Embed Size (px)
Citation preview

How can exercise help
people with MS?
John M Saxton Department of Sport, Exercise & Rehabilitation Northumbria University
As early as the ninth century B.C., the ancient Indian system of medicine (Ayurveda) recommended exercise and massage for the treatment of rheumatism
Greek philosopher Hippocrates (‘the father of medicine’) acknowledged the virtues of exercise for physical and mental health in the 4th century B.C.
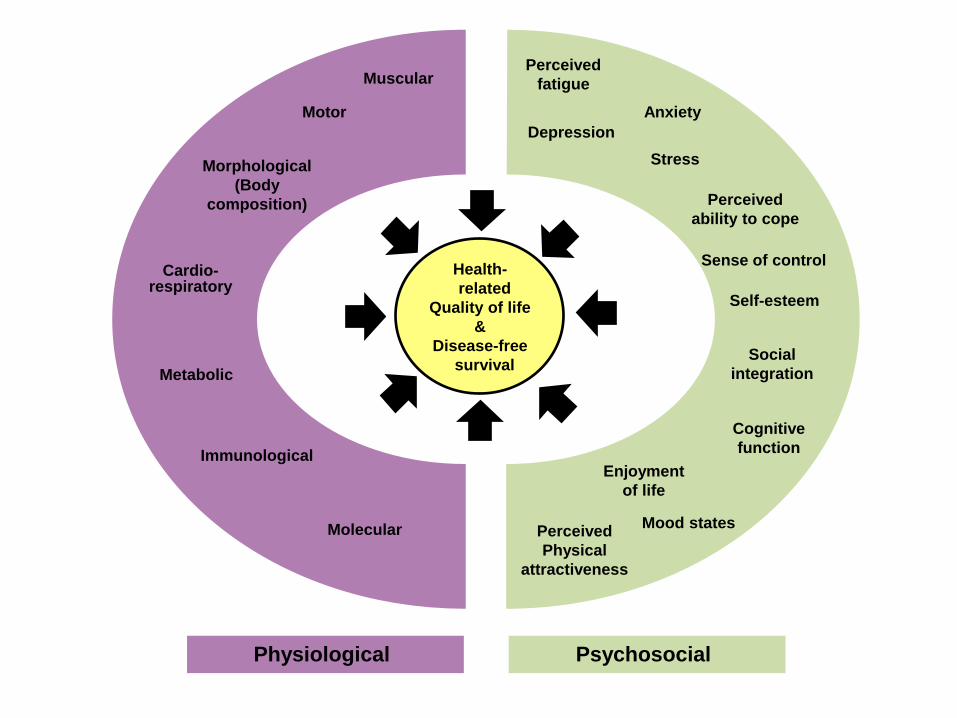
Health-
related
Quality of life
&
Disease-free
survival
Morphological
(Body
composition)
Cardio-respiratory
Metabolic
Motor
Immunological
Molecular
Muscular
Depression
Anxiety
Stress
Self-esteem
Cognitive
function
Mood states
Sense of control
Perceived
fatigue
Perceived
ability to cope
Perceived
Physical
attractiveness
Social
integration
Enjoyment
of life
Physiological Psychosocial
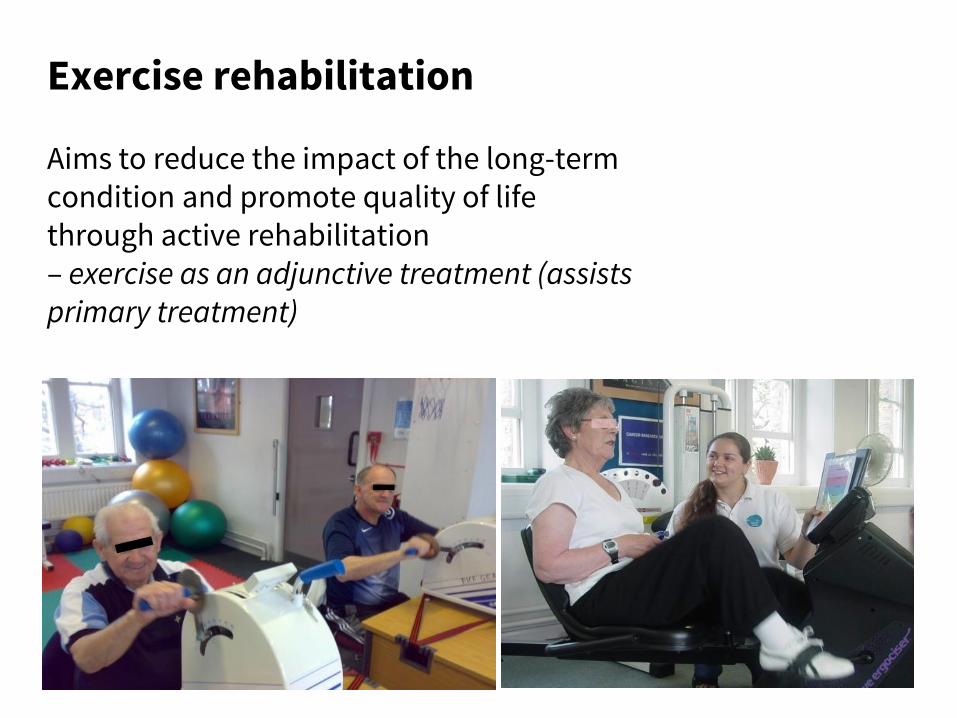
Exercise rehabilitation Aims to reduce the impact of the long-term condition and promote quality of life through active rehabilitation – exercise as an adjunctive treatment (assists primary treatment)
• How can exercise therapy be optimised (frequency, intensity, time type) to bring the greatest health or therapeutic benefits?
• What is the role of exercise therapy in disease modification?
• How does exercise therapy interact with drug treatments?
• Why do some people respond/adapt differently to exercise therapy?
• What are the contra-indications to exercise therapy?
Research questions
EXIMS – EXercise Intervention for people with MS A practical approach to providing accessible exercise training for people with MS
Purpose of EXIMS
• Long-term supervised (facility-based) exercise programmes are likely to prove difficult due to time barriers, transport issues and health constraints (e.g. fatigue) in PwMS.
• A major challenge is to develop pragmatic and cost-effective interventions that can safely engage PwMS in their preferred modes of exercise and provide robust evidence of a long-lasting impact on important health outcomes, such as quality of life and fatigue.
Randomised Controlled Trial Research Questions
• Can a practically-designed exercise intervention evoke long-term improvements in physical activity behaviour and important health outcomes, including quality of life and fatigue?
• Is this a cost effective treatment strategy?
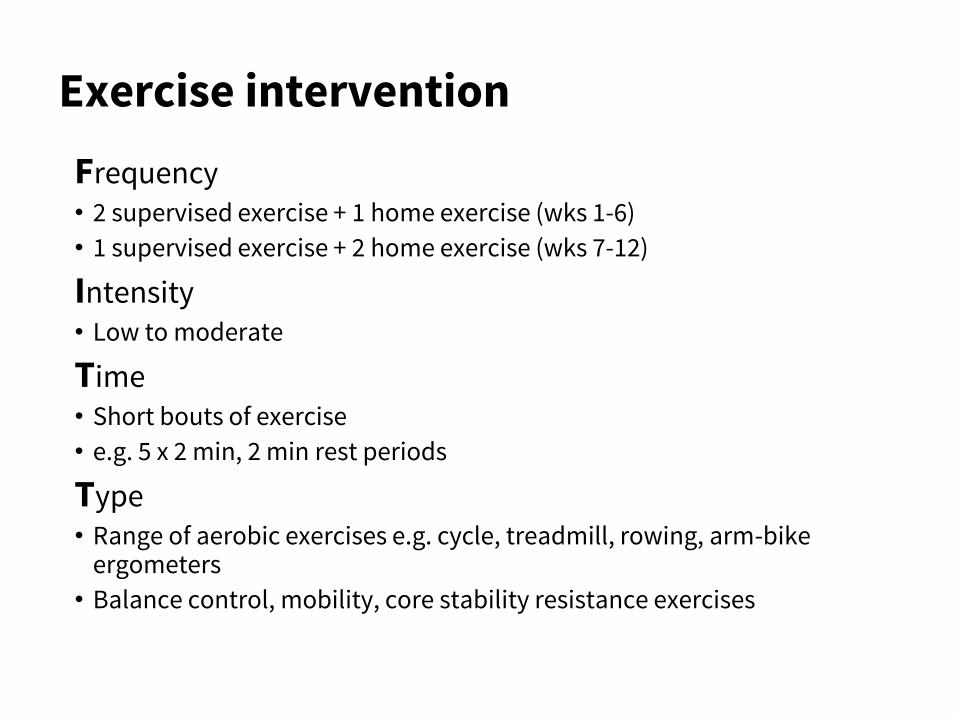
Frequency • 2 supervised exercise + 1 home exercise (wks 1-6)
• 1 supervised exercise + 2 home exercise (wks 7-12)
Intensity • Low to moderate
Time • Short bouts of exercise
• e.g. 5 x 2 min, 2 min rest periods
Type • Range of aerobic exercises e.g. cycle, treadmill, rowing, arm-bike
ergometers
• Balance control, mobility, core stability resistance exercises
Exercise intervention
Aerobic exercise
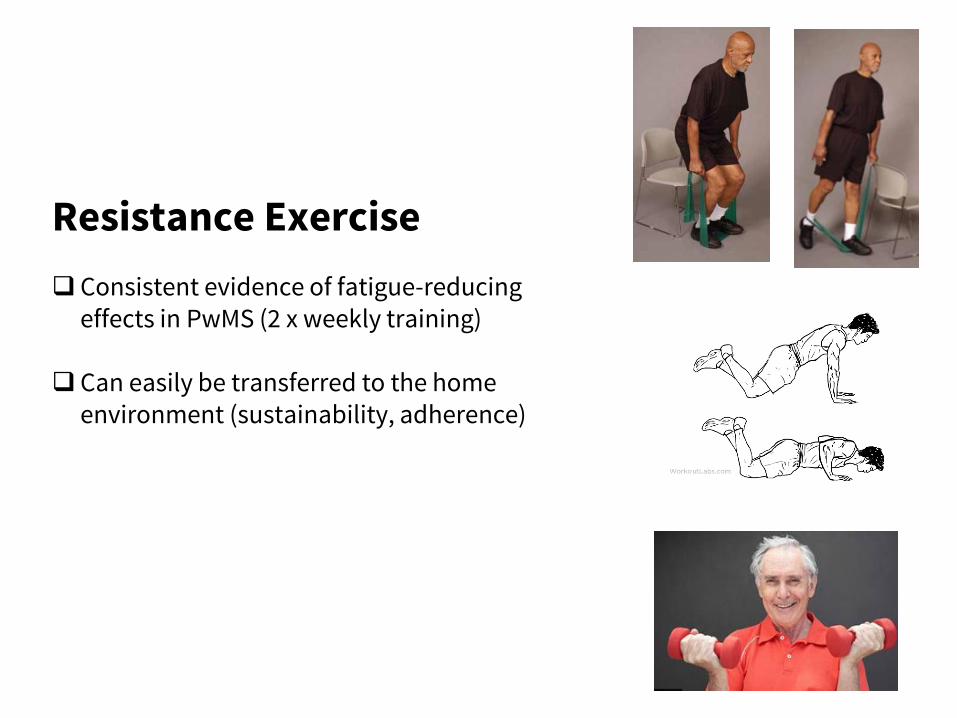
Resistance Exercise
Consistent evidence of fatigue-reducing effects in PwMS (2 x weekly training)
Can easily be transferred to the home environment (sustainability, adherence)
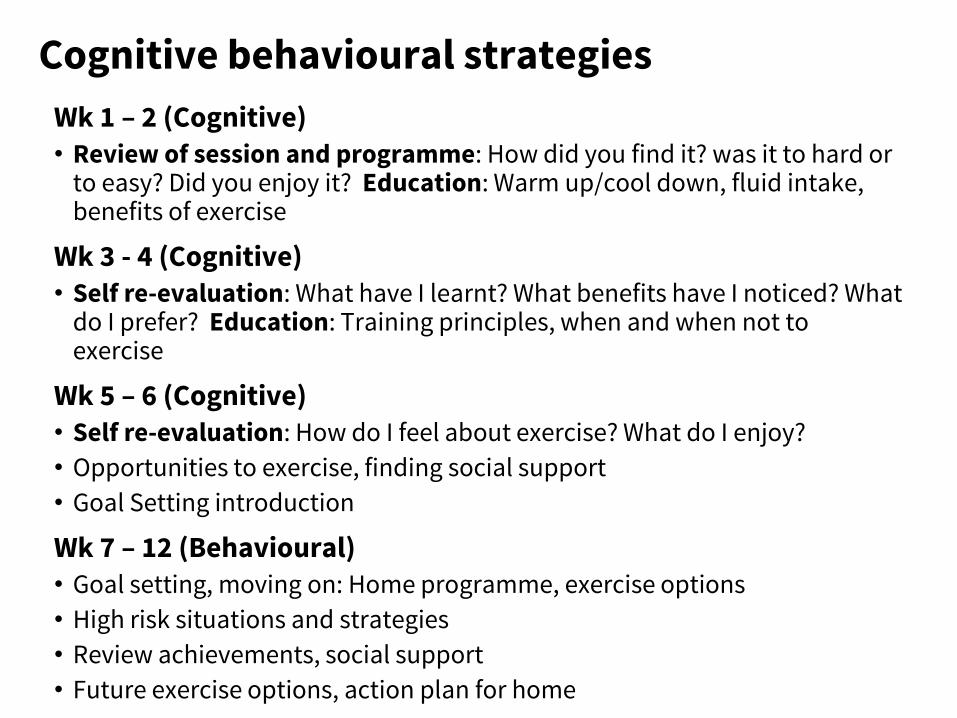
Wk 1 – 2 (Cognitive) • Review of session and programme: How did you find it? was it to hard or
to easy? Did you enjoy it? Education: Warm up/cool down, fluid intake, benefits of exercise
Wk 3 - 4 (Cognitive) • Self re-evaluation: What have I learnt? What benefits have I noticed? What
do I prefer? Education: Training principles, when and when not to exercise
Wk 5 – 6 (Cognitive) • Self re-evaluation: How do I feel about exercise? What do I enjoy?
• Opportunities to exercise, finding social support
• Goal Setting introduction
Wk 7 – 12 (Behavioural) • Goal setting, moving on: Home programme, exercise options
• High risk situations and strategies
• Review achievements, social support
• Future exercise options, action plan for home
Cognitive behavioural strategies
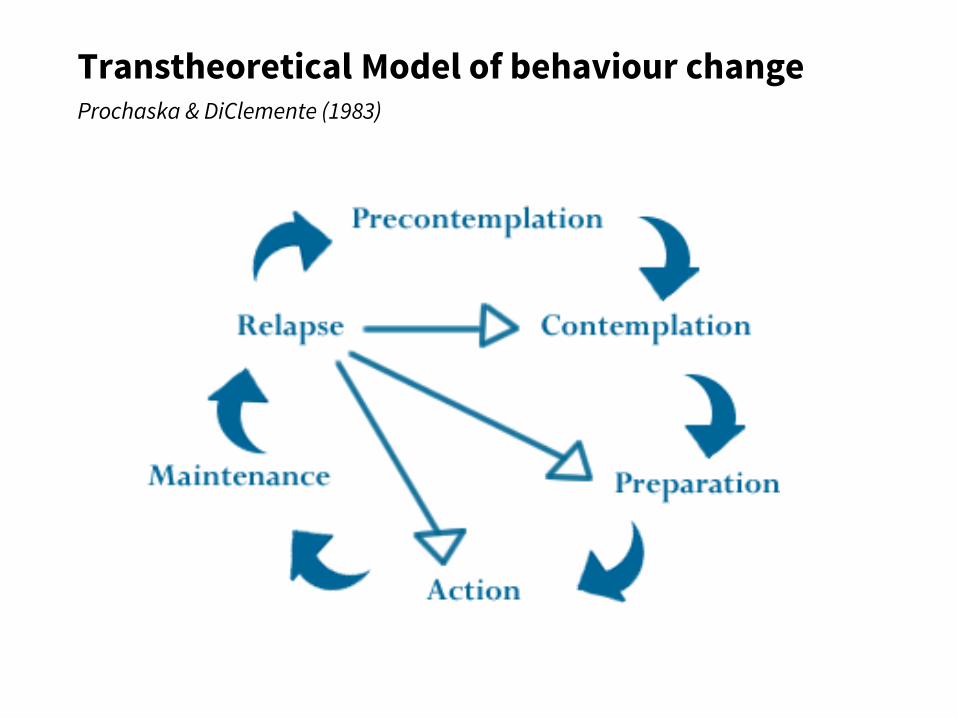
Transtheoretical Model of behaviour change Prochaska & DiClemente (1983)
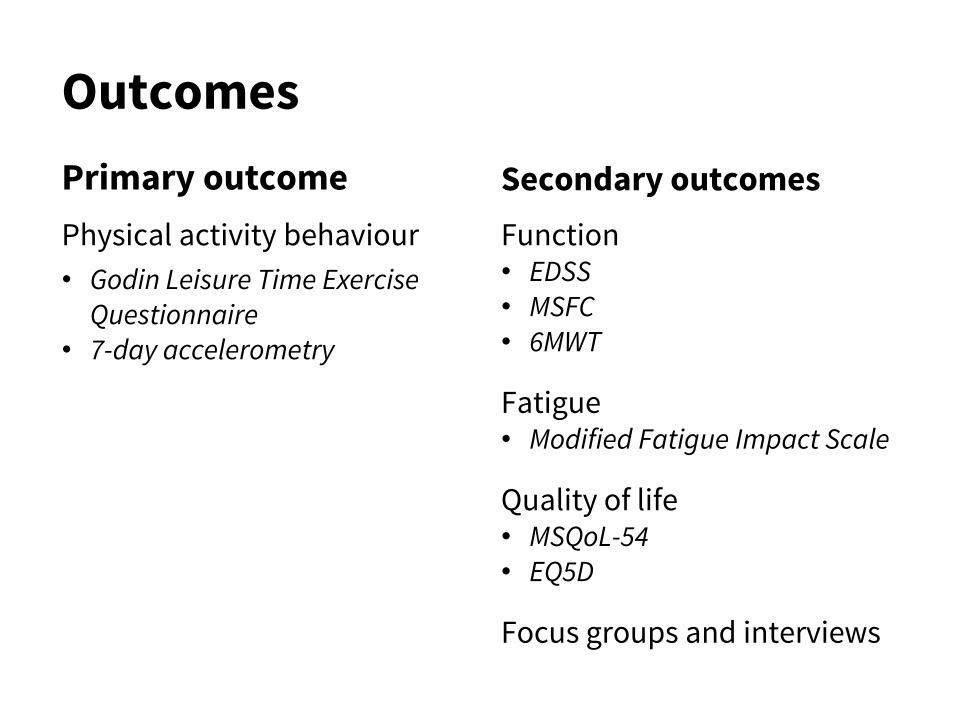
Outcomes
Primary outcome
Physical activity behaviour
• Godin Leisure Time Exercise Questionnaire
• 7-day accelerometry
Secondary outcomes
Function • EDSS • MSFC • 6MWT
Fatigue • Modified Fatigue Impact Scale
Quality of life • MSQoL-54 • EQ5D
Focus groups and interviews
Results
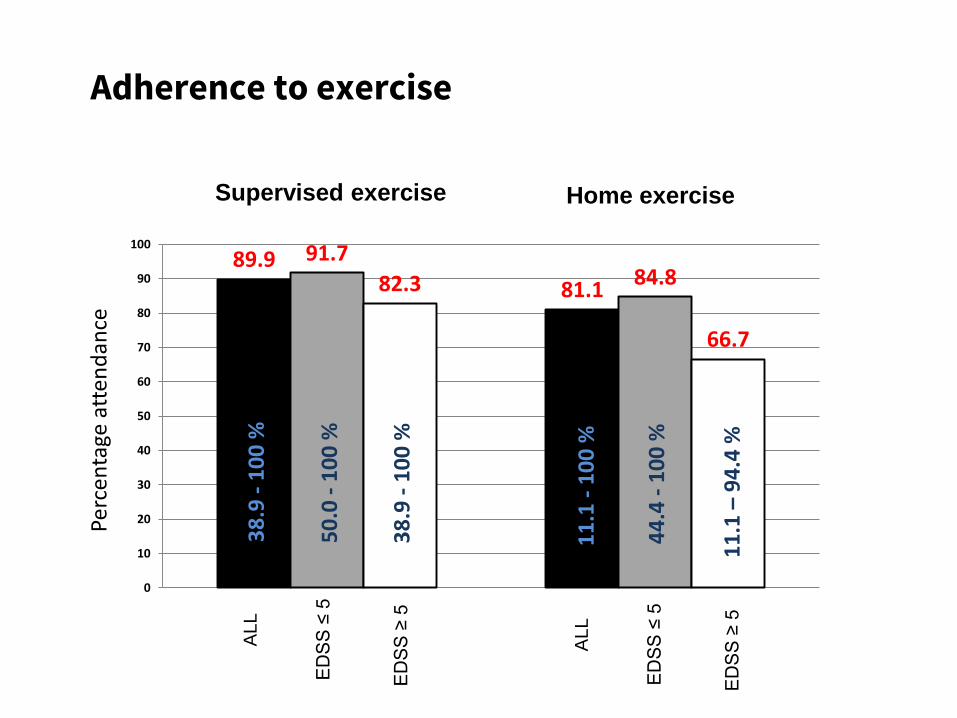
89.9
81.1
91.7 84.8 82.3
66.7
0
10
20
30
40
50
60
70
80
90
100
Adherence to exercise
ED
SS
≤ 5
ED
SS
≥ 5
AL
L
ED
SS
≤ 5
ED
SS
≥ 5
ALL
Supervised exercise Home exercise
38
.9 -
10
0 %
50
.0 -
10
0 %
38
.9 -
10
0 %
11
.1 -
10
0 %
44
.4 -
10
0 %
11
.1 –
94
.4 %
Perc
enta
ge a
tten
dan
ce
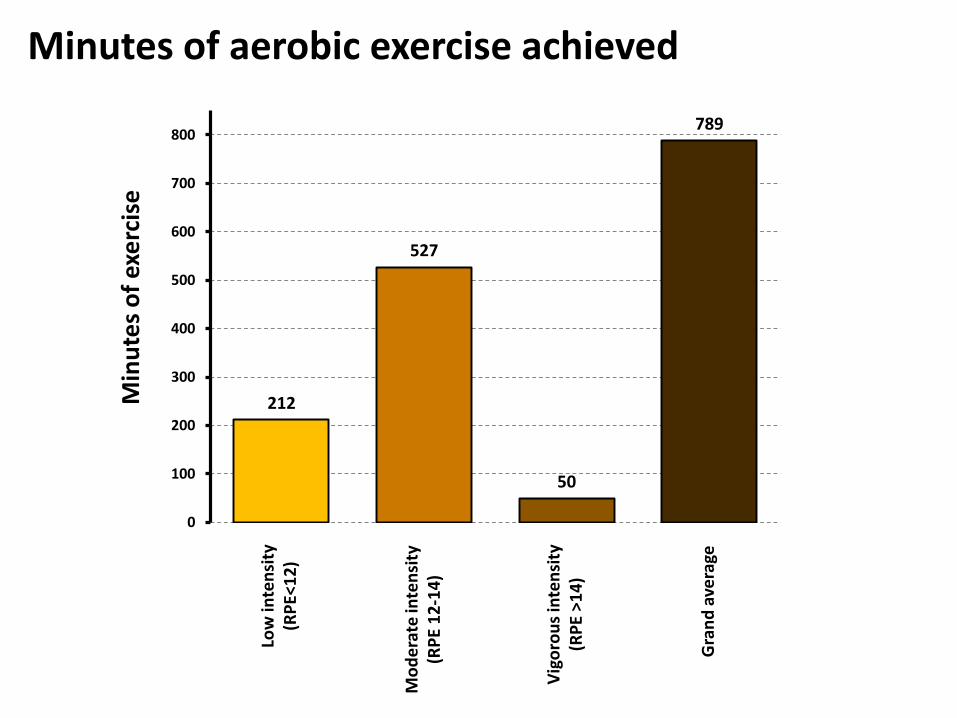
Minutes of aerobic exercise achieved
Low
inte
nsi
ty
(RP
E<1
2)
Mo
de
rate
inte
nsi
ty
(RP
E 1
2-1
4)
Vig
oro
us
inte
nsi
ty
(RP
E >
14
)
Gra
nd
ave
rage
Min
ute
s o
f ex
erc
ise
212
527
50
789
0
100
200
300
400
500
600
700
800
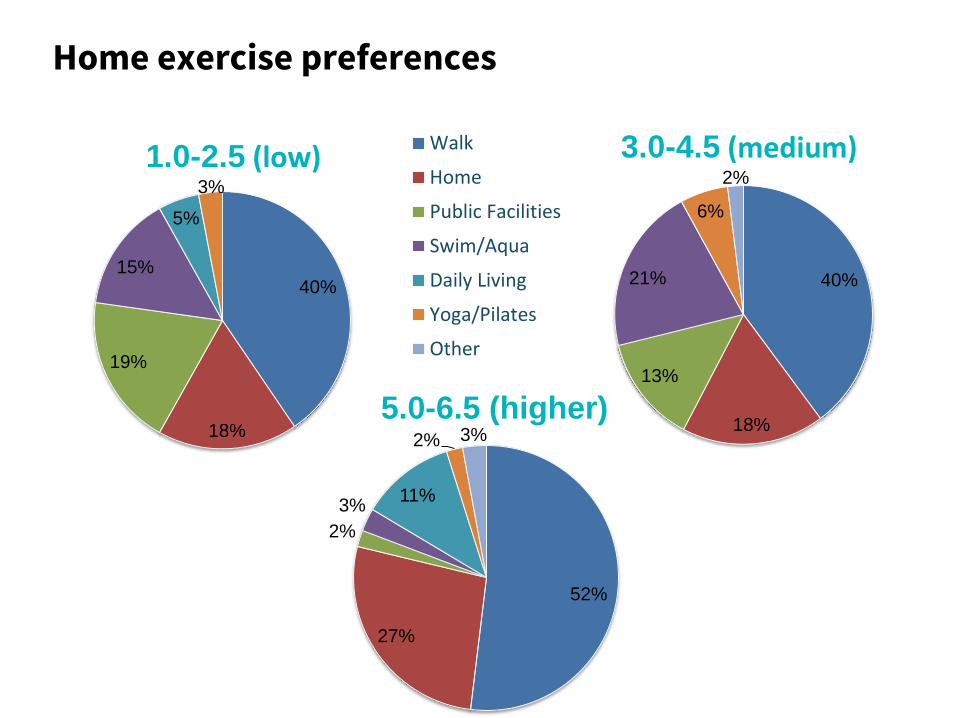
40%
18%
19%
15%
5%
3%
1.0-2.5 (low) Walk
Home
Public Facilities
Swim/Aqua
Daily Living
Yoga/Pilates
Other
40%
18%
13%
21%
6%
2%
3.0-4.5 (medium)
52%
27%
2%
3% 11%
2% 3%
5.0-6.5 (higher)
Home exercise preferences
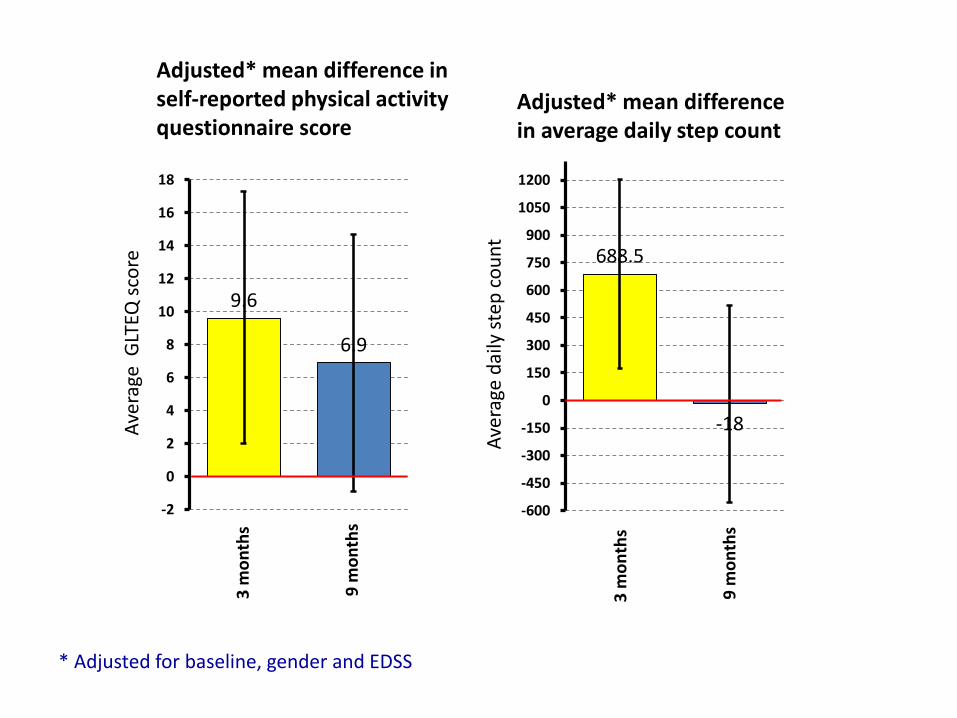
9.6
6.9
-2
0
2
4
6
8
10
12
14
16
18
688.5
-18
-600
-450
-300
-150
0
150
300
450
600
750
900
1050
1200
Adjusted* mean difference in self-reported physical activity questionnaire score
Adjusted* mean difference in average daily step count
3 m
on
ths
9 m
on
ths
3 m
on
ths
9 m
on
ths
* Adjusted for baseline, gender and EDSS
Ave
rage
GLT
EQ s
core
Ave
rage
dai
ly s
tep
co
un
t
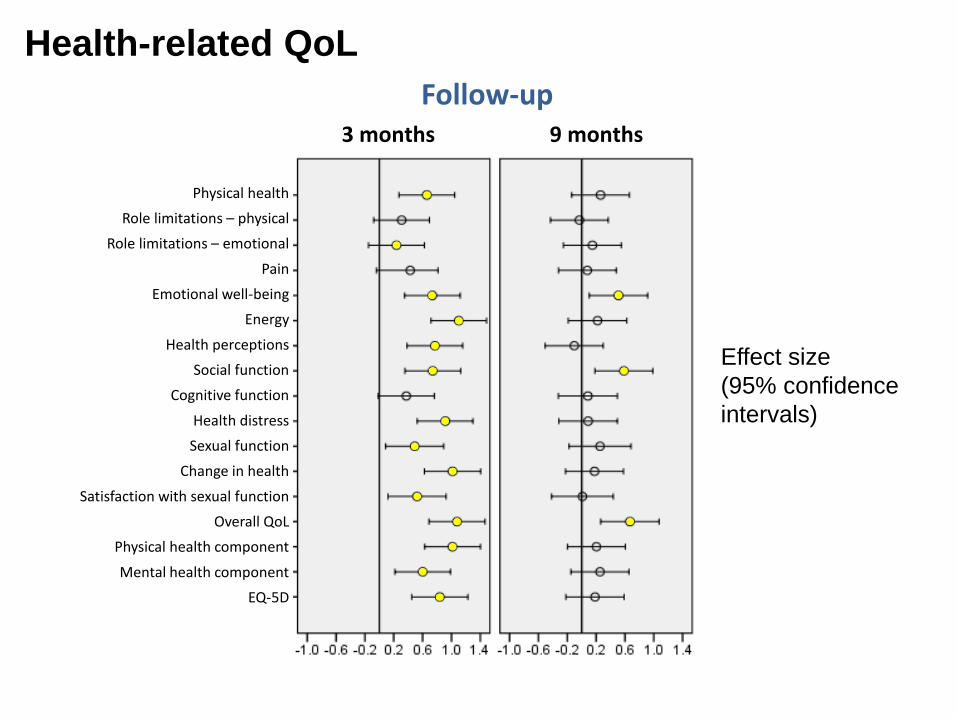
Physical health
Role limitations – physical
Role limitations – emotional
Pain
Emotional well-being
Energy
Health perceptions
Social function
Cognitive function
Health distress
Sexual function
Change in health
Satisfaction with sexual function
Overall QoL
Physical health component
Mental health component
EQ-5D
Effect size
(95% confidence
intervals)
Follow-up 3 months 9 months
Health-related QoL
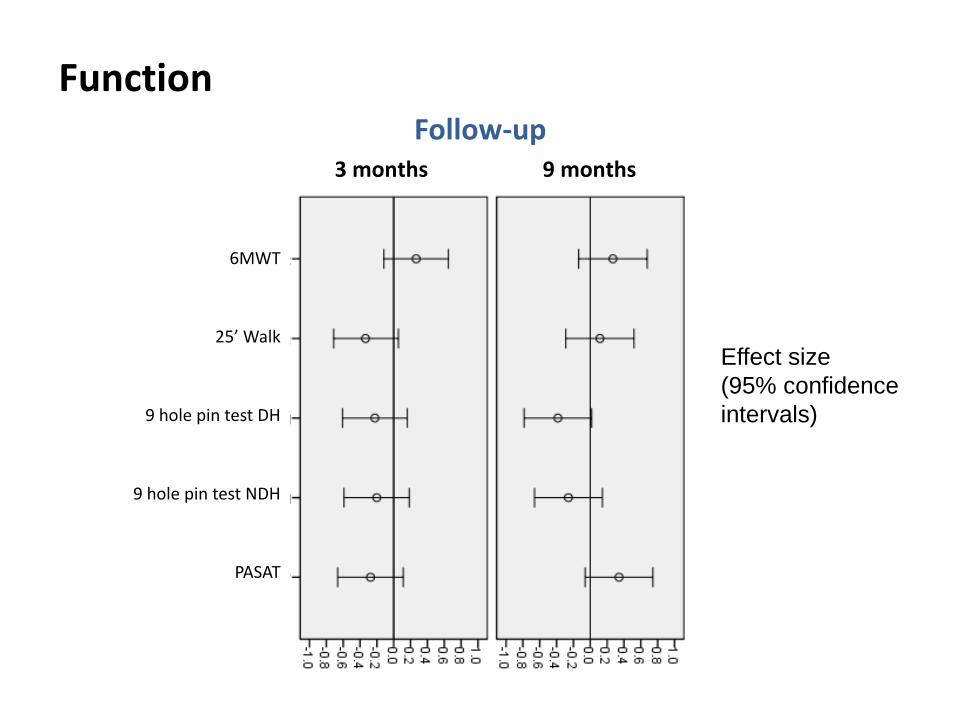
Function
6MWT
25’ Walk
9 hole pin test DH
9 hole pin test NDH
PASAT
Effect size
(95% confidence
intervals)
Follow-up 3 months 9 months
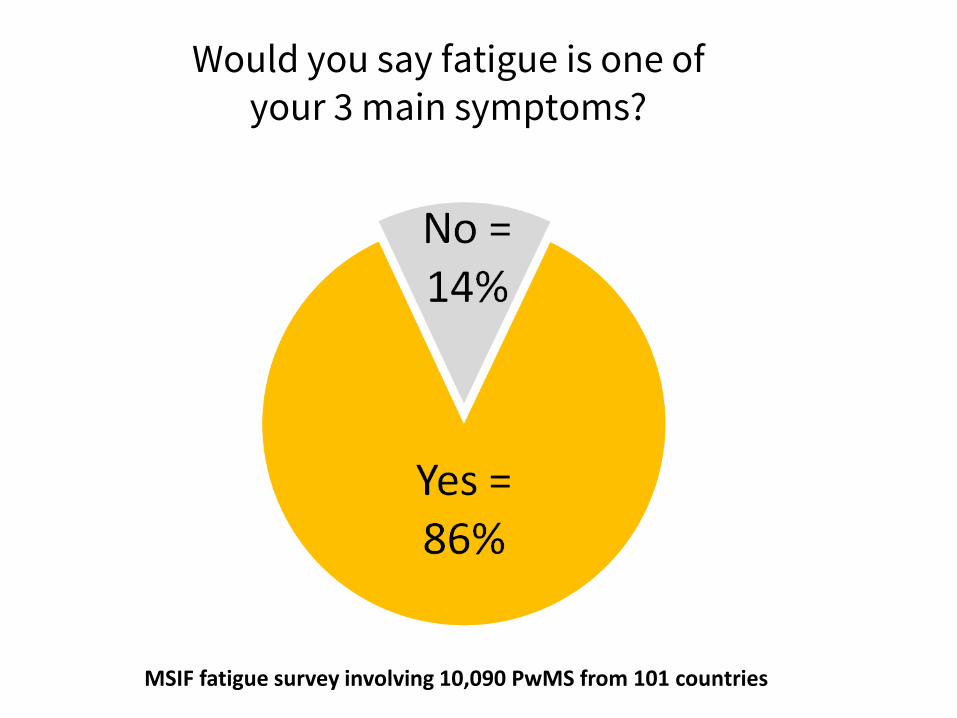
Would you say fatigue is one of your 3 main symptoms?
MSIF fatigue survey involving 10,090 PwMS from 101 countries
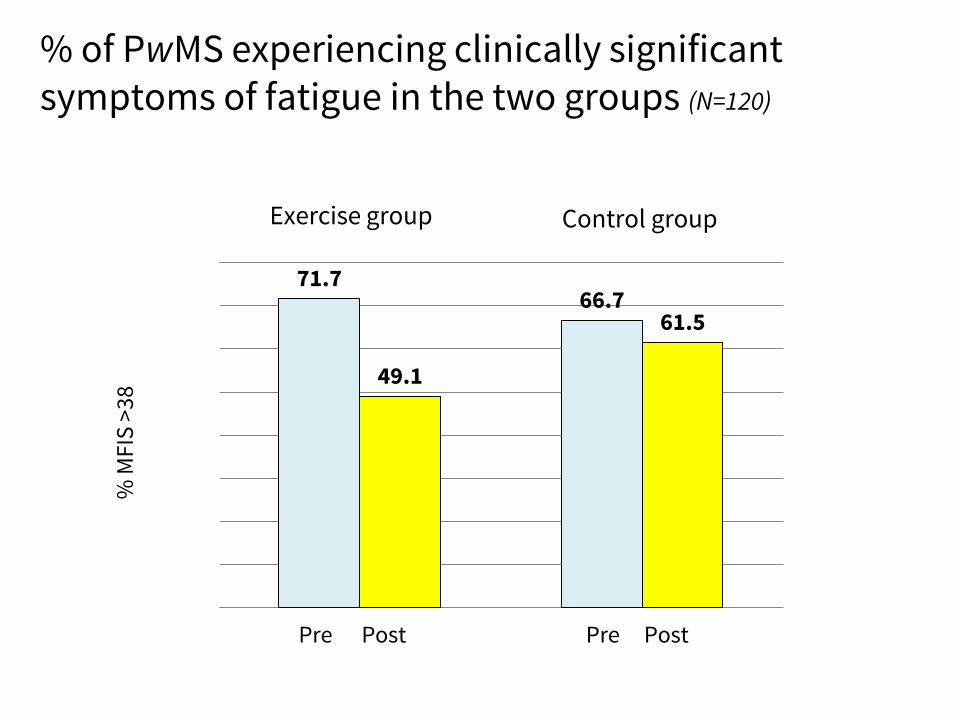
Exercise group Control group
Pre Post Pre Post
% of PwMS experiencing clinically significant symptoms of fatigue in the two groups (N=120)
71.7 66.7
49.1
61.5
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
% M
FIS
>3
8

Focus Groups & Structured Interviews
Participant quotes
“When I was diagnosed I asked specifically if there was anything I could do to help myself, diet wise and exercise and I was told there was nothing you could whatsoever”
“I don't recall any professionals mentioning anything about exercise at all and I don't believe I asked”
“You have no advice
really. So you were
scared about doing
the wrong thing ...”
Experience of MS exercise-related advice and support
Variable experiences, usually non-existent advice or non-specific to MS
“I did enjoy coming and I am the kind of person that will stick to an arrangement I've made. I will stick to a commitment”
“... Just everything about it, I just enjoyed coming so much. I looked forward to it”
“ Very good. I
needed it”
Participant's views of taking part in the EXIMS study
Generally grateful to have had the opportunity to take part in the exercise programme
“I think when you've got MS you put, your world becomes smaller, you think "I can't do that, I might feel tired before I get far", and then you realise that you can”
“I feel as though I'm less fatigued. I don't have as many floppy days. I still get the odd one but nowhere near like it was”
“I do find simple things
like turning over in bed
which isn’t a very easy
task and picking things
up of the floor without
collapsing; things of that
nature are a lot easier”
Perceived benefits of exercise participation Commitment and discipline needed but a worthwhile investment
FATIGUE PHYSICAL BENEFITS
OUTLOOK
“For me I think it was taking the mystery out of exercise and giving the confidence that it’s safe to do this and you’ll get benefit from it...and I think guided exercise in the initial stages was the key”
“My little boy will be surprised when I say "Yeah, alright I'll go swimming" or "yeah OK let's go for a walk", and he'll think "Oh, that doesn't sound quite right".
“I really enjoyed the social
aspect of meeting people
and talking because you
don't always get that when
you have MS. You tend to
be at home a lot on your
own so I enjoyed coming
and I miss not coming”
FAMILY IMPACT
CONFIDENCE
SOCIAL IMPACT
Perceived benefits of exercise participation
Low EDSS (1.0 - 2.5)
more confident, more motivated, stronger, fitter, less tired, feel more alive and positive, walking more
Medium EDSS (3.0 - 4.5)
fitter, more energy and enthusiasm, less fatigued, improved stamina, walking further, better balance
Higher EDSS (5.0 - 6.5)
more confident, better mobility, fitter, stronger legs, functional improvements (standing, sitting, stairs, getting up off floor), feel better, healthier, more energy
Participant perceptions by EDSS score
Conclusions Physical activity and health outcomes
• EXIMS had a positive impact on self-reported physical activity and objectively assessed movement counts at 3 months (non-significant increase in self-reported physical activity at 9 months).
• EXIMS reduced physical, cognitive and psychosocial fatigue symptoms at 3 months.
• EXIMS improved most HRQoL dimensions at 3 months, with sustained enhancements in emotional wellbeing, social function and overall QoL score at 9 months.
• The improvements in fatigue and other HRQoL dimensions observed in the EXIMS group at 3 months were not maintained to 9 months.
Acknowledgements MS Society
Research staff •Anouska Carter •Liam Humphreys •Robert Scaife •Nicky Snowdon
Co-investigators and Trial Steering Committee members •Amanda Daley •Basil Sharrack •Nicola Woodroofe •Jane Petty & Liz Whilde •Andrea Roalfe •Jon Tosh & Simon Dixon •Rachel Milner & Amber Sheridan
•Howard Capelin & James Bramel
Consultant Neurologists involved in recruitment •Sian Price
•Stephen Howell
Lack of activity destroys the good condition of every human being, while movement and methodical physical exercise save it and preserve it.
Plato 428-347 B.C.
The End