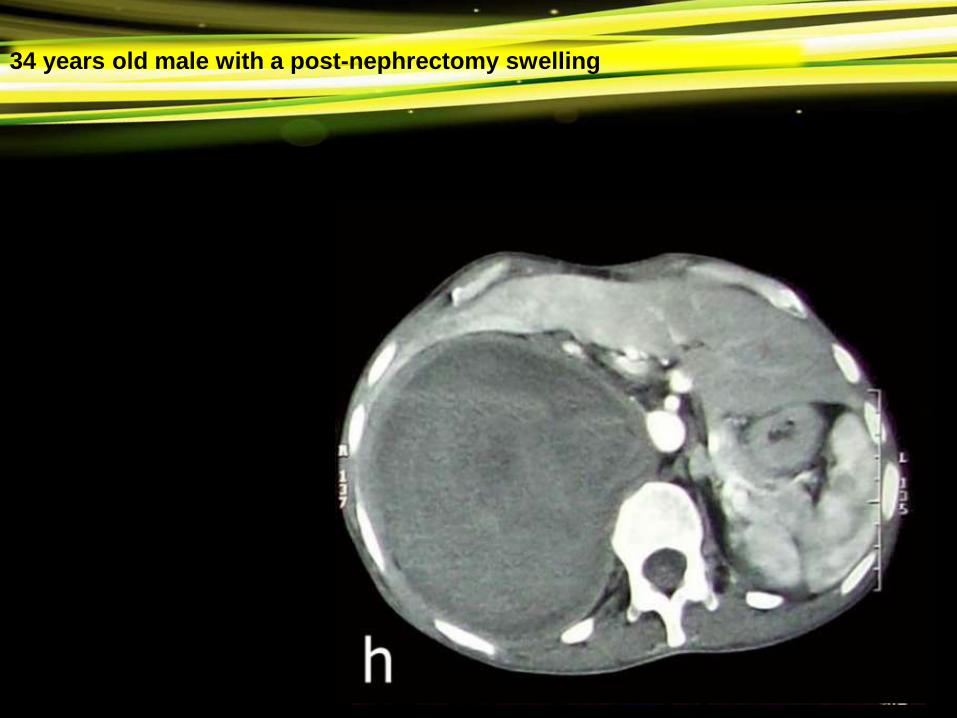
34 years old male with a post-nephrectomy swelling

• About 40 years ago arterial embolization was
introduced to facilitate the surgical excision of
the carcinomatous kidney or to palliate
symptoms, such as haemorrhage from non-
resectable tumours.
• The role of this technique as a therapeutic
procedure has been a source of debate in the
literature.

• Indications for embolization include:
1. Prophylaxis
2. Life-threatening hemorrhage
3. Recurrent flank pain
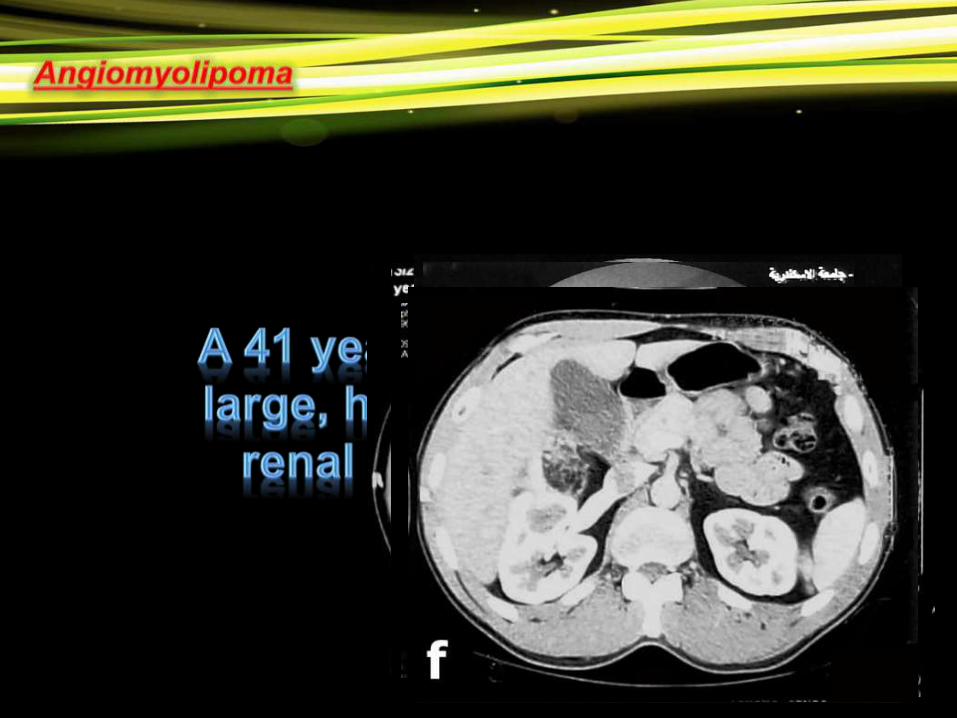
• Symptoms rarely occur in lesions measuring
less than 4 cm in contrast to those measuring 4
cm or larger, of which 80%– 90% are
symptomatic and 50%–60% bleed
spontaneously.
• Angiomyolipoma less than 4 cm can be managed
conservatively.
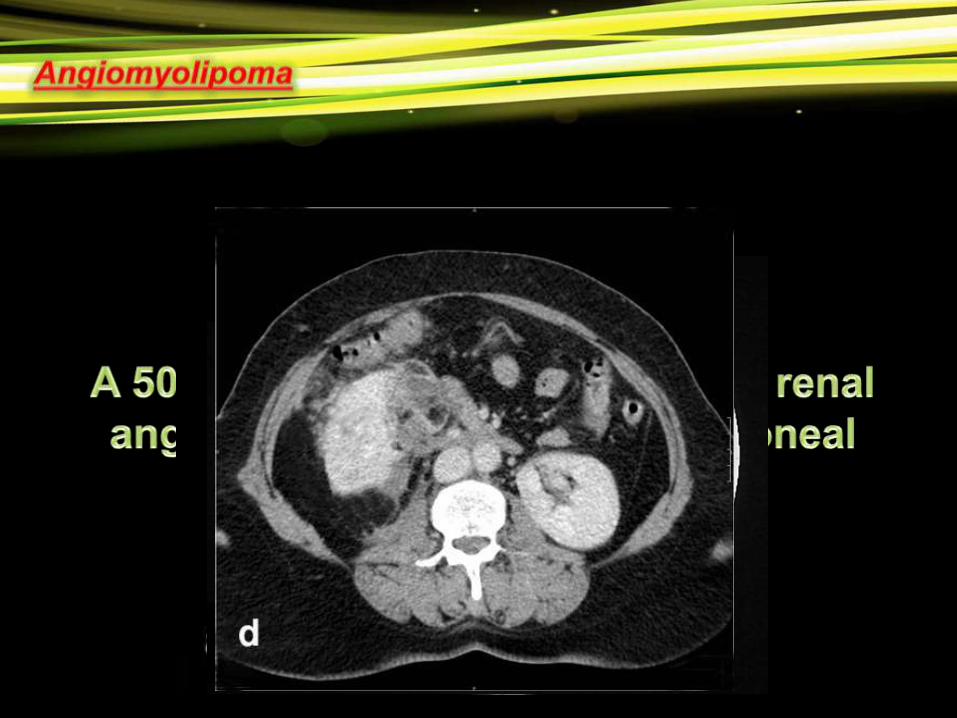
• Larger lesions are at greater risk of spontaneous bleeding
and are treated with Selective embolization particularly in
patients with multiple and bilateral disease.
• The basis of treatment for localized disease is surgical
resection, as the tumors are relatively resistant to
both radiotherapy and chemotherapy.
• Transarterial embolization (TAE) of renal tumours was
first described in 1973 as a preoperative aid to
resecting localized RCC and to palliate symptoms in
metastatic disease.
Pre-Operative:
• Decreases vascularity and hence bleeding.
• Creates edema to facilitate resection.
Palliative:
• Stops massive hematuria.
• Cytoreductive.

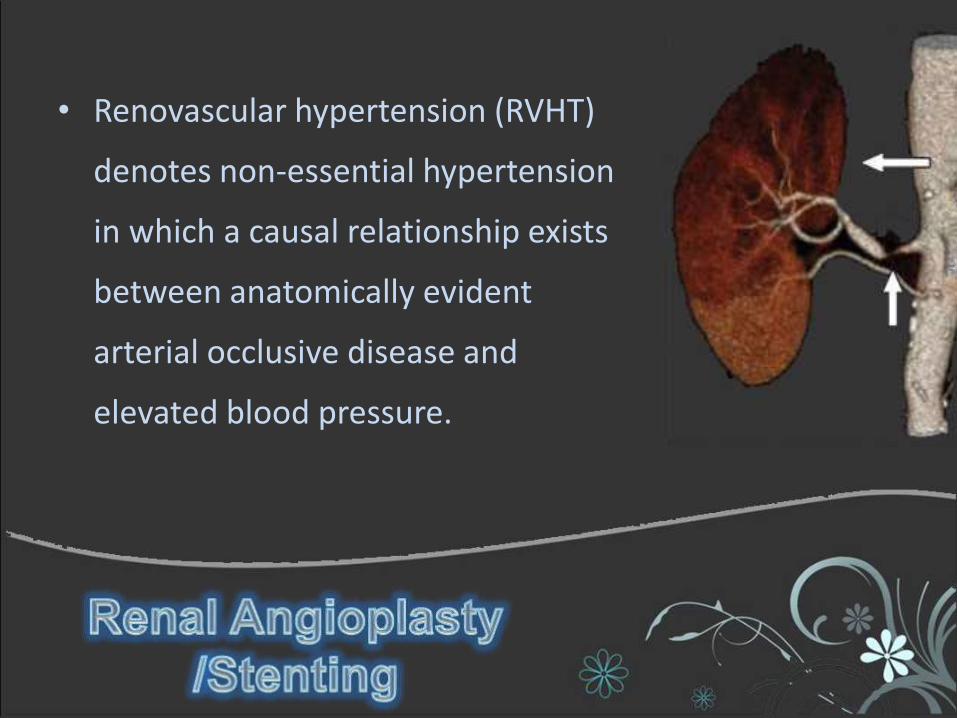
• Renovascular hypertension (RVHT)
denotes non-essential hypertension
in which a causal relationship exists
between anatomically evident
arterial occlusive disease and
elevated blood pressure.
• RVHT is the clinical consequence of
renin-angiotensin-aldosterone
activation as a result of renal
ischemia
• Renal artery stenosis (RAS) is a major
cause of RVHT. In older patients,
atherosclerosis is the most common
cause of RAS while Medial fibroplasia
(MFP), as a cause of RAS, usually affects
young to middle-aged adults, mostly
women, but it can also affect children.
• PTRA appears to be as
effective as open surgery for
the treatment of isolated renal
artery stenosis.

Thank
You